
One of the cornerstones of PEPFAR has been making a major investment in meeting the tremendous challenge of supporting and scaling up services for HIV care and treatment in countries with limited resources and infrastructure and a high burden of disease. The congressional charge for this evaluation, as laid out in the Lantos-Hyde Act of 2008, requested an evaluation of the impact of treatment and care efforts on health, including an assessment of progress toward treatment and care targets and an evaluation of the effects of treatment and care programs on survival rates, drug adherence, and the emergence of drug resistance.1
This chapter describes the committee’s assessment of PEPFAR’s support for testing, care, and treatment services together, as part of a continuum of access to and delivery of HIV-related services (see Figure 6-1) (Das, 2011; Eldred and Malitz, 2007; Gardner et al., 2011; IOM, 2012). All along this continuum there are interventions and efforts supported by PEPFAR: testing and diagnosis as the entry point into care and treatment services; referrals and linkages to care services; the provision of clinical care services, nonclinical support services, and monitoring for those not eligible for antiretroviral therapy (ART); the initiation of ART for those who are eligible; maintenance and retention on ART with the continuation of non-ART clinical care and nonclinical support services; and monitoring for treat-
__________________
1 Tom Lantos and Henry J. Hyde United States Global Leadership Against HIV/AIDS, Tuberculosis, and Malaria Reauthorization Act of 2008, P.L. 110-293, 110th Cong., 2nd sess. (July 30, 2008), ![]() 101(c), 22 U.S.C. 7611(c)(2).
101(c), 22 U.S.C. 7611(c)(2).
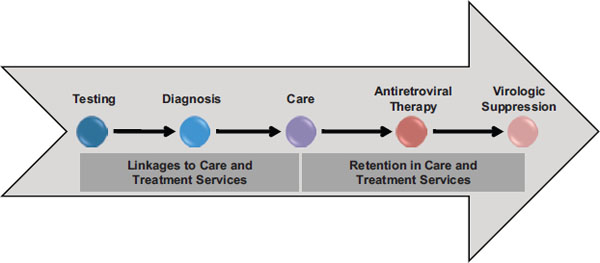
FIGURE 6-1 Implementation cascade for the continuum of care.
SOURCE: Adapted from Das, 2011, and IOM, 2012.
ment failure with the initiation of second-line treatment as needed. This chapter describes the committee’s assessment of PEPFAR’s efforts, focused on its activities to support the scale-up of service delivery, in each of the components of this continuum sequentially, providing for each some brief background and then following the program impact pathway framework of inputs, activities, and, to the extent possible, outcomes and impact of PEPFAR’s efforts.
The continuum of care described here is directed toward virological suppression and improved health, well-being, and survival for individuals who are HIV positive; however, another ultimate goal of the HIV response is a population-level reduction of the burden of HIV and of mortality due to HIV/AIDS. The contribution of PEPFAR to this aim, to the extent that it can be assessed, is discussed at the end of this chapter.
Although this chapter will focus on PEPFAR’s support for the provision of testing, care, and treatment services, it is also important to note that this continuum for care and treatment intersects with other services supported by PEPFAR programming and other opportunities where PEPFAR has a role in facilitating an effective response as well as where interrelated challenges that affect care and treatment can arise. These other program areas are discussed elsewhere in this report, including prevention services (Chapter 5), programs for orphans and vulnerable children (Chapter 7), and efforts to address gender-specific aspects of HIV (Chapter 8). Along with the intersection with these other services, care and treatment programs also are inextricably linked to elements of the health system, including infrastructure, commodities and supply chain, workforce, management, leadership, and financing that are required to support service delivery; these areas are
touched upon only briefly in this chapter, while the primary discussion can be found in Chapter 9 on health systems strengthening. Finally, a multisectoral response to HIV also relies on other, non-health systems and operates in the broader context of the economic, social, cultural, and political environments, which are all part of the broader context of a multisectoral response to HIV. This broader context both contributes to and poses challenges for the effectiveness of the HIV response.
Early in the HIV epidemic, voluntary HIV testing programs were intended to increase the number of people aware of their HIV status and to serve as an entry point for counseling and other prevention services, both for those who were HIV positive and those who were HIV negative, with the aim of reducing HIV transmission and infection. Early programs faced such challenges as the fear of stigma and discrimination, complex laboratory methods, and a lack of available care and treatment services. With the introduction of more widespread access to care and treatment services and support for laboratory and other related services, HIV testing now serves as a crucial gateway to HIV care and treatment and to services for the prevention of mother-to-child transmission (PMTCT), while still serving the initial major purpose of providing counseling and an entry point to prevention services (Marum et al., 2012). Access to testing early in the course of HIV infection is of particular importance given that people living with HIV (PLHIV) who receive treatment later in their disease consequently have poorer outcomes (WHO, 2012d).
The following section presents the committee’s assessment of PEPFAR-supported HIV counseling and testing programs, with information on PEPFAR’s funding history and activities as well as on the effects of these activities, including achievements and challenges. This section focuses primarily on testing services because it was difficult to comprehensively assess the effects of counseling services, such as discussions that take place before and after an HIV test with the purpose of increasing knowledge, conveying prevention and risk reduction messages, providing supportive counseling, and facilitating referrals to services. There is very little information available to track this component of counseling and testing in terms of how PEPFAR-supported activities have been implemented and what the outcomes of these activities have been.
PEPFAR Guidance for Supported Activities for Counseling and Testing
PEPFAR does not issue specific programmatic guidance on counseling and testing, but instead refers programs to the World Health Organization
(WHO) standards. PEPFAR provides operational guidance in its annual Country Operational Plan (COP) guidance (OGAC, 2011a,b). HIV counseling and testing is part of the package of services in a range of PEPFAR technical areas, including medical male circumcision, prevention for PLHIV, preventing mother-to-child transmission, services for populations at high risk, adult treatment, care and support, pediatric treatment, and tuberculosis (TB) services. Guidance for counseling and testing was also included in PEPFAR’s recent Guidance for the Prevention of Sexually Transmitted HIV Infections (OGAC, 2011c).
The available guidance includes HIV testing and counseling provided through both client-initiated approaches and provider-initiated approaches and describes a range of settings for counseling and testing, such as health facilities (e.g., antenatal clinics, TB clinics, and outpatient clinics); stand-alone counseling and testing sites; and home-based, mobile, and outreach programs, including special events, campaigns, and promotional activities to create demand. Related activities may include training or refresher training in areas such as retesting recommendations, couples counseling and testing, and quality assurance; strengthening and monitoring referrals and linkages, including tracking or follow-up of HIV-positive individuals not enrolling in care or treatment services; and activities for quality assurance of both testing and counseling. For planning activities through implementing partners, the guidance also states that target populations should be specified along with information, if available, on the HIV prevalence and testing coverage in those populations and that the linkages should be specified between testing and services in other technical areas (OGAC, 2011a,b,c).
PEPFAR Funding History for Counseling and Testing
PEPFAR’s funding for counseling and testing is captured in a single budget code. Figure 6-2 shows the funding over time in this budget code in both the dollar amount and as a proportion of all PEPFAR funding. The total for this budget code increased substantially over time during the first phase of PEPFAR, then leveled off starting in FY 2008 at just more than $200 million per year (OGAC, 2005, 2006g, 2007c, 2008b, 2010c, 2011d,e).
Effects of PEPFAR-Supported HIV Testing
PEPFAR Testing Indicator Data: Targets and Results
PEPFAR has limited central reporting of indicators to provide information about the performance of its testing programs. The primary indicator is an overall output indicator that captures the number of individuals who re-
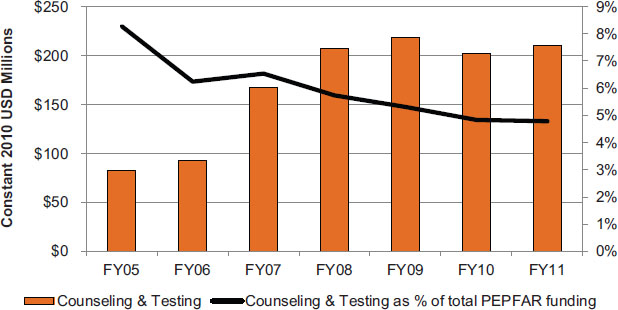
FIGURE 6-2 Planned/approved funding over time for counseling and testing services.
NOTES: This figure represents funding for all PEPFAR countries as planned/approved through PEPFAR’s budget codes. The budget codes are the only available source of funding information disaggregated by type of activity, and are therefore used in this report as the most reasonable and reliable approximation of PEPFAR investment by programmatic area. Data are presented in constant 2010 USD for comparison over time. Currently, funding for testing and counseling in the context of PMTCT can be included under the PMTCT budget code or the Counseling and Testing budget code, and so some investment in testing in that context may not be reflected here. Similarly, funding for testing and counseling in the context of tuberculosis (TB) services is under the TB/HIV budget code and is not reflected here (OGAC, 2010b). See Chapter 4 for a more detailed discussion of PEPFAR’s budget codes and the available data for tracking PEPFAR funding.
SOURCES: OGAC, 2005, 2006g, 2007c, 2008b, 2010c, 2011d,e.
ceived counseling and testing for HIV and who received test results (OGAC, 2007b, 2009d). Table 6-1 shows that the number tested with the support of PEPFAR has increased notably over time and that since the initial year of implementation the annual target has been consistently met or exceeded.
| FY 2004 | FY 2005 | FY 2006 | FY 2007 | FY 2008 | FY 2009 | FY 2010 | |
| Result | 1.3 | 2.5 | 5.1 | 9.3 | 16.4 | 21.2 | 32.7 |
| Target | — | 2.6 | 4.8 | 6.1 | 9.0 | 13.2 | 25.8 |
| % of Target | — | 96 | 106 | 153 | 182 | 160 | 127 |
NOTES: This table represents data for the 31 countries identified as the focus of this evaluation (see Chapter 2). Results and targets for FY 2004–FY 2009 correspond to OGAC indicator 9.2 (direct) (OGAC, 2007b). Results and targets for FY 2010 correspond to OGAC indicator P11.1.D (OGAC, 2009d).
SOURCE: Program monitoring indicators provided by OGAC.
Challenges in Monitoring of Testing Services
The monitoring of testing services and outcomes affects planning and management not only for testing services but also for other target areas that are dependent on the estimates of the numbers of people identified as living with HIV. There are a number of challenges in the accurate monitoring of testing services, especially where there are not unique patient identifiers. In tracking the number of individuals who have received testing services, for example, there is the potential for double counting of testing clients, some of whom may be accessing testing services repeatedly, either because of a lack of confidence in the results or because they have tested negative but are getting tested periodically because of high, ongoing, or new risks of exposure. In addition, without unique identifiers it is difficult to track whether individuals are being successfully referred for additional services once they have received their test results; the data are largely cross-sectional and do not allow for longitudinal individual follow-up. These challenges were identified by interviewees in several countries, who described that patients will be tested more than once, will go to more than one community to be tested, or will hide previous testing (587-18-PCGOV; 587-2-USG; 587-9-USG; 331-23-USNGO; 461-16-USG).2 The lack of unique identifiers for the people tested makes it difficult to adjust reported numbers appropriately (461-16-USG; 587-2-USG), and also poses a challenge for tracking whether people reach care and treatment programs after being tested (116-9-PCNGO; 587-3-USG; 461-7-PCNGO; 587-13-USG; 396-21-USG). Other issues that interfere with the collection of quality data on testing services, as identified by interviewees in various countries, are the use of different counseling and testing reporting systems by PEPFAR and the national system (587-9-USG) and the practice of only registering those who test positive in patient-tracking databases (272-21-PCNGO).
PEPFAR Achievements in the Scale-Up of Testing
WHO estimates indicate that there has been an increase in the numbers and proportion of individuals in PEPFAR partner countries who are aware of their HIV status (WHO, 2012f; WHO et al., 2011), which is consistent with the considerable expansion of HIV testing through the implementa-
__________________
2 Country Visit Exit Synthesis Key: Country # + ES Country Visit Interview Citation Key: Country # + Interview # + Organization Type Non-Country Visit Interview Citation Key: “NCV” + Interview # + Organization Type Organization Types: United States: USG = U.S. Government; USNGO = U.S. Nongovernmental Organization; USPS = U.S. Private Sector; USACA = U.S. Academia; Partner Country: PCGOV = Partner Country Government; PCNGO = Partner Country NGO; PCPS = Partner Country Private Sector; PCACA = Partner Country Academia; Other: CCM = Country Coordinating Mechanism; ML = Multilateral Organization; OBL = Other (non-U.S. and non-Partner Country) Bilateral; OGOV = Other Government; ONGO = Other Country NGO.
tion of PEPFAR-supported services. Although challenges related to HIV testing remain (discussed later in this chapter), interviewees in the countries visited for this evaluation overall considered PEPFAR’s efforts in testing a success that has led to increased access to testing and counseling services, with the result that many more individuals have learned their HIV status and, if positive, have been linked to clinical services. Interviewees in several countries observed that before PEPFAR there had been no counseling and testing program, or, if available, it had existed on only on a small scale with few facilities to provide this service and the uptake of counseling and testing was low (240-2-USG; 396-23-USG; 116-16-PCGOV). PEPFAR has helped partner countries initiate counseling and testing programs and scale up the number of facilities and other venues providing this service (461-14-USG; 396-23-USG; 116-16-PCGOV; 272-ES; 331-32-PCNGO; 935-17-USG; 240-2-USG). As a contribution to this scale-up, PEPFAR has not only supported testing services but has also helped develop guidelines related to counseling and testing, promoted the implementation of innovative approaches and emergent testing methods, and advocated for more aggressive policies for HIV testing in the setting of not only high-prevalence countries but also concentrated epidemics (196-11-USNGO; 396-23-USG; 272-13-USG; 542-8-USNGO; 396-23-USG; 331-18-USNGO). By supporting activities related to the scale-up of testing PEPFAR has also contributed to increased public awareness of both HIV and the availability of HIV counseling and testing in partner countries. Awareness efforts have involved a variety of strategies and settings, such as the use of hotlines, national testing initiatives, drop-in centers, health fairs, posters, and media channels as well as the engagement of peer educators, worksites and employers, community service organizations, and faith-based organizations (587-14-PCGOV; 166-5-USG; 331-7-PCNGO; 331-22-PCNGO; 396-32-PCGOV; 196-20-PCNGO; 166-14-PCNGO; 240-2-USG; 272-24-USG; 587-8-PCGOV; 636-6-USG; 636-17-PCGOV; 331-38-USPS; 934-17-PCGOV; 331-22-PCNGO; 396-12-USG; 396-44-PCGOV; 196-23-PCNGO).
Evolution of Testing Approaches Over Time
In scaling up testing services, PEPFAR has supported both client-initiated approaches and, increasingly over time, provider-initiated approaches. Initially most PEPFAR-supported testing was client-initiated testing based in separate testing facilities; later the integration of testing with other key services was recognized as a way to facilitate access to and provide a less stigmatized environment for HIV testing and efforts were made toward more integration with, for example, antenatal care, child health programs, primary health care, and TB services (272-24-USG; 331-28-PCGOV; 272-24-USG; 587-5-PCGOV; 636-17-PCGOV; 396-18-USG). As another way to increase the access to and availability of HIV testing, PEPFAR moved to implement more client-initiated testing services outside of facilities. These approaches include home-based testing, testing in community settings, and testing in
mobile clinics (116-12-PCNGO; 116-13-PCNGO; 331-11-PCNGO; 461-7-PCNGO; 461-24-PCNGO; 935-17-USG; 240-2-USG). Interviewees identified these approaches as ways to expand testing, allow for earlier detection of HIV, and facilitate access to testing and referrals to services for specific populations at high risk, including those who are highly mobile or transient (166-13-PCGOV; 542-11-PCNGO; 935-17-USG; 542-14-PCGOV; 396-44-PCGOV; 196-25-PCNGO). Home-based counseling and testing has been implemented on an increasingly larger scale recently in several countries, and interviewees pointed to the initial achievements of adopting a home-based approach as an indication of this approach’s potential to better integrate HIV treatment and prevention and to reach more couples, especially male partners (935-17-USG; 461-7-PCNGO; 116-12-PCNGO).
In addition to expanding client-initiated testing services, as the adoption of provider-initiated counseling and testing (PICT) emerged globally (Marum et al., 2012; WHO and UNAIDS, 2007), PEPFAR widely supported its implementation in partner countries in both outpatient and inpatient health facilities (935-17-USG; 116-12-PCNGO; 240-8-USG; 272-24-USG; 240-24-USG). This approach was encouraged as another means to increase access to testing; to improve coverage in facility-based testing in general; and to reduce missed opportunities to test those patients who present to health facilities under circumstances where there is reason to consider them at high risk for HIV, such as TB patients or patients hospitalized with illnesses that could be due to opportunistic infections (196-11-USNGO; 196-17-PCGOV; 934-21-PCGOV; 935-17-USG). In addition to PEPFAR’s support of PICT in PEPFAR-supported service delivery, interviewees also mentioned PEPFAR’s contributions to the inclusion of PICT in the national strategy, the scaling up of training for PICT to the national level, and the development of training guidelines (196-11-USNGO; 636-6-USG).
Targeted Testing
Interviewees highlighted several efforts to target vulnerable or difficult-to-serve populations for counseling and testing. In addition to the above-mentioned use of targeted community-based and mobile testing to reach populations at high risk, interviewees offered such examples of specific efforts as a campaign to offer counseling and testing services in locations and at times that guarantee privacy for men who have sex with men, night-time mobile testing services to reach sex workers and their clients, a referral system for sex workers to increase their access to testing, efforts to improve referrals and access to testing services specifically for women who inject drugs, and mobile outreach services that include testing for street children (396-44-PCGOV; 196-25-PCNGO; 935-17-USG; 935-16-USNGO; 331-22-PCNGO; 542-11-PCNGO; 196-24-PCNGO; 542-14-PCGOV). PEPFAR’s support for services for these populations is discussed in more depth in Chapter 5 on prevention and Chapter 8 on gender.
Another important population for counseling and testing is pregnant women; reaching this population ideally provides an entry point into both services for PMTCT and care and treatment services for women who are HIV positive. Interviewees noted PEPFAR’s achievements in the effort to reach pregnant women with HIV testing, especially in antenatal clinics and in the health facilities where they give birth. Interviewees said that pregnant women are increasingly likely to be offered and to accept testing for HIV when receiving antenatal care, particularly during their first antenatal visit (166-5-USG; 331-28-PCGOV; 166-27-PCNGO; 587-5-PCGOV; 636-22-PCNGO; 636-1-USG; 636-6-USG). Despite the relative success and progress in testing for this population, interviewees emphasized that coverage gaps remain, especially for pregnant women who do not make a visit to antenatal care clinics or to facilities for delivery (240-ES; 240-2-USG; 240-13-PCGOV; 240-19-USACA; 240-24-USG; 636-2-USG; 461-7-PCNGO; 396-42-PCGOV; 587-5-PCGOV; 636-6-USG). Issues related to access to testing and PMTCT services for pregnant women are discussed in more depth in Chapter 5 on prevention. There are also gaps in linking testing for pregnant women with testing for their male partners; PEPFAR has supported efforts to involve male partners in PMTCT services (331-27-PCGOV; 587-9-USG; 636-9-USACA; 116-15-USNGO).
Infants and children are another critical and challenging population with respect to HIV testing; efforts for this population are discussed in depth later in this section of the chapter.
In some cases interviewees described the targeting of testing services as resulting in some conflict and lack of alignment with national priorities and planning in partner countries. In these cases, generalized testing was typically a priority for the partner government, while PEPFAR was advocating that the most strategic use of available resources for testing would be to prioritize identified high-risk populations or higher-prevalence geographic areas (587-22-USG; 240-2-USG; 396-23-USG).
Other Efforts Related to Testing
In addition to its support for the delivery of counseling and testing services to clients, PEPFAR has provided support in partner countries at the level of health systems for activities in other areas that are critical for testing. These are noted briefly here; health systems strengthening is discussed in more depth in Chapter 9.
Interviewees across countries described PEPFAR’s contribution to testing through the construction of laboratories, strengthening central laboratory services to receive district samples, and capacity building of technical staff (935-8-PCGOV; 542-8-USNGO; 396-25-PCGOV; 934-5-USG). Beyond training laboratory staff, other workforce activities funded by PEPFAR with respect to testing have included the training of counselors in counseling and testing, the training of health care providers and supervisors on PICT, and the training
of health care workers and lay counselors to do rapid HIV testing (272-13-USG; 116-12-PCNGO; 935-17-USG; 240-ES). The training of non-laboratory workers to do testing was described by one interviewee as having a ‘huge impact’3(272-13-USG), but this approach has encountered barriers related to policies on scope of work that limit the ability of programs to expand home-based testing and testing in facilities without laboratory staff (935-ES). PEPFAR has also supported the supply chain for testing through the provision of test kits as well as through transportation solutions for delivery of samples (166-11-USG; 935-8-PCGOV; 935-13-PCGOV). Other examples include PEPFAR support for the strengthening of information systems and providing access to electronic tools used to track samples and to register the positive cases tested (396-36-PCGOV; 935-17-USG).
Interviewees also mentioned several examples of PEPFAR introducing counseling and testing quality-assurance strategies, including efforts such as setting up quality-assurance programs at the national level, the use of the HIVQUAL system, internal and external quality management systems, quality checks of test kit batches, and training of supervisors on PICT and HIV testing and counseling to ensure providers maintain quality services (461-18-USG; 116-12-PCNGO; 587-9-USG; 935-17-USG; 272-13-USG; 934-5-USG). At the same time, interviewees noted that in some countries there were challenges associated with quality assurance, due, for example, to the lack of a system to measure the quality of services and issues with standardization for counseling and testing and services (166-5-USG; 272-25-USG).
Ongoing Challenges with Coverage of HIV Testing
Despite the achievements in the scale-up of HIV testing in PEPFAR partner countries, challenges remain in achieving adequate coverage, including low rates of testing and low knowledge of HIV serostatus (particularly among HIV-infected persons), which contribute to gaps in achieving coverage goals of HIV treatment and prevention programs (Gilliam et al., 2012; OGAC, 2011b). This limits the ultimate success of testing services as part of the continuum of HIV prevention, care, and treatment services in a comprehensive response to HIV. Several interviewees on country visits remarked that, although the progress in testing coverage since the initiation of PEPFAR has been a notable achievement, there continue to be large numbers of people who do not know their HIV status (196-14-PCGOV; 331-10-PCGOV; 240-9-USG; 935-8-PCGOV; 636-11-PCNGO; 166-13-PCGOV). As one interviewee put
__________________
3 Single quotations denote an interviewee’s perspective with wording extracted from transcribed notes written during the interview. Double quotations denote an exact quote from an interviewee either confirmed by listening to the audio-recording of the interview or extracted from a full transcript of the audio-recording.
it, a ‘key challenge is getting more people access to counseling and testing’ (166-13-PCGOV). Interviewees noted a host of factors that, in their experience supporting the implementation and delivery of these services, affect whether people access counseling and testing services. In most cases these are barriers that PEPFAR has been attempting to overcome and, as described above, PEPFAR’s contribution has led to remarkable progress. Nonetheless, the ongoing challenge of coverage remains an important factor to address as it will otherwise hinder efforts to further advance PEPFAR’s efforts and to achieve future HIV-related goals.
Many of the factors affecting coverage that interviewees mentioned had to do with availability of testing services. This availability is affected by long wait times; the availability of trained counseling and testing and laboratory personnel; the availability of laboratory equipment and commodities such as test kits and reagents; and the necessity in some geographic locations of referring clients to another, more distant site for testing which can lead to barriers related to cost and transportation (240-2-USG; 396-25-PCGOV; 587-5-PCGOV; 396-21-USG; 934-5-USG; 272-13-USG; 196-24-PCNGO; 196-27-USG; 166-5-USG; 166-15-USACA; 196-10-PCGOV; 461-10-PCNGO; 636-22-PCNGO; 935-17-USG; 935-24-USNGO; 935-14-USG; 461-14-USG; 166-10-USNGO; 272-25-USG; 116-20-USNGO; 636-17-PCGOV; 196-17-PCGOV; 542-8-USNGO). Other factors described by interviewees had more to do with the engagement of individuals in accessing these services, which they described as affected by stigma, concern about discrimination, cultural norms about accessing health services, fear of experiencing violence or separation from a spouse or partner, and fear of losing family support (636-11-PCNGO; 331-7-PCNGO; 935-15-ONGO; 166-5-USG; 240-ES; 166-27-PCNGO; 331-6-CCM).
These interviewee perspectives on barriers leading to a lack of coverage of HIV testing are consistent with the research literature, which has shown that even when HIV testing is available, discrepancies persist between the intention to be tested and actually being tested (Obermeyer and Osborn, 2007) and that engagement in testing is affected by complex factors such as the awareness of and access to testing and health care as well as perceived risk, stigma, fear, discrimination, and threat of violence (Bartlett et al., 2008; Padian et al., 2011). Women are particularly vulnerable to stigma, domestic violence, and abandonment related to testing outcomes and disclosure (Medley et al., 2004; Visser, 2012; WHO, 2006a), yet they are more likely to report having had an HIV test than men (WHO et al., 2011). One contributing factor to this increased likelihood of testing among women is their greater access to testing services as a result of more frequent contact with health services, such as participation in antenatal care (WHO, 2012d).
The fear of violence or abandonment as a result of an HIV diagnosis was raised by interviewees in several countries as a salient and critically important issue for some women, and it is discussed in more depth in
Chapter 8 on gender along with an additional discussion of cultural norms and gender differences in accessing HIV and other health services.
HIV Testing for Children
PEPFAR has supported activities for the identification and diagnosis of children who are HIV positive as part of its PMTCT and pediatric HIV programs since early in the program, but it was not until the second PEPFAR Five-Year Strategy that specific goals were articulated that by 2014 every partner country with a generalized epidemic reach national coverage of 65 percent for early infant diagnosis and 80 percent for testing of older children of HIV-positive mothers, along with increased referrals and linkages to care and treatment (OGAC, 2009e). PEPFAR’s activities include efforts to increase early identification of HIV exposure and infection status in children. However, HIV testing for infants and children is a particularly challenging area.
HIV Testing for Infants
Early infant diagnosis (EID) has received increasing attention in PEPFAR-supported programs over time. In the FY 2009 annual report to Congress, PEPFAR reported its support for “expanding polymerase chain reaction (PCR) testing to identify the presence of HIV,” including “country-level policy change to allow PCR-based dried blood spot testing in order to reduce the cost and burden of infant diagnosis” (OGAC, 2009a, p. 49). Centrally reported indicators used to monitor testing over time do not reflect performance specific to the scale-up of EID, but the introduction in the Next Generation Indicators (NGIs) of an EID indicator should serve to improve the monitoring of this programmatic goal at the country program level (OGAC, 2009d).
Interviewees in partner countries described how PEPFAR has supported programs to implement and scale-up EID by using strategies such as the integration of EID into other services and the improvement of laboratory access, capabilities, technology, and training, including the use of dried blood spot collection to obtain samples for testing. Interviewees highlighted the progress in establishing infant diagnosis programs as an accomplishment and noted that wider access to these specialized laboratory services has led to improved diagnostic efforts, including, for example, improved turnaround time for lab results (240-2-USG; 240-21-PCGOV; 240-24-USG; 396-21-USG; 636-17-PCGOV; 116-19-PCGOV; 935-7-USG; 461-13-USACA; 461-18-USG).
Despite considerable progress, PEPFAR-supported programs and partner country HIV programs have challenges with identifying children for
treatment and have been unable to achieve goals for infant testing and, consequently, for pediatric HIV treatment (240-2-USG; 240-21-PCGOV; 636-19-USNGO; 935-ES). Several steps in the chain necessary to the process of EID can pose challenges to successful implementation. This chain includes identifying HIV-exposed infants in maternal and child health services (for example, by documenting on an infant’s record the mother’s HIV status and receipt of appropriate PMTCT services), obtaining and sending the specimens to the lab, performing the tests, getting the results returned to the clinic, and finally getting the results to the families. Interviewees said that, even as laboratory and technical capacity to do the appropriate test is slowly being built, there remain geographic areas without access to testing, and even in areas where testing is available, difficulties in the logistics of the transport of specimens, in conveying the results, and in linking infants to treatment services cause delays in diagnosis and initiation of treatment (240-24-USG; 240-21-PCGOV; 396-21-USG; 331-28-PCGOV; 636-17-PCGOV; 935-7-USG).
Providing technical expertise and assisting in the country development of a national implementation plan for EID is important, but implementation at scale takes time, and in the meantime infected infants continue to be undiagnosed and, consequently, untreated in the first year of life. One interviewee described the consequences of limited access to infant diagnosis by noting that ‘so many infants were not recruited for treatment, even though treatment was available’ (240-21-PCGOV). As a result of the challenges to the scale-up of EID services, availability is far from universal in most low-and middle-income countries. WHO recently estimated, based on reporting from 65 countries, that only about 28 percent of infants born to mothers living with HIV were tested within the first 2 months of life (WHO et al., 2011). This lack of or delay in HIV testing and diagnosis in this age group represents an important problem because early initiation of treatment in infants is critical for their survival. Based on evidence from across regions in Africa, without treatment, 50 percent of HIV-infected infants die by the age of 2 years (Brahmbhatt et al., 2006; Newell et al., 2004). A study in South Africa showed that early diagnosis and early initiation of antiretroviral therapy reduced early infant mortality by 76 percent and HIV progression by 75 percent (Violari et al., 2008). Given the urgency and importance of early diagnosis and the reality that it will take time for universal access to testing to be instituted and successfully implemented, there appears to be a relative lack of parallel emphasis in PEPFAR on supporting alternative means to diagnose young infants, despite an evidence base for presumptive diagnosis based on clinical presentation, serology, and CD4 count (Grundmann et al., 2011).
HIV Testing for Older Children
Older HIV-infected children in need of treatment are also often identified late in the course of their disease. Although children older than 2 years may be tested for HIV with the standard rapid serological test, few interviewees in PEPFAR partner countries indicated that routine provider-initiated HIV testing of ill and hospitalized children was being performed (461-13-USNGO; 542-3-USG). One reason offered for this was that providers have generally not been trained to readily recognize HIV symptoms in children, which underscores the need to educate general pediatricians and other providers caring for children about detecting HIV in children (396-42-PCGOV; 396-43-ML). Testing the children of identified adults with HIV is another way to identify infected children. However, provider-initiated testing of all children in the families of adults receiving care and treatment was not routinely described, although interviewees did identify some examples of efforts to identify family members of index patients or implement whole-of-family care and treatment models (240-19-USACA; 116-21-PCNGO; 116-19-PCACA). PEPFAR has also supported alternative strategies, such as outreach testing, to identify HIV-infected children and adolescents, including specific populations at elevated risk, such as street children (542-4-USG; 542-14-PCGOV; 240-24-USG).
Linkages from HIV Testing to Care and Treatment
Getting patients who have accessed testing services and been found to be HIV positive successfully enrolled in care and treatment is essential to improving HIV outcomes; indeed, the availability and awareness of successful care and treatment is one of the contributing factors to the successful scale-up of testing. In the words of one interviewee,
‘Before, people were afraid to get tested, but now there are known advantages of getting tested: linkages to care and support, as well as treatment.’ (240-9-USG)
To this end, PEPFAR-supported counseling and testing is implemented with a strong emphasis on linking with care and treatment (OGAC, 2011a). Interviewees in the countries visited described the importance of linking patients not only to HIV care and treatment but also to other services, such as appropriate antenatal care, reproductive health and family planning, sexually transmitted infection (STI) services, TB services, and, for people who inject drugs, community-based rehabilitation and ongoing harm-reduction services and counseling (396-25-PCGOV; 587-5-PCGOV; 331-14-USG; 331-44-USNGO; 461-18-USG; 935-13-PCGOV).
Despite the intent to establish these linkages, there is concern about the actual success of referrals to link HIV testing to care and treatment. A
lag between testing and enrollment in care and treatment can delay early therapy for those already eligible for ART. Patients can also be lost entirely to follow-up in this gap, falling almost immediately off the continuum of services for people living with HIV. The available literature shows that the reasons for the loss of patients in this period are related to the low risk perceived by asymptomatic patients, the little therapeutic care that may be provided at this point in the course of the disease, and the effort and investment required by patients to attend health care facilities for follow-up (Rosen and Fox, 2011).
These challenges are consistent with the perspectives of interviewees in PEPFAR partner countries. Interviewees noted that patients face a number of challenges after testing, such as an insufficient emphasis on referrals in some testing programs, a lack of facilities to be referred to, the long distances required to reach facilities, long waiting times, the need for return trips to receive results for CD4 counts in order to determine the need for ART, stigma, and denial or non-acceptance of HIV-positive status (636-6-USG; 461-14-USG; 461-7-PCNGO; 272-13-USG; 542-11-PCNGO; 331-11-PCNGO; 587-12-USG).
As described previously, another challenge to assessing and addressing the loss of patients that interviewees identified was the lack of a system of unique patient identifiers to help track whether people reach care and treatment programs after being tested (116-9-PCNGO; 587-3-USG; 461-7-PCNGO; 587-13-USG; 396-21-USG). As one interviewee observed, there is a ‘disconnect between testing and care and treatment because there is no name-based reporting for testing—it is hard to track patients from testing to care’ (587-13-USG). Another interviewee mentioned the problem of not being able to account for the gap in HIV-positive patients being linked to treatment: ‘we do not know why they are not seeking treatment’ (396-21-USG).
There have been several PEPFAR-supported efforts to address this problem of linkages and referrals to care and treatment services, including home-and community-based programs and efforts to improve linkages among different health services, which will be described later in this chapter. In a comprehensive example from one country, the lessons learned from a pilot program using referrals included using lay persons for testing, addressing supply chain management issues for testing commodities, involving people living with HIV and local leaders, and multiple strategies for community mobilization (461-7-PCNGO). Interviewees also suggested that providing testing and treatment services in the same facility could help link HIV-positive patients to treatment (196-11-USNGO; 935-20-PCNGO; 396-25-PCGOV; 396-32-PCGOV). In some cases, special effort has been made to link marginalized populations to the services they need at facilities known to be accepting of individuals from these populations (331-14-USG; 396-25-PCGOV; 196-ES; 331-22-PCNGO; 331-44-USNGO).
Conclusion: PEPFAR’s efforts have led to a considerable achievement in increasing the availability of and access to HIV testing, counseling, and diagnosis. As a result, many more individuals have learned their HIV status and, if positive, been linked to clinical services. However, challenges remain in achieving adequate coverage of testing services, especially in scaling up and improving access to testing for infants and children and testing for pregnant women who do not attend antenatal care or deliver in health facilities. For those who test positive, challenges also remain in consistently ensuring they are linked to care and treatment as well as to prevention services to reduce HIV transmission. Overcoming these challenges and continuing to make progress in HIV counseling and testing will be a critical factor in achieving a successful comprehensive response to HIV.
CLINICAL CARE AND NONCLINICAL SUPPORT SERVICES
Overview of Program Guidance and PEPFAR-Supported Activities for Care and Support
Care and support services, considered here separately from antiretroviral treatment, are an important component of programs for PLHIV as the step in the continuum of care after testing and diagnosis for those who are HIV positive and not yet eligible for ART. Ongoing care and support services are also important once ART is initiated. The Lantos-Hyde Act of 2008 set a target of supporting care for 12 million people living with or affected by HIV/AIDS, including 5 million children orphaned or made otherwise vulnerable by HIV/AIDS (discussed further in Chapter 7). The legislation emphasizes promoting a “comprehensive, coordinated system of services to be integrated throughout the continuum of care.”4
PEPFAR defines care and support services as “the wide range of services other than ART” for PLHIV and for others who are affected, such as family members (OGAC, 2009a, p. 16). For adults this includes facility-based as well as home- and community-based activities. For pediatric care and support, this category includes services for children when they are provided at a facility; community- and home-based services for children living with HIV, including some of the same services included in care and support when not provided in facilities, are implemented under the programmatic area category of programs for orphans and vulnerable children (discussed in full in Chapter 7). Both adult and pediatric care and support activities are aimed at “extending and optimizing quality of life for HIV-infected clients
__________________
4Supra, note 1 at ![]() 101(a), 22 U.S.C. 7611(a)(4)(C).
101(a), 22 U.S.C. 7611(a)(4)(C).
and their families throughout the continuum of illness” by providing clinical care services, psychological, spiritual, and social support services, and prevention services (OGAC, 2010b, p. 22). These services are ultimately intended to promote health for people living with HIV, slow the progression of AIDS, and reduce HIV-related complications and mortality.
The PEPFAR-issued guidance for care and support services includes HIV/AIDS Palliative Care Guidance for the United States Government In-Country Staff and Implementing Partners and Guidance for United States Government In-Country Staff and Implementing Partners for a Preventive Care Package for Adults (OGAC, 2006a,c). There is also guidance for preventive care for children (0–14 years) with a similar menu of services as well as additional services that are specific to pediatric needs, such as childhood immunizations (OGAC, 2006b); guidance for care and support services that are implemented through programs for orphans and vulnerable children is discussed in Chapter 7. Additional operational guidance for care and support programs is provided through PEPFAR’s annual COP guidance as well as technical considerations provided by headquarters-level technical working groups (OGAC, 2011a,b).
The categories of care and support services are summarized in Figure 6-3; the types and combinations of interventions in a care and support portfolio vary by country and by implementing partner. Clinical care includes prevention and treatment of TB and other opportunistic infections and HIV/AIDS-related complications, including malaria and diarrhea, by providing pharmaceutical prophylaxis, insecticide-treated nets, safe water interventions, and related laboratory services; pain and symptom relief; and nutritional assessment and support, including food. Psychological and spiritual support may include counseling, end-of-life care, and bereavement services. Social support may include social and legal protection, training and support of caregivers, vocational training, and income-generating activities. Other services may include behavioral counseling and the counseling and testing of family members (OGAC, 2006a,c). Efforts to integrate care and support services with other health and development programs, such as voluntary family planning and reproductive health services, are also a key component of PEPFAR II (OGAC, 2009a).
A review of annual PEPFAR COPs from the countries selected for visits for this evaluation revealed the implementation of a broad and widely ranging array of care and support activities; this was similarly described by interviewees across countries. Given the breadth of services, these activities, which will be discussed in more detail later, are implemented across levels of stakeholders in the response, from national and local governments to facilities to communities, and PEPFAR uses widely ranging types of partners within and beyond the health sector, including local community and nongovernmental organizations. Interviewees in partner countries noted
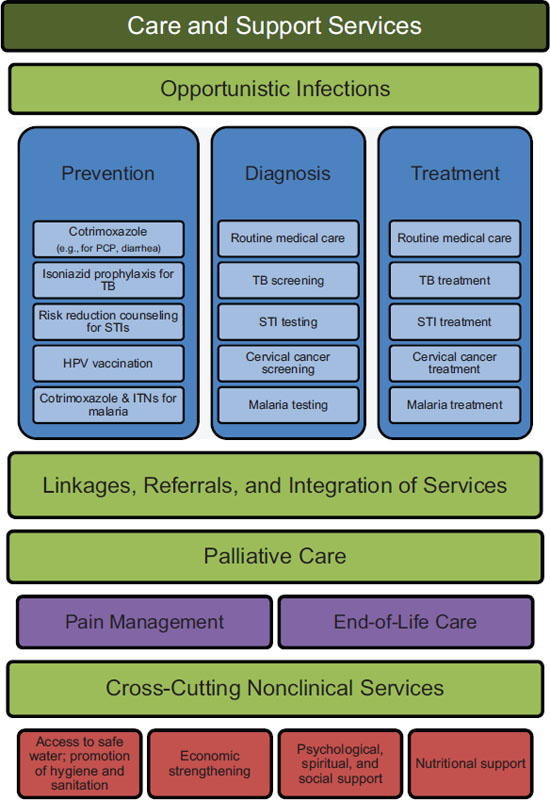
FIGURE 6-3 PEPFAR care and support services.
NOTES: HPV = human papillomavirus; ITNs = insecticide-treated nets; PCP = Pneumocystis jiroveci pneumonia; STIs = sexually transmitted infections; TB = tuberculosis.
SOURCE: Adapted from IOM and NRC, 2010.
that collaboration is essential since partnering with agencies and programs across sectors and levels, down to the community, makes it possible to offer cross-cutting interventions (240-15-USG; 331-5-ML).
Funding History for PEPFAR Care and Support Activities
The funding for PEPFAR’s activities for care and support is captured within several budget codes: Adult Care and Support, TB/HIV, Pediatric Care and Support, and OVC. (Funding for OVC, or orphans and vulnerable children, is also discussed in more detail in Chapter 7.) Figure 6-4 shows the funding in these budget codes over time in both the dollar amount and as a proportion of all PEPFAR funding. The total across these budget codes increased steadily in the years following the beginning of PEPFAR and then leveled off, starting in FY 2009, at just less than $900 million per year. Care and support has represented about 20 percent of all PEPFAR funding since the beginning of the initiative. Since the pediatric care and support budget code was introduced, it has been a relatively constant proportion of care and support funding (OGAC, 2005, 2006g, 2007c, 2008b, 2010c, 2011d,e).
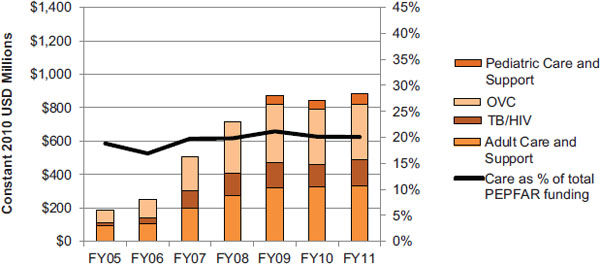
FIGURE 6-4 Planned/approved funding over time for care and support services.
NOTES: This figure represents funding for all PEPFAR countries as planned/approved through PEPFAR’s budget codes. The budget codes are the only available source of funding information disaggregated by type of activity and are therefore used in this report as the most reasonable and reliable approximation of PEPFAR investment by programmatic area. Data are presented in constant 2010 USD for comparison over time. As defined in the FY 2011 COP guidance, PEPFAR funding for Care includes budget codes for Adult Care and Support, Pediatric Care and Support, TB/HIV, and OVC. The TB/HIV budget code includes funding for all TB activities, including commodities and laboratory as well as pediatric TB/HIV services (OGAC, 2010a). Funding for Pediatric Care and Support was not reported separately until FY 2009. See Chapter 4 for a more detailed discussion of PEPFAR’s budget codes and the available data for tracking PEPFAR funding.
SOURCES: OGAC, 2005, 2006g, 2007c, 2008b, 2010c, 2011d,e.
Overview of Effects of PEPFAR Care and Support Activities
Overall Care and Support Indicator Data: Targets and Results
To reflect the performance of PEPFAR’s care and support programs, PEPFAR has an overall output indicator, reported centrally, that captures the number of individuals provided with HIV-related care. This was revised in the NGIs to be the number of eligible adults and children provided with a minimum of one care service. To be counted under this indicator, individuals must receive a minimum of one service. However, in its guidance PEPFAR specifies that the goal should be to provide a comprehensive set of support and clinical services appropriately tailored to the status of the individual or family, including linkages among partners (OGAC, 2009d). As of the NGI revision, the overall care indicator is reported with the data disaggregated by age, and the grouping of less than 18 years of age replaces the previous OVC indicator (see Chapter 7). This overall-care indicator serves to track the overall legislative target of reaching 12 million people with care services (Table 6-2).
Since the implementation of the NGIs in 2009, another centrally reported indicator has been a subset of the overall care indicator that is specific to clinical care. This indicator is available with disaggregation by sex and by two age groups, under 15 and 15 and older (see Table 6-3). A greater number of females than males received at least one clinical care service in FY 2010, with females representing 64 percent of the total and males 36 percent. Of the total number provided with clinical care services, 10 percent were children under the age of 15.
A small number of other centrally reported output indicators for TB/HIV, cotrimoxazole, and food/nutrition services were also available to the committee and will be presented in the sections that follow on the specific sub-areas of activities within care and support. There are no centrally reported indicators for isoniazid preventive therapy; insecticide-treated nets; testing and treatment for malaria; prevention, testing, and treatment for STIs and other infections; safe drinking water, basic hygiene and sanitation; pain management services and policy efforts; economic strengthening services; or psychological and social support.
Many country programs and partners also collect additional indicators on intervention areas within care and support that are not routinely reported centrally. However, even with the additional data that may be available at the country and program level, there are major limitations to the utility of the program monitoring data for fully understanding the effects of PEPFAR’s programs. The monitoring of PEPFAR’s care and support activities is complicated by changes in indicators over time, because 14 of the essential PEPFAR indicators for care have changed significantly, have
TABLE 6-2 Number of Individuals Provided with Care (in Millions)
| Number of Individuals Provided with HIV-Related Carea | Number of Eligible Adults and Children Provided with a Minimum of One Care Serviceb | ||||||
| FY 2004 | FY 2005 | FY 2006 | FY 2007 | FY 2008 | FY 2009 | FY 2010 | |
| Result | 0.5 | 1.2 | 2.3 | 3.4 | 5.3 | 7.4 | 11.4 |
| Target | — | 1.0 | 1.7 | 2.4 | 4.4 | 6.4 | 12.4 |
| % of Target | — | 119 | 134 | 144 | 122 | 115 | 91 |
NOTE: This table represents data for the 31 countries identified as the focus of this evaluation (see Chapter 2).
aResults and targets correspond to OGAC indicator 6.2 (direct): Total number of individuals provided with HIV-related palliative care (including those HIV-infected individuals who received treatment for tuberculosis). This indicator is defined to include palliative care from facilities and/or community-/home-based organizations. Clients may include HIV-infected individuals and family members. How much care is needed in order to count within the indicator is determined by national standards. All persons served during the reporting period, regardless of frequency, will be counted once (OGAC, 2007b).
bResults and targets correspond to OGAC indicator C1.1.D: Number of eligible adults and children provided with a minimum of one care service. This indicator is defined to include support, preventative, and clinical services from facilities and/or community/home-based organizations. Individuals eligible for care services include people living with HIV/AIDS; family members, caregivers, or other household members living with an HIV-positive individual; children orphaned by HIV (<18 years old); children made vulnerable due to HIV (<18 years old); and infants born to HIV-infected mothers (OGAC, 2009d).
SOURCE: Program monitoring indicators provided by OGAC.
| Results Disaggregated by Sex | ||||||
| FY 2010 | Male | Female | Total | |||
| Result | Target | Result | Target | Result | Target | |
| 2.1 | 2.1 | 3.8 | 3.2 | 5.9 | 5.5 | |
| Results Disaggregated by Agea | ||||||
| FY 2010 | <15 Years Old | 15+ Years Old | Total | |||
| 0.6 | 5.3 | 5.9 | ||||
NOTES: This table represents data for the 31 countries identified as the focus of this evaluation (see Chapter 2). Data correspond to indicator C2.1.D: Number of HIV-positive adults and children receiving a minimum of one clinical care service (subset of C1.1.D). “Clinical services may be provided in facilities, the community, or in the home, and may include both assessment of the need for interventions (e.g., assessing pain, clinical staging, eligibility for cotrimoxazole, or screening for tuberculosis) and provision of needed interventions: prevention and treatment of TB/HIV, prevention and treatment of other opportunistic infections, alleviation of HIV-related symptoms and pain, nutritional rehabilitation for malnourished PLHIV” (OGAC, 2009d, p. 77).
a OGAC did not provide age-specific targets for this indicator.
SOURCE: Program monitoring indicators provided by OGAC.
been dropped, or are new since the beginning of the program.5 This limits the possibility of examining longitudinal trends for some data. The lack of unique identifiers for participants in most PEPFAR activities constitutes a major methodological challenge. Care and support programs are offered within different settings in which eligible clients may receive multiple services from different providers and partners. Therefore, there is a risk of an individual being counted several times (“double counting”), potentially leading to an exaggeration of the number receiving services. This also makes it difficult to track the scope of services received by an individual client and to track that client through programs and services over time. In addition, aggregated data reported to OGAC provide limited insight about the types of populations accessing care. The lack of disaggregation by sex, populations (including those at elevated risk), and age-range subgroups within children under 15 years old also makes it difficult to assess how services are distributed across identified populations and to assess progress toward goals for equitable service delivery across the whole of PEPFAR. Finally, most of these indicators do not reflect outcomes for the clients who received services and therefore cannot inform an assessment of the effectiveness or the quality of PEPFAR-supported care and support programs.
__________________
5 Essential indicators are those for which OGAC requires PEPFAR mission teams to track data to monitor PEPFAR’s progress (OGAC, 2009d).
Overall Effects of PEPFAR Care and Support Activities
Achievements and challenges in specific areas of PEPFAR’s care and support activities are described in the sections that follow; a few examples of overall achievements are described here. Interviewees described a range of PEPFAR-related achievements that they associated with the provision of HIV-related care and support. One major area discussed by interviewees was improvements in availability of and access to care. These improvements resulted from what interviewees described as an often-remarkable increase in the number of sites offering HIV-related care since the initiation of PEPFAR, including facilities, community-based sites, and workplace programs (196-1-PCGOV; 240-2-USG; 587-6-CCM). Another factor identified across interviews and countries as contributing to access to care is the use of community- and home-based care primarily provided by volunteers and community health workers, many of whom are PLHIV (272-7-USG; 272-32/35-PCNGO; 166-23-USG; 396-31-PCGOV; 461-13-USACA; 240-15-USG; 240-2-USG; 272-18-PCNGO; 331-14-USG; 331-16-USG). In addition, some interviewees described access as being improved by new models for care and integration of services. Although in many instances HIV services continue to be offered separately from other health services, some partner countries have initiated complete integration of all HIV-related service provision, co-location of services, referral systems, and new models of care such as family-centered approaches (166-11-USG; 934-15-PCGOV; 934-16-PCGOV; 396-41-PCGOV; 587-13-USG). Increasing the provision of comprehensive services was described as leading to increased access and quality of services (116-4-USG). Service integration is discussed in depth in Chapter 9 on health systems strengthening.
In addition to its support for service delivery, PEPFAR has also contributed to systems-level efforts in partner countries. PEPFAR facilitated the initiation or modification of partner country national policies, guidelines, protocols, and standard operating procedures related to care and support (166-13-PCGOV; 461-18-USG; 166-9-ML/OBL/USACA/USNGO/PCNGO/PCPS; 272-7-USG; 240-2-USG; 396-29-PCGOV; 461-13-USACA). Examples of this include supporting partner country government efforts to define a comprehensive care package, to decentralize comprehensive HIV services, to establish or take over the coordination and ownership of home-based care and community health worker programs, to develop national policies on community- and home-based care and palliative care, and to develop training manuals related to care and support (272-7-USG; 240-2-USG; 396-29-PCGOV; 461-13-USACA; 166-9-ML/OBL/USACA/USNGO/PCNGO/PCPS). Further examples include efforts to provide technical assistance, to build capacity and structures to improve access to care, and to strengthen public–private partnerships regarding care and support (166-8-USG; 272-32/35-PCNGO; 586-18-PCGOV; 396-12-USG; 240-2-USG).
Interviewees from PEPFAR-funded partners also reported that government and community advocacy have been part of their efforts to improve and provide care and support, particularly around such issues as palliative
care, pain control, treatment access, and leadership training for PLHIV, especially women (331-9-PCNGO; 196-7-PCNGO; 116-13-PCNGO; 396-44-PCGOV; 272-7-USG). In one partner country the findings of a PEPFAR-supported care and support evaluation ‘came to conclude that there are huge gaps,’ which was used as an advocacy tool (272-7-USG).
Building on this overview of PEPFAR’s care and support efforts, the following sections will describe in more depth the efforts and effects, including achievements and challenges, in specific components of care and support programs, including TB services, other clinical care services, and home- and community-based services.
Screening, Diagnosis, and Treatment of Tuberculosis
Tuberculosis infection in people living with HIV is one of the most common co-infections and has devastating consequences. Globally, TB is a leading cause of death for PLHIV; it is estimated that about a quarter of all HIV-related deaths are attributable to tuberculosis. HIV infection increases the risk of active TB disease more than 20-fold (WHO, 2012e). WHO has identified three major objectives in its guidelines for TB and HIV. The first objective is to establish and strengthen collaborations between HIV- and TB-control programs to deliver integrated services through, for example, the creation of an HIV/TB coordinating body that functions at the district, regional, local, and facility levels and is responsible for determining and monitoring the prevalence of HIV in TB patients and vice versa as well as integrating the delivery of services through joint planning. The second objective is to reduce the burden of tuberculosis in people with HIV by intensifying the identification of cases of TB among those who are HIV positive and providing those who are positive for TB with treatment and early initiation of antiretroviral therapy; by introducing isoniazid preventive therapy (IPT) to reduce progression to active tuberculosis in HIV-positive patients; and by controlling TB infections in health care facilities. The third objective is to reduce the burden of HIV in patients with tuberculosis by providing HIV testing and counseling for patients with TB; by introducing HIV prevention interventions for patients with TB, including condoms and behavior change interventions; by introducing cotrimoxazole preventive therapy for TB patients who are HIV positive, which has consistently reduced the risk of death and improved survival for co-infected patients when administered during routine tuberculosis care; and by linking to and enrolling those TB patients who are HIV-positive in HIV care and treatment services, including initiation of ART irrespective of CD4 count (WHO, 2012f).
PEPFAR-Supported TB/HIV Activities
The first PEPFAR Five-Year Strategy acknowledged the importance of linkages between HIV and TB and emphasized screening and treatment for TB and HIV co-infection as an area for rapid scale-up and programmatic synergies (OGAC, 2004). The second Five-Year Strategy further committed PEPFAR to scale up efforts to screen, diagnose, and, when necessary, treat all HIV patients for TB, while ensuring that all TB patients are tested for HIV and, if positive, referred to HIV care and treatment (OGAC, 2009g). In some years PEPFAR appropriations have included a global budgetary requirement for TB/HIV; when this has not been the case, COP guidance has nonetheless emphasized the importance of this aspect of the response to HIV and country programs with COP budgets in which resource commitments were not commensurate to the TB burden were instructed to justify those allocation decisions and to expect to receive “additional scrutiny in the review process” (OGAC, 2010b, p. 23).
PEPFAR-supports TB/HIV efforts through technical assistance to develop and strengthen national guidelines, policies, systems, and operational tools and through support for direct delivery of services, including exams; clinical monitoring; related laboratory services; TB screening; the diagnosis, treatment, and prevention of TB in PLHIV; and HIV testing and clinical care of patients in TB service locations (OGAC, 2010b). PEPFAR has also recently instituted technical assistance and support for the planning, policy development, and implementation and rollout of Xpert diagnostic testing for TB, which is an automated rapid test that greatly reduces the time to confirm a TB diagnosis (OGAC, 2011b, 2012).
PEPFAR-Supported TB/HIV Activities: Indicator Data Targets and Results
There are a number of centrally reported indicators that reflect PEPFAR’s activities in the area of TB/HIV. Because of indicator changes and the introduction of new indicators over time, not all indicators are available for all years, but the available indicators do offer some information to assess PEPFAR’s progress. With regard to the objective of reducing the burden of tuberculosis in people with HIV, two measures with centrally reported data over time were available to the committee; these reflect that PEPFAR has contributed to increased TB treatment for HIV-positive patients in terms of both the number of patients in HIV care who receive TB treatment (Table 6-4) and the number of service outlets with available TB treatment services (Table 6-5). However, PEPFAR has had more difficulty meeting the targets set for this area than it has for overall care (presented
TABLE 6-4 Number of HIV-Positive Patients in HIV Care Who Started TB Treatment (in Thousands)
| FY 2004 | FY 2005 | FY 2006 | FY 2007 | FY 2008 | FY 2009 | FY 2010 | |
| Result | 101.5 | 179.6 | 147.5 | 215.2 | 277.6 | 308.7 | 256.2 |
| Target | — | 158.9 | 188.9 | 264.2 | 341.9 | 368.2 | 369.4 |
| % of Target | — | 113 | 78 | 81 | 81 | 84 | 69 |
NOTES: This table represents data for the 31 countries identified as the focus of this evaluation (see Chapter 2). Data for FY 2004–FY 2009 correspond to indicator 7.2 (direct): number of HIV-infected clients attending HIV care/treatment services that are receiving treatment for TB (OGAC, 2007b). Data for FY 2010 correspond to indicator C2.5.D (numerator): number of HIV-positive patients in HIV care who started TB treatment (OGAC, 2009d). Patients in HIV care who receive TB treatment may be counted in this indicator regardless of where TB diagnosis and treatment was delivered (OGAC, 2009d). TB = tuberculosis.
SOURCE: Program monitoring indicators provided by OGAC.
| FY 2004 | FY 2005 | FY 2006 | FY 2007 | FY 2008 | FY 2009 | |
| Overall | 2.6 | 2.8 | 4.9 | 6.6 | 8.3 | 9.8 |
NOTES: This table represents data for the 31 countries identified as the focus of this evaluation (see Chapter 2). Data correspond to OGAC indicator 7.1: “This indicator measures the subset of service outlets providing TB/HIV care. A service outlet refers to the lowest level of service. For example, with regard to clinical activities, the lowest level for which data exists should be a service outlet such as a hospital, clinic, or mobile unit. A service outlet that will count in this indicator will provide treatment for tuberculosis to HIV-infected individuals (diagnosed or presumed)” (OGAC, 2007b, p. 61). TB = tuberculosis; USG = U.S. government.
SOURCE: Program monitoring indicators provided by OGAC.
earlier in this section) and for other areas, such as antiretroviral therapy (discussed later in this chapter).
To assess the coverage of TB screening in HIV-positive patients served by PEPFAR as part of the objective of reducing the burden of tuberculosis in people with HIV, the NGI indicators introduced a new centrally reported indicator for percentage screened, calculated using as the denominator the number of HIV-positive adults and children receiving a minimum of one clinical service (OGAC, 2009d). As shown in Table 6-6, 49 percent of the HIV-positive adults and children in care were screened for TB in FY 2010. The target for the number screened represented 68 percent of the target set for number of clients reached with clinical care services. The denominator (number in clinical care) exceeded the target set, while the numerator (number screened for TB) fell short.
Concerning the objective to reduce the burden of HIV in patients with tuberculosis, from FY 2007 to FY 2009 PEPFAR also tracked an indicator for the number of registered TB patients tested for HIV in TB service outlets supported with U.S. government (USG) assistance, which increased over time (Table 6-7).
| Number Screeneda | Number in Clinical Careb | % Screened for TBc | ||||
| FY 2010 | Result | Target | Result | Target | Result | Target |
| Total | 2.9 | 3.8 | 5.9 | 5.5 | 49 | 68 |
NOTES: This table represents data for the 31 countries identified as the focus of this evaluation (see Chapter 2). TB = tuberculosis.
a Indicator C2.4.D (numerator): number of HIV-positive adults and children screened for TB in HIV care or treatment settings (OGAC, 2009d).
b Indicator C2.1.D: number of HIV-positive adults and children receiving a minimum of one clinical service (OGAC, 2009d).
c Indicator C2.4.D: percent of HIV-positive patients who were screened for TB in HIV care or treatment settings (OGAC, 2009d).
SOURCE: Program monitoring indicators provided by OGAC.
| FY 2007 | FY 2008 | FY 2009 | |
| Total | 181.6 | 607.1 | 767.8 |
NOTES: This table represents data for the 31 countries identified as the focus of this evaluation (see Chapter 2). Data correspond to OGAC indicator 7.4: number of registered TB patients who received HIV counseling, testing, and their test results at a USG supported TB service outlet (OGAC, 2007b). TB = tuberculosis; USG = U.S. government.
SOURCE: Program monitoring indicators provided by OGAC.
PEPFAR-Supported Activities for Integrated TB/HIV Services
Interviewees across PEPFAR partner countries recognized high TB/HIV co-infection rates as a critical aspect of the HIV response (196-11-USNGO; 396-12-USG; 636-10-PCGOV; 934-5-USG; 542-8-USNGO). As one interviewee noted, “we also saw the need to do TB/HIV intervention. HIV and TB are bedfellows” (331-44-USNGO). The review of annual PEPFAR COPs from the countries selected for visits for this evaluation, along with the interview data, reflected PEPFAR’s support for the delivery of integrated TB/HIV services. Interviewees described various models or types of HIV/TB integration that have been supported at the level of service delivery. The range of integration and coordination of services included complete integration of TB and HIV services; co-location of HIV prevention, care, and treatment services and TB services or close proximity between clinics; HIV services integrated into TB clinics; and TB services integrated into HIV clinics (542-16-PCGOV; 542-13-USG; 935-19-PCGOV; 935-21-PCGOV; 935-24-USNGO; 935-25-PCGOV; 636-12-USACA; 636-22-PCNGO; 116-9-PCNGO; 240-15-USG; 272-20-PCNGO; 396-44-PCGOV; 166-15-USACA; 636-9-USACA; 934-15-PCGOV; 636-17-PCGOV). Another form of integration involved offering HIV and TB screening at both HIV and TB clinic sites and inpatient settings, and interviewees noted successes in improving
coverage of both HIV and TB screening and testing (587-5-PCGOV; 396-21-USG; 636-17-PCGOV; 934-15-PCGOV; 935-13-PCGOV; 636-9-USACA; 396-41-PCGOV; 116-9-PCNGO; 331-44-USNGO). One partner, for example, described the successful implementation of standard screening for TB for every patient at every visit in the HIV care and treatment clinic (934-15-PCGOV), and an interviewee from another country program described similar success in one city district in achieving systematic provision of HIV counseling and testing for outpatient TB patients (396-21-USG). Another model is to have separate HIV and TB clinics with referral systems (636-9-USACA; 272-21-PCNGO; 935-13-PCGOV; 396-31-PCGOV), including facilitated referrals by patient escorts and the use of TB/HIV coordinators and lay counselors (934-24-USNGO; 636-9-USACA). The approach may also depend on the clinical presentation, such as referring out of the HIV care and treatment clinic for active TB while having latent TB management done in the HIV clinic (587-18-PCGOV). In at least one example, a linkage between the HIV clinic and the TB clinic was created by linking lab results (935-19-PCGOV).
Interviewees also described examples where PEPFAR has supported partners to initiate integrated TB/HIV activities, to institute quality management in TB/HIV services, to pilot the implementation of IPT, to train providers on TB/HIV, and to incorporate education about TB into services for PLHIV (196-11-USNGO; 396-21-USG; 331-44-USNGO; 331-16-USG; 935-24-USNGO).
Although interviewees across countries described these activities as examples of progress that have occurred as a result of PEPFAR’s efforts in the area of TB/HIV services, especially in more recent years, there are still a number of critical challenges and unmet needs in this important area of the response to HIV. There are still gaps in the screening of both HIV patients for TB and TB patients for HIV, hindered in part by a lack of clinical diagnostic capabilities and laboratory capacity (935-24-USNGO). A major challenge that persists is ensuring the delivery of treatment services needed for those who are identified as co-infected, including loss to follow-up for both TB patients identified as HIV positive and HIV patients diagnosed with TB (935-22-PCGOV; 935-24-USNGO; 935-7-USG; 240-15-USG; 331-30-USPS). Among the contributing factors identified by interviewees are resistance to testing, a desire among some patients to complete TB treatment before starting ART, and a lack of providers and facilities to provide the needed services (935-22-PCGOV; 935-24-USNGO; 116-8-USG). In some countries, interviewees also described challenges with instituting infection control practices (542-8-USNGO; 935-22-PCGOV).
PEPFAR’s Systems-Level Support for TB/HIV
The review of annual PEPFAR COPs from the countries selected for visits for this evaluation as well as the interview data collected reflected that in addition to supporting service delivery for TB/HIV, PEPFAR has also provided systems-level support for TB/HIV programs, emphasizing
an integrated approach. As described by interviewees across countries, PEPFAR and its implementing partners have supported ministry of health TB/HIV activities and have contributed to efforts to link the national TB program and national AIDS program so that they work together (196-11-USNGO; 935-22-PCGOV; 636-9-USACA; 196-14-PCGOV; 331-16-USG). In one country, for example, this included supporting ministry-level staff positions dedicated to this effort (935-22-PCGOV). PEPFAR has also supported a range of capacity building efforts for TB/HIV clinical and laboratory services through technical assistance and training (196-14-PCGOV; 331-16-USG; 396-21-USG; 396-22-USG; 396-41-PCGOV; 935-22-PCGOV; 935-24-USNGO; 934-35-PCNGO).
An implementing partner in one partner country described ‘huge progress’ recently with TB/HIV (636-9-USACA). Signs of this progress include that the ministry of health sees the need for TB/HIV integration and that the separate government programs for TB and HIV and the separate implementing partners for TB and HIV were brought, with PEPFAR’s assistance, into an HIV/TB technical working group; this working group helped develop guidelines on how to integrate TB and HIV, which allowed for the implementation of new models of TB/HIV integration (636-9-USACA). PEPFAR has supported other efforts to work with national programs to develop guidelines and tools, such as treatment guidelines for TB/HIV (240-15-USG), an algorithm to improve the diagnosis of TB (396-21-USG), guidelines and screening tools for pediatric clients (461-13-USACA), and standard operating procedures to improve TB case detection among HIV patients and to improve infection control in facilities in order to reduce the exposure of HIV-positive patients to TB (331-16-USG).
PEPFAR has also contributed to national TB/HIV efforts by supporting policies for the expansion of services, such as contributing to the decentralization of comprehensive HIV services, including integrated TB services, in order for them to be provided in lower-level health facilities (240-2-USG; 461-13-USACA). In addition, PEPFAR has contributed to building an evidence base to support policy efforts. In one country, supporting an IPT pilot program led the government to adopt this policy for adults and children, although the implementation to date varies by region (396-21-USG). PEPFAR has also supported the implementation of integrated or coordinated TB/HIV monitoring and evaluation (542-8-USNGO; 196-14-PCGOV; 935-24-USNGO; 240-10-USG). In at least one country PEPFAR has also contributed to TB more generally than as part of the HIV response, by supporting efforts to increase case detection of TB within the general population and initiatives to focus on multidrug-resistant TB (396-12-USG).
Several interviewees also identified challenges at the systems level. Funding is one such challenge. Interviewees described limited additional funding for HIV and TB (396-12-USG; 935-24-USNGO; 542-25-USG) and separate donor or national funding streams for TB and HIV (331-16-USG; 396-12-USG; 935-22-PCGOV),
which posed challenges to integrating services for the two health issues. As one interviewee observed, while integration may be well accepted as a PEPFAR-supported policy initiative, ‘programs have a positive view of integration until they are competing for funding’ (331-16-USG). In addition to the challenges posed by separate funding, interviewees also described the challenges of integrating pre-existing, well-established, but very separate and vertical programs and clinical services for the two diseases (396-21-USG; 935-ES; 636-9-USACA; 396-22-USG; 542-25-USG; 272-7-USG). Progress in TB/HIV integration and coordination sometimes varied by the level of the system. In one example, ‘the collaboration is good at the national and provincial level but variable at the district level’ (396-21-USG), while in another integration worked well at the service level but not centrally (636-19-USNGO). The challenge of separate systems also extends to separate systems for monitoring and evaluation (935-ES; 542-8-USNGO; 636-9-USACA; 542-15-USG); one interviewee described implementing monitoring and evaluation of TB, HIV, and TB/HIV programs as ‘the hardest part of the TB/HIV program’ although this was in part because of the overall limitations in the country’s systems for monitoring and evaluation (542-8-USNGO).
Conclusion: The importance of TB/HIV efforts is well-recognized within PEPFAR and in partner countries. PEPFAR has increasingly supported the integration and coordination of screening, diagnosis, and referrals or other linkages to treatment for both infections. PEPFAR has also made a notable contribution in its support for advancing policies and systems for TB/HIV integration in partner countries. However, progress in this area has come more slowly than in other clinical services for HIV, and challenges persist in achieving adequate coverage of both HIV screening for TB patients and TB screening for HIV patients, as well as in ensuring and monitoring subsequent referral and retention in treatment for both infections. Concerted efforts in this area will be critical for reducing mortality from TB/HIV as part of an effective response to HIV.
Other Supportive Clinical Care Services
In addition to services for TB/HIV, PEPFAR’s care and support portfolio includes support for a number of clinical care services, including the prevention and treatment of other opportunistic infections and HIV/AIDS-related complications. PEPFAR supports these services through health facilities, discussed here, as well as through home- and community-based care programs (discussed in more detail in the section that follows) and through linkages with other USG health and development programs.
Prophylactic and Therapeutic Drugs for Opportunistic Infections
One major component of care for HIV-infected individuals is the use of cotrimoxazole (CTX), a broad-spectrum antimicrobial agent, to prevent Pneumocystis jiroveci pneumonia (formerly Pneumocystis carinii pneumonia), toxoplasmosis, and malaria (WHO, 2006b). WHO recommends CTX prophylaxis for adults living with HIV as a cost-effective method to significantly reduce morbidity and mortality; however, country-level policies on CTX vary according to the capacity and infrastructure of health systems and the burden of HIV and other diseases (WHO, 2008). PEPFAR’s NGI indicator revisions introduced a centrally reported indicator that was available to the committee for the number of HIV-positive persons receiving cotrimoxazole prophylaxis (OGAC, 2009d) (see Table 6-8). In FY 2010, PEPFAR met its target for this service.
WHO also recommends that all infants born to HIV-infected mothers receive CTX until they are shown not to be HIV infected (WHO, 2006b). Age disaggregation is not reported centrally for the CTX indicator, so it was not possible to assess PEPFAR’s output in reaching infants with the recommended prophylaxis using the data available to the committee.
Cryptococcal disease is also common in PLHIV and is often treatable. However, many countries lack the infrastructure and skilled personnel necessary for diagnosis and without early recognition, mortality from cryptococcal disease is high (OGAC, 2009b; WHO, 2008). Where cryptococcal disease is common and the diagnostic capacity does exist, WHO recommends consideration of antifungal prophylaxis (fluconazole or itraconazole) for severely immunocompromised PLHIV (WHO, 2008). PEPFAR has provided limited training and laboratory capacity building for diagnosis, and although currently there is limited availability of antifungal prophylaxis, PEPFAR is working with its partner, Supply Chain Management System, and with Pfizer, which runs a fluconazole donation program, to increase access to these drugs for treatment and prevention (OGAC, 2009b).
TABLE 6-8 Number of HIV-Positive Persons Receiving Cotrimoxazole Prophylaxis (in Millions)
| FY 2010 Result | FY 2010 Target | |
| Total | 2.9 | 2.9 |
NOTES: This table represents data for the 31 countries identified as the focus of this evaluation (see Chapter 2). Data correspond to indicator C2.2.D: number of HIV-positive persons receiving cotrimoxazole prophylaxis (OGAC, 2009d).
SOURCE: Program monitoring indicators provided by OGAC.
Screening for Cervical Cancer
Women who are HIV positive have high rates of infection with cancer-causing strains of human papilloma virus, and they have increased risk of cervical cancer. WHO recommends that, where possible, women living with HIV should be screened annually for cervical cancer (WHO, 2008). As part of a comprehensive approach to opportunistic infections, PEPFAR has supported cervical cancer pilot programs for HIV-positive women using the “see and treat” approach, which includes visual inspection with acetic acid, visual inspection with Lugol’s iodine, or direct visual inspection (Kaur and Singh, 2010; OGAC, 2009a). PEPFAR recently initiated a public–private partnership through the launch of the “Pink Ribbon, Red Ribbon” campaign to support and scale up improved services for cervical cancer as well as breast cancer in HIV-positive women (George W. Bush Institute et al., 2012). This initiative is in its early stages, so it was too early for the committee to make any assessment of its progress or effects.
Several interviewees in partner countries described PEPFAR-supported efforts to integrate cervical cancer screening programs, including offering cervical cancer screening in care and treatment facilities, launching a nationwide human papilloma virus vaccination campaign, and fully integrating a cervical cancer screening program into the ministry of health with a PEPFAR partner providing quarterly oversight and health care professional training for cervical cancer screening and treatment (636-17-PCGOV; 272-20-PCNGO; 461-18-USG; 461-13-USACA; 587-10-USG; 587-13-USG; 587-18-PCGOV). One organization described success in this area through an intensified screening program that ensures that all its sites have cervical screening programs, noting, however, that it is the only nongovernmental organization (NGO) implementing partner in that country with these intensified screening services (272-20-PCNGO).
Prevention and Treatment of Malaria
Malaria is another area of focus in services for those who are HIV-positive. WHO recommends the integration of malaria and HIV services with a particular focus on prevention (WHO, 2008). As previously mentioned, CTX may reduce malaria-related morbidity and mortality in PLHIV. Insecticide-treated bed nets (ITNs), when used properly and regularly, are a cost-effective approach to greatly reduce exposure to malaria infection. To reduce the risk of malaria and its consequences for HIV-positive pregnant women who are not taking CTX, WHO also recommends intermittent preventive therapy (IPTp) (WHO, 2008). The President’s Malaria Initiative (PMI) is a USG interagency initiative to reduce malaria that was originally implemented in 15 focus countries and has since expanded to 19 countries and one regional program (PMI, 2013). PMI is working to expand coverage
of effective interventions for malaria prevention and treatment, including ITNs, indoor residual spraying with insecticides, IPTp, and artemisinin-based combination therapy (PMI, 2013). Thirteen of the PMI countries also have PEPFAR country programs operating at the level of COPs where the intent is that PEPFAR routinely link with PMI, and the efforts of the two initiatives overlap in ITN distribution and education programs as well as in the coordination of lab services (OGAC, 2009a; PMI, 2009). Interviewees in partner countries described collaboration of this kind between PEPFAR and other USG malaria efforts (240-12-USG; 240-15-USG; 331-12-USG; 166-11-USG; 461-7-PCNGO; 461-19-USG).
Increased Access to Safe Drinking Water and the Promotion of Basic Hygiene and Sanitation
Another source of infection in those who are HIV positive is waterborne and enteric pathogens, the risk of which is exacerbated in many developing countries by poor infrastructure and the lack of safe management of human waste (WHO, 2008). Diarrhea from these pathogens affects 90 percent of PLHIV, and diarrhea-related morbidity can be greatly reduced by interventions to improve water, sanitation, and hygiene, such as the provision of safe water storage vessels and education regarding hand washing (OGAC, 2009b). The latest USG Framework for Addressing Water Challenges in the Developing World, which guides U.S. Agency for International Development (USAID) and Department of State (DoS) efforts, encourages the incorporation of these interventions into all HIV/AIDS programs (USAID and DoS, 2009). PEPFAR’s preventive care package for PLHIV includes support for products to treat and properly store drinking water as well as soap and promotion of hand washing (OGAC, 2006a), and interviewees in partner countries described PEPFAR support for these interventions (166-9-ML/OBL/USACA/USNGO/PCNGO/PCPS; 461-3-USG; 461-7-PCNGO; 331-12-USG; 116-20-USNGO; 116-23-USPS).
Food and Nutrition Support Services
HIV infection may cause or intensify malnutrition by reducing appetite, increasing energy needs, and impairing nutrient absorption (OGAC, 2009b). Nutritional and micronutrient supplementation may reduce HIV-related morbidity and mortality and improve outcomes for patients on ART, and proper nutrition also supports the immune system, preventing opportunistic infections (OGAC, 2009f). Through Food by Prescription and similar programs, PEPFAR targets clinically malnourished children and adults living with HIV, pregnant and lactating women and their infants in PMTCT programs, and orphans and other vulnerable children, especially
| FY 2010 Result | FY 2010 Target | |
| Total | 256.7 | 457.3 |
NOTES: This table represents data for the 31 countries identified as the focus of this evaluation (see Chapter 2). Data correspond to indicator C2.3.D: number of HIV-positive clinically malnourished clients who received therapeutic or supplementary food. This includes only clients who meet diagnostic criteria based on anthropometric assessment. Food provided for household use or as a safety net is not included this indicator (OGAC, 2009d).
SOURCE: Program monitoring indicators provided by OGAC.
those under 5 years old, regardless of HIV status. These programs provide food and nutrition care and support, including nutrition assessment and counseling services, prescribed specialized food products, including those for treatment of malnutrition, and micronutrient supplementation (OGAC, 2009b). PEPFAR does not support direct food distribution to families, but emphasizes linkages and referrals of those in need to the USG Global Hunger and Food Security Initiative, USAID’s Title II programs, and other initiatives, such as the United Nations World Food Program (OGAC, 2009a,b,g). Linkages of this kind were described in several interviews in partner countries (240-15-USG; 636-9-USACA; 116-24-USNGO; 331-14-USG; 331-19-USNGO; 331-23-USNGO; 240-3-USG). Interviewees also described technical assistance for guidelines and training on nutrition and food support as well as the provision of nutrition services through various organizations and partners, including nutritional counseling at community health care centers and food support (934-7-PCGOV; 272-18-PCNGO; 240-25-PCGOV; 272-32/35-PCNGO; 587-6-CCM; 331-23-USNGO; 331-16-USG; 396-21-PCGOV).
With the NGI indicator revision, PEPFAR has a centrally reported indicator for the number of clinically malnourished HIV-positive persons receiving therapeutic or supplementary food (see Table 6-9). For FY 2010, PEPFAR fell short of its target for this service.
Palliative Care, Including Management of Pain and Other Symptoms
PEPFAR defines palliative care as a “holistic approach to providing services that includes a focus on pain and symptom management and on improving quality of life,” which is consistent with the WHO definition (OGAC, 2009b, p. 25; WHO, 2013). Palliative care, including end-of-life care, can also reduce the burden of caregiving on families (OGAC, 2009f). In many countries, restrictive policy environments are a barrier to effective pain management programs, and access is limited to strong pain medications such as opioids (OGAC, 2009f). PEPFAR’s second Five-Year Strategy calls for continued efforts to “support policy changes that ensure pain management is included both in guidelines and actual clinical services” for
PLHIV as well as increased efforts to “strengthen commodity systems, train providers, and expand access to opioids for pain management” (OGAC, 2009f, p. 19). Many of the home- and community-based care programs described in the next section include pain management among the services they provide. PEPFAR has also supported partners to assist in national efforts to improve palliative care and pain management through guidelines and training of providers and to participate in advocacy (116-12-PCNGO; 116-13-PCNGO; 396-18-USG). One interviewee described a local association’s role as a pain control advocate as follows:
‘They have been successful through advocacy, so that [the country] is now procuring morphine. Through PEPFAR funding, [the country] now has morphine. Talking about morphine is a taboo, but the association has managed to convince the government. Using the PEPFAR funding, they sent the director for the “medicine and poison fund” to go to [another country] to learn about how they are doing with morphine. After that exposure, the government was convinced.’ (116-13-PCNGO)
Home- and Community-Based Care and Support Services
PEPFAR supports the provision of care and support services through home- and community-based mechanisms across the spectrum of both the clinical services described earlier (when a health facility is not required) and nonclinical services, which are also critical for the health of people who are HIV positive and for their adherence to treatment once initiated. One interviewee emphasized the need for these services, describing that the initiation of HIV treatment can be associated with ‘a cascade of effects—lack of social support, loss of income, hard to maintain adequate nutrition’ (331-8-PCNGO).
Across the countries visited for this evaluation, a review of COPs and information gathered from interviewees revealed a wide range of clinical and nonclinical services and activities provided through home- and community-based care, which some interviewees indicated were first introduced or funded by PEPFAR (396-18-USG; 272-32/35-PCNGO). To offer just a few examples (not a comprehensive listing), interviewees mentioned the management and prevention of opportunistic infections, pain assessment, palliative care, nutrition, the treatment of STIs, adherence monitoring, home-based care kits, psychosocial and social support, and home visits for persons who are bedridden (461-3-USG; 396-21-USG; 272-32/35-PCNGO; 395-56-USNGO; 240-29-USNGO; 331-32-PCNGO; 587-13-USG).
This section first describes the overall findings from interview data collected for this evaluation that apply generally to home- and community-based care, then discusses some findings for specific subsets of PEPFAR-
supported nonclinical services for adults. Nonclinical services for children are discussed in full in the section on OVC programs in Chapter 7.
Evolution of Care and Support Services: From Caring for the Dying to Supporting the Living
One common theme that emerged across many countries and types of interviewees was that a shift has occurred over time in the nature of care services. Initially, in most countries home-based care focused on the critically ill and on providing end-of-life care and hospice. Although there is still a need for services for the critically ill, the increased availability of care and treatment services, the move from inpatient to outpatient care, and the generally improved health status of PLHIV have led to a decline in patient populations requiring end-of-life care and to a change in the needs to different kinds of care and support services (272-32/35-PCNGO; 272-7-USG; 240-2-USG; 935-10-USG). As described by one interviewee,
‘For the first 5 years, the beginning of PEPFAR, the care and support activities were very much focused on the late stages of illness through palliative and hospice care. As the lay of the land has changed, so have the care activities. They are focusing on a wider range of care aspects.’ (272-7-USG)
One implementing partner described home-based care as divided into three categories: one in which the patient can perform all activities without any assistance, one in which the patient needs minimal assistance, and one in which the patient is bedridden. Currently the majority of patients fall into the middle category, although at the beginning of PEPFAR the implementing partner was mostly providing home-based care and hospice, mostly for terminal patients discharged from the hospital (272-32/35-PCNGO). Home- and community-based care has shifted its focus to keeping those infected with HIV healthy as well as to case management and to more integrated services, such as chronic disease management (461-3-USG; 240-2-USG; 587-18-PCGOV). One interviewee stated that just as the introduction of ART has reduced the need for home-based care, the need for such care may also be reduced by effective care for PLHIV who are pre-ART, consistent with the concept that ‘care starts at diagnosis’ (272-7-USG).
Implementation with a Focus on the Community and Using Local NGOs
Another overall characteristic of PEPFAR-supported home- and community-based care programs that was highlighted across countries is that these programs have been implemented with a strong focus on
the community and on the use of local community and nongovernmental organizations (166-14-PCNGO; 934-10-PCGOV; 272-32/35-PCNGO; 935-19-PCGOV; 240-15-USG). In addition, many programs are implemented using community volunteers or community health workers, many of whom are also PLHIV. These workers provide such services as case management; adherence monitoring and counseling; personal care; palliative care; pain assessment; nutritional assessment; assistance in navigating health services; and referrals to help lines, health facilities, and other program linkages, including to facilities known to be ‘friendly’ to high-risk targeted populations (272-7-USG; 272-32/35-PCNGO; 166-23-USG; 396-31-PCGOV; 461-13-USACA; 240-15-USG; 240-2-USG; 272-18-PCNGO; 331-14-USG; 331-16-USG). In an example in one partner country, a restructuring was taking place to shift to community care provided by a cadre of workers with the capacity to do ART management and counseling (272-7-USG). In another example, an NGO partner provided traditional healers and community authorities with education about HIV and associated diseases since these individuals played an integral role in community health care; this was described as an important approach because a large proportion of the population used traditional healers for care (331-19-USNGO).
Linkages Between Home- and Community-Based Care and Facility-Based Care
One of PEPFAR’s aims for care and support activities has been to support the implementation of different approaches to link facility-based care services with community- and home-based care services. Several interviewees described home-based care programs that emphasized promoting linkages between home-based care and HIV care and treatment clinics, health facilities, and providers who can make appropriate referrals (272-32/35-PCNGO; 331-10-PCGOV; 396-25-PCGOV; 166-23-USG). In other cases, programs for home-based care or home visits for adherence support and reducing loss to follow-up are based out of outpatient facilities or other care and treatment programs and are therefore directly linked to patients enrolled in clinical care and treatment (935-15-ONGO; 935-25-PCGOV; 396-29-PCGOV; 396-21-USG; 240-19-USACA; 240-25-PCGOV). There were also a few examples involving children and adolescents in which community and nonclinical services were linked with clinical services in health facilities, such as age-specific clubs for children in HIV care and treatment clinics; youth-friendly services for HIV-positive youth that include support groups; education, and programs for youth in school and those not in school; and community workers who focus on helping children stay in treatment (636-17-PCGOV; 935-13-PCGOV; 272-14-PCNGO). (See Chapter 7 for a further discussion of services for children and adolescents.)
Overall Challenges with Home- and Community-Based Care
Although interviewees in many countries described achievements in home- and community-based care, interviewees also identified challenges with the implementation and scale of these services. These challenges included a lack of knowledge, training, policies, and funding support for home-based care, which was described as ‘capital intensive’ (331-27-PCGOV; 587-10-USG; 272-32/35-PCNGO). Interviewees in one partner country described home-based care as not very strong (331-8-PCNGO) or lacking (331-11-PCNGO). In another country, clients in remote areas not reached by home-based counseling and testing were coming to facilities for testing late in the progression of their disease (461-17-PCNGO). Limitations on the scope of interventions that could be done in the community were also described as a challenge, as was the lack of clinical services available for referral, which was linked to the need for health systems improvements to increase the availability of ‘adequate services at public health facilities’ (461-7-PCNGO).
Another specific challenge described by implementing partners was the interpretation of indicators and the quality and timeliness of reporting, primarily because of challenges with the capacity of local providers and with barriers to reporting, such as lack of transportation for monitoring remote programs and collection of paper-based forms (272-32/35-PCNGO; 331-22-PCNGO; 272-15-PCNGO).
Specific Areas of PEPFAR-Supported Nonclinical Services
Psychological and spiritual support Psychological and spiritual support supported by PEPFAR may include group and individual counseling and culturally appropriate end-of-life care and bereavement services (OGAC, 2010b, 2011a). Several interviewees talked about the provision of psychosocial care or, more rarely, spiritual care, including services such as peer education and peer support; self-help groups for PLHIV and their families; and provision of psychosocial counseling for PLHIV or “psychosocial support,” although what this entailed as a service or set of services was difficult to clearly define (331-10-PCGOV; 396-21-USG; 461-10-PCNGO; 461-17-PCNGO; 461-18-USG; 587-13-USG; 331-32-PCNGO; 196-7-PCNGO; 396-44-PCGOV; 166-8-USG; 240-14-USPS).
Although ‘a lot has happened since 2004’ (166-15-USACA), interviewees generally echoed the perspective that ‘psychosocial and spiritual support is the area of greatest need but no strong undertaking’ (240-15-USG). One partner described psychosocial support as “a big need to tackle; it is overwhelming” (272-22-USG). Another interviewee’s observation that ‘psychosocial support is weak nationwide’ (166-29-PCGOV) was echoed by another interviewee’s statement that such support is an area ‘that needs more attention’ (396-21-USG),
particularly since, in this country, the need is not being met in the general population in addition to those affected by HIV (396-45-USNGO).
Some interviewees discussing the providers for such care commented that few trained professionals are available for service provision (272-15-PCNGO; 461-10-PCNGO). In one country, qualified social workers were described as difficult to recruit and retain, particularly in rural areas (272-15-PCNGO). An interviewee in another country observed that ‘counselors and clinical psychologists are cadres that don’t really exist in the public service payroll’ (461-10-PCNGO). PLHIV have played an increasingly important and direct role in offering individual, family, community-, or hospital-based psychosocial or spiritual support. As volunteers or recipients of stipends, they offer such support primarily by means of organizing and facilitating HIV support groups, providing peer education that involves psychosocial support, and serving as role models (331-9-PCNGO; 240-15-USG; 240-25-PCGOV; 331-32-PCNGO).
Social support Social support services supported by PEPFAR may include social and legal protection for PLHIV as well as the training and support of caregivers (OGAC, 2010b, 2011a). Interviewees mentioned various programs and activities that offered “social support” or in some cases described an unmet need for social support. However, as was the case with “psychosocial support,” it was difficult to establish a clear understanding of exactly what this entailed in terms of a service or set of services across the scope of PEPFAR-supported programs (196-20-PCNGO; 396-21-USG; 396-32-PCGOV; 396-50-PCGOV; 461-10-PCNGO; 331-8-PCNGO).
Several interviewees identified efforts to provide training and support for caregivers of PLHIV. One partner described caregivers as “wounded healers” for whom care is provided in some programs (272-11-PCNGO). Another highlighted the role of women as caregivers:
‘In terms of care, women are the primary caregivers. This role has been acknowledged and there have been efforts to lighten the burden. “Women have borne the brunt of HIV/AIDS.”’ (934-7-PCGOV)
Home- and community-based support for legal protection is primarily implemented in the context of OVC programs or gender-focused programs; these are discussed in Chapters 7 and 8, respectively.
Economic strengthening activities Recognizing that a lack of economic assets increases vulnerability, PEPFAR supports activities that “supply, protect, or grow physical, natural, financial, human, and social assets” (OGAC, 2009g, p. 17). These activities may include vocational training; microfinance and microcredit programs to expand access to financial services; and income-generating activities, including communal gardens (which
may also provide food) (OGAC, 2009g, 2010b). Interviewees in partner countries indicated that this area of intervention is important. One interviewee described a need for more ‘social interventions’ for people with HIV in order to assist them to become more employable and productive, “like any other person” (331-8-PCNGO). Another described the ideal as supporting PLHIV so that they will be able to return to the jobs they held or businesses they had prior to becoming ill (331-32-PCNGO). Yet another described the positive outcomes of participation by PLHIV in income-generating activities, including providing them with a source of productive work, an opportunity for skills building, a means of contributing to the community, improved self-esteem and morale, and presumed improved treatment adherence. According to this organization, ‘they don’t just let patients sit and say I’m sick. [. . .] It is not only about giving them ARVs’ (272-32/35-PCNGO). One partner organization discussed the link between income-generating activities and reducing risk, as exemplified by the predicament of sex workers who could find no other means of employment (331-08-PCNGO).
A number of partner organizations across countries, including many local community-based organizations, described providing PLHIV with small grants to start businesses or providing or linking PLHIV with support for income-generating activities (IGAs) such as farming; raising animals; or making products to sell, such as beads, candles, or soap (240-14-USPS; 240-26-PCNGO; 240-29-USNGO; 331-20-USNGO; 272-32/35-PCNGO; 240-25-PCGOV; 331-8-PCNGO). As described by an interviewee in one partner country,
‘The most important success in our PEPFAR-funded project is that all our beneficiaries are linked to local support and some have been successful in their income-generating activity. [. . .] This program has been very successful due to close monitoring; we have conducted certain case studies in some of our projects and most of the IGA beneficiaries have been successful.’ (240-26-PCGOV)
Although interviewees generally endorsed IGAs, some did report doubts about the value and viability of IGAs for PLHIV (272-32/35-PCNGO; 240-24-USG).
A number of interviewees across countries described success with PEPFAR support for vocational training and employment opportunity programs (396-31-PCGOV; 396-44-PCGOV; 461-7-PCNGO; 331-19-USNGO; 587-13-USG; 587-21-PCNGO; 272-26-PCNGO; 196-9-USNGO; 196-23-PCNGO; 166-27-PCNGO; 935-16-USNGO). However, interviews also described challenges in this area. Resources associated with vocational training posed challenges as did being able to transition into adequate employment, and, despite isolated program successes, vocational training remained a largely unmet need for PLHIV (396-31-PCGOV: 396-36-PCGOV; 396-45-USNGO;
331-19-USNGO; 331-32-PCNGO; 935-16-USNGO; 461-17-PCNGO; 196-17-PCGOV; 196-24-PCNGO). The challenges are compounded for those PLHIV in marginalized populations:
“Livelihood options, vocational trainings, that type of thing, it’s not that people are not trying to meet it, but it’s just very difficult because you have these double-stigmatized populations. Many of them are really uneducated, and the very urban environment, relatively high cost, and no land. So it’s a huge, huge gap. But not for want of trying.” (396-45-USNGO)
In addition to supporting specific income-generating and vocational training activities, PEPFAR has also contributed to the availability and stability of employment for people living with HIV through activities to reduce workplace discrimination, including policy and legislative efforts as well as support for workplace programs for HIV awareness and HIV counseling and testing in the workplace (587-14-PCGOV; 587-17-PCNGO; 331-40-PCPS; 934-11-USG).
Conclusion: PEPFAR has made a tremendous contribution to a wide variety of clinical and nonclinical care and support services, beyond the provision of antiretroviral therapy, through a scale-up of services and programs in facilities and communities and through support for partner country policies, guidelines, and protocols. However, in the area of nonclinical care and support in particular, services span a diffuse range of activities across countries, and it is difficult to assess their effects. Information is lacking on the distribution of services, the intended outcomes, how well the services are matched to population and subpopulation needs, and the effectiveness of these services.
Recommendation 6-1: To improve the implementation and assessment of nonclinical care and support programs for adults and children, including programs for orphans and vulnerable children,6 the Office of the U.S. Global AIDS Coordinator should shift its guidance from specifying allowable activities to instead specifying a limited number of key outcomes. The guidance should permit country programs to select prioritized outcomes to inform the selection, design, and implementation of their activities. The guidance should also specify how to measure and monitor the key outcomes.
__________________
6 The discussion of programs for orphans and vulnerable children leading to this aspect of this recommendation can be found in Chapter 7.
Further considerations for implementing this recommendation:
• Outcomes for consideration should reflect the aims of care and support programs, which are to optimize quality of life, promote health, slow the progression of AIDS, and reduce HIV-related complications and mortality. Other outcomes of importance for the performance and effectiveness of care and support programs include measures of quality of services and equitable access to services.
• PEPFAR mission teams should work with partner country stakeholders and implementers to assess country-specific needs and to select a subset of the core key outcomes to focus on when planning, selecting, and developing evidence-informed activities and programs for implementation.
• OGAC should provide general guidance for country programs on continuous program evaluation and quality improvement to help them measure and monitor achievement of the key outcomes. This guidance may include, for example, template evaluation plans and methodological guidance. To allow for comparability across countries and programs, evaluation plans should include (but not be limited to) the defined indicators or other measures of the core key outcomes. Evaluations should emphasize the use of in-country local expertise (e.g., local implementing partners and subpartners and local academic institutions) to enhance capacity building and contribute to country ownership. (See also recommendations for PEPFAR’s knowledge management in Chapter 11.)
• PEPFAR should develop a system for active dissemination and sharing of evaluation outcomes and best practices both within and across countries that is driven as much by country-identified needs for information as by opportunities for exchange of information identified by headquarters-level leadership and technical working groups. (See also recommendations for PEPFAR’s knowledge management in Chapter 11.)
Global Context for the Scale-Up of Antiretroviral Therapy
The rapid scale-up of ART in the past decade resulted from intense advocacy efforts, unprecedented political commitments at the highest levels, dramatic reductions in the cost of antiretroviral drugs, and record increases in donor country foreign assistance dedicated to HIV/AIDS. It represents
one of the most significant achievements in the more than 30-year global fight against AIDS (Kapstein and Busby, 2009; UNAIDS, 2011).
When combination ART became available in 1996, it cost more than $10,000 per patient annually, placing the life-saving treatment largely out of reach for those in low- and middle-income countries. A lack of political will to address the pandemic from leaders in donor countries as well as in many developing countries—largely because of the high cost of treatment, but also because of ongoing stigma and the pervasive opinion that HIV/AIDS treatment was too complicated to implement in low-resource settings—meant that an HIV diagnosis continued to be a death sentence for the majority of the world’s population (Kapstein and Busby, 2009; UNAIDS, 2011).
By the turn of the 21st century, however, the tide had begun to change. By then, the ability of ART to bring patients from the brink of death to relative good health had transformed HIV/AIDS in high-income countries to a largely manageable chronic disease. This was a stark difference from the ongoing and rapidly increasing mortality rates that remained in low-and middle-income countries (UNAIDS, 2011). There was increasing recognition among a wide range of stakeholders of the profound and growing toll of HIV/AIDS on health, the economies, and future development in the most affected developing countries, and there was increasing evidence that it was possible to treat HIV/AIDS in low-income settings. Under increasing pressure to take concerted action to expand access to life-saving ART and prevention tools in developing countries, the world’s political leaders stood poised to finally recognize the significance of the HIV/AIDS pandemic and to make meaningful commitments to address the global crisis. The 2001 United Nations General Assembly Special Session (UNGASS) on HIV/AIDS resulted in a major worldwide political commitment at the highest levels to address the pandemic along with established global targets and goals for the response (UNAIDS, 2011).
Momentum from UNGASS on HIV/AIDS led to the WHO 3 by 5 Initiative in 2003, which set the goal of placing 3 million patients in need on life-saving ART by 2005. This represented an ambitious goal in the international response to HIV/AIDS, given that when the initiative began in 2003, only an estimated 400,000 people living with HIV were receiving ART. As a part of the 3 by 5 Initiative, WHO also established global guidelines for the eligibility and treatment of HIV in developing countries (WHO, 2004a).
The global political commitment that emerged from the 2001 UNGASS on HIV/AIDS also led to an unprecedented increase in financial commitments to combat the pandemic, including the establishment of the Global Fund to Fight AIDS, Tuberculosis, and Malaria (the Global Fund) in 2002, with financial pledges totaling $28.8 billion as of 2012 from most of the world’s leading donor nations, who also support bilateral HIV programs
(Global Fund, 2013; Kapstein and Busby, 2009; UNAIDS, 2011; WHO et al., 2009) and the initiation of PEPFAR, with its commitment to scaling up HIV/AIDS treatment and prevention programs in the countries most affected by the epidemic.7
By the end of 2011, more than 8 million people living with HIV in low-and middle-income countries were receiving ART; of these, about 562,000 were children (UNAIDS, 2012c). This was a 20-fold increase in the number of people receiving ART in developing countries from the 400,000 who had been receiving ART in 2003 (UNAIDS, 2012b). The costs of providing ART have also come down dramatically since it first became available, with the current per patient-year cost estimated to be less than $1,000 (Menzies et al., 2011; PEPFAR, 2012; UNAIDS, 2012d). The benefits of using ART to reduce the mortality and morbidity of persons living with HIV/AIDS and to reduce HIV transmission cannot be overemphasized, and there is increasing evidence of the effectiveness of ART in resource-constrained settings (Bussmann et al., 2008; Herbst et al., 2009; Jahn et al., 2008; Mat Shah et al., 2012; Mermin et al., 2008). Global efforts to expand the availability of ART have contributed to lower HIV-related mortality in multiple countries and regions. ART has added an estimated 14 million life-years since 1995, of which 9 million life-years have been in sub-Saharan Africa (UNAIDS, 2012b).
The financial support of PEPFAR and the Global Fund, reductions over time in the cost of ART, robust political commitments, and efforts to strengthen health systems that support service delivery have combined to allow for the rapid scale-up of HIV programs in low- and middle-income countries. As a result, progress is being made in increasing coverage, but a large proportion of PLHIV who are in need of antiretroviral drugs are currently not receiving such services. UNAIDS estimated that in 2011 coverage for people eligible for ART was 58 percent worldwide and 54 percent in low- and middle-income countries (UNAIDS, 2012b). Furthermore, an estimated 57 percent of pregnant women living with HIV in low- and middle-income countries received effective antiretroviral drugs to avoid transmission to their children in 2011. Although this coverage has increased over time, it is not yet approaching the 80 percent global target (UNAIDS, 2012b; WHO et al., 2010). In 2011, an estimated 330,000 children acquired HIV infection. This represents a steady decline since 2003, when an estimated 560,000 children became newly infected. However, UNAIDS reported that the estimated coverage of eligible children receiving ART worldwide in 2011 was only 28 percent (UNAIDS, 2012b).
__________________
7 United States Leadership Against HIV/AIDS, Tuberculosis, and Malaria Act of 2003, P.L. 108-25, 108th Cong., 1st sess. (May 27, 2003).
PEPFAR’s Contribution to Antiretroviral Therapy: Overview
Recognizing that the need to deliver life-saving treatment to the millions of people living with HIV was a global health emergency, the rapid scale-up of HIV treatment services and an increase in ART coverage was a major focus of PEPFAR in its early years (IOM, 2007). PEPFAR’s support for adult and pediatric ART, which it refers to as its treatment programs, includes the procurement of ARV drugs as well as the funding of infrastructure, training clinicians and other providers, exams, clinical monitoring, related laboratory services, and community-adherence activities (OGAC, 2010b). Patients enrolled in ART also continue to be eligible for the care and support services for PLHIV described in the previous section of this chapter, which are a critical ongoing component of the continuum of care. In addition, PEPFAR supports both care and treatment services through its health systems strengthening activities, which are described in detail in Chapter 9, where discussion of workforce training, laboratory services, and supply chain management can be found. Although not discussed in detail in this chapter, these systems-level activities are nonetheless an integral part of treatment programs and of supporting the continuum of care for HIV-positive patients.
The committee’s assessment of PEPFAR’s treatment programs described in this section followed the program impact pathway framework. The committee assessed how PEPFAR’s investments in and other support for the delivery of ART services (inputs) affected the availability of ARVs and access to treatment interventions through enrollment in ART (outputs). Within the limitations of the available data, the committee attempted to assess PEPFAR’s effects on the coverage of those in need of and eligible for treatment and on the retention in treatment of those enrolled (outcomes) as well as the ultimate effect on mortality in patients enrolled in ART (impact).
Overall, the scale-up of ART was seen across countries and across stakeholders as a major success of PEPFAR, which had a tremendous impact in saving the lives of HIV-positive patients (935-ES; 636-ES; 461-ES; 240-ES; 331-ES; 116-ES; 166-ES; 272-ES; 396-ES; 934-ES). One interviewee described the progress made after the introduction of PEPFAR-supported care and treatment programs in this way:
‘There was a dramatic increase in uptake of testing and ART, increased awareness and willingness to be tested, increased number of clinicians trained to provide ART, and the number of sites providing ART increased.’ (240-15-USG)
The sections that follow will address in more detail the achievements and challenges in the component areas of the committee’s assessment of PEPFAR’s ART programs.
Guidelines for Antiretroviral Therapy
PEPFAR does not issue its own programmatic guidance for treatment but instead defers to the normative guidance of WHO (NCV-10-USG; NCV-13-USG). In its 2010 HIV treatment guidelines, WHO updated its recommendation for ART initiation and is now recommending that all HIV-positive adults and adolescents, including pregnant women, start antiretroviral drug treatment if their CD4 counts are less than 350 cells/mm3 (compared to the previous recommended level of less than 200 cells/mm3) as a means to curb HIV-related mortality and to prevent opportunistic infections, such as tuberculosis. This treatment should be commenced regardless of the presence or absence of clinical symptoms (WHO, 2010b). More recently WHO has released new treatment guidelines for serodiscordant couples in which only one partner is HIV positive; the guidelines recommend offering ART to the HIV-positive partner, regardless of immune status (CD4 count), in order to reduce the likelihood of HIV transmission to the HIV-negative partner (WHO, 2012a). These guidelines were released after almost all of the data collection for this evaluation of PEPFAR was completed, and therefore consideration of them in this report is limited.
WHO also has guidelines for the use of antiretrovirals to reduce the risk of mother-to-child transmission during pregnancy, delivery, or breast feeding. WHO recommends antiretroviral prophylaxis for all HIV-positive pregnant women and also has guidelines for the use of antiretrovirals for the mother–infant pair in order to reduce the risk of HIV transmission during breast feeding (WHO, 2010a). These are discussed further in the section on PMTCT in Chapter 5. In terms of antiretrovirals for ongoing treatment for HIV-positive pregnant women during and after pregnancy, delivery, and breast feeding, the guidelines indicate that existing WHO adult guidelines for ART initiation should be followed, except for countries electing to implement what is known as option B+, which suggests that ART be continued beyond pregnancy regardless of CD4 count, making pregnant women a priority for treatment (WHO, 2012b).
Concerning HIV treatment for children, current WHO guidelines call for all HIV-infected infants and children less than 2 years of age to be started on ART immediately upon diagnosis, regardless of CD4 count or clinical stage. WHO suggests specific regimens depending on exposure to antiretrovirals used for maternal treatment or PMTCT. WHO also suggests that sick infants with a presumptive clinical diagnosis of HIV infection should be treated promptly even without a definitive diagnosis (Grundmann et al., 2011; WHO, 2010c). The decision of when to begin treatment for HIV-positive children older than 24 months should be based on their age-specific CD4 cell count levels (WHO, 2010c).
According to interviewees, PEPFAR has supported ministries of health in the development of national care and treatment guidelines, taking into account the WHO guidelines, and it has also supported their implementation through training and support for increased service delivery, both for adults and for pediatric HIV patients, emphasizing integration and increased services for children (240-12-USG; 587-13-USG; 196-10-PCGOV; 116-18-PCNGO; 587-5-PCGOV; 240-19-USACA; 240-24-USG; 396-21-USG; 240-24-USG; 461-13-USACA; 116-9-PCNGO; 636-20-PCGOV). Table 6-10 is a summary, based on data available at the time this report was finalized, of the development of national treatment guidelines and the adoption of WHO updates in the 31 PEPFAR partner countries that were the main focus for this evaluation. At the time of the country visits for this evaluation (late 2010 through early 2012), interviewees in many countries stated that they had started the implementation of updated WHO treatment guidelines for adults, while in some countries there was a lag in adopting the guidelines for children (116-5-PCGOV; 116-7-USG; 116-9-PCNGO; 116-18-PCNGO; 396-30-PCGOV; 935-5-USG; 542-9-USPS; 272-22-USG; 934-5-USG; 636-10-PCGOV). Interviewees described several challenges with the adoption and implementation of the updated WHO guidelines, many of which were related to the resulting anticipated increase in the demand for treatment services, including the human resources capacity and the costs and availability of drugs to meet the need (272-32/35-PCNGO; 934-5-USG; 934-10-PCGOV; 934-2-USG; 934-12-CCM; 542-3-USG; 542-9-PCGOV; 116-7-USG; 116-18-PCNGO). Interviewees reported a lack of funding to accomplish the transition to the new guidelines (934-17-PCGOV), with great concern about the failure to receive or the cancellation of Global Fund rounds and other potential decreases in funding from international donors (396-30-PCGOV; 934-5-USG; 934-12-CCM). Interviewees also noted operational challenges related to, for example, staff training and adaptation of data systems; these were compounded by how little time they had between receiving the final version of the guidelines and the implementation phase (116-18-PCNGO; 116-7-USG; 116-9-PCNGO). The expansion of ART eligibility as a result of changes in the WHO guidelines will be discussed further in the subsequent section of this chapter on ongoing challenges with coverage for ART.
Funding History for PEPFAR-Supported Treatment Programs
PEPFAR’s activities for treatment are captured within the budget codes for ARV Drugs, Adult Treatment, and Pediatric Treatment. Figure 6-5 shows the funding over time in these budget codes in both the dollar amount and as a proportion of all PEPFAR funding. The total across these budget codes increased steadily from the beginning of PEPFAR until FY 2008, when funding peaked at more than $1.3 billion a year, after which it declined somewhat, leveling off by FY 2011 at about $1.1 billion (OGAC, 2005, 2006g, 2007c, 2008b, 2010c, 2011d,e).
TABLE 6-10 Adult and Pediatric Treatment Guidelines Adoption by Country
| Country | Adult ART Guidelines Issued in: | Adopted WHO 2010 Adult ART Recommendations?a | Pediatric ART Guidelines Issued in: | Adopted WHO 2010 Pediatric ART Recommendations?a |
| Angola | 2003 | Yes | 2003 | Yes |
| Botswana | 2005, 2008, 2012 | Yes | 2005, 2008, 2012 | Yes |
| Cambodia | 2003, 2007 | Yes | 2004, 2007, 2011 | Yes |
| China | 2005 | Yes | 2005 | Yes |
| Côte d'Ivoire | xxxx, 2005 | Yes | xxxx, 2005 | Yes |
| Democratic Republic of the Congo | 2002, 2005 | Yes | 2005 | Yes |
| Dominican Republic | 2004 | No | 2004 | No |
| Ethiopia | 2003, 2005, 2008 | Yes | 2003, 2005, 2007, 2008 | Yes |
| Ghana | 2002, 2005, 2008 | Yes | 2002, 2005, 2008 | Yes |
| Guyana | 2004, 2006, 2009, 2010/2011 (draft) | No | 2004, 2006, 2009, 2010/2011 (draft) | No |
| Haiti | 2003, 2008 | No | 2006 | No |
| India | 2003, 2004, 2007 | Yes | 2006 | Yes |
| Indonesia | 2004, 2007, 2011 | Yes | 2008 | Yes |
| Kenya | 2001, 2002, 2005, 2011 | Yes | 2005, 2011 | Yes |
| Lesotho | 2007 (draft) | Yes | 2007 (draft) | Yes |
| Malawi | 2003, 2006, 2008, 2011 | Yes | 2006, 2008, 2011 | Yes |
| Mozambique | 2006, 2009/2010 | Yes | xxxx, 2008 | Yes |
| Namibia | 2003, 2007, 2010 | Yes | 2003, 2010 | Yes |
| Nigeria | 2001, 2005, 2007, 2010 | Yes | 2007, 2010 | Yes |
| Russia | 2007 | No | — | |
| Rwanda | xxxx, 2007, 2009 | Yes | 2007, 2009 | Yes |
| South Africa | 2004, 2010 | Yes | 2004, 2010 | Yes |
| Sudan | xxxx, 2009 | Yes | xxxx, 2009 | Yes |
| Swaziland | 2003, 2006, 2010 | Yes | 2006 | Yes |
| Tanzania | 2002, 2005, 2009 | Yes | 2002, 2005, 2009 | Yes |
| Thailand | 2008, 2010 | Yes | 2010 | Yes |
| Uganda | 2003, 2008, 2009 | Yes | 2003, 2008, 2009 | Yes |
| Ukraine | 2004, 2006 | Yes | 2004, 2007 | Yes |
| Vietnam | 2005, 2009 | Yes | 2005, 2009 | Yes |
| Zambia | 2007 | Yes | 2007, 2010 | Yes |
| Zimbabwe | 2010 | Yes | 2010 | Yes |
NOTES: The primary sources for this table were AIDSTAR-One’s summaries of national treatment guidelines(AIDSTAR-One, 2011a,b, 2012), a multi-country survey on implementation of the 2010 WHO ART recommendations (Renaud-Théry, 2010), and national treatment guidelines (see table sources). Content not available in these sources is in orange when found within supporting documents and in blue when inferred after review of supporting documents. In these cases, guideline documents were not available to confirm. Pediatric guidelines may have been issued as separate documents or as components of national treatment guidelines. ART = antiretroviral therapy; WHO= World Health Organization. xxxx = year unknown.
a A “yes” indicates that the latest version of a country's national treatment guidelines are aligned with at least one component of WHO 2010 recommendations (e.g., thresholds for initiation of ART or choice of antiretroviral regimen).
SOURCES: AIDSTAR-One, 2011a,b, 2012; Botswana Ministry of Health, 2008; Cambodia Ministry of Health, 2003, 2007; China CDC, 2005; Ethiopia Ministry of Health, 2003, 2007; G and Adewumi, 2004; Ghana Ministry of Health, 2002; Government of India, 2007; Guyana Ministry of Health, 2009; Haiti Ministry of Public Health and Population, 2008; Indonesia Ministry of Health, 2007, 2008, 2011; Kayigamba et al., 2012; Kenya Ministry of Health, 2001; Malawi Ministry of Health, 2006; Namibia Ministry of Health and Social Services, 2010; Nigeria Ministry of Health, 2007; PEPFAR, 2005; PEPFAR/Mozambique, 2009; PEPFAR/Sudan, 2009; PNPEC, 2005; Renaud-Théry, 2010; Rossi and Ojikutu, 2011; Sungkanuparph et al., 2010; Swaziland Ministry of Health and Social Welfare, 2006; Talam et al., 2008; Tanzania Ministry of Health, 2005; Uganda Ministry of Health, 2008; Ukraine Ministry of Health, 2004a,b; WHO, 2004b, 2005a,b,c.
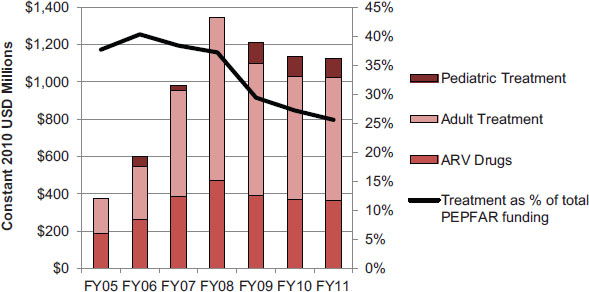
FIGURE 6-5 Planned/approved funding over time for treatment.
NOTES: This figure represents funding for all PEPFAR countries as planned/approved through PEPFAR’s budget codes. Funding for pediatric treatment was not reported in FY 2005 and FY 2008. The budget codes are the only available source of funding information disaggregated by type of activity, and are therefore used in this report as the most reasonable and reliable approximation of PEPFAR investment by programmatic area. Data are presented in constant 2010 USD for comparison over time. See Chapter 4 for a more detailed discussion of PEPFAR’s budget codes and the available data for tracking PEPFAR funding.
SOURCES: OGAC, 2005, 2006g, 2007c, 2008b, 2010c, 2011d,e.
From FY 2005 through FY 2011, the pediatric treatment budget code was, on average, 9 percent of the total adult and pediatric treatment budget codes. This percentage fluctuated in the early years of PEPFAR, when the budget code definition was also changing, including years in which pediatric treatment was not reported. It was steady at 13 to 14 percent from FY 2009 to FY 2011 (OGAC, 2005, 2006g, 2007c, 2008b, 2010c, 2011d,e).
Legislative Budgetary Allocation Requirement for Care and Treatment Funding
The original legislation authorizing PEPFAR mandated that not less than 55 percent of the budget be used for therapeutic medical care for those with HIV.8 In the Lantos-Hyde Act of 2008 reauthorizing PEPFAR, this was changed to a requirement that more than 50 percent of funds be used for care and treatment of people living with HIV.9 PEPFAR’s instructions for tracking this budgetary requirement are provided to country programs through COP guidance, where it is interpreted as a percentage of the total funds for prevention, care, and treatment (OGAC, 2010a). Tracking PEPFAR’s compliance with the proportional budgetary requirement over
__________________
8Supra, note 7 at ![]() 403(a).
403(a).
9Supra, note 1 at ![]() 403(3), 22 U.S.C. 7673(c).
403(3), 22 U.S.C. 7673(c).
time and across countries is complicated because the budget code definitions and guidance on what funding and activities were to be included in some budget codes changed over time (OGAC, 2006f, 2007a, 2008a, 2009c, 2010b, 2011a, 2012). The committee chose to assess the available planned/approved funding data using the FY 2011 budget code definitions retrospectively for all years. As shown in Table 6-11, based on planned/approved funds aggregated across all PEPFAR countries, PEPFAR has met this budgetary requirement consistently, with the percentage fluctuating across years between 60 percent and 70 percent.
Some service delivery sites with HIV care and treatment programs may receive financial and other support from more than one source. For treatment programs supported by PEPFAR, the partner country may use the Global Fund, other donors, or country resources at the national or subnational level to support specific components of services in sites where PEPFAR also supports treatment (PEPFAR and USAID, 2007). Indeed, several interviewees said that part of PEPFAR’s work in scaling up treatment was in helping the country government also scale up its own response in partnership with PEPFAR, building on the government’s strong commitment to treatment (272-22-USG; 461-18-USG). Despite this scale-up in government support, the proportion of a government’s contribution to ARV procurement and to treatment varies among countries, and one major theme that emerged about funding from interviewees in many PEPFAR partner countries was that external donor resources, especially PEPFAR and the Global Fund, provide a significant proportion of treatment costs. This issue will be discussed briefly later in this chapter and in much more depth in Chapter 9 in the section on financing and in Chapter 10 on sustaining the response.
PEPFAR-Supported Enrollment in ART
PEPFAR Treatment Indicator Data: Targets and Results
PEPFAR has only very limited central reporting of indicators to reflect the performance of PEPFAR’s treatment programs. The primary indicator is an overall output indicator that reports the number of adults and children with advanced HIV infection who are receiving ART (OGAC, 2009d). This indicator serves to track the overall legislative target for treatment. Table 6-12 shows that the number of people on treatment supported by PEPFAR has increased over time and that, after the initial year of implementation, the annual target has been consistently met or exceeded. PEPFAR reached the initial legislative 5-year target of providing treatment to more than 2 million people (OGAC, 2009a). In the second Five-Year Strategy PEPFAR set a target of providing direct support for more than 4 million people on treatment by 2014, which would more than double the number of people
| FY 2005 | FY 2006 | FY 2007 | FY 2008 | FY 2009 | FY 2010 | FY 2011 | Total | |
| Prevention | $382.1 | $383.7 | $634.2 | $904.7 | $1,086.9 | $1,142.5 | $1,259.1 | $5,793.2 |
| Care | $187.9 | $252.9 | $505.2 | $714.9 | $870.1 | $841.3 | $883.3 | $4,255.5 |
| Treatment | $376.3 | $602.3 | $980.7 | $1,342.6 | $1,209.0 | $1,135.5 | $1,126.7 | $6,773.1 |
| Prevention/Care/Treatment Total | $946.3 | $1,238.9 | $2,120.1 | $2,962.2 | $3,166.0 | $3,119.3 | $3,269.1 | $16,821.8 |
| Care and Treatment % of Total | 60% | 69% | 70% | 69% | 66% | 63% | 61% | 66% |
NOTES: This table represents funding for all PEPFAR countries as planned/approved through PEPFAR’s budget codes. The budget codes are the only available source of funding information disaggregated by type of activity and are therefore used in this report as the most reasonable and reliable approximation of PEPFAR investment by programmatic area. Data are presented in constant 2010 USD for comparison over time. See Chapter 4 for a more detailed discussion of PEPFAR’s budget codes and the available data for tracking PEPFAR funding.
SOURCES: OGAC, 2005, 2006g, 2007c, 2008b, 2010c, 2011d,e.
who had been directly supported on treatment during the first 5 years of PEPFAR (OGAC, 2009a). This target was recently increased and the timeline was shortened, so that the target is now 6 million people by the end of 2013 (Obama, 2011). In FY 2010, PEPFAR provided ART to more than 3 million individuals.
TABLE 6-12 Number of Adults and Children with Advanced HIV Infection Receiving ART (in Millions)
| FY 2004 | FY 2005 | FY 2006 | FY 2007 | FY 2008 | FY 2009 | FY 2010 | |
| Result | 0.1 | 0.2 | 0.5 | 1.1 | 1.7 | 2.5 | 3.2 |
| Target | — | 0.3 | 0.5 | 0.9 | 1.4 | 2.2 | 2.9 |
| % of Target | 86 | 102 | 117 | 124 | 113 | 109 | |
NOTES: This table represents data for the 31 countries identified as the focus of this evaluation (see Chapter 2). Data correspond to indicator 11.4 (FY 2004–FY 2009): number of individuals receiving ART at the end of the reporting period (OGAC, 2007b) and indicator T1.2.D (FY 2010): number of adults and children with advanced HIV infection receiving ART (OGAC, 2009d).
SOURCE: Program monitoring indicators provided by OGAC.
Because so many treatment programs in PEPFAR partner countries receive joint funding to varying degrees from the Global Fund, it is important to note that the total number of individuals directly supported on ART includes an estimated overlap of individuals receiving ART with support by both PEPFAR and the Global Fund. This overlap estimate is also included in the treatment results reported by the Global Fund. To estimate the overlap, PEPFAR conducts a review of the treatment and funding data with the Global Fund and WHO on a country-by-country basis. In this review, PEPFAR and the Global Fund take into account the percentage or level of contribution from each source to the national HIV/AIDS program in order to determine where there is likely to be overlap (PEPFAR, 2010).
The program monitoring data available to the committee had limited utility for fully understanding the effects of PEPFAR’s treatment programs. One key limitation was that indicator data over time provided to the committee by OGAC had limited disaggregation. Age disaggregation is important in assessing PEPFAR’s pediatric HIV programs and the legislative commitment to providing care and treatment to children in proportion to their relative burden. The current indicator guidance does include central reporting of age-disaggregated data to include infants under 1 year old (OGAC, 2009d). Disaggregation by sex and by specific populations is important in assessing how services are distributed across these identified populations and in assessing the success of PEPFAR’s efforts to implement women- and girl-centered approaches to delivering services, including reaching women through entry points other than PMTCT, and to work toward gender equity in service delivery as well as equitable access for marginalized populations, including men who have sex with men, people who inject drugs, and people who engage in sex work. Another limitation
is a lack of outcome measures for the clients who received services, which is critical to being able to assess the effectiveness or quality of PEPFAR-supported care and support programs.
Results from PEPFAR’s Track 1.0 Partners10
Although the centrally reported treatment indicator data are limited, most country programs and partners collect additional indicators for treatment programs that are not routinely reported centrally. To review additional data that were systematically collected longitudinally across as many countries as possible, the committee requested data from the CDC that were collected through the Track 1.0 partner care and treatment programs. Four Track 1.0 partners have, since PEPFAR was initiated, been major implementers of ART and other HIV services through a program centrally managed by CDC and the U.S. Health Resources and Services Administration. They are each active in multiple countries, implement programs through a wide range of facilities and subpartners, and provide services to a large number of clients (McCullough and Miller, 2009; Sessions, 2006). Taken together, the data provided by CDC reflects Track 1.0 programs in a subset of 13 PEPFAR partner countries that receive a large proportion of PEPFAR treatment investment; the total funding for these 13 countries represented over 90 percent of the total planned/approved treatment funding from FY 2005 to FY 2011 (OGAC, 2005, 2006g, 2007c, 2008b, 2010c, 2011d,e). The Track 1.0 partners were not the only implementers of that funding, but they represented a large proportion of the clients served in each of the countries (OGAC, 2013).
The following section presents data on enrollment from these partners, who are also a source of data used in the subsequent sections on retention and mortality. These data are presented in the aggregate, without identification or disaggregation by partners and countries.
Track 1.0 Enrollment in ART
Since the beginning of PEPFAR in 2005, Track 1.0 partners have supported a steadily increasing total number of people enrolled in ART. Table 6-13 shows the annual number of individuals currently enrolled for the Track 1.0 partners and, for the purpose of comparison, the annual num-
__________________
10 Track 1.0 partners in this report refers to four partners that were the primary large-scale implementers of ART in PEPFAR’s centrally funded Track 1.0 program (for more information, see Appendix C, Methods). These partners also implemented other HIV services and programs, and there were also other centrally funded Track 1.0 partners in other program areas (OGAC, 2006e).
TABLE 6-13 Currently Enrolled Adults in ART, in Thousands (Annual, FY 2005–FY 2010)
| FY 2005 | FY 2006 | FY 2007 | FY 2008 | FY 2009 | FY 2010 | |
| Total currently enrolled in ART, n | ||||||
| Track 1.0 partners | 92.8 | 203.2 | 339.7 | 513.6 | 694.2 | 856.5 |
| Entire PEPFAR program | 249.2 | 541.5 | 1,091.7 | 1,743.7 | 2,485.3 | 3,209.7 |
| Track 1.0 contribution to PEPFAR (%) | 37 | 38 | 31 | 29 | 28 | 27 |
SOURCE: Programmatic data from Track 1.0 partners provided by CDC.
bers across all PEPFAR ART programs. The proportion of PEPFAR ART enrollment supported by the Track 1.0 partners decreased over time as the number of partners implementing ART programs expanded. Beginning in 2011, as the Track 1.0 partners begin to transition patients to other programs, the numbers enrolled for Track 1.0 partners began to decrease (see Figure 6-6); the Track 1.0 transition process is described in more detail in Chapter 10 on the sustainability of the response.
Figure 6-6 shows the increase over time, by quarter, in the number of people enrolled in ART. Not only did the total quarterly enrollment increase steadily until 2011, but also the number of newly enrolled ART patients each quarter increased rapidly through 2009, at which point new enrollment began to level off and even drop slightly. The decrease in new enrollment even as total enrollment continued to increase could in theory be explained by a decrease in individuals newly in need of ART; however, this is not the case in most PEPFAR partner countries. Therefore, the relative slowing of new enrollment in the programs supported by these partners may be because as the number surviving who need to be maintained in care and treatment accumulates and represents an increasing proportion of total capacity, the number of newly enrolled patients may be limited by the available funding, the availability of facilities providing care and treatment, and the availability of providers.
Figure 6-7 and Table 6-14 show the annual new enrollment of adults in these care and treatment programs, disaggregated by sex. Each year there are more initial enrollments in ART among women than among men; the proportion has remained steady over time at about 65 percent women and 35 percent men (see Table 6-14). A greater proportion of women is to be expected, given international estimates of the disparity of HIV infection rates and prevalence between men and women in the largest generalized epi-
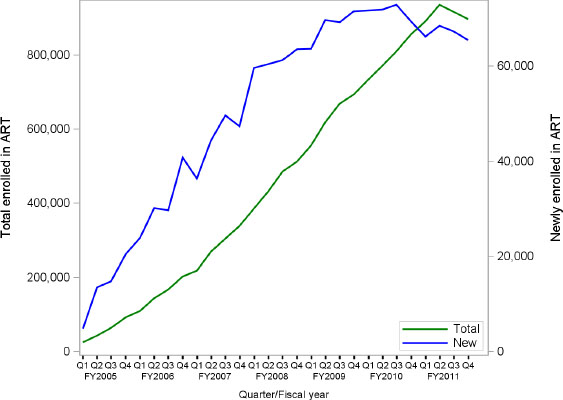
FIGURE 6-6 Total enrolled and newly enrolled individuals (adults and children) in ART (quarterly, FY 2005–FY 2011).
SOURCE: Programmatic data from Track 1.0 partners provided by CDC.
demics and in the key PEPFAR-supported regions where these implementing partners are operating; for example, women account for a disproportionate share of prevalence in Africa, where they make up an estimated 60 percent of people living with HIV (UNAIDS, 2011). However, the data for this subset of countries and partners indicate a larger imbalance than in the prevalence estimates, with men proportionately under-enrolled compared to women. It is important to note that it is very difficult to draw conclusions about these sex differences. The data presented here are aggregated from programs in 13 countries and thus are not matched to country-specific information on the relative disease burden between men and women in these settings; they are not matched to estimates of the need for ART in men and women, which also vary by country. Data in these countries on men and women who are in need but not receiving care and treatment would make it possible to compare coverage rather than simply numbers enrolled.
Within this limitation, it is feasible to observe that the reasons for this imbalance would likely be consistent with the observations described previously in this chapter that men may not be accessing testing and subsequent referrals for enrollment in care and treatment services as readily as women. One reason for this disparity may be differences in provider-initiated test-
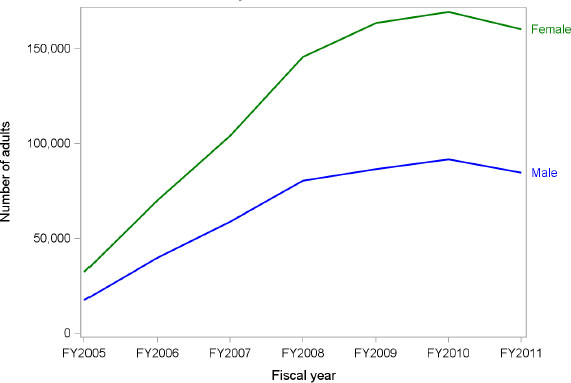
FIGURE 6-7 Number of newly enrolled adults in ART by sex (FY 2005–FY 2011).
SOURCE: Programmatic data from Track 1.0 partners provided by CDC.
ing, primarily because of increased access for pregnant women who are enrolled in ART through the entry point of antenatal care and PMTCT services (WHO, 2012d). Another contributing factor may be differences in health-seeking behavior, which may be influenced by culturally determined gender roles for men and women (Chen et al., 2008). As an interviewee in one country observed:
‘Most [of the] people that go to health centers and access counseling and testing programs are pregnant women getting prenatal care. Men essentially do not go to health centers unless they are dying.’ (166-5-USG)
Differences in access between men and women may also be affected by how services are planned by policymakers or how outreach is targeted by providers. Gaps in access to services for men—and the resulting coverage gaps—have negative implications for the health and well-being of men and for controlling the epidemic. For example, among serodiscordant heterosexual couples with an HIV-positive male partner who is not in treatment there is an increased risk of transmission to the female partner.
Although the relative under-enrollment of men is a major challenge, there are also barriers in accessing services for women, and the contribu-
TABLE 6-14 Newly Enrolled Adults in ART by Sex(Annual, FY 2005–FY 2011)(in Thousands)
| FY 2005 | FY 2006 | FY 2007 | FY 2008 | FY 2009 | FY 2010 | FY 2011 | Total | |
| Newly enrolled adults in ART, n | 50.0 | 110.2 | 163.2 | 226.2 | 250.0 | 261.2 | 244.8 | 1,305.6 |
| Male, n (%) | 17.6 (35) | 39.9 (36) | 58.9 (36) | 80.5 (36) | 86.6 (35) | 91.8 (35) | 84.6 (35) | 459.9 (35) |
| Female, n (%) | 32.4 (65) | 70.2 (64) | 104.2 (64) | 145.7 (64) | 163.4 (65) | 169.4 (65) | 160.2 (65) | 845.7 (65) |
SOURCE: Programmatic data from Track 1.0 partners provided by CDC.
tion from PMTCT as an entry point facilitates access only for pregnant women, primarily those who attend antenatal care at least once in a clinic or who deliver in a health facility. Even when PMTCT does contribute to access to testing and thus may contribute to the proportionally higher enrollment of women in ART, the reality is that results are mixed for efforts to link PMTCT and ART. Interviewees described widely variable experiences across countries concerning the coverage of ongoing ART in women initially identified as eligible during pregnancy, with reports ranging from around 90 percent at the very high end to only 10 percent (272-24-USG; 636-17-PCGOV; 166-13-PCGOV; 116-5-PCGOV; 116-18-PCNGO; 934-5-USG). Several interviewees mentioned efforts to improve ongoing provision of ART to women identified during pregnancy (396-25-PCGOV; 587-5-PCGOV; 636-6-USG; 166-13-PCGOV; 542-9-PCGOV; 116-18-PCNGO; 935-7-USG; 935-13-PCGOV). For example, in one country all maternity hospitals registered HIV-positive women at the government’s AIDS centers and referred them for sero-staging for ongoing treatment (542-9-PCGOV). Some of the challenges in enrolling and retaining women identified as HIV-positive during pregnancy in ongoing ART programs included limited access to CD4 testing, including point-of-care testing; limited staff to provide follow-up and linkages to ART; and a lack of systems for sharing data between PMTCT programs and care and treatment programs (116-18-PCNGO; 587-5-PCGOV; 636-6-USG; 166-13-PCGOV; 935-7-USG).
TABLE 6-14 Newly Enrolled Adults in ART by Sex(Annual, FY 2005–FY 2011)(in Thousands)

SOURCE: Programmatic data from Track 1.0 partners provided by CDC.
Gender-related aspects of access to services for both men and women are discussed in more depth in Chapter 8 on gender.
Pediatric Enrollment in ART
In its OVC guidance, PEPFAR recommends organizing programming according to age-specific health requirements, developmental needs, and interventions using the following age groupings: infants (<2 years), early childhood/toddler (2-4 years), middle childhood (5-11 years), and late childhood/adolescence (12-17 years) (OGAC, 2006d). However, data using these subgroups for age disaggregation are not routinely collected at any level of treatment programs.
The data requested from the CDC for the Track 1.0 partners included age disaggregation of children newly enrolled in ART for the years 2008-2011 (Table 6-15). The total number of children newly enrolled on ART decreased from 2009 to 2011, illustrating the difficulties of implementing treatment for children. The largest number and proportion (Table 6-15 and Figure 6-8) of children enrolled in care are 5 years of age or older. Many of these may be children with HIV infection from maternal transmission who survived even without therapy in the early period that is critical for identifying HIV infection and initiating treatment. The greatest increase
TABLE 6-15 Newly Enrolled Children in ART (FY 2005–FY 2011)(in Thousands)
| FY 2005 | FY 2006 | FY 2007 | FY 2008 | FY 2009 | FY 2010 | FY 2011 | Total | |
| Newly enrolled children in ART, n | 3.8 | 9.9 | 14.6 | 18.8 | 28.1 | 24.9 | 22.7 | 122.6 |
| 0–1 years, n (%) | 3.9 (21) | 6.4 (23) | 6.9 (28) | 7.0 (31) | 24.1 (20) | |||
| 2–4 years, n (%) | 5.3 (28) | 6.5 (23) | 6.3 (25) | 5.5 (24) | 23.7 (19) | |||
| 5–14 years, n (%) | 8.7 (46) | 10.4 (37) | 11.7 (47) | 9.6 (42) | 40.4 (33) | |||
| Unclassified, n (%) | 3.8 (100) | 9.9 (100) | 14.6 (100) | 0.8 (4) | 4.8 (17) | 0.1 (<1) | 0.6 (2) | 34.5 (28) |
NOTES: Dissagregated pediatric ages were not reported prior to FY 2008. When the total number of children enrolled exceeds the sum of those classified within specific age ranges, the difference is displayed in the Unclassified row.
SOURCE: Programmatic data from Track 1.0 partners provided by CDC.
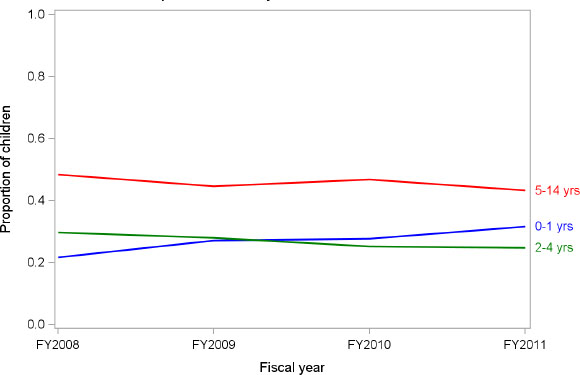
FIGURE 6-8 Proportion of newly enrolled children in ART by age groups (FY 2008–FY 2011).
SOURCE: Programmatic data from Track 1.0 partners provided by CDC.
between 2008 and 2009 occurred in those who were less than one year old, but the increase in that age group slowed from 2009 to 2011. This is likely the net of successes in preventing infections with PMTCT combined with the challenges of identifying infected infants in the first 12 months of life. The proportion of newly enrolled children who are less than 1 year old has increased to about 30 percent of all children who are treated, while the 2- to 4-year-old age group has dropped to about 25 percent, and the 5- to 14-year-old age group has also declined over time.
These data are consistent with the experiences of interviewees, who also described low enrollment in pediatric ART and a failure to start children early enough on ART (240-24-USG; 461-19-USG; 166-18-USNGO; 636-17-PCGOV; 934-25-USPS; 396-7-PCGOV; 461-18-USG; 166-18-USNGO; 331-44-USNGO; 396-42-PCGOV; 461-10-PCNGO; 116-20-USNGO). However, they also observed that the numbers of children being enrolled in treatment had increased with PEPFAR’s support, noting that the first pediatric treatment offered in facilities was supported by PEPFAR and that PEPFAR had extended life for children infected with HIV (240-8-USG; 461-24-PCNGO; 166-18-USNGO; 166-29-PCGOV; 461-26-PCACA; 636-12-USACA). PEPFAR provided funding for first- and second-line treatment for children in several countries visited (240-5-PCGOV; 587-6-CCM; 587-13-USG; 587-22-USG; 166-15-USACA; 396-56-USNGO) and supported partners that were leaders in pediatric care and treatment (240-19-USACA; 272-22-USG; 396-25-PCGOV; 396-42-PCGOV; 636-17-PCGOV; 396-56-USNGO; 461-13-USACA). One interviewee
described how PEPFAR had supported scale-up of pediatric HIV services by having all of its treatment partners implement pediatric units in their facilities (272-22-USG). Other interviewees described PEPFAR as working closely with the partner country government and with other external donors, such as the Clinton Foundation (240-19-USACA; 935-6-USACA; 396-21-USG). PEPFAR has also covered gap periods for pediatric ART when it was needed (934-5-USG; 934-12-CCM).
Another contribution mentioned by interviewees in several countries was PEPFAR’s support for the training of providers in pediatric treatment, from working with the ministry of health and local universities to provide pediatric HIV training and develop technical materials, curricula, and standard operating procedures (240-19-USACA; 240-24-USG; 272-22-USG; 461-13-USACA; 636-12-USACA) to the direct training and mentoring of staff on the treatment of HIV-exposed infants and HIV-positive children (636-17-PCGOV; 166-18-USNGO; 166-29-PCGOV; 396-21-USG; 396-42-PCGOV; 461-24-PCNGO; 636-12-USACA; 636-19-USNGO; 935-6-USACA; 935-7-USG). Among the examples provided were the training of generalist doctors and medical officers to deal with the special issues associated with HIV in children and also the use of experienced physicians as the trainers with follow-up for remote provinces. Other efforts have sought to shift pediatric treatment from medical doctors to nurses and lower-level health care providers (240-24-USG; 272-22-USG; 636-19-USNGO), but this has met with varying levels of success as the physicians, pharmacists, and newly trained providers were less comfortable with taking on initiation and management of treatment for pediatric patients than for adult patients (272-22-USG).
Integration with other health services was another PEPFAR-supported strategy for improving access to and enrollment in pediatric treatment. Interviewees described examples of integration with maternal and child health, especially for children less than 5 years old (240-24-USG; 116-2-USG; 461-13-USACA); integrated care in ‘family clinics’ (116-7-USG); efforts to better identify children in need of HIV services through maternal and child health programs (461-13-USACA; 240-24-USG; 166-10-USNGO; 396-21-USG); and identification of HIV-infected sick children in HIV/TB nutrition wards (461-13-USACA).
PEPFAR has also supported community involvement, working with home-based care programs, social workers, lay counselors, and others in the community to reduce stigma, provide ART adherence counseling, identify children for referrals for HIV testing, and mentor parents as a way to increase access to pediatric ART (396-21-USG; 934-29-USNGO; 636-15-PCNGO; 461-13-USACA; 396-42-PCGOV; 461-19-USG; 272-15-PCNGO). This linkage between the community and treatment facilities was identified by one interviewee as an area where more attention would be warranted (934-29-USNGO) and by another as something that has been piloted successfully but that is too expensive to continue (461-19-USG). Another PEPFAR contribution to this population has been advocacy to bring pediatrics to the forefront of the agenda in ministries of health
through organizing national workshops with high-level ministry of health officials (240-19-USACA) and the support of an advocacy focal person at the ministry of health who specialized in pediatrics (461-13-USACA).
Retention and Adherence
Retention in care and treatment and patient adherence to ART are both critical to increasing the survival of patients, improving the quality of their lives, increasing HIV viral suppression, reducing viral transmission, and reducing rates of drug resistance. Four stages for retention in the continuum of HIV care have been described: from the diagnosis of HIV to the enrollment of a patient in care, from the enrollment in care to ART eligibility, from ART eligibility to ART initiation, and from ART initiation to lifelong ART. All four of these stages offer challenges for retention in care and treatment (Rosen and Fox, 2011; WHO, 2012c).
Studies to understand retention in ART often do not share the same methodology, making it difficult to compare the results, and there is a lack of studies that assess long-term retention (WHO, 2012c). Rosen and Fox, who reviewed data from patients in sub-Saharan Africa, estimated 60 to 70 percent retention in ART at two years (Fox and Rosen, 2010; Rosen et al., 2007). A study conducted in Tanzania, Zambia, and Uganda through medical chart reviews and questionnaires sent to health care center managers concluded that men, the very sick, and younger people had more chance to be lost to follow-up and that dispensing ART at the community facility level was an important strategy for retention (Koole et al., 2012). A systematic review has shown that physical tracing of patients is associated with better retention, with a decrease of loss to follow-up as well as greater ascertainment of patient outcomes such as mortality and transfer (McMahon et al., 2012). Several studies have concluded that community-based adherence support improves ART outcomes in adults, such as reduced mortality and loss to follow-up and improved virological suppression after starting ART (Chang et al., 2010; Fatti et al., 2012; Igumbor et al., 2011).
Track 1.0 Data on Retention and Loss to Follow-Up
Although the retention of patients in care—as well as patient adherence to ART—is considered essential to successful treatment, the centrally reported indicators made available to the committee did not serve to assess retention over time across PEPFAR country programs. However, in the provision of treatment at the facility, district, and sub-partner levels, adherence and retention have been monitored by implementing partners who need the data to assess the delivery of ART and the quality of care and treatment.
One of the four Track 1.0 partners was able to share with the committee an analysis of retention and loss to follow-up for more than 200,000 patients at more than 200 care and treatment sites across nine PEPFAR partner countries. Treatment retention at 12 months, defined as the number of patients whose care terminated for any reason subtracted from the number of patients who ever began treatment, is shown in Figure 6-9, disaggregated by population and by the year ART was started. The populations with the highest retention were the pediatric population and adult females, while the lowest retention was found among adult males. Retention rates trend downward for more recent initiation of ART start, with a significantly lower retention rate among those who started in 2010 compared to previous years.
Data on loss to follow-up (LTFu), defined as a patient having missed a clinic appointment for 90 days or more, show a similar pattern, as reflected by the proportion of patients that remain in care, attending appointments, by population (see Figure 6-10) and by year of ART initiation (see Figure 6-11). LTFu was higher among adult males than among adult females and pediatric patients. LTFu also increased for more recent years of ART initiation. After 12 months on ART, patients who started in 2004 had the lowest LTFu, while those who started in 2010 had the highest. Similar trends were observed at 24, 36, 48, 60, and 72 months. It is important to note that one limitation to these analyses is that some deaths may have been reported as losses to follow-up because the patients’ treatment records were not linked to mortality records.
One explanation for the trend toward increasing loss to follow-up in the more recent years of ART initiation may be that financial resources and staff became more and more constrained over time in the face of increasing numbers of patients in care and treatment and therefore efforts focused on retention, such as tracking activities, became more difficult to sustain. In addition, compared to those enrolled in the early years of PEPFAR, when the focus was rapid scale-up in areas with high population density and facility capacity, those enrolled in recent years are being reached as ART expands to more geographically remote areas with lower-level health facilities, and these newly enrolled patients may face disproportionately greater challenges to retention, such as transportation barriers, economic limitations, and facilities with lower overall capacity. The following section presents perspectives from interviewees in partner countries that further inform the issues of retention and adherence in the context of implementing PEPFAR-supported programs.
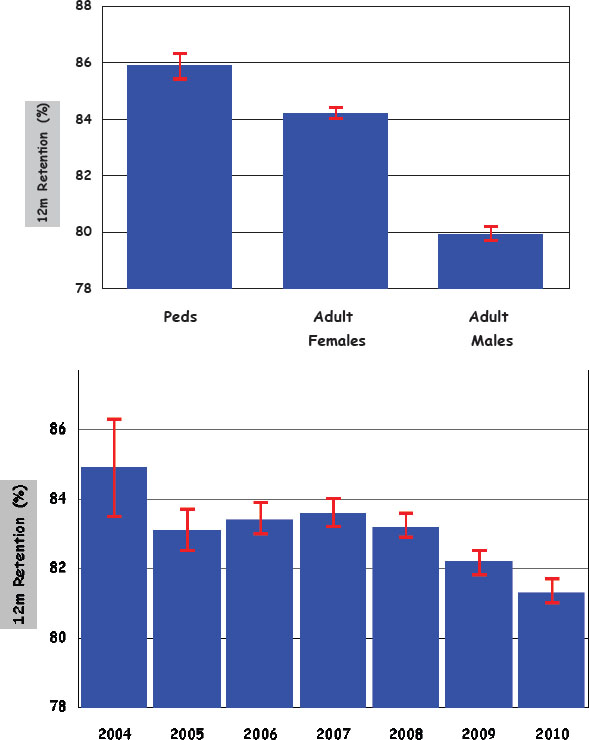
FIGURE 6-9 Twelve-month retention (alive and in care) by population and by the year ART was started in a subset of patients in nine PEPFAR partner countries.
NOTE: Red bars correspond to 95% confidence intervals.
SOURCE: Programmatic data provided by Track 1.0 partner.
Perspectives on Challenges with Retention, Loss to Follow-Up, and Adherence
During the country visits conducted by the committee, interviewees identified the retention of PLHIV in care and treatment services and ad-
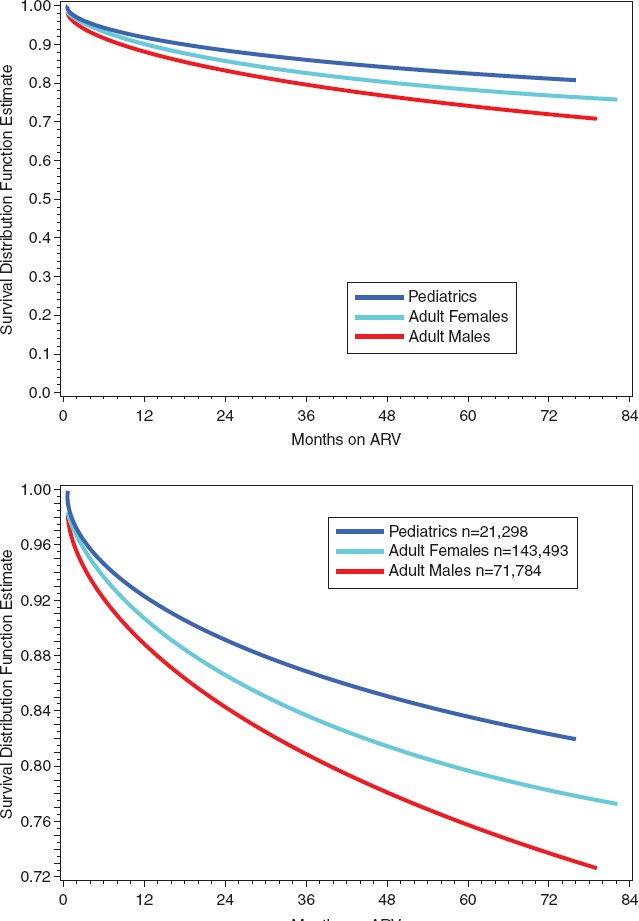
FIGURE 6-10 Proportion of patients on ART that remain in care on ART over time by population in a subset of patients in nine PEPFAR partner countries
NOTES: A decreasing proportion of patients on ART that remain in care reflects increasing loss to follow-up. Bottom panel shows expanded view of top panel. Some deaths may be included in these data as losses to follow-up when patient treatment records were not linked to mortality records.
SOURCE: Programmatic data provided by Track 1.0 partner.
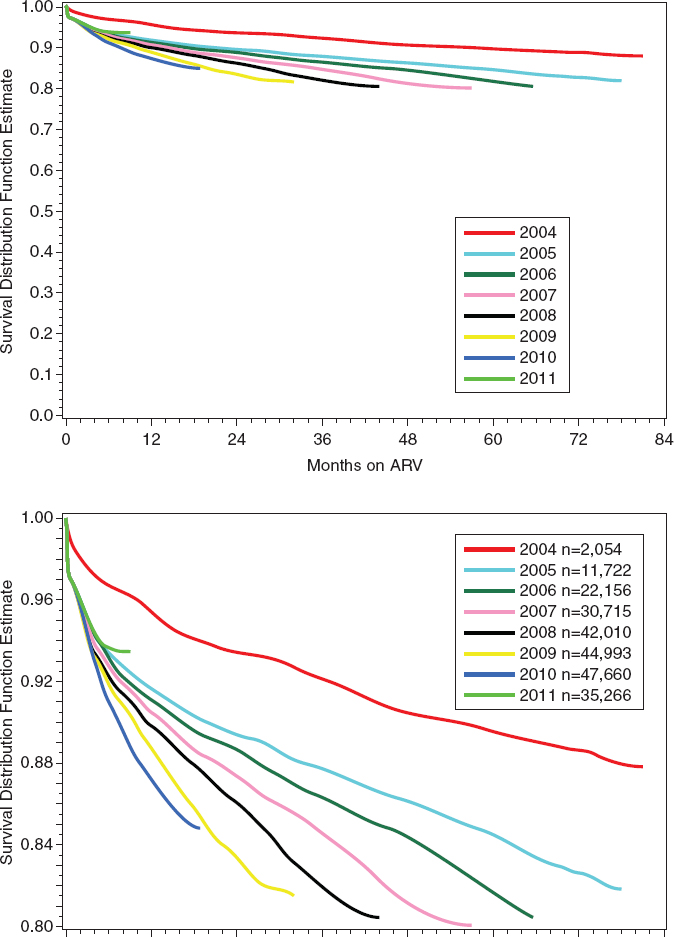
FIGURE 6-11 Proportion of patients on ART that remain in care over time by year of ART initiation in a subset of patients in nine PEPFAR partner countries.
NOTES: A decreasing proportion of patients on ART that remain in care reflects increasing loss to follow-up. Bottom panel shows expanded view of top panel. Some deaths may be included in these data as losses to follow-up when patient treatment records were not linked to mortality records.
SOURCE: Programmatic data provided by Track 1.0 partner.
herence of patients to treatment as an area of great concern with respect to both HIV-positive individuals who had been diagnosed but had not yet initiated treatment and to individuals who had been linked to services (240-15-USG; 240-19-USACA; 331-14-USG; 166-15-USACA; 272-22-USG; 240-24-USG; 935-16-USNGO; 636-17-PCGOV). The challenges with linkages from testing to care and treatment were described earlier in this chapter. The follow-up of those who had initiated treatment was similarly reportedly as a ‘huge challenge for treatment’ (240-19-USACA). Interviewees recognized that ‘HIV patients need to have strong adherence, but loss to follow-up is very high’ (166-15-USACA) and also that adherence ‘is a big problem’ (240-15-USG). One reason for concern about patients’ adherence to prescribed ARV regimens centered on the following perspective voiced by one interviewee: ‘[I]f [we] don’t push adherence, then resistance will become outrageous’ (272-22-USG).
Retention and adherence monitoring is usually done by keeping track of return visits and pill counts as well as through clinical assessments, self-reporting, and tracing of patients in the community (935-15-ONGO; 935-16-USNGO; 272-32/35-PCNGO; 935-29-USACA; 116-18-PCNGO). Interviewees differed on the specific criteria for designating an individual as lost to follow-up, but they generally referred to missed appointments as signaling an initial loss of contact with the patient and potential loss to follow-up. Interviewees cited death as a major contributor to loss of follow-up (166-15-USACA; 240-19-USACA), due in part to HIV-infected individuals being identified late at a point when they had advanced disease. The type of facility was also described as affecting loss to follow-up, with mortality being a more likely cause for loss to follow-up at hospitals serving more critically ill patients (240-15-USG).
Among the other reasons for loss to follow-up or lack of adherence that interviewees described were patient-initiated treatment cessation or ‘drop out,’ transfer to another treatment site, distance from treatment site and lack of access to transportation, stigma, and cultural beliefs (240-25-PCGOV; 166-18-USNGO; 240-19-USACA; 272-32/35-PCNGO; 587-18-PCGOV). In general, distance combined with a lack of resources for transportation to treatment sites was commonly noted as a major contributor to loss to follow-up (272-3235-PCNGO; 240-19-USNGO; 935-15-ONGO; 636-17-PCGOV). Transportation was a particular barrier when there was a need to travel greater distances for specialized care, such as care at a hospital-based pediatric center (166-18-USNGO; 587-18-PCGOV). Concerns about stigma and lack of family support affected some individuals’ willingness to continue treatment or their willingness to use health facilities in their home communities; this exacerbated the barrier of transportation when PLHIV sought health facilities more distant from their places of residence to have a greater degree of privacy (935-11-PCNGO; 166-18-USNGO; 587-18-PCGOV). Interviewees also recognized malnutrition or lack of food as an important issue for PLHIV who are taking ARVs (461-10-PCNGO; 935-13-PCGOV; 636-17-PCGOV). In addition to the need for food security among some partner country populations in general
and for nutritional support among PLHIV in particular, one interviewee observed, ‘people on ARVs’ bodies change, and they have an appetite. Appropriate nutrition improves adherence’ (461-10-PCNGO). Individuals’ cultural beliefs and experiences were also described as having a role in adherence. A treatment-related program in one country, for example, faced the ongoing challenge of getting people to understand how ART works and the need to continue treatment: ‘people would do well in the beginning and then stop taking medication’ (331-12-USG). In some cases patients perceived that ARVs were aggravating their ill health because of their experience of side effects upon initiating drug treatment (240-25-PCGOV; 587-18-PCGOV). In some countries interviewees reported that some PLHIV believed ARVs were unnecessary because they were using traditional methods they thought would heal them (240-25-PCGOV; 935-13-PCGOV; 935-15-ONGO; 636-17-PCGOV).
Although pediatric patients had relatively better retention in the Track 1.0 data presented here, interviewees reported that achieving retention and adherence among the pediatric population is particularly challenging (935-19-PCGOV; 166-18-USNGO). Adolescents were of particular concern because of the lack of a support structure and because of their adjustment as they mature as a person living with HIV, which is sometimes accompanied by anger or fear about their status and a rebellion against ARVs (272-22-USG; 636-6-USG).
PEPFAR Efforts to Improve Adherence and Retention
Interviewees spoke about the personnel and the strategies they used to follow up and to increase retention and adherence among PLHIV on ARVs. Most of the strategies were based on the premise of personal contact with patients. In general, interviewees believed that ‘some kind of individual contact is important for adherence’ (272-22-USG). The personnel involved in following up with patients were peer educators, counselors, case managers, urban or rural health extension workers, home-care workers, health care providers, and trained volunteers (331-12-USG; 240-19-USACA; 272-22-USG; 166-18-PCNGO; 196-21-PCGOV; 272-14-PCNGO; 935-15-ONGO; 935-16-USNGO; 935-20-PCNGO; 935-25-PCGOV; 935-29-USACA; 461-18-USG; 396-44-PCGOV; 116-18-PCNGO; 166-15-USNGO; 166-8-USG; 240-15-USG). The follow-up and adherence-promotion strategies that interviewees described were pre-treatment patient preparation, monitoring, tracking, empowerment, home visits, phone calls and text messages (including automated cell systems), and hospital–health center networks with outreach workers (272-22-USG; 331-12-USG; 935-15-ONGO; 240-19-USACA). In many cases PLHIV served as peer educators, counselors, case managers, and trained volunteers in providing adherence support (240-ES; 331-ES; 935-ES). Another strategy that interviewees said they used to improve retention and adherence were improving laboratory services to improve efficiency and reduce wait times for CD4 testing, including implementing point-of-care testing (934-14-PCGOV; 935-7-USG; 935-13-PCGOV). Challenges
related to accessing care and treatment are also being addressed in some countries by expanding the availability of clinics in more geographically widespread areas, efforts made feasible in part by task shifting of ART provision and removing restrictions on the services that can be provided at lower-level facilities (934-14-PCGOV; 240-2-USG; 240-15-USG; 166-22-USPS).
Conclusion: Retention and adherence are critical and persistent challenges in PEPFAR-supported HIV care and treatment programs. Understanding the factors that contribute to the lack of retention and the most effective strategies to improve it is needed to fully maximize the role of care and treatment in a sustainable HIV/AIDS response.
ARV Drug Resistance and Treatment Failure
Data regarding the emergence of HIV drug resistance in resource-limited countries have not been collected in a systematic, standardized, or representative manner; nevertheless, two recent analyses of the published literature provide sufficient information to generate a reasonable sense of the impact of treatment rollout on HIV drug resistance. Besides conferring substantial benefits on survival and quality of life, broad access to antiretroviral therapy in resource-limited settings has, not surprisingly, led to the emergence of both acquired and transmitted drug resistance (Gupta et al., 2012; Stadeli and Richman, 2012).
The prevalence of transmitted drug resistance (TDR) varies with geographic region, which is likely related to the different timelines for access to ART. For example, significantly higher rates of TDR exist in Middle and East Africa than in West or Southern Africa, which in general reflects the timing of the roll-out of ART, with the magnitude of drug resistance increasing with the duration of access to treatment in the population. In addition to differences in the length of time that ART was available, the differences in the rates of TDR could be attributable to various known risk factors for the development of HIV drug resistance: interruption in medication availability (such as the stock of medication running out), suboptimal adherence, the regimens prescribed (cheaper but less effective and less well-tolerated regimens are associated with more rapid failure and rates of drug resistance), the stage of the disease at the time of treatment initiation, and limited use of viral load monitoring to detect regimen failure (Gupta et al., 2012; Hamers et al., 2011, 2012; Stadeli and Richman, 2012).
The available data largely come from studies of convenience samples rather than from studies designed to be representative of the total populations at risk for drug resistance. Furthermore, available studies vary widely in their designs, methodologies of data analysis, patient popula-
tions, inclusion criteria, viral load thresholds for genotype sequencing, sequencing protocols, and drug resistance mutation lists. Even given these limitations, these data taken together offer potential implications for what needs to be addressed for the future of HIV/AIDS treatment programs in resource-limited settings. High rates of acquired drug resistance suggest poor adherence, suboptimal regimens, and a lack of monitoring for treatment failure and drug resistance (Gupta et al., 2012; Stadeli and Richman, 2012). Drug-resistance monitoring programs in resource-limited settings are limited by cost and laboratory availability (Kimmel et al., 2010). In the absence of laboratory monitoring, strategies to monitor and improve treatment delivery and patient adherence may help minimize sustained virologic failure more than clinical monitoring alone (El-Khatib et al., 2011; Hong et al., 2010).
In the countries visited for this evaluation, interviewees expressed concerns about treatment failure. These concerns included the potential consequences of interrupted drug treatment regimens due to stock-outs or changes in drug regimens that occurred for nonclinical reasons (i.e., drug treatment from neighboring countries that used different regimens, often sought as a result of stock-outs) (934-5-USG), a lack of strategies and tools to diagnose and address treatment failure (461-18-USG), and low treatment failure detection rate for both adults and children (240-24-USG) as well as a lack of information about the proportion of people taking ARVs who were failing treatment (240-15-USG). Interviewees reported varying degrees of access to ARV drug-resistance testing resources across countries and in some cases reported that the expense of specific testing for drug resistance made it unaffordable (461-10-PCNGO; 272-32/35-PCNGO). Although interviewees described that most of those on ARVs were taking first-line drugs (587-18-PCGOV; 461-18-USG), the expectation was that ‘as we move down the road we will need drug resistance testing and support for second-line drugs’ (461-18-USG). One interviewee emphasized the need to evaluate ‘the number of patients on second-line therapy [since it] is very low and, based on knowledge from other countries, it should be higher’ (240-15-USG). An interviewee in one country who emphasized the challenge that patients are not adherent noted that there is resistance to second-line regimens and a need for third-line regimens (396-44-PCGOV), and an interviewee in another country identified a lack of guidance from OGAC on how to switch from second- to third-line drugs (461-18-USG).
Interviewees in several countries did identify PEPFAR as supporting not only ART but also advancing the monitoring of the emergence of drug resistance using advanced molecular techniques and conventional techniques (240-21-PCGOV; 587-18-PCGOV). Several countries mentioned efforts to monitor drug resistance. Some countries were awaiting their drug resistance threshold survey results (934-15-PCGOV; 240-21-PCGOV). Drug resistance surveillance monitoring recently started in one partner country (272-13-USG), with the government
implementing pharmacovigilance work and many partners tracking genome changes (272-22-USG). WHO was implementing an HIV drug-resistance protocol survey through a national care and treatment center, with plans to distribute the survey to sentinel sites in order to facilitate routine data collection on drug resistance (587-13-USG; 587-18-PCGOV). PEPFAR supported drug-resistance surveillance activities using the WHO early warning indicators in several countries (240-21-PCGOV; 116-1-USG; 587-18-PCGOV), including pediatric drug-resistance surveillance activities (116-1-USG). The Global Fund was also mentioned as supporting drug-resistance studies in drug-naïve patients in one partner country (331-24-PCGOV; 331-28-PCGOV).
Conclusion: The expansion of treatment has an ancillary effect of increasing drug resistance. The earlier that ART programs were implemented in a region, the more drug resistance is present. Because of the limited availability of second-line antiretroviral drugs in resource-limited settings, as drug resistance increases, the need for an expanded pharmaceutical arsenal for effective treatment intensifies. The emergence of HIV drug resistance is cause for greater efforts to improve the effectiveness and expand the implementation of adherence support, treatment-failure and drug-resistance monitoring strategies, and treatment options in resource-limited settings.
Impact of PEPFAR-Supported Care and Treatment Programs on Mortality
Across countries, many interviewees of all stakeholder types identified the lives saved through HIV care and treatment programs as one of the greatest successes of PEPFAR (935-ES; 636-ES; 461-ES; 240-ES; 331-ES; 116-ES; 166-ES; 272-ES; 396-ES; 934-ES). As one interviewee simply put it: ‘people are not dying because they are on ART’ (272-22-USG).
The congressional mandate for this evaluation requested an evaluation of the impact of care and treatment programs on 5-year survival rates. As described earlier in this chapter, the benefits of ART in reducing mortality have been well established (Bussmann et al., 2008; Herbst et al., 2009; Jahn et al., 2008; Mat Shah et al., 2012; Mermin et al., 2008). However, in general for ART programs, data on 5-year survival rates is very limited in any setting and for any population, and it is not available across PEPFAR countries and programs. Therefore, it was not possible to assess this outcome comprehensively for PEPFAR beneficiaries. One of the four Track 1.0 partners was able to share with the committee an analysis of survival from a subset of patients enrolled in ART representing facilities in nine PEPFAR countries. Figure 6-12 shows survival by population, and Figure 6-13 shows survival by year of ART start.
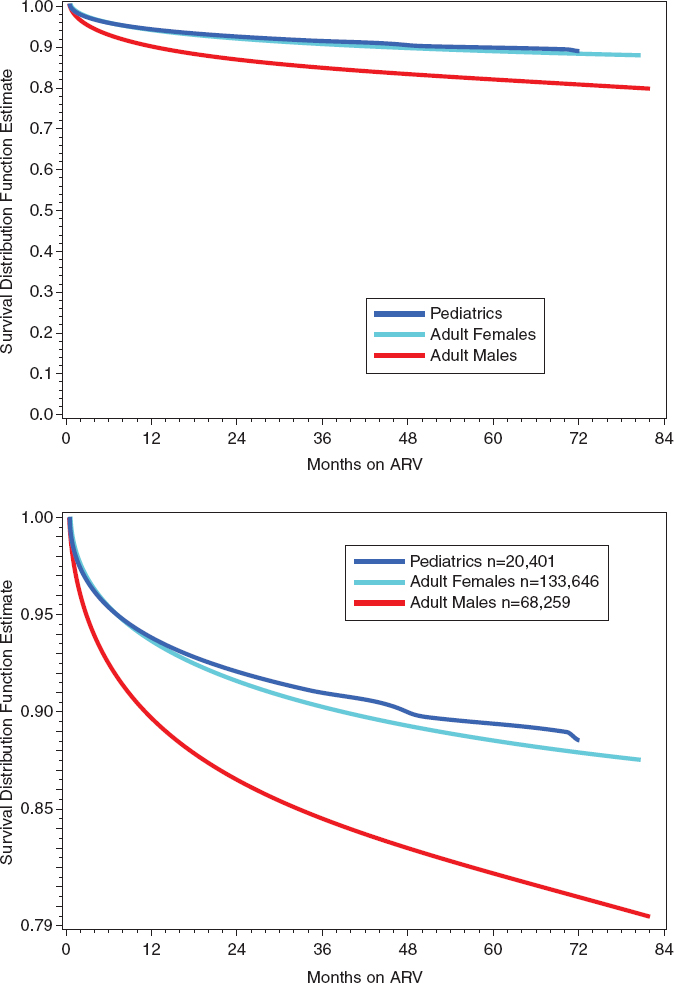
FIGURE 6-12 Survival by population (2004–2011) in a subset of patients in nine PEPFAR partner countries.
NOTE: Bottom panel shows expanded view of top panel.
SOURCE: Programmatic data provided by Track 1.0 partner.
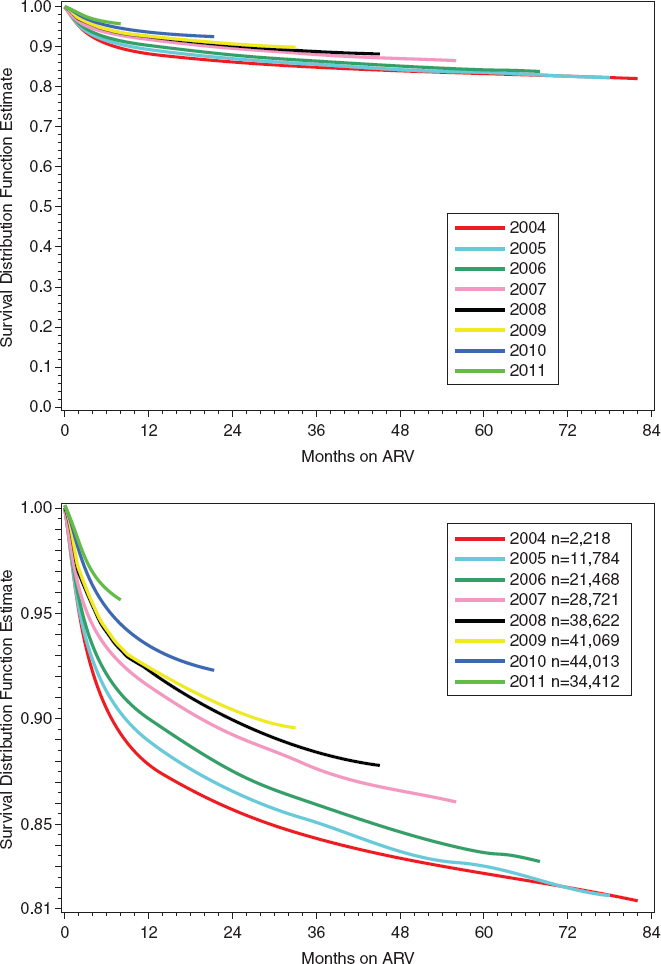
FIGURE 6-13 Survival by year of ART initiation (2004–2011) in a subset of patients in nine PEPFAR partner countries.
NOTE: Bottom panel shows expanded view of top panel.
SOURCE: Programmatic data provided by Track 1.0 partner.
These data suggest that survival after initiation of ART improved each year. This trend may result from patients starting treatment at earlier stages of disease and thus having better outcomes. This is consistent with a theme, described earlier in the section on care and support, that emerged from the interviews—that the increasing availability and success of ART has led to improved health outcomes for PLHIV. These data also exhibit clear sex differences in survival, with women faring better than men; this is similar to the result on retention presented earlier. An additional analysis from a subset of these data representing seven PEPFAR countries reveals similar sex differences in survival on ART (Figure 6-14a), including a breakdown of characteristics at baseline (Figure 6-14b).
These data indicate that men present later in the disease course and with more complications. One reason for this may be that, as described earlier, many women enrolled in ART are identified through screening for PMTCT (WHO, 2012d), an entry point that is not dependent on symptomatic presentation for HIV and is likely to catch more women in earlier stages.
The enrollment, retention, and mortality outcomes presented in this chapter for patients enrolled in these PEPFAR-supported treatment programs are consistent with the published literature, where men have also been shown to have a higher mortality rate than women when receiving antiretroviral therapy (Chen et al., 2008; Taylor-Smith et al., 2010). Possible reasons for the poorer outcomes on ART for men than for women include poor adherence to therapy (Chen et al., 2008; Taylor-Smith et al., 2010); starting therapy at a more advanced stage of the disease (Chen et al., 2008; Geng et al., 2011; Hawkins et al., 2011; Taylor-Smith et al., 2010); cultural norms with respect to stigma, fear, and pride (e.g., the culture of masculinity) (Chen et al., 2008); biological sex differences related to doses of the specified drugs in therapy (Taylor-Smith et al., 2010); and other outside factors such as smoking, alcohol consumption, and life expectancy (Taylor-Smith et al., 2010).
Issues related to the differences between men and women in HIV-related services are also discussed in Chapter 8.
Impact of PEPFAR on Population Health Outcomes
In addition to information about survival and mortality outcomes for patients enrolled in PEPFAR-supported care and treatment programs, an important question for an impact evaluation of PEPFAR is whether the PEPFAR program has had an impact on mortality at the population level. PEPFAR-supported HIV programs have the potential to reduce population mortality through their full range of activities and efforts, but the most
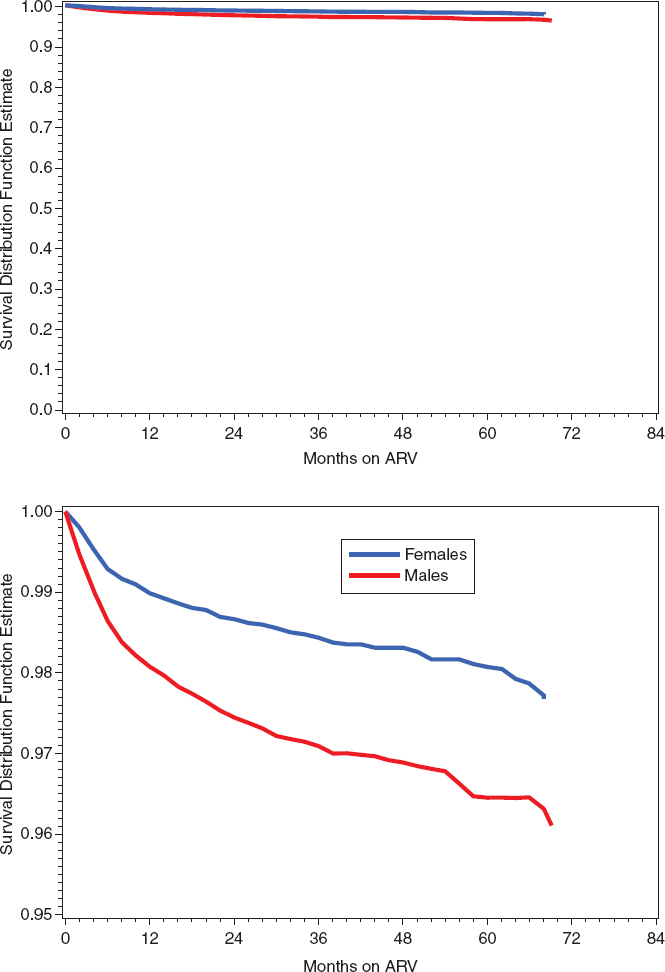
FIGURE 6-14a Differences between men and women on ART in survival (7 countries, 165 clinics), 2004-2011.
NOTE: Bottom panel shows expanded view of top panel.
SOURCE: Programmatic data provided by Track 1.0 partner.
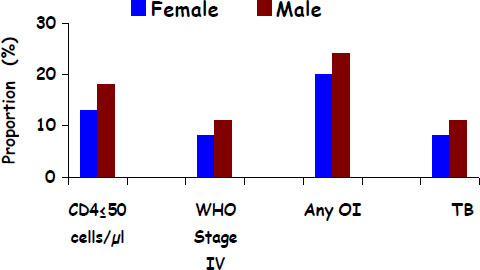
FIGURE 6-14b Differences between men and women on ART in baseline characteristics (7 countries, 165 clinics), 2004–2011.
NOTE: CD4 = cluster of differentiation 4; OI = opportunistic infection; TB = tuberculosis; WHO = World Health Organization.
SOURCE: Programmatic data provided by Track 1.0 partner.
direct plausible pathway to affect mortality is through PEPFAR’s support of HIV care and treatment programs.
Several recently published papers using statistical methods to address this question have compared PEPFAR focus countries to non-focus countries (Bendavid and Bhattacharya, 2009; Bendavid et al., 2012; Duber et al., 2010). The committee reviewed these analyses as one source of information to assess the impact of PEPFAR on HIV/AIDS. One of these analyses did not find an effect on health outcomes (Duber et al., 2010), perhaps due to timeframe and data limitations, but the other analyses indicated a measurable population health impact of PEPFAR on adult mortality in a subset of partner countries (Bendavid and Bhattacharya, 2009; Bendavid et al., 2012). However, none of the studies covered the full scope of countries included in this evaluation, and using non-focus countries as a control is problematic because, although they were not focus countries, they nonetheless received some level of PEPFAR funding. These studies also had other limitations related to the difficulty of evaluating a large, complex program retrospectively, such as limited data availability and quality and the difficulty of controlling for non-PEPFAR factors in the analyses.
During its deliberations, the committee explored the possibility of conducting its own modeling to evaluate the impact of PEPFAR. After careful consideration, the evaluation committee determined that within the scope, time, and resources of this evaluation it was not feasible to conduct statisti-
cal analyses to correlate changes in key outcome or impact indicators with explanatory variables in order to compare countries with variable levels of PEPFAR funding over time. Several key factors contributed to this decision.
One such factor was that there are critical differences among PEPFAR countries in demographics, social and economic factors, the epidemiology of the epidemic, and the availability of appropriate data. Similarly, in order to compare PEPFAR countries, which were not chosen randomly, to non-PEPFAR countries, an analysis would need to account for important differences related to economic, political, and health factors; population sizes; the stage of the epidemic; and available infrastructure and capacity prior to the introduction of PEPFAR. Furthermore, many countries receive some level of PEPFAR investment (see Chapter 1), and where PEPFAR has not been implemented or has been implemented with less intensity, programs with support from other external or national funding sources may have implemented similar interventions to achieve similar objectives. Therefore, it is a critical challenge to identify control countries that can be appropriately compared to PEPFAR countries.
Another important factor was the lack of reliable data across all of the countries of interest for key benchmark indicators, including HIV-related deaths and all-cause mortality, despite intense efforts reviewing multiple sources for these data. Potential sources of mortality data that were considered are described in more detail in Appendix C. In addition, for a number of measures of interest for this evaluation, data are not collected across PEPFAR and non-PEPFAR countries.
Finally, as described in more depth in Chapter 4, complete and reliable data on annual PEPFAR expenditures by country were not readily available. Ideally the committee would have designed a model to determine if a bigger annual investment of PEPFAR funding over time, across all PEPFAR-funded partner countries, had led to a greater impact on health. This would cover a larger scope of countries than prior analyses, and the use of a continuous funding variable as the input to the model rather than the dichotomous comparison of focus versus non-focus countries would address some of the limitations of the existing analyses.
Ultimately, the committee determined that the limitations were too great to design and carry out analyses in the time available that would meaningfully add to the existing analyses in the published literature. Although these limitations prevented the committee from quantitatively modeling the impact of PEPFAR, the many data sources reviewed by the committee and presented in this chapter did make it feasible to conclude that PEPFAR’s support for care and treatment services has had a major positive effect in partner countries.
SUMMATION FOR PEPFAR’S SUPPORT FOR CARE AND TREATMENT SERVICES
Conclusion: PEPFAR has made a major contribution to increasing the number of people living with HIV who are in care and on ART through the expansion of the number and geographic distribution of care and treatment sites, the training of providers, the procurement and delivery of drugs, improvements in laboratory services, and support for the adoption and implementation of national policies and guidelines in partner countries. Support for care and treatment programs is a success that has contributed to saving lives and improving the quality of life for people living with HIV in PEPFAR partner countries.
Conclusion: The ability to assess the impact of PEPFAR-supported care and treatment programs across countries and partners is restricted by limitations in the available data. The available program-wide output measures provide a sense of the growth of PEPFAR-supported treatment programs over time but do not provide an understanding of the distribution of those services in populations of interest and do not provide a measure of effectiveness and outcomes. It was a missed opportunity not to invest more resources earlier in standardized, realistic, and useful monitoring of outcomes.
Recommendation 6-2: To contribute to sustainable care and treatment programs in partner countries, PEPFAR should build on its experience and support efforts to develop, implement, and scale up more effective and efficient facility- and community-based service delivery models for the continuum of adult and pediatric testing, care, and treatment. These efforts should aim to enhance equitable access, improve retention, increase clinical and laboratory monitoring, ensure quality, and implement cost efficiencies.
Further considerations for implementation of this recommendation:
• This recommendation should be implemented in coordination with recommendations and considerations discussed in Chapter 9 on health systems strengthening.
• PEPFAR should develop a system for active dissemination and sharing of best practices in service delivery both within and across countries. (See also recommendation for PEPFAR’s knowledge management in Chapter 11.)
Recommendation 6-3: To assess PEPFAR-supported HIV care and treatment programs and to evaluate new service delivery models, the Office of the U.S. Global AIDS Coordinator should support an enhanced, nested program monitoring effort in which additional longitudinal data on core outcomes for HIV-positive adults and children enrolled in care and treatment are collected and centrally reported from a coordinated representative sample across multiple countries and implementing partners.
Further considerations for implementation of this recommendation:
• This activity would serve as a targeted, nested evaluation within routine program monitoring systems to allow for long-term operational assessment of performance and outcomes for care and treatment across a representative sample of PEPFAR-supported programs. The aim would be to focus on key areas for evaluation and improvement of programs going forward, including as PEPFAR supports innovations in service delivery and as PEPFAR-supported programs transition to new models of implementation.
• Data collected and reported for this sample should be harmonized with existing data collection whenever possible, including data already collected by implementing partners but not centrally reported (e.g., see the discussion of Tier 3 data in the implementation considerations for Recommendation 11-1A). Collaborative opportunities may be feasible with existing or new large-scale national and multi-country samples.
• This data-collection effort should be designed by first identifying and prioritizing the key questions that require longitudinal data and then focusing on relevant key outcomes with measures that are standardized across the sample. Priorities should include core outcomes related to clinical care and treatment, including adherence and retention; outcomes related to the reduction of HIV transmission through biomedical and behavioral prevention interventions for people living with HIV; quality measures; and program measures, such as the costs of services, that can help inform strategies for efficiencies, sustainable management, and resource planning for the trajectory of need.
• There may also be opportunities for an established data-collection effort of this kind to serve as a synergistic platform for targeted implementation research studies in subset samples to assess innovations and advance those best practices that are most ready for translation and scale-up.
• In addition to implementing this approach prospectively, OGAC should explore working with and coordinating Track 1.0 partners to pool data for retrospective outcome analyses.
ONGOING CHALLENGES WITH ART COVERAGE
ART Coverage in PEPFAR Partner Countries
Although PEPFAR has had a major effect on increased access to ART, interviewees reported widely varying proportions of people eligible for treatment who were actually receiving treatment, and across countries there remains a large unmet need for care and treatment, including ART.
One issue that interviewees raised related to assessing treatment coverage is a lack of current, consistent data related to the total number of people in need of treatment (587-13-USG; 240-15-USG). In addition, the current understanding of who is eligible depends on where the partner country is in the transition to implementing the revised WHO HIV treatment guidelines, which expand eligibility and thus the number in need (934-2-USG; 934-10-PCGOV; 934-5-USG; 934-12-CCM; 542-3-USG; 542-9-PCGOV; 272-32/35-PCNGO; 116-7-USG; 116-18-PCNGO).
To get a reasonable sense of the status of coverage in PEPFAR partner countries and how this has changed over time, the committee used the best available consistent data to look at two time points since PEPFAR was initiated, 2006 (see Figure 6-15) and 2009 (see Figure 6-16). The need and the coverage varies widely by country; nonetheless, these figures provide an overall sense that coverage has increased in PEPFAR partner countries, as has the proportion of the national coverage supported by PEPFAR. However, the underlying need has also increased, and gaps in coverage remain.
Factors That Contribute to Coverage Challenges
The major factors affecting the ability of a partner country to achieve greater coverage of ART are financial resources (discussed in the next section on sustainability), capacity in the health system, and access to care and treatment services.
Health Systems Capacity
In many countries, HIV continues to overwhelm the health system (166-10-USNGO). Sustaining a large number of PLHIV on treatment requires the support of a particularly strong health system. Interrelated health systems factors affect the availability, accessibility, and quality of treatment, including health facilities, information systems, laboratory services, trained health care providers, and ARVs and other drugs to treat TB and other
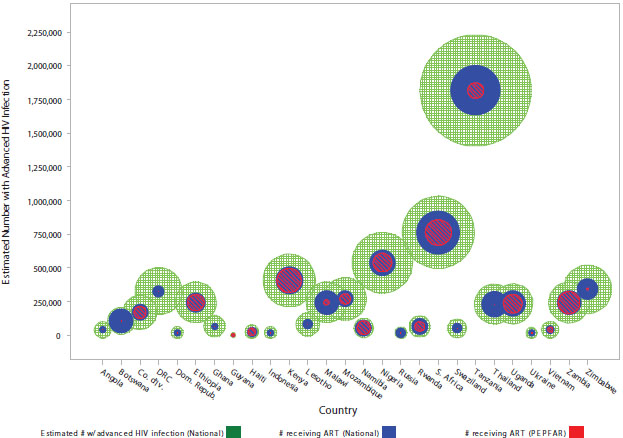
FIGURE 6-15 2006 estimated HIV prevalence and ART coverage.
NOTES: The area of the green circles, as well as the height of the center of these circles on the vertical axis, represents the estimated magnitude of advanced HIV infection within each country (UNGASS indicator 4, denominator). The area of the blue circle within a green circle represents the national ART coverage (UNGASS indicator 4, numerator). The area of the red circle within a blue circle corresponds to the amount of ART coverage contributed by PEPFAR programs (OGAC indicator 11.4). This figure represents data for the 31 countries identified as the focus of this evaluation (see Chapter 2) except Cambodia, China, India, and Sudan, which were excluded because national estimates were not available for 2006 and 2009.
SOURCES: Program monitoring indicators provided by OGAC; UNAIDS, 2012a.
opportunistic infections. Health systems factors that contribute to coverage challenges are discussed briefly here; a full assessment of PEPFAR’s health systems strengthening efforts can be found in Chapter 9.
Facilities in poor condition and a lack of infrastructure posed serious impediments to treatment access and care (240-15-USG; 461-13-USACA). Donor-funded renovations of facilities in some countries were undertaken to improve quality in care and treatment (240-24-USG). In addition to the poor physical condition of some health facilities, the compartmentalization of function in some countries caused by designating facilities as ART-initiating sites, ARV/drug dispensing sites, and follow-up care sites had implications for patient access, continuity of care, and retention (934-15-PCGOV). Although targeted patient needs could be addressed at individual sites, when comprehensive care was unavailable at a single site, it forced some patients to
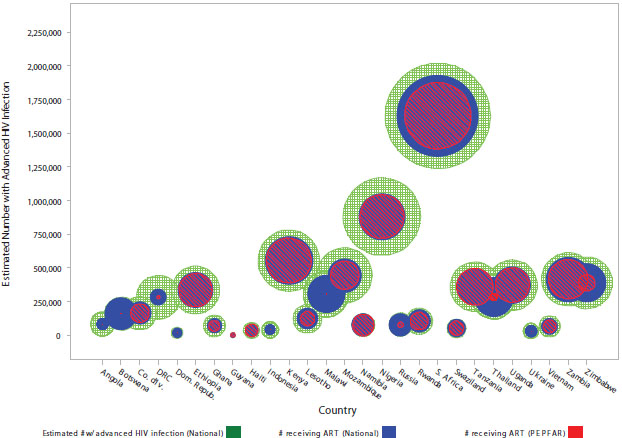
FIGURE 6-16 2009 estimated HIV prevalence and ART coverage.
NOTES: The area of the green circles, as well as the height of the center of these circles on the vertical axis, represents the estimated magnitude of advanced HIV infection within each country (UNGASS indicator 4, denominator). The area of the blue circle within a green circle represents the national ART coverage (UNGASS indicator 4, numerator). The area of the red circle within a blue circle corresponds to the amount of ART coverage contributed by PEPFAR programs (OGAC indicator 11.4). This figure represents data for the 31 countries identified as the focus of this evaluation (see Chapter 2) except Cambodia, China, India, and Sudan, which were excluded because national estimates were not available for 2006 and 2009.
SOURCES: Program monitoring indicators provided by OGAC; UNAIDS, 2012a.
travel, which raised access issues of distance and transportation. In addition, interviewees in several countries described challenges with establishing care and treatment in rural areas, where services were not available and either few health facilities existed or it was difficult to staff existing local health centers (240-5-PCGOV; 240-21-PCGOV; 240-25-PCGOV; 461-8-PCGOV; 587-5-PCGOV; 196-8-ML; 636-2-USG; 166-15-USACA; 272-13-USG; 272-20-PCNGO; 461-13-USACA; 934-8-USNGO). The time and expense of travelling to access services, a challenge noted in both urban and rural settings, poses a difficulty that is magnified for residents in rural and remote areas where the distances to services are largest. Indeed, transportation for individuals to sites of care continues to be one of the primary issues in accessing care in many countries (166-29-PCGOV; 240-19-USACA; 272-32/35-PCNGO; 461-7-PCNGO; 934-12-CCM; 934-15-PCGOV; 934-23-USNGO; 935-ES; 166-ES). Innovations such as decentralization of services, mobile service delivery units, and cell
phone and Internet communication to help with, for example, lab results and consultations increase the feasibility of delivering care in some remote areas (272-13-USG; 272-21-PCNGO; 934-10-PCGOV; 240-21-PCGOV; 934-8-USNGO).
As care and treatment services were expanded, the need arose for an adequate health care workforce to oversee ART. Many countries had shortages of physicians or other trained, knowledgeable health care providers. In addition to training efforts, task shifting from physicians to trained nurses and other health professionals was commonly implemented in countries as a workforce capacity-building strategy (396-21-USG), which facilitated the provision of routine patient care and clinical management (934-15-PCGOV). In many cases, task shifting addressed the clinician shortage problem and brought health care services to those in need (240-15-USG; 240-24-USG; 934-15-PCGOV), particularly those living in remote rural areas. However, there were varying levels of implementation and degrees of success in such shifting in responsibilities (272-22-USG), particularly since some people believed that HIV care and treatment was ‘too complex’ to be delivered by providers other than physicians (587-13-USG). A significant policy- and implementation-related challenge for task shifting in some countries was establishing “nurses to prescribe ART” (934-5-USG), particularly for pediatric populations, and training nurses in the diagnosis and treatment of tuberculosis, a major cause of death in PLHIV (331-12-USG).
Countries also experience drug shortages, including lack of ARVs and unavailable drugs for opportunistic infections for various reasons, including drug procurement and supply chain management issues (331-8-PCNGO; 240-25-PCGOV; 461-18-USG). Ineffective supply chain management systems sometimes impaired patient’s access to treatment to a significant degree. Interviewees reported periodic stock-outs of drugs (587-18-PCGOV; 166-18-PCNGO; 272-22-USG), a situation that some viewed as ‘a critical area to wrestle with’ (331-43-USG). Countries that had effectively organized functioning supply chain management systems rarely experienced stock-out occurrences (240-25-PCGOV; 272-32/35-PCNGO) that were linked to systems management. Different countries and health facilities had varying ways of coping with stock-outs, one of which was to pool resources from regional clinics. In these circumstances, patients sometimes received medication substitutions (166-18-USNGO) but were able to continue ART. In emergency circumstances, PEPFAR occasionally came to the aid of the country by serving in a gap-filling role and by providing buffer stocks to cover stock-outs (461-10-PCNGO; 934-5-USG; 272-22-USG). A particular gap-filling need arose in some countries when they experienced a transition from one donor to another.
Laboratory services are another component of the unmet need for ART (461-18-USG). An interviewee described the importance of laboratory services in HIV/AIDS treatment by referring to the lack of such services as ‘one of the major challenges that limits access to ART’ (461-10-PCNGO). Another interviewee
echoed that perspective, describing that ‘low case detection rates were due to low laboratory capacity’ (240-24-USG). Challenges related to laboratory services that ultimately affected ART access included the long turnaround time required for results from some laboratories and the difficult transport of laboratory samples, particularly in the more remote and rural areas where transportation is difficult and there are fewer laboratory facilities. In addition, few personnel were trained in such techniques as obtaining dried blood spot samples and performing early infant diagnosis (396-21-USG), and some personnel had limited or no access to equipment or reagents for such services as CD4 testing in the health facilities where they worked (240-24-USG). Occasional stock-outs of reagents or HIV rapid tests also posed access challenges in the provision of laboratory services (166-15-USACA).
Overall, interviewees perceived the need for a significant investment in health systems strengthening efforts (272-22-USG; 396-21-USG; 587-2-USG). One aspect of this was the need for integration of HIV-related services with other health services, as described by one interviewee: ‘HIV is being treated as a separate entity and not integrated with other health services. ART clinics will only provide care to HIV patients. This is a missed opportunity’ (240-24-USG).
Access to Care and Treatment
Each of the preceding sections of this chapter describes challenges with access to care and treatment services. In summary, across the continuum of services interviewees identified the key elements that affect access such as physical distance to facilities (resulting in transportation barriers), stigma, and the costs to clients of accessing care. Some specific barriers to accessing care were discussed in this chapter for key vulnerable populations, including people who inject drugs, sex workers, and men who have sex with men; these populations are discussed in more depth in Chapters 5 and 8. As noted throughout this chapter, interviewees across countries consistently observed that PEPFAR has contributed to improving both the availability of and access to care and treatment, both in general due to its support for scale-up of services and also through efforts to address barriers to access.
Conclusion: Despite progress in the availability of and access to HIV services, there remains a large unmet need for care and treatment in PEPFAR partner countries. Intrinsic limitations of the health system infrastructure continue to pose barriers to the delivery of care treatment services, including clinical care, clinical and laboratory monitoring, and antiretroviral therapy.
ART Coverage Challenges for Children
Providing treatment to the many children affected by HIV/AIDS has been a persistent challenge. A number of factors have contributed to a lack of coverage for children, including a lack of accessible testing for children of all ages, especially the difficulties in obtaining early infant diagnosis and the failure to adequately support alternate diagnostic measures to indicate when to initiate therapy; a lack of providers familiar with treating children; a lack of pediatric ART services at primary care, postnatal, and other maternal–child health care facilities; and shortages of ART regimens for children.
As described earlier in the chapter, efforts to identify HIV-positive children are suboptimal and the diagnosis of children less than 1 year old is particularly challenging. Without treatment, HIV infection in children follows an aggressive course, generally progressing faster to AIDS and to death than in adults. Without ART, about one-third of HIV-infected infants will die before they reach the age of 1 year, and 50 percent will die by age 2 (Newell et al., 2004; Violari et al., 2008). Despite PEPFAR-supported progress in supporting early infant diagnosis, when testing is conducted to identify children, the results are often too delayed (240-24-USG; 240-21-PCGOV; 396-21-USG; 331-28-PCGOV; 636-17-PCGOV; 935-7-USG). This contributes to a chain of events leading to the delayed initiation of treatment and poor outcomes, including a need for complex treatment for children in whom the disease has progressed and, quite often, death.
Improved access to pediatric treatment depends on the ability to identify women and children routinely through maternal–child care service entry points such as services in maternal and child health, including PMTCT, and to refer them to care and treatment facilities or provide integrated care. PEPFAR has put in place several efforts—described previously in this chapter—to increase pediatric enrollment by improving linkages to care and treatment after identification of children in need, but this continues to often be lacking.
According to interviewees, another contributing factor to the lack of coverage for children is a lack of a trained workforce for pediatric care and treatment (272-20-PCNGO; 272-22-USG; 935-13-PCGOV; 240-24-USG; 166-18-PCNGO; 461-13-USACA), including a shortage of trained pediatricians. Training in pediatric treatment and care is a critical factor because of the sense of insecurity that many providers have about their ability to provide these services. For this reason, task shifting for pediatric treatment has resulted in mixed results, as has the integration of pediatric services into general health facilities (331-12-USG; 272-22-USG; 461-13-USACA).
Stock-outs of drugs for children are also a challenge (934-29-USNGO), in one example forcing the purchase of medicine using local city funds when no
other external resources were available (542-16-PCGOV). Facilities in poor conditions (934-29-USNGO; 461-13-USACA), a scarcity of laboratories with the technology required for testing (166-13-PCGOV), and concern for the quality of laboratory services (240-2-USG) have restricted the number of children who can be initiated on ART.
Stigma is another factor that plays a role in the identification of children with HIV. Parents would take their children to health facilities outside their communities to avoid disclosing their status (240-25-PCGOV). Moreover, there was a fear of the negative impact on the development of the child if the child was identified as HIV positive in school or through participation in support groups, as this would mean the child could not participate in some school activities (116-15-USNGO).
Finally, interviewees described the lack of data to assess progress as a great challenge (587-5-PCGOV; 166-18-USNGO). In one country, PEPFAR is planning an interagency pediatric treatment assessment and working to increase indicators to assess more outcomes, including loss to follow-up, and to assess more by different age groups (272-22-USG).
The challenges facing pediatric treatment are compounded by inadequate funding for pediatric treatment. Although PEPFAR purchases pediatric ARVs in some countries, in several countries UNITAID11 and the Clinton Foundation are the sole purchasers of ART formulations and second-line regimens for children, commodities for early infant diagnosis, and cotrimoxazole and other drugs for opportunistic infections (OGAC, 2009b). Where UNITAID/Clinton Foundation support for some of these commodities decreases, countries will need to make up for the gap.
Another challenge is meeting the specific needs of HIV-positive adolescents in care and treatment programs and transitioning them to adult care and treatment programs. There are some PEPFAR-supported programs in a few countries that have developed strong adolescent components, including, for example, adolescent-specific care and support programs, bimonthly provider forums to discuss challenges in the adolescent population, and facilitation of referrals between clinics and community services (Sharer, 2012). However, comprehensive services that focus specifically on the unique needs of adolescents living with HIV are a remaining gap that was identified by interviewees across countries (396-43-ML; 396-42-PCGOV; 272-22-USG; 935-13-PCGOV; 935-19-PCGOV; 636-6-USG). Challenges in services for adolescents are discussed further in Chapter 7.
__________________
11 UNITAID is an international facility dedicated to increasing access to drugs and diagnostics for HIV/AIDS, malaria, and tuberculosis, primarily for people in low-income countries. UNITAID leverages its funds, received through airline ticket taxes or regular multiyear budget contributions from governments and a foundation, to reduce the price of quality diagnostics and medicines as well as to accelerate the availability of these products in low- and middle-income countries (UNITAID, 2013).
Conclusion: Treatment of infants and children remains a persistent challenge across the continuum of care. The main barriers, especially for infants, come at the stages of testing and diagnosis, linkages to care and treatment, and timely initiation of therapy. Limitations in health systems for the support of pediatric HIV services are also a major factor. PEPFAR has contributed to increasing pediatric treatment, but the coverage of pediatric HIV remains proportionally much lower than the coverage for adults, despite the goal in the reauthorization legislation to provide care and treatment services in partner countries to children in proportion to their percentage within the HIV-infected population.
Expansion of Eligibility Under Evolving WHO Guidelines
The issue of gaps in coverage and unmet need is complicated by the changes in the WHO HIV treatment guidelines recommending that ART treatment initiation begin earlier, at a CD4 count of less than 350 cells/mm3. Implementing these guidelines will expand the eligible population for whom treatment is indicated. UNAIDS recently estimated that, in 2011, 12.8 million adults in low- and middle-income countries were eligible for ART under the 2010 guidelines (UNAIDS, 2013).
To illustrate the effect of the change in guidelines on the population in need, Figure 6-17 shows an estimate from 2010 of the difference over time in the number of eligible adults in different regions of the world based on the different eligibility criteria. As described earlier, interviewees in partner
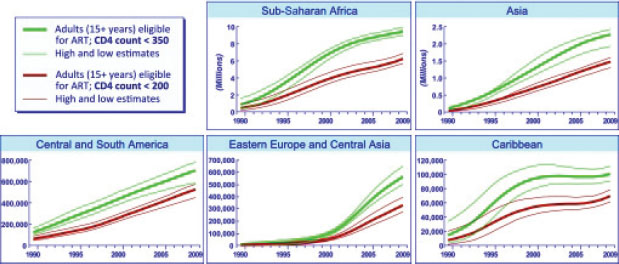
FIGURE 6-17 Number of adults (>15 years) eligible for ART in low- and middle-income countries, by region, according to WHO 2006 (CD4<200) and 2010 (CD4<350) guidelines.
SOURCE: Stanecki et al., 2010.
countries noted the challenges that they anticipate related to the resulting increase in the demand for treatment services (934-2-USG; 934-10-PCGOV; 934-5-USG; 934-12-CCM; 542-3-USG; 542-9-PCGOV; 272-32/35-PCNGO; 116-7-USG; 116-18-PCNGO).
The expansion of coverage and its associated challenges will be compounded further by implementation of PMTCT Option B+ and the recently released WHO guidelines recommending that antiretroviral therapy be offered to the HIV-positive partner in serodiscordant couples, regardless of CD4 count (WHO, 2012a,b).
SUSTAINABILITY OF CARE AND TREATMENT
While the rapid scale-up of ART has been a success of the global AIDS response, and while PEPFAR has made a major contribution to this success, there is still a long way to go before the goal of universal coverage is achieved. As described in the preceding section, there remains a large unmet need overall in low- and middle-income countries, and access and coverage among several populations—most notably children, marginalized populations, and pregnant women—continues to lag behind that of the general population or behind the global targets. Important challenges for the future of the response to HIV, given the realities of limited resources, is how to maintain those currently enrolled in care and treatment, address the care and treatment needs for the many currently eligible patients who may remain untreated, and plan for those who will become eligible in the future. There is a critical need for PEPFAR, its partner countries, and other global stakeholders to focus on how to support countries in discussing what resources are needed to respond to the HIV/AIDS epidemic, how to prioritize the large unmet need for treatment of adults, adolescents, and children, and how to identify resources for the gap.
Currently in many partner countries the vast majority of treatment is funded by PEPFAR, the Global Fund, or, most commonly, some combination of the two. This can represent a very fragile state for care and treatment programs, especially as there is ongoing uncertainty related to future HIV/AIDS funding levels due to the global economic recession, which has complicated planning efforts for continued ART scale-up (UNAIDS, 2011; WHO et al., 2009). This fragility was seen on several country visits when a Global Fund proposal had been rejected or a round had been cancelled. As one interviewee put it, ‘now that the Global Fund is out, there’s no other back-up plan’ (331-12-USG).
While financial resources are a clear challenge to sustainability, a number of other challenges also hamper the effort to maintain the current levels of care and treatment and to achieve universal access as called for in the WHO treatment guidelines. These challenges include distribution and supply chain challenges such as stock-outs, infrastructure challenges such as
poor laboratory infrastructure, inadequate human resources for health in many low- and middle-income countries, and challenges relating to ensuring patient adherence to treatment. In addition, challenges with retention and adherence, the emergence of drug resistance, and the co-infection of HIV patients with tuberculosis continue to undermine care and treatment efforts.
Interviewees conveyed their awareness of a desire by PEPFAR to foster sustainability and, in that light, to reduce or eliminate support for the HIV response in partner countries. Their central concern was the continuing availability of funding for ARVs. As one interviewee stated,
“Obviously, absolutely, we should be looking at long-term sustainability. But at the same time, don’t let that be the catchall. And right now, PEPFAR, we have the money, and one of the most important things right now is saving lives. We’ve lost too many lives here in [this country]. It was an absolute horror and a tragedy. And we’re stopping that now. And we should continue to stop it. But treatment is one of the most important things that we can do. Obviously, as we all know, it’s not the only thing. We’ve also got to focus on prevention. But this is an inexpensive way to stop the deaths.” (934-5-USG)
Interviewees described initiatives they had undertaken that would eventually become self-sustaining such as, in the case of one country, implementing fees to subsidize a laboratory quality-assurance program (934-5-USG). Overall, however, interviewees across countries questioned the readiness of their countries for anticipated sustainability-related funding reductions or cessation (240-15-USG; 396-21-USG; 934-5-USG) and made recommendations or raised concerns about the pace or timeframe for such reductions (272-5-PCGOV; 272-22-USG). As one interviewee explained,
‘It’s not that sensible for PEPFAR to leave tomorrow [. . .] it would be difficult to keep scaling up and adding money and replace PEPFAR funding at the same time. If PEPFAR pulled out, the funding would probably just not be replaced. If done over time, it’s far more likely it would be a smooth process to sustainability.’ (272-5-PCGOV)
Barriers to partner country readiness for sustainability included such issues as funding treatment scale-up efforts that are currently under way (272-5-PCGOV), a lack of partner government capacity to ‘take over the response’ (240-24-USG), meeting salary expectations of those previously employed by PEPFAR (240-15-USG), and absorbing demands for services (272-32/35-PCNGO). One interviewee observed that ‘a weak [ART] program is not sustain-
able,’ implying the need for program strengthening as a pre-condition for sustainability (396-21-USG). Another interviewee focused on facilitating drug treatment adherence, noting that making treatment ‘easier and cheaper is sustainability’ (272-22-USG).
In summary, the all-encompassing challenge for care and treatment, as for other HIV services, is that despite the remarkable scale-up in PEPFAR partner countries, there remains substantial unmet need. The large numbers of currently enrolled patients who need to be maintained, those currently eligible but not yet enrolled, and the potential for expansion of eligibility if changing WHO guidelines are adopted and implemented are fundamental challenges for achieving adequate coverage and for the sustainability of care and treatment across PEPFAR partner countries. Intrinsic limitations in the health system and other systems involved in the response continue to be barriers to the delivery of services, as do the realities of resource constraints, especially with the possible flattening or decreasing of external resources.
Therefore, for care and treatment, as with other HIV programs, the most critical challenge for the future is for PEPFAR to work with partner countries and global partners to sustain the gains made, to continue to make progress, and to ensure the ongoing quality of services provided and programs implemented. Given that this challenge must be confronted while facing limited resources, contributing stakeholders will need to allocate resources with a strategic and ethical balance among coverage priorities. Critically important issues related to this overarching challenge for the future, including strengthening systems, building capacity, and considerations and efforts related to achieving a sustainable, country-led response to HIV in PEPFAR partner countries, are discussed in depth in Chapters 9 and 10.
AIDSTAR-One (AIDS Support and Technical Assistance Resources Project). 2011a. Summary table of HIV treatment regimens: Pediatric and adult national treatment guidelines: January 2011. Arlington, VA: AIDSTAR-One Project, Sector I, Task Order 1.
AIDSTAR-One. 2011b. Summary table of HIV treatment regimens: Pediatric and adult treatment guidelines for PEPFAR focus and non-focus countries: June 2011. Arlington, VA: AIDSTAR-One Project, Sector I, Task Order 1.
AIDSTAR-One. 2012. Summary table of HIV treatment regimens: Pediatric and adult treatment guidelines for PEPFAR focus and non-focus countries: October 2012. Arlington, VA: AIDSTAR-One Project, Sector I, Task Order 1.
Bartlett, J., B. M. Branson, K. Fenton, B. C. Hauschild, V. Miller, and K. H. Mayer. 2008. Opt-out testing for human immunodeficiency virus in the United States: Progress and challenges. Journal of the American Medical Association 300(8):945-951.
Bendavid, E., and J. Bhattacharya. 2009. The President’s Emergency Plan for AIDS Relief in Africa: An evaluation of outcomes. Annals of Internal Medicine 150(10):688-695.
Bendavid, E., C. B. Holmes, J. Bhattacharya, and G. Miller. 2012. HIV development assistance and adult mortality in Africa. Journal of the American Medical Association 307(19):2060-2067.
Botswana Ministry of Health. 2008. Botswana national HIV/AIDS treatment guidelines: 2008 version. Gaborone: Botswana Ministry of Health, Department of HIV/AIDS Prevention and Care.
Brahmbhatt, H., G. Kigozi, F. Wabwire-Mangen, D. Serwadda, T. Lutalo, F. Nalugoda, N. Sewankambo, M. Kiduggavu, M. Wawer, and R. Gray. 2006. Mortality in HIV-infected and uninfected children of HIV-infected and uninfected mothers in rural Uganda. Journal of Acquired Immune Deficiency Syndromes 41(4):504-508.
Bussmann, H., C. W. Wester, N. Ndwapi, N. Grundmann, T. Gaolathe, J. Puvimanasinghe, A. Avalos, M. Mine, K. Seipone, M. Essex, V. Degruttola, and R. G. Marlink. 2008. Five-year outcomes of initial patients treated in Botswana’s national antiretroviral treatment program. AIDS 22(17):2303-2311.
Cambodia Ministry of Health. 2003. National guidelines for the use of antiretroviral therapy in adults and adolescents. Phnom Penh: Cambodia Ministry of Health, National Center for HIV/AIDS, Dermatology and STD.
Cambodia Ministry of Health. 2007. National guidelines for the use of pediatric antiretroviral therapy in Cambodia. Phnom Penh: Cambodia Ministry of Health, National Center for HIV/AIDS, Dermatology and STD.
Chang, L. W., J. Kagaayi, G. Nakigozi, V. Ssempijja, A. H. Packer, D. Serwadda, T. C. Quinn, R. H. Gray, R. C. Bollinger, and S. J. Reynolds. 2010. Effect of peer health workers on AIDS care in Rakai, Uganda: A cluster-randomized trial. PLOS One 5(6):e10923.
Chen, S. C., J. K. Yu, A. D. Harries, C. N. Bong, R. Kolola-Dzimadzi, T. S. Tok, C. C. King, and J. D. Wang. 2008. Increased mortality of male adults with AIDS related to poor compliance to antiretroviral therapy in Malawi. Tropical Medicine & International Health 13(4):513-519.
China CDC (Chinese Center for Disease Control and Prevention). 2005. China free ART manual. Beijing: China CDC.
Das, M. 2011. Intensifying HIV prevention in the communities where HIV is most heavily concentrated. Presented at the 2011 National HIV Prevention Conference, Atlanta, Georgia.
Duber, H. C., T. J. Coates, G. Szekeras, A. H. Kaji, and R. J. Lewis. 2010. Is there an association between PEPFAR funding and improvement in national health indicators in Africa? A retrospective study. Journal of the International AIDS Society 13:21.
El-Khatib, Z., D. Katzenstein, G. Marrone, F. Laher, L. Mohapi, M. Petzold, L. Morris, and A. M. Ekstrom. 2011. Adherence to drug-refill is a useful early warning indicator of virologic and immunologic failure among HIV patients on first-line ART in South Africa. PLOS ONE 6(3):e17518.
Eldred, L., and F. Malitz. 2007. Introduction. AIDS Patient Care & STDs 21:S1-S2.
Ethiopia Ministry of Health. 2003. Guidelines for use of antiretroviral drugs in Ethiopia. Addis Ababa: Ethiopia Federal HIV/AIDS Prevention and Control Office, Ministry of Health.
Ethiopia Ministry of Health. 2007. Guidelines for paediatric HIV/AIDS care and treatment in Ethiopia. Addis Ababa: Ethiopia Federal HIV/AIDS Prevention and Control Office, Ministry of Health.
Fatti, G., G. Meintjes, J. Shea, B. Eley, and A. Grimwood. 2012. Improved survival and antiretroviral treatment outcomes in adults receiving community-based adherence support: 5-year results from a multicentre cohort study in South Africa. Journal of Acquired Immune Deficiency Syndromes 61(4):50.
Fox, M. P., and S. Rosen. 2010. Patient retention in antiretroviral therapy programs up to three years on treatment in sub-Saharan Africa, 2007-2009: Systematic review. Tropical Medicine & International Health 15(Suppl 1):1-15.
G, U. L., and A. Adewumi. 2004. Nigeria country presentation. Presented at Pharmacovigilance: First Training workshop to introduce monitoring of safety and efficacy of antiretrovirals in Africa, Pretoria, South Africa.
Gardner, E. M., M. P. McLees, J. F. Steiner, C. del Rio, and W. J. Burman. 2011. The spectrum of engagement in HIV care and its relevance to test-and-treat strategies for prevention of HIV infection. Clinical Infectious Diseases 52(6):793-800.
Geng, E. H., P. W. Hunt, L. O. Diero, S. Kimaiyo, G. R. Somi, P. Okong, D. R. Bangsberg, M. B. Bwana, C. R. Cohen, J. A. Otieno, D. Wabwire, B. Elul, D. Nash, P. J. Easterbrook, P. Braitstein, B. S. Musick, J. N. Martin, C. T. Yiannoutsos, and K. Wools-Kaloustian. 2011. Trends in the clinical characteristics of HIV-infected patients initiating antiretroviral therapy in Kenya, Uganda and Tanzania between 2002 and 2009. Journal of the International AIDS Society 14:46.
George W. Bush Institute, U.S. President’s Emergency Plan for AIDS Relief (PEPFAR), Susan G. Komen for the Cure, and Joint United Nations Programme on HIV/AIDS (UNAIDS). 2012. Pink Ribbon, Red Ribbon. http://www.pinkandredribbon.com (accessed May 31, 2013).
Ghana Ministry of Health. 2002. Guidelines for antiretroviral therapy in Ghana. Accra: Ghana Ministry of Health/Ghana Health Service.
Gilliam, B. L., D. Patel, R. Talwani, and Z. Temesgen. 2012. HIV in Africa: Challenges and directions for the next decade. Current Infectious Disease Reports 14(1):91-101.
Global Fund (The Global Fund to Fight AIDS, Tuberculosis, and Malaria). 2009. Global Fund ARV fact sheet: 1st December, 2009. Geneva: Global Fund.
Global Fund. 2013. Government donors. http://www.theglobalfund.org/en/donors/public/ (accessed May 31, 2013).
Government of India. 2007. Antiretroviral therapy guidelines for HIV-infected adults and adolescents including post-exposure prophylaxis. New Delhi: Government of India Ministry of Health & Family Welfare.
Grundmann, N., P. Iliff, J. Stringer, and C. Wilfert. 2011. Presumptive diagnosis of severe HIV infection to determine the need for antiretroviral therapy in children less than 18 months of age. Bulletin of the World Health Organization 89(7):513-520.
Gupta, R. K., M. R. Jordan, B. J. Sultan, A. Hill, D. H. J. Davis, J. Gregson, A. W. Sawyer, R. L. Hamers, N. Ndembi, D. Pillay, and S. Bertagnolio. 2012. Global trends in antiretroviral resistance in treatment-naive individuals with HIV after rollout of antiretroviral treatment in resource-limited settings: A global collaborative study and meta-regression analysis. Lancet 380(9849):1250-1258.
Guyana Ministry of Health. 2009. National guidelines for management of HIV-infected and HIV-exposed adults and children. Georgetown: Guyana Ministry of Health.
Haiti Ministry of Public Health and Population. 2008. Manuel de normes de prise en charge clinique et thérapeutique des adultes et adolescents vivant avec le VIH. Port-au-Prince: Haiti Ministry of Public Health and Population.
Hamers, R. L., C. L. Wallis, C. Kityo, M. Siwale, K. Mandaliya, F. Conradie, M. E. Botes, M. Wellington, A. Osibogun, K. C. Sigaloff, I. Nankya, R. Schuurman, F. W. Wit, W. S. Stevens, M. van Vugt, T. F. de Wit, and PharmAccess African Studies to Evaluate Resistance. 2011. HIV-1 drug resistance in antiretroviral-naive individuals in sub-Saharan Africa after rollout of antiretroviral therapy: A multicentre observational study. Lancet Infectious Diseases 11(10):750-759.
Hamers, R. L., C. Kityo, J. M. A. Lange, T. F. de Wit, P. Mugyenyi. 2012. Global threat from drug resistant HIV in sub-Saharan Africa. British Medical Journal 344:e4159.
Hawkins, C., G. Chalamilla, J. Okuma, D. Spiegelman, E. Hertzmark, E. Aris, T. Ewald, F. Mugusi, D. Mtasiwa, and W. Fawzi. 2011. Sex differences in antiretroviral treatment outcomes among HIV-infected adults in an urban Tanzanian setting. AIDS 25(9):1189-1197.
Herbst, A. J., G. S. Cooke, T. Barnighausen, A. KanyKany, F. Tanser, and M. L. Newell. 2009. Adult mortality and antiretroviral treatment roll-out in rural KwaZulu-Natal, South Africa. Bulletin of the World Health Organization 87(10):754-762.
Hong, S. Y., A. Jonas, E. Dumeni, A. Badi, D. Pereko, A. Blom, V. S. Muthiani, A. N. Shiningavamwe, J. Mukamba, G. Andemichael, R. Barbara, D. E. Bennett, and M. R. Jordan. 2010. Population-based monitoring of HIV drug resistance in Namibia with early warning indicators. Journal of Acquired Immune Deficiency Syndromes 55(4):27-31.
Igumbor, J. O., E. Scheepers, R. Ebrahim, A. Jason, and A. Grimwood. 2011. An evaluation of the impact of a community-based adherence support programme on ART outcomes in selected government HIV treatment sites in South Africa. AIDS Care 23(2):231-236.
Indonesia Ministry of Health. 2007. National guidelines for antiretroviral therapy: A guide to clinical management of HIV infection in adults and youth (Panduan tatalaksana klinis Infeksi HIV pada orang dewasa dan remaja). Jakarta: Directorate General of Disease Control and Environmental Health, Indonesia Ministry of Health.
Indonesia Ministry of Health. 2008. Guidelines for treatment of HIV infection and antiretroviral therapy in children in Indonesia (Pedoman tatalaksana infeksi HIV dan terapi antiretroviral pada anak di Indonesia). Jakarta: Directorate General of Disease Control and Environmental Health, Indonesia Ministry of Health.
Indonesia Ministry of Health. 2011. National guidelines for the clinical management of HIV infection and antiretroviral therapy in adults (Pedoman nasional tatalaksana klinis infeksi HIV dan terapi antiretroviral pada orang ewasa). Jakarta: Directorate General of Disease Control and Environmental Health, Indonesia Ministry of Health.
IOM (Institute of Medicine). 2007. PEPFAR implementation: Progress and promise. Washington, DC: The National Academies Press
IOM. 2012. Monitoring HIV care in the United States: A strategy for generating national estimates of HIV care and coverage. Washington, DC: The National Academies Press.
IOM and NRC (National Research Council). 2010. Strategic Approach to the Evaluation of Programs Implemented under the Tom Lantos and Henry J. Hyde U.S. Global Leadership Against HIV/AIDS, Tuberculosis, and Malaria Reauthorization Act of 2008. Washington, DC: The National Academies Press.
Jahn, A., S. Floyd, A. C. Crampin, F. Mwaungulu, H. Mvula, F. Munthali, N. McGrath, J. Mwafilaso, V. Mwinuka, B. Mangongo, P. E. Fine, B. Zaba, and J. R. Glynn. 2008. Population-level effect of HIV on adult mortality and early evidence of reversal after introduction of antiretroviral therapy in Malawi. Lancet 371(9624):1603-1611.
Kapstein, E. B., and J. Busby. 2009. Making markets for merit goods: The political economy of antiretrovirals. Washington, DC: Center for Global Development (CGD).
Kaur, G., and A. Singh. 2010. The “see and treat” approach to cervical cancer. http://www.thelancetstudent.com/legacy/2010/02/16/the-see-and-treat-approach-to-cervical-cancer (accessed May 31, 2013).
Kayigamba, F. R., M. I. Bakker, H. Fikse, V. Mugisha, A. Asiimwe, and M. F. Schim van der Loeff. 2012. Patient enrolment into HIV care and treatment within 90 days of HIV diagnosis in eight Rwandan health facilities: A review of facility-based registers. PLOS ONE 7(5):e36792.
Kenya Ministry of Health. 2001. Guidelines to antiretroviral drug therapy in Kenya. Nairobi: National Aids and STD Control Programme, Kenya Ministry of Health.
Kimmel, A. D., M. C. Weinstein, X. Anglaret, S. J. Goldie, E. Losina, Y. Yazdanpanah, E. Messou, K. L. Cotich, R. P. Walensky, and K. A. Freedberg. 2010. Laboratory monitoring to guide switching antiretroviral therapy in resource-limited settings: clinical benefits and cost-effectiveness. Journal of Acquired Immune Deficiency Syndromes 54(3):258-268.
Koole, O., S. Tsui, F. Wabwire-Mangen, G. Kwesigabo, J. Menten, M. Mulenga, A. Auld, S. Agolory, Y. D. Mukadi, R. Colebunders, D. R. Bangsberg, E. Van Praag, K. Torpey, S. Williams, J. Kaplan, A. Zee, and J. Denison. 2012. Retention and risk factors for attrition among adults in antiretroviral treatment programs in Tanzania, Uganda and Zambia. Presented at the XIX Inernational AIDS Conference, Washington, DC.
Malawi Ministry of Health. 2006. Treatment of AIDS: Guidelines for the use of antiretroviral therapy in Malawi. Second Edition: April 2006. Lilongwe: National AIDS Commission, Malawi Ministry of Health.
Marum, E., M. Taegtmeyer, B. Parekh, N. Mugo, S. Lembariti, M. Phiri, J. Moore, and A. Cheng. 2012. “What Took You So Long?” The impact of PEPFAR on the expansion of HIV testing and counseling services in Africa. Journal of Acquired Immune Deficiency Syndromes 60(Suppl 3):S63-S69.
Mat Shah, R., A. Bulgiba, C. K. C. Lee, J. Haniff, and M. Mohamad Ali. 2012. Highly active antiretroviral therapy reduces mortality and morbidity in patients with AIDS in Sungai Buloh Hospital. Journal of Experimental & Clinical Medicine 4(4):239-244.
McCullough, R., and L. Miller. 2009. Surveying the global HIV/AIDS landscape. http://ftguonline.org/ftgu-232/index.php/ftgu/article/view/2050/4096 (accessed June 10, 2011).
McMahon, J., J. Elliott, S. Hong, and M. Jordan. 2012. Effects of patient tracing on estimates of lost to follow-up, mortality and retentation in antiretroviral therapy programs in low-middle income countries: A systematic review. Abstract no. MOAC0302. Presented at the XIX International AIDS Conference, Washington, DC.
Medley, A., C. Garcia-Moreno, S. McGill, and S. Maman. 2004. Rates, barriers and outcomes of HIV serostatus disclosure among women in developing countries: implications for prevention of mother-to-child transmission programmes. Bulletin of the World Health Organization 82(4):299-307.
Menzies, N. A., A. A. Berruti, R. Berzon, S. Filler, R. Ferris, T. V. Ellerbrock, and J. M. Blandford. 2011. The cost of providing comprehensive HIV treatment in PEPFAR-supported programs. AIDS 25(14):1753-1760.
Mermin, J., W. Were, J. P. Ekwaru, D. Moore, R. Downing, P. Behumbiize, J. R. Lule, A. Coutinho, J. Tappero, and R. Bunnell. 2008. Mortality in HIV-infected Ugandan adults receiving antiretroviral treatment and survival of their HIV-uninfected children: A prospective cohort study. Lancet 371(9614):752-759.
Namibia Ministry of Health and Social Services. 2010. National guidelines for antiretroviral therapy. Third edition. Windhoek: Directorate of Special Programmes, Namibia Ministry of Health and Social Services.
Newell, M. L., H. Coovadia, M. Cortina-Borja, N. Rollins, P. Gaillard, and F. Dabis. 2004. Mortality of infected and uninfected infants born to HIV-infected mothers in Africa: A pooled analysis. Lancet 364(9441):1236-1243.
Nigeria Ministry of Health. 2007. Guidelines for HIV and AIDS care and treatment in adolescents and adults. Abuja: Nigeria Federal Ministry of Health.
Obama, B. 2011. Remarks by the President on World AIDS Day, December 1, Washington, DC.
Obermeyer, C. M., and M. Osborn. 2007. The utilization of testing and counseling for HIV: A review of the social and behavioral evidence. American Journal of Public Health 97(10):1762–1774.
OGAC (Office of the U.S. Global AIDS Coordinator). 2004. The President’s Emergency Plan for AIDS Relief: U.S. five-year global HIV/AIDS strategy. Washington, DC: OGAC.
OGAC. 2005. Emergency Plan for AIDS Relief Fiscal Year 2005 operational plan: June 2005 update. Washington, DC: OGAC.
OGAC. 2006a. Guidance for United States government in-country staff and implementing partners for a preventive care package for adults. Washington, DC: OGAC.
OGAC. 2006b. Guidance for United States government in-country staff and implementing partners for a preventive care package for children aged 0-14 years old born to HIV-infected mothers. Washington, DC: OGAC.
OGAC. 2006c. HIV/AIDS palliative care guidance #1 for the United States government in-country staff and implementing partners. Washington, DC: OGAC.
OGAC. 2006d. Orphans and other vulnerable children programming guidance for the United States government in-country staff and implementing partners. Washington, DC: OGAC.
OGAC. 2006e. The President’s Emergency Plan for AIDS Relief FY 2007 supplemental COP guidance resource guide. Washington, DC: OGAC.
OGAC. 2006f. The President’s Emergency Plan for AIDS Relief: FY 2007 country operational plan guidance. Washington, DC: OGAC.
OGAC. 2006g. The U.S. President’s Emergency Plan for AIDS Relief Fiscal Year 2006: Operational plan. 2006 August update. Washington, DC: OGAC.
OGAC. 2007a. The President’s Emergency Plan for AIDS Relief: FY 2008 country operational plan Guidance. Washington, DC: OGAC.
OGAC. 2007b. The President’s Emergency Plan for AIDS Relief: Indicators, reporting requirements, and guidelines. Indicators reference guide: FY 2007 Reporting/FY 2008 Planning. Washington, DC: OGAC.
OGAC. 2007c. The U.S. President’s Emergency Plan for AIDS Relief Fiscal Year 2007: Operational plan. 2007 June update. Washington, DC: OGAC.
OGAC. 2008a. The President’s Emergency Plan for AIDS Relief: FY 2009 country operational plan guidance. Washington, DC: OGAC.
OGAC. 2008b. The U.S. President’s Emergency Plan for AIDS Relief (PEPFAR) Fiscal Year 2008: PEPFAR operational plan. June 2008. Washington, DC: OGAC.
OGAC. 2009a. Celebrating life: Fifth annual report to Congress on PEPFAR. Washington, DC: OGAC.
OGAC. 2009b. PEPFAR: State of the program area. Washington, DC: OGAC.
OGAC. 2009c. The President’s Emergency Plan for AIDS Relief: FY 2010 country operational plan guidance: Programmatic considerations. Washington, DC: OGAC.
OGAC. 2009d. The President’s Emergency Plan for AIDS Relief: Next generation indicators reference guide. Version 1.1. Washington, DC: OGAC.
OGAC. 2009e. The U.S. President’s Emergency Plan for AIDS Relief: Five-year strategy. Washington, DC: OGAC.
OGAC. 2009f. The U.S. President’s Emergency Plan for AIDS Relief: Five-year strategy. Annex: PEPFAR and prevention, care and treatment. Washington, DC: OGAC.
OGAC. 2009g. The U.S. President’s Emergency Plan for AIDS Relief Five-year strategy. Annex: PEPFAR’s contribution to the Global Health Initiative. Washington, DC: OGAC.
OGAC. 2010a. The President’s Emergency Plan for AIDS Relief: FY 2011 country operational plan guidance. Washington, DC: OGAC.
OGAC. 2010b. The President’s Emergency Plan for AIDS Relief: FY 2011 country operational plan guidance appendices. Washington, DC: OGAC.
OGAC. 2010c. The U.S. President’s Emergency Plan for AIDS Relief (PEPFAR) Fiscal Year 2009: PEPFAR operational plan. November 2010. Washington, DC: OGAC.
OGAC. 2011a. The President’s Emergency Plan for AIDS Relief: FY 2012 country operational plan guidance and appendices. Washington, DC: OGAC.
OGAC. 2011b. The President’s Emergency Plan for AIDS Relief: FY 2012 country operational plan guidance technical considerations. Washington, DC: OGAC.
OGAC. 2011c. The President’s Emergency Plan for AIDS Relief: Guidance for the prevention of sexually transmitted HIV infections. Washington, DC: OGAC.
OGAC. 2011d. The U.S. President’s Emergency Plan for AIDS Relief (PEPFAR) Fiscal Year 2010: PEPFAR operational plan. April 2011. Washington, DC: OGAC.
OGAC. 2011e. The U.S. President’s Emergency Plan for AIDS Relief (PEPFAR) Fiscal Year 2011: PEPFAR operational plan. December 2011. Washington, DC: OGAC.
OGAC. 2012. The President’s Emergency Plan for AIDS Relief: FY 2013 country operational plan guidance. Washington, DC: OGAC.
OGAC. 2013. Partners. http://www.pepfar.gov/funding/budget/partners/index.htm (accessed May 31, 2013).
Padian, N. S., S. I. McCoy, S. S. Karim, N. Hasen, J. Kim, M. Bartos, E. Katabira, S. M. Bertozzi, B. Schwartlander, and M. S. Cohen. 2011. HIV prevention transformed: the new prevention research agenda. Lancet 378(9787):269-278.
PEPFAR (The President’s Emergency Plan for AIDS Relief). 2005. Focusing on our future: Prevention, diagnosis, and treatment of pediatric HIV/AIDS. Washington, DC: OGAC.
PEPFAR. 2010. Technical note on PEPFAR’s reporting methodology: Results of USG Global Fund contributions. http://www.pepfar.gov/2009results (accessed October 5, 2012).
PEPFAR. 2012. Report on costs of treatment in the President’s Emergency Plan for AIDS Relief (PEPFAR). Washington, DC: OGAC
PEPFAR and USAID (U.S. Agency for International Development). 2007. Data quality assurance tool for program-level indicators. Washington, DC: USAID.
PEPFAR/Mozambique. 2009. Country operational plan FY 2010. Washington, DC: OGAC. PEPFAR/Sudan. 2009. Country operational plan FY 2010. Washington, DC: OGAC.
PMI (President’s Malaria Initiative). 2009. Global Health Initiative and President’s Malaria Initiative. http://www.pmi.gov/about/ghi/increase.html (accessed May 31, 2013).
PMI. 2013. Fast facts: The President’s Malaria Initiative (PMI). Washington, DC: PMI.
PNPEC (National Program for Medical Care for People Living with HIV/AIDS). 2005. Guide de prise en charge de l’infection a VIH/SIDA de l’adulte et de l’enfant. Yamoussoukro: PNPEC Côte d’Ivoire.
Renaud-Théry, F. 2010. Annual 2010 survey on ARV use and trends in implementation of WHO 2010 ART recommendations. Presented at WHO & UNAIDS Annual Consultation with Pharmaceutical Companies—Global Forecasts of Antiretroviral Demand 2011-2012, Geneva, Switzerland.
Rosen, S., and M. P. Fox. 2011. Retention in HIV care between testing and treatment in sub-Saharan Africa: A systematic review. PLOS Medicine 8(7).
Rosen, S., M. P. Fox, and C. J. Gill. 2007. Patient retention in antiretroviral therapy programs in sub-Saharan Africa: a systematic review. PLOS Medicine 4(10):e298.
Rossi, V., and B. Ojikutu. 2011. HIV treatment guidelines in Guyana: The fast track to diagnosis and treatment. Arlington, VA: AIDSTAR-One.
Sessions, M. 2006. Overview of the President’s Emergency Plan for AIDS Relief (PEPFAR). Washington, DC: CGD.
Sharer, M., Fullem, A. 2012. Transitioning of Care and Other Services of Adolescents Living with HIV in Sub-Saharan Africa. Arlington, VA: USAIDS’s AIDS Support and Technical Assistance Resources, AIDSTAR-One, Task Order I.
Stadeli, K. M., and D. D. Richman. 2012. Rates of emergence of HIV drug resistance in resource-limited settings: A systematic review. Antiviral Therapy 18(1):115-123.
Stanecki, K., J. Daher, J. Stover, M. Beusenberg, Y. Souteyrand, and J. M. Garcia Calleja. 2010. Antiretroviral therapy needs: The effect of changing global guidelines. Sexually Transmitted Infections 86(Suppl 2):ii62-ii66.
Sungkanuparph, S., W. Techasathit, C. Utaipiboon, S. Chasombat, S. Bhakeecheep, M. Leechawengwongs, K. Ruxrungtham, and P. Phanuphak. 2010. Thai national guidelines for antiretroviral therapy in HIV-1 infected adults and adolescents 2010. Asian Biomedicine 4(4):515-528.
Swaziland Ministry of Health and Social Welfare. 2006. National guidelines for antiretroviral treatment and post exposure prophylaxis for adults and adolescents. Mbabane: Swaziland Ministry of Health and Social Welfare.
Talam, N. C., P. Gatongi, J. Rotich, and S. Kimaiyo. 2008. Factors affecting antiretroviral drug adherence among HIV/AIDS adult patients attending HIV/AIDS clinic at Moi Teaching and Referral Hospital, Eldoret, Kenya. East African Journal of Public Health 5(3):74-78.
Tanzania Ministry of Health. 2005. National guidelines for the clinical management of HIV and AIDS. Dar es Salaam: National AIDS Control Programme, Ministry of Health, United Republic of Tanzania.
Taylor-Smith, K., H. Tweya, A. Harries, E. Schoutene, and A. Jahn. 2010. Gender differences in retention and survival on antiretroviral therapy of HIV-1 infected adults in Malawi. Malawi Medical Journal 22(2):49-56.
Uganda Ministry of Health. 2008. National antiretroviral treatment guidelines for adults, adolescents, and children. Second edition. Kampala: Uganda Ministry of Health.
Ukraine Ministry of Health. 2004a. Clinical protocol for ARV therapy for HIV infection in adults and teens. Kiev: Ukraine Ministry of Health.
Ukraine Ministry of Health. 2004b. Clinical protocol for conducting antiretroviral therapy in children with HIV infection and AIDS. Kiev: Ukraine Ministry of Health.
UNAIDS (Joint United Nations Programme on HIV/AIDS). 2011. AIDS at 30: Nations at a crossroads. Geneva: UNAIDS.
UNAIDS. 2012a. AIDSinfo. http://www.aidsinfoonline.org (accessed October 4, 2012).
UNAIDS. 2012b. Global report: UNAIDS report on the global AIDS epidemic 2012. Geneva: UNAIDS.
UNAIDS. 2012c. Together we will end AIDS. Geneva: UNAIDS.
UNAIDS. 2012d. UNAIDS World AIDS Day report 2012. Geneva: UNAIDS.
UNAIDS. 2013. Email communication between UNAIDS staff and IOM: “FW: U.S. Institute of Medicine (IOM) Request for Permission to Use Figure in Upcoming PEPFAR Evaluation Report.” Washington, DC: IOM.
UNITAID. 2013. About UNITAID. http://www.unitaid.eu/en/who/about-unitaid (accessed May 31, 2013).
USAID and DoS (U.S. Department of State). 2009. Addressing water challenges in the developing world: A framework for action. Washington, DC: Bureau of Economic Growth, Agriculture, and Trade, USAID and Bureau of Oceans, Environment and Science, DoS. Violari, A., M. F. Cotton, D. M. Gibb, A. G. Babiker, J. Steyn, S. A. Madhi, P. Jean-Philippe, and J. A. McIntyre. 2008. Early antiretroviral therapy and mortality among HIV-infected infants. New England Journal of Medicine 359(21):2233-2244.
Visser, M. 2012. Women, HIV and stigma. Future Virology 7(6):529-532.
WHO (World Health Organization). 2004a. Scaling up antiretroviral therapy in resource limited settings: Treatment guidelines for a public health approach, 2003 revision. Geneva: WHO.
WHO. 2004b. Summary country profile for HIVAIDS treatment scale-up: Sudan. Geneva: WHO.
WHO. 2005a. Summary country profile for HIVAIDS treatment scale-up: Angola. Geneva: WHO.
WHO. 2005b. Summary country profile for HIVAIDS treatment scale-up: Democratic Republic of the Congo. Geneva: WHO.
WHO. 2005c. Summary country profile for HIVAIDS treatment scale-up: Rwanda. Geneva: WHO.
WHO. 2006a. Addressing violence against women in HIV testing and counselling: A meeting report. Geneva: WHO.
WHO. 2006b. Guidelines on co-trimoxazole prophylaxis for HIV-related infections among children, adolescents and adults: Recommendations for a public health approach. Geneva: WHO.
WHO. 2008. Essential prevention and care interventions for adults and adolescents living with HIV in resource-limited settings. Geneva: WHO.
WHO. 2010a. Antiretroviral drugs for treating pregnant women and preventing HIV infection in infants: Recommendations for a public health approach. 2010 revision. Geneva: WHO.
WHO. 2010b. Antiretroviral therapy for HIV infection in adults and adolescents: recommendations for a public health approach. 2010 revision. Geneva: WHO.
WHO. 2010c. Antiretroviral therapy for HIV infection in infants and children: Towards universal access. Recommendations for a public health approach. 2010 revision. Geneva: WHO.
WHO. 2012a. Guidance on couples HIV testing and counselling including antiretroviral therapy for treatment and prevention in serodiscordant couples: Recommendations for a public health approach. Geneva: WHO.
WHO. 2012b. Programmatic update: Use of antiretroviral drugs for treating pregnant women and preventing HIV infection in infants. Geneva: WHO.
WHO. 2012c. Retention in HIV programmes: Defining the challenges and identifying solutions: meeting report, 13-15 September 2011. Geneva: WHO.
WHO. 2012d. Service delivery approaches to HIV testing and counselling (HTC): A strategic HTC programme framework. Geneva: WHO.
WHO. 2012e. Tuberculosis fact sheet. http://www.who.int/mediacentre/factsheets/fs104/en/(accessed November 17, 2012).
WHO. 2012f. WHO policy on collaborative TB/HIV activities: Guidelines for national programmes and other stakeholders. Geneva: WHO.
WHO. 2013. WHO definition of palliative care. http://www.who.int/cancer/palliative definition/en (accessed May 31, 2013).
WHO and UNAIDS. 2007. Guidance for provider-initiated testing and counseling in health facilities. Geneva: WHO and UNAIDS.
WHO, UNAIDS, and UNICEF (United Nations Children’s Fund). 2009. Towards universal access: Scaling up priority interventions in the health sector. Progress Report 2009. Geneva: WHO, UNAIDS, and UNICEF.
WHO, UNAIDS, and UNICEF. 2010. Towards universal access: Scaling up priority interventions in the health sector. Progress Report 2010. Geneva: WHO, UNAIDS, and UNICEF.
WHO, UNAIDS, and UNICEF. 2011. Global HIV/AIDS Response: Epidemic update and health sector progress towards universal access. Progress report 2011. Geneva: WHO.




































































































