
Courts, Jails, and Drug Treatment in a California County
Mary Dana Phillips
No understanding of the contemporary drug scene in the United States can be achieved without focusing in part on the role of the criminal justice system. Large numbers of drug users and addicts are processed through various phases of the system at one time or another (Peterson, 1974; Weissman and DuPont, 1983; Bureau of Justice Statistics, 1983), and there is an important body of research on the extent of drug use among arrestees, felons, and misdemeanants convicted on drug law violations and drug-related criminal activity, on jail and prison inmates with histories of drug use, and on the criminal records of drug treatment clients (Allison and Hubbard, 1985; Flanagan and Jamieson, 1988; Hubbard et al., 1989). So intertwined are the treatment and justice systems that the goals of drug treatment often directly include the elimination or reduction of criminal activity.
It is difficult to say with precision what proportion of all drug users are involved with the criminal justice system. Although the numbers of individuals arrested and prosecuted for illicit drug involvement are widely used as indicators of the prevalence and severity of the drug problem (Gandossy et al., 1980; Gropper, 1984), these numbers are equally a measure of law enforcement priorities and resources (Sloan, 1980; Krivanek, 1988). The direction of the relationship between drugs and crime—which comes first and which causes the other—continues to be contested (Watters et al., 1985; Inciardi, 1987).
The developing interface between the criminal justice system and community and institutional treatment programs poses a number of practical and philosophical questions. By most accounts, drug use constitutes an ever-increasing problem for the community and for law enforcement,
Mary Dana Phillips is a research associate with the Alcohol Research Group, Institute of Epidemiological and Behavioral Medicine, Medical Research Institute of San Francisco, Berkeley, California.
adjudication, and corrections. This trend has three corollaries in recent history: (1) more offenses are seen to be ''caused'' by drugs; (2) drug and drug-related offenses, as such, are contributing more and more clients to the justice system; and (3) drug treatment is increasingly being sought as an adjunct or alternative to conventional punishment. Whereas public concern over drug-generated offenses has led to a stiffening of sentencing practices and contributed to the crowding of courts and detention facilities, programs that provide treatment and education for addicts and other users are often substituted for regular detention.
This paper offers a preliminary look at the overlap and connections between the criminal justice system and publicly supported drug treatment, assessing at the county level the appropriateness of the relationships between the justice system, drug users, and treatment programs. Although the two systems often work in parallel to handle drug-using persons, choosing from a complex set of alternative responses to particular circumstances, the two systems diverge in orientation and mission: one is designed to render judgment and due punishment according to a moral and legal code, the other to provide diagnostic and therapeutic services for a quasi-medical condition using scientific and clinical principles. The result is tension: political, philosophical, ethical, and instrumental. The recent "drug wars" increase the pressure on both systems to provide winning solutions. There is confusion as to how a person and a problem are to be defined; it is unclear how and when the definition (and thus, solution) changes from a criminal to a therapeutic one. There are different standards applied in different jurisdictions and even within jurisdictions at different administrative levels. Mandates to treatment, like many other judicial mandates, are subject to much local discretion and variability, in terms of selection criteria, sanction patterns, procedures, and the balance between the civil liberties of the individual and the prerogatives of the state (Kittrie, 1971; Wexler, 1973; President's Commission on Mental Health, 1978; Weissman and DuPont, 1982; Brown et al., 1987).
This paper seeks to provide a level of historical perspective to set the stage for a detailed case study analysis. It discusses the statutes that guide the criminal justice/drug treatment interface, the typical practices of the personnel within the systems, and the larger criminal justice and drug treatment ecologies in which they operate. There is reference to the drug treatment literature, the criminological literature on the emergence of alternatives to incarceration, discussions in both literatures on the specifics of the involvement of the two systems, and federal policy-setting documents, such as the papers from the Second National Commission on Marihuana and Drug Abuse (1973a,b,c), the task panel reports to the President's Commission on Mental Health (1978), and the report from the White House Conference for a Drug Free America (1988).
Data for the case study were taken from in-depth interviews with representatives of the criminal justice and drug treatment systems and various state and county statistical and substantive reports. The case study provides a detailed view of a particular region, its statutes and processes, and the gaps that tend to exist between theory and practice. State and local governments have substantial autonomy with regard to how they apprehend and behave toward drug-involved offenders. In-depth exploration of a county jurisdiction reveals both the strengths and weaknesses of its response to drug users. The overwhelming crowding of the courts and detention facilities, the lack of suitable or effective treatment for inmates, and the underuse of community programs—which stems in part from the need for more and different levels of treatment and other supportive services to augment these programs—have policy implications for the county.
THE NEXUS BETWEEN THE DRUG TREATMENT AND CRIMINAL JUSTICE SYSTEMS
Treatment provision has widened into a "two-worlds" model: one system is for those who have private insurance or can otherwise afford to pay; the other system is funded with public money and designed to treat citizens who cannot pay to receive services. Because publicly funded drug treatment capabilities currently fall short of the demand for services, citizens who cannot pay for their own treatment compete in a stream of referrals from the criminal justice, social welfare, and mental health systems. Only a fraction of those seeking such help can find a timely slot in the publicly funded programs that are squeezed for staff, facilities, and support from the communities they are supposed to serve. Client mixes in drug treatment programs have for years been a combination of people experiencing varying degrees of coercion or motivation to avoid criminal sanctions, but there is an argument to be made for paying closer attention to the composition of the client pool in treatment. Pressure from one's doctor, family, or employer to participate in treatment is symbolically and instrumentally different from a judicial motion to enroll in a program. It is not currently known, however, what effect the proportions of criminal justice-referred and noncriminal justice-referred clients have on treatment experience and outcome (Stitzer and McCaul, 1987; Nurco et al., 1988).
Formal control is the cornerstone of public policy regarding drug-dependent and drug-using persons, and the judicial system has been relied on in a variety of ways to secure and maintain such control. There is a resurgence of interest now in adapting the justice system to assume the task of channeling persons into drug treatment. The issues raised by this
linkage were highlighted in the report presented by the Liaison Task Panel on Psychoactive Drug Use/Misuse to the President's Commission on Mental Health (1978:2118):
Today, the drug treatment system is caught in a fundamental conflict about "what is being treated". The basic confusion commences with the unwillingness of the formal institutional structures to explore the boundaries between psychoactive drug use and misuse. Even that separation is further confused by the question of who decides what the adverse consequences are: the patient, the physician or counselor, or a variety of agencies affiliated with the criminal justice system. The law enforcement establishment circularly labels all use of illegal psychoactive substances as misuse or "abuse," and the medical establishment labels all nonmedical use of psychoactive substances as misuse. Thus, by definition, psychoactive drug use is seen as demanding legal intervention and medical treatment.
The controversy generated by these authors in 1978 remains vigorous (see Anglin [1988] and Leukefeld and Tims [1988] for recent articles covering a range of opinions). Current interest in drug use and drug users is reflected by the regular and frequent discussions of them in the media and by national and local policymakers.
HISTORICAL PERSPECTIVES
The connection between the drug treatment system and the criminal justice system is longstanding and complicated. A chronological overview of some of the major legislative, judicial, medical, and social developments of the last century helps to set the scene for a more informed discussion of the present. Several pieces by Weissman detail the history of these developments, and an overview may be found in Drug Abuse, the Law and Treatment Alternatives (Weissman, 1978a; see also Duster, 1970; Musto, 1973a,b; Brecher, 1972; and Inciardi and Chambers, 1974). For a history of opiate addiction in America before 1940, see Courtwright (1982) and Terry and Pellens (1928).
The Criminalization of Drugs
During most of the nineteenth century, all drugs in the United States were licit, including opium, morphine, cocaine, and marijuana, and could be legally sold (Terry and Pellens, 1928; Brecher, 1972); regulation and criminalization occurred in the early decades of the twentieth century (Duster, 1970; Courtwright, 1982). In 1914, largely in response to treaty
obligations derived from ratification of the Hague Convention of 1912, Congress passed the Harrison Narcotic Act (Brecher, 1972; Weissman, 1978a). This act relied on federal customs and excise tax power to require manufacturers, distributors, and dispensers of opiates and coca products to register with the Treasury Department and to keep records of transactions involving these substances (King, 1974). As interpreted in the years after its passage, the Harrison Act in effect criminalized possession, use, and sale of opiates and cocaine for nonmedical purposes; it was the first time in the United States that criminal sanctions were uniformly imposed (Weissman, 1978a). Because doctors were not permitted to administer controlled substances to patients merely to maintain addiction, addicts were cut off entirely from all sources of legal (medical) relief. "Exit the addict-patient; enter the addict-criminal" (King, 1974).
The resultant generational change in the identity of a typical American opiate addict over the last century has been documented repeatedly (Musto, 1973a; Courtwright, 1982). The addicted population of the late nineteenth century was mostly middle-aged, middle-class, small-town white women. It became largely lower class urban males by roughly 1940, often of criminal occupations (Fort, 1968; Courtwright, 1982). Courtwright's view is that the transformation of the American addict was also a function of prevailing medical practices over time: addicts were common in the nineteenth century mainly as a result of physicians' wide use of opiate-based medicines. Patterns of nonmedically induced drug use also began in the nineteenth century but did not account for the bulk of the addicted or drug-using population until after the criminalization of drug use had already begun (Fort, 1968; Duster, 1970). Shifting medical therapies reduced reliance on opium derivatives; the concurrent shifts in American policies toward narcotic addiction, addicts, and users "paralleled and were entirely consistent with the independent and underlying transformation of the addict population" for nonlegal reasons (Courtwright, 1982:4).
Lindesmith, King, Trebach, Brecher, and others have advanced the view that the transformation of the American addict population was a function of abrupt changes in the legal status of the addict. The Harrison Narcotic Act of 1914 forced those who sought narcotics to turn to nonmedical supplies of opiates and increased the likelihood of association with other criminal activities. "The government's anti-maintenance policy succeeded in making a bad situation worse: criminal activity was at least in part a function of [high] black-market prices" (Courtwright, 1982:147). Supreme Court and Treasury Department decisions between 1919 and 1923 established a policy of virtual prohibition that included strict regulation of prescription drugs and criminal sanctions for use of illegal drugs or for illegal use of medicinal drugs (King, 1974; Weissman, 1978a; Courtwright,
1982).
From this time on, drug users and sellers began to constitute a considerable proportion of all those arrested at the federal level (Klein, 1983). Treatment for addicted persons began as a response to the "choking of federal prisons with addict-criminals" (King, 1974). In 1929, in part to relieve the crowding of federal prisons with drug law violators, the Public Health Service and the Bureau of Prisons received congressional authorization to open two narcotic farms: one in Lexington, which was opened in 1935, and one in Fort Worth, which was opened in 1938 (King, 1974; Weissman, 1978a). Addicted persons convicted in federal courts could be sent to these Public Health Service prison hospitals in lieu of ordinary imprisonment (King, 1974). Although the hospitals also accepted voluntary clients, they were run as medium-security penal institutions and had both rehabilitative and addiction research purposes (King, 1974; Weissman, 1978). The criminal justice system and the drug treatment system have "shared" clients, then, ever since punishment became an option for drug addicts in the United States. Some writers have categorized the criminal justice system as the drug treatment system's ''main casefinding mechanism" (President's Commission on Mental Health, 1978; Klein, 1983).
In 1930 Congress replaced the scandal-ridden Narcotic Unit within the Treasury Department's Bureau of Prohibition with the Federal Bureau of Narcotics (King, 1974; Weissman, 1978; Courtwright, 1982). Harry Anslinger was its director until 1962, a period Musto has called "the peak of punitive legislation against drug addiction in the United States" (Musto, 1973a). Mandatory minimum penalties were common for drug offenders; most were not remanded to the farms but to traditional incarcerative settings with other criminals.
Except for heroin, the prescription of narcotics remained legal in the United States. After 1914 some addicts were able to obtain drugs from physicians by exhibiting "symptoms" of an illness. Physicians were under pressure to demonstrate the legitimacy of the patient's condition for whom narcotics were prescribed. At the same time a subculture of users and addicts relied on imported heroin or illegally obtained but legally manufactured pharmaceuticals. Many of the drug users and addicts who were arrested and channeled into the criminal justice system until the 1960s were also found to be heavily involved in other forms of criminal activity.
Reforming Drug Policy in the 1960s
The 1960s were a decade of experimentation, both on the part of drug users and on the part of drug policy administrators. One manifestation of
this prevailing mood was the report, Drug Addiction: Crime or Disease? issued in 1961 by the Joint Committee of the American Bar Association and the American Medical Association on Narcotic Drugs. Heavily indebted to the work of Indiana University sociologist Alfred Lindesmith (1965), it called for an open and, when necessary, critical discussion of the current policies and laws governing the handling of narcotic substances and those who used them. Without attempting to provide solutions, it reflected "a degree of dissatisfaction within the legal and medical professions concerning current policies which tend to emphasize repression and prohibition to the exclusion of other possible methods of dealing with addicts and drug traffic" (Joint Committee of the American Bar Association and the American Medical Association on Narcotic Drugs, 1961:161). Some of the report's conclusions were that medicine and public health could be called on to make greater contributions to the handling of drug-involved offenders, the prevention of problems needed a place in the debate, and outpatient or community-based care ought to be explored. Overall, more research was needed, especially to explore an expansion of treatment services and to establish a basis for more balanced and informed debate.
The White House Conference on Narcotics and Drug Abuse was convened in 1962, and rehabilitation rather than punishment emerged as its theme (Weissman, 1978a). Lindesmith's classic contribution to the debate, The Addict and the Law, appeared in 1965. It highlighted the subtle and complex nature of the issues that frame whether drug users are treated as criminals or as individuals with a disease. In addition, it provided further intellectual inspiration to the energies then moving toward reform.
In 1961 California authorized the involuntary civil commitment of narcotics addicts in need of treatment. The use of coercion to induce treatment became sanctioned by the judicial system; accordingly, the treatment that was delivered retained a more punitive than therapeutic tint. In California the Civil Addict Program was administered by the Department of Corrections and not by a health or drug and alcohol department.
Early California rehabilitation legislation had two main emphases: (1) short-term crisis intervention and detoxification programs in the community for gravely disabled drug-dependent persons, and (2) long-term post-conviction inpatient treatment and closely supervised parole (under the Department of Corrections) for addicts only. Legislation in 1972 encouraged multimodality community-based outpatient and inpatient programs, including methadone maintenance. This legislation (partly reflected in current California statutes—see Appendix A) also provided for diversion into treatment of drug law violators from the criminal justice system; it has since been expanded to allow diversion of people with other types of offenses as well (Second National Commission on Marihuana and Drug Abuse, 1973a).
New York passed a similar law in 1962. Similar federal legislation, the Narcotic Addict Rehabilitation Act (NARA) of 1966, also set the stage for massive federal funding of treatment programs in the 1970s. This legislation provided more broadly for civil commitment as an alternative to prison. NARA authorized (1) pretrial civil commitment in lieu of prosecution for persons charged with certain nonviolent, nontrafficking federal crimes who could convince a federal district attorney that they were addicted but had a high probability of rehabilitation; (2) voluntary civil commitment for addicts not under criminal charges, a program administered by the National Institute of Mental Health; and (3) sentencing of some addicts convicted of certain federal crimes to commitment for treatment, a program administered by the Bureau of Prisons. The clients of the latter were treated in selected prisons and could then be paroled to outpatient care in the community. NARA also authorized federal grants to communities to fund treatment programs for addicts (Bonnie and Sonnereich, 1973; King, 1974; Maddux, 1988).
According to the report and appendices of the Second National Commission on Marihuana and Drug Abuse (1973a,b,c), civil commitment is not a treatment mechanism as such but rather a mechanism for retaining and supervising individuals while they participate in a course of treatment. It is in this enforced and prolonged supervision that it differs chiefly from voluntary programs. Maddux (1988) has recently reviewed 50 years of clinical experience with addicts in treatment, including those being treated voluntarily, those under various criminal law coercions, and those under civil commitment, using data from the U.S. Public Health Service hospitals and from NARA. He concludes that civil commitment brings people into treatment who might not otherwise get there. But it cannot assure their participation, it cannot overcome deficits in services, and it remains restricted by constitutional guarantees of individual liberty (Maddux, 1988).
The shift to view addiction as a health issue rather than (only) a criminal or moral issue was well under way by the mid-1960s. The idea that intractable social problems—such as drug problems—undergo periodic redefinition and are turned over to or are shared by different social institutions and occupations has been developed extensively in the literature (Gusfield, 1967; Pitts, 1968; Brüün, 1971; Room, 1978). This change in perspective led to what has been called "the medicalization of deviance" (Gusfield, 1967; Pitts, 1968; President's Commission on Mental Health, 1978; Conrad and Schneider, 1980): the identified "deviant" is committed to a hospital instead of a prison, and the objective becomes curing rather than punishing (Wexler, 1973; Glaser, 1974; see Kittrie, 1971, for a detailed legal and philosophical history of these shifts).
This reaction to some but not all types of drug addicts and users accelerated rapidly after 1962, when Robinson v. California was decided by
the Supreme Court. The case involved an appeal from a misdemeanor conviction under a statute that made it unlawful to be "addicted to narcotics." The Supreme Court held that to penalize an addict was a violation of the Eighth Amendment provision against cruel and unusual punishment: the conviction was not based on anything the defendant had done but on his illness (Sloan, 1980); the statute was thus ruled unconstitutional. The ruling also suggested that it would be legitimate to declare addiction a disease justifying civil commitment (Glaser, 1974).
During the 1960s the amounts and types of drug use, and the ways people were using drugs, as well as the social class of users, changed as well. Drug users were no longer exclusively associated with patterns of frequent street crime. Experimentation with a variety of substances, including marijuana, LSD, amphetamines, and prescription pharmaceuticals, became widespread. People from middle and upper class backgrounds joined the ranks of those who used a variety of licit and illicit substances for pleasure, or "kicks," as well as for generational symbolism, including displaying disapproval of the mores of society and the policies of government.
The criminal justice system itself was in the throes of upheaval and experiencing a period of disenchantment with traditional practices and their underlying philosophies. This was a time of riots in the prisons and exposés in the media of cruel and unusual conditions within them (Packer, 1968; Goldfarb, 1975; Feeley, 1983). High rates of criminal recidivism among drug users and a continuing rise in the cost, frequency, and seriousness of crime linked to drug users frustrated officials and perhaps encouraged them to try something else (Ohlin, 1973; Weissman, 1978). A philosophy that proposed humane rehabilitation and opportunities for treatment in place of deprivation and incarceration for those whose criminality could be linked to drug use found resonance in a criminal justice system looking for alternatives to traditional but unsuccessful methods (Jaffe, 1979).
Treatment approaches for drug users, especially heroin addicts, expanded as a part of a "war on heroin" and, more generally, reactions against drugs, crime, and accompanying lifestyles (Second National Commission on Marihuana and Drug Abuse, 1973a; Klein, 1983). Law and order campaigns in the late 1960s and early 1970s drew support from the fears of a voting populace that had been assailed by anti-Vietnam war activities, the civil rights movement, student unrest, and more broadly defined cultural shifts among youth with respect to both drug use and sexual behavior.
Treatment provided opportunities for recovery and encorporated more progressive methods of dealing with drug users than imprisoning them. Nonetheless, treatment was also seen as a way of maintaining careful
supervision of drug-involved offenders, only partially extricating them from the traditional criminal justice system. The Nixon administration's "War on Drugs" had weapons to reduce the supply side, including the Drug Enforcement Agency to interdict imported substances, and "get-tough" laws to reduce the ''demand" side through the detection and punishment of users and the deterrence of future consumers.
At the same time there was substantial growth in the federally and state-funded social service apparatus. Demarcations between treatment as a part of the social welfare and health care systems and the criminal justice system were becoming less clear. "Community-based" programs were favored over incarcerative models for juvenile delinquency prevention, health (especially mental health) care, and other public services (Fox, 1973; Wexler, 1978). Both political and fiscal considerations were at work here; decarceration was envisioned as more efficient, serving more people per dollar. The local service providers welcomed a chance to provide flexible care at the local level where they had greater authority and discretion. This marriage between community care providers and judicial system referral mechanisms resulted in a vast network of treatment opportunities for people whose original interaction was with the justice system. The marriage was paid for by federal-state cost sharing during the early 1970s.
Diversion from the Criminal Justice System to Treatment in the 1970s
The demand for policy alternatives offering the penal features of criminal law but the therapeutic features of health care had been building for half a century. The growth of the federally funded system of community-based programs authorized by NARA and later by the National Institute on Drug Abuse (NIDA) made the practice of court referral of addicts to community treatment a commonplace. In 1972, through the efforts of the Special Action Office for Drug Abuse Prevention (located in the Executive Office of then-President Richard Nixon), the routing of addicts to treatment was further increased by the referral of unsentenced defendants to community-based treatment in lieu of prosecution. This move was based on the assumed causal relationship between drug taking and criminal behavior. It was buttressed by a coexisting belief that treatment was beneficial for drug-dependent persons, whether such treatment occurred voluntarily or involuntarily (Smith, 1974). This system interface—and the assumptions underlying it—remains at the heart of the national approach to drug users.
Diversion at the pretrial stage of the adjudication process was made possible in the United States by recommendations of the President's
Commission on Law Enforcement. The commission proposed the practice in 1967, claiming that "it is more fruitful to discuss, not who can be tried and convicted as a matter of law, but how the offices of the administration of criminal justice should deal with people who present special needs and problems.. .[the solution being] the early identification and diversion to other community resources of those offenders in need of treatment, for whom full criminal disposition does not appear required" (President's Commission of Law Enforcement and Administration of Justice, 1967:134). Diversion was originally designed for alcohol-involved offenders and people with chronic mental problems, but it quickly became popular for a variety of dispositions. These offenders were seen to be burdensome to the criminal justice system, preventing it from catching and punishing "real" criminals more efficiently. Moreover, in the words of two veterans of the American judicial system, it offered "the promise of the best of both worlds: cost savings, along with rehabilitation and more humane treatment" (Vorenberg and Vorenberg, 1973; see also the Yale Law Journal, [1974]).
The classical definition of diversion is therapeutic intervention that takes place following arrest but before either a trial or adjudication. Several of the papers found in the appendices to the report of the Second National Commission on Marihuana and Drug Abuse (1973b,c) include the following procedures as falling under the category of diversion:
-
pre-arrest, formally authorized diversion for purposes of detoxification or withdrawal;
-
postarrest, diversion to detox;
-
treatment as a condition of pretrial release;
-
emergency treatment while awaiting trial;
-
treatment in lieu of prosecution;
-
treatment as a condition of deferred entry of a judgment of guilt and conditional discharge, or as a condition of suspension of sentence or probation;
-
treatment as a condition of probation or parole; and
-
commitment for treatment in lieu of other sentence, or while serving a sentence in a correctional facility or following administrative transfer from a penal institution.
Nationwide, procedures at the local court level that may be formally designated or loosely categorized as "diversionary" are many and varied. Diversion programs vary not only with respect to a lack of uniformity of procedures but also in the extent to which the defendant penetrates the criminal justice system, a factor that may vary even within states by county or judicial jurisdictions (Carter, 1972; Agopian, 1977; Weissman, 1978b;
1979; Gottlieb, 1985). Specific operations may be driven in part by legal or policy considerations, fiscal realities, the relative climate of the local courts, and the size and schedules of their caseloads. Some diversionary procedures derive their authority from statute law, whereas others rely on court rules or prosecutorial discretion. However indirectly, all rely on the existence of (and availability of space within) treatment programs. Most diversion programs seem to share certain goals and principles. These include the early identification and referral to treatment of drug-involved offenders, goals that allow the workload imposed on the criminal justice system to be reduced by the volume of drug-related cases that are dispensed with in an alternative fashion.
At its best, diversion allows the court to recognize the seriousness of official concern for certain offenses while retaining a flexible range of alternative sentencing measures at the pretrial stage of the proceedings. It was designed to benefit the defendant, prosecutors, the court, and the community. As an alternative to standard options, diversion is also appealing because it represents a continuing attempt to structure and make visible many informal prosecutorial practices found across a range of dispositions. It may also be submitted as evidence of an ideological shift in emphasis from deterrence to rehabilitation; pretrial diversion minimizes penetration into the formal processes of the justice system. As a result, diversion is endorsed as a process capable of avoiding the stigmatizing experiences of traditional justice system processing.
Diversion, not unlike probation, may be seen as both an exchange and as a sentencing process. As in plea bargaining, there is a ''legitimate exchange of tactical concessions to the mutual advantage of the defense and the prosecution" (Yale Law Journal, 1974:843). Diverted cases and defendants allow costs associated with traditional adjudicatory and correctional practices to be averted. Society in turn is expected to benefit from reduced recidivism rates linked to diversionary practices that are characterized as therapeutic rather than punitive.
At its worst, diversion may be viewed as a supralegal mechanism, a tool available to the court to dispose of defendants and cases using alternative strategies that do not uniformly adhere to laws and procedures specifically in place to protect defendants' civil liberties (Second National Commission on Marihuana and Drug Abuse, 1973a,b,c, Senay et al., 1974; Yale Law Journal, 1974; Alper and Nichols, 1981; Harrington, 1985). Critics of diversion share common concerns about the guarantee of due process rights during diversion procedures, which stem in part from the enormous variance in the extent to which defendants penetrate the system. A failure in the adjudication process to define clear boundaries that are explicitly linked to judicial practices and based in the law often allows unpredictable and even disturbing levels of discretion to be exercised by
the courts. Violations of due process are best prevented through the systematic use of procedural safeguards that are explicitly required and based in constitutional law and that are comprehensive with regard to the shifting patterns of diversionary cases and clients (Klapmuts, 1974; Harrington, 1985). Otherwise, efforts to evaluate diversion programs are placed in a precarious position along with more basic constitutional guarantees. Although diversion programs are not necessarily invalidated by these concerns, procedural safeguards of due process rights are not always fully observed.
Research on police behavior and lower courts in the early 1960s suggested that official attitudes and practices toward defendants were best characterized by a crime control model rather than a due process model (Packer, 1968; Harrington, 1985). The court reforms of the late 1960s to the mid-1970s were concentrated on the lower courts and on delineating the amount of discretion police, prosecutors, and judges had in previously unregulated proceedings. The ideal of diversion is an "attempt to structure and make visible the informal prosecutorial practices on noncriminal disposition" (Yale Law Journal, 1974:852). This involved the use of procedural fairness and official guidelines to control official discretion, not increase it, and to protect rather than jeopardize individual rights in these situations (Harrington, 1985). Thus, diversion was not just "a unique approach to the management of deviance but an essential part of a much broader movement of social and criminal justice reform" (Klapmuts, 1974).
The rapid and sweeping moves of federal and state governments to establish and support diversion programs represent a convergence of several complementary forces. Discussions were held in 1971 by the Law Enforcement Assistance Administration, the White House's Special Action Office for Drug Abuse Prevention, and the National Institute of Mental Health's Division of Narcotic Addiction and Drug Abuse (NIDA's predecessor) on how to link treatment and the judicial process, thereby interrupting the relationship between drugs and property crimes (Bureau of Justice Assistance, 1988). The resulting federal initiative, modeled after earlier experiments with diversion projects in New York City and Washington, D.C., was funded under the Drug Abuse Office and Treatment Act of 1972 and was known as Treatment Alternatives to Street Crime (TASC). The program represented a formalization of various criminal justice pressures to move addicts into treatment and hold them there for as long as was indicated.
TASC components include identification of the drug-dependent offender, assessment of the individual's drug dependency and community risk, referral to the appropriate community treatment resources, and case management of the individual to maintain compliance with justice and treatment criteria (Toborg et al., 1976). When arrested, the suspect is
evaluated by a diagnostic unit and held pending transfer to a treatment program. Dropping out of treatment prematurely or any other act of noncompliance is treated by the courts as violation of the conditions of release. TASC program participants are under direct supervision of the court, the treatment program, and the TASC worker assigned to their case. Because of the leniency of some treatments, TASC programs often diverted those who were not addicted to an illicit substance and for whom criminal conviction was seen as too severe, such as occasional users of marijuana.
TASC originally focused on pretrial intervention, but this approach was resisted by some courts and prosecutors and was broadened or constrained according to local preferences (Weissman, 1979). By 1974, each locality was allowed to decide whether screening was to be mandatory or voluntary and to determine eligibility standards, points of referral, choice of treatment modality, and criteria of success (Kadish, 1983). Advocates of the program extol its evolution from originally a heroin addict identification program aimed at crime reduction into a social services and treatment brokerage system for criminal justice adjudicatory and offender-serving agencies (Weissman, 1979).
TASC was funded through the 1970s by both federal and state dollars to the local community, usually either a county or greater municipal area. In an article reviewing every state's drug diversion policies in 1979, Weissman demonstrates the broad discretion states exercised in how programs were administered. The federal government last provided money and specific procedural guidelines by direct allotment to states or local communities in 1980. Since then, diversity in state and local practices has only increased, as both program rules and funds are no longer directly overseen by a federal body that provides some measure of uniformity. TASC money became part of what is still available under the federal block grant program, but there is enormous variation in programs and program components currently in operation and funded by TASC block grants. A broad range of legal, fiscal, and philosophical judicial systems design and administer programs that compete for support. TASC may be seen as successful in the sense that many jurisdictions have continued to offer programs that were begun with pre-block grant federal funds and have received support for them from both state and local government sources (Weissman, 1978b, 1979). Currently, 100 sites in 18 states have programs using the name TASC (Bureau of Justice Assistance, 1988).
There has been no systematic comparison of all these programs with one another, especially to review and evaluate their components and the relative success or failure of services for the drug-involved offender in treatment. The evaluations of some TASC programs point to its ability to keep people in treatment longer, but they do not necessarily show
better results once treatment has ended (Bureau of Justice Assistance, 1988). "These studies have also shown that the lack of data collection and evaluation as critical program elements has hindered TASC programming" (Bureau of Justice Assistance, 1988:6).
The TASC philosophy and program components lend themselves to compartmentalization; various combinations of services and functions are adopted by jurisdictions with specific funding or legal restrictions. One part of the TASC program that may be active in one place, such as TASC workers acting as advocates for their clients with the criminal justice system, may not necessarily be found in another (Weissman, 1979). This in fact has been one of the criticisms of the strategy: that it is different everywhere; diversion as part of the judicial system is under state jurisdiction, and many states in turn give local courts the power to interpret state laws using their own discretion.
Programs described as "diversionary" or "community-based" are potentially more effective in achieving the desired result of rehabilitation. There is no question that a medically managed detoxification is preferable to ''sweating it out" in a cell. There is also little doubt that the criminal justice system can introduce people to treatment who might not otherwise ever experience it. Yet the potential for abuse latent within the administrative discretion operationalized in many diversion programs is also real (Yale Law Journal, 1974; NIDA, 1978; Toborg, 1981; Mosher, 1983). Hudson and colleagues (1975:19) issue a sharp warning that may yet deserve attention:
[The potential for abuse] is especially the case when clearly articulated and openly established program policies and procedures are lacking. Most diversion programs are viewed as treatment or quasi-treatment alternatives to conventional processing by the criminal justice system. These programs, however, have in common with the criminal justice system a governmental policy aimed at solving social problems by obtaining individual compliance to a given social structure. Given the assumption that most of these programs provide closer surveillance or supervision of their clients, have quicker reactions to client behaviors, and greater political leverage with community decision-makers, what may begin as a benevolent program designed to help the offender could turn into a more oppressive program than the conventional correctional alternative.
The debate about the relative value of mandates to treat drug-involved offenders continues. For more current discussions of diversion, probation and the nexus between the criminal justice and drug treatment systems, see Chambers and coworkers (1987), NIDA Monograph No. 86 (Leukefeld and Tims, 1988), Brown and associates (1987), and the entire issue of the Journal of Drug Issues (Anglin, 1988) on the compulsory treatment of opiate dependence. At this juncture, however, it is instructive
to turn to the case study of a California county as a critical departure for more general remarks about the pathways to treatment from the criminal justice system.
CASE STUDY OF A CALIFORNIA COUNTY
The California county analyzed here1 is a case in which no formal TASC-type program exists to guide the courts and treatment providers as they interpret the laws regarding drug users as the basis for intervention. No formal program has ever existed within this county's criminal justice system to systematically broker for treatment services. This function has always been a part of the domain of the probation department. In contrast to numerous other California counties and administrative regions around the country that have TASC programs or other formal mechanisms that are specifically assigned to the management of criminal justice-referred drug treatment clients, the county's drug treatment system has no personnel, programs, or program components specifically designed to manage criminally involved clients.
The case study site was a choice of convenience. The experiences and practices of a single county are probably neither unique nor typical but representative in a generic way of non-TASC jurisdictions, which constitute the great majority of counties across the country. The purpose of this inquiry is to examine objectively how the criminal justice and drug treatment systems are linked, how the links have withstood or resolved some of the previously identified tensions, and how the "system" continues to function in the absence of a formal arrangement.
Data in this section were drawn from a series of in-depth interviews with administrative officials connected to both systems, as well as with both clients and treatment providers in methadone programs, residential treatment settings, outpatient programs, and two of the county's detention facilities. Other sources include the California State Penal Code and statistical reports compiled by the Judicial Council of California, the California State Department of Justice, the county municipal court system, the probation department, the county's detention facilities, and the Drug Abuse Program administrative office.
Before examining the relationship between the criminal justice and drug treatment systems, it is helpful to have an overview of the study county. It includes urban, suburban, and rural areas. A full range of socioeconomic statuses can be found in its mix of older industrial towns and neighborhoods as well as in its newer technocratic urban centers and their accompanying housing and commercial developments. Like all California counties, its criminal justice system is governed by the state
constitution and laws.
The population of the county was approximately 750,000 in 1987, with nearly 80 percent residing in cities and the remaining 20 percent in unincorporated areas. The majority of the county's residents are white (85 percent), with blacks representing somewhat less than 10 percent of the total. People identifying themselves as being of Spanish origin make up most of the remainder.
The county is characterized by communities in which individuals, no matter what their ethnicity, tend to share socioeconomic status. The mean income of all families was $30,000 in 1979, but when the population is stratified by race and the mean family income is recalculated, white and Asian families enjoy incomes above the county mean. Black and Native American families and families of Spanish origin have family incomes considerably below the county mean, although only 8 percent of the total county population live below the poverty level. One geographically segregated section of the county also contains a large proportion of minority and poor individuals. One could say that the county is basically a wealthy suburban area with pockets of poverty.
County Drug Abuse Treatment System
The county Drug Abuse Program is a branch of the Alcohol, Drug Abuse, and Mental Health Division, one of five divisions within the county's Department of Health Services. The drug program administrator reports to the deputy division director and is advised by a drug abuse advisory board. The county-operated drug programs each employ a program director who reports to the drug program administrator. The program directors are responsible for facility management, staff supervision, and the provision of direct services.
Some programs are run by the county, and others provide services on a contract basis. The budget for all programs was nearly $2 million for FY 1986-1987. Funding sources for program activities can be broken down as follows: 45 percent state, 23 percent federal, 16 percent Medi-Cal (a California state program roughly similar to Medicare), 3 percent user fees, and 13 percent county funds. The types of services offered in the county are prevention, education, and treatment for youth; prenatal and perinatal educational services for women; and outpatient prevention, education, and some treatment services for parents, families, and some individuals. The Drug Abuse Program Office uses its funds to provide residential treatment (23 percent), methadone treatment (17 percent), and prevention and outpatient counseling services (50 percent); the remaining 10 percent is spent on administration and overhead. The number of county employees
working in drug services as of September 1988 was 16. The number of county contractor program employees working in drug services as of September 1988 was 39.
The county provides a range of services in its 11 outpatient counseling and education programs. These include primary prevention and secondary prevention or early intervention with those identified as being at high risk for drug abuse. Targeted clients of these programs tend to be adolescents, other school-aged children and adults who are part of the targeted adolescent's family, and pregnant drug-abusing females. The number of outpatient treatment program admissions for FY 1987-1988 was 693. (This figure does not include those who participated in education and prevention programs.) Of those admissions, 22 percent were black, 68 percent white, and 9 percent Hispanic; 42 percent of the total were women.
The county operates two drug-free adult residential treatment programs, one coed and one for males. Both offer care from 12 to 16 months; the all-male program is licensed for 30 adults, the coed facility, for 15. The number of residential treatment program admissions for FY 1987-1988 was 167. Of those, 56 percent were black, 39 percent white, and 5 percent Hispanic; 36 percent of the total admissions were women.
Methadone services for both detoxification and maintenance are offered at two sites in the county. Within the last two years the county has introduced a fee-for-service type of payment scheme, quadrupling the number of available slots while cutting the number of publicly supported patients. Of the 150 detox slots, 14 are publicly supported; of the 300 maintenance slots, 140 are paid for by Medi-Cal. The county's methadone budget was cut in half in 1988; it accounts for only 17 percent of all drug treatment monies in the 1988 budget, down from the 35 percent share it had in 1987. For the paying clients, methadone maintenance costs $165 per month; detox costs $250 for a 21-day dosing schedule.
The source for the above information is a report commissioned by the Health Services Department and the county's drug abuse advisory board; it includes a multiyear plan for drug abuse services. Some of the report is a series of tally sheets required by the state for funder accountability, much of the rest of it deals with the advisory board's elaborate planning process to meet its goal of a drug-free county. Although some mention was made of monitoring activities to evaluate the progress made toward measurable objectives, neither the report nor the administrator had any data that provided evaluative outcome information. One of the objectives of the report was to evaluate existing services as a part of the planning process. The priorities of the board are reflected in the levels of funding.
The report is inconsistent in several respects. In the first place, one
of the indicators cited as proof of the severity of the drug problem is the large number of county residents identified as being at high risk for drug abuse. This group includes people living below the poverty line, especially minorities, disproportionately high numbers of single and divorced persons under age 30, and people who are too old or too young to be in the work force. Yet very few of the planned or extant services are directed toward these populations. Furthermore, much of the statistical information in the report detailing the county's drug problem was taken from criminal justice system data (reviewed in the next section) and other data estimating the number of current illicit drug users. Very little mention is made in the report of plans to meet the treatment needs of these people.
The problem indicator data do not appear actually to govern the setting of priorities for types and levels of services offered by the county. The bulk of the county's drug budget goes for prevention or education activities aimed at youth and their families who are not identified as necessarily being single or divorced, minority, elderly, between the ages of 15 and 29, or criminally involved. Instead, services are designed for grade school-aged children and their parents. Programs are sited pre-dominantly in middle-and upper-class neighborhoods where contributions from the schools augment county efforts. Another goal emphasized in the report was to secure increased funding or to broaden current service delivery through other means, including third-party payments to county-sponsored services, the use of self-help groups as a part of treatment and aftercare, and increasing both public and private funds to service providers.
There is little mention made of criminal justice system referrals to county-funded programs. One out of eight methadone and residential treatment clients' referral sources were reported to be from the criminal justice system. Most program clients were self-referred, even to these modes of treatment for which nationwide the percentage of criminal justice system-referred clients is closer to 50 percent (Hubbard et al., 1989). Commenting on this fact, "[t]he Planning Committee [of the case study county] noted that only a small percentage of the total arrests for drug-related violations were referred for treatment. This is unfortunate as the cost of treatment is lower than the cost of incarceration; and treatment is more likely to assist the person in adopting a productive, crime-free lifestyle." One of the 12 recommendations in the report was to establish 50 long-term and 50 short-term beds for incarcerated individuals in need of residential treatment, but publicly funded special services neither exist nor were planned for nonincarcerated criminally involved illicit drug users.
There were few data available from the drug abuse treatment system report or from interviews conducted with providers to identify or elaborate the linkages between the drug treatment system and the criminal justice system. For example, the drug abuse program administrator stated his
commitment to cooperate with the probation department, but there was no evidence that justice system-referred clients deserved special consideration. The administrator stated that they were evaluated as candidates for treatment along with everyone else; in his mind they were perhaps disadvantaged to the extent that they were often without funds to help pay for their care and were additionally burdened with their criminal records. His feeling was not that drug users identified by the criminal justice system did not need treatment but that he ''had his hands full" securing the money to provide the rest of the community with services. No mention was made of potential linkages with the justice system or joint funding schemes to begin to serve criminally involved illicit drug users, despite the stress their presence placed on the county's drug treatment and criminal justice systems.
A worker in one of the methadone clinics mentioned the difficulty of working with criminal justice personnel because of a lack of understanding on their part about methadone treatment. For example, her clinic writes letters verifying the dosing schedule of a client rearrested during treatment, despite the reluctance she senses on the part of the justice system to provide methadone to incarcerated offenders. (According to her, criminal justice personnel view methadone more as a drug and less as a medicine.) She also expressed the need for some of the judges and probation officers to appreciate the different types of treatment that were available as well as what could realistically be expected in terms of progress and outcome for the client-offender. She spoke of trying to explain to criminal justice system personnel, for example, why a drug-free residential setting was not an appropriate referral for a methadone maintenance client. She said that there had been a movement under way in the county for the last several years in favor of drug-free treatment.
The cut in methadone funding is clearly a reflection of the county planning committee's sense of priorities. The report stated that, although heroin addicts make up a relatively small proportion of the total drug abusers in the county, their treatment had historically consumed a substantial percentage of available county resources. To this trend may be added the increasing popularity of fee-for-service payment schemes in the county, especially for expensive services like methadone. Thus, cuts in the drug budget for publicly supported methadone slots were almost unanimously supported. This sentiment exists in contrast to another priority of the county, which is to provide services to clients with a high risk for HIV (human immunodeficiency virus) infection. Education has been identified as the means to this goal, in place of continuing the previous level of publicly supported methadone slots.
Both people who are diverted from the criminal justice system and those who are given probation as a condition of their release rely pre-
dominantly on publicly funded, community-based treatment programs. These are each discussed in turn below. The contradictions implied by the overlap of punitive with therapeutic measures as a response to drug-using offenders in this county are mentioned. They may reflect more general societal confusion regarding the handling of illicit drug users who are apprehended by the criminal justice system.
The Criminal Justice System: Processing the Offender
This section contains a description of the county's criminal justice system, its law enforcement agencies, court system, and detention facilities. It attempts to trace the progression of an offender through the system from the point of initial detention to the time of sentencing. Because the county has sole jurisdiction over offenders accused and prosecuted in its municipal courts, only those offenders who are processed in this system are discussed. The California state constitution provides the mandate for all its counties to have identical processes for such activities. Many dispositions are available for individuals whose cases are drug related. Here, the focus is on the most common pathways to drug treatment through the criminal justice system rather than the identification of every possible trail or outcome.
The county's criminal justice system is the joint enterprise of a number of interrelated institutions: (1) the police, who apprehend the offender; (2) the judiciary or court, which insures due process; (3) the jail, which detains or incarcerates the individual; (4) the public defender's office or private lawyers (or both), whose task is to defend the accused; (5) the district attorney's office, which prosecutes the accused; and (6) the judge, who determines whether prosecution is proceeding lawfully and then sentences the convicted. Of the county's total criminal justice expenditures for 1986, 54 percent went to law enforcement, 7 percent to prosecution, 3 percent to public defense, 12 percent to courts and court-related matters, and 24 percent to corrections.
The police provide protection for the citizenry, bring charges against putative offenders, and have the power of arrest. The county's chief police officer is the sheriff. The sheriff's office has police jurisdiction over all unincorporated areas of the county and 4 recently incorporated towns that contract for police services from the sheriffs office. There are 11 incorporated areas in the county with independent city police departments. In addition, a variety of special districts or local institutions have autonomous police forces: for example, the California State Police, the California Highway Patrol, community college patrols, regional district park
rangers, and railroad and other transportation authority police.
All such police have arrest power, arrest being the act of taking a putative offender into custody—that is, temporarily depriving him or her of liberty. An arrest may occur because a police officer (or a citizen) has observed an offense or has reason to suspect that someone has committed an offense, or because a warrant for arrest has been issued by the judiciary to the appropriate police department. A citizen may also be taken into temporary custody without an arrest having occurred—for example, when a person is sought for questioning about some offense and released, or when he or she is taken to the police station but the peace officer determines that there are insufficient grounds for making a criminal complaint and releases the individual.
A little more than 3 percent of all adults in the county were arrested for misdemeanor offenses in 1986, a proportion that stayed roughly equivalent in 1987 and 1988. Of the total number of adult misdemeanor arrest offenses reported by law enforcement agencies in the county in 1986, 7.9 percent were released at the police level, and misdemeanor complaints were sought in 92.1 percent of the cases. More than 16 percent of the people arrested for a misdemeanor offense were women.
The various stages of the criminal justice system through which a person must pass appear in Figure 1. The first opportunity for diversion from the system occurs during the prearrest phase. The arresting officer determines that the person in custody is in need of detoxification from drugs or alcohol, or both; California law allows for that person to be taken to a legitimate facility for detox services. However, a police officer may still lodge a complaint against a person who is suffering from an illicit drug overdose or drug-related medical problem even if they are delivered to a hospital or clinic because drug use itself constitutes a violation of the drug laws and is thus regarded as a crime. (The same is not true for alcohol intoxication because alcohol is legal.) There are scores of specific laws concerned with the use of illicit drugs and the misuse of licit drugs in the various California codes, including the Penal Code, the Health and Safety Code, the Motor Vehicle Code, and the Business and Professions Code.
Whether or not an arrest has occurred, technically speaking, a putative offender who has been deprived of liberty is detained either in a city lock-up (in one of the 11 incorporated municipalities with independent police departments) or at the main county holding facility. Currently, many misdemeanants are charged and released without being taken into custody, a procedure known as a "cite release." After being taken into custody, the citizen may be (1) booked, issued a "Notice to Appear," and then released, (2) booked, held in custody until a bail amount is set at a hearing, and then released when bail is paid, or (3) booked and held in
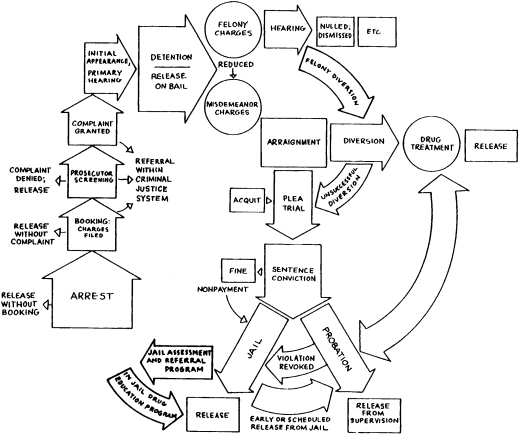
custody until arraignment. The admission of the citizen into the jail-whether he or she is held or later released—is called the "booking."
The next step in processing is arraignment, a judicial proceeding in which the accused citizen is formally charged with an offense in public court by the district attorney's office. It is the initial court appearance of a person charged with a crime. When the charges involve misdemeanor offenses the case remains in the lower, or municipal, court.
Felonies refer to all offenses punishable by imprisonment in a state prison or by death, including certain crimes charged under the Vehicle Code. Such complaints are filed in municipal courts for a preliminary hearing to determine if there is sufficient evidence to adjudicate the offense in a superior court. Even when the case is consigned to a higher court, it may be reintroduced at the lower court level if the felony charges are reduced to misdemeanor charges (indicated by arrows on Figure 1).
The county is divided into four judicial districts or municipal court jurisdictions in which all arraignments occur. The State Code requires the district attorney to evaluate information provided by the arresting officer and to decide whether to prosecute or bring to trial the person charged with or reasonably suspected of the offense. Thus, not everyone who is detained is technically arrested and booked, but everyone who is booked is arraigned. At the time of arraignment the district attorney may dismiss the charges against the defendant because of improper arrest procedures or insufficient evidence to prosecute, or if so instructed by the court.
At arraignment the defendant is given a chance to plead and to designate a private defense attorney or request that a public defender be appointed by the court. One may (1) "plead out," or plead guilty immediately, (2) defer the plea until counsel has been procured by "standing mute," which is the same as pleading not guilty; or (3) plead not guilty. In addition to dismissal, other misdemeanor cases are disposed of during arraignment through bail forfeiture, actions after pleas of guilty, or by transfer to another court. After arraignment, the court sets a date for another hearing, either to hear evidence by the prosecuting and/or defending attorneys or for sentencing, depending on the plea.
It is at this point that presentencing diversion is possible at both the felony and misdemeanor levels. In California, diversion is an official disposition that occurs prior to the trial and involves a special proceeding, governed by legislation passed in 1972. The district attorney determines when the diversion provisions apply to the defendant and must advise the defendant and his or her attorney in writing of such a decision. The eligibility of the defendant is restricted by the nature of the drug-involved offense, by what violations to certain codes have occurred, and in what combination with other offenses. By law, defendants must meet the six requirements outlined in Penal Code chapter 2.5, "Special Proceedings in
Narcotics and Drug Abuse Cases'' article 1000, subdivision (a):
-
The defendant has no conviction for any offense involving controlled substances prior to the alleged commission of the charged divertible offense.
-
The offense charged did not involve a crime of violence or threatened violence.
-
There is no evidence of a violation relating to narcotics or restricted dangerous drugs other than a violation of the sections listed in this subdivision.
-
The defendant's record does not indicate that probation or parole has ever been revoked without thereafter being completed.
-
The defendant's record does not indicate that he or she has been diverted pursuant to this chapter within five years prior to the alleged commission of the charged divertible offense.
-
The defendant has no prior felony conviction within five years prior to the alleged commission of the charged divertible offense.
Drug diversion was intended for those users of illicit drugs who are, as one probation officer said, "not immersed in the drug culture; it's for the recreational users. . . ." Illicit drug traffickers or those suspected of heavy selling activities are considered to be too far along—both in their criminal activities and in the amount of drugs they are suspected of using-to be candidates for diversion.
A defendant may attempt to qualify for diversion by self-enrolling in a treatment program, but more often the court or the defense attorney initiates the action by requesting that the district attorney begin eligibility proceedings. The case is always referred to the probation department where the defendant's suitability for education, treatment, or rehabilitation is assessed. This assessment is provided in written form and is called the presentence investigation report. Sometimes the presentence report discloses information such as prior convictions for certain offenses or a record of a failed probation that renders the defendant ineligible for diversion. All of the county's reports are handled by one section of the probation department and contain the probation officer's findings, which are presented to the court with a recommendation. The district attorney must agree to the diversion disposition, but the court makes the final determination regarding the terms of the release. The period during which further criminal proceedings against the defendant may be diverted is no less than six months and no longer than two years. Progress reports are filed by the probation department with the court no less than every six months.
Although the box marked "Diversion" in Figure 1 is the official point
at which it is noted by the court, activity toward this disposition begins soon after the arrest is made. The defense or prosecuting attorney may request continuances from the court to forestall the date of arraignment to allow time for the probation department to conduct its investigation. If the court does not deem that the defendant would benefit by diversion, however, or if the defendant does not agree to participate, the proceedings continue as in any other case. Trial may be by court or by jury; both have the power to dismiss, acquit, or convict. A conviction results in another hearing to deliver the sentence, which may include but is not limited to (1) a jail term; (2) a jail term and a fine; (3) a jail term, a fine, and probation; (4) a fine only; (5) probation only because of a suspended jail term; or (6) a jail term and probation.
Terms of incarceration may be served at the main detention facility, at a minimum security facility, or at a work furlough station. It is possible to be sentenced to a jail term without probation and to apply for it while in confinement. Terms of probation may include drug treatment. Both diversion and probation are pathways out of the criminal justice system into the drug treatment system and are considered in detail in the next section.
Diversion and Probation: Pathways to Treatment
This section focuses on pathways to treatment through the criminal justice system and the implied transfer of criminal justice functions to other social institutions such as drug treatment programs. Although they may be described as "systems," there are few clearly delineated policies that govern the overlap of criminal justice and drug treatment activities and how clients are "shared." Each system must be thought of as being its own freedom within the county, and each operates accordingly. Each has its own mandated mission, budget, hierarchy, and governing philosophy, which has relevance both internally and as it views its place in the total county system.
Diverted criminal justice "clients" and those on probation have increasingly found themselves enrolled in drug treatment facilities, outpatient programs in the community, or some alternative program (such as Narcotics Anonymous meetings or group therapy) in lieu of incarceration. The types of offenders involved in such programs may range from those arrested for possession of small amounts of controlled substances to those charged with offenses in which drugs are not officially specified as part of the offense. The latter type of offender is considered to have a problem with drugs that is specifically linked to his or her crime (e.g., shoplifting,
reckless driving, wife-battering, burglary).
Both informal and formal mechanisms allow for these alternative dispositions. Informally, private attorneys or public defenders may contact treatment centers to arrange for a possible placement prior to sentencing, thereby supporting to the court their argument for a lighter sentence. Probation officers may refer someone to a treatment agency, and a shorter probationary period may result. Sheriffs working in the jail, along with the substance abuse mental health worker, may evaluate whether those inmates already convicted are suitable for early release into a treatment program as part of probation in lieu of continued incarceration.
Operationally, probation cases and diversion cases are handled by the same officers through the same department and are subject to similar conditions. Diversion is a process of extrication from the criminal justice system; in that sense, probation is a form of diversion because it entails a less restrictive disposition than straight jail time. The main difference is that diversion occurs before sentencing and probation occurs afterward. Therefore, successful completion of the former means the record of arrest may be expunged. Probation is a sentence arising from a conviction that may come after or in lieu of jail. If it is violated, the person may be rejailed immediately as well as arraigned on the charge that precipitated the violation, which is carried over (see Figure 1 for a graphic view of this process).
Probation departments and public defender offices provide positions for resource officers who are assigned to locate alternative placements for divertees and convicted misdemeanor offenders whose problems are viewed as drug related. Pretrial drug diversion programs consist mainly of supervising an arrestees participation in a treatment program. People who have spent time in jail are sometimes released directly into a residential program in the community, with resource officers again providing the coordination.
These long-standing, informal approaches to sentencing have been supplemented in California by structured arrangements in the criminal justice system. The California Penal Code provision permits a civil procedure for the diversion of certain arrestees prior to sentencing, with local jurisdictions deciding whether and how to implement such activities (see Appendix A for the text of Penal Code section 1000). Such programs suspend prosecutorial action and eventually result in the dropping of charges if an appropriate program is completed to the court's satisfaction.
The Penal Code contains provisions that specifically prohibit the applicability of drug diversion to (1) defendants who have had prior convictions for any offense involving controlled substances; (2) defendants whose offense involved a crime of violence or threatened violence; and (3) defendants who have violated parole or probation in the past. Moreover,
diversion can be employed for only a limited number of the Penal Code violations that involve controlled substances.
Table 1 shows reported numbers of arrests by charge for drug law violators in the county during 1986, 1987, and 1988. It also provides the same information in percentages. Felony-level arrests for drug law violations account for a larger percentage of total arrests for all felony charges each year, with charges for dangerous drugs and narcotics showing the greatest increase. Misdemeanor-level arrests for all drug law violations account for only slightly more of the total misdemeanor arrests over the three years; despite the percentage of those arrested for "all other drugs" nearly doubling between 1986 and 1988. Both felony-and misdemeanor-level arrests for marijuana decreased, whereas the number of women arrested for all felony-and misdemeanor-level drug law violations increased. Felony-level arrests for drug law violations accounted for an average of 27.6 percent of all felonies over the three years; misdemeanor-level arrests for drug law violations accounted for an average of 9.3 percent of all misdemeanor arrests during that time.
In the study county for 1986, 842 people were officially diverted; in 1988, 1,786 people were officially diverted, but it is not known how many of these were diverted specifically for drug law violations. Diversion is now an option for a variety of charged offenses, including writing checks with insufficient funds, domestic violence, child abuse, and child sexual abuse, and for offenses committed by mentally retarded people. Data that differentiate among the cases are not easily accessible.
People diverted under all diversion laws, including those charged with drug law violations, become the responsibility of the probation department. Officers use the presentence report and an interview with the person to determine what sort of program is appropriate. A variety of programs are accepted by the probation department as sufficient for the conditions of release under this law, including nondrug treatment programs. Sometimes the person returns to his or her home in another jurisdiction and participates in a program outside the county while keeping in touch with the probation department. Outpatient individual or group therapy is also acceptable but is rarely used because of the cost involved. Regular participation—daily, weekly, or less often—in Narcotics Anonymous or another appropriate 12-step Anonymous group is also a standard disposition.
The majority of drug diversion clients, however, participate in the probation department's own diversion class, which is held for three hours at a time during six consecutive weeks. The curriculum of the class is didactic. A probation officer who teaches the course said some time is spent on issues surrounding illicit drug use and dependence, but the bulk of the time is spent on the legal ramifications of continued use: "We want
TABLE 1 Reported Information for Drug Law Violations by Level of Charge and Year in Number and Percentage of Adults Arrested
|
|
1986 |
1987 |
1988 |
|||
|
Level of Charges |
No. |
% |
No. |
% |
No. |
% |
|
Felony-Level Charges |
||||||
|
Arrests for marijuana |
248 |
123 |
174 |
7.9 |
213 |
75 |
|
Arrests for dangerous drugs |
596 |
29.7 |
688 |
31.2 |
813 |
28.8 |
|
Arrests for narcotics |
1,143 |
56.9 |
1313 |
59.6 |
1,761 |
62.4 |
|
Arrests for all other drugs |
21 |
1.0 |
28 |
13 |
32 |
1.1 |
|
Male arrests for all drug law violations |
1,673 |
83.3 |
1,774 |
80.5 |
2,270 |
80.5 |
|
Female arrests for all drug law violations |
335 |
16.7 |
429 |
19.5 |
549 |
19.5 |
|
Total arrests for all drug law violations |
2,008 |
26.6 |
2,203 |
26.8 |
2,819 |
29.3 |
|
Total arrests for all charges |
7,557 |
23.9 |
8,215 |
24.7 |
9,603 |
28.4 |
|
Misdemeanor-Level Charges |
||||||
|
Arrests for marijuana |
365 |
16.0 |
374 |
18.2 |
369 |
14.7 |
|
Arrests for glue sniffing |
7 |
.993 |
6 |
.003 |
3 |
.001 |
|
Arrests for selling/trafficking |
1,561 |
68.4 |
1,248 |
60.6 |
1,353 |
54.0 |
|
Arrests for all other drugs |
349 |
15.3 |
430 |
20.9 |
778 |
31.1 |
|
Male arrests for all drug law violations |
1,995 |
87.4 |
1,789 |
86.9 |
2,170 |
86.7 |
|
Female arrests for all drug law violations |
287 |
12.6 |
269 |
13.1 |
333 |
13.3 |
|
Total arrests for all drug law violations |
2,282 |
9.4 |
2,058 |
8.2 |
2,503 |
10.4 |
|
Total arrests for all charges |
24,063 |
76.1 |
24,990 |
75.2 |
24,154 |
71.5 |
|
Felony-and Misdemeanor-Level Charges |
||||||
|
Total arrests for all drug law violations |
3,955 |
13.5 |
4,261 |
12.8 |
5,322 |
15.7 |
|
Total arrests for all charges |
31,620 |
100.0 |
33,205 |
100.0 |
33,757 |
100.0 |
|
Source: State of California Department of Justice, Sacramento, Calif., 1986, 1987, and 1988. |
||||||
to make sure they have the information about what to expect if they get arrested again, so they can't say they didn't know any better two times in a row. Even drug offenders are aware of accountability; they already have a degree of responsibility because they qualified for the program and have shown up for the class. We try to emphasize that they will have to take full responsibility for their actions if they continue using and get caught again."
The official procedures and actions of drug diversion programs are
not always the same as the programs' unofficial procedures and functions. In practice, the official provisions of the law are not always followed to the letter. Several probation department workers spoke of diverted cases that were more serious than section 1000 of the Penal Code allows. The language of the statute is imprecise (see section 1000.2); to leave terms like ''eligibility" and "suitability" undefined and unqualified gives discretionary power to the courts, the district attorney and public defenders, and the probation department.
Diversion may also be viewed as a set of rigidly stipulated concessions on the part of the court in the interest of justice. Cases involving first-time offenders on drug-related misdemeanor charges are often seen in the court; in these cases, diversionary proceedings were enacted to redirect the system's efforts to treatment rather than punishment. Sometimes, too, the chance for a conviction is unlikely owing to shaky evidence or improper arrest procedures. At other times the court may wish to retain some control without continuing the adjudication process by identifying the defendant for diversion and carefully outlining the conditions surrounding release under this provision.
Diversion allows the case to be transferred out of overcrowded courts and jails to the probation department and preferably to the treatment system. The defendant is given an opportunity to escape incarceration and erase a mark in his or her criminal record. The defense attorney can "get the client off" while working to make treatment available. Both private attorneys and public defenders are likely to strategically raise the defendant's drug problem during the adjudication process. Their aim is to have the charges dropped (suspended) in the interest of justice, to have their client diverted instead of prosecuted, or at least to obtain a lighter sentence. Some sources called drug diversion a "tidy compromise mechanism" and a "deal struck in everyone's best interest" Nevertheless, a senior attorney from the public defender's office raised some grave doubts that he and other members of the staff had about the process of diversion into treatment. His reservations have come to outweigh his belief in the viability of the process, especially for the offender. He had several reasons for this, which he used to explain his office's reticence to support diversion for drug law violators.
His first concern is with the selection criteria used to establish eligibility. Beyond statutory considerations, the report compiled by the probation department is, in his eyes, neither thorough nor fair (see Division of Probation, Administrative Office of the United States Courts [1978]; McPike [1978]; Weissman [1979]; and the Bureau of Justice Assistance [1988] for discussions of the presentence report that echo the views of the public defender from a broader perspective). The presentence report is used by the court to decide the fate of the accused, and it always
becomes part of the person's permanent record. It contains explicit discussions of the individual's licit and illicit drug (and alcohol) use. The descriptions of usage patterns, along with the conclusions based on them, are made by someone who has had only brief contact with the accused and who has had little if any formal training in diagnosing the severity of drug involvement or dependence. Understandably, many of the comments made to establish the nature of the accused's drug use are directly related to criminal justice considerations (like prior arrest history) and do not make use of more objective medical or behavioral criteria. Discerning dependence, making the diagnosis, and then matching the client with a punishment or a treatment, or both, is difficult even for someone with clinical training and more time in which to examine the client and explore treatment options.
A related concern involves the judgment made in the presentence investigative report regarding what constitutes a support system. This factor is most often second only to criminal record in deciding whether a person will go to jail or to treatment. The county's public defender talked about this issue at some length. He said he felt the probation officer's judgments about who and what would help the person recover, if treatment were to be provided, were arbitrary and speculative. What is generally recognized by the probation department and by the court as legitimate support in the community is both class and culturally bound. It becomes a real challenge for the public defender to legitimize the support systems of clients of lower socioeconomic status and racial minority clients. Yet many of the clients provided with public defender assistance are from ethnic subcultures that contain disproportionate numbers of individuals living below the poverty line.
Presentence reports are often arbitrary yet predictable documents (Division of Probation, Administrative Office of the United States Courts, 1978; Feeley, 1983). Being middle class, from a traditional intact family, and having some education and employment positively influences the presentence report. Such people are more likely to be considered a good candidate for diversion. Someone with neither a stable family nor prospects for productive employment is at a substantial disadvantage. Chances for alternative sentencing are significantly reduced from the outset.
The public defender also noted that the current treatment system cannot begin to provide all the elements necessary for behavioral change. Literacy skills, job training, employment, and a residential arrangement that allows for long-term sheltered living along with drug treatment are simply not provided. Yet without such bolsters to enhance an individual's support during treatment, the likelihood of sustained recovery is reduced. In his opinion the result is that minorities are less likely to be placed in
treatment settings and are instead incarcerated, whereas whites are more likely to receive treatment in addition to or instead of incarceration.
Most compelling was this public defender's view that to struggle for diversionary dispositions for his clients was to "set them up for failure." In this county, diversion either means loose supervision by a severely understaffed probation department or participation in a rigorous drug-free residential program whose high attrition rate speaks to its difficulty. Very few clients sent to either a therapeutic community or to the probation department succeed—so few, in fact, that the public defender, in a personal interview, stated that he feels he can serve them better by convincing them to spend a little time in jail instead:
The success rate is low. . . when the judge sees the person return with another string of offenses he is predisposed to behave more harshly. Someone who has violated the trust that the court has placed on them by mandating treatment in lieu of incarceration, who then commits more crime, is likely to be prosecuted and sentenced with a vengeance. These guys are viewed as being not only criminals-and recidivists at that-what's worse is that they are treatment failures who carelessly used up their one chance for a free bite of the apple along with the indulgence of the court.
The public defender feels his clients are better served when he bargains with the judge for a reduced sentence instead of diversion to community supervision. Then he spends considerable time trying to convince his client to accept probation and 120 days in jail rather than probation and 30 days in treatment. His views are reflected in the conduct of his fellow public defenders as well who join him in trying to avoid placing clients in the treatment system where their chances for success are small.
There are so many failures because any treatment only works when the person is ready for it and wants to change. Our office [the public defender's] tries less than it used to for alternative dispositions; there are too many probation violators who we just see again and there is less of a need than there was in the seventies, say, to assuage our own guilt and try to get people into treatment when it's only going to make matters worse.
Regardless of the type of class or program in which a drug-diverted person participates, he or she must stay in regular contact with the probation officer. Several individuals in the probation department verified that drug diversion cases receive the minimum amount of supervision. Probation officers classify their cases according to the amount of danger they pose to the community, and set the level of supervision accordingly.
Drug diversion clients are thought to present the lowest amount or minimum risk to the community. As a result, regular contact becomes once a month or less often and may not involve a visit or a phone call. Often the client is only required to send a postcard (known as a "mailer") to the probation officer once a month.
Drug divertees are not sent to any special probation officer who exclusively handles drug law violators; they are included in a regular caseload of people on parole and probation. There are 70 deputies who each oversee an average of 185 cases per month; at present the county has an active adult probation caseload of more than 13,000. The probation officer is mandated by the court to submit progress reports on every person no less than once every six months, but everyone in the criminal justice system considers these documents to be meaningless. Unless the person is rearrested or does something else that is extreme enough to require an office visit or increased surveillance, the officer retains little knowledge of the client's behavior.
Probation
Probation technically means that the imposition or execution of a sentence is suspended and an order issued for conditional and revocable release in the community under the supervision of the probation department. More than 30 pages of the Penal Code are devoted to the laws governing probation; space prohibits their inclusion or a detailed discussion of them here. Briefly, probation may not be applied to certain cases involving specific violations of the State Code unless it is shown that "justice will better be served" through granting probation; it must be requested by the defendant or applied for by the inmate and is subject to the approval of the court during a formal hearing for which a report and recommendation are filed by the probation department; probation is revocable if the conditions stipulated by the court are violated; it involves different levels of supervision in the community and may include a mandate to undergo drug treatment; and the level of supervision and type of treatment are set by the resource officer who is assigned to the case.
If a defendant is convicted and the sentence involves probation without a jail term, the defendant is ordered to contact the probation office. The case is reviewed by a probation officer who acts as a case manager. The client's history is assessed, and a plan is developed that allows for retributive payment and/or finding a treatment program that will accept the client and provide appropriate services. If the treatment site is not residential, the client is less easily supervised, and the conditions of the probation are more difficult to enforce.
As deputies, probation officers have the power to rearrest people at any time on the charge of violation of probation. Recently, however, the department lost its main form of detection and enforcement, the power to subject people to urinary screens. Some officers feel that it is difficult to monitor a person's behavior under minimum supervision without such a surprise tactic. Others are less preoccupied with the detection of drug use and more concerned with how to prove in a court that the terms of diversion or probation have been violated if they decide to turn someone in.
The ritual of contacts that establishes rapport between the offender and the probation officer often allows violations to escape detection or, if they are detected, to be overlooked. The relationship may resemble one between a caseworker and a client, or it may be closer to what happens between a police officer and a suspect. It depends on the two personalities, the attitude and level of commitment of the client, the current and past offense record, and the progress made along the way. A supervisor at the probation department said that increasing caseloads almost prohibit a true therapeutic relationship from developing; the probation officer is most often seen as "the man, the one who can lock you up."
Probation is viewed by probation officers as a period of proving. The court designs the conditions of the release and sets up the legal relationship between itself and the offender. The offender must then prove worthy of the trust of the court. The tether that the probation officer maintains on his client can be pulled and tightened, or modified and reduced. Good behavior is measured in part by the willingness of the client to honor the terms of the probation: to keep appointments, to gather signatures to prove attendance at Narcotics Anonymous meetings, to remember to call in on schedule.
In exceptional cases, a person is turned back to the court for gross misconduct: probation may be violated or diversion revoked and proceedings restarted toward conviction (see Figure 1). The department had no data on how often violation occurs generally across all cases, much less how often it occurs for drug-involved offenders. One contact spoke of the increasing frequency with which desperate crack-cocaine users are pleading with their probation officers to "violate" them and send them back to jail because they cannot stop using even while participating in outpatient treatment. To move people in that condition to protective custody is considered a viable treatment intervention by probation department supervisors and some users.
Several probation officers reported that they were not encouraged in this county to violate their charges unless circumstances were so extreme and clear that incarceration was justifiable to the supervisor, who must
then make the case to the jailer. The main detention facility fluctuates between being 200 and 300 percent overoccupied; the county's unofficial policy is to disregard many probation violations that do not directly threaten the safety of the community. It is commonly believed in the department that enough of the people who are on probation and persist in illicit activities are apprehended by the police apart from any action by the probation officer.
The jail is so overcrowded that compulsive use of crack-cocaine leading to a plea for intense and restricted supervision is not always a good enough reason to reincarcerate an individual. The supervisor stated that unless other crimes were being committed where the person was caught and arrested (besides or in addition to the use of crack), jail was not an option. He said that the amount of paperwork needed and the time lost to process the violation and get the person booked into jail were not worth the trouble unless other crimes could make the case more compelling.
It should be noted that the above was not reported in a way that implied the probation officers were shirking their responsibilities. Throughout the interviews with probation department personnel, several factors were mentioned repeatedly: the heavy caseloads of the officers; the crowded conditions of the jail; the fact that, in the county lock-up, people are serving only 30 percent of their sentences; and the lack of effective treatment for crack and little available treatment for other drug-involved offenders.
Despite the heavy caseloads of the officers and the lack of adequate treatment slots, some clients who are referred by the criminal justice system do get to treatment. Special probation workers known as resource officers are responsible for this function, along with the placement of all other types of offenders. State and local laws also allow probationers to be placed in facilities outside the jurisdiction of the court. The department had no data available on the number of cases referred to treatment out of the state or out of the county, or the percentage of the total number of clients sent to treatment anywhere that these referrals constitute. (See Stitzer and McCaul [1987] for a discussion of criminal justice interventions and the use of different treatment modalities for their clients.)
Resource officers feel constricted by the drug abuse treatment system and speak of a lack of services for all county residents in general and for most of their clients in particular. There is an acute shortage of the intensely supervised modalities that are more appropriate for some criminal justice system clients. The probation department's resource officers also feel they are in direct competition with the sheriffs office for bed space in residential settings, the preferred type of treatment for criminal justice
system clients. Moreover, the current emphasis in the county is to favor paying clients and to favor clients who are judged to be motivated to recover. In this county a mandate to drug treatment from the criminal justice system lacks effectiveness because the treatment system has its pick of clients and criminal justice system clients appear to be close to the bottom of the barrel. In addition, resource officers do not want to alienate the service providers by pushing too hard. They seemed to understand that a balance had been struck that allowed them to refer a certain unspecified number of clients but that they could not expect to enjoy unlimited placement of their clients, given the current condition of the treatment system.
Another resource officer described the dilemma facing the criminal justice system in a slightly different way. He said that if clients can be placed on probation for drug law violations and drug-related charges (and thus are not considered a serious threat to the community), the level of supervision they receive is minimal—once per month or less. This schedule does not allow the probation officer to offer enough support or supervision to the offender, especially if the offender's treatment has ended or if it consists solely of attendance at 12-step groups. This officer said that trying to stay off drugs and out of trouble is difficult even when someone is actively engaged in treatment; it is even harder when the offender returns to the community without a regular, enforced schedule of contacts with the probation department. It was clear that this probation officer was equally as interested in offering his clients an opportunity to ''check in with someone," out of genuine concern for them, as he was in monitoring their behavior from a purely disciplinary posture.
In substituting treatment for criminal justice action, the police, prosecutor, court, and corrections system are using a legal basis to mitigate increasing fiscal problems by reducing both court calendars and overcrowding in incarcerative facilities. The rationale to replace traditional with alternative dispositions is therapeutic, but the system's severe resource limitations on delivering services defeat the value of this process to both offenders and the community. It is difficult to know when a decision of diversion or probation handed down "in the interest of justice" is really meant to reduce jail overcrowding, to release impacted courts, or, almost incidentally, to benefit the person by prudently matching the client with the most appropriate available treatment modality (Mosher, 1983).
Occasionally a probation officer is able to place one of his clients in a drug treatment program and arrange for the county to pay for the service. Evidence is mixed in this county that the criminal justice-drug treatment nexus is expanding; it appears that the shortage of drug treatment system services is condensing the flow of clients from the criminal justice system. Yet the number of those who are arrested on drug law
violations or are otherwise drug involved—and who might benefit from drug treatment services—continues to increase. The judicial system, whether driven by pragmatic concerns with caseflow or by humane considerations to provide treatment, has allowed alternatives to adjudication and incarceration to become formal mechanisms. It appears that most offenders are considered for diversion or, once convicted, for early release and probation simply because of the limits of the detention facility.
In fact, the number of drug cases flowing into the courts has sparked an innovative program on the part of the county clerk administrator. This office oversees the caseflow of all the county-level courts, assuring that each legal procedure involving every defendant and every case proceeds in a timely manner consistent with the law. A pilot program that has been in operation for a year directs a large portion of its "petty theft with priors" and misdemeanor drug cases to an early disposition track or calendar. The program compiles the defendant's prior arrest record, open and closed conviction and probation records, and all pending charges into a file that is reviewed by the district attorney, the defense attorney, and the judge. The defendant is offered a sentence that can be refused; a refusal returns the defendant and the case to normal court proceedings.
A representative from that office said that "the defendant is offered a sweeter deal at that stage; everyone is interested in compromise in the name of reducing the burden of cases in the court." The participants in this pilot program are all multiple-case defendants; combining pending cases and disposing of them in one court procedure accelerates the adjudication process. Although presumably some of the cases have involved sentences that included probation and potentially referrals to treatment, no data were available. This program is further evidence that the judicial system is going to great lengths to find ways of relieving court calendars. It is another place that linkages could occur between the criminal justice and drug treatment systems.
Diversion, probation, and early disposition all involve cooperation and coordination among representatives from both systems. Unfortunately, the resources available to probation officers and treatment providers are not commensurate with the increased demands placed on them by the criminal justice system and by police arrest activities. Even so, the percentage of publicly funded residential treatment clients who are referred by the criminal justice system has risen from 10 percent five years ago to approximately 25 percent today (anecdotal estimate derived from an interview with a criminal justice system supervisor). Data are not available that indicate the source of referral for clients of all publicly funded drug treatment programs.
Moreover, it is possible that the choice of participation in drug services represents more than simply a desire—on the part of the client or
on the part of the system—to get into treatment. If a defendant can argue that his or her crime was in some sense "caused" by drugs, then the appropriate action under the prevailing disease concept of addiction is treatment rather than criminal punishment. Speiglman and Weisner (1982:9) stated this clearly when they argued that "[b]arriers between the drug treatment and criminal justice structures give way under the weight of reasonable treatment needs, pressures to retain elements of social control while lightening correctional caseloads, defense team maneuvers, and efforts by local officials and treatment agencies to strengthen their economies by recruiting new clients or transferring costs."
The ensuing entanglement of drug treatment and criminal justice systems is thus partially clarified by a consideration of court-related concerns. The criminal justice system is faced with the problems of having its population increasingly identified as drug related, both in the courtroom and in its incarceration facilities. At the same time a tendency is visible on the part of the criminal justice system to allow drug-involved "clients" to escape back into the community by seeking treatment as a part of their official justice system disposition through diversion and probation programs. In part this tendency is due to tremendous court overload and a willingness to consider treatment in lieu of punishment. But even at the sentencing stage, probation decisions are crucial. Mosher (1983:23) calls the mechanisms of diversion and probation an "escape valve in a system that actually incarcerates a very small proportion of all criminal offenders."
The Drug Abuse Treatment System and Inmates
A recent study (commissioned by the county's drug advisory board) stated that, of people incarcerated in the main county detention facility during three months in the spring of 1987, 48 percent were charged with a drug or alcohol offense or admitted that they had a problem with drugs or alcohol (or both). Among the total number of inmates incarcerated at that time, 20 percent were charged with a drug law violation. Of those who did not admit to drug use, 38 percent were arrested on a drug charge. Nearly 75 percent of the inmates who were known by the staff to have a drug problem were male; half were between 18 and 29 years of age, and about 42 percent were in the 30- to 39-year-old age group.
Black males constituted the largest racial group in jail; they were incarcerated at six times the rate of black females. Blacks are over-represented in county arrest data, and a disproportionate number of blacks—39 percent—are incarcerated and report drug use. Tables 2a and 2b show arrest data for drug law violators by ethnicity for 1986, 1987, and 1988 in the case study county. Although the rate of felony-level arrests
for narcotics among Hispanics decreased over these three years, the rates for both blacks and whites increased. By 1989, blacks who were arrested and charged with narcotics law violations accounted for more than 62 percent of all those arrested for drug law violations whereas for whites, narcotics charges accounted for only 15 percent of all drug law violations. Although the rate of whites arrested for all felony-level drug violations decreased (over the same three years) to about 44 percent by 1989, the rate of blacks arrested for all felony-level drug violations increased in the same time and by 1988 accounted for 48 percent of all felony-level drug law violations. (Blacks account for only 10 percent of the county's total population while whites make up 85 percent.)
The county drug administrator and other officials consider these figures on drug-involved arrestees to be quite low, in part because other offenders are often drug involved but charged with other violations. Without a specific study of arrestees, it is not possible to know how many are involved with drugs and how many are or are not specifically being identified as drug violators. Some of those interviewed in the county systems estimate that up to 90 percent of all inmates had drug and alcohol problems that were related to their offense.
A jail brochure states that the main detention facility's substance abuse assessment and referral program is "designed to identify and to work with the few substance abusing inmates who have the best chance of success in treatment and rehabilitation." There is one program administrator who oversees all mental health programs including drug and alcohol abuse, and one substance abuse outreach worker for more than 980 inmates. Only a portion of the people who might have a legitimate drug problem and be interested in undergoing an evaluation can be assessed for possible treatment.
The only form of drug treatment per se in jail is the weekly volunteer-facilitated Narcotics Anonymous meetings for any inmate who wishes to attend. There are beds designated for inmates with mental health (including substance abuse) problems; these are filled with people who have been diagnosed as schizophrenic or who suffer from extreme cases of combined mental health and substance abuse problems (termed "dual diagnosis"). The supervisor of the Mental Health and Substance Abuse Program in the detention facility estimated that more than 80 percent of the identified and actively open cases that receive mental health services also suffer from drug problems. The program in the jail is understaffed, employing six clinicians (only one of whom was a designated substance abuse worker) whose primary responsibility is to perform intake mental health screenings on every person booked at the facility (more than
TABLE 2a Reported Information for Drug Law Violations by Ethnic Group, Level of Charge, and Year in Numbers of Adults Arrested
|
|
Adult Total |
White Total |
Hispanic Total |
Black Total |
Other Total |
||||||||||
|
Level of Charges |
1986 |
1987 |
1988 |
1986 |
1987 |
1988 |
1986 |
1987 |
1988 |
1986 |
1987 |
1988 |
1986 |
1987 |
1988 |
|
Felony Level Drug |
|
||||||||||||||
|
Law Violations |
|
||||||||||||||
|
Narcotics |
1,143 |
1,313 |
1,761 |
293 |
383 |
440 |
81 |
86 |
93 |
743 |
826 |
1,206 |
26 |
19 |
22 |
|
Marijuana |
248 |
174 |
213 |
98 |
95 |
112 |
7 |
9 |
11 |
137 |
70 |
89 |
9 |
0 |
1 |
|
Dangerous drugs |
596 |
688 |
813 |
512 |
594 |
703 |
37 |
49 |
54 |
37 |
37 |
48 |
10 |
8 |
8 |
|
Other drugs |
21 |
28 |
32 |
15 |
21 |
19 |
0 |
1 |
2 |
6 |
10 |
6 |
0 |
0 |
1 |
|
Total drug violations |
2,008 |
2,203 |
2,819 |
918 |
1,092 |
1,274 |
125 |
145 |
160 |
923 |
943 |
1,353 |
45 |
27 |
32 |
|
Total all felonies |
7,557 |
8,215 |
9,603 |
3,484 |
3,801 |
4,249 |
555 |
618 |
795 |
3,326 |
3,611 |
4,311 |
192 |
185 |
248 |
|
Misdemeanor-Level Drug |
|
||||||||||||||
|
Law Violations |
|
||||||||||||||
|
Marijuana |
365 |
374 |
369 |
236 |
268 |
265 |
14 |
26 |
28 |
95 |
75 |
67 |
20 |
5 |
9 |
|
glue sniffing |
7 |
6 |
3 |
2 |
6 |
3 |
4 |
0 |
0 |
1 |
0 |
0 |
1 |
0 |
0 |
|
Selling/Trafficking |
1,561 |
1,248 |
1,353 |
1,224 |
950 |
899 |
120 |
90 |
101 |
194 |
188 |
318 |
23 |
20 |
35 |
|
Other drugs |
349 |
430 |
778 |
200 |
278 |
552 |
28 |
35 |
61 |
107 |
116 |
189 |
14 |
1 |
6 |
|
Total drug violations |
2,282 |
2,058 |
2,503 |
1,662 |
1,502 |
1,719 |
166 |
151 |
190 |
397 |
379 |
574 |
58 |
26 |
50 |
|
Total all misdemeanors |
24,063 |
24,990 |
24,154 |
15,586 |
15,777 |
15,299 |
2,374 |
2,614 |
2,603 |
5,224 |
5,938 |
5,501 |
874 |
661 |
751 |
|
Felony- and Misdemeanor- |
|
||||||||||||||
|
Level Drug Violations |
4,290 |
4,261 |
5,322 |
2,580 |
2,594 |
2,993 |
291 |
296 |
350 |
1,320 |
1,322 |
1,927 |
103 |
53 |
82 |
|
All Felony and Misdemeanor- |
|
||||||||||||||
|
Level Charges |
31,620 |
33,205 |
33,757 |
19,070 |
19,578 |
19,548 |
2,929 |
3,232 |
3,398 |
8,550 |
9,549 |
9,812 |
1,066 |
846 |
999 |
|
Source: Slate of California Department of Justice, Sacramento, Calif., 1986, 1987, and 1988. |
|||||||||||||||
TABLE 2b Reported Information for Drug Law Violations by Ethnic Group, Level of Charge, and Year in Percentages of Adults Arrested
1,700 per month).
Inmates may not refer themselves for assessment by the substance abuse mental health worker. The caseworker spends the majority of his or her time complying with requests from the court, the defense attorneys, and the sheriffs department to evaluate inmates for early release. The inmate's perceived danger to the community, history of drug and crime involvement, and potential for successful completion of a treatment program are the main variables addressed in caseworker reports. If inmates manage to have an informal contact with the caseworker, they are advised to apply for probation or to ask their attorney or public defender to make a formal request for referral to the substance abuse office. This approach is the only guarantee that their drug problem and case will be assessed, albeit none too soon. Once incarcerated, probation is the only pathway to treatment.
The caseworker cooperates with probation officers, attorneys, judges, and treatment providers to place prescreened inmates from the jail directly into acceptable substance abuse treatment programs. Although the ''best" placements are thought to be direct transfers from the structure of incarceration to the structure of long-term residential treatment facilities, there are very few of these types of slots available to inmates. According to the caseworker, this is partially because there are not enough slots to meet the demand in the community at large and in part because of the preference on the part of providers not to take convicts as clients.
Sources revealed a discrepancy between the goals of detention facility staff and the goals of treatment providers. The former work to reduce overcrowding in the jail by getting as many people out into the community for treatment as possible without seriously endangering the public. Treatment providers prefer to admit only those people as clients whose case histories and circumstances match the type of setting they can locate.
There is a special sheriffs parole office inside the main detention facility whose staff look for inmates to propose as candidates for early release. This approach also involves deputy sheriff supervision of treatment but through a special office. One official claims that their guiding principle, to reduce jail crowding, may not reflect the inmate's best interest. The office sometimes utilizes resources for treatment in the community that may not be up to the standards followed by the probation department but that meet the general criteria—and get the person out of jail. According to a senior probation department worker, the clients referred to treatment by the sheriffs parole office have "the worst record of failure anywhere in the system." Some people understand this to mean that the officers do not always act as judiciously as they might; however, there is only anecdotal information on this point and no official data evaluating treatment outcomes of the sheriffs paroled clients versus other
criminal justice system-and nonjustice system-referred offenders.
Inmates may receive medical supervision for a primary medical condition that drugs have caused or recent withdrawal has exacerbated, but there is no medical staff assigned to provide drug abuse treatment services inside the jail. Those people who go into opioid withdrawal after admission into jail are offered methadone as part of a detoxification program administered through the medical services division of the main detention facility. Inmates who are concurrently enrolled in a community methadone detox or maintenance program when they become detainees are given complimentary doses while incarcerated without having to wait until withdrawal begins. The jail's medical staff obtain the individual's dosing schedule (frequency, amount, and rate of dose reduction) and medical case history from the community methadone program staff. The detention facility will then dose the individual for the remainder of their detox schedule (up to 21 days) and may administer maintenance-level doses for up to 60 days pending case disposition.
If a woman is jailed and found to be pregnant and opioid dependent during the mandatory medical examination, a decision is made by the medical staff as to whether to begin a schedule of methadone maintenance doses. The criteria for this action are the trimester of pregnancy and the level of danger detoxification would pose to her fetus. The final decision is made by the medical staff rather than the woman.
Perhaps the most prominent program concerned with substance abuse in the county detention facility is not a treatment program but an education program originally begun to deal with repeat-offender drunk drivers. It was quickly expanded to accommodate all kinds of poly-substance abusers and is run solely out of the minimum security facility, which is set apart from the main detention facility. Funded by the state Department of Education, the project is a voluntary, in-custody, residential education program for which participants obtain school credit. As with any other education program, inmates can apply their time in the program toward reduction of the term of their sentence. In addition, the program offers other privileges: inmates enjoy less crowded and newer barracks, better televisions, pass privileges, and the opportunity for family counseling sessions.
Inmates may apply for the program with or without a referral from their attorney. Interested inmates complete an application form, thereby alerting case managers to work with the sheriffs classification officers to determine at what point in the adjudication process the inmate may be admitted. More often, inmates begin the drug education program after they have already been placed at the main facility, having heard about it from other inmates rather than through a judicial or jail officer. Offenders on methadone are not eligible because medical services are available only at
the main facility and the education program is only offered at one medium- and one low-level security facility. Drug-involved offenders who committed serious crimes may not be housed in such facilities and thus cannot participate. When and if accepted, inmates are transferred from the main facility to take part in the program while serving their sentence in less restricted surroundings.
There is a feeling among jail staff that participation in the drug education program is commonly used by inmates who need to bolster their case for early release or probation by demonstrating good intentions and the right attitude. Nevertheless, it is a popular program and has received broad support for bringing information about drugs and alcohol to the incarcerated. The project quadrupled in size in 1988 to accommodate 120 inmates out of a total of approximately 1,000 in the minimum security facility. It must be borne in mind, however, that it is strictly an education program and not drug treatment. Part of the program involves education about substance abuse, but the bulk of the curriculum consists of cooperative learning activities aimed at increasing detainees' postrelease employability. The program is funded with state Department of Education dollars, and its content is not required to reflect the goals of drug treatment.
There are intrinsic differences in the philosophies of drug treatment and educational programs: rehabilitative treatment usually means theoretically based programs stressing a continuum of care that includes detailed aftercare plans once a person is released, concepts that education does not embrace. Treatment involves staff who are more highly trained than educators, small-group interaction, and individual therapy conducted by credentialed professionals. Educational classes may provide information, but it is not at all clear that information alone produces—much less sustains—lasting behavioral changes.
Educational programs of this sort are based on learning by repetition, which is thought by some to be not only superficial but either too easy or too hard a way to demonstrate competence: "You go to a class, you take a test, you get your pass for the weekend." As one of the criminal justice system contacts puts it, "It's an easy game to fake and to play, unless you can't read to begin with, and then it's just as unfair as everything else."
The jail's education program provides no coordinated services for reentry or links to community treatment resources because the project has no formal connection with the drug treatment system. In addition, no case management may be done to help prevent inmates from reoffending for drug-related or nondrug-related reasons. The project was originally conceived and sponsored through the cooperative efforts of the sheriffs office, the state and county offices of education, and the county health/ mental health/substance abuse program staff. It was originally designed in
part to reduce jail overcrowding. Inmates who successfully completed the program were to be prime candidates for early release into residential treatment facilities.
Now, because of an ill-defined rift between the state Department of Education and the local detention facility Substance Abuse Program officials, the two no longer cooperate to coordinate service delivery on the outside with program participation on the inside. The friction has something to do with program funding: the former's budgetary allotment is based on "average daily attendance" and comes directly from the state Department of Education; the latter's is meager by comparison and comes from criminal justice system monies. Thus, the jail's substance abuse division must compete with other more detention-and control-oriented agendas for its survival in a system that is already vastly overspending. The result has been fragmentation and the loss of an opportunity to administer a comprehensive, uninterrupted program of education plus treatment that may be continued once the offender is back in the community.
Case Study Conclusions
This preliminary examination of the interplay between one county's criminal justice and drug treatment systems reveals that there are opportunities at several stages in the adjudication process for transfer out of the former and into the latter. Attempts to secure presentencing diversion may be made at any point after an offender is "booked," but they are officially recorded in the court's files following arraignment. Diversion out of the criminal justice system is based on special provisions in the Penal Code for drug-involved offenders. The defendant maintains the right to choose to reject the diversionary proceedings in favor of adjudication for the offense. The terms of the diversion are mandated by the court and include treatment and supervision by the probation department. Divertees who fail to conform to the conditions of their release may be rearraigned for the original offense as well as for any additional offense.
If diversion is not possible and the person is convicted, the defense attorney may argue for a light sentence, often requesting probation in lieu of jail or a shorter jail term with probation following release. The terms of the sentence are set by the court, based in part on recommendations from the prosecuting attorney; reports from the probation department evaluating the person's perceived threat to the community and disposition toward treatment, if applicable; and the offender's prior arrest and conviction history. Often the person serves a partial sentence in jail, applies for probation, and, if probation is granted, is released early into
the community to be supervised by the probation department. Again, these decisions are made by the court with recommendations from jail staff, both sheriffs and substance abuse workers, with an accompanying report from the probation department. The probation department may make a recommendation that early release be denied based on an evaluation of the person's suitability for community-based treatment. Probationary procedures are also regulated by provisions in the Penal Code.
Few attempts have been made at a county level to study the process that governs transfers between the criminal justice and drug treatment systems and clarifies their relationship as social institutions. The law is distinct in its stipulations concerning diversion and probation proceedings and about the roles of the key players in these activities. It seems less clear that the original intent of such laws, that is, to grant drug-involved offenders a chance to be ''treated" rather than penalized for their actions, is what currently drives the process of transfer.
Both diversion and probation provide opportunities to reduce court and jail overcrowding without severing the ties of supervision. Mandated treatment in the community overseen by a probation officer is a lesser form of social control than incarceration. It is less expensive and, in the study county, more uneven. Yet the integrity and viability of these dispositions as "justice being served" is threatened because of the increasingly large number of adults who qualify for them, in combination with one or more of the following:
-
mismatches between what the law stipulates and what often occurs, resulting from operational pressures on an overcrowded system and prejudicial decision-making that may involve class and racial cleavages;
-
the ambiguity that characterizes the seques between the criminal justice and drug treatment systems and the means by which people become involved in one system after initial referral to the other, both of which hinder the system's capacity for planning or evaluation activities;
-
aggregate mismatches between what the criminal justice system is intended to manage and what the treatment system is designed to process, which requires close coordination, case-by-case matching, and mechanisms for evaluation;
-
the absence of an authentic drug treatment program for inmates that is appropriate for a large population diversified by race, gender, age, literacy skills, education, family background, and patterns of drug and alcohol use;
-
the dearth of suitable programs in the community that can accommodate the treatment and rehabilitation needs of an undeniably large group of drug users living in the county—those who have interacted
-
with the criminal justice system-who have committed different kinds of offenses and have different types of drug problems, as well as the shortage of treatment programs sensitive to the gender and cultural backgrounds of drug-involved offenders;
-
the lack of coordination between jail and community so as to offer a continuum of services and supervision;
-
the lack of administrative support for coordination and follow-through between criminal justice supervision and treatment agencies, which is especially subject to breakdown when caseloads are high on either or both sides and the climate is competitive because of funding shortages;
-
the low level of supervision given to their cases by probation officers; and
-
the overall lack of secure funding in either the criminal justice or the drug treatment systems for mutually supported programs or program components that have as an explicit goal a comprehensive model of working together with an offender, sharing resources and contacts both in the jail and in the community while respecting each other's domain.
A relatively small number of criminally involved drug abusers in this county are actually mandated from the criminal justice system, and to the treatment system, and such low diversion rates suggest that diversion to treatment does not realize its full potential as an alternative strategy. This underuse is tied to the scarcity of treatment resources; an interview with the director of the detention facility mental health and substance abuse services revealed that there have been no new beds for inpatient care added in the county for 10 years. The resource officers in the probation department can neither place their clients in suitable programs nor provide the level of supervision necessary to monitor their clients effectively. Until additional treatment services are funded, the potential opportunity to positively affect the lives of criminally involved drug abusers by referrals out of the criminal justice system and into drug treatment will remain lost.
Continued and informed debate on these issues is necessary, especially now that diversionary programs and legal mandates to treatment are commonplace. This report is an overview, and quite possibly it poses more questions than it answers. More study is needed to ascertain the nature and number of offenders who follow a pathway from arrest to drug treatment. How many divertees were arrested because of their involvement with a controlled substance or paraphernalia versus the number arrested for an offense that was "caused" by drugs, for example, larceny? What are the outcomes when they receive treatment? Do these differ according to type or level of offense, type of treatment, level of supervision by the probation department, ability of the defendant to escape recapture, or the
sociodemographic characteristics of the individual? How does the court measure outcomes? Is its notion of success commensurate with that of drug treatment program providers? Is the jail-based education program making a dent in recidivism among drug-involved offenders? Can it be accepted as "treatment"? Is its popularity and growing budget justified by this or other evaluative outcome measures?
Perhaps it is the sheer frequency with which the court sees drug-using offenders and drug-related offenses in its case calendars that contributes to the appeal of both alternatives to incarceration and sentence reduction clauses—which often rest on shared caveats of offender participation in drug treatment, education, and rehabilitation. Not everyone can be sent to jail or even be made to serve a full sentence when the county detention facilities operate at twice or three times their intended capacity. It is not possible at this time to determine the size or long-term effect of newly adopted procedures and programs endorsed by the courts other than to note that they seem to facilitate caseflow, mediate the numbers of offenders sent to jail, and shorten the length of their stays once they have been incarcerated.
The caseloads of each court differ in size, with unequal proportions of "clients" from each jurisdiction participating in diversion and probation programs that involve some sort of drug treatment Research is needed to determine whether the variability in sentencing practices among courts is accounted for by the severity of the offense, the potential for rearrest, past arrest and conviction records, or evidence of social support or stability demonstrated by employment or family affiliation. What drives the decision, and how? Is it the appropriateness for referral to an available mode of treatment? Is it the ability of the defense attorney to bring the case to the attention of the system? Do the climates of the court, the district attorney's and public defender's offices, and the probation department influence more than just the terms of the release? Without research specifically designed to follow criminal justice system clients as they are processed by the courts and become involved in drug treatment programs, these questions remain unanswerable.
Several main implications of this report deserve further study. Growing numbers of people who get arrested end up being supervised in the community because their "crime" is transformed into "drug addiction" or ''drug abuse" by the court. This trend has implications with regard to whether the criminal justice or drug treatment system pays for the services they receive. Which agency's budget contains allowances for cases that overlap? It is known that most of the people who end up in jail and who are on probation do not have health insurance to cover treatment schedules mandated by the court. Whose responsibility is it to cover these costs, and what mechanism is in place to evaluate the outcomes of the clients
who are covered? Are there people choosing not to apply for diversion or probation because they cannot pay for the treatment they may be mandated to undergo?
Moreover, should the type of care offered to drug-abusing criminals be different from the care other people receive? Will the terms of the treatment necessarily reflect that it is mandated, and does this render the client "involuntary" or "nonvoluntary?" The clientele arriving from the criminal justice system may have patterns of use that are more likely to be defined by chronicity and criminality, should there be specially designed treatment programs for these clients?
Participation in 12-step model recovery programs seems to be part of nearly every treatment center's care plan in this county. Yet two of the guiding philosophies of such programs are that individuals join them voluntarily and that they are able to remain anonymous as members. What does this mean for court-ordered meeting affiliates? How do they understand the concepts presented by the 12-step model under these circumstances? What effect does the presence of involuntary referrals and the seemingly contradictory position of the "Anonymous" groups themselves in relation to the legal system have on those people who do attend meetings out of a sincere desire to find help? The usefulness of participation in 12-step activities may be jeopardized when these basic elements of the program philosophy are compromised or distorted. (See Phillips [1988] for a discussion of legal mandates and attendance at Alcoholics Anonymous meetings.)
The study county has no resources to systematically assess, refer, supervise, and secure drug treatment services for all those criminal justice system clients who may need them. The apparent lack of coordination between the jail-based drug program officials and resource officers in the community, the minimal supervision offered by probation officers for drug cases, and the shortage of publicly supported drug treatment slots point to a system that is severely underfinanced, overburdened, and incapable of coordinating the services that are available. Diversion or probation programs do not seem to qualify as uniform or legitimate efforts to deliver drug treatment services. From what the literature reveals about the nature of drug use and addiction, the activities of the study county to reduce or eliminate it seem somewhat unfocused and unrealistic.
Finally, as the "War on Drugs" continues, more people are being arrested and processed through the criminal justice system on drug law violations and drug-related charges. Can either the criminal justice or the publicly supported drug treatment systems remain effective without massive increases in their resources? If the criminal justice system continues to increase the number of referrals to drug treatment facilities in the community and the resources of those facilities are not increased
accordingly, will this not erode and dilute the entire publicly supported system for drug treatment? Should less time and money be spent on programs to reduce court caseflow and facility overcrowding in favor of developing strategies that allow new and varied models of drug treatment programs to be established and utilized?
Currently, the discourse at both local and national levels infers that the use of civil and criminal sanctions to buttress judicial mandates to drug treatment is an idea that has been put into practice because its efficacy has been conclusively demonstrated. Measures of success—reduced use of drugs or abstinence and lack of rearrest-are strongly associated with length of stay in residence, which in turn is positively associated with the level of sanctions in place to encourage the client to remain in treatment (Anglin, 1988; Leukefeld and Tims, 1988). But these discussions and their data also reveal serious shortcomings in current knowledge about the practice of dictating compulsory treatment; they might be better used as a departure for future inquiry (Brown et al., 1987; Stitzer and McCaul, 1987).
Many of the arguments in support of mandating treatment are constructed on a heroin model of drug use. Heroin is very different from crack-cocaine and appeals to an equally different type of user. The presence of crack-cocaine users and addicts in the criminal justice system quite possibly causes the greatest strain both to it and to treatment providers. To date, there have been very few reports of large-scale, experimentally designed studies that provide information about the costs of a compulsory treatment response, both for state and county budgets, and its effect on local courts, jails, and public treatment systems—but with specific attention to the ramifications of crack use as the behavior to be eliminated. Current policies, practices, and debates all suffer most acutely from a lack of basic information and understanding that could offer a foundation for sound policies, which are difficult to formulate in the absence of systematic study.
Both additional information and a broader, more informed perspective would result from more comprehensive and evaluative study of the county's drug treatment and criminal justice systems. This report contains data drawn from a series of interviews with key players and targeted clients in both systems: representatives from law enforcement agencies, court officials, detention facility workers (both sworn and civilian personnel) probation and resource officers, people receiving drug treatment services because of diversion and probation programs, and some of the counselors, administrators and other staff that provide them. As a case study it could be greatly enhanced by the collection of statistical data using a rigorous research design to ensure validity and reliability. The initial observations regarding the county that presented here were generated mainly through qualitative methods, which could be tested—refined, disproven, elaborated,
or discarded. Any further understanding of the complexities of the drug treatment and criminal justice systems as they share clients and problems, if not philosophies, would be useful. The value of dedicating time and resources to these issues lies in the resultant ability to base decisions about legal mandates to treatment on facts about what happens to whom as an individual encounters and moves through both systems.
The use of systematic inquiry to consider both milieus, especially to sharpen the picture of how they interact, would yield valuable details about what "works" and for whom, what is affordable, and what is feasible, politically and legally. Information of this nature benefits the clients or consumers of services while allowing costs and other outlays of time and resources to be anticipated and monitored. Differentiating among drug-involved offenders makes sense for purposes of determining the best possible calculus of response—as mediated by the two systems—to interrupt individual drug use patterns. The response that is then negotiated and carried out by the treatment and criminal justice systems might prove to be more effective, than one that is less informed and could result in safer communities that require less effort devoted to protection.
DISCUSSION AND SUMMARY
A brief review of this history and the case study analysis raises a number of unresolved issues. Establishing the boundary between punishing drug law offenses and treating drug use disorders is difficult. Disagreement and confusion about how and where to make the distinction are reflected in both the literature and in the practices described in the case study. The ambiguous connection among the courts, the jails, and the drug treatment system; the critical shortage of drug treatment services; and the unevaluated quality of the care provided in the study county only exacerbate these dilemmas. Indeed, the connections among the courts, jails, and drug treatment system and among their personnel in the study county appear to be not only ambiguous but ungrounded and inconsistent; fiscal, legal, medical, and philosophical issues are further obscured.
Some concerns might be mitigated if greater care were taken to differentiate between and among addicts and users. Proceeding as if all users were addicts and all addicts led irregular, nonproductive criminal lives seems problematic (Velmen and Haddox, 1989). The reality is a spectrum that ranges from the criminal addict who may genuinely be a menace to society and not a strong candidate for rehabilitation, through all kinds of permutations to the "controlled," socially responsible user whose only crime is the use of a prohibited substance (Krivanek, 1988). Both extremes raise particular sets of problems, especially for two
institutionalized systems that struggle to remain flexible and offer appropriate programs and solutions to drug-using offenders and non-offenders whose drug use, dependence, and addiction patterns are so varied.
Other considerations come to mind as well. There is a confusion of roles among both health care providers and criminal justice personnel in terms of primary loyalty to the patient versus loyalty to the public. There is also the potential for co-optation of treatment providers by criminal justice agendas. Therapeutic elements of treatment are in danger of being overwhelmed by the number of referrals as well as superseded by the punitive aspects of criminal justice concerns (President's Commission on Mental Health, 1978; Feeley, 1983; DeLeon, 1988). Criminal justice personnel in the study county have almost the opposite concern: in their view, treatment milieus are not restrictive enough in their supervision of criminal offenders and may somehow undermine the primary mission of the criminal justice system, which is to protect the community. The roles assumed by both sets of personnel (with the client-offender, with their own institutions and professions, and with other cooperative systems) can become confused, and this confusion can affect the quality and effectiveness of each of these relationships as well as the outcome of the offender. Treatment provided under health care auspices is distinctive in both philosophy and practice from criminal justice requirements and goals.
Deciding whether an individual is eligible for treatment is a sorting function undertaken within the constraints of the two systems and the community on two different client dimensions: criminal record and suitability for treatment. The decision involves status determinations on these two dimensions, neither of which may be made by the district attorney or the clinician acting alone. Both are presumably guided by the language of the statutes that emanate from legislation. It is a language that is often stretched or constrained, depending on the particulars of a given case, by professionals who are called on to make judgments and weigh evidence that may be well outside the range of their expertise and training.
Problems arise when clinicians retain the ability to turn down clients from the criminal justice system, whether because of unsuitability or insufficient funding. Judicial intervention in the treatment process raises other issues. The passing of laws that dictate the type and quantity of treatment or that require or forbid certain methods preempt the clinician's discretion to select treatment according to his or her own judgments. When the extent of the caseflow threatens the uniform execution of the laws, as is occurring in the study county, the actual or latent value to the defendant of alternatives to incarceration is sacrificed. Any discretion left to the resource officers or to the clinician to make referrals is further eroded when services are insufficient in terms of availability or in terms of
availability plus appropriateness to the client.
Discretion and authority can be shared without sacrificing the individual concerns of the personnel in each system or the drug-involved offender. Presumably, having more options or slots available would improve overall service delivery by lessening the competition within and among the systems for placements. An increased number of slots is advisable even if the drug treatment system cannot or should not be expanded to accommodate everyone in the criminal justice system and the community who wants treatment. Matching the systems' resources with client characteristics and needs becomes more plausible, making a wider range of services available as options increase with added client slots. Additionally, the criminal justice system could establish and maintain its own range of drug treatment services for offenders, services that reflect the special status of the clients as both drug users and criminal offenders. These services could include treatment during incarceration and aftercare in the community following release.
The current obsession in the literature with compulsory treatment and civil commitment reflects the language and mind-set of the times: the nation is in the midst of a war on drugs. Wars justify the use of force and the subjugation of individual concerns to the good of the community and the maintenance of order. There are also treatment issues relating to coercion: whether legal controls on the patient are good or bad for therapy. Coercing a person to enter treatment as an alternative to more traditional criminal penalties seems attractive. Compared with imprisonment, it is both economical and cost-effective—not so much because existing treatment is enormously successful and inexpensive but because the usual process of criminal law is singularly costly and often ineffective (Krivanek, 1988).
The dilemmas become especially acute when treatment fails to rehabilitate the criminal justice-entangled client. The therapeutic rationale is withdrawn as punitive sanctions are reapplied. The current policy seems to imply that sickness ends when compliance ends or failure in treatment occurs. The evaporation of concepts of illness according to this model is neither therapeutic nor just. Failure to become or remain drug free is too often characterized as the exclusive fault of the individual rather than as an indication that there may be shortcomings within the treatment system that deserve attention as well. Should an individual's criminal status (and the criminal solution) so easily override what had been considered at least in part a medical condition-especially one from which it is difficult to recover (Gusfield, 1967; Wexler, 1973; Brown et al., 1987)?
It has been argued that the medicalization of a social problem such as drug use is a more guileful form of social control than pure imprisonment (Becker, 1963; Pitts, 1968; Kittrie, 1971; Glaser, 1974; Conrad and
Schneider, 1980; Makela, 1980; Alper and Nichols, 1981; Feeley, 1983; Morgan, 1983; Harrington, 1985; Krivanek, 1988). This shift was begun in part out of a decision that drug addiction was a disease of sorts that could be more effectively managed by the medical profession. Yet the client who is characterized as suffering from the disease is expected to assume some measure of responsibility in order to allow recovery to occur. Decisions are made about a person's fate based on "medical" evidence as to what treatment would facilitate a cure. Doing straight time in prison among other regular offenders is very different from being placed in a drug treatment program and monitored by the court, a probation officer, and treatment staff. Drug treatment regimens generally are not considered to be easy to follow-either when a sincere attempt is made to recover or if one only wants to "do the time" in order to stay out of jail or to get out sooner than would otherwise be possible.
The various roles assumed by the government and the actions performed in its name by a range of service provision systems seem also to be conflicted. A constitutional and philosophical responsibility to safeguard a citizen's civil rights and fundamental liberties is considerably challenged by the endorsement or use of direct or indirect coercion to motivate that same individual to enter treatment. Proper measures to assure the safety of the community must be undertaken at the same time. Over the years these issues have not lost their ability to incite controversy, and few to date have found resolution.
Treatment was never meant to be offered or forced upon every drug user who came into contact with the criminal justice system. It was viewed as an expensive but cost-effective way to handle certain people who both the treatment and criminal justice systems felt would benefit from it. Extraction from the adjudication process, whether pretrial or post-conviction, is meant to be cumbersome, and perhaps this contributes in part to the ill-defined process that governs diversion to treatment.
Clinical evidence reported to date does not conclusively support blanket referrals to compulsory treatment (Toborg, 1981; De Leon, 1988; Leukefeld and Tims, 1988; Maddux, 1988). The efficacy of compulsory treatment is related to the quality of the available programs as well as their implementation, client differences, client motivations, and the multivariate complexity of the recovery process itself (Brown et al., 1987; Stitzer and McCaul, 1987; De Leon, 1988). Evidence of the relative success or failure of treatment or of the retention of clients in treatment without legal coercion is not definitive. Evaluative outcome studies refer largely to heroin-using populations of the past and not to the cocaine-and crack-cocaine-using populations of the present. These data do not justify compulsory treatment participation without reference to the fundamental shortages in resources where services are offered.
Drug treatment has not been given high priority for funding since the mid-1970s. Now that the drug issue has regained political prominence and the specter of human immunodeficiency virus infection looms large, interest in treatment has been resparked. Yet known methods of treatment and their efficacy—especially for users of crack-cocaine—may still be regarded as uncertain and varying in quality (Brown et al., 1987; Stitzer and McCaul, 1987; Nurco et al., 1988). If treatment is advisable for a criminal justice-involved drug user, its best use is as a disposition regulated by a judicial proceeding that is separate from the legal determination of guilt or innocence. To date, neither diversion nor probation proceedings function in this way. The mandate to treatment as a sentence for drug-involved offenders is neither orthodox treatment nor a traditional punitive sanction. Further efforts to clarify the distinction between the two, while at the same time improving treatment modalities that accommodate this type of client, are needed.
The criminal justice system has long been used for providing services, however inadequate, for those who cannot afford them. Thus, the problem of reducing the scope of criminal and legal justice is complicated by the critical need for concurrent development of nonjudicial health care service delivery systems in the interest of social justice (Klapmuts, 1974). Currently, alternatives to incarceration seem to be conceived of—or at least function best as—escape valves of the criminal justice system rather than as carefully planned therapeutic interventions. Perhaps gains made in treatment program availability and effectiveness will soon match the reductions in courtroom caseflow that have already been realized.
The causes of drug abuse are complex, but they may be explored and faced directly. The analogy between drug addiction and contagious disease is often made. Within that context, even when a readily defined illness exists and even when that illness can be effectively treated with appropriate measures, the elimination of the problem from a community typically requires broad measures that extend beyond supervision, quarantine, and imprisonment at the level of the individual.
The rate of tuberculosis was reduced by medicine and treatment regimens but only finally controlled when living conditions were substantially improved. The disease remains strong in areas where such improvement has not occurred despite the fact that individual patients are readily identified and treated. Similarly, drug use, abuse, and addiction are, to some extent, a social problem. They will never be eliminated by measures levied solely at individuals that are not also designed to consider and address broader social issues (Newman, 1973).
Good public health practice dictates that the target of interventions should include the ecology of drug use and drug users. The complex social, political, and economic issues underlying drug use, especially on
the part of those who are criminally involved and incarcerated, require more substantial responses than treatment alone. Although treatment can help some people some of the time and should be available, concepts of medicalization, disease, and pathology at the level of individual cannot override the need for structural changes. The social and environmental causes of—and solutions to—criminally involved illicit drug use must be emphasized in addition to constructing a public order response. The report of the White House Conference for a Drug Free America (1988:71) correctly identifies treatment as ''simply the clinical event which initiates the ongoing and more complex cultural process of recovery." In viewing the drug problem as both a socially and criminally generated problem, the public health response appears to be more comprehensive. It extends the focus to education, jobs, and other quality of life issues involved in the continued use of drugs. Thus, the treatment episode may be complemented rather than undermined by placing it in a broader context that highlights additional opportunities for improvement.
FOOTNOTE
|
1 |
The reports cited in this section are not included in the reference list in order to protect the identity of the case study county. |
ACKNOWLEDGMENT
I wish to thank Craig Reinarman, Ron Roizen, Robin Room, and Raul Caetano for their comments on earlier versions of this paper, and Adrienne M. Radkoff for her assistance with graphics.
REFERENCES AND BIBLIOGRAPHY
Agopian, M.W. (1977) Evaluation of adult diversion programs: the California experience. Federal Probation 41(3):15-18.
Allison, M., and R.L Hubbard (1985) Drug abuse treatment process: a review of the literature. International Journal of Addictions 20:1321-1345.
Alper, B.S., and L.T. Nichols (1981) Beyond the Courtroom. Lexington, Mass.: Lexington Books, D.C. Heath and Company.
Ancel, M. (1971) Suspended Sentence. New York: Humanities Press.
Anglin, D., ed. (1988) A social policy analysis of compulsory treatment
for opiate dependence. Journal of Drug Issues 18(4):503-704.
Becker, H. (1963) The Outsiders. New York: The Free Press.
Bonnie, R.J., and M.R. Sonnereich (1973) Proposed uniform drug dependence treatment and rehabilitation act and commentary. Pp. 826-856 in Second National Commission on Marihuana and Drug Abuse, Drug Use in America: Problem in Perspective. Treatment and Rehabilitation, Vol. 4. Washington, D.C.: U.S. Government Printing Office.
Brecher, E.M. (1972) Licit and Illicit Drugs. Boston: Little, Brown and Co.
Brown, B., G. Buhringer, C. Kaplan, and J. Platt (1987) German/American report on the effective use of pressure in the treatment of drug addiction. Psychology of Addictive Behaviors 1(1):38-54.
Brüün, K. (1971) Finland: the non-medical approach. Pp. 545-558 in L.G. Kiloh and D.S. Bell, eds., Society, Culture and Drinking Patterns. New York: John Wiley.
Bureau of Justice Assistance (1988) Treatment Alternatives to Street Crime: TASC Programs. Washington, D.C.: U.S. Department of Justice.
Bureau of Justice Statistics (1983) Prisoners and Drugs. Washington, D.C.: U.S. Department of Justice.
Carter, R.M. (1972) The diversion of offenders. Federal Probation 36(4):31-36.
Chaiken, M.R., and B.D. Johnson (1988) Characteristics of Different Types of Drug-Involved Offenders. Issues and Practices series. Washington, D.C.: National Institute of Justice.
Chambers, C, J. Inciardi, D. Peterson, H. Siegal, and O.Z. White, eds., (1987) Chemical Dependencies: Patterns, Costs and Consequences. Athens, Ohio: Ohio University Press.
Chute, C.L., and M. Bell (1956) Crime, Courts and Probation. New York: The MacMillan Company.
Conrad, P., and J. Schneider (1980) Deviance and Medicalization: From Badness to Sickness. Toronto: The C.V. Mosby Company.
Courtwright, D. (1982) Dark Paradise: Opiate Addiction in America Before 1940. Cambridge, Mass.: Harvard University Press.
Danaceau, P. (1973) Methadone Maintenance: The Experience of Four Programs. Washington, D.C.: The Drug Abuse Council, Inc.
De Leon, G. (1988) Legal pressure in therapeutic communities. Pp. 160-177 in C. Leukefeld and F. Tims, eds., Compulsory Treatment of Drug Abuse: Research and Clinical Practice. NIDA Research Monograph No. 86. Rockville, Md.: National Institute on Drug Abuse.
Division of Probation, Administrative Office of the United States Courts (1978) The Presentence Investigation Report. Pub. No. 105.
Washington, D.C.
DuPont, R., A Goldstein, and J. O'Donnell, eds. (1979) Handbook on Drug Abuse. Washington, D.C.: National Institute on Drug Abuse.
Duster, T. (1970) The Legislation of Morality: Law, Drugs and Moral Judgment. New York: The Free Press.
Feeley, M.M. (1983) Court Reform on Trial: Why Simple Solutions Fail. New York: Basic Books.
Flanagan, T.J., and K.M. Jamieson, eds. (1988) Sourcebook of Criminal Justice Statistics—1987. Bureau of Justice Statistics, NCJ-111612. Washington, D.C.: U.S. Department of Justice.
Fort, J. (1968) Social problems of drug use and drug policies. California Law Review 56(1):17-28.
Fox, R. (1978) So Far Disordered In Mind. Berkeley, Calif.: University of California Press.
Gandossy, R.P., J.R. Williams, J. Cohen et al. (1980) Drugs and Crime: A Survey and Analysis of the Literature. Washington, D.C.: National Institute of Justice.
Glaser, D. (1974) Interlocking dualities in drug use, drug control, and crime. Pp. 39-56 in J. Inciardi and C. Chambers, eds., Drugs and the Criminal Justice System. Beverly Hills, Calif.: Sage Publications.
Goldfarb, R. (1975) Jails: The Ultimate Ghetto. Garden City, N.Y.: Anchor Press/Doubleday.
Gottlieb, B. (1985) Public Danger as a Factor in Pretrial Release: A Comparative Analysis of State Laws. U.S. Department of Justice, National Institute of Justice, research report. Washington, D.C.: U.S. Government Printing Office.
Gropper, B.A. (1984) Probing the Link Between Drugs and Crime. Washington, D.C.: National Institute of Justice.
Grossman, J. (1974) Methadone Treatment: Legal Aspects. Arlington, Va.: National Drug Abuse Training Center.
Gusfield, J.R. (1967) Moral passage: the symbolic process in public designations of deviance. Social Problems 15(2)(Fall):175-188.
Hall, A., E. Gaynes, D.A. Henry, and W.F. Smith (1984) Pretrial Release Program Options. Issues and Practices series. Washington, D.C.: National Institute of Justice.
Harrington, C.B. (1985) Shadow Justice: The Ideology and Institutionalization of Alternatives to Court. Contributions in Political Science No. 133. Westport, Conn.: Greenwood Press.
Hubbard, R., M. Marsden, J. Rachal, H. Harwood, E. Cavanaugh, and H. Ginzburg (1989) Drug Abuse Treatment: A National Study of Effectiveness. Chapel Hill, N.C: University of North Carolina Press.
Hudson, J., B. Galaway, W. Henschel, J. Lindgren, and J. Penton (1975) Diversion programming in criminal justice: the case of Minnesota.
Federal Probation 39(1):11-19.
Inciardi, J.A. (1981) The Drugs-Crime Connection. Beverly Hills, Calif.: Sage Publications.
Inciardi, J.A. (1987) Crime and alternative patterns of substance abuse. Pp. 485-524 in C. Chambers et al., eds., Chemical Dependencies: Patterns, Costs and Consequences. Athens, Ohio: Ohio University Press.
Inciardi, J.A, and C. Chambers, eds. (1974) Drugs and the Criminal Justice System. Beverly Hills, Calif.: Sage Publications.
Jaffe, J. (1979) The swinging pendulum: the treatment of drug users in America. Pp. 3-16 in R. DuPont et al., eds., Handbook on Drug Abuse. Washington, D.C.: National Institute on Drug Abuse.
Joint Committee of the American Bar Association and the American Medical Association on Narcotic Drugs (1961) Drug Addiction: Crime or Disease? Interim and Final Reports of the Joint Committee. Bloomington, Ind.: Indiana University Press.
Kadish, S.H. (1983) Encyclopedia of Crime and Justice, Vol. 3. New York: The Free Press.
Kaplan, J. (1983) The Hardest Drug: Heroin and Public Policy. Chicago: University of Chicago Press.
King, R. (1974) The American system: legal sanctions to repress drug abuse. Pp. 17-56 in J. Inciardi and C Chambers, eds., Drugs and the Criminal Justice System. Beverly Hills, Calif.: Sage Publications.
Kittrie, N. (1971) The Right To Be Different. Baltimore, Md.: The Johns Hopkins Press.
Klapmuts, N. (1974) Diversion from the justice system. Crime and Delinquency Literature 6:108-131.
Kleiman, M.A (1986) The AIDS epidemic and the criminal justice system: developing a policy agenda. Paper in progress, Program in Criminal Justice Policy and Management, John F. Kennedy School of Government, Cambridge, Mass.
Klein, D. (1983) III and against the law: the social and medical control of heroin users. Journal of Drug Issues (Winter):31-55.
Kramer, J.C. (1970) The state versus the addict: uncivil commitment. Boston University Law Review 50(1).
Krivanek, J. (1988) Heroin: Myths and Reality. Boston: Allen and Urwin.
Leukefeld, C, and F. Tims, eds. (1988) Compulsory Treatment of Drug Abuse: Research and Clinical Practice. NIDA Research Monograph No. 86. Rockville, Md.: National Institute on Drug Abuse.
Levine, H.G. (1978) The discovery of addiction. Journal of Studies on Alcohol 39:143-174.
Lidz, C.W., and AL. Walker (1980) Heroin, Deviance and Morality. Sage Library of Social Research, Vol. 112. Beverly Hills, Calif.: Sage
Publications.
Lindesmith, A.R. (1965) The Addict and The Law. Bloomington, Ind.: Indiana University Press.
Maddux, J. (1988) Clinical experience with civil commitment. Journal of Drug Issues 18(4):575-594.
Mäkelä, K. (1980) What can medicine properly take on? Pp. 225-233 in G. Edwards, and M. Grant, eds., Alcoholism Treatment in Transition. London: Croom Helm, Alcohol Education Centre and Addiction Research Unit.
McGlothlin, W., M.D. Anglin, and W. Bruce (1977) An Evaluation of the California Civil Addict Program. Rockville, Md.: National Institute on Drug Abuse.
McPike, T.K. (1978) Criminal diversion in the federal system: a congressional examination. Federal Probation 42(4):10-15.
Mecca, A.M. (1978) A State of the Art Assessment of the Treatment Alternatives to Street Crime Program. Unpublished dissertation, University of California, Berkeley.
Morgan, P.A. (1983) The political economy of drugs and alcohol: an introduction. Journal of Drug Issues 13(1):1-7.
Mosher, J.F. (1983) Alcohol: both blame and excuse for criminal behavior. Pp. 437-460 in R. Room, and G. Collins, eds., Alcohol and Disinhibition: Nature and Meaning of the Link. NIAAA Monograph No. 12. Washington, D.C: U.S. Government Printing Office.
Mullen, J. (1975) The Dilemma of Diversion (monograph). Washington, D.C.: U.S. Department of Justice, Law Enforcement Assistance Administration, National Institute of Law Enforcement and Criminal Justice.
Musto, D. (1973a) The American Disease. New Haven, Conn.: Yale University Press.
Musto, D. (1973b) Evolution of American narcotic controls. Pp. 335-348 in Second National Commission on Marihuana and Drug Abuse, Drug Use in America: Problem in Perspective. The Legal System and Drug Control, Vol 3. Washington, D.C.: U.S. Government Printing Office.
Narcotic and Drug Research, Inc. (1986) Crime Rates among Drug Abusing Offenders. New York: Narcotic and Drug Research, Inc.
Narcotic and Drug Research, Inc. (1988) Comprehensive State Department of Correction Drug Treatment Strategy Proposal. New York: Narcotic and Drug Research, Inc.
National Institute on Drug Abuse (1978) Criminal Justice Alternatives for Disposition of Drug Abusing Offender Cases. Washington, D.C.: U.S. Government Printing Office.
Newman, C.L., and B.R. Price (1976) Jails and drug treatment: a national perspective. Federal Probation 40(3):3-12.
Newman, R. (1973) We'll make them an offer they can't refuse. Pp. 94-100 in Proceedings of the Fifth National Conference on Methadone Treatment. New York: National Association for the Prevention of Addiction to Narcotics.
Nurco, D.N., T.E. Hanlon, J.W. Shaffer, T.W. Kinlock, N. Duszynski, and P. Stephenson (1988) Differences among treatment clinic types in attitudes toward narcotic addiction. Journal of Nervous and Mental Disease 176(12):714-718.
Ohlin, L, ed. (1973) Prisoners in America. Englewood Cliffs, N.J.: Prentice-Hall.
Packer, H.L. (1968) The Limits of the Criminal Sanction. Stanford, Calif.: Stanford University Press.
Palmer, J.W. (1974) Pre-arrest diversion: victim confrontation. Federal Probation 38(3):12-18.
Perlman, H.S. (1974) Legal Issues in Addict Diversion: A Layman's Guide. Washington, D.C.: Drug Abuse Council, Inc., and American Bar Association Commission on Correctional Facilities and Services.
Perlman, H.S., and P.A. Jaszi (1975) Legal Issues in Addict Diversion: A Technical Analysis. Washington, D.C.: Drug Abuse Council, Inc., and American Bar Association Commission on Correctional Facilities and Services.
Peterson, D.M. (1974) Some reflections on compulsory treatment. Pp. 143-182 in J. Inciardi and C. Chambers, eds., Drugs and the Criminal Justice System. Beverly Hills, Calif.: Sage Publications.
Phillips, M.D. (1988) The American criminal justice system and mandates to alcohol treatment: the role of alcoholics anonymous. Paper presented at the First Meeting of the International Collaborative Study of Alcoholics Anonymous, Helsinki, Finland, August.
Pitts, J.R. (1968) Social control: (I) the concept. Pp. 381-396 in D. Sills, ed., International Encyclopedia of the Social Sciences, Vol. 14. New York: Macmillan Company and The Free Press.
President's Commission of Law Enforcement and Administration of Justice. (1967) The Challenge of Crime in a Free Society. Washington, D.C.: U.S. Government Printing Office.
President's Commission on Mental Health (1978) Report of the liaison task panel on psychoactive drug use/misuse . Pp. 2118-2138 in Vol. 4, Appendix of the Task Panel Reports Submitted to the President's Commission on Mental Health. Pub. No. PCMH/P-7827. Washington, D.C.: U.S. Government Printing Office.
Room, R. (1978) Governing Images of Alcohol and Drug Problems: The Structure, Sources, and Sequels of Conceptualizations of Intractable
Problems. Unpublished Ph.D. dissertation, University of California, Berkeley.
Second National Commission on Marihuana and Drug Abuse (1973a) Drug Use in America: Problem in Perspective. Final Report. Washington, D.C.: U.S. Government Printing Office.
Second National Commission on Marihuana and Drug Abuse (1973b) Drug Use in America: Problem in Perspective. The Legal System and Drug Control, Vol 3. Washington, D.C.: U.S. Government Printing Office.
Second National Commission on Marihuana and Drug Abuse (1973c) Drug Use in America: Problem in Perspective. Treatment and Rehabilitation. Vol. 4. Washington, D.C.: U.S. Government Printing Office.
Selke, W. (1982) Diversion and crime prevention. Criminology 209(3-4):395-406.
Senay, E. (1978) Treatment goals for substance abusers. American Journal of Drug and Alcohol Abuse 5(3):299-305.
Senay, E., V. Shorty, and H. Alksne, eds. (1974) Developments in the Field of Drug Abuse: National Drug Abuse Conference Papers. Cambridge, Mass.: Schenkman Publishing Company.
Sills, D., ed. (1968) Encyclopedia of the Social Sciences, Vol. 14. New York: Macmillan Company and The Free Press.
Sloan, IJ. (1980) Alcohol and Drug Abuse and the Law. Dobbs Ferry, N.Y.: Oceana Publications, Inc.
Smith, R (1974) Addiction, coercion, and treatment: reflections on the debate. Pp. 852-862 in E. Senay et al., eds., Developments in the Field of Drug Abuse: National Drug Abuse Conference Papers. Cambridge, Mass.: Schenkman Publishing Company.
Speiglman, R., and C. Weisner (1982) Accommodation to coercion: changes in alcoholism treatment paradigms. Working paper prepared for presentation at the Annual Meeting of the Society for the Study of Social Problems, San Francisco, September.
Staples, W.G., and C.A.B. Warren (1983) Social junk as human commodities: a historical perspective on the privatization and profitization of social control. Paper presented at the Annual Meetings of the Pacific Sociological Association, San Jose.
Stitzer, M., and M.E. McCaul (1987) Criminal justice interventions with drug and alcohol abusers: the role of compulsory treatment. Pp. 331-362 in E.K. Morris and C.J. Braukman, eds., Behavioral Approaches to Crime and Delinquency. New York: Plenum Press. Sutherland, E.H., and D.R. Cressey (1974) Criminology. Philadelphia/New York/Toronto: J.B. Lippincott Company.
Terry, C.E., and M. Pellens (1928) The Opium Problem. New York:
Bureau of Social Hygiene.
Toborg, M.A. (1981) Pretrial Release: A National Evaluation of Practices and Outcomes. National Evaluation Program, Phase II Report. Series B, No. 2. Washington, D.C.: U.S. Department of Justice.
Toborg, M.A., D.R. Levin, R.H. Milkman, and L.J. Center (1976) Treatment Alternative to Street Crime. National Evaluation Program, Phase 1 Report. Series A, No. 3. Washington, D.C.: U.S. Department of Justice.
Vanagunas, S. (1979) Police diversion of juvenile offenders: an ambiguous state of the art. Federal Probation 43(3):48-52.
Velmen, G.F., and V.G. Haddox (1989) Drug Abuse and The Law Sourcebook, Vol. 1. New York: Clark Boardman Company, Ltd.
Vorenberg, E., and J. Vorenberg (1973) Early diversion from the criminal justice system: practice in search of a theory. Pp. 151-166 in L. Ohlin, ed., Prisoners in America. Englewood Cliffs, N.J.: Prentice-Hall.
Watters, J.K., C. Reinarman, and J. Fagan (1985) Causality, context and contingency: relationships between drug abuse and delinquency. Contemporary Drug Problems 12(3):351-374.
Weissman, J. (1978a) Drug Abuse, The Law and Treatment Alternatives. Criminal Justice Studies. Cincinnati, Ohio: Anderson Publishing Company.
Weissman, J. (1978b) Survey of state drug offender diversion policies. Contemporary Drug Problems 7(4):533-556.
Weissman, J. (1979) Drug offender diversion: philosophy and practices. Drug Abuse and Alcoholism Review 2(1):1-8.
Weissman, J., and B. Berns (1976) Patient confidentiality and the criminal justice system: a critical examination of the new federal confidentiality regulations. Contemporary Drug Problems 5(4):531-552
Weissman, J., and R. DuPont (1982) Criminal Justice and Drugs: The Unresolved Connection. New York/London: Kennikat Press.
Wexler, D. (1973) Therapeutic justice. Pp. 450-473 in Second National Commission on Marihuana and Drug Abuse, Drug Use in America: Problem in Perspective. Treatment and Rehabilitation, Vol. 4. Washington, D.C.: U.S. Government Printing Office.
Wexler, H.K., and R. Williams (1986) The Stay'n Out therapeutic community: prison treatment for substance abusers. Journal of Psychoactive Drugs 18(3):221-230.
Wexler, H.K., D.S. Lipton, and K. Foster (1985) Outcome evaluation of a prison therapeutic community for substance abuse treatment: preliminary results. Paper presented at the American Society of Criminology Annual Meeting, San Diego, November.
Wexler, H.K, D.S. Lipton, and B.D. Johnson (1988) A Criminal Justice
System Strategy for Treating Cocaine-Heroin Abusing Offenders in Custody. National Institute of Justice, Issues and Practices Series. Washington, D.C.: U.S. Department of Justice.
White House Conference for a Drug Free America (1988) Final Report. Washington, D.C: U.S. Government Printing Office.
Yale Law Journal (1974) Note: pretrial diversion from the criminal process. Yale Law Journal 83(4)(March):827-854.
































































