
Drug Treatment in State Prisons
Gregory P. Fallin
Harry K. Wexler
and
Douglas S. Lipton
Since the 1970s, when retribution replaced rehabilitation as the dominant sentencing philosophy, prison populations have climbed dramatically while crime has continued unabated. The public outcry against sharply rising crime rates during the early 1970s led politicians to call for more certain and severe sentences. A strong belief that corrections could not rehabilitate offenders was fueled by research studies that essentially concluded that "nothing works" (Lipton et al., 1975; Martinson, 1974). As rehabilitation fell into disfavor, determinant sentencing and persistent felony offender laws were enacted. Legislators also responded to the alarming increase in drug abuse during the 1980s by mandating tougher sentences against drug dealers and users. As a result of the new sentencing laws, the nation's prisons became full of serious drug-abusing offenders, many of them recidivists. Looking for ways to reduce recidivism and control overcrowding (and recognizing the close connection between substance abuse and crime), correctional authorities have begun expanding prison-based drug treatment programs during the past few years. In contrast to the viewpoint that nothing works in rehabilitation, the efficacy of a policy of expanding drug treatment for prisoners and parolees can now be supported by social science research.
Indeed, there is sufficient scientific evidence to demonstrate that certain types of prison-based drug treatment (e.g., therapeutic communities) can substantially curb recidivism. The need to reduce recidivism is paramount because of the many crimes perpetrated by career criminals and the problems stemming from prison overcrowding. Yet, despite a recognition of this need, sentencing policy during the last decade has led to a tremendous expansion of prison capacity without a commensurate decline in crime. Although this policy may be supported on the basis of "just deserts" for criminals, it is evident that incarceration is not adequate either
The authors are social scientists associated with Narcotic and Drug Research, Inc., New York, New York.
as a deterrent or as a means of controlling recidivism. The majority of inmates, especially the most serious among them, have severe lifestyle problems manifested most significantly by chronic substance abuse. Without appropriate treatment while in prison, a high percentage will relapse to drug use after release and will recidivate. The fundamental issue, then, is whether there are any forms of treatment that can reduce the likelihood of offenders recidivating. There is enough evidence currently to demonstrate that high-rate offenders with chronic polydrug abuse problems can be treated effectively.
Our conclusion, based on the available scientific evidence and our best professional judgment of what works, is that drug treatment in correctional settings can curb recidivism provided the programs have the following central features: (1) a competent and committed staff, (2) the support of correctional authorities, (3) adequate resources, (4) a comprehensive, intensive course of therapy aimed at affecting the lifestyle of clients beyond their substance abuse problem, and (5) continuity of care after inmates are paroled. In the absence of any of these features, it would be difficult to expect a drug treatment program to substantially reduce recidivism. Given the current array of treatment programs (many offering only occasional counseling, drug education, or other limited services), the finding of evaluation research that many programs are ineffective is not surprising. To adjudge that drug treatment is unable to control recidivism because many programs do not is to miss the crucial point that some programs have been quite successful. With the proper program elements in place, treatment programs could achieve a significantly greater reduction in recidivism than by continuing a policy of imprisonment without adequate treatment. This conclusion is, of course, tempered by the fact that only a limited number of programs have been scientifically demonstrated to be effective. This finding compels us to call for further research as treatment programs are implemented in correctional settings.
Because there is still considerable opposition to rehabilitation in any form, this paper next assesses the validity of the arguments against expanding drug treatment in corrections. The justification for treating prisoners and parolees rests primarily on the fact that there is a high correlation between drug abuse and crime and that certain types of treatment have been found to be effective in controlling relapse to drug use and recidivism. Each of these issues is discussed in subsequent sections. Based on an assessment of what works and what does not work in drug treatment, there are several guidelines we recommend following in establishing prison-based and aftercare drug treatment programs for offenders.
OPPOSITION TO PRISON-BASED DRUG TREATMENT: A RESPONSE
Although the number of prison-based drug treatment programs has increased during the past few years, there is still considerable opposition to them. Funds for prison construction and maintenance have clearly been given priority over funds for treatment. Policymakers who are against expanding drug treatment programs for convicted felons rest their case on several arguments: rehabilitation programs treat criminals too leniently; the public wants more criminals punished rather than more rehabilitation programs; and rehabilitation programs cost too much and do not work. Prisons, many contend, deter criminals and ensure that they receive their just deserts. Each of these arguments warrants serious consideration. To best understand the basis of these beliefs and their implications for drug treatment, a brief explanation of their origin is required.
The Belief That ''Nothing Works" in Rehabilitation
Perhaps the most important point to note is that much of the opposition to drug treatment for offenders stems from an opposition to correctional rehabilitation in general. During the mid-1970s, after a decade of social strife (antiwar demonstrations, prison riots, rising crime rates, drugs being used openly and their benefits popularly espoused), a consensus developed that reforms needed to be made in criminal justice (Cullen and Gendreau, 1989). The time had come for a social shift from turbulent conditions and libertine lifestyles to greater social order and morality. Indeterminant sentencing, the centerpiece of the rehabilitation philosophy for decades, became the target of both conservatives and liberals. They shared the view that prisons did not rehabilitate and found support for their beliefs in contemporary scientific research.
Conservatives by and large perceived the problem as a lack of law and order in society. Their rhetoric focused on sharply rising crime rates, and the solution they sought was to "get tough" with criminals. Determinant sentencing and related policies, such as mandatory minimum sentencing, selective incapacitation, and the abolition of parole, would, in their view, control crime and ensure just deserts. Liberals in the main were disheartened with perceived social injustices and felt that indeterminant sentencing was causing gross inequities. Prisons were seen as "factories of crime" and not places of reform. Determinant sentencing in general, and sentencing and parole guidelines in particular—policies based on the "justice model"—would, according to the liberal prescription, ensure fairness and eliminate the abuses of discretionary authority. Thus, for
different reasons and with different reforms in mind, a consensus emerged that rehabilitation was no longer a primary function of the postadjudicatory system.
The rhetoric against rehabilitation was bolstered by the fact that opponents of rehabilitation were able to corroborate their deeply held beliefs with scientific research findings. In 1974, Robert Martinson published a highly influential article in The Public Interest entitled "What Works?—Questions and Answers About Prison Reform." His central conclusion was that "[w]ith few and isolated exceptions, the rehabilitative efforts that have been reported so far have no appreciable effect on recidivism" (1974:25). The phrase, "nothing works," was thus coined and became an accepted part of the corrections vocabulary; it was treated as fact. The belief that "nothing works'' still has widespread acceptance and is one of the main reasons drug treatment programs are given low priority despite high recidivism rates, especially among drug-abusing offenders. But how true is it that ''nothing works?"
Martinson's article was a more widely read popularization of a scholarly assessment of the outcomes of 30 years of rehabilitation efforts for criminal offenders, a project directed by Douglas Lipton in which Martinson participated. The basic conclusion of their book, The Effectiveness of Correctional Treatment, was that "the field of corrections has not as yet found satisfactory ways to reduce recidivism by significant amounts" (Lipton et al., 1975:627). Other authors reviewing evaluation studies of rehabilitation programs came to essentially the same conclusion (Bailey, 1966). Few people who espoused the view that nothing works questioned the validity of the research on which it was based or understood the problems inherent in the design of most treatment programs and in the methodologies used to evaluate them. They also did not recognize the difference between Martinson's pessimistic viewpoint and the more guarded conclusion of Lipton and colleagues, which left open the possibility that rehabilitation could work.
So influential were the research findings in the policy debate about sentencing reform and rehabilitation that they became the subject of a scholarly assessment by the National Academy of Sciences. In its report, The Rehabilitation of Criminal Offenders, the Academy tempered the assessment that nothing works by stating that "we do not now know of any program or method of rehabilitation that could be guaranteed to reduce the criminal activity of released offenders" (Sechrest et al., 1979:3). Rather, it raised the question of whether some programs might work for certain types of offenders. Since that time, a growing body of evaluation studies has come under careful scrutiny, and several authors have concluded that certain rehabilitation programs effectively reduce recidivism (Gendreau, 1981; Gendreau and Ross, 1979, 1983-1984, 1987; Greenwood
and Zimring, 1985; Palmer, 1975; Van Voorhis, 1987).
Ironically, a few years after publishing his "What Works?" article, Martinson revised his conclusion, based on further review of the research, in which he found that "some treatment programs do have an appreciable effect on recidivism" (1979:244). As Cullen and Gendreau state, "the doctrine of nothing works is best seen not as an established scientific truth, but as a socially constructed reality" (1989:30). Just the same, the generalized belief that nothing works has been, as we suggested earlier, a major factor in the reluctance of many policymakers to support prison-based drug treatment.
Accordingly, we later present a detailed review of the evaluation research on drug treatment programs for offenders, focusing on what has been found to work. This research, all of it conducted since the studies reported by Lipton and coworkers, demonstrates that there are promising approaches to the treatment of drug-abusing offenders. In fact, a major outcome evaluation study conducted during the 1980s by Lipton and the present authors (Wexler et al., 1988b) demonstrates that the prison-based therapeutic community is a highly effective modality; this research in particular (summarized below) illustrates the profound changes that have taken place since the earlier assessment of rehabilitation. Indeed, there is sufficient scientific evidence for us to conclude that there are now, to quote the earlier statement of Lipton and associates, "satisfactory ways to reduce recidivism by significant amounts."
Belief in Imprisonment
The belief that nothing works is, as the evaluation literature demonstrates, a misconception. Just the same, it is often used to justify a policy of imprisonment for convicted felons. For many, this policy is based on a retributive ideology, which stems fundamentally from a desire to see offenders receive their just deserts. Policymakers who support imprisonment usually believe that the public wants offenders punished and that supporting treatment would be a show of leniency. This belief is supported by the argument that incarceration is the most, perhaps the only, effective means of controlling crime. Imprisonment, it is thought, will keep criminals off the streets (the incapacitation argument) and prevent them from recidivating afterwards (individual deterrence); in addition, others will refrain from crime, fearing the consequences (general deterrence). Because longer and more certain sentences lead to increases in prison populations and because court orders limit overcrowding, more prisons must be built. Thus, resources should be allocated for prison construction, not treatment programs.
Our basic response to these beliefs is that support for drug treatment programs is consistent with the goals of a policy of incarceration. In other words, offenders can be punished and society protected by placing them in drug treatment programs while they are in prison and on parole. Indeed, to alter the criminal proclivities of some offenders, it may be necessary for them to both serve a term in prison and receive treatment for their substance abuse. Furthermore, the fact that recidivism rates continue to be high gives one reason to question the belief that incarceration is an effective deterrent. Thus, the issue is whether drug treatment programs for prisoners and parolees can reduce recidivism better than the current practice, which limits treatment. Because of the high correlation between drug abuse and recidivism, we believe it is in the public interest to place offenders in the kinds of prison-based and community treatment programs that have been found to be effective.
During the past decade, the number of inmates in the nation's prisons doubled, approaching nearly three-quarters of a million. The vast majority (more than 80 percent) are recidivists; about three-quarters previously used drugs (Innes, 1988). Many of these prisoners have severe substance abuse problems. Indeed, about one-third of the inmates previously used a major drug (heroin, methadone, cocaine, LSD [lysergic acid diethylamide], PCP [phencyclidine]) on a regular basis; more than half reported using drugs during the month prior to committing the crime for which they were incarcerated (Innes, 1988). Slightly more than half were under the influence of alcohol or drugs, or both, at the time of the offense for which they were incarcerated. Some of these inmates are predatory criminals with severe substance abuse problems; they are responsible for an extraordinary amount of crime and are involved in a variety of violent crimes, property offenses and drug deals.
Indeed, the extensive research on the relationship between drug abuse and crime (summarized in the next part of this paper) provides convincing evidence that a relatively few severe substance abusers are responsible for an extraordinary proportion of crime (Gropper, 1985, based on the work of Johnson et al., 1985; Ball et al, 1983; and Inciardi, 1979). Because of the seriousness of their crimes and their criminal records, many of these drug-abusing offenders are incarcerated; therefore, a logical, cost-effective, and convenient point of intervention is while they are in prison and on parole.
Without treatment in prison, a high percentage will relapse to drug use after release and will return to crime. These behaviors are part of a lifestyle that is both highly destructive and resistant to change. In fact, about one-quarter of the drug users in prison were previously in treatment (Bureau of Justice Statistics, 1983). There is, however, enough evidence (described later) to demonstrate that even the most severe offenders, that
is, career criminals with chronic polydrug abuse problems, can be effectively treated. Yet despite this evidence, corrections has, for the most part, made limited attempts to institute programs aimed at treating substance abusers in prison and on parole.
Some legislators oppose drug treatment in prisons because they believe that correctional officials do not want these programs in their institutions. Although there are some wardens who do not believe in treating inmates with drug abuse problems, the issue is really more a matter of priorities. Currently, the overriding concern of correctional authorities is to ensure that they have adequate space to house inmates. Their budgetary needs reflect a priority for additional prison space over rehabilitation programs. In some cases, correctional officials may also be in conflict among themselves as to where to treat offenders; that is, they may disagree over whether resources should be allocated to community-based or prison-based programs. Furthermore, prison administrators may sometimes feel that prison-based treatment programs make it more difficult for them to manage inmate housing. (This problem occurs when they dedicate a separate housing unit to the program in an attempt to separate general population inmates from program residents.) Although correctional officials do have legitimate concerns about the priority of prison-based drug treatment programs, we believe they are more than offset by the programs' advantages.
In addition to their effect on recidivism, the major benefit of prison-based drug treatment programs is that they enhance security in institutions. Drug use and drug dealing (which are rampant in many prisons) decline with the introduction of drug treatment programs and random urinalysis testing (Vigdal and Stadler, 1989). Infractions of prison rules as well as violence and threats of violence also decline, and the danger of prison riots is reduced. In fact, there have been instances in which inmate leaders in drug treatment programs quelled disturbances that could have led to rioting. Correctional authorities evidently recognize the value of treating prisoners for their drug abuse and have given it increasing priority during the past decade. Between 1979 and 1987, the percentage of inmates in some form of treatment tripled.
Many policymakers, especially legislators, oppose funding for prison-based drug treatment programs because they believe that the public wants offenders punished and that treatment programs coddle criminals. Although it is true that Americans want criminals punished and that there has been a substantial decline in public support for rehabilitation since the late 1960s, Cullen and Gendreau (1988) provide evidence that "support for rehabilitation remains surprisingly strong." For example, although only 12 percent of Michigan policymakers assumed that citizens favored prison rehabilitation, 66 percent of the public believed rehabilitation should be
a primary goal of prisons (cited in Cullen and Gendreau, 1988). This is not an isolated finding; Cullen and Gendreau note several other national and state surveys that show that the public still believes in prison rehabilitation. According to a study commissioned by the Edna McConnell Clark Foundation, citizens want "assurances of safety much more than they want assurances of punishment," and they "want prisons to promote rehabilitation as a long-term means of controlling crime" (Public Agenda Foundation, 1987:5; cited in Cullen and Gendreau, 1988). As we conclude from the evidence on the relationship between drug use and crime and the existence of effective treatment programs (described in the next two parts of this paper) prison-based drug treatment is essential as a means of protecting society. Furthermore, good drug treatment programs do not coddle criminals; residents usually find these programs quite demanding because of the profound changes in attitudes and behaviors they require.
THE NEED FOR DRUG TREATMENT IN PRISONS
Although a small percentage of the nation's prisoners receive drug treatment, there is still a considerable need for effective treatment programs. Estimates by social science researchers and correctional authorities indicate that as much as 70 to 80 percent of the nation's prisoners used drugs prior to incarceration; however, only about 10 percent are in prison-based treatment programs (Chaiken, 1989; Innes, 1988). Drug-dependent offenders are responsible for a substantial, indeed disproportionate amount of crime in comparison with offenders who do not use drugs. Studies of serious substance abusers, in particular, offenders who use heroin and cocaine, show that they have extremely high crime rates. As the extent of abuse increases, the frequency and severity of their crimes escalate. Furthermore, many of these drug users are also involved in drug dealing, an enterprise that also has an attendant effect on other forms of crime, especially crimes of violence. A review of the empirical studies of the association between drug use and crime provides an appreciation of the enormous impact of drug abuse on crime.
The Relationship Between Drug Use and Crime
Numerous studies consistently report exceedingly high crime rates among substance abusers, especially heroin and cocaine abusers. Although cocaine and crack use have increased dramatically in the past few years and many prisoners are dependent on these drugs, only a few research studies of the relationship between crack and crime have been completed. Thus,
the following discussion focuses primarily on the connection between heroin use and crime, highlighting the effects of cocaine and crack use where research evidence is available. Inciardi (1979) has reported that active heroin users commit an average of 423 crimes per arrest. Johnson and colleagues report that the average heroin abuser in New York City commits more than 1,000 crimes (including crimes for money, drug dealing, and minor offenses such as shoplifting) per year (1985:77). During periods of daily heroin use, the average offender commits 100 to 300 crimes a year, including robbery and a variety of property crimes (Johnson et al., 1985). Such users commit thousands of crimes during their drug abuse careers, according to studies in New York, Miami, Baltimore, California, Michigan, and Texas (Chaiken, 1986; Johnson et al., 1985).
Not only do drug-dependent offenders commit a substantial amount of crime, but as the frequency of abuse increases, so does the frequency of crime (Ball, 1986; Ball et al., 1981; Chaiken and Chaiken, 1983; Johnson et al., 1985; McGlothlin et al., 1977). During times when offenders use heroin or cocaine daily, they commit two to six times as much crime as when they use these drugs less frequently (Ball et al., 1982; Speckart and Anglin, 1986). Ball and coworkers (1981) found that daily heroin users commit more than six times as much crime as offenders who use heroin less than daily. In this study, daily heroin abusers reported an average of 248 "crime-days" (24-hour periods in which an individual commits one or more crimes) per year at risk, whereas nondaily users reported only 40.8 crime-days per year at risk. Similarly, Johnson and associates (1985) reported that daily heroin users (six or seven days per week) claimed an average of about 1,400 crimes (including crimes for money, drug dealing, and minor offenses such as shoplifting) per year; however, regular heroin users (three to five days per week) committed about 1,200 crimes, and irregular users (one or two days per week) committed only about 500 crimes. Research on the relationship between crime and cocaine use demonstrates that, as the frequency of cocaine use increases, criminal activity also increases (Collins et al., 1985; Hunt et al. 1986).
As the frequency of drug use increases, the severity of the crimes committed also increases. Criminal income is approximately $55,000 annually during periods of daily cocaine or heroin use, but it is less than half as much during periods of less regular use (Collins et al., 1985; Johnson et al., 1985; Speckart and Anglin, 1986). The most serious crimes (robbery, burglary, aggravated assault) are common during daily cocaine or heroin use but rare during periods of nondaily use (Ball et al., 1983; Chaiken and Chaiken, 1982; Hunt et al., 1984; Speckart and Anglin, 1986). A study of career criminals found that a majority of the most violent criminals were heroin users, and most of these were daily users with high-cost heroin habits (more than $50 per day, Chaiken, 1986). Crack abusers
appear to commit an equal if not greater number of crimes than heroin abusers. Whereas heroin abusers tend to commit more property crimes (e.g., burglary, larceny), crack abuse seems to have accelerated the rates of violence, drug dealing, and sexual crimes, as well as robbery (Goldstein et al., 1989, 1990; Johnson et al., in press).
In addition to property crimes and crimes of violence, drug-dependent offenders are also heavily involved in drug dealing. Estimates range from 100 to more over 1,000 drug distribution crimes per year, depending on the location and type of heroin abuser studied. Chaiken and Chaiken (1982) found that their sample of incarcerated felons claimed 90 to 160 drug sales per year. Johnson and colleagues (1985) report that daily heroin users commit about 1,000 drug distribution crimes each year. In addition to direct sales of drugs, illegal drug distribution activities include directing customers to dealers ("steering"), recruiting customers for dealers ("touting"), and buying drugs for customers ("copping").
Involvement in drug dealing perpetuates criminal activity of all sorts. Drug dealing and drug use often involve violence, as reported in the ethnographic work of Goldstein (1985, 1989). According to Goldstein, violence and threats are utilized to enforce and maintain smooth operations of the drug distribution system. Lower level dealers are controlled by threats of violence, and upper level distributors are often targets for violent "rip-offs" by drug users and dealers. Statistical reports indicate that 20 to 30 percent of homicides are drug related (McBride, 1981; New York City Police Department, 1983). Estimates in 1988 are that more than 50 percent of New York City's homicides are drug related (Goldstein et al., 1989).
The prevalence of drugs and alcohol in criminal populations has recently been studied. Wish and associates pioneered the use of urinalysis in a series of studies of male arrestees in New York City to reveal the presence of illegal drugs at the time of arrest (Wish et al., 1984). (It is assumed that most of the arrests occurred shortly after the crime.) They found that 80 percent of arrestees charged primarily with serious nondrug crimes tested positive for one or more drugs (primarily cocaine and heroin). This basic finding has been replicated in 12 large cities that participate in the National Institute of Justice's Drug Use Forecasting (DUF) system (1988). Between April and June 1988, 50 percent or more of male arrestees in 10 of the cities tested positive for one or more drugs (excluding marijuana). In New York City, 83 percent tested positive for cocaine, and 27 percent tested positive for heroin.
Several other studies have provided information on the actual utility of drugs in criminal activity among samples of hard drug users (Goldstein et al., 1990; Strug et al., 1984). Large amounts of alcohol, cocaine, and heroin are often ingested by criminals before and after a crime to reduce
their anxiety and enhance their courage. The proceeds from the crime are then used to obtain additional drugs and alcohol.
Assessing the Drug-Crime Connection from a Treatment Perspective
Although the relationship between drug use and crime illustrates the need for prison-based treatment, the precise nature of causality is more of theoretical interest than of practical value as far as treatment is concerned. In other words, one does not have to debate whether crimes are committed because of the pharmacological properties of drugs or whether they are economically motivated (to finance drug habits or to enhance power in the drug distribution system). The important point is that, for many prisoners, both crime and substance abuse (including alcohol as well as illicit drugs) are inextricably tied into a lifestyle characterized by hedonistic, self-destructive, and antisocial behaviors.
The most significant manifestation of this lifestyle is polydrug use (but it also includes problems related to poor interpersonal skills, a lack of job skills, dependency on others, and frequent conflict with criminal justice authorities). The use of expensive drugs (heroin and cocaine, in particular) is highly related to crime; discerning whether the use of other substances (such as PCP, marijuana, and alcohol) causes crime is less important than understanding that for many offenders the use of these substances is also part of an antisocial lifestyle, which often involves polydrug use (Collins et al., 1985).
Although a large proportion of the nation's prisoners lead a lifestyle associated with problems of drug abuse, only a small percentage receive treatment while in prison. Few of these programs, however, are intensive enough to have a significant effect on relapse and recidivism (most programs offer only drug education, Alcoholics Anonymous meetings, occasional counseling, or other limited services). Without effective treatment for their drug use and related lifestyle problems, the likelihood that they will recidivate is quite high. Can treating them in prison reduce their criminality after they return to the community? As the next section demonstrates, there is enough evidence that drug treatment is an effective means of controlling recidivism and that intensive programs such as therapeutic communities are well suited to serious drug abusers in prisons.
EVALUATION RESEARCH ON PRISON-BASED AND COMMUNITY DRUG TREATMENT PROGRAMS
Although there are a variety of treatment modalities (e.g., methadone maintenance, residential drug-free programs, outpatient counseling), not all programs are relevant for prisoners and parolees. Because serious offenders generally require intensive drug treatment and methadone maintenance is neither relevant to the treatment of cocaine addiction nor available in prisons (see Magura et al., 1989, which discusses a jail-based methadone program), this part of the paper reviews only outcome evaluation studies of the residential drug-free modality. A fairly exhaustive search of the published literature on prison-based drug treatment reveals only a limited number of evaluation studies. Accordingly, the research conducted in a few of the more notable prison-based programs is described in detail, following which the research on community-based programs is reviewed.
Although only a small percentage of the clients in residential programs have entered treatment after prison—most admissions are made either on a voluntary basis or as a condition of probation—evaluations of these programs give insight into the types of treatment that are likely to be effective in prison and aftercare programs. (Because the focus here is on postadjudicatory treatment, studies of diversion programs, such as Treatment Alternatives to Street Crime, or TASC, and other alternatives to incarceration, such as intensive probation supervision, are not reviewed.) Because drug treatment programs for offenders may be based on different models (e.g., self-help, addiction as a disease) and may include a variety of program components (e.g., counseling, drug education, confrontation groups), the section below discusses specific approaches, both successful and unsuccessful, in the treatment of offenders.
Prison-Based Drug Treatment Programs
Despite many obstacles to prison rehabilitation, some efforts have been made to treat substance abusers while they are in prison. Although there is a paucity of information about the extent of prison drug treatment programs in the United States, some indications about the extent and quality of these programs are available. In 1979 the National Institute on Drug Abuse (NIDA) conducted a comprehensive survey of drug abuse treatment programs in prisons (NIDA, 1981). The survey identified 160 prison treatment programs serving about 10,000 inmates (4 percent of the prison population). In 1979, 49 programs (32 percent of all programs) were based on the therapeutic community model. They served about 4,200
participants (or 42 percent of all participants). Chaiken estimated that, in 1987, 11.1 percent of the inmates in the 50 states were in drug treatment programs (Chaiken, 1989). Although this figure represents a sizable increase (from 10,500 inmates in 1979 to 51,500 inmates in 1987), the vast majority of inmates with substance abuse problems still do not receive treatment while in prison.
Although a number of therapeutic communities (TCs) within prison settings have been established in state and federal prisons, relatively few outcome research studies have been conducted (NIDA, 1981). Accordingly, this section presents the existing literature on evaluations of prison-based drug treatment programs, focusing primarily on recidivism outcomes. First, our own research on the Stay'n Out program in New York State is described in detail. Then, evaluations of several other prison-based programs (the Cornerstone, Simon Fraser University, Wharton Tract Narcotics Treatment, and Terminal Island treatment programs) are summarized.
Stay'n Out
The Stay'n Out program is a therapeutic community for the treatment of incarcerated drug offenders that has been identified as a national model (see the REFORM newsletter published in 1988 by the New York-based Narcotic and Drug Research, Inc.). Stay'n Out began as a joint effort of the New York State Division of Substance Abuse Services (DSAS), which funded the program during its first years; New York Therapeutic Communities, which operates it; the New York State Department of Correctional Services (DOCS), which currently funds it; and the New York State Division of Parole. It has two sites: a program for male offenders established in 1977 at the New York State Arthur Kill Correctional Facility on Staten Island, and a treatment program for females, opened in 1978 at the Bayview Correctional Facility in Manhattan. Currently, there are three treatment units at the Arthur Kill Correctional Facility with about 35 beds per unit (a total capacity of 146 beds) and one treatment unit at the Bayview Correctional Facility, with 40 beds.
In 1984 the National Institute on Drug Abuse provided a grant to Narcotic and Drug Research, Inc., to evaluate Stay'n Out and compare it to other prison drug abuse treatment programs. The evaluation was designed to test the proposition that effective treatment of substance abusers is possible within prison (Wexler et al., 1988b, 1990). A large-scale, quantitative analysis was conducted relating several measures of treatment outcome (e.g., rearrest, reincarceration) to both client characteristics and program attributes (time in program and termination status). The study included males and females as well as treatment and
no-treatment comparison groups. Statistical analyses were performed to test several hypotheses about the effectiveness of Stay'n Out treatment. The two main ones were that the Stay'n Out therapeutic community is more effective than no treatment or than alternative prison-based drug treatment modalities in reducing recidivism, and that increases in time in the program are related to reductions in recidivism. These two hypotheses were by and large confirmed, with the main finding being that, as time in therapeutic community treatment increases, recidivism declines significantly.
Since the program began, nearly 1,000 males and more than 500 females have been admitted to treatment. The aim of the program is to treat felony offenders for their drug abuse and related problems so that they are less likely to recidivate after leaving prison. Inmates selected for the programs are recruited at state correctional facilities; they must show an official history of drug abuse (or indication of involvement in the drug culture); be at least 18 years of age; have evidence of positive institutional participation; show no history of extensive violence, arson, sex crimes, or mental illness; and be no more than 12 months nor less than 6 months away from their first parole hearing. The expected minimum treatment period is from 6 to 9 months.
On average, male clients in the Stay'n Out program have previously been convicted four times and have been incarcerated for four years (prior to admission into Stay'n Out). Most of the offenders are in prison for robbery (43 percent), drug sales (18 percent), or burglary (18 percent). The Stay'n Out program admits drug abusers who have been heavily involved in drug use since the mean age of 16-1/2 Seventy-three percent of the clients have abused opiates; 77 percent have abused cocaine (and other stimulants). Their previous attempts at changing their lifestyle have failed. On average, they have previously been in two treatment programs for 18 months combined.
The programs at Arthur Kill and Bayview are therapeutic communities modified to fit into a correctional institution (see Wexler and Williams, 1986 for a full description of the program). During the early phase of treatment, the major clinical thrust involves observation and assessment of client needs and problem areas. Orientation to prison therapeutic community procedures is provided through individual counseling, encounter sessions, and seminars. At the outset, clients are given low-level jobs and granted little status. During the latter phases of the recovery process, residents are given opportunities to earn higher level positions and increased status through sincere involvement in the program and hard work. Encounter groups and counseling sessions explore issues in greater depth and focus on the areas of self-discipline, self-worth, self-awareness, respect for authority, and acceptance of guidance for problem areas. Seminars take on a more intellectual quality. Debate is encouraged to
enhance self-expression and to increase self-confidence.
Stay'n Out clients are housed in units segregated from the general prison population. They eat in a common dining room, however, and attend morning activities with the other prisoners. Most program staff are former addicts who are graduates of community-based therapeutic communities as well as ex-offenders. They act as role models demonstrating successful rehabilitation. All but one of the units are staffed by a unit director and three counselors; one unit at Arthur Kill has only two counselors. Support is provided by the administrative staff of New York Therapeutic Communities.
Upon release, participants are encouraged to seek further substance abuse treatment at cooperating community-based TCs. About half of program graduates actually continue in residential programs. Extensive involvement with a network of such community TCs is thus central to the program's operation. Staff and upper level residents of community TCs visit Stay'n Out on a regular basis to recruit resident inmates for their programs. As ex-addicts and ex-felons who are leading productive lives, these visitors act as role models and provide inspiration to those in earlier stages of recovery.
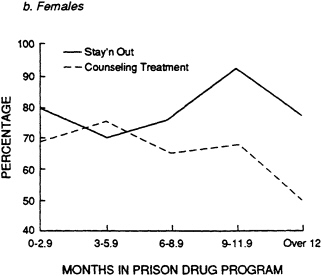
The evaluation research design compared the Stay'n Out male TC treatment group (N = 435) and the female TC group (N = 247) with no-treatment control and alternative treatment groups. The male treatment group was compared with a no-treatment control group (N = 159) that consisted of inmates who were on a waiting list for the program. They met all the criteria for admission except the parole time eligibility criterion and therefore completed their prison term without treatment. The male TC group was also compared with a milieu treatment group (N = 576), a residential treatment program that offered a less intensive treatment regimen than the TC (i.e., time was less structured, there was no hierarchy of jobs or social roles, counselors were not ex-addicts or ex-offenders but trained correctional officers, good conduct in the program was not rewarded with greater responsibility, and interaction with community TCs was less extensive). In addition, the male TC group was compared with a counseling group (N = 261), that received only individual and group counseling once a week. The female TC group was compared with a no-treatment control group (N = 38) and a counseling treatment group (N = 113); these groups were similar to their male counterparts (i.e., the control group met the basic criteria for admission but did not receive treatment, and the alternative treatment group received only counseling services).
In general, the background characteristics of the samples were comparable, except that the male milieu group had a significantly higher mean age and criminal history score (a weighted average of prior criminal
arrests, convictions, and sentences) and had spent more time in prison than the other male groups. Multivariate statistical analyses were performed to control for the possible confounding effects of these differences on treatment outcomes. The groups were compared according to several recidivism measures: the percentage arrested, the mean number of months until arrest, the percentage positively discharged from parole, and the percentage not reincarcerated. The sampling time frame was based on inmates released from prison between 1977 and 1984; therefore, the follow-up period (which ended in 1986) ranged from two to nine years, depending on the year prisoners were released.
Statistical analyses were performed to compare the effectiveness of TC treatment with alternative interventions and no treatment and to assess the relationship between treatment outcomes and time in treatment. The across-group comparisons yielded mixed results (i.e., when compared with the other groups, the TC groups had significantly lower arrest rates but differences in other outcome variables were not significant); however, the most powerful finding was that there was a consistent and significant correlation between treatment outcomes and time in the program. The failure to find significant differences between the TC group and comparison groups for some of the outcome variables stems from the fact that average treatment effects mask the differential impact of time in treatment within the groups. Indeed, the Stay'n Out evaluation research, like other TC evaluation research, consistently found statistically significant and salient effects between time in the program and treatment outcomes.
As Figures 1a and 1b show, male and female Stay'n Out clients do better on parole if they remain in the program for 9 to 12 months rather than terminating earlier (or later). Furthermore, while there is generally a positive relationship between time in Stay'n Out treatment and positive parole discharge (which tapers off after 12 months), time in the comparison modalities does not produce a positive effect. This pattern (as depicted in the figures) was found to be consistent for the other outcome variables as well, leading to the conclusion that Stay'n Out is more effective that no treatment and alternative treatments, provided clients remain in treatment for an optimal period, which appears to be 9 to 12 months. Although it is conceivable that clients who remain in treatment longer are more motivated than those who dropout, and that therefore the time-in-program effect might be related more to self-selection than to treatment effectiveness, one must keep in mind that motivation is a dynamic aspect of treatment. Indeed, the therapeutic process—with all its ups and downs-is intended to motivate clients to change, while enabling clients who are not adequately motivated to dropout. To assume that motivation to change is sufficient to bring about behavioral change would mean that anyone who wanted to improve could do so on his or her own.
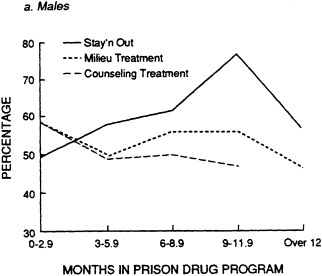
Motivation is necessary but not sufficient for most offenders, and change requires participation in a therapeutic process.
Insofar as testing the hypothesis that treatment outcomes improve as time in the program increases, several statistical analyses were performed on subgroups of TC clients who spent varying amounts of time in treatment. For example, when clients who completed the program in 9 to 12 months were compared with clients who left within 3 months, differences between the percentages of those positively discharged from parole for the two treatment periods were significant. Among the males who terminated in less than 3 months, the percentage of those positively discharged was only 49.2 percent, whereas the rate positively discharged for the males who stayed in the program for the longer period was 77.3 percent. Similar findings were obtained for the females, although the percentages positively discharged from parole were higher than for their male counterparts (79 percent for females in treatment less than 3 months, 92 percent for the 9- to 12-month group).
For those who recidivated (i.e., those rearrested or reincarcerated), more time in TC treatment was related to positive treatment outcomes. When the mean time until arrest was compared for the two termination periods, it was found that clients who received less treatment were arrested much sooner than those who stayed in the program for 9 to 12 months. Furthermore, the percentage of Stay'n Out male clients who were not reincarcerated after 9 to 12 months of treatment was considerably higher (72 percent within three years after release from prison) than for males who resigned or were dismissed earlier (60 percent within three years). Indeed, a logistic regression analysis showed that the odds of not being reincarcerated were nearly three times greater for clients who remained in treatment for 9 to 12 months than for clients who spent less than 9 months in treatment.
In addition to comparing the two subgroups, statistical analyses evaluated the functional relationship between time in the program and treatment outcomes. Perhaps the most important finding in this regard was that, as time in treatment increased, there was a (linear) improvement in treatment outcomes that tapered off after one year. One of several statistical analyses compared parole discharges among subjects who spent less than one year in treatment. Male clients who were positively discharged from parole spent more time in treatment (5.5 months on average) than males who were not positively discharged (they spent an average of only 4.5 months in treatment).
A related analysis compared clients who completed the program favorably (53 percent) with those who resigned and were dismissed (32 percent). (Neutral terminations, such as transfers for institutional reasons, or death, accounted for 15 percent of the terminations.) A significantly
higher percentage of clients who completed the program favorably were not reincarcerated (72 percent within three years) as compared with clients who terminated negatively (61 percent within three years). The positive influence of time in the program on outcomes was independent of the effects of background variables. Regression analyses showed that time in the program was positively related to time until arrest and reincarceration when other significant background variables (age and criminal history) were held constant. Furthermore, time spent in the Stay'n Out TC reduced reincarceration, whereas time spent in the comparison modalities did not.
Clients who received 9 to 12 months of treatment were not only less likely to recidivate than clients who spent less time in treatment, but they also did better than clients who remained in treatment more than one year. This finding was consistent for most of the outcome measures tested (time until arrest, positive parole discharge, reincarceration). Indeed, a multiple regression analysis confirmed a statistically significant decline in time until arrest for clients who remained in treatment for more than 12 months. It should be noted, however, that the clients in this group are still significantly less likely to recidivate than those who terminate from the treatment in less than 9 months. Thus, the central conclusions of the research are that hard-core drug abusers who remain in the prison-based therapeutic community longer are more likely to succeed than those who leave earlier and that 9 to 12 months appears to be the optimal duration for the treatment.
Although differences among the groups were not statistically significant for all outcome measures (as shown in Table 1), the results indicate that the prison-based TC was generally more effective than the no-treatment group and the comparison treatment modalities. Among the most important findings were that the percentage of TC males arrested (27 percent) was significantly lower than the percentage arrested from the control (41 percent) and comparison treatment groups (35 percent for the milieu group, 40 percent for the counseling group). Similarly, the percentage of TC females arrested (18 percent) was significantly lower than the percentage arrested from the no-treatment control group (24 percent) and the counseling group (30 percent). The mean number of months until arrest was significantly greater for the male TC group (13 months) than for the alternative treatment groups (about 12 months) but not for the no-treatment control group (15 months). In contrast, the mean number of months until arrest for the female group (12 months) was considerably higher than for the control group (9 months) but not the counseling group (15 months). these differences, however, were not statistically significant.
The percentage of females positively discharged from parole (77 percent) was significantly greater for the TC group than for the control (53 percent) and counseling groups (68 percent). Although the differences
TABLE 1 Recidivism Outcomes in the Stay'n Out Program
|
|
Positive |
|||||
|
|
Arrested |
Mean |
Parole Dischargeb |
|||
|
|
|
Months |
|
|||
|
Comparison |
|
Until |
|
|||
|
Groups |
Number |
N |
% |
Arresteda |
N |
% |
|
Male Groups |
||||||
|
TC treatment |
435 |
117 |
26.9 |
13.1 |
157 |
58.1 |
|
Milieu |
576 |
198 |
34.6 |
11.4 |
164 |
52.6 |
|
Counseling |
261 |
104 |
39.8 |
12.0 |
69 |
52.7 |
|
No treatment |
159 |
64 |
40.9 |
15.0 |
66 |
60.6 |
|
Statistic |
|
Chi Sq=17.2 |
|
F=2.32 |
Chi Sq=3.40 |
|
|
Significance |
|
p<.001 |
|
p=.07 |
n.s. |
|
|
Female Groups |
||||||
|
TC treatment |
247 |
44 |
17.8 |
12.4 |
98 |
77.2 |
|
Counseling |
113 |
33 |
29.2 |
14.6 |
58 |
68.2 |
|
No treatment |
38 |
9 |
23.7 |
86 |
9 |
52.9 |
|
Statistic |
|
Chi Sq=537 |
|
F=1.03 |
Chi Sq=535 |
|
|
Significance |
|
p=.07 |
|
n.s. |
p=.07 |
|
|
a Represents time until arrest for prisoners who were arrested after their release from prison. b For parole discharge data, 401 cases are missing for males and 169 cases are missing for females because the subjects had not been discharged by the time the data set was prepared for analysis. Source: Wexler et al (1988b:107). |
||||||
in the parole discharge variable were not significantly different among the male groups, the percentage of TC males positively discharged (58 percent) was slightly higher than that for the two alternative treatment groups (53 percent). The percentage of males not reincarcerated was about the same for the TC group (56 percent) as for the comparison treatment groups (55 percent for the milieu group, 59 percent for the counseling group). Despite the mixed results, however, the clearly lower recidivism rates (in terms of the percentage of the TC groups arrested) and the differences in several of the comparisons of the number of months until arrest and the percentage positively discharged from parole support the hypothesis that TC treatment reduces recidivism in comparison to no treatment and the alternative modalities.
Assessment of the possible influence of several psychological traits of
clients did not produce significant or systematic associations between measures of psychological traits (e.g., depression, anxiety, and schizophrenia) and treatment outcomes. Furthermore, the research design (utilization of treatment and no-treatment comparison groups) adequately controlled for the subtle effects of motivation, deterrence, and treatment. Thus, the Stay'n Out positive outcome results appear quite robust and replicate earlier findings in community-based TCs (De Leon, 1984).
The study of the Stay'n Out program is the first large-scale evaluation to provide fairly convincing evidence that prison-based therapeutic community treatment can produce significant reductions in recidivism rates. Indeed, dissemination of preliminary results has already had an important impact on the field and has generated interest as well as funding to support effective treatment for substance abusers while in prison (see the later discussion of Project REFORM).
Cornerstone
The Cornerstone program is a highly respected prerelease treatment program for alcohol-and drug-dependent offenders (see Field, 1984, for a detailed description). The program began in 1976 and is situated on the grounds of the Oregon State Hospital in Salem. It consists of a 32-bed residential unit and a 6-month aftercare program. Cornerstone is jointly administrated by the Oregon Divisions of Mental Health and Corrections.
Inmates are referred to the program by prison counselors. Admission criteria require that candidates have a history of substance abuse but no history of psychosis or sex offenses, are at least 6 months but not more than 12 months from parole, qualify for minimum security, and plan to remain in the state after release. In 1984 Cornerstone clients had an average of about seven felony convictions and had served more than 7 years in prison. The mean age of first substance use was 12 years of age. Ninety-five percent of the clients had histories of polydrug abuse.
Like Stay'n Out, Cornerstone is modeled on the therapeutic community concept. Inmates participate in the operation of the program and in a self-help recovery process. The program has a clearly articulated set of rules and consequences. The violation of cardinal rules (such as using drugs or violence) are grounds for dismissal. Consequences for infractions of other rules generally require clients to practice appropriate behaviors rather than submit to punishment. On the other hand, inmates earn privileges (in the form of increased freedom) for good behavior while in the program.
Clients are responsible for developing treatment plans at various stages of the recovery process. In addition to family meetings, encounter
groups, and classes, they receive guidance and feedback from counselors. Family counseling is available for clients with spouses, and all members attend Alcoholics or Narcotics Anonymous groups in the community. Classes are given to help residents develop basic skills such as money management and work skills. After completing the residential treatment phase of the program, the clients enter a six-month aftercare phase in which they live and work in the community. During this phase, they maintain contact with Cornerstone staff, their parole officers, and, if their treatment requires, outpatient drug treatment programs.
Two evaluation studies of the Cornerstone program assessed several treatment outcomes, including recidivism (Field, 1984, 1989). We summarize the findings of both studies because they demonstrate the effectiveness of the program over time. The 1984 study evaluated all clients who graduated between 1976 and 1979 against three comparison groups: (1) clients who dropped out in less than one month during the same time frame, (2) all Oregon parolees (from 1974 to 1977) who had a history of substance abuse, and (3) a sample of Michigan parolees. There were no statistical differences between the demographic characteristics of the program graduates (N = 144) and the dropouts (N = 27). The group of Oregon parolees (N = 179) had significantly less severe histories of substance abuse and crime than the program graduates. The sample of Michigan offenders (N = 217) was based on a population similar in background to the Cornerstone groups.
A three-year follow-up study compared the groups according to two outcome measures: the percentage not returned to prison and the percentage not convicted of any crime. Program graduates had a significantly higher success rate for both outcome measures than each of the other groups. Seventy-one percent of program graduates were not reincarcerated three years after release; only 26 percent of the dropouts avoided reincarceration. Similarly, although slightly more that half the program graduates were not convicted of any crimes (including minor offenses), less than 15 percent of the dropouts were not convicted of any crimes. As Field points out, the factors that cause residents to dropout may also influence recidivism; however, the favorable comparison with the other two groups supports the hypothesis that treatment in the Cornerstone program is associated with reduced recidivism. Indeed, chi-square tests of both outcome measures showed that program graduates had significantly better outcomes (p <.01) than the Oregon parole sample (63 percent of the parolees were not reincarcerated and only 36 percent were not convicted of any crimes). These univariate statistical differences, however, tend to understate the effect of the treatment because program graduates had significantly more severe criminal histories and substance abuse problems than the parole group.
Field's 1989 study produced similar results, using a different research design. A group of program graduates (N = 43) with an average stay of 11 months in treatment was compared with three groups of clients who did not graduate: (1) clients who spent more than 6 months in the program (N = 43), (2) clients who spent from 2 to 6 months in treatment (N = 58), and (3) clients who were in treatment for less than 2 months (N = 65). Three measures of recidivism were assessed in a three-year follow-up: the percentage of each group without a record of (1) arrest, (2) conviction, and (3) reincarceration (which included jail terms greater than 6 months as well as prison sentences).
The results for program graduates in this sample were quite similar to the findings in the earlier evaluation. Slightly more than half the graduates were not convicted, and about three-quarters were not reincarcerated; in addition, 37 percent were not arrested. These results compared quite favorably to the three groups that did not graduate. For example, 21 percent of the nongraduates who were in treatment for more than 6 months were not arrested, 28 percent of them were not convicted, and 37 percent were not reincarcerated. The findings for the other dropouts are even more startling. Indeed, only 8 percent of the clients who dropped out in less than 2 months were not arrested during the three-year follow-up, only 11 percent were not convicted, and only 15 percent were not reincarcerated. These findings are consistent with the findings on the Stay'n Out program, which showed that increased time in the program was associated with more positive treatment outcomes.
In addition to comparing the percentage in each group that did not recidivate, Field assessed the effect of treatment on rates of recidivism, that is, the average number of times clients in each group were arrested, convicted, and incarcerated. (These measures imply an expected probability of the number of times offenders will recidivate, depending on the amount of time they spend in treatment.) The three-year posttreatment period was compared with two different three-year intervals prior to prison term that involved treatment in the Cornerstone program. These intervals were the 36 months ''at risk'' prior to Cornerstone incarceration and the prior 37 to 73 months "at risk." (The "at-risk" intervals represent time in the community; they exclude time spent incarcerated.) Because some subjects were too young to be "at risk" for six years before the Cornerstone incarceration, only about 75 percent of the subjects in each sample were included in this analysis.
The results of the analysis across the three recidivism rate variables were consistent and support the findings on the variables that measured outcomes in terms of the percentage of each group that did not recidivate. The arrest, conviction, and incarceration rates for the group of program graduates were lower than those rates for each of the comparison groups.
Furthermore, as the length of time in treatment increased, recidivism rates declined. Perhaps the most interesting findings pertain to the comparisons between pretreatment and posttreatment intervals. Whereas the recidivism rates during both pretreatment intervals were about the same for each of the groups, recidivism rates during the posttreatment period were considerably lower among program graduates. In addition, the decline in recidivism rates between the pretreatment and posttreatment periods was greatest for program graduates.
The Simon Fraser University Program
This program provides treatment to prisoners in Vancouver, Canada (see Chaiken, 1989). The Department of Continuing Education administers the Prison Education Program under a contract with the government. The program is housed in trailers and bungalows (with classrooms, offices, a library, and a study area) on the grounds of four institutions. Although funding for the program was initially intended to reduce illiteracy, the goal of the program has broadened to include enhancing the moral development of offenders through a humanistic approach to education.
Simon Fraser faculty conduct a variety of classes in the liberal arts for student-prisoners who have histories of serious drug abuse and criminal activity. Students are expected to attend lectures and seminars, conduct library research, write papers, and participate in informal discussions of literature, current events, family practices, and publications. Two hundred students attend all-day sessions; they are given time for meals and appointments with medical, psychological, and social service staff. Seven full-time faculty members develop the curriculum and, with the assistance of adjunct faculty, teach courses. The faculty also oversees extracurricular activities and advises the students. There are no security guards assigned to the program, and substance use is not monitored. The program has an open admissions policy, but it requires participation for a minimum of one semester. There is no limit to the time students can stay in the program, and after they are released from prison, they can finish their degrees as regular university students at the Burnaby campus.
In 1980 an evaluation of the program compared a group of 65 former student-inmates with a group of 65 inmates who did not attend the program but were released during the same time frame (Duguid, 1987). Although the mean age of the two groups was the same, the student-inmates had both a significantly higher percentage of individuals convicted of drug offenses and addicted to opiates (56 percent of the students were previously addicts, whereas only 21 percent of the nonstudents were addicts). The nonstudents were more likely to have been convicted of burglary than
the students. Although 65 percent of the students had not completed high school, their average level of education (10.3 years) was higher than that of the nonstudents (8.5 years). A 3-year follow-up study found that half the nonstudents were returned to prison, whereas only 16 percent of the students were reincarcerated.
The Wharton Tract Narcotics Treatment Program
This program, which opened in New Jersey in 1970 (and is described in Platt et al., 1980), housed 45 youthful offenders (over 19 years of age) in a former state forestry camp situated in Wharton State Forest. The program was a satellite unit of the Youth Reception and Correction Center in Yardville. Youthful offenders were admitted to the program if they met the following criteria: an 8- to 12-month period of incarceration remaining, more than 6 months but less than 5 years of dependency on heroin, no extreme psychopathology, no recent escape, and no serious offense pending.
The program was based on the therapeutic community model and included guided group interaction (GGI) in the therapeutic process. (The essence of GGI is that the development of a group enhances the recovery of its members through a process of interaction.) In addition, the program included interpersonal problem-solving group therapy as a technique. Problem-solving skills (e.g., identification of a problem and the feelings associated with it, acquiring information, searching for possible solutions, and assessing consequences) were developed through a series of group exercises. The program also offered couples therapy, family counseling, individual counseling, and recreational activities. Residents completed the program in three phases: a 30-day evaluation period, intensive therapy (lasting at least 60 days), and a transition phase to ease residents back into the community.
An evaluation of the Wharton Tract program compared a group of graduates (N = 160) with a control group (N = 148) that met all the criteria for admission but did not enter treatment (Platt et al., 1980). There were no significant differences between the background characteristics of the two groups. Based on a two-year follow-up of parole outcomes, the research found that the addict control group had a significantly higher (p <.05) recommitment rate (30 percent) than the program graduate group (18 percent). Furthermore, the percentage of individuals who remained arrest free was significantly higher among program graduates (51 percent) than in the control group (34 percent).
The Terminal Island Drug Treatment Program
The Terminal Island program was established under Title II of the Narcotic Addiction Rehabilitation Act (NARA), which authorized federal judges to commit convicted felons to prison drug treatment programs after an examination had determined that they were addicts who could be rehabilitated. In 1968 a drug treatment program was established at the federal correctional facilities on Terminal Island and at two other institutions. The program consisted of several components: a therapeutic community, psychotherapy and counseling, biofeedback training, a transactional analysis group, and educational, vocational, and social activities. An aftercare component ensured that a plan would be developed for parole supervision (including continued therapy, job or educational placement, assignment to a halfway house, and urinalysis).
Although legislative authority for the NARA program was repealed during the mid-1980s, evaluation studies garnered support for the program while it was in operation. Compared with the general federal prison population, inmates in the program were younger (25 years old on average), less educated (10 years), less employable (90 percent were unskilled), more heavily involved in drugs (heroin use averaging five years), and more likely to be recidivists (20 percent had previously violated parole) (Chaiken, 1989). Although the design of the evaluation research did not compare the treatment group with a control group, there is evidence to support the contention that the treatment reduced recidivism. The reincarceration rate for the Terminal Island group was only 31 percent after three years. More than half the NARA inmates in another institution were reincarcerated during the same time frame, and studies of recidivism rates among federal parolees (not in treatment) have been found to be even higher (Glaser, 1965).
The efficacy of the therapeutic community as a modality suitable for the treatment of inmates is further substantiated by a study conducted by Nash (1975). In this evaluation, changes in arrest rates for a total of 173 inmates who attended seven prison-based drug programs were assessed. Four of these programs were TCs based on the original Synanon model, two were counseling programs, and one was a drug-free residential program. The original study by Nash did not find significant differences in arrest rates between any of the programs and a comparison group; however, a more extensive analysis of the data by Des Jarlais and Wexler (1979) found that two of the four TCs did significantly better than the comparison groups.
Community-Based Drug Treatment
A review of community-based drug treatment programs gives insight into the types of interventions that are likely to be effective for prisoners and parolees. A major national study that supported the efficacy of residential drug treatment was the Drug Abuse Reporting Program (DARP). This research study collected data on a sample of approximately 44,000 drug abusers admitted to 52 drug treatment programs between 1969 and 1973 (Simpson, 1984; Simpson and Sells, 1982). Outcome studies of two cohorts (subsamples interviewed at 6- and 12-year follow-up intervals) were conducted (Simpson and Friend, 1988).
The major findings relevant to the issue of prison-based drug treatment are as follows. Favorable outcomes (i.e., reductions in drug use and criminality) were associated with therapeutic communities, methadone maintenance, and drug-free outpatient treatment. About 28 percent of the TC group showed highly favorable outcomes, that is, no illicit drug use (except less than daily marijuana use) and no arrests or incarcerations. About 40 percent of the TC group had moderately favorable outcomes (no daily use of illicit drugs, not more than 30 days in jail, and no arrests for crimes of violence or property crimes). The outcomes for the TC group were not significantly different from those of the methadone maintenance or drug-free outpatient treatments, but they were significantly more favorable than detoxification.
Follow-up studies have also been conducted in the Treatment Outcome Prospective Study (TOPS), which is based on a sample of 11,750 clients admitted to treatment between 1979 and 1981 (Hubbard et al., 1984, 1988). TOPS also evaluated the outcomes of each of the drug modalities discussed above. According to Hubbard and colleagues, "[t]he largest changes in predatory illegal activity occurred for residential clients. Where 60 percent reported at least one act in the year before TOPS treatment, only about one third reported activity in the year after treatment" (Hubbard et al., 1984:60).
Although a small percentage of long-term methadone clients and outpatient drug-free clients reported illegal activities in the year after treatment (about 20 percent each), the decline in the percentage of clients engaging in illegal activities was greatest after treatment in residential programs. Criminal justice system referrals stayed in treatment longer than clients with no legal involvement, and clients who stayed in residential programs longer than six months had significantly lower recidivism rates than clients who dropped out of treatment earlier.
TCs such as Phoenix House have been effective in curbing drug use and crime among clients with extensive histories of antisocial behavior. Phoenix House is one of the oldest and largest concept-based TCs. The
pioneering research efforts at Phoenix House under the leadership of George De Leon have set a model for the field and produced a prolific body of work that has been influential in gaining recognition of TC effectiveness (De Leon, 1984; De Leon et al., 1972; De Leon et al., 1979). The program has recognized the dual importance of maintaining ex-addict leadership and opening the process to meaningful research that would enhance the program without compromising its treatment efforts. The Phoenix House research is of particular importance because the Stay'n Out prison TC program (described previously) was founded by a Phoenix graduate and is a modification of the Phoenix approach.
The major Phoenix outcome research study included two cohorts (N = 731) which were samples of the 1970-1971 and 1974-1975 residential populations (De Leon, 1984). The use of two samples adds power to the findings because the results are replicated across groups. The findings for both groups were quite similar; therefore, our summary is limited to the more recent cohort (1974-1975). This cohort included graduates and dropouts who were followed up to two years after treatment.
Comparisons were made between the year prior to treatment and the second year of the follow-up period. Drug use showed dramatic declines: among graduates, opiate use decreased to zero from 66 percent prior to treatment, and dropouts also showed a decrease from 67 to 18 percent. Moreover, there was a significant decline in criminality: the percentage of graduates reporting arrests decreased from 55 percent pretreatment to 3 percent during the second year posttreatment, and dropouts decreased from 37 to 18 percent. Furthermore, the research found improvements in employment and posttreatment measures of psychological adjustment that were correlated with positive behavior changes. The positive changes in posttreatment behavior were generally correlated with time spent in treatment.
WHAT WORKS AND WHAT DOES NOT WORK IN PRISON-BASED TREATMENT
Based on evaluation studies of effective treatment programs and observation of clinical practices, it is possible to identify several elements of treatment programs that tend to work well and others that have been found not to work. This section describes the forces that impede success and the factors conducive to it. As new programs are implemented, further research should be conducted to determine whether the current state of knowledge stands up to more rigorous scientific scrutiny. Based on the factors related to success, we set forth several guidelines we believe should be followed in establishing treatment programs for prisoners and
parolees. Finally, we briefly describe a national program (sponsored by the Bureau of Justice Assistance) that has adopted these guidelines to foster the development of drug treatment in corrections.
Impediments to Prison-Based Drug Treatment
Broadly defined, there are two sets of forces that impede successful treatment outcomes (i.e., reduction of recidivism). The origin of one set is external to the program and may best be characterized as institutional resistance; the other emanates from within the program and is primarily related to intervention techniques.
The institutional environment plays a large role in shaping the quality of treatment. A lack of support from correctional administrators and officers can easily hamper a program. Many programs are met with hostility on the part of correctional authorities during their early stages. Indeed, program residents and staff often complain about the tactics used by correctional staff to sabotage their program (e.g., requiring a count of inmates in the middle of a group therapy session). In addition, inmates are often skeptical about rehabilitation programs. Perhaps more important is the pervasive, insidious, antisocial inmate code, which is antithetical to treatment and which, will, if not effectively dealt with, inevitably undermine even the most promising of therapeutic approaches. The easiest and least costly method for dealing with the inmate subculture is to establish separate treatment units that isolate clients from the general prison population. Usually the first task treatment staff must undertake is to break down the attitude of machismo and confront the disruptive behavior of inmates when they enter treatment.
Perhaps more significant is that certain structural characteristics of treatment interventions are prone to failure. These factors are related primarily to the theoretical basis of the treatment and its attitude toward offenders. Evaluation studies have found several rehabilitation approaches to be unsuccessful (for a detailed review, see Gendreau and Ross, 1983-1984, 1987). Interventions based on deterrence models (such as "Scared Straight" programs, which attempt to instill fear) have shown very limited effects, and some have been associated with increased offending. On the other hand, counseling programs based on a model of trust (e.g., counselors who treat clients as "friends" or permit inmates to run therapy groups) are also counterproductive. Finally, there is no evidence to support the contention that programs based on a disease model work. Following a review of several studies, Gendreau and Ross concluded, "[w]hether the disease is some form of psychopathology or biological deficit (e.g., extra chromosomes), we have not found one well controlled positive
report. . ." (1983-1984:34).
The lack of success of these treatment models stems from the failure of the programs to strike a balance between recognizing the antisocial behaviors of clients and emphasizing the development of prosocial conduct. Behavioral programs that are imposed without involving inmates in their development do not work as well as those that do involve inmates. Such programs are often targeted at antisocial rather than prosocial behaviors, which gives undue attention and reinforcement to negative behavior.
Programs that either fail to neutralize the inmate code (e.g., by recruiting inmate leaders into treatment or housing the program in a unit separated from the general prison population) or to utilize inmate peer pressure in a positive way (e.g., through encounter groups that encourage confrontation) tend to be unsuccessful Other factors that tend to inhibit success are a lack of well-trained, dedicated staff, insufficient resources, and a lack of aftercare services. Indeed, recidivism rates are higher when there is no continuity of care, that is, when the treatment begun in prison is not sustained after inmates return to the community. In conclusion, drug treatment programs that do not overcome resistance from external forces and do not tailor treatment to the characteristics peculiar to prison inmates tend to be unsuccessful.
Elements of Effective Correctional Treatment Programs
Although the number of studies of effective treatment programs is limited, there is enough evidence to suggest that certain approaches are conducive to success. In general, the main factors related to success are as follows: (1) treatment is based on a social learning theory of behavior, (2) programs offer an array of treatment options appropriate to the needs of offenders, (3) relationships are built to engender respect for the program, and (4) the integrity and authority of treatment staff are emphasized. Each of these factors is discussed briefly in the following paragraphs; a set of guidelines for implementing treatment in corrections is suggested in the next section (for a detailed discussion, see Lipton, 1989, 1990; Wexler et al., 1988a).
In contrast to the treatment models that have not been found effective, the majority of successful community-based and prison-based programs are founded on a social learning theory of criminal behavior (see Bandura, 1979; Nietzel, 1979). This theory suggests that criminal behavior is learned through a process of social interaction; treatment, therefore, develops prosocial behaviors by improving interpersonal relations. Effective interventions include self-help approaches (such as therapeutic communities),
family therapy, contingency contracting, role playing and modeling, vocational and social skills training, interpersonal cognitive problem-solving skills training, and peer-oriented behavioral programs (Gendreau and Ross, 1983-1984, 1987). An important point is that none of these techniques have been found to be superior; rather, most successful programs combine several approaches. Common to them all is that antisocial attitudes and behaviors are altered by reinforcing prosocial behaviors. A final note is that some evidence exists that techniques based on the theories of relapse prevention and self-efficacy enhance success (Annis and Davis, 1987; Bandura, 1977; Brownwell et al., 1986). These theories are especially relevant to prison-based treatment in that they focus the intervention on the reasons why inmates relapse and instill confidence that inmates can cope with problems after release—they also justify the need for continuity of care.
Although some approaches such as drug education or occasional counseling may be adequate for certain inmates (i.e., those with little prior involvement with drugs), offenders who exhibit serious lifestyle problems (in particular, chronic polydrug abuse and extensive involvement in crime) require comprehensive and intensive treatment. Programs that have been successful in treating serious offenders include a variety of components, such as encounter groups, individual counseling, drug education, and specialty groups (which focus on specific topics such as anger management, the problems of adult children of alcoholics, and stress reduction techniques). These programs tend to emphasize the development of problem-solving capabilities. They are generally quite intensive; that is, inmates live together and their shared experiences become the subject of discussion at regularly scheduled group therapy sessions. Program residents have access to staff when needed, and the programs are designed to keep inmates in treatment for an adequate duration (usually more than six months).
A critical factor influencing the success of programs is the nature of the relationships built by staff with prison authorities, nonprogram inmates, and program residents. Success in this area requires good public relations and diplomacy. Care must be taken to demonstrate the integrity of the program to prison officials and general population inmates. Respect and trust are developed by finding a balance between a treatment attitude (which requires empathy and caring) and a corrections ethos (which emphasizes institutional authority). The support of correctional authorities depends very much on their belief that the program maintains security. When programs create a safe environment for their residents (including psychological as well as physical safety), they can focus their attention on treatment, and the number of inmates requesting admission tends to increase.
The success of treatment programs in correctional settings also
depends on the degree of integrity and authority they exhibit. Program integrity requires a commitment to the goals of the program, effective leadership, and competent staff (Quay, 1977; Sechrest et al., 1979). Successful programs have capable directors who provide adequate supervision to well-trained staff. They are able to establish credible authority by clearly setting forth the rules of the program and treating violations with appropriate consequences.
Guidelines for Effective Treatment
Based on the evaluation research and our observation of clinical practices, we have elsewhere suggested a strategy for treating substance-abusing offenders (Wexler et al., 1988a). The following are several guidelines for implementing drug treatment programs for prisoners and parolees.
-
Programs should emphasize a self-help approach. Therapeutic communities such as Stay'n Out are based on this philosophy. Although compulsory participation may be required for some offenders (and evaluations of community-based programs have found that legal pressure increases client retention), we believe that persuasion is a better strategy. Offering incentives to join (e.g., early release for successful program completion, better living conditions, a safer environment) and allowing inmates to participate in the operation of the program foster the self-help process. Successful programs include inmates in program development and involve them in virtually all aspects of the recovery process.
-
Corrections should establish a variety of treatment options appropriate to the needs of offenders. A sequence of interventions should be planned. These include diagnostic tests as part of intake procedures, assignment to programs based on level of need (e.g., drug education, counseling, intensive treatment, aftercare), and case reviews and reassignment based on client progress. Treatment plans developed through consultation between clients and their counselors clarify goals and expectations and structure the recovery process.
-
Although the vast majority of inmates are in need of some form of treatment, resources should be directed first toward the minority that are chronic polydrug abusers. These offenders account for a disproportionate amount of crime; they commit hundreds of serious crimes each year. As discussed earlier, intensive prison-based treatment programs (such as Stay'n Out and Cornerstone) have been able to prolong the time that parolees remain crime free as well as reduce the likelihood that they recidivate. Thus, a cost-effective strategy would involve high-rate offenders
-
in intensive treatment programs while engaging prisoners with less severe drug problems in less costly interventions. It is essential, however, that these programs address the overall lifestyle problems of their clients and not merely their substance abuse.
-
Residential prison-based treatment programs should be allocated a separate unit to minimize the harmful effects of the inmate subculture and code.
-
Programs should establish and enforce a clearly articulated set of rules and rewards. Successful programs respond to the violation of cardinal rules (e.g., violence, sexual activity) with immediate dismissal. Developing a hierarchy of rules (e.g., some dealing with actions that affect security, others dealing with conduct during therapy groups) allows correctional officials to decide on sanctions for infractions that relate to security while permitting program residents to be responsible for conduct within the group. Progress in treatment and good conduct in the program should be rewarded with increased privileges while in the institution.
-
Program staff should include ex-offender/ex-addicts. Graduates of treatment programs who are able to remain drug free and to abstain from crime while in the community serve as excellent role models. After adequate training, they should be offered opportunities for employment in community-and prison-based treatment programs.
-
For many offenders, prison-based treatment should be followed by treatment in the community. This can be in the form of intensive supervision, prerelease to a halfway house that offers drug counseling, or residence in a therapeutic community program. The possible use of drugs should be monitored by regular urinalysis. Incentives in the form of increased liberty can be given to parolees who do not violate the conditions of their parole.
-
Coordination between prison authorities and aftercare providers is essential. Continuity of care should be built into the design of prison-based programs. The concept of ''aftercare'' has fostered the belief that prison-based treatment and community-based treatment are separate functions. Although responsibility for prisoners and parolees may reside with different correctional authorities, effective treatment for offenders requires that they operate in tandem. Thus, prison treatment staff should develop reentry plans with parole officers a few months before release. Coordination with self-help groups (e.g., Alcoholics Anonymous, Narcotics Anonymous) is also necessary.
-
Evaluations of treatment programs should be integrated into the design of the programs. The evaluations should focus on implementation issues and the effects on outcome variables. There are models for conducting such evaluation research (see, for example, Wexler et al., 1988b).
PROJECT REFORM: A NATIONAL PROJECT TO ESTABLISH DRUG TREATMENT PROGRAMS IN CORRECTIONS
Project REFORM (Comprehensive State Department of Corrections Treatment Strategy for Drug Abuse) was funded by the Bureau of Justice Assistance in July 1987 and attempts to develop drug treatment programs in corrections settings based on the guidelines described in the previous section. As such, this project provides a rare opportunity to bridge the realms of abstract concepts and concrete reality. Narcotic and Drug Research, Inc., was asked to serve as the national coordinator for the REFORM technical assistance project, with the goal of assisting states to plan for and then implement or expand statewide drug treatment and rehabilitation strategies in state departments of corrections.
The project provides funding, guidance, technical assistance, training, and monitoring for two phases: (1) a planning phase (lasting 6 months to a year) in which a comprehensive state plan for correctional substance abuse treatment is developed; and (2) an implementation phase (approximately 18 months) for states that successfully complete the planning phase. Currently, seven states (Alabama, Connecticut, Delaware, Florida, New Mexico, New York, and Oregon) have completed the planning phase and are engaged in implementation; California, Hawaii, New Jersey, and Washington are currently participating in the planning phase.
Overall, then, this program assists states in developing a comprehensive set of drug treatment programs through a statewide correctional strategy for dealing with drug offenders. The strategies are developed on the basis of research that has demonstrated effective models of drug treatment. A major goal of the project is to reduce recidivism; other goals relate broadly to improving drug treatment in corrections. A major target group of the project is inmates with chronic drug abuse problems.
CONCLUSION: THE FUTURE OF DRUG TREATMENT IN CORRECTIONS
The trend in corrections during recent years has been for more prisoners to receive some form of drug treatment. Because policymakers and the public are concerned about drug abuse and crime, it is likely that this trend will continue. In this conclusion, we suggest a direction for the future that is likely to be a constructive, if only partial, solution to the crime problem.
The complexity of the problem and the limitations in both the current state of knowledge and practice suggest that a period of experimentation
with treatment interventions is needed and that new techniques should be thoroughly evaluated. The guidelines presented earlier represent our best judgment as to what approaches offer promise for the future of correctional drug treatment. Our assessment of the situation, however, is constrained by the fact that the evidence of effective interventions is limited, as is the current state of the art in correctional treatment. Accordingly, corrections should expand on what currently works, and it should attempt innovative approaches in the future. These interventions should be carefully evaluated so that drug treatment in correctional settings can be modified based on the best available scientific knowledge.
As our guidelines suggest, a logical starting point is to increase the number of chronic polydrug abusers in intensive prison-based treatment programs and enable them to continue their recovery in residential programs after they are released. Currently, corrections offers a variety of treatment options, such as Alcoholics Anonymous meetings, counseling, and drug education. We need to know much more about the effectiveness of these and other approaches. In particular, what kinds of treatment are appropriate for different types of offenders? Moreover, emphasis should be placed on developing cooperation between drug treatment providers and custodial staff. This effort can be assisted, for example, by cross-training treatment staff in security and correctional officers in treatment. Coordination between correctional treatment providers and other human services providers (educational, vocational, medical, social, and psychological) needs to be improved. Similarly, community resources need to be mobilized and integrated into an improved continuity of care system.
In addition to expanding on current practice, new program innovations should be attempted. For example, there is some evidence that shock incarceration is effective with youthful offenders (MacKenzie and Shaw, 1988); combining shock incarceration with an intensive drug treatment program for addicts might be a valuable approach. New techniques in intensive parole supervision can also be implemented. Developments in community-based drug treatment should be considered for their possible inclusion in correctional settings. Chemotherapy treatment is another possibility. For example, research currently under way at a methadone program in the jail on Rikers Island suggests that this might be an effective intervention (Magura et al., 1989). Although there are no methadone maintenance programs in prisons at this time, an experiment to see if such a program could stabilize heroin addicts in prison so that they can continue treatment in community-based programs after release might be worth trying.
Regardless of the specific innovations that are attempted, they must all be properly tested. Evaluation research should search especially for cost-effective strategies for reducing recidivism (that is, strategies that do
not negatively affect other policy goals such as maintaining security and controlling overcrowding). Our ability to reduce recidivism among drug users depends almost entirely on our ability to develop effective intervention techniques and our ability to reach agreement on which programs to fund.
ACKNOWLEDGMENT
This project was supported in part by Grants No. 87-DD-CX-K060 and 88DD-CX-0008 awarded by the Bureau of Justice Assistance, Office of Justice Programs, U.S. Department of Justice.
REFERENCES
Allison, M., and R.L. Hubbard (1985) Drug abuse treatment process: a review of literature. International Journal of the Addictions 20(9):1321-1345.
Anglin, M.D., and W.H. McGlothlin (1984) Outcome of narcotic addict treatment in California. In F.M. Tims and J.P. Ludford, eds., Drug Abuse Treatment Evaluation: Strategies, Progress and Prospects. NIDA Research Monograph 51. Rockville, Md.: National Institute on Drug Abuse.
Anglin, M.D., M.L. Brecht, J.A. Woodward, and D.G. Conett (1986) An empirical study of maturing out: conditional factors. International Journal of the Addictions 21:233-246.
Annis, H., and C.S. Davis (1987) Self-efficacy and the treatment trial. In T.B. Baker and D. Cannon, eds., Addictive Disorders: Psychological Research in Assessment and Treatment. New York: Praeger.
Bailey, W.C. (1966) Correctional outcome: an evaluation of 100 reports. Journal of Criminal Law, Criminology and Police Sciences 57:153-160.
Bale, R.N. (1979) Outcome research in a therapeutic community for drug abusers: a critical review . International Journal of the Addictions 14(8):1053-1074.
Ball, J.C. (1986) The hyper-criminal opiate addict. Pp. 81-104 in B.D. Johnson and E. Wish, eds., Crime Rates Among Drug Abusing Offenders: Final Report to the National Institute of Justice. New York: Narcotic and Drug Research, Inc.
Ball, J.C., L. Rosen, S.A. Flueck, and D.N. Nurco (1981) The criminology of heroin addicts when addicted and when off opiates. Pp. 39-65 in J.A Inciardi, ed., The Drugs-Crime Connection. Beverly Hills, Calif.:
Sage Publication.
Ball, J.C., L. Rosen, S.A. Flueck, and D.N. Nurco (1982) Lifetime criminality of heroin addicts in the United States. Journal of Drug Issues 3:225-239.
Ball, J.C, J.W. Shaffer, and D.N. Nurco (1983) Day to day criminality of heroin addicts in Baltimore—a study in the continuity of offense rates. Drug and Alcohol Dependence 12:119-142.
Bandura, A. (1977) Self-efficacy: toward a unifying theory of behavioral change. Psychological Review 94:191-215.
Bandura, A. (1979) Social Learning Theory. Englewood Cliffs, N.J.: Prentice-Hall.
Barton, W.I. (1974) Drug abuse histories and criminality survey of inmates of state correctional facilities. International Journal of the Addictions 15:233-258.
Brewington, V., L. Arella, S. Deren, and J. Randell (1987) Obstacles to the utilization of vocational services: an analysis of the literature. International Journal of the Addictions 22(11):1091-1118.
Brownwell, D.D., G.A. Marlatt, E. Lichtenstein, and G.T. Wilson (1986) Understanding and preventing relapse. American Psychologist 41:765-782.
Bureau of Justice Statistics (1983) Prisoners and Drugs. Washington, D.C.: U.S. Department of Justice.
Chaiken, M.R. (1986) Crime rates and substance abuse among types of offenders. In B.D. Johnson and E. Wish, eds., Crime Rates Among Drug-Abusing Offenders: Final Report to the National Institute of Justice. New York: Narcotic and Drug Research, Inc..
Chaiken, M.R. (1989) Prison Programs for Drug-Involved Offenders. Washington, D.C.: National Institute of Justice.
Chaiken, J.M., and M.R. Chaiken (1982) Varieties of Criminal Behavior. Santa Monica, Calif.: The Rand Corporation.
Chaiken, J., and M. Chaiken (1983) Crime rates and the active offender. Pp. 11-29 in J.Q. Wilson, ed., Crime and Public Policy. New Brunswick, NJ.: Transaction Books.
Chaiken, M.R., and B.D. Johnson (1988) Characteristics of Different Types of Drug Involved Offenders. Washington, D.C.: National Institute of Justice.
Collins, JJ., R.L. Hubbard, and J.V. Rachal (1985) Expensive drug use in illegal income: a test of explanatory hypotheses. Criminology 23(4):743-764.
Cullen, F., and P. Gendreau (1989) The effectiveness of correctional rehabilitation. In L. Goodstein and D.L. MacKenzie, eds., The American Prison: Issues in Research Policy. New York: Plenum.
De Leon, G. (1979) The therapeutic community: study of effectiveness.
Internal report submitted to the National Institute on Drug Abuse, Rockville, Md.
De Leon, G. (1984) The Therapeutic Community: Study of Effectiveness. Treatment Research Monograph Series. Rockville, Md.: National Institute on Drug Abuse.
De Leon, G. (1985) The therapeutic community: status and evolution. International Journal of the Addictions (20)6-7:823-844.
De Leon, G., and J. Ziegenfuss, Jr. (1986) Therapeutic Communities for Addictions. Springfield, Ill.: Charles C Thomas.
De Leon, G., S. Holland, and M.S. Rosenthal (1972) Phoenix House: criminal activity of dropouts. Journal of the American Medical Association 226(6):686-689.
De Leon, G., M. Andrews, H.K. Wexler, J. Jaffe, and M.S. Rosenthal (1979) Therapeutic community dropouts: criminal behavior five years after treatment. Drug and Alcohol Abuse 6(3):253-271.
Des Jarlais, D., and H.K. Wexler (1979) Internal Report for the New York State Division of Substance Abuse Services, Albany.
Duguid, S. (1987) University Prison Education in British Columbia. Burnaby, B.C.: Simon Fraser University.
Field, G. (1984) The cornerstone program: a client outcome study. Federal Probation 48:50-55.
Field, G. (1989) A study of the effects of intensive treatment on reducing the criminal recidivism of addicted offenders. Federal Probation 53(10):51-56.
Gandossy, R.P., J.R. William, J. Cohen, et al. (1980) Drugs and Crime: A Survey and Analysis of the Literature. National Institute of Justice Report. Washington, D.C.: U.S. Department of Justice.
Gendreau, P. (1981) Treatment in corrections: Martinson was wrong. Canadian Psychology 22:332-338.
Gendreau, P., and R.R. Ross (1979) Effective correctional treatment: bibliography for cynics. Crime and Delinquency 25(4):463-489.
Gendreau, P., and R.R. Ross (1983-1984) Correctional treatment. Some recommendations for successful intervention. Juvenile and Family Court Journal 34:31-39.
Gendreau, P., and R.R. Ross (1987) Revivification of rehabilitation: evidence from the 1980s. Justice Quarterly 4(3):349-407.
Glaser, D. (1965) The Effectiveness of a Prison and Parole System. Indianapolis, Ind.: Bobbs-Merrill.
Goldstein, P.J. (1981) Getting over: economic alternatives to predatory crime among street drug users. Pp. 67-84 in J.A. Inciardi, ed., The Drugs/Crime Connection. Beverly Hills, Calif.: Sage Publications.
Goldstein, P.J. (1985) The drugs/violence nexus: a tripartite conceptual framework. Journal of Drug Issues Fall:493-506.
Goldstein, P.J. (1985) Drugs and violent crime. Pp. 16-48 in N.A. Weiner and M.E. Wolfgang, eds., Pathways to Criminal Violence. Beverly Hills, Calif.: Sage Publications.
Goldstein, P.J., H.H. Brownstein, P.J. Ryan, and P.A. Bellucci (1989) Crack and Homicide in New York City, 1988: A Conceptually-Based Event Analysis. New York: Narcotic and Drug Research, Inc.
Goldstein, P.J., P.A. Bellucci, B. Spunt, and T. Miller (1990) Frequency of Cocaine Use and Violence: A Comparison Between Men and Women. New York : Narcotic and Drug Research; Inc.
Greenwood, P.W., and F.E. Zimring (1985) One More Chance: The Pursuit of Promising Intervention Strategies for Chronic Juvenile Offenders. Santa Monica, Calif.: The Rand Corporation.
Gropper, B.A. (1985) Probing the Links Between Drugs and Crime. Washington, D.C.: U.S. Department of Justice.
Hubbard, R.L., J.V. Rachel, S.G. Craddock, and E.R. Cavanaugh (1984) Treatment outcome prospective study (TOPS): client characteristics and behaviors before, during, and after treatment. Pp. 29-41 in F.M. Tims and J.P. Ludford, eds., Drug Abuse Treatment Evaluation: Strategies, Progress and Prospects. NIDA Research Monograph 51. DHHS Pub. No. (ADM) 84-1349. Rockville, Md.: National Institute on Drug Abuse.
Hubbard, R.L, J.J. Collins, J.V. Rachel, and E.R. Cavanaugh (1988) The criminal justice client in drug abuse treatment. Pp. 57-80 in C.G. Leukefeld and F.M. Tims, eds., Compulsory Treatment of Drug Abuse: Research and Clinical Practice. NIDA Research Monograph 86. Rockville, Md.: National Institute on Drug Abuse.
Hunt, D.E., D.S. Lipton, and B. Spunt (1984) Patterns of criminal activity among methadone clients and current narcotics users not in treatment. Journal of Drug Issues Fall:687-702.
Hunt D.E., B.J. Spunt, D.S. Lipton, D.S. Goldsmith, and D.L. Strug (1986) The costly bonus: cocaine related crime among methadone treatment clients. Advances in Alcohol and Substance Abuse 6(2, Winter):107-122.
Inciardi, J.A. (1979) Heroin use and street crime. Crime and Delinquency 25(3):335-346.
Innes, C.A. (1988) Profile of State Prison Inmates: 1986. Bureau of Justice Statistics Special Report. Washington, D.C.: U.S. Department of Justice.
Johnson, B.D., P. Goldstein, E. Preble, J. Schmeidler, D.S. Lipton, B. Spunt, and T. Miller (1985) Taking Care of Business: The Economics of Crime By Heroin Abusers. Lexington, Mass.: Lexington Books. Johnson, B.D., D.S. Lipton, and E.D. Wish (1986) Facts About the Criminality of Heroin and Cocaine Abusers and Some New Alternatives
to Incarceration. New York: Narcotic and Drug Research, Inc.
Johnson, B.D., T. Williams, K.A. Dei, and H. Sanabria (in press) Drug abuse in the inner city: impact on hard-drug users and the community. In J.Q. Wilson and M Tonry, eds., Drugs and Crime. Crime and Justice Series, Vol. 13. Chicago: University of Chicago Press.
Kalish, C.B., and W.T. Masumura (1983) Prisoners and Drugs. Bureau of Justice Statistics Bulletin. Washington, D.C.: U.S. Bureau of Justice.
Kassebaum, G., D. Ward, and D. Wilner (1971) Prison Treatment and Parole Survival: An Empirical Assessment. New York: John Wiley & Sons, Inc.
Leukefeld, C.G., and F.M. Tims (1988) Compulsory Treatment of Drug Abuse: Research and Clinical Practice. NIDA Research Monograph 86. Rockville, Md.: National Institute on Drug Abuse.
Lipton, D. (1983) Important conditions for successful rehabilitation. Paper presented at the Bellevue Forensic Psychiatry Conference, New York City.
Lipton, D.S. (1989) The Prevention of Recidivism: A Manifesto Regarding the Role of Rehabilitation for Drug Abusing Offenders. New York: Narcotic and Drug Research, Inc.
Lipton, D.S. (1990) Principles of successful correctional intervention. Paper presented at the Bureau of Justice Statistics/State Justice Institute Regional Seminar: Drugs and the Judicial Response, Washington, D.C.
Lipton, D.S., and H.K. Wexler (1988) Breaking the drug-crime connection—rehabilitation projects show promise. Corrections Today 50(5):144-147.
Lipton, D., R. Martinson, and J. Wilks (1975) The Effectiveness of Correctional Treatment. New York: Praeger Publishers.
Magura, S., H. Joseph, and A. Rosenblum (1989) Methadone Maintenance in the New York City Jails. New York: Narcotic and Drug Research, Inc.
Macdonald, D.G., and K. Canestrini (1987) Follow-up Study of a Sample of Participants in the Stay'n Out Drug Program. Albany, N.Y.: New York State Department of Correctional Services.
MacKenzie, D.L., and J.W. Shaw (1988) Inmate adjustment and change during shock incarceration. Paper presented at a meeting of the American Society of Criminology, Chicago.
Maltz, M.D. (1984) Recidivism. Orlando, Fla.: Academic Press, Inc.
Martinson, R. (1974) What works? Questions and answers about prison reform. The Public Interest 35:22-45.
Martinson, R. (1979) New findings, new views: a note of caution
regarding sentencing reform. Hofstra Law Review 7:243-258.
McBride, D. (1981) Drugs and violence. In J.A Inciardi, ed., The Drugs/Crime Connection. Beverly Hills, Calif.: Sage Publications.
McGlothlin, W.C., D.M. Anglin, and B.D. Wilson (1977) An Evaluation of the California Civil Addict Program. Rockville, Md.: National Institute on Drug Abuse.
McGlothlin, W.H., M.D. Anglin, and D.B. Wilson (1978) Narcotic addiction and crime. Criminology 16:293-315.
Nash, G. (1973) The Impact of Drug Abuse Treatment Upon Criminality: A Look at 19 Programs. Upper Montclair, N.J.: Montclair State College.
National Institute of Justice (1988) Drug Use Forecasting (DUF): April Through June 1988 Data. Washington, D.C.: U.S. Department of Justice.
National Institute on Drug Abuse (1981) Drug Abuse Treatment in Prisons. Treatment Research Report Series. DHHS Pub. No. (ADM) 81-1149. Rockville, Md.: National Institute on Drug Abuse.
New York City Police Department (1983) Homicide analysis: 1981. New York.
New York State Division of Substance Abuse Services (1980) Prison drug program evaluation report. Albany, New York.
Nietzel, M.T. (1979) Crime and Its Modification: A Social Learning Perspective. Elmsford, N.Y.: Pergamon Press.
Palmer, T. (1975) Martinson revisited. Journal of Research in Crime and Delinquency 12:133-152.
Platt, J., C. Labate, and R. Wicks (1977) Evaluative Research in Correctional Drug Treatment. Lexington, Mass.: Lexington Books.
Platt, J.J., G.M. Perry, and D.S. Metzger (1980) The evolution of a heroin addiction treatment program within a correctional environment. In R.R. Ross and P. Gendreau, eds., Effective Correctional Treatment. Toronto: Butterworths.
Public Agenda Foundation (1987( Crime and Punishment: The Public's View. New York: Edna McConnell Clark Foundation.
Quay, H.C. (1977) The three faces of evaluation: what can be expected to work? Criminal Justice and Behavior 4:341-354.
Ross, R.R., and P. Gendreau (1980) Effective Correctional Treatment. Scarborough, Ont.: Butterworths.
Ross, R.R, E.A. Fabiano, and H.B. McKay (1978) Treatment in corrections: requiem for a panacea. Canadian Journal of Criminology 20:279-295.
Sechrest, L, S.O. White, and E.D. Brown (1979) The Rehabilitation of Criminal Offenders: Problems and Prospects. Washington, D.C.: National Academy of Sciences.
Sells, S.B., D. Simpson, G. Joe, R. Demaree, L. Savage, and M.A. Lloyd (1976) National follow-up study to evaluate the effectiveness of drug abuse treatment: A report of cohort 1 of the DARP five years later. American Journal of Drug and Alcohol Abuse 3(4):545-556.
Shearer, A, and J.B. Moore (1978) Personality dimensions of felonious probationers in Texas. Paper presented to the American Society of Criminology, Dallas, Texas.
Simpson, D.D. (1979) The relation of the time in drug abuse treatment to post treatment outcomes. American Journal of Psychiatry 136:1449-1453.
Simpson, D.D. )1980) Follow-up Outcomes and Length of the Time Spent in Treatment for Drug Abuse. Ft. Worth, Tex.: Institute of Behavioral Research, Texas Christian University.
Simpson, D.D. (1984) National treatment system evaluation based on the Drug Abuse Reporting Program (DARP) followup research. Pp. 2941 in F.M. Tims and J.P. Ludford, eds., Drug Abuse Treatment Evaluation: Strategies, Progress and Prospects. NIDA Research Monograph 51. DHHS Pub. No. (ADM) 84-1239. Rockville, Md.: National Institute on Drug Abuse.
Simpson, D.D., and J.H. Friend (1988) Legal status and long-term outcomes for addicts in the DARP followup project. Pp. 81-98 in C.G. Leukefeld and F.M. Tims, eds., Compulsory Treatment of Drug Abuse: Research and Clinical Practice. NIDA Research Monograph 86. Rockville, Md.: National Institute on Drug Abuse.
Simpson, D.D., and S.B. Sells (1982) Effectiveness of treatment for drug abuse: an overview of the DARP research program. Advances in Alcohol & Substance Abuse 2(1):7-29.
Speckart, G., and M.D. Anglin (1986) Narcotics use and crime: a causal modeling approach. Journal of Quantitative Criminology 2:3-28. Strug, D.L, E.D. Wish, B.D. Johnson, K. Anderson, and T. Miller (1984) The role of alcohol in the crimes of heroin abusers. Crime and Delinquency 30(4):551-567.
System Sciences, Inc. (1973) A comparative analysis of twenty-four therapeutic communities in New York City. Prepared for the Addiction Services Agency of the City of New York, December.
Tims, F.M., and J.P. Ludford (1984) Drug Abuse Treatment Evaluation: Strategies, Progress and Prospects. NIDA Research Monograph 51. DHHS Pub. No (ADM) 84-1349. Rockville, Md.: National Institute on Drug Abuse.
Toborg, M.A., J.B. Bellassai, A.M.J. Yezer, J. Carver, J. Clarke, and E. Pears (1986) The Washington, D.C. urine testing program for arrestees and defendants awaiting trial: a summary of interim findings. Toborg Associates, Washington, D.C.
Van Voorhis, P. (1987) Correctional effectiveness: the high cost of ignoring success. Federal Probation 51(March):56-62.
Vigdal, G.L., and D.W. Stadler (1989) Controlling inmate drug use: cut consumption by reducing demand. Corrections Today 51(3):96-97.
Wexler, H.K. (1986) Therapeutic communities within prisons. Pp. 227-237 in G. De Leon and J. Ziegenfuss, Jr., eds., Therapeutic Communities for Addictions. Springfield, Ill.: Charles C Thomas.
Wexler, H.K., and J. Chin (1981) Evaluation of a system to evaluate prison based drug treatment. Paper presented at the Eastern Evaluation Research Society Conference, Philadelphia.
Wexler, H.K., and V.A Lostlen (1979) Implementation of a prison therapeutic community for substance abusers: an environmental evaluation. Paper presented at the Eastern Psychological Association, Philadelphia.
Wexler, H.K, and R. Williams (1986) The Stay'n Out therapeutic community: prison treatment for substance abusers. Journal of Psychoactive Drugs 18(3):221-230.
Wexler, H.K., D.S. Lipton, and B.D. Johnson (1988a) A Criminal Justice System Strategy for Treating Cocaine-Heroin Abusing Offenders in Custody. Washington, D.C.: U.S. Department of Justice.
Wexler, H.K, G.P. Falkin, and D.S. Lipton (1988b) A Model Prison Rehabilitation Program: An Evaluation of the Stay'n Out Therapeutic Community. New York: Narcotic and Drug Research, Inc.
Wexler, H.K., G.P. Falkin, and D.S. Lipton (1990) Outcome evaluation of a prison therapeutic community for substance abuse treatment. Criminal Justice and Behavior 17(1):71-92.
Wish, E.D., E. Brady, and M. Cuadrado (1984) Drug use and crime in arrestees in Manhattan. Paper presented at the 47th Meeting of the Committee on Problems of Drug Dependence. Narcotic and Drug Research, Inc., New York.
Wish, E.D., and B.D. Johnson (1986) The impact of substance abuse on criminal careers. Pp. 52-58 in A. Blumstein et al., eds., Criminal Careers and Career Criminals, Vol. 2. Washington, D.C.: National Academy Press.












































