
1
Introduction
Why Use This Guidebook?
-
To help you deliver high quality nutritional care as a part of comprehensive health care for women before, during, and after pregnancy.
What Does the Guidebook Contain?
-
a sample nutrition questionnaire to identify women who may be at nutritional risk;
-
weight gain charts for pregnant women;
-
a chart of prenatal weight gain recommendations;
-
a body mass index (BMI) chart;
-
a table of cutoff values for anemia, with adjustments for cigarette smoking and altitude;
-
a chart of indications for vitamin/mineral supplementation;
-
clinical care outlines that equip the practitioner with items to check on, tips, and practical information by type of visit; and
-
supplementary information for delivering effective care.
Who Should Use This Guidebook?
-
Primary care providers who care for women in the preconceptional, prenatal, or postpartum periods—obstetricians, family practice physicians, pediatricians, midwives, nurse-practitioners, nurses, physicians' assistants, dietitians, and others.
-
Those involved in the education or training of the practitioners mentioned above.
Some of the care activities outlined here are carried out mainly by physicians or nurse-midwives. Other care providers refer to the medical record for related information.
Ways to Use This Book
-
Look in Tab 1 to find forms and charts to assist with basic nutritional assessment.
-
Look in Tabs 2-5 to find current recommendations for basic nutritional care before, during, and after pregnancy The bold italics identify sample questions and statements, and the “Explanatory Information" gives the rationale. Use the checklists at the beginning of these tabs as a ready reference.
-
Read through Part II (Tabs 6-10) for useful background information.
Tips for Using This Book
Skim the book to spark ideas for improving nutritional care and to locate sections of special interest. Apply durable tape to the first tab in each section to make the tabs easier to use. Consider using the entire book as a step-by-step guide for integrating nutrition into health care.
Approach
This guidebook encourages health care providers to build on the woman's strengths and reinforce the positive aspects of her diet while working to change behaviors that increase health risks for either the woman or her baby Regardless of the setting, the aim is for health care or its providers to have the following characteristics:
-
care structured for easy access and continuity;
-
providers familiar with the cultural backgrounds and social circumstances of the patients they serve;
-
providers aware that their own culture influences their attitudes toward patients and the delivery of services;
-
recommendations that consider the individual woman's needs, preferences, culture, and resources;
-
interactions that convey respect and concern for the woman; and
-
joint goal setting by the health care provider or team and the woman.
Terminology
In this guidebook, the term dietitian is used to represent a qualified nutrition professional, ordinarily a registered or a licensed dietitian or a nutritionist who is eligible for registration.
Dietitian Referral and Consultation
Enhanced nutrition services can be provided if the health care team includes a dietitian. In those instances in which a dietitian is not a member of the team, the subcommittee urges practitioners to make arrangements for outside referral to a dietitian if the woman needs specialized nutritional care. When such referral is impossible, consultation by the primary care provider with a dietitian is indicated. For more information on this, see the companion document Nutrition Services in Perinatal Care,5 which outlines the personnel requirements and the knowledge and skills needed to deliver nutrition services of varying degrees of complexity.
Record Keeping
Record keeping is a vital aspect of nutritional care delivery that is not covered explicitly in this guidebook. It varies depending on the type of record keeping system used and conventions at the health care facility.6 For example, the Popras III Form 1B (see POPRAS Ltd.7 includes easily identified places for recording most of the prenatal nutrition-related information, and the Hollister Prenatal Module includes similar items.8 The American
College of Obstetricians and Gynecologists antenatal record9 does not include specific items for recording some of the information, but the nonspecific items ("Other") could be used for documentation.
Introduction to the Nutrition Questionnaire
This nutrition questionnaire is intended to serve as an example of a useful tool that many women can complete on their own before meeting with the provider. Adaptations would be needed for many clinical settings. For example, it may be necessary to substitute the names of foods and beverages commonly consumed by a specific ethnic group. The questions are intended to be easy for women to answer even if they do not read or write very well. If a face-to-face interview is necessary because the woman cannot read, it is desirable to rephrase the questions to make them open-ended. For example, Question 2 "Do you skip meals at least 3 times a week?" becomes "How often do you skip meals?" and Question 5 becomes "What foods do you avoid for health or religious reasons?"
Although food intake on the previous day is often typical of usual intake, certain life events may make it atypical. This must be assessed (as in Question 13) and considered in interpreting yesterday's reported intake. Nonetheless, the foods circled on the questionnaire provide a useful starting point for identifying possible areas of dietary concern and the need for further face-to-face questioning.
The questionnaire is not meant to replace more extensive ones used in many practices. It is recommended primarily for practices that have not yet included a nutrition questionnaire as a part of routine health care. Guidelines for choosing more extensive approaches to dietary assessment are included in Tab 7, pages 97 to 100.
Nutritional Questionnaire
What you eat and some of the life-style choices you make can affect your nutrition and health now and in the future. Your nutrition can also have an important effect on your baby's health. Please answer these questions by circling the answers that apply to you.
Eating Behavior
|
1. |
Are you frequently bothered by any of the following? |
|||
|
(circle all that apply): |
||||
|
Nausea |
Vomiting |
Heartburn |
Constipation |
|
|
2. |
Do you skip meals at least 3 times a week? |
No |
Yes |
|
|
3. |
Do you try to limit the amount or kind of food you eat to control your weight? |
No |
Yes |
|
|
4. |
Are you on a special diet now? |
No |
Yes |
|
|
5. |
Do you avoid any foods for health or religious reasons? |
No |
Yes |
|
Food Resources
|
6. |
Do you have a working stove? |
No |
Yes |
|
|
Do you have a working refrigerator? |
No |
Yes |
|
7. |
Do you sometimes run out of food before you are able to buy more? |
No |
Yes |
|
8. |
Can you afford to eat the way you should? |
No |
Yes |
|
9. |
Are you receiving any food assistance now? |
No |
Yes |
|
|
(circle all that apply): |
||
|
Food stamps |
School breakfast |
School lunch |
|
|
WIC |
Donated food/commodities |
CSFP |
|
|
Food from a food pantry, soup kitchen, or food bank |
|||
|
10. |
Do you feel you need help in obtaining food? |
No |
Yes |
Food and Drink
|
11. |
Which of these did you drink yesterday? |
||
|
|
(circle all that apply): |
||
|
Soft drinks |
Coffee |
Tea |
Fruit drink |
|
Orange juice |
Grapefruit juice |
Other juices |
Milk |
|
Kool-Aid® |
Beer |
Wine |
Alcoholic drinks |
|
Water |
Other beverages (list) |
||
|
12. |
Which of these foods did you eat yesterday? |
|||
|
|
(circle all that apply): |
|||
|
Cheese |
Pizza |
Macaroni and cheese |
||
|
Yogurt |
Cereal with milk |
|||
|
Other foods made with cheese (such as tacos, enchiladas, lasagna, cheeseburgers) |
||||
|
Corn |
Potatoes |
Sweet potatoes |
Green salad |
|
|
Carrots |
Collard greens |
Spinach |
Turnip greens |
|
|
Broccoli |
Green beans |
Green peas |
Other vegetables |
|
|
Apples |
Bananas |
Berries |
Grapefruit |
|
|
Melon |
Oranges |
Peaches |
Other fruit |
|
|
Meat |
Fish |
Chicken |
Eggs |
|
|
Peanut butter |
Nuts |
Seeds |
Dried beans |
|
|
Cold cuts |
Hot dog |
Bacon |
Sausage |
|
|
Cake |
Cookies |
Doughnut |
Pastry |
|
|
Chips |
French fries |
|||
|
Other deep-fried foods, such as fried chicken or egg rolls |
||||
|
Bread |
Rolls |
Rice |
Cereal |
|
|
Noodles |
Spaghetti |
Tortillas |
||
|
Were any of these whole grain? |
No |
Yes |
||
|
13. |
Is the way you ate yesterday the way you usually eat? |
No |
Yes |
|
Life-Style
|
14. |
Do you exercise for at least 30 minutes on a regular basis (3 times a week or more)? |
No |
Yes |
|
15. |
Do you ever smoke cigarettes or use smokeless tobacco? |
No |
Yes |
|
16. |
Do you ever drink beer, wine, liquor, or any other alcoholic beverages? |
No |
Yes |
|
17. |
Which of these do you take? |
||
|
|
(circle all that apply): |
||
|
|
Prescribed drugs or medications |
||
|
|
Any over-the-counter products (such as aspirin, Tylenol®, antacids, or vitamins) |
||
|
|
Street drugs (such as marijuana, speed, downers, crack, or heroin) |
||
Interpretation of Nutrition Questionnaire
When looking over the woman's responses to the nutrition questionnaire, look at the items below for reasons for concern, sources of additional information, and suggested follow-up questions or actions. The numbers below match the question numbers.
Introduce the follow-up questions by telling the woman that: It would help us with planning your care if you would answer some additional questions.
Eating Behavior
1. Regardless of the responses on the questionnaire, ask: How has your appetite been recently?
At the initial prenatal visit, ask:
• Is_______ [symptom] keeping you from eating or from drinking liquids?
• What have you done to try to decrease _____ [these symptoms]? Has this helped?
Strategies for managing nausea and vomiting are on page 47; those for heartburn and constipation are on page 63.
2. Skipping meals one or more times daily, three or more times per week, may lead to inadequate nutrient intake or to the eating of large meals, which may cause discomfort.
3. If yes, ask, Do you sometimes feel that you can't stop eating? Women who consistently restrict their food intake to control weight may have difficulty changing to more appropriate eating habits to support a healthy pregnancy or may find they gain large amounts of weight when their eating becomes less restricted. Further assessment may be desirable.
4. If on a special diet, ask, What kind? Who told you to follow this diet? Women who require special diets benefit from referral to a dietitian. Self-imposed diets require further assessment.
5. If yes, ask, What foods do you avoid? Women who avoid major sources of nutrients may benefit from diet counseling or from vitamin/mineral supplementation or both. See supplement chart, page 17.
Food Resources
6-10. A "Yes" answer to Questions 7 or 10, or a "No" answer to Question 8 indicates the probable need to facilitate linkage with food assistance programs, income support programs, or both, especially if the woman is not receiving appropriate benefits. (See responses to Question 9 and check the medical record for information about public assistance, Medicaid, and unemployment insurance.) See Tab 10, pages 114-115, for information about food and nutrition programs.
Food and Drink
11. Soft drinks, coffee, tea, fruit drink, Kool-Aid®, and alcoholic beverages provide few essential nutrients and often crowd out better sources of nutrients. Milk is the only dependable food source of vitamin D. Orange juice is an important source of vitamin C and folate. Drinking of alcoholic beverages is not recommended for pregnant women or for women trying to conceive. Drinking of two to three servings of caffeinated beverages is unlikely to have adverse effects.
12. Foods that contain milk, cheese, or yogurt are all good sources of calcium, as well as many other minerals, protein, and vitamins. Many are also good sources of vitamin A. A calcium supplement is recommended for women who do not drink milk or do not eat one of these foods daily.
The vegetables listed are mainly those most commonly eaten across the United States. Carrots, spinach and other greens, sweet potatoes, and winter squash are very high in vitamin A. Asparagus, broccoli, avocados, okra, brussels sprouts, greens, and corn provide more folate per usual serving than do other vegetables. If no
vegetables other than potatoes or corn are eaten regularly, dietary guidance and vitamin/mineral supplementation may be appropriate.
The fruits listed are mainly those most commonly eaten across the United States. Citrus fruits and juices, strawberries, and cantaloupe are especially good sources of vitamin C and folate. If no juices or fruits are eaten regularly, dietary guidance and vitamin/mineral supplementation may be appropriate.
Meat, poultry, fish, eggs, and beans provide protein, iron, zinc, many other minerals, and vitamins.
Cold cuts, pastries, and deep-fried foods are all high in fat and calories. Frequent use of high-fat foods may crowd out better sources of nutrients.
Grains provide vitamins, minerals, protein, and energy without providing much fat. Whole grains are a source of fiber. Highly fortified cereals such as Total® and Special K® provide vitamins in amounts comparable to those in standard-strength vitamin pills.
See pages 27, 28, and 45 for information about dietary guidance.
13. If intake was not usual, ask: What was different about the way you ate yesterday? If a problem with diet is suspected, it is desirable to assess intake more thoroughly. (See Tab 7.)
Life-Style
14. Pregnant women need guidance concerning safe activity levels and may need encouragement to continue moderate exercise.
15-17. A "Yes" answer (indicating that the woman ever uses tobacco, alcoholic beverages, or street drugs) calls for questions to determine if any changes in behavior have been made already:
-
About how much did you use this past week?
-
Is this more or less than before?
-
Do you want to stop?
16. For women who ever drink alcoholic beverages, ask the next four questions.
-
How many drinks does it take to make you feel high?
-
Have people annoyed you by criticizing your drinking?
-
Have you felt you ought to cut down on your drinking?
-
Have you ever had a drink first thing in the morning to steady your nerves or get rid of a hangover?
A response to Question 16a of more than two drinks indicates tolerance to alcohol and is given 2 points. Score 1 point for each additional "Yes" answer. A score of 2 or more indicates an at-risk drinker.10
17. See follow-up material under Tab 2, pages 25 and 26, or Tab 3, page 42.
Charts for Assessing Weight
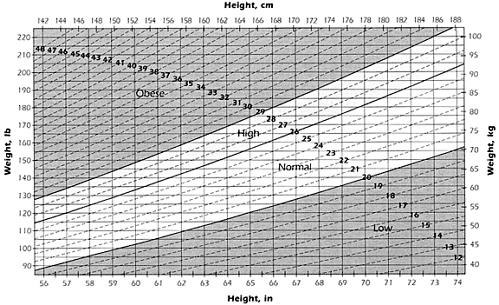
Body Mass Index
Use the chart on page 14 to estimate the woman's prepregnancy body mass index (BMI) category. Find the number that is closest to her height (inches are at the bottom margin, centimeters at the top). Then find the number closest to her weight (pounds are on the left, kilograms on the right). Now, find the point where the height and weight intersect. For example, a woman who is 65 inches tall and weighed 145 lb had a normal prepregnancy BMI—slightly higher than 24.
The chart below also gives the weight classifications and BMI ranges.1
|
Weight Gain During Pregnancy
Plot the pregnant woman's weight on the weight gain chart using one of the following methods. Use a colored pen to highlight the dashed line that corresponds to the woman's BMI category.
When prepregnancy weight is known: (1) write the woman's prepregnancy weight, rounded to the nearest pound, on the blank line to the left of the zero on the left-hand side of the grid; then mark an x at 0 gain for 0 weeks; (2) fill in the rest of the blanks along the left side of the grid, adding the prepregnancy weight to the weight gain shown at each horizontal line (for example, if the woman's prepregnancy weight was 121 lb, 126 lb is the prepregnancy weight plus a 5-lb gain, 131 lb is the prepregnancy weight plus a 10-lb gain, and so on); (3) at each subsequent visit, have the woman plot her current weight at the point corresponding to the number of weeks of gestation.
If prepregnancy weight is not known: (1) mark an x on the highlighted dashed line at the point that corresponds to the correct number of weeks of gestation; (2) move horizontally from that point to find the corresponding point on the vertical axis, which shows weight, and write the woman's current weight to the left of that point; (3) if the woman's initial weight does not fall on a horizontal line, estimate the number to write in the blank at the nearest horizontal line (add or subtract up to 2 lb); then fill in the rest of the blanks up the left side of the grid by adding 5 lb for each horizontal line.
Prenatal Weight Gain Chart
Prepregnancy BMI <19.8 (· · · · ·), prepregnancy BMI 19.8-26.0 (Normal Body Weight) (- - - - - -), Prepregnancy BMI >26.0 (— — —)
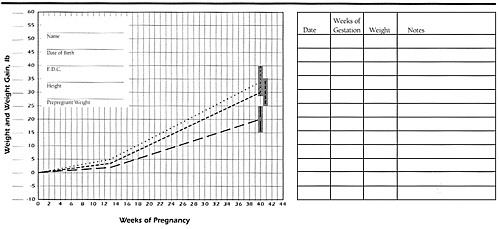
Adapted from Nutrition During Pregnancy.1
Laboratory Tests and Nutrient Supplements
The selection of supplements depends on the presence of anemia, as determined by analysis of hemoglobin or hematocrit, and the presence of risk factors, as determined by a history that includes diet and by physical examination. Begin routine iron supplementation for all pregnant women by the 12th week of gestation.
The taking of vitamin/mineral supplements does not lessen the need for the consumption of a nutritionally balanced diet, nor should it be used to replace nutrition education and counseling. Women should be cautioned about taking self-prescribed vitamins, minerals, or other supplements because of the potential of such supplements for producing nutrient imbalances, excesses, or toxicities.
TABLE 1. Cutoff Values for Anemia for Womena
|
Pregnancy Status |
Hemoglobin (g/dl) |
Hematocrit (%) |
|
|
Nonpregnant |
12.0 |
36 |
|
|
Pregnant |
|||
|
Trimester 1 |
11.0 |
33 |
|
|
Trimester 2 |
10.5 |
32 |
|
|
Trimester 3 |
11.0 |
33 |
|
|
a From CDC.11 See Tab 9, Table 3, for corrections for high altitude. |
|||
TABLE 2. Cutoff Values for Anemia for Women Who Smoke Cigarettesa,b
|
Cigarettes per day |
10-20 |
21-40 |
||
|
Pregnancy status |
Hgbc (g/dl) |
Hctd (%) |
Hgb (g/dl) |
Hct (%) |
|
Nonpregnant |
12.3 |
37 |
12.5 |
37.5 |
|
Pregnant |
||||
|
Trimester 1 |
11.3 |
34 |
11.5 |
34.5 |
|
Trimester 2 |
10.8 |
33 |
11.0 |
33.5 |
|
Trimester 3 |
11.3 |
34 |
11.5 |
34.5 |
|
a From CDC.11 b No adjustment is necessary for women who smoke less than 10 cigarettes daily. c Hgb = hemoglobin. d Hct = hematocrit. |
||||
Indications for Nutrient Supplementation
|
Reproductive Period and Condition |
Low-Dose Multivitamin/ Mineral Preparationd |
600 mg of Calcium |
||
|
Preconception, interconception |
|
|
|
|
|
Iron deficiency anemia |
|
✓ |
✓ |
|
|
Pregnancy |
|
|
|
|
|
Normal |
✓ |
|
|
|
|
Complete vegetarian |
|
|
✓ |
|
|
Multiple gestation |
|
|
✓ |
|
|
Poor-quality diet and resistant to change |
|
|
✓ |
|
|
Heavy cigarette smoking |
|
|
✓ |
|
|
Alcohol abuse |
|
|
✓ |
|
|
Under age 25, consuming no calcium-rich milk products, and resistant to change |
|
|
✓e |
✓ |
|
Iron deficiency anemia |
|
✓ |
✓ |
|
|
Lactation |
|
|
|
|
|
Low energy intake |
|
|
✓ |
|
|
Low intake of milk products |
|
|
✓e |
✓ |
|
Iron deficiency anemia |
|
✓ |
✓ |
|
|
a Begin routine iron supplementation for all pregnant women by the 12th week of gestation. b Iron should be taken with juice or water, apart from meals. c Therapeutic doses of iron should be taken apart from other supplements. |
d For the suggested composition, see Tab 9. e The vitamin supplement is indicated to supply vitamin D. Regular exposure to sunshine reduces the need for this supplement. |
|||


















