
SURGERY PANEL REPORT1
INTRODUCTION
The surgery panel, one of eight established, was charged with examining physician manpower requirements for surgeons and anesthesiologists. This nine-member panel comprised six surgeons, two anesthesiologists, and one health services researcher. The chairman of the panel was also a member of the study committee. The panel roster is attached.
This draft report will describe the surgery panel's analyses, conducted in the framework of the “panel process” described in the “Overview” to this section of Volume II. Reported here will be the results of these analyses, along with the panel's commentary and recommendations.
EXPERT JUDGMENT APPROACHES TO DETERMINING PHYSICIAN REQUIREMENTS IN SURGERY AND ANESTHESIOLOGY
The DSE Approach
Initial Efforts
The first meeting of the surgery panel was convened in the early spring of 1990. The principal purpose was to determine whether the expert judgment process, as the study committee first conceived of it, was viable for the specialties under the purview of this panel. This process included the development of staffing instruments that would allow the panel to see
|
1 |
The initial draft of this report was prepared by Bobbie J.Alexander, Staff Associate to the Surgery Panel during the conduct of the study. This final report was prepared by the editors of this Volume. |
information about workload, about various nonphysician personnel that might be available to deliver care, and then, given that conditional information, to make judgments about the physician FTEE appropriate to meet that workload.
Study staff tested the feasibility of this process in the first panel meeting, and found that it was generally acceptable and that panel members could successfully render reasonable judgments about physician staffing. The panel concluded that study staff should proceed with the expert judgment process, but that many of the underlying assumptions within the initial staffing exercise should be better defined in the next iteration of the instrument:
-
more detail was needed concerning the type of resident (surgical, medical, etc.), the availability of residents (for coverage purposes), and the level of resident (PGY 1, 2, 3, etc.)
-
staffing instruments should be sensitive to particular aspects of anesthesiology staffing:
-
an intern (PGY 1) needs one-on-one coverage
-
a resident (PGY 2 & 3) needs one-on-one or one-on-two coverage; therefore, a ratio of one and one-half is recommended
-
an average of 30 minutes transpires between surgical cases
-
both a resident and staff physician must be on-call during nights and weekends
-
the same resident and staff physician usually cover the ICU
-
recovery time is unrealistic, but can be covered by the operating room anesthesiologists.
-
-
more information was needed concerning the type and mix of O.R. procedures.
-
more detailed information on case load was required
-
since surgery and anesthesiology are procedure oriented, more clinical information to describe case mix was desirable. In particular, it is important to consider severity of illness.
-
many of the quality issues concern not only physician staffing, but also the availability of all support services (nursing, administrative services, pathology, radiology, etc.)
-
without-compensation (WOC) and consultant and attending (C&A) physicians are desired for teaching purposes, and can augment VA staff physicians in the delivery of patient care
-
consultations should be designated as “high consultative” services and “low consultative” services, as appropriate
-
while the panel recognized that staffing data from the VA's cost distribution report (CDR) are the best currently available for the empirically based models, members still had reservations about the accuracy of reported physician FTEE
-
FTEE for full-time VA physicians should be better defined, and it should be recognized that full-time VA surgeons and anesthesiologists typically contribute more than 40 hours a week at the VAMC.
In the course of the first panel meeting, the panelists also reviewed and critiqued the initial versions of the empirically based staffing model. As a possible method to evaluate physician staffing, the panel requested that study staff explore external, non-VA physician staffing norms for review at the next meeting.
At the conclusion of the first round of all eight specialty and clinical program panel meetings, a “joint meeting” was convened involving the study committee (whose membership includes all eight specialty and clinical program panel chairmen), the data and methodology panel, and the VA liaison committee. This meeting (on May 2–3, 1990) was devoted to a review and critique of the key concepts and modeling assumptions underlying both the empirically based and expert judgment approaches.
The IOM study staff emerged from this meeting (later termed Joint Meeting I) with a set of recommendations from the committee on how to proceed with the panel process. Staff began to implement these recommendations on a panel-specific basis.
DSE: Overall Rationale
The next stage in the development of expert judgment staffing methodology centered on the preparation for, and conduct of, the second panel meeting. Again, to focus the analysis, three VA Medical Centers (designated here and in the committee report as VAMCs I, II, and III) were selected to represent a range in numbers of beds, staffing levels, services/programs, and affiliation status.
A revised staffing instrument, later termed the Detailed Staffing Exercise (DSE), was developed in response to the panel's request for instrument modification. It provided a more specific description of the VAMC, including the type of patients, number of admissions, length of stay, and the DRG-mix of patients in each PCA. All three VAMCs were presented in context and in
sufficient detail, it was hoped, that physician staffing decisions could be considered just as they are in the “real world.”
Instructions and Assumptions
Each DSE described a real (though unidentified) VAMC, including all specialty and clinical services. As in their first meeting, panelists were asked to complete the exercises by estimating physician staffing requirements for surgeons and anesthesiologists for each service in these medical centers.
In Section A of each exercise, the basic question was still the same for all patient care areas: How much time must be contributed by physicians in this medical center's surgery and anesthesiology services to meet a specified workload level during an average weekday in each VAMC, under certain assumptions about patient mix and support staff availability?
In Section B of each exercise, panelists were asked to estimate the additional surgery and anesthesiology FTEE associated with night as well as weekend coverage, certain educational and research activities, administration, and other factors.
An illustrative, unabridged Detailed Staffing Exercise, appears as Exhibit 1 in the “Overview” to this section of Volume II. While this DSE applies formally to physician staffing in medicine, it is nearly identical structurally to the DSEs prepared for surgery and anesthesiology.
Nature of Panel Consensus
The panel members individually received, completed, and returned to study staff two DSEs as homework assignments prior to the second meeting. At the meeting, however, they elected to use a group consensus judgment approach for assessing physician requirements for each of the three facilities. During the meeting, DSEs for each of the three VAMCs were analyzed thoroughly, ward by ward, ensuring that all assumptions were discussed by all panel members.
Interim Assessment of the Expert Judgment Process
These analyses showed that panel members could, with some degree of satisfaction on their own part, staff individual VAMCs. But what wasn't so clear was how to extend the logic of that process in a compact way in order to staff any and all VA facilities. This was discussed at the end of the second panel meeting and members expressed interest in some alternative assessment process that would be less cumbersome, but maintain (or even increase) the level of patient-specific detail provided.
The SADI Approach
SADI: Overall Rationale
At the conclusion of the second round of panel meetings, study staff implemented a sequence of postmeeting activities designed to assist the eight panels in arriving at consensus positions regarding the appropriate methodology and data for an expert judgment approach to physician staffing.
This postmeeting process was formally initiated with the development of a new Staffing Algorithm Development Instrument (SADI). The purpose of this new instrument was to test, build upon, and ultimately strengthen the algorithms and rules of thumb for staffing that emerged from the previous meetings of all eight specialty and clinical program panels. The instrument was designed to determine whether panel members could be asked a set of generic staffing questions whose answers could be applied to selected data from individual VAMCs to derive appropriate staffing levels for these facilities.
Instructions and Assumptions
As a preliminary response to the surgery panel's request for further specificity of acuity, SADI Section A (dealing with direct patient care and resident education in the PCAs) was developed in two parts. The first asked for estimates of physician hours for an “average” caseload. Average was characterized as consisting of a mix of highly complicated, moderately complicated, and uncomplicated patients. The second part asked for estimates of physician hours for a “typical” caseload. Typical was characterized as highly complicated patients.
Although median treatment times were slightly greater for the “typical” caseload, the differences were not great. In the illustrative applications of SADI to three VAMCs, the “average” caseload assumption was used, to be as consistent as possible with the case acuity levels assumed by the other seven panels.
When estimating time per initial consultation in various PCAs, panelists were asked to assume that when a resident is present, he/she is performing the consult under the supervision of the attending physician.
The complete SADI instruments for surgery and anesthesiology are shown in Figures 1 and 2, respectively, of this report. For each physician task or function, the panelists' median time estimate is presented; the panel's six surgeons completed the surgery SADI, and the two anesthesiologists completed that specialty's SADI. A detailed demonstration of how SADI task time estimates can be used to calculate physician requirements at a VAMC is presented in Exhibit 3 of the “Overview” to this section of Volume II. Although the application pertains specifically to internists, it well illustrates the process by which surgeon and anesthesiologist FTEE can be determined via the SADI.
EMPIRICALLY BASED APPROACHES TO DETERMINING SURGEON AND ANESTHESIOLOGIST FTEE
In the course of its deliberations, the panel had the opportunity to evaluate and make recommendations regarding alternative specifications of the empirically based physician staffing models (EBPSM) that pertained specifically to surgery and anesthesiology. As discussed in chapter 4 of the study committee's report (Volume I), the EBPSM have two variants: the production function (PF) and the inverse production function (IPF).
Production Functions
A portion of each of the panel's two meetings was devoted to an examination of alternative specifications of PF models for the inpatient surgery patient care area (PCA) and the ambulatory care surgery PCA.
While the derivation of total surgeon FTEE at a VA medical center via the PF approach requires an analysis of surgeon FTEE on all PCAs, this panel (like all others) restricted its focus to those PCAs where the surgeon was the “dominant” physician specialty. No PF model was estimated for anesthesiology
since this specialty is not uniquely associated with any one of the 14 PCAs defined in the study (see chapter 4 of the committee's report Volume I).
The final versions of the inpatient surgery and ambulatory care surgery PF models, as developed by the study's data and methodology panel in conjunction with this panel, are presented in Table 3.A.
Inverse Production Functions
During the postmeeting period, the panel had the opportunity to review and evaluate IPF models estimated for both surgery and anesthesiology. Final versions of these equations, as developed in conjunction with the data and methodology panel, are shown in Table 3.B.
EBPSM Assessment
The panel acknowledges that, on purely statistical grounds, the PF and IPF equations estimated for surgery and anesthesiology were among the strongest emerging in the entire study. Indeed, the inpatient surgery production function, with an ![]() of about 0.94 and estimated coefficients that are clinically plausible in all cases, is particularly noteworthy.
of about 0.94 and estimated coefficients that are clinically plausible in all cases, is particularly noteworthy.
But the panel has reservations about adopting a physician staffing methodology, at this point in time, that relies predominantly on such statistical models. These reservations arise largely from concerns about the accuracy of the physician FTEE data used in the models.
If the PF or the IPF were to be the primary tool for determining physician requirements, greater attention must be paid to improving the overall accuracy of the CDR data. In surgery, it may be particularly important for empirically based models to distinguish between full-time and part-time FTEE, since a substantial amount of the VA's surgery is performed by physicians whose major appointments are elsewhere. Eight of these surgeons working one-eighth time each in the VA are not likely to be the productivity-equivalent of one full-time VA surgeon. A similar issue arises for anesthesiology. Another issue affecting both surgery and anesthesiology is that some VAMCs have no distinct cost center for anesthesiology (cost center 212); in those facilities, all anesthesiologist FTEE is counted in the surgery cost center (202). In such cases, the number of surgeons would be overestimated and anesthesiologists underestimated.
PHYSICIAN STAFFING RESULTS FROM APPLICATION OF EXPERT JUDGMENT AND EMPIRICALLY BASED APPROACHES
Presented in Tables 1 and 2, respectively, are surgeons and anesthesiologists for VAMCs I, II, and III, as derived from: the VA's cost distribution report (CDR), the PF and IPF variants of the EBPSM, the DSE (from the second panel meeting), the SADI, and a mail survey of panel members just prior to Joint Meeting II (held September 7–9, 1990). As noted earlier, the PF model cannot be applied satisfactorily to anesthesiology, but the IPF can be.
Regarding total surgeon FTEE (Table 1.A), there is a clear distinction between the range of staffing results obtained from the CDR and both empirically based models, on the one hand, and both expert judgment models and the panel's survey-based assessment, on the other. The major source of this broad disparity is evident from Table 1.B. There is little systematic difference across all methods in surgeon requirements for patient care and resident education only (though the survey did not probe this issue). Hence, the SADI and DSE estimates are significantly greater than those from the PF and IPF because many more FTEEs were allocated by the panel under these expert judgment approaches to research, continuing education, leaves of absence, purchased coverage for nights and weekends, and non-VA consulting physicians.
Table 2 reveals a roughly similar pattern for anesthesiologist staffing. Total FTEE derived from the expert judgment approaches significantly exceeds that from the IPF and the CDR (Table 2.A); but now the SADI-based estimates also tend to be larger than those from either the DSE or the Survey. From Table 2.B it can be seen that the CDR, IPF, and DSE yield roughly similar FTEE for patient care and resident education, while the SADI estimates are larger for each VAMC. However, it can be inferred again that the large disparity between empirically based and expert judgment estimates in Table 2.A derives from large differences in FTEE allocated to activities other than patient care and resident education in the PCAs.
EXTERNAL (NON-VA) PHYSICIAN STAFFING NORMS
Data on physician staffing in surgery were collected by study staff from external (to the VA) health care organizations in order to compare staffing
methodologies or productivity performance norms that may exist in the public and private sectors.
All IOM committee and panel members were asked to recommend organizations for staff to contact. In addition, study staff attempted to obtain unpublished or informal “rules of thumb” used for staffing by hospitals and medical centers suggested by committee and panel members.
Also acquired were “internal” VA data indicating how VA staffing patterns were determined for surgery service in the past. The earliest documentation in VA Central Office, circa 1965, was very simple. At that time, it was considered appropriate to have 1.0 surgeon per 15 surgical beds for affiliated hospitals, 1.0 surgeon per 19 surgical beds for unaffiliated hospitals, and 1.0 anesthesiologist was required per operating room.
The Department of Defense (DoD) provided perhaps the most useful specific criteria since it utilizes full-time physician equivalents much like the VA; still, the patient population is generally younger and includes women and children. DoD defines physician performance levels by the number of outpatient and inpatient visits (the standard varies from 50 to 480 visits per month depending on the availability of teaching staff and the surgical specialty) and the number of inpatient days of care provided (30 to 190 days per month). A different criterion applies if the workload number conflicts with the number of residents, since it is assumed that residents require some minimum amount of supervision regardless of workload.
For the Indian Health Service (IHS), inpatient staffing is dependent on surgical cases: 2.0 FTEE surgeons for the first 300 cases+1.0 FTEE per 190 cases thereafter. Outpatient staffing is based on a formula of 1.0 FTEE per 5000 annual visits.
Another external norms application was based on a 1987 survey conducted by the American Medical Association, “1987 AMA Socioeconomic Monitoring System Core Survey,” which included only active, nonfederal, patient care physicians. By comparing the stated number of hospital visits, office visits, amount of time spent in rounds, and discharges, very rough conclusions could be drawn about appropriate VA staffing.
The New York Health and Hospitals Corporation (NYH&HC) provided data showing the ratio of their physician FTEE per annual admission and per average daily census (ADC).
Finally, staff were able to obtain data from a large HMO that had physician staffing and workload statistics for inpatient and outpatient visits. Again, the patient population at this HMO was generally younger and included more females than the VA population, with considerably different disease patterns.
Table 4 illustrates the computational approach used to derive each of the internal and external norm staffing standards.
Making comparisons between current VA staffing and the external norms was difficult because of differences in how workload is measured, how a physician FTEE is defined, and the type of patient population being compared. Many private institutions were willing to reveal their staffing patterns, but it was found that they did not measure their use of physician time in any fashion consistent with translating that time into FTEE, as defined by the VA. University hospitals, in particular, were able to state the number of faculty in the surgical service; but that number often included hundreds of physicians who had “privileges” at that institution regardless of whether they were retired, seldom used their admission privileges, or gave only an occasional lecture.
Nonetheless, each of the available external norms was applied to VAMCs I, II, and III to illustrate the staffing pattern that would occur if the VA used the norm as a staffing guideline. Table 5.A provides the inferred staffing patterns for surgeons and Table 5.B does the same for anesthesiologists.
In considering the usefulness of the external norm data, the surgical panel noted the following:
-
Across institutions there were a number of different workload measures employed, e.g., admissions, discharges, beds, and average daily census. This makes valid comparisons very difficult.
-
Some staffing ratios are not “norms” in the sense of being explicit standards consciously developed by the organization, but rather reflect an existing staffing pattern as it has evolved at the institution over time.
-
The definition of an FTEE is not universal at each institution. For example, the workload expected by one FTEE at some institutions may represent patient care only, while at others a large amount of teaching and/or research is also assumed in each FTEE.
-
Most hospitals have not analyzed how their physician staff may relate to some defined unit of workload. Therefore, the numbers provided are informally produced and cannot be validated in a written or computerized form.
Although external norms are of great interest to many practitioners, surgery panel members expressed reservations about the norms they analyzed for these practical reasons.
CONCLUSIONS
For determining VA physician requirements in both surgery and anesthesiology, the panel recommends particular variants of the Reconciliation Strategy (the “disaggregated weighted-average” approach proposed by the study committee). Regarding the FTEE components of the Reconciliation Strategy, the panel proposes the following:
Patient Care, Resident Education, and Administration
For surgery, the panel concludes that both the DSE and the SADI are viable approaches for determining FTEE for these activities. Purely statistical approaches to staffing, although conceptually well founded, are problematic at present because of flaws in the VA data used in their estimation. On the basis of its experience with both expert judgment methodologies, the panel regards the DSE as closer to a “gold standard” approach to staffing, yet recognizes that it would be highly cumbersome to implement regularly across the VA system. Hence, the panel believes that adopting a suitably refined version of the SADI instrument would be the more appropriate option; these refinements should include, in particular, a more detailed specification of case acuity, on the wards as well as in the operating room.
The panel has several concerns about the empirically based models ' reliance on data from the VA CDR. If the PF or the IPF were to be the primary tool for determining physician requirements, then greater attention must be paid to improving the overall accuracy of the CDR data. In surgery, it may be particularly important for the EBPSM to distinguish between full-time and part-time FTEE, since a substantial amount of the VA's surgery is performed by physicians whose major appointments are elsewhere. Eight of these surgeons each working one-eighth time in the VA are not likely to be the productivity equivalent of one full-time VA surgeon. A similar issue arises for anesthesiology. Another issue affecting both surgery and anesthesiology is that some VAMCs have no distinct cost center for anesthesiology (cost center 212); in those facilities, anesthesiologist FTEE are counted in the surgery cost center (202). In such cases, the number of surgeons would be overestimated and anesthesiologists underestimated.
In sum, for determining surgeon FTEE for patient care, resident education, and administration, the panel endorses a weighted-average strategy
with all of the weight placed on a SADI-based approach. (In the terminology of the Reconciliation Strategy, this is equivalent to setting b=1; see Equation 6.1 in Volume I.)
For anesthesiology, the panel recommends a variant of the Reconciliation Strategy that allows (but does not require) the VA decision maker to place ‘due weight on both expert judgment and empirically based approaches in calculating physician requirements. As described in chapter 6 of Volume I, the analytical vehicle for accomplishing this is a particular specification of the Reconciliation Strategy in which the parameter b is allowed to vary between 0 and 1.
To arrive at compromise positions about the appropriate FTEE levels for the VA medical centers studied here in depth, the panel's two anesthesiologists engaged in an exercise to derive a “consensus” value of b for each facility. For VAMCs I, II, and III, the means (midpoints) of the anesthesiologists' b values were, respectively, 0.43, 0.49, and 0.38.
The panel emphasizes that these particular weightings are specific to these particular facilities; hence, they are a reflection of, and serve to articulate, the anesthesiologists' professional judgments about appropriate physician staffing for these facilities. If other VAMCs had been examined, different b values would likely have emerged. In general, the Reconciliation Strategy should be executed on a facility-specific basis, so that relevant local data and circumstances can be factored into the staffing decision process. In this way, the parameter b becomes an appropriate reflection (or articulator) of the decision process, not the mechanical driver of that process.
Research
The panel feels strongly that FTEE allocations for research should be related to measurable indicators of research productivity and excellence. The amount of VA and non-VA research support is considered the single most important indicator. Quite clearly, not all surgery and anesthesiology services in the VA merit the same level of research FTEE.
Continuing Education
There ought to be some minimal level of continuing education built into the FTEE requirements of all VAMCs. A figure of 10 days per year was discussed, but there was no consensus about the exact amount of time to be
devoted to continuing education. There was, however, a clear consensus that continuing education is important for quality assurance and should be specifically recognized in calculating surgeon and anesthesiologist requirements.
Leaves of Absence
The percentage of time allocated to various types of leave should be calculated in a way consistent with the VA's own policies and practices. The panel believes that these analyses would suggest that about 12 percent of total FTEE is a reasonable allocation.
Purchased Coverage for Nights and Weekends
Assuming an adequate availability of residents, none is required.
Consulting & Attending and Without-Compensation Coverage
The use of C&A and WOC physicians enhances the quality of clinical and educational activities in the VAMC. The panel also notes that in affiliated VAMCs, C&A and WOC surgeons can make important contributions to handling some portions of patient workload and resident training. However, given the increasing cost pressures facing the academic affiliates, the panel urges that when the VA computes surgeon requirements, it does not make unwarranted assumptions about the availability of C &As and WOCs. Rather, the fraction of total surgeon FTEE requirements to be filled by VA staff physicians should be determined only after careful consideration of the local availability of C&A and WOC surgeons.
External Norms
Developing non-VA physician staffing standards to which the VA's own staffing could be validly compared proved difficult for several reasons.
First, most non-VA facilities do not measure physician time in terms of an FTEE. There is no need for these hospitals to do this since surgeons,
anesthesiologists, and other physicians are not paid from a central budget but participate in clinical and educational activities as “attending” physicians with widely varying time commitments.
Second, a portion of the surgery workload at many non-VA institutions is comparable to the workload found in VAMCs. But, given current data systems in the private sector, it is exceedingly hard to determine how much physician time is devoted to caring for the VA-comparable portion of total workload.
Third, since few private institutions have established explicit staffing standards, and there are no nationally recognized standards, one can question how much policy significance should be given to observed staffing ratios.
Overall Adequacy of Physician Staffing in the VA
It is evident from Tables 1 and 2 that the panel does not regard surgery and anesthesiology staffing to be adequate (in FY 1989) at the three VAMCs studied in depth. However, the panel feels that it is premature to draw general conclusions about the adequacy of staffing in these specialties across the VA. If the SADI or the DSE could be applied to facilities across the board, the panel is confident that the question of staffing adequacy could be addressed quantitatively.
Other Points
First, all FTEE estimates derived from the SADI and the DSE assumed a 40-hour work week. In reality, surgeons and anesthesiologists work much longer than this—perhaps closer to a 55-hour week. If some such higher (and more realistic) hours per week assumption were to be used, the derived FTEE levels presented in the panel's report would be reduced accordingly. The way in which hours are converted into FTEE is an important issue the study committee may want to review.
Second, though the panel kept to its charge of examining the physician FTEE (rather than physician expenditures) required to meet workload, it emphasizes that one budgetary complication cannot be ignored. In most areas, the going market rate for one FTEE surgeon or anesthesiologist is considerably more than the VA's top salary level. Thus, a VA requiring X anesthesiologist FTEE would need to budget for some greater number (X+Y) to have sufficient
funds to purchase X. Failing that, the VA must work out some form of reciprocal agreement with its affiliated medical center to augment its anesthesiology staffing. But these affiliates are under increasing pressure to cut costs, and they may become increasingly resistant to such sharing arrangements.
Final Remarks
For establishing VA staffing standards in surgery and anesthesiology, the panel endorses the study committee's Reconciliation Strategy, with the components of FTEE specified as indicated above.
TABLE 1 Estimates of Physician Requirements in Surgery at Three VAMCs
|
SURGERY |
||||||
|
A. Total FTEE |
||||||
|
VAMC |
CDR |
PF |
IPF |
DSE |
SADI |
Survey1 |
|
VAMC I |
14.4 |
17.3 |
19.1 |
31.1 |
34.1 |
28.0 |
|
VAMC II |
17.3 |
15.7 |
17.9 |
34.2 |
37.8 |
30.8 |
|
VAMC III |
9.4 |
10.0 |
10.6 |
14.8 |
18.5 |
14.5 |
TABLE 2 Estimates of Physician Requirements in Anesthesiology at Three VAMCs
|
ANESTHESIOLOGY |
|||||
|
A. Total FTEE |
|||||
|
VAMC |
CDR |
IPF |
DSE |
SADI |
Survey2 |
|
VAMC I |
7.2 |
4.0 |
17.7 |
30.9 |
(8, 25) |
|
VAMC II |
6.0 |
8.2 |
23.9 |
36.9 |
(14, 25) |
|
VAMC III |
1.0 |
1.5 |
10.0 |
16.9 |
(4, 6) |
TABLE 3 Estimated Production Functions for Inpatient and Ambulatory Surgery and Inverse Production Functions for Inpatient Surgery and Anesthesiology
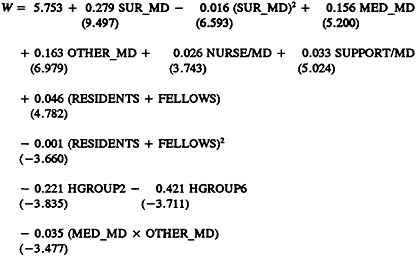
|
OTHER_MD |
=total FTEE allocated to inpatient surgery PCA by VA staff physicians not in medicine, surgery, psychiatry, neurology, or rehabilitation medicine cost centers; |
|
NURSE/MD |
=nursing-staff FTEE divided by total FTEE for physicians involved in hands-on delivery of care in the inpatient surgery PCA, defined to include internists, surgeons, psychiatrists, neurologists, and rehabilitation medicine physicians (hereafter, this variable will be labeled more succinctly, “nursing-staff FTEE per total physician FTEE in this PCA”); |
|
SUPPORT/MD |
=support staff FTEE per physician FTEE in this PCA; |
|
RESIDENTS+FELLOWS |
=total FTEE of residents PGY 2 and above allocated to this PCA; |
|
HGROUP2 |
=categorical variable assuming a value of 1 if the facility is in RAM Group 2 (small general unaffiliated VAMC); and |
|
HGROUP6 |
=categorical variable assuming a value of 1 if facility is in RAM Group 6 (psychiatric hospital); |
|
(MED_MD×OTHER_MD) |
=interaction term for the joint influence of VA staff internists and VA “other” physicians on the rate of workload production in the inpatient surgery PCA. |
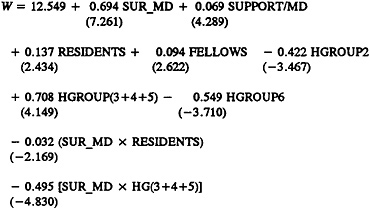
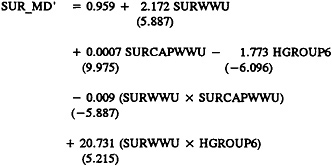
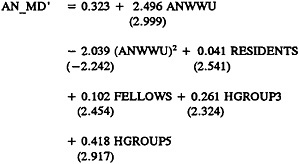
TABLE 4 External Norms—Surgery
|
Source, Result, and Derivation, if any: |
||
|
VA—affiliated VAMC=1 MD/15 beds; unaffiliated=1 MD/19 beds |
||
|
Indian Health Service—2 surgeons+1 additional for every 190 cases over 300/yr |
||
|
American Medical Association Core Survey |
||
|
Dis1 |
=5.3 dis/wk×47.1 wk/yr×(40 hr/wk/58.1 hr/wk) ×(52.6 hr/wk/58.1 hr/wk) eff factor |
|
|
×(52.6 hr/wk/7.8+14.6) hr/wk hosp= |
365 dis/MD/yr |
|
|
Dis2 |
=1 dis/4.2 hr×2,080 hr/yr×(52.6 hr/wk/ 58.1 hr/wk) eff factor×0.85 availability |
|
|
factor |
=381 dis/MD/yr |
|
|
ADC |
=14.6 pt day/wk×47.1 wk/yr×1 ADC/ 365 pt day×(52.6 hr/wk/58.1 hr/wk) eff factor×(52.6 hr/wk/(7.8+14.6) |
|
|
hr/wk hosp) |
=4.0 ADC/MD/yr |
|
|
Amb |
=3.33 vis/hr×40 hr/wk×47.1 wk/yr |
|
|
×52.6/58.1 eff factor |
=5,700 vis/MD/yr |
|
|
NYH&HC |
||
|
ADC |
=ADC/attendings |
=5.0 ADC/MD/yr |
|
Amb |
=visits/attendings |
=6,420 vis/MD/yr |
|
Group Health Inc. of St. Paul |
||
|
90 visits/MD/wk×45 wks/yr |
=4,050 vis/MD/yr |
|
|
Large Health Maintenance Organization (HMO) |
||
|
Dis |
=2/3 surg ratio×291 pt days/1,000 members ×5,436 k mem/365 days/yr/0.4 input factor |
|
|
×40 hr/wk/47 hr/wk/883.5 MD |
=7.0 ADC/MD |
|
|
Amb |
=200 vis/k mem×5,436 k mem/883.5 MD/ |
|
|
0.6 OP factor×(40 hr/wk/47 hr/wk) |
=1,750 vis/MD/yr |
|
|
DoD |
||
|
Standards for the workload per MD per year are specified separately by DoD for each of the large number of specialists, e.g., internists, neurologists, general surgeons, orthopaedic surgeons, neurosurgeons, etc. Further, different standards are specified for teaching versus nonteaching hospitals. Thus, the overall workload per MD for a given hospital is a function of the type of hospital as well as the mix of patients seen there. For example, for an ADC in surgery of 100 at a teaching facility, the inpatient physician requirement would be |
||
|
100 ADC/7.1 ADC/MD=14.1 MD |
TABLE 5.A Surgery External Norms Applied to VAMCs
|
Computed Inpatient FTEE at |
|||||
|
Source |
Statistic |
Wkld/MD |
VAMC I |
VAMC II |
VAMC III |
|
DoD |
ADC/MD |
7.1 |
9.3 |
17.1 |
6.5 |
|
HMO |
ADC/MD |
7.0 |
9.4 |
17.3 |
6.6 |
|
IHS |
Cases/MD |
190.0 |
13.6 |
26.7 |
13.6 |
|
AMA |
ADC/MD |
4.0 |
16.5 |
30.3 |
11.5 |
|
Disch/MD |
365.0 |
6.8 |
13.7 |
6.8 |
|
|
Disch/MD |
381.0 |
6.6 |
13.1 |
6.6 |
|
|
NYH&HC |
ADC/MD |
5.0 |
13.2 |
24.2 |
9.2 |
|
1965 VA Stds |
BEDS/MD |
15 or 19 |
5.1 |
9.5 |
2.8 |
|
Computed Outpatient FTEE at |
|||||
|
Source |
Statistic |
Wkld/MD |
VAMC I |
VAMC II |
VAMC III |
|
DoD |
vis/MD |
5,100 |
5.2 |
6.3 |
5.3 |
|
HMO |
vis/MD |
1,750 |
15.1 |
18.3 |
15.9 |
|
IHS |
vis/MD |
5,000 |
5.3 |
6.4 |
5.6 |
|
AMA |
vis/MD |
5,700 |
4.6 |
5.6 |
4.9 |
|
NYH&HC |
vis/MD |
6,420 |
5.4 |
6.5 |
5.6 |
|
GHA-St.Paul |
vis/MD |
4,050 |
6.5 |
7.9 |
6.9 |
|
1965 VA stds |
vis/MD |
3,500 |
7.6 |
9.2 |
7.9 |
|
Computed Total FTEE at |
|||
|
Source |
VAMC I |
VAMC II |
VAMC III |
|
DoD |
14.5 |
23.4 |
11.8 |
|
HMO |
24.6 |
35.6 |
22.4 |
|
IHS |
18.9 |
33.1 |
19.1 |
|
AMA |
11.5 |
19.3 |
11.7 |
|
NYH&HC |
18.6 |
30.7 |
14.8 |
|
1965 VA stds |
12.6 |
18.6 |
10.8 |
FIGURE 1 The Staffing Algorithm Development Instrument (SADI) for Surgery: The Complete Instrument with Statistical Summary of the Panel's Assessments
INTRODUCTION AND INSTRUCTIONS (Abbreviated)
The purpose of the SADI is to gather the data needed to construct, test, formalize, and enhance the algorithms and rules of thumb for staffing that emerged from prior meetings of each specialty and clinical program panel. The ultimate intention is to develop algorithms which could be applied to estimate staffing requirements at VA medical centers (VAMCs), presumably duplicating the results specialty and clinical program panelists themselves would have derived.
Section A of the SADI requests time estimates, in some cases by workload unit. In other cases, it requests time estimates by major job elements (tasks). These elements had previously been indicated by some panel members as accounting for the bulk of the work of VA surgeons. We seek your estimates of how physician requirements in your specialty vary with respect to such variables as the volume of patients and the availability of residents and nonphysician practitioners. By systematically varying the levels of workload and personnel, we hope to infer from your numerical responses the implicit formulas you used to relate physician time to these variables as well as the nature of the relationship between workload and staffing, e.g., linear or nonlinear.
Section B seeks responses to a series of questions for the time spent in activities other than direct patient care.
Instructions: In Section A, for each cell of each table, please estimate the number of physician hours required from the Surgery Service to deliver good-quality care under the specified circumstances. Section B is self-explanatory.
SECTION A: PATIENT CARE ACTIVITIES—SURGERY
ADMISSIONS—AVERAGE CASELOAD
Please fill in the average time in hours required by a staff physician in your service to accomplish an admission work-up, for a caseload of “average” severity, either with or without the assistance of a resident in your service. This “average” caseload will, of course, consist of a mix of highly complicated, moderately complicated, and uncomplicated patients.
Chart 1
|
Time per Admission Work-Up without Resident |
Time per Admission Work-up with Resident (Resident Does Work-Up, Staff Physician Reviews Data) |
||||||
|
High |
Low |
Mean |
Median |
High |
Low |
Mean |
Median |
|
1.00 |
0.50 |
0.70 |
0.75 |
0.50 |
0.20 |
0.30 |
0.25 |
ADMISSIONS—COMPLICATED CASELOAD
Please fill in the average time in hours required by a staff physician in your service to accomplish an admission work-up for a typical caseload only of complicated patients, either with or without the assistance of a Resident in your service. This “typical” case-load will, of course, present the very difficult and more complex patients characterized as “highly complicated” patients.
Chart 2
|
Time per Admission Work-up without Resident |
Time per Admission Work-Up with Resident (Resident Does Work-Up, Staff Physician Reviews Data) |
||||||
|
High |
Low |
Mean |
Median |
High |
Low |
Mean |
Median |
|
2.00 |
1.25 |
1.55 |
1.50 |
1.50 |
0.33 |
0.65 |
0.50 |
ROUTINE DAILY PATIENT CARE—AVERAGE CASELOAD
For each workload factor and alternative average daily census (ADC) level below, please fill in the average number of physician hours required from the Surgery Service for a caseload of “average” severity for an average weekday. This “average” caseload, will, of course, consist of a mix of highly complicated, moderately complicated, and uncomplicated patients. In responding, assume the proportion of each type of case reflects what one would expect in a typical VAMC with a university-sponsored affiliation in Surgery (and perhaps with other specialties). Keep in mind that the Daily Rounds do not include new admission work-ups, since they are covered in Chart 1.
Chart 3
|
Assume No Residents |
|||||||
|
Gen Surg Ward Average LOS=7 |
ADC 5 |
ADC 10 |
ADC 15 |
ADC 20 |
ADC 25 |
ADC 30 |
|
|
Daily Rounds |
High |
0.75 |
1.50 |
2.00 |
2.50 |
3.00 |
3.50 |
|
Low |
0.33 |
0.67 |
1.00 |
0.70 |
0.80 |
1.00 |
|
|
Mean |
0.50 |
1.00 |
1.30 |
1.60 |
1.90 |
2.30 |
|
|
Median |
0.50 |
1.00 |
1.00 |
1.50 |
1.50 |
2.00 |
|
|
Charting, Phone, and Paperwork |
High |
0.50 |
1.00 |
1.25 |
1.50 |
1.75 |
2.00 |
|
Low |
0.20 |
0.40 |
0.60 |
0.70 |
0.80 |
1.00 |
|
|
Mean |
0.30 |
0.60 |
0.80 |
1.00 |
1.20 |
1.40 |
|
|
Median |
0.25 |
0.50 |
0.75 |
1.00 |
1.25 |
1.50 |
|
|
Patient and Family Contacts and Teaching |
High |
0.50 |
1.00 |
1.00 |
1.25 |
1.50 |
1.75 |
|
Low |
0.15 |
0.25 |
0.45 |
0.33 |
0.40 |
0.50 |
|
|
Mean |
0.30 |
0.50 |
0.70 |
0.90 |
1.00 |
1.20 |
|
|
Median |
0.25 |
0.50 |
0.75 |
1.00 |
1.20 |
1.30 |
|
|
Assume No Residents |
|||||||
|
Gen Surg Ward Average LOS=7 |
ADC 5 |
ADC 10 |
ADC 15 |
ADC 20 |
ADC 25 |
ADC 30 |
|
|
Supervision and Teaching (Residents/Staff) |
High |
0.10 |
0.10 |
0.10 |
0.67 |
0.80 |
1.00 |
|
Low |
0.00 |
0.00 |
0.00 |
0.00 |
0.00 |
0.00 |
|
|
Mean |
0.00 |
0.00 |
0.00 |
0.20 |
0.20 |
0.20 |
|
|
Median |
0.00 |
0.00 |
0.00 |
0.00 |
0.00 |
0.00 |
|
|
Any special procedures apart from those conducted on SICU (e.g., Starting IVs, Thoracentesis, Inserting Urinary Catheters, and Suture Removal) |
High |
0.50 |
1.00 |
1.50 |
2.00 |
2.50 |
3.00 |
|
Low |
0.00 |
0.00 |
0.33 |
0.00 |
0.00 |
0.00 |
|
|
Mean |
0.30 |
0.60 |
1.00 |
1.20 |
1.40 |
1.70 |
|
|
Median |
0.50 |
0.75 |
1.00 |
1.25 |
1.25 |
1.50 |
|
|
Overall Mean Time |
1.40 |
2.70 |
3.80 |
4.80 |
5.70 |
6.90 |
|
|
Overall Median Time |
1.60 |
3.00 |
4.25 |
5.50 |
6.00 |
7.25 |
|
Chart 4
|
Assume Full Component of Residents (PGY 1–5) Integrated with Residents of an Affiliated University |
|||||||
|
Gen Surg Ward Average LOS=7 |
ADC 5 |
ADC 10 |
ADC 15 |
ADC 20 |
ADC 25 |
ADC 30 |
|
|
Daily Rounds |
High |
0.50 |
0.60 |
0.90 |
1.20 |
1.50 |
1.80 |
|
Low |
0.25 |
0.33 |
0.50 |
0.67 |
0.80 |
1.00 |
|
|
Mean |
0.30 |
0.50 |
0.70 |
0.90 |
1.10 |
1.10 |
|
|
Median |
0.30 |
0.50 |
0.75 |
0.75 |
1.00 |
1.00 |
|
|
Charting, Phone, and Paperwork |
High |
0.25 |
0.33 |
0.50 |
0.67 |
0.80 |
1.00 |
|
Low |
0.00 |
0.00 |
0.00 |
0.00 |
0.00 |
0.00 |
|
|
Mean |
0.30 |
0.20 |
0.30 |
0.40 |
0.50 |
0.50 |
|
|
Median |
0.10 |
0.20 |
0.30 |
0.40 |
0.50 |
0.60 |
|
|
Patient and Family Contacts and Teaching |
High |
0.70 |
0.25 |
0.50 |
0.50 |
0.75 |
0.75 |
|
Low |
0.00 |
0.00 |
0.00 |
0.00 |
0.00 |
0.00 |
|
|
Mean |
0.20 |
0.10 |
0.20 |
0.30 |
0.40 |
0.50 |
|
|
Median |
0.10 |
0.15 |
0.23 |
0.33 |
0.40 |
0.50 |
|
|
Assume Full Component of Residents (PGY 1–5) Integrated with Residents of an Affiliated University |
|||||||
|
Gen Surg Ward Average LOS=7 |
ADC 5 |
ADC 10 |
ADC 15 |
ADC 20 |
ADC 25 |
ADC 30 |
|
|
Supervision and Teaching (Residents/Staff) |
High |
1.00 |
1.00 |
1.50 |
1.60 |
2.00 |
2.40 |
|
Low |
0.00 |
0.00 |
0.00 |
0.00 |
0.00 |
0.00 |
|
|
Mean |
0.40 |
0.60 |
0.80 |
1.00 |
1.20 |
1.40 |
|
|
Median |
0.40 |
0.80 |
1.00 |
1.25 |
0.15 |
1.50 |
|
|
Any special procedures apart from those conducted on SICU (e.g., Starting IVs, Thoracentesis, Inserting Urinary Catheters, and Suture Removal) |
High |
0.25 |
0.25 |
0.50 |
0.50 |
0.80 |
0.60 |
|
Low |
0.00 |
0.00 |
0.00 |
0.00 |
0.00 |
0.00 |
|
|
Mean |
0.10 |
0.10 |
0.20 |
0.20 |
0.30 |
0.30 |
|
|
Median |
0.05 |
0.10 |
0.15 |
0.20 |
0.25 |
0.30 |
|
|
Overall Mean Time |
1.20 |
1.50 |
2.20 |
2.70 |
3.40 |
4.00 |
|
|
Overall Median Time |
1.45 |
1.90 |
2.80 |
3.30 |
4.25 |
4.50 |
|
ROUTINE DAILY PATIENT CARE—COMPLICATED CASELOAD
For each workload factor and alternative average daily census (ADC) level below, please fill in the average number of physician hours required from the Surgery Service for a typical caseload only of complicated patients. This “typical” caseload, will, of course, present the very difficult and more complex patients characterized as “highly complicated” patients. In responding, assume the proportion of each type of case reflects what one would expect in a typical VAMC with a university-sponsored affiliation in Surgery (and perhaps with other specialties). Keep in mind that the Daily Rounds do not include new admission work-ups, since they are covered in Chart 2.
Chart 5
|
Assume No Residents |
|||||||
|
Gen Surg Ward Average LOS=7 |
ADC 5 |
ADC 10 |
ADC 15 |
ADC 20 |
ADC 25 |
ADC 30 |
|
|
Daily Rounds |
High |
1.50 |
3.00 |
4.00 |
5.00 |
6.00 |
7.00 |
|
Low |
0.50 |
0.67 |
0.83 |
1.00 |
1.15 |
1.50 |
|
|
Mean |
0.80 |
1.60 |
2.20 |
3.60 |
3.30 |
3.90 |
|
|
Median |
0.50 |
1.25 |
1.50 |
2.00 |
2.50 |
3.00 |
|
|
Charting, Phone, and Paperwork |
High |
0.75 |
1.50 |
1.80 |
2.00 |
2.50 |
3.00 |
|
Low |
0.25 |
0.50 |
0.75 |
1.00 |
1.25 |
1.50 |
|
|
Mean |
0.50 |
1.00 |
1.30 |
1.50 |
1.80 |
2.00 |
|
|
Median |
0.50 |
1.00 |
1.25 |
1.50 |
1.75 |
1.75 |
|
|
Patient and Family Contacts and Teaching |
High |
0.50 |
1.00 |
1.25 |
1.50 |
1.75 |
2.00 |
|
Low |
0.20 |
0.40 |
0.50 |
1.00 |
1.00 |
1.20 |
|
|
Mean |
0.30 |
0.60 |
0.80 |
1.10 |
1.30 |
1.60 |
|
|
Median |
0.30 |
0.50 |
0.75 |
1.00 |
1.25 |
1.50 |
|
|
Supervision and Teaching (Residents/Staff) |
High |
0.20 |
0.20 |
0.20 |
0.40 |
0.40 |
0.40 |
|
Low |
0.00 |
0.00 |
0.00 |
0.00 |
0.00 |
0.00 |
|
|
Mean |
0.00 |
0.00 |
0.00 |
0.10 |
0.10 |
0.10 |
|
|
Median |
0.00 |
0.00 |
0.00 |
0.00 |
0.00 |
0.00 |
|
|
Assume No Residents |
|||||||
|
Gen Surg Ward Average LOS=7 |
ADC 5 |
ADC 10 |
ADC 15 |
ADC 20 |
ADC 25 |
ADC 30 |
|
|
Any special procedures apart from those conducted on SICU (e.g., Starting IVs, Thoracentesis, Inserting Urinary Catheters, and Suture Removal) |
High |
1.00 |
2.00 |
3.00 |
4.00 |
5.00 |
6.00 |
|
Low |
0.25 |
0.50 |
0.75 |
1.00 |
1.25 |
1.83 |
|
|
Mean |
0.70 |
1.10 |
1.60 |
2.10 |
2.50 |
3.00 |
|
|
Median |
0.75 |
1.00 |
1.25 |
1.50 |
1.75 |
2.00 |
|
|
Overall Mean Time |
2.30 |
4.30 |
5.90 |
8.30 |
9.00 |
10.50 |
|
|
Overall Median Time |
2.25 |
4.50 |
5.50 |
6.25 |
7.25 |
7.80 |
|
Chart 6
|
Assume Full Component of Residents (PGY 1–5) Integrated with Residents of an Affiliated University |
|||||||
|
Gen Surg Ward Average LOS=7 |
ADC 5 |
ADC 10 |
ADC 15 |
ADC 20 |
ADC 25 |
ADC 30 |
|
|
Daily Rounds |
High |
0.06 |
1.20 |
1.80 |
2.40 |
3.00 |
3.50 |
|
Low |
0.50 |
0.75 |
0.75 |
1.00 |
1.25 |
1.50 |
|
|
Mean |
0.50 |
0.90 |
1.10 |
1.60 |
1.90 |
2.30 |
|
|
Median |
0.50 |
0.80 |
1.00 |
1.67 |
2.00 |
2.30 |
|
|
Charting, Phone, and Paperwork |
High |
0.25 |
0.33 |
0.50 |
0.67 |
0.83 |
1.00 |
|
Low |
0.00 |
0.00 |
0.00 |
0.00 |
0.00 |
0.00 |
|
|
Mean |
0.90 |
0.20 |
0.30 |
0.40 |
0.50 |
0.60 |
|
|
Median |
0.17 |
0.25 |
0.40 |
0.50 |
0.50 |
0.70 |
|
|
Patient and Family Contacts and Teaching |
High |
0.25 |
0.25 |
0.05 |
0.50 |
0.75 |
0.75 |
|
Low |
0.08 |
0.17 |
0.25 |
0.33 |
0.40 |
0.50 |
|
|
Mean |
0.10 |
0.20 |
0.30 |
0.40 |
0.50 |
0.60 |
|
|
Median |
0.10 |
0.20 |
0.30 |
0.40 |
0.50 |
0.60 |
|
|
Supervision and Teaching Residents/Staff |
High |
2.00 |
2.00 |
3.00 |
3.00 |
4.00 |
4.00 |
|
Low |
0.00 |
0.00 |
0.00 |
0.00 |
0.00 |
0.00 |
|
|
Mean |
0.70 |
0.90 |
1.30 |
1.50 |
1.90 |
1.80 |
|
|
Median |
0.50 |
0.50 |
1.00 |
1.00 |
1.25 |
1.25 |
|
|
Any special procedures (e.g., Insertion of Monitors and Nutritional Devices) |
High |
0.20 |
0.30 |
0.40 |
0.50 |
0.60 |
0.70 |
|
Low |
0.00 |
0.00 |
0.00 |
0.00 |
0.00 |
0.00 |
|
|
Mean |
0.10 |
0.20 |
0.20 |
0.20 |
0.30 |
0.40 |
|
|
Median |
0.00 |
0.20 |
0.25 |
0.25 |
0.50 |
0.50 |
|
|
Overall Mean Time |
1.30 |
2.30 |
3.30 |
3.90 |
5.10 |
5.80 |
|
|
Overall Median Time |
1.50 |
2.00 |
3.00 |
3.33 |
4.25 |
5.00 |
|
Chart 7
|
Assume Full Component of Residents (PGY1–5) Integrated with Residents of an Affiliated University |
|||||||
|
Gen Surg Ward Average LOS=5 |
ADC 3 |
ADC 5 |
ADC 7 |
ADC 9 |
ADC 11 |
ADC 13 |
|
|
Daily Rounds |
High |
0.50 |
1.00 |
1.00 |
1.50 |
1.50 |
2.00 |
|
Low |
0.25 |
0.25 |
0.50 |
0.50 |
0.50 |
0.75 |
|
|
Mean |
0.40 |
0.60 |
0.80 |
1.00 |
1.10 |
1.40 |
|
|
Median |
0.50 |
0.60 |
0.67 |
0.80 |
1.00 |
1.50 |
|
|
Charting, Phone, and Paperwork |
High |
0.40 |
0.60 |
0.80 |
0.90 |
1.00 |
1.10 |
|
Low |
0.00 |
0.00 |
0.00 |
0.00 |
0.00 |
0.00 |
|
|
Mean |
0.20 |
0.20 |
0.30 |
0.30 |
0.40 |
0.50 |
|
|
Median |
0.10 |
0.20 |
0.20 |
0.30 |
0.33 |
0.50 |
|
|
Patient and Family Contacts and Teaching |
High |
0.25 |
0.40 |
0.50 |
0.70 |
0.90 |
1.20 |
|
Low |
0.00 |
0.00 |
0.00 |
0.30 |
0.17 |
0.30 |
|
|
Mean |
0.20 |
0.20 |
0.20 |
0.40 |
0.50 |
0.60 |
|
|
Median |
0.20 |
0.20 |
0.25 |
0.40 |
0.40 |
0.50 |
|
|
Supervision and Teaching Residents/Staff |
High |
1.50 |
1.60 |
1.70 |
1.80 |
2.00 |
2.00 |
|
Low |
0.00 |
0.00 |
0.00 |
0.00 |
0.00 |
0.00 |
|
|
Mean |
0.60 |
0.70 |
0.80 |
0.90 |
1.10 |
1.10 |
|
|
Median |
0.50 |
0.50 |
0.50 |
0.75 |
0.75 |
0.83 |
|
|
Any special procedures (e.g., Insertion of Monitors and Nutritional Devices) |
High |
0.50 |
0.70 |
0.90 |
1.10 |
1.30 |
1.50 |
|
Low |
0.00 |
0.00 |
0.00 |
0.00 |
0.00 |
0.00 |
|
|
Mean |
0.10 |
0.30 |
0.30 |
0.40 |
0.40 |
0.50 |
|
|
Median |
0.00 |
0.25 |
0.25 |
0.25 |
0.25 |
0.25 |
|
|
Overall Mean Time |
1.70 |
2.00 |
2.40 |
3.00 |
3.40 |
4.00 |
|
|
Overall Median Time |
1.40 |
1.50 |
1.75 |
2.25 |
2.50 |
2.83 |
|
TIME PER INITIAL CONSULTATION OFF YOUR PCA
Fill in the average time in hours required by a staff physician in your service for each initial (new) consult on another service, noting the presence or absence of a resident in your own service. (When the resident is present, assume that she/he is performing the consult under the supervision of an attending physician.)
Chart 8
|
Time per Consult Without Resident |
Time per Consult with Resident |
|||||||
|
Consultation off your PCA |
High |
Low |
Mean |
Median |
High |
Low |
Mean |
Median |
|
Neurology |
0.50 |
0.33 |
0.48 |
0.50 |
0.50 |
0.20 |
0.25 |
0.25 |
|
Medicine |
0.50 |
0.33 |
0.48 |
0.50 |
0.50 |
0.20 |
0.25 |
0.25 |
|
Nursing Home |
0.75 |
0.25 |
0.48 |
0.50 |
0.33 |
0.20 |
0.25 |
0.33 |
|
Intermediate Care |
0.50 |
0.25 |
0.42 |
0.50 |
0.33 |
0.20 |
0.25 |
0.25 |
|
Rehab Med |
0.75 |
0.25 |
0.48 |
0.50 |
0.33 |
0.20 |
0.25 |
0.25 |
|
Psychiatry |
0.50 |
0.33 |
0.42 |
0.50 |
0.33 |
0.20 |
0.25 |
0.25 |
TIME PER FOLLOW-UP VISIT (POST-CONSULTATION) OFF YOUR PCA
Fill in the average time in hours required by a staff physician in your service for each follow-up consultation visit (post-consultation) on another service, noting the presence or absence of a resident from your service.
Chart 9
|
Time per Consult Without Resident |
Time per Consult with Resident |
|||||||
|
Follow-Up Visit (Post-Consult) |
High |
Low |
Mean |
Median |
High |
Low |
Mean |
Median |
|
Neurology |
0.25 |
0.08 |
0.20 |
0.25 |
0.25 |
0.00 |
0.10 |
0.10 |
|
Medicine |
0.25 |
0.08 |
0.20 |
0.25 |
0.20 |
0.00 |
0.10 |
0.10 |
|
Nursing Home |
0.25 |
0.08 |
0.20 |
0.20 |
0.20 |
0.00 |
0.10 |
0.10 |
|
Intermediate Care |
0.25 |
0.08 |
0.20 |
0.20 |
0.20 |
0.00 |
0.10 |
0.10 |
|
Rehab Med |
0.25 |
0.08 |
0.20 |
0.20 |
0.20 |
0.00 |
0.10 |
0.10 |
|
Psychiatry |
0.25 |
0.08 |
0.20 |
0.20 |
0.20 |
0.00 |
0.10 |
0.10 |
OUTPATIENT VISITS
Please fill in the average time in hours required by a staff physician in your service for the average ambulatory care clinic visit by a typical patient to one of the clinics run by the surgical/anesthesiology service, noting the presence or absence of residents and nonphysician practitioners, and whether the visit is by a new or returning patient.
Chart 10
|
Physician Time per Visit |
||||
|
Type of Visit |
High |
Low |
Mean |
Median |
|
New Patient Visit No Resident |
0.50 |
0.33 |
0.40 |
0.50 |
|
New Patient Visit With Resident |
0.33 |
0.20 |
0.25 |
0.25 |
|
New Patient Visit With NP or PA |
0.33 |
0.10 |
0.25 |
0.33 |
|
Follow-Up Visit No Resident |
0.25 |
0.10 |
0.20 |
0.20 |
|
Follow-Up Visit With Resident |
0.20 |
0.10 |
0.10 |
0.10 |
|
Follow-Up Visit With NP or PA |
0.20 |
0.10 |
0.10 |
0.10 |
SECTION B: NON-PATIENT-CARE TIME
Part 1. The activities listed below generally do not occur every day, but may be time consuming when looked at over a longer period, such as a week or month. List the time in hours that you would add to each physician's average weekday to allow for the types of non-patient-care work listed below:
Chart 11
|
Assume the amount of research accomplished at this VAMC is: |
High1 |
Medium1 |
Low1 |
|
|
Education of Residents (didactic, classroom, not on the PCA) |
High |
4.00 |
1.00 |
0.80 |
|
Low |
0.50 |
0.50 |
0.00 |
|
|
Mean |
1.80 |
0.60 |
0.40 |
|
|
Median |
1.50 |
0.50 |
0.50 |
|
|
Administration by Chief (time required to manage your whole service by a Chief and/or Assistant Chief) |
High |
8.00 |
6.00 |
4.00 |
|
Low |
1.50 |
0.75 |
1.50 |
|
|
Mean |
3.40 |
2.60 |
2.10 |
|
|
Median |
2.00 |
2.00 |
2.50 |
|
|
Administration by Others (time required per individual-non chief-physician |
High |
2.00 |
1.00 |
1.00 |
|
Low |
0.50 |
0.25 |
0.15 |
|
|
Mean |
0.90 |
0.50 |
0.50 |
|
|
Median |
0.60 |
0.50 |
0.50 |
|
|
Hospital-Related Activities (Mortality and Morbidity, Q.A., Staff Meetings) |
High |
1.10 |
1.10 |
1.10 |
|
Low |
0.25 |
0.25 |
0.25 |
|
|
Mean |
0.70 |
0.70 |
0.70 |
|
|
Median |
0.50 |
0.80 |
0.80 |
|
|
1Examples of research level by total amount of funding (VA plus non-VA) in FY 1988: High: e.g., VAMC I with $8.8 million in total funding; Median: e.g., VAMC II with $2.75 million in total funding; Low: e.g., VAMC III with about $176,000 in total funding. |
||||
|
Assume the amount of research accomplished at this VAMC is: |
High1 |
Medium1 |
Low1 |
|
|
Total Hours per Average Weekday |
||||
|
For Chief2 |
Overall |
3.40 |
2.60 |
2.10 |
|
Mean |
2.00 |
2.00 |
2.50 |
|
|
For Non-Chief |
Overall |
2.80 |
2.00 |
1.60 |
|
Mean |
2.25 |
2.00 |
1.50 |
|
|
1Examples of research level by total amount of funding (VA plus non-VA) in FY 1988: High: e.g., VAMC I with $8.8 million in total funding; Medium: e.g., VAMC II with $2.75 million in total funding; Low: e.g., VAMC III with about $176,000 in total funding. 2Assume that Chief does not participate significantly in the Education of Residents and Hospital-Related Activities; SADI users may easily modify this assumption. |
||||
Part 2. In order to determine the actual staffing in this hospital, the number of FTEE must be adjusted to allow for CME, research, and any off-time required. What do you believe to be the appropriate percentage of time the “average” (typical) staff (nonresident) member of your service should devote to each of the following categories of non-patient-care-related activities?
Chart 12
|
Assume the amount of research accomplished at this VAMC is: |
High1 |
Medium1 |
Low1 |
|
Continuing Education |
7 |
7 |
7 |
|
Research (off the PCA) |
30 |
15 |
2 |
|
Vacation, Administrative Leave, Sick Leave, Other |
10 |
10 |
10 |
|
Total Percentage of Time |
|||
|
Mean |
45 |
31 |
19 |
|
Median |
47 |
32 |
19 |
|
1Examples of research level by total amount of funding (VA plus non-VA) in FY 1988: High: e.g., VAMC I with $8.8 million in total funding; Median: e.g., VAMC II with $2.75 million in total funding; Low: e.g., VAMC III with about $176,000 in total funding. |
|||
FIGURE 2 The Staffing Algorithm Development Instrument (SADI) for Anesthesiology: The Complete Instrument with Statistical Summary of the Panel's Assessments
INTRODUCTION AND INSTRUCTIONS (Abbreviated)
The purpose of the SADI is to gather the data needed to construct, test, formalize, and enhance the algorithms and rules of thumb for staffing that emerged from prior meetings of each specialty and clinical program panel. The ultimate intention is to develop algorithms which could be applied to estimate staffing requirements at VA medical centers, presumably duplicating the results specialty and clinical program panelists themselves would have derived.
Section A of the SADI requests time estimates, in some cases by workload unit. In other cases, it requests time estimates by major job elements (tasks). These elements had previously been indicated by some panel members as accounting for the bulk of the work of VA anesthesiologists. We seek your estimates of how physician requirements in your specialty vary with respect to such variables as the volume of patients and the availability of residents and nonphysician practitioners. By systematically varying the levels of workload and personnel, we hope to infer from your numerical responses the implicit formulas you used to relate physician time to these variables as well as the nature of the relationship between workload and staffing, e.g., linear or non-linear.
Section B seeks responses to a series of questions for the time spent in activities other than direct patient care.
Instructions: In Section A, for each cell of each table, please estimate the number of physician hours required from the Anesthesiology Service to deliver good-quality care under the specified circumstances. Section B is self-explanatory.
SECTION A: PATIENT CARE ACTIVITIES—ANESTHESIOLOGY
ADMISSIONS—AVERAGE CASELOAD
Please fill in the average time in hours required by a staff physician in your service to accomplish an admission work-up, for a caseload of “average” severity, either with or without the assistance of a resident in your service. This “average” caseload will, of course, consist of a mix of highly complicated, moderately complicated, and uncomplicated patients.
Chart 1
|
Time per Admission Work-Up Without Resident |
Time per Admission Work-Up with Resident (Resident Does Work-Up, Staff Physician Reviews Data) |
||||
|
Mid-pt |
Mid-pt |
||||
|
0.50 |
0.20 |
0.35 |
0.20 |
0.60 |
0.40 |
NEW ADMISSIONS—COMPLICATED CASELOAD
Please fill in the average time in hours required by a staff physician in your service to accomplish an admission work-up for a typical caseload only of complicated patients, either with or without the assistance of a resident in your service. This “typical” caseload will, of course, present the very difficult and more complex patients characterized as “highly complicated” patients.
Chart 2
|
Time per Admission Work-Up Without Resident |
Time per Admission Work-Up with Resident (Resident Does Work-Up, Staff Physician Reviews Data) |
||||
|
Mid-pt. |
Mid-pt. |
||||
|
1.20 |
0.50 |
0.85 |
0.30 |
1.00 |
0.65 |
ROUTINE DAILY PATIENT CARE—AVERAGE CASELOAD
For each workload factor and alternative average daily census (ADC) level below, please fill in the average number of physician hours required from the anesthesiology service for a caseload of “average ” severity for an average weekday. This “average” caseload will, of course, consist of a mix of highly complicated, moderately complicated, and uncomplicated patients. In responding, assume the proportion of each type of case reflects what one would expect in a typical VAMC with a university-sponsored affiliation in surgery (and perhaps with other specialties). Keep in mind that the Daily Rounds do not include new admission work-ups, since they are covered in Charts 1.
Chart 3
|
Assume No Residents |
|||||||
|
General Surgery Ward Average LOS=7 |
ADC 5 |
ADC 10 |
ADC 15 |
ADC 20 |
ADC 25 |
ADC 30 |
|
|
Daily Rounds |
Low |
0.40 |
0.80 |
1.20 |
1.60 |
2.00 |
2.40 |
|
High |
0.50 |
1.00 |
1.51 |
2.00 |
2.50 |
3.00 |
|
|
Median |
0.45 |
0.90 |
1.35 |
1.80 |
2.25 |
2.70 |
|
|
Charting, Phone, and Paperwork |
Low |
0.00 |
0.00 |
0.00 |
0.00 |
0.00 |
0.00 |
|
High |
0.50 |
1.00 |
1.50 |
2.00 |
2.50 |
3.00 |
|
|
Median |
0.45 |
0.50 |
0.75 |
1.00 |
1.25 |
1.50 |
|
|
Patient and Family Contacts and Teaching |
Low |
0.00 |
0.00 |
0.00 |
0.00 |
0.00 |
0.00 |
|
High |
0.00 |
0.00 |
0.00 |
0.00 |
0.00 |
0.00 |
|
|
Median |
0.00 |
0.00 |
0.00 |
0.00 |
0.00 |
0.00 |
|
|
Supervision and Teaching (Residents/Staff) |
Low |
0.40 |
0.40 |
0.40 |
0.40 |
0.40 |
0.40 |
|
High |
0.50 |
1.00 |
1.00 |
1.00 |
1.00 |
1.00 |
|
|
Median |
0.45 |
0.70 |
0.70 |
0.70 |
0.70 |
0.70 |
|
|
Assume No Residents |
|||||||
|
General Surgery Ward Average LOS=7 |
ADC 5 |
ADC 10 |
ADC 15 |
ADC 20 |
ADC 25 |
ADC 30 |
|
|
Any Special Procedures Apart from those Conducted on SICU (e.g., Starting IVs, Thoracentesis, Inserting Urinary Catheters, and Suture Removal) |
Low |
0.20 |
0.20 |
0.20 |
0.40 |
0.40 |
0.40 |
|
High |
0.00 |
0.00 |
0.00 |
0.00 |
0.00 |
0.00 |
|
|
Median |
0.10 |
0.10 |
0.10 |
0.20 |
0.20 |
0.20 |
|
|
Total |
Low |
1.00 |
1.40 |
1.80 |
2.40 |
2.80 |
3.20 |
|
High |
1.50 |
3.00 |
4.00 |
5.00 |
6.00 |
7.00 |
|
|
Median |
1.25 |
2.20 |
2.90 |
3.70 |
4.40 |
5.10 |
|
Chart 4
|
Assume Full Component of Residents (PGY1–5) Integrated with Residents of an Affiliated University |
|||||||
|
General Surgery Ward Average LOS=7 |
ADC 5 |
ADC 10 |
ADC 15 |
ADC 20 |
ADC 25 |
ADC 30 |
|
|
Daily Rounds |
Low |
0.10 |
0.20 |
0.30 |
0.40 |
0.50 |
0.60 |
|
High |
0.50 |
0.50 |
0.75 |
1.00 |
1.00 |
1.00 |
|
|
Median |
0.30 |
3.50 |
0.53 |
0.70 |
0.75 |
0.80 |
|
|
Charting, Phone, and Paperwork |
Low |
0.10 |
0.10 |
0.20 |
0.20 |
0.30 |
0.30 |
|
High |
0.00 |
0.00 |
0.00 |
0.00 |
0.00 |
0.00 |
|
|
Median |
0.05 |
0.05 |
0.10 |
0.10 |
0.15 |
0.15 |
|
|
Patient and Family Contact and Teaching |
Low |
0.00 |
0.00 |
0.00 |
0.00 |
0.00 |
0.00 |
|
High |
0.00 |
0.00 |
0.00 |
0.00 |
0.00 |
0.00 |
|
|
Median |
0.00 |
0.00 |
0.00 |
0.00 |
0.00 |
0.00 |
|
|
Supervision and Teaching Residents/Staff |
Low |
0.50 |
0.50 |
0.50 |
0.50 |
1.00 |
1.00 |
|
High |
0.50 |
0.50 |
0.50 |
1.00 |
1.00 |
1.00 |
|
|
Median |
0.50 |
0.50 |
0.50 |
0.75 |
1.00 |
1.00 |
|
|
Any special procedures apart from those conducted on SICU (e.g., Starting IVs, Thoracentesis, Inserting Urinary Catheters, and Suture Removal) |
Low |
0.20 |
0.20 |
0.20 |
0.40 |
0.40 |
0.40 |
|
High |
0.00 |
0.00 |
0.00 |
0.00 |
0.00 |
0.00 |
|
|
Median |
0.10 |
0.10 |
0.10 |
0.20 |
0.20 |
0.20 |
|
|
Total |
Low |
0.90 |
1.00 |
1.20 |
1.50 |
2.20 |
2.30 |
|
High |
1.00 |
1.00 |
1.25 |
2.00 |
2.00 |
2.00 |
|
|
Median |
0.95 |
1.00 |
1.23 |
1.75 |
2.10 |
2.15 |
|
ROUTINE DAILY PATIENT CARE—COMPLICATED CASELOAD
For each workload factor and alternative average daily census (ADC) level below, please fill in the average number of physician hours required from the anesthesiology service for a typical caseload only of complicated patients. This “typical” caseload will, of course, present the very difficult and more complex patients characterized as “highly complicated” patients. In responding, assume the proportion of each type of case reflects what one would expect in a typical VAMC with a university-sponsored affiliation in surgery (and perhaps with other specialties). Keep in mind that the Daily Rounds do not include new admission work-ups, since they are covered in Chart 2.
Chart 5
|
Assume No Residents |
|||||||
|
General Surgery Ward Average LOS=7 |
ADC 5 |
ADC 10 |
ADC 15 |
ADC 20 |
ADC 25 |
ADC 30 |
|
|
Daily Rounds |
Low |
0.30 |
0.60 |
0.90 |
1.20 |
1.50 |
1.80 |
|
High |
1.00 |
2.00 |
3.00 |
3.50 |
4.00 |
4.50 |
|
|
Median |
0.65 |
1.30 |
1.95 |
2.35 |
2.75 |
3.15 |
|
|
Charting, Phone, and Paperwork |
Low |
0.20 |
0.40 |
0.60 |
0.80 |
1.00 |
1.20 |
|
High |
0.20 |
0.50 |
1.00 |
1.50 |
2.00 |
2.50 |
|
|
Median |
0.20 |
0.45 |
0.80 |
1.15 |
1.50 |
1.85 |
|
|
Patient and Family Contacts and Teaching |
Low |
0.20 |
0.40 |
0.60 |
0.80 |
1.00 |
1.20 |
|
High |
0.00 |
0.00 |
0.00 |
0.00 |
0.00 |
0.00 |
|
|
Median |
0.10 |
0.20 |
0.30 |
0.40 |
0.50 |
0.60 |
|
|
Supervision and Teaching (Residents/Staff) |
Low |
0.40 |
0.40 |
0.40 |
0.40 |
0.40 |
0.40 |
|
High |
0.50 |
0.50 |
0.50 |
0.50 |
1.00 |
1.00 |
|
|
Median |
0.45 |
0.45 |
0.45 |
0.45 |
0.70 |
0.70 |
|
|
Assume No Residents |
|||||||
|
General Surgery Ward Average LOS=7 |
ADC 5 |
ADC 10 |
ADC 15 |
ADC 20 |
ADC 25 |
ADC 30 |
|
|
Any special procedures apart from those conducted on SICU (e.g., Starting IVs, Thoracentesis, Inserting Urinary Catheters, and Suture Removal) |
Low |
0.20 |
0.40 |
0.50 |
0.80 |
1.00 |
1.20 |
|
High |
0.00 |
0.00 |
0.00 |
0.00 |
0.00 |
0.00 |
|
|
Median |
0.10 |
0.20 |
0.30 |
0.40 |
0.50 |
0.60 |
|
|
Total |
Low |
1.30 |
2.20 |
3.10 |
3.00 |
2.45 |
5.80 |
|
High |
1.70 |
3.00 |
4.50 |
5.50 |
7.00 |
8.00 |
|
|
Median |
1.50 |
2.50 |
3.80 |
4.25 |
4.73 |
6.90 |
|
Chart 6
|
Assume Full Component of Residents (PGY1–5) Integrated with Residents of an Affiliated University |
|||||||
|
General Surgery Ward Average LOS=7 |
ADC 5 |
ADC 10 |
ADC 15 |
ADC 20 |
ADC 25 |
ADC 30 |
|
|
Daily Rounds |
Low |
0.20 |
0.40 |
0.60 |
0.80 |
1.00 |
1.20 |
|
High |
0.50 |
1.00 |
1.50 |
2.00 |
2.50 |
2.50 |
|
|
Median |
0.35 |
0.70 |
1.05 |
1.40 |
1.75 |
1.85 |
|
|
Charting, Phone, and Paperwork |
Low |
0.10 |
0.20 |
0.30 |
0.40 |
0.50 |
0.60 |
|
High |
0.00 |
0.00 |
0.00 |
0.00 |
0.00 |
0.00 |
|
|
Median |
0.50 |
0.10 |
0.15 |
0.20 |
0.25 |
0.30 |
|
|
Patient and Family Contacts and Teaching |
Low |
0.10 |
0.20 |
0.30 |
0.40 |
0.50 |
0.60 |
|
High |
0.00 |
0.00 |
0.00 |
0.00 |
0.00 |
0.00 |
|
|
Median |
0.05 |
0.10 |
0.15 |
0.20 |
0.25 |
0.30 |
|
|
Supervision and Teaching Residents/Staff |
Low |
0.50 |
1.00 |
1.50 |
2.00 |
2.50 |
3.00 |
|
High |
0.50 |
1.00 |
1.50 |
2.00 |
2.00 |
2.00 |
|
|
Median |
0.90 |
1.00 |
1.50 |
2.00 |
2.25 |
3.00 |
|
|
Any special procedures apart from those conducted on SICU (e.g., Starting IVs, Thoracentesis, Inserting Urinary Catheters, and Suture Removal) |
Low |
0.20 |
0.20 |
0.20 |
0.40 |
0.40 |
0.40 |
|
High |
0.00 |
0.00 |
0.00 |
0.00 |
0.00 |
0.00 |
|
|
Median |
0.10 |
0.10 |
0.10 |
0.20 |
0.20 |
0.20 |
|
|
Total |
Low |
1.10 |
2.00 |
2.90 |
4.00 |
4.90 |
5.80 |
|
High |
1.00 |
2.00 |
3.00 |
4.00 |
4.50 |
4.50 |
|
|
Median |
1.05 |
2.00 |
2.95 |
4.00 |
4.70 |
5.15 |
|
Chart 7
|
Assume Full Component of Residents (PGY1–5) Integrated with Residents of an Affiliated University |
|||||||
|
SICU UNIT Average LOS=5 |
ADC 3 |
ADC 5 |
ADC 7 |
ADC 9 |
ADC 11 |
ADC 13 |
|
|
Daily Rounds |
Low |
0.20 |
0.20 |
0.30 |
0.40 |
0.60 |
0.80 |
|
High |
0.30 |
0.50 |
0.70 |
0.90 |
1.10 |
1.30 |
|
|
Median |
0.25 |
0.35 |
0.50 |
0.65 |
0.85 |
1.15 |
|
|
Charting, Phone, and Paperwork |
Low |
0.10 |
0.10 |
0.20 |
0.20 |
0.30 |
0.40 |
|
High |
0.50 |
0.70 |
0.90 |
1.10 |
1.30 |
1.50 |
|
|
Median |
0.30 |
0.40 |
0.55 |
0.65 |
0.80 |
0.95 |
|
|
Patient and Family Contacts and Teaching |
Low |
0.10 |
0.10 |
0.20 |
0.20 |
0.30 |
0.40 |
|
High |
0.10 |
0.20 |
0.30 |
0.50 |
0.70 |
1.00 |
|
|
Median |
0.10 |
0.15 |
0.25 |
0.35 |
0.50 |
0.70 |
|
|
Supervision and Teaching Residents/Staff |
Low |
0.50 |
0.75 |
1.00 |
1.25 |
1.50 |
2.00 |
|
High |
1.00 |
1.00 |
1.00 |
1.50 |
2.00 |
2.00 |
|
|
Median |
0.75 |
0.88 |
1.00 |
1.38 |
1.75 |
2.00 |
|
|
Any special procedures (e.g., Insertion of Monitors and Nutritional Devices) |
Low |
0.20 |
0.20 |
0.40 |
0.40 |
0.40 |
0.40 |
|
High |
0.20 |
0.30 |
0.50 |
0.80 |
1.00 |
1.20 |
|
|
Median |
0.20 |
0.25 |
0.45 |
0.60 |
0.70 |
0.80 |
|
|
Total |
Low |
1.10 |
1.35 |
2.10 |
2.45 |
3.10 |
4.00 |
|
High |
1.20 |
2.70 |
3.40 |
4.80 |
6.10 |
7.00 |
|
|
Median |
1.15 |
2.04 |
2.75 |
3.93 |
4.60 |
5.50 |
|
TIME PER INITIAL CONSULTATION OFF YOUR PCA
Fill in the average time in hours required by a staff physician in your service for each initial (new) consult on another service, noting the presence or absence of a resident in your own service. (When the resident is present, assume that he/she is performing the consult under the supervision of an attending physician.)
Chart 8
|
Consultation off your PCA |
Time per Consult without Resident |
Time per Consult with Resident |
||||
|
Neurology |
1.20 |
0.50 |
0.85 |
0.30 |
0.20 |
0.25 |
|
Medicine |
1.20 |
0.50 |
0.85 |
0.30 |
0.20 |
0.25 |
|
Nursing Home |
1.20 |
0.00 |
1.20 |
0.30 |
0.00 |
0.30 |
|
Intermediate Care |
1.20 |
0.00 |
1.20 |
0.30 |
0.00 |
0.30 |
|
Rehab Med |
1.20 |
0.5–1.0 |
1.00 |
0.30 |
0.30 |
0.30 |
|
Psychiatry |
1.20 |
0.00 |
1.20 |
0.30 |
0.00 |
0.30 |
|
Surgery |
1.20 |
0.5–1.0 |
1.00 |
0.30 |
0.50 |
0.40 |
TIME PER FOLLOW-UP VISIT (POST-CONSULTATION) OFF YOUR PCA
Fill in the average time in hours required by a staff physician in your service for each follow-up consultation visit (post-consultation) on another service, noting the presence or absence of a resident from your service.
Chart 9
|
Follow-Up Visit (Post-consult) |
Time per Visit without Resident |
Time per Visit with Resident |
||||
|
Neurology |
0.30 |
0.20 |
0.25 |
0.10 |
0.10 |
0.10 |
|
Medicine |
0.30 |
0.20 |
0.25 |
0.10 |
0.10 |
0.10 |
|
Nursing Home |
0.30 |
0.00 |
0.30 |
0.10 |
0.00 |
0.10 |
|
Intermediate Care |
0.30 |
0.20 |
0.25 |
0.10 |
0.10 |
0.10 |
|
Rehab Med |
0.30 |
0.00 |
0.30 |
0.10 |
0.00 |
0.10 |
|
Psychiatry |
0.30 |
0.20 |
0.25 |
0.10 |
0.10 |
0.10 |
|
Surgery |
0.30 |
0.00 |
0.30 |
0.10 |
0.00 |
0.10 |
SECTION B: NON-PATIENT-CARE TIME
Part 1. The activities listed below generally do not occur every day, but may be time consuming when looked at over a longer period of time, such as a week or month. List the time in hours that you would add to each physician's average weekday to allow for the types of non-patient-care work listed below:
Chart 10
|
Assume the amount of research accomplished at this VAMC is: |
High1 |
Medium1 |
Low1 |
|
|
Education of Residents (didactic, classroom, not on the PCA) |
High |
0.50 |
0.50 |
0.50 |
|
Low |
3.00 |
2.00 |
1.00 |
|
|
Midpoint |
1.75 |
1.25 |
0.75 |
|
|
Administration by Chief (time required to manage your whole service by a Chief and/or Assistant Chief) |
High |
3.00 |
2.00 |
2.00 |
|
Low |
5.00 |
4.00 |
3.00 |
|
|
Midpoint |
4.00 |
3.00 |
1.50 |
|
|
Administration by Others (time required per individual—non-chief— physician) |
High |
1.00 |
0.50 |
0.50 |
|
Low |
2.00 |
1.00 |
1.00 |
|
|
Midpoint |
1.50 |
0.75 |
0.75 |
|
|
Hospital-Related Activities (Mortality and Morbidity, Q.A., Staff Meeting) |
High |
1.00 |
0.50 |
0.50 |
|
Low |
3.00 |
2.00 |
2.00 |
|
|
Midpoint |
2.00 |
1.25 |
1.25 |
|
|
1Examples of research level by total amount of funding (VA plus non-VA) in FY 1988. High: e.g., VAMC I with $8.8 million in total funding; Medium: e.g., VAMC II with $2.75 million in total funding; Low: e.g., VAMC III with about $176,000 in total funding. |
||||
|
Assume the amount of research accomplished at this VAMC is: |
High1 |
Medium1 |
Low1 |
|
|
Total Hours Per Average Weekday: |
||||
|
Chief2 |
High |
3.00 |
2.00 |
2.00 |
|
Low |
5.00 |
4.00 |
3.00 |
|
|
Midpoint |
4.00 |
3.00 |
1.50 |
|
|
Other |
High |
2.50 |
1.50 |
1.50 |
|
Low |
8.00 |
5.00 |
4.00 |
|
|
Midpoint |
5.25 |
3.25 |
2.75 |
|
|
1Examples of research level by total amount of funding (VA plus non-VA) in FY 1988. High: e.g., VAMC I with $8.8 million in total funding; Medium: e.g., VAMC II with $2.75 million in total funding; Low: e.g., VAMC III with about $176,000 in total funding. 2Assume that Chief does not participate significantly in the Education of Residents and Hospital-Related Activities; SADI users may easily modify this assumption. |
||||
Part 2. In order to determine the actual staffing in this hospital, the number of FTEE must be adjusted to allow for CME, research, and any off-time required. What do you believe to be the appropriate percentage of time the “average” (typical) staff (nonresident) member of your service should devote to each of the following categories of non-patient-care-related activities?
Chart 11
|
Assume the amount of research accomplished at this VAMC is: |
High1 |
Medium1 |
Low1 |
|
Continuing Education |
7 |
7 |
7 |
|
Research (off the PCA) |
30 |
15 |
2 |
|
Vacation, Administrative Leave, Sick Leave, Other |
10 |
10 |
10 |
|
Total Percentage of Time |
47 |
32 |
19 |
|
1Examples of research level by total amount of funding (VA plus non-VA) in FY 1988: High: e.g., VAMC I with $8.8 million in total funding; Medium: e.g., VAMC II with $2.75 million in total funding; Low: e.g., VAMC III with about $176,000 in total funding. |
|||
ADDITIONAL QUESTIONS FOR ANESTHESIOLOGY
For each of the following combinations of operating rooms (in use), level of resident/CRNA support, and number of operative procedures per day, please estimate the average time (in hours) required of anesthesiologists:
Chart 12
|
Procedures per Day—Assume Six Major OR Suites and One Cysto Room |
||||||
|
Major Suites |
6 |
12 |
14 |
16 |
18 |
|
|
Cysto Room |
1 |
2 |
2 |
0 |
3 |
|
|
No Resident No CRNA |
Low |
19.50 |
39.00 |
45.00 |
48.00 |
58.50 |
|
High |
24.00 |
42.00 |
45.00 |
48.00 |
56.00 |
|
|
Median |
21.75 |
40.50 |
45.00 |
48.00 |
57.25 |
|
|
One Resident No CRNA |
Low |
10.50 |
21.00 |
24.00 |
24.00 |
31.50 |
|
High |
24.00 |
42.00 |
45.00 |
48.00 |
56.00 |
|
|
Median |
17.25 |
30.50 |
34.50 |
36.00 |
43.75 |
|
|
No Resident One CRNA |
Low |
10.50 |
21.00 |
24.00 |
24.00 |
31.50 |
|
High |
24.00 |
42.00 |
45.00 |
48.00 |
56.00 |
|
|
Median |
17.25 |
30.50 |
34.50 |
36.00 |
43.75 |
|
Chart 13
|
Procedures per Day—Assume Four Major OR Suites, One Cysto Room, and One Endo Room |
||||||
|
Major OR Suites |
4 |
8 |
13 |
15 |
16 |
|
|
Cysto Room |
1 |
1 |
1 |
0 |
1 |
|
|
Endo Room |
1 |
1 |
1 |
0 |
1 |
|
|
No Resident No CRNA |
Low |
15.00 |
21.00 |
42.00 |
45.00 |
51.00 |
|
High |
16.00 |
32.00 |
40.00 |
45.00 |
49.00 |
|
|
Median |
15.50 |
26.50 |
41.00 |
45.00 |
50.00 |
|
|
One Resident No CRNA |
Low |
7.50 |
10.50 |
22.50 |
24.00 |
25.50 |
|
High |
16.00 |
32.00 |
40.00 |
45.00 |
49.00 |
|
|
Median |
11.50 |
16.25 |
31.25 |
34.50 |
37.25 |
|
|
No Resident |
Low |
7.50 |
10.50 |
22.50 |
24.00 |
22.50 |
|
High |
16.00 |
32.00 |
40.00 |
45.00 |
49.00 |
|
|
Median |
11.50 |
16.25 |
31.25 |
34.50 |
37.25 |
|
Chart 14
|
Procedures per Day—Assume Seven Major OR Suites, Two Cysto Rooms, and Two Eye Rooms |
||||||
|
Major Suites |
7 |
14 |
20 |
26 |
26 |
|
|
Cysto Room |
2 |
2 |
3 |
0 |
3 |
|
|
Eye Room |
2 |
2 |
3 |
0 |
3 |
|
|
No Resident No CRNA |
Low |
27.00 |
48.00 |
78.00 |
78.00 |
87.00 |
|
High |
26.00 |
50.00 |
63.00 |
78.00 |
81.00 |
|
|
Median |
26.50 |
49.00 |
70.50 |
78.00 |
84.00 |
|
|
One Resident No CRNA |
Low |
15.00 |
27.00 |
39.00 |
45.00 |
51.00 |
|
High |
26.00 |
50.00 |
63.00 |
78.00 |
81.00 |
|
|
Median |
20.50 |
38.50 |
51.00 |
61.50 |
66.00 |
|
|
No Resident One CRNA |
Low |
12.00 |
27.00 |
39.00 |
45.00 |
51.00 |
|
High |
26.00 |
50.00 |
63.00 |
78.00 |
81.00 |
|
|
Median |
19.00 |
38.50 |
51.00 |
61.50 |
66.00 |
|
INSTITUTE OF MEDICINE
Committee to Develop Methods Useful to the Department of Veterans Affairs in Estimating Its Physician Requirements
SURGERY PANEL
DAVID C.SABISTON, Jr. (Chair),*† Professor and Chairman, Department of Surgery, Duke University Medical Center, Durham, North Carolina
ELIZABETH BATES, Director, Health Services Research and Development, Ann Arbor VA Medical Center, Ann Arbor, Michigan
KIRBY I.BLAND, Professor and Associate Chairman, Department of Surgery, University of Florida College of Medicine, Gainesville
DON E.DETMER,* Vice President for Health Sciences, University of Virginia, Charlottesville
McIVER W.EDWARDS, Chief, Anesthesiology Section, Philadelphia VA Medical Center, Philadelphia, Pennsylvania
JAMES M.GUERNSEY, Chief, Surgical Service, Martinez VA Medical Center, Martinez, California
RONALD D.MILLER, Professor and Chairman, Department of Anesthesia, University of California at San Francisco
VALLEE L.WILLMAN, Professor and Chairman, Department of Surgery, St. Louis University Hospital, St. Louis, Missouri
MARK W.WOLCOTT, Chief, Surgical Service, Salt Lake City VA Medical Center, Salt Lake City, Utah
Staff: Bobbie J.Alexander, Staff Associate
|
*Member of the Institute of Medicine. |
|
†Member of the study committee. |






























































