
NEUROLOGY PANEL REPORT1
INTRODUCTION
This panel was established in early 1990 to assist the IOM study committee in developing a VA physician requirements methodology that successfully incorporated the specialty of neurology. The panel, consisting of five neurologists, met twice during the year and participated in other efforts to advise the study committee on appropriate physician staffing for this specialty. The chairman of the panel was a member of the study committee; the panel roster is attached. A detailed description of the analysis process followed by this and the other seven specialty and clinical program panels is found in the “Overview ” to this section of Volume II.
The following report summarizes the analyses conducted by the panel and its recommendations to the study committee.
EXPERT JUDGMENT APPROACHES TO DETERMINING PHYSICIAN REQUIREMENTS IN NEUROLOGY
The Detailed Staffing Exercise (DSE) Approach
Initial Efforts
A central purpose of the panel's first meeting, held in March 1990, was to help determine whether the expert judgment approach to staffing being developed by the study committee could be applied validly to neurology. The focus of this analysis was the initial draft of a physician staffing instrument,
|
1 |
The initial draft of this report was prepared by Nancy Kader, Staff Officer to the Neurology Panel during the conduct of the study. This final report was prepared by the editors of this Volume. |
which required the expert to assess the time (and hence FTEE) required by neurologists to render patient care, work with residents, and perform other tasks at the VA medical center. To test this approach, staffing instruments were constructed for three actual VAMCs. Each facility was portrayed as consisting of a set of patient care areas (PCAs), where direct patient care and resident training occur. For each PCA, data were presented on the volume of patient workload expected, the number of residents available, and the overall availability of nursing and support staff. The critical question with respect to each PCA focuses on the amount of neurologist time required, in total, to meet these VA mission-related demands in the course of a typical workday. Each PCA was analyzed in turn, and total neurologist FTEE for the facility was computed. Additional questions at the end of the instrument elicited FTEE requirements for weekend coverage, special procedures, and non-VA physician consultants.
In the course of this first meeting the panel reached several initial conclusions about the assumptions that should underlie the development of subsequent physician staffing instruments:
-
Education of staff and residents is carried out mostly in the clinical setting, often as part of daily rounds. However, education time is not always documented properly in the VA's cost distribution report (CDR) for the neurology service. It is often allocated under the cost center for medicine.
-
Insufficient nurse and support staff is a major factor in reducing the efficiency of neurologists and may reduce the quality of care.
-
Physicians generally work 50 or more hours weekly, but 40 was used in estimating requirements in order to be consistent across panels.
-
The amount of research varies by the individual physician and is sometimes obscured by university exchanges. Research per physician cannot be inferred on the basis of the direct patient care requirements.
-
Vacation, leave, and sick time are not currently considered in physician requirements, and might be derived via a “multiplier” applied to the direct care requirements.
-
Although there was a great deal of debate about the issue of night and weekend coverage, panelists generally agreed that it is usually provided by “house officers” who are not purchased specifically by the neurology service, or else by residents. Therefore no extra staff physician FTEE would be allocated specifically for these off-hours.
-
The number of patients currently receiving neurology services is not an indicator of need, since a current lack of physician staffing in this specialty discourages many patients from presenting for treatment. Nonetheless, the panel
-
agreed to continue estimating physician requirements for the actual volume of workload anticipated, in keeping with the overall philosophy of the larger study.
-
The panelists believed that, in many cases, neurologists should have primary responsibility for administering the spinal cord injury (SCI) service and performing electromyocardiogram (EMG) procedures; however, it was recognized that physiatrists typically play this role in the VA at present. Hence, it would be assumed that neurologists would serve largely as consultants in the delivery of SCI and EMG procedures.
At this first meeting the panel also reviewed and evaluated the initial versions of the empirically based physician staffing model. A special concern, identified early on, was whether the VA's CDR properly captured the productive contributions of neurologists at the VAMCs.
Following the first round of meetings for all eight specialty and clinical program panels, there was convened (in May 1990) Joint Meeting I involving the study committee, data and methodology panel, and VA liaison committee. Progress to date on both the expert judgment and empirical model approaches was evaluated. After reviewing the reports submitted by each panel, the study committee recommended that work proceed on developing a more internally consistent and comprehensive instrument for determining physician requirements by expert judgment. A broadly similar approach should be adopted by each panel, but the instrument for each specialty or program area should be tailored to its specific characteristics.
DSE: Overall Rationale
For the panel's second meeting, held in June 1990, three additional VAMCs (denoted here and in the committee report [Volume I] as VAMCs I, II, and III) were analyzed using a revised version of the initial staffing instrument. This new instrument—later termed the Detailed Staffing Exercise (DSE) —was developed on the basis of the panel's critique delivered at the first meeting, plus general instructions from the study committee at the conclusion of Joint Meeting I. As before, each DSE was specific to an actual VAMC. This revised instrument described each PCA in greater detail than before, including more specific information on the VA patient population (e.g., admission rate, length of stay, and DRG mix). The ambulatory care clinics at each VAMC were now described in much greater detail.
In general, the underlying concept behind the DSE is to provide information in sufficient detail about the VAMC that the respondent can assess physician staffing requirements almost as if he/she were reviewing data at the facility.
Instructions and Assumptions
To illustrate how the DSE works, a completed version of the instrument is presented as Exhibit 1 of the “Overview” to this section of Volume II. While constructed specifically for determining internist FTEE requirements, this DSE is nearly identical structurally to the one developed for neurology.
As indicated in that Exhibit 1, each DSE has an A and B section. Section A elicits the amount of time, in hours, required to provide quality care for individual patient care areas (PCAs) of the hospital. For each PCA, information is provided on the volume and DRG mix of workload, number of residents by postgraduate year, number of nonphysician practitioners (e.g., nurse practitioners, physician assistants), and general information about the adequacy of nursing and support staff. Section B focuses on physician activities not addressed in Section A, such as night and weekend coverage, non-patient-care-related activities off the PCA, and leaves of absence.
The Panel Responds
Before the second meeting, panelists were mailed DSEs for VAMCs I and II; these were completed independently and returned prior to the meeting. The staff compiled these results on a spreadsheet showing the high, low, mean, and median responses.
At the second panel meeting, these DSEs were discussed thoroughly to determine whether panelists were using the same assumptions and to allow members to discuss the underlying reasoning behind these calculations.
Following this, the panelists were asked to reassess physician requirements in medicine at VAMCs I and II, again working independently. Then the actual level of neurologist staffing at each VAMC, as reported in the CDR, was displayed for comparison.
After discussion of actual versus DSE-based staffing, a third exercise was distributed pertaining now to VAMC III (another actual facility), and the panel worked as a group to estimate staffing requirements. Following the assessment, the actual CDR numbers for VAMC in were displayed for comparison. During
The Staffing Algorithm Development Instrument (SADI) Approach
SADI: Overall Rationale
Following the second round of panel meetings, the study committee initiated a set of “postmeeting” activities to assist the specialty and clinical program panels in arriving at consensus positions regarding the most appropriate methodology for VA physician staffing. These recommendations should be regarded as being advisory to the committee.
A central feature of these activities was the introduction of the Staffing Algorithm Development Instrument (SADI). The overall purpose of the SADI was to help test, build upon, and ultimately strengthen the rules of thumb for staffing that emerged from the second meetings of all eight panels. It represents an alternative, more compact means to derive physician requirements, by specialty or program, for any given VAMC.
Instructions and Assumptions
Like the DSE, the SADI has two sections, A and B, which focus on patient care and nonpatient care activities, respectively. In Section A, the respondent is asked to estimate the amount of physician time required to complete a number of patient care functions and tasks under varying assumptions about the availability of residents and nonphysician practitioners. In section B, the respondent must determine the amount of physician time that should be allocated to research, classroom instruction, continuing education, administra-tion, and leaves of absence. To derive physician requirements for a given VAMC, the estimated physician hours for patient care and nonpatient care activities are summed, then converted to FTEE under the assumption that 40 hours per week translates into one FTEE. (Obviously, if this 40-hour-per-week equivalency assumption is replaced by one reflecting the average workweek of full-time VA staff physicians, the SADI-derived FTEE estimates would change accordingly; this is true also for the DSE estimates.)
Presented in Figure 1 of this report is the neurology SADI, complete with the panel's median estimates for physician task times. A detailed, self-contained, illustration of how the SADI can be applied to determine the number of physicians required at a given VAMC is found in Exhibit 3 of the “Overview” to this section of Volume II. This example happens to focus on internist requirements at VAMC I; the application of SADI to determining
neurology FTEE at a given facility proceeds in a virtually identical fashion. A careful study of the example reveals the type of facility-specific data needed to implement any SADI. Although the information requirements of the DSE are greater, both of these expert judgment approaches require data (e.g., on frequency of consults across PCAs) not presently collected in the VA system.
EMPIRICALLY BASED APPROACHES TO DETERMINING PHYSICIAN STAFFING IN NEUROLOGY
In its two meetings and a subsequent conference call, the panel evaluated alternative specifications of the empirically based physician staffing models (EBPSM) that pertained expressly to neurology. As noted in chapter 4 of the study committee's report (Volume I), there are two variants of the EBPSM: the production function (PF) and inverse production function (IPF).
Production Functions
Among the 14 VAMC patient care areas (PCAs) defined for analysis in this study, two were of particular concern to the panel: inpatient neurology and ambulatory neurology. While the derivation of total physician FTEE in neurology at a VAMC via the PF model requires an analysis of internist FTEE in all PCAs, this panel (like the others) restricted its focus to the PCAs where the neurologist is the “dominant ” physician specialty.
The final versions of the inpatient and ambulatory neurology PF models, as developed in conjunction with the study's data and methodology panel, are presented in Table 2.A.
Inverse Production Function
In the early fall of 1990 (following its two meetings), the panel was asked to evaluate an IPF model estimated for physicians in the neurology service. The final version of the neurology IPF is shown in Table 2.B.
EBPSM Assessment
Neither the PF nor IPF variant of the EBPSM is acceptable for determining neurologist requirements at present because the VA data used in their estimation is flawed in at least two significant respects. First, these data (of necessity) reflect current neurologist FTEE-neurologist workload relationships, and these may reflect less-than-adequate care in those VAMCs (and there are many) where neurology is understaffed. Second, in more than half of all VAMCs, there is no neurology service; when this occurs, the existing neurologist FTEE is in fact attributed to the medicine service, leading to biased observations for both the NEU_MD and MED_MD variables.
Between the two variants, the IPF is preferred because NEU_MD did not merit entry into most PF equations, based on the criterion of statistical significance. Hence, adoption of the PF approach would lead to a systematic undercalculation of total neurologist FTEE for patient care and resident education at the VAMC.
These criticisms are discussed further in the final section of this report.
PHYSICIAN STAFFING RESULTS FROM APPLICATION OF EMPIRICALLY BASED AND EXPERT JUDGMENT APPROACHES
In Table 1 are alternative estimates of physician requirements in neurology at VAMCs I, II, and III in FY 1989 as derived from: the VA's cost distribution report (CDR), the PF and IPF variants of the EBPSM, the DSE (from the second panel meeting), the SADI (in both its “ pure” and modified application format), and a mail survey of panel members conducted just prior to Joint Meeting II (held September 7–9, 1990).
The most striking conclusion from Table 1.A. is that these three VA facilities are understaffed in neurology by virtually every approach put forward to estimate physician requirements. With one exception (the Modified SADI approach applied to VAMC II), all empirically based and expert opinion approaches lead to total FTEE estimates for neurologists that exceed the levels recorded in the CDR. (The latter is not likely to undercount actual neurologist FTEE at these facilities, since VAMCs I and II have a neurology cost center, and the study staff ascertained by direct communication with VAMC III that the most appropriate neurologist count there for FY 1989 was, on balance, 1.0 FTEE.)
A second conclusion from Table 1.A. is that both expert judgment approaches lead generally to a higher recommended total FTEE level than either empirically based approach. The panel's overall assessment of appropriate neurologist staffing at the three facilities—as indexed by the median response to the survey conducted prior to Joint Meeting II—was much closer to the estimates derived from the DSE and (pure) SADI approaches.
On the other hand, Table 1.B. indicates there is little systematic difference across these approaches in the recommended neurologist FTEE for direct care and resident education only—at least for these three VAMCs. Hence, the trends noted above for total FTEE would appear to be largely attributable to how the approaches assign FTEE to those activities not reflected in Table 1.B.: research, continuing education, leaves of absence, purchased coverage for nights and weekends, and consultation by non-VA neurologists.
EXTERNAL NORMS
Data on physician staffing in neurology were collected from external (to the VA) health care organizations in order to determine whether productivity performance norms that may exist elsewhere in the public and private sectors could be applied usefully to determine appropriate neurologist staffing in the VA. In addition, the study staff attempted to obtain “internal” VA guidelines on physician staffing in neurology. However, no such guidelines were available.
The Department of Defense (DoD) provided perhaps the most useful specific criteria since it utilizes full-time physician equivalents much like the VA; however the DoD patient population is generally younger and includes a higher percentage of women and children. DoD defines physician performance levels on the basis of the number of outpatient and inpatient visits rendered; the standard varies from 160 to 180 visits per month depending on the availability of teaching staff. Also considered is the number of inpatient days of care provided, where a standard of 95 days of care per month is considered the DoD norm. A different criterion applies if the workload number conflicts with the number of residents, since it is assumed that residents need supervision regardless of workload.
Several panel members obtained productivity information from neurologists working either in private practice or in a private hospital or university medical center. The contribution of neurologists in these settings was rarely measured in terms of FTEE; more typically, these physicians serve as “faculty” or private practitioners whose time spent at a facility and workload production have to be
estimated informally. Most facilities were able to provide annual workload, expressed in admissions, discharges, or outpatient visits.
Summarized in Table 3 are the results from applying the norms derived from DoD and these private-sector providers to calculate the implied levels of neurologist FTEE at VAMCs I, II, and III. The logic behind these calculations is presented and illustrated in the “Overview” to this section of Volume II (see “External Norms”).
The FTEE estimates derived based on staffing standards at university and other teaching hospitals reflect in part the substantial commitment of such institutions to education and research, as well as patient care: the DoD-based estimates, on the other hand, are presumably driven by patient care requirements only.
The panel also investigated data from several other sources that had proven useful in developing staffing norms for internal medicine: The Indian Health Service, the American Medical Association, the New York Health and Hospitals Corporation, and a large health maintenance organization. However, none of these organizations had explicit criteria, or available data, relating neurologist FTEE to patient workload.
In considering the usefulness of the external norms, the panel noted several points:
-
Hospitals employ many different workload measures, e.g., admissions, discharges, annual bed-days of care, or average daily census, but none uses the VA's concept of the weighted work unit (WWU); this complicates comparisons across facilities.
-
Most of these staffing data do not represent “norms” in the sense of being explicit standards consciously developed by the organization; rather these data simply reflect existing staffing patterns as they have evolved at the institution.
-
There is no universal definition of an FTEE.
-
Most hospitals have not systematically analyzed the relationship between physician requirements and some defined unit of workload. Consequently, many of the numbers provided to staff were informally produced and cannot be validated in a written or computerized form.
-
A major problem in comparing neurology staffing patterns is that many hospitals do not have a distinct neurology department; in such cases, neurology is considered to be part of internal medicine.
Furthermore, many patients who should be managed by a neurologist are treated primarily by internists, perhaps with a neurology consult, and thus are considered to be medicine patients.
CONCLUSIONS
The panel endorses the study committee's Reconciliation Strategy (the “disaggregated weighted-average” approach) as a framework for computing physician requirements in neurology. Regarding the FTEE components of this strategy, the panel recommends the following:
Patient Care, Resident Education, and Administration
Neurology FTEE for these activities should be calculated from an expert-judgment-based staffing model, not from an empirically based model that relies on current VA staffing data. Both the SADI and the DSE are acceptable expert judgment models. Because the DSE provides a richer array of details about workload and other facility-specific factors, it is arguably closer to a “gold standard” methodology than the SADI. Yet, for determining VA neurologist FTEE over the long term, the panel favors the SADI. Because it is a generic rather than a facility-specific construct, it will be more economical to apply on a systemwide basis than the DSE. The SADI's task-time estimates can be periodically reevaluated and updated as new data become available. The neurology version of the SADI is ready for its initial systemwide application; this should proceed without delay.
Neither the PF nor the IPF version of the EBPSM is acceptable at present because the VA data used in their estimation is flawed in at least two significant respects.
First, these data (of necessity) reflect current input-output relationships, which are skewed because (in the panel's view) neurology is seriously understaffed in many VAMCs. That is, the current data reflect the status quo, and that is an inadequate basis for drawing policy conclusions about appropriate staffing in neurology.
Second, in more than half of all VAMCs there is no neurology service (though one or more neurologists at such facilities may perform consultations on other services). In these cases, the existing neurology FTEE may be attributed, in all or in part, to the medicine service; when this occurs, both the NEU_MD and the MED_MD variables in the PF and the IPF models will reflect some measurement error, which will lead to biased coefficient estimates in the EBPSM. In addition, the panel has concerns that the outpatient workload
variable used in the present PF and IPF models (NEUCAPWWU) may also suffer from measurement error problems.
Of the two empirically based models, the IPF function is preferred. Even though neurologists consult on many types of VA services, the neurologist FTEE variable is statistically significant in only three of the 14 PCA-specific PF equations (see chapter 4 of Volume I). Thus, deriving neurologist FTEE from these equations will almost certainly underestimate total neurologist requirements for patient care at a given facility. Because the IPF properly acknowledges all recorded neurologist FTEE at a facility, regardless of the degree to which it appears to “produce” workload, this form of underestimation will not arise with the IPF. A second advantage of the IPF is that, because it is estimated at the facility level, it does not require neurologist FTEE allocated across PCAs or between patient care and resident education. Because FTEE allocations to PCAs and among activities are frequently made arbitrarily, it is preferable to avoid models, such as the PF, that require them.
Research
An empirically based, rather than expert-judgment-based, approach should be adopted for determining FTEE allowances for research. The most straightforward reasonable procedure is to assign each neurology service (or consultant service) the amount of research FTEE allocated on the facility's CDR in the previous fiscal year. An alternative approach deserving investigation is to make these FTEE allowances dependent on quantitative measures of research productivity, such as grant funding levels. The greater the demonstrated research productivity of a neurology service, the higher should be its FTEE allocation to research, both in absolute terms and (typically) as a percentage of total FTEE.
Continuing Education
Like the research allocation, physician FTEE for continuing education should be based on what the individual VAMC has deemed to be an appropriate level; the most straightforward indicator of this is the amount of FTEE allocated to continuing education on the facility's CDR in the previous fiscal year.
Leaves of Absence
The percentage of total FTEE earmarked for vacation, sick leave, administrative leave, and other authorized absences should be based on existing VA policies.
Purchased Coverage for Nights and Weekends
Assuming an adequate availability of residents, none is required.
Consulting & Attending and Without-Compensation Coverage
Assuming the VAMC is adequately staffed with VA physicians, there is no need for additional C&A and WOC FTEE.
External Norms
The panel concludes that it is difficult to apply non-VA staffing standards to determine the appropriate number of neurologists for the VA. Across facilities there are substantial differences in what is meant by “patient workload” and “physician FTEE.” In many institutions, neurology is still part of internal medicine. Staffing in private hospitals is frequently driven by concerns about profit margins, which may influence physician staffing intensity; this calls into question whether a desirable norm is being observed. University medical centers generally deliver high-quality care, but serve a patient population quite different that the VA's.
Overall Adequacy of Physician Staffing in the VA
From Table 1 it is evident that actual neurology staffing in FY 1989 at all three VAMCs examined in detail by the panel is below that recommended by any of the proposed approaches to staffing. These results are consistent with the conclusion that neurologist staffing in the VA may not be adequate at present. But because of the small sample size of facilities examined, it is not possible
from these analyses to render a quantitative assessment of neurologist under-staffing for the system.
Other Points
Regardless of whether the VA adopts an empirically based or expert-judgment-based approach (or some combination) to physician staffing, the models should distinguish sharply between VAMCs that have a full neurology service and those that offer only neurology consultation.
If the VA does adopt an empirically based approach, it is crucial that neurologist FTEE allocations in the CDR be made more accurately. As noted, this is especially important for the PF, wherein physician FTEE are allocated by function to various PCAs. In addition, the ambulatory workload variable used in the present models (NEUCAPWWU) must be refined so that it becomes a better direct indicator of the work performed by the neurologist in the clinic setting.
Final Remarks
For neurologist staffing, the panel recommends a variant of the Reconciliation Strategy in which the FTEE required for patient care, resident education, and administration would be determined through the SADI.
TABLE 1 Estimates of Physician Requirements in Neurology at Three VAMCs
|
A. Total FTEE |
|||||||
|
VAMC |
CDR |
PF |
IPF |
DSE |
SADI |
SADI-Modified1 |
Survey2 |
|
VAMC I |
1.6 |
1.7 |
3.4 |
4.8 |
8.2 |
3.6 |
7.5 |
|
VAMC II |
5.5 |
5.8 |
6.3 |
7.1 |
8.6 |
5.2 |
8.3 |
|
VAMC III |
1.03 |
0.0 |
0.9 |
1.5 |
2.0 |
1.3 |
2.0 |
|
B. Direct Care Plus Resident Education FTEE Only |
|||||||
|
VAMC |
CDR |
PF |
IPF |
DSE |
SADI |
SADI-Modified |
Survey |
|
VAMC I |
1.0 |
1.1 |
2.8 |
2.7 |
1.7 |
1.7 |
N.A. |
|
VAMC II |
4.3 |
4.6 |
5.1 |
4.2 |
3.4 |
3.4 |
N.A. |
|
VAMC III |
1.03 |
0.0 |
0.9 |
1.2 |
1.0 |
1.0 |
N.A. |
|
1Derived by replacing the SADI-based estimates for non-patient-care activities with estimates based on the DSE; all FTEE for patient care and resident training in the PCAs continue to be derived from the SADI. 2Panel median response to the question, posed by mail survey in September 1990, of what is the overall preferred physician FTEE level at each VAMC. To provide a context for the response, each panel member was presented a summary of the physician FTEE level emerging, alternatively, from the CDR, from both empirically based approaches (as applicable), and from both expert judgment approaches. 3Because there is no separate CDR cost center for neurology at VAMC III, the CDR submitted by that facility indicates (of necessity) that total neurologist FTEE was 0 in FY 1989. However, personal communication with the facility revealed the presence of approximately 1 FTEE neurologist, dedicated entirely to direct care. In response, the CDR counts above have been adjusted in both cases to reflect this FY 1989 reality. On the other hand, the decision was made to leave the PF-derived FTEE projections at 0, in both cases above, to reflect candidly what the panel feels is an undesirable feature of the way this particular model is used presently to derive physician staffing requirements. That is, if the CDR indicates that, at baseline, NEU_MD is 0 across all PCAs, the “multiplier adjustment” approach presently being used to calculate “projected FTEE” for a given year will always imply that 0 neurologists are required that year—regardless of workload and other factors (see “Using the PF to Compare Projected and Actual Physician FTEE Devoted to Direct Patient Care” in chapter 4, Volume I). These comments underscore the importance of ensuring that CDR data reflect the actual count of physicians, by specialty, at each VAMC. They also illustrate how direct communications with a VAMC can avert errors in interpretation. |
|||||||
TABLE 2 Estimated Production Functions and Inverse Production Function for Neurology
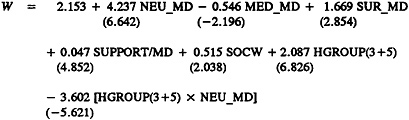
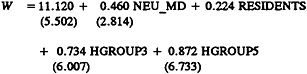
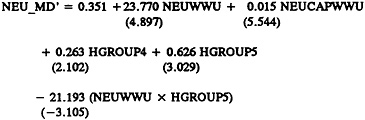
TABLE 3 External Norm Comparison
|
Each of the available external norms was applied to the three VA facilities studied by the expert panel, in order to illustrate the staffing pattern that would occur if the VA used the same staffing guidelines. This table provides the inferred staffing pattern for each VAMC. |
|||
|
VAMC I |
VAMC II |
VAMC III |
|
|
Actual Neurologist Staffing as Inferred from VA Cost Distribution Report |
1.6 |
5.5 |
1.0 |
|
DoD |
3.0 |
4.3 |
0.6 |
|
Private City Hospital (Indiana) |
3.0 |
8.5 |
0.5 |
|
University Hospital (Indiana) |
6.5 |
18.0 |
1.0 |
|
Private Practice |
3.0 |
8.5 |
0.5 |
|
University Hospital (Chicago) |
2.0 |
7.6 |
1.0 |
FIGURE 1 The Staffing Algorithm Development Instrument (SADI) for Neurology: The Complete Instrument with a Statistical Summary of the Panel's Assessments
INTRODUCTION AND INSTRUCTIONS (Abbreviated)
The purpose of the SADI is to gather the data needed to construct, test, formalize, and enhance the algorithms and rules of thumb for staffing that emerged from prior meetings of each specialty and clinical program panel. The ultimate intention is to develop algorithms which could be applied to estimate staffing requirements at VA medical centers (VAMCs), presumably duplicating the results specialty and clinical program panelists themselves would have derived.
Section A of the SADI requests time estimates in some cases by workload unit. In other cases, it requests time estimates by major job elements (tasks). These elements had previously been indicated by some panel members as accounting for the bulk of the work of VA neurologists. For the latter cases we seek your estimates of how physician requirements in your specialty vary with respect to such variables as the volume of patients and the availability of residents and nonphysician practitioners. By systematically varying the levels of workload and personnel, we hope to infer from your numerical responses the implicit formulas you used to relate physician time to these variables as well as the nature of the relationship between workload and staffing, e.g., linear or nonlinear.
Section B seeks responses to a series of questions for the time spent in activities other than direct patient care.
Instructions: In Section A, for each cell of each table, please estimate the number of physician hours required from the Neurology Service to deliver good-quality care under the specified circumstances. Section B is self-explanatory.
SECTION A: PATIENT CARE ACTIVITIES
ADMISSIONS
Please fill in the average time in hours required by a staff physician in your service to accomplish an admission work-up, either with or without the assistance of a resident in your service.
Chart 1
|
Time per Admission Work-Up without Resident |
Time per Admission Work-Up with Resident |
|
|
High |
2.50 |
1.50 |
|
Low |
1.00 |
0.50 |
|
Mean |
2.00 |
1.08 |
|
Median |
2.25 |
1.25 |
ROUTINE DAILY PATIENT CARE
For each workload factor and alternative average daily census (ADC) level below, please fill in the average number of physician hours required from the Neurology Service. Keep in mind that the daily rounds do not include new admission work-ups, since they are covered in Chart 1.
Chart 2
|
Assume No Residents |
|||||||
|
Neurology Ward Average LOS=7 |
ADC 1 |
ADC 5 |
ADC 10 |
ADC 15 |
ADC 20 |
ADC 25 |
|
|
Daily Rounds |
High |
0.50 |
1.50 |
2.00 |
2.50 |
3.00 |
3.50 |
|
Low |
0.08 |
0.50 |
1.00 |
1.50 |
2.00 |
2.50 |
|
|
Mean |
0.33 |
1.33 |
1.80 |
2.17 |
2.75 |
3.17 |
|
|
Median |
0.42 |
1.00 |
1.75 |
2.42 |
2.75 |
3.25 |
|
|
Neurology Ward Average LOS=7 |
ADC 1 |
ADC 5 |
ADC 10 |
ADC 15 |
ADC 20 |
ADC 25 |
|
|
Charting, Phone, and Paperwork |
High |
0.25 |
0.75 |
1.00 |
1.50 |
2.00 |
2.50 |
|
Low |
0.08 |
0.50 |
1.00 |
1.25 |
1.50 |
1.75 |
|
|
Mean |
0.27 |
0.55 |
1.00 |
1.33 |
1.67 |
2.00 |
|
|
Median |
0.25 |
0.50 |
1.00 |
1.25 |
1.50 |
1.87 |
|
|
Patient and Family Contacts plus Teaching |
High |
0.50 |
0.75 |
1.00 |
1.25 |
1.50 |
1.50 |
|
Low |
0.05 |
0.25 |
0.50 |
0.75 |
1.00 |
1.25 |
|
|
Mean |
0.27 |
0.45 |
0.75 |
1.33 |
1.08 |
1.50 |
|
|
Median |
0.27 |
0.42 |
0.73 |
1.00 |
1.08 |
1.38 |
|
|
Supervision and Teaching (Residents/Staff) |
High |
0.50 |
0.50 |
0.75 |
1.00 |
1.00 |
1.25 |
|
Low |
0.00 |
0.00 |
0.00 |
0.00 |
0.00 |
0.00 |
|
|
Mean |
0.12 |
0.28 |
0.38 |
0.55 |
0.57 |
0.67 |
|
|
Median |
0.00 |
0.28 |
0.42 |
0.62 |
0.62 |
0.75 |
|
|
Overall Mean Time |
1.00 |
2.07 |
3.45 |
5.00 |
6.00 |
7.20 |
|
|
Overall Median Time |
0.50 |
2.27 |
4.00 |
5.12 |
6.05 |
7.15 |
|
Chart 3
|
For ADC of 10 or less, assume one PGY 2 or 3 resident. For ADC greater than 15, assume two PGY 2 or 3 residents. |
|||||||
|
Neurology Ward Average LOS=7 |
ADC 1 |
ADC 5 |
ADC 10 |
ADC 15 |
ADC 20 |
ADC 25 |
|
|
Daily Rounds |
High |
0.50 |
1.50 |
2.00 |
2.50 |
3.00 |
3.50 |
|
Low |
0.08 |
0.25 |
0.50 |
0.75 |
1.00 |
1.25 |
|
|
Mean |
0.35 |
0.82 |
1.08 |
1.25 |
1.83 |
2.08 |
|
|
Median |
0.42 |
0.75 |
1.00 |
1.25 |
1.63 |
1.87 |
|
|
Charting, Phone, and Paperwork |
High |
0.50 |
0.75 |
1.00 |
1.25 |
1.67 |
2.00 |
|
Low |
0.08 |
0.25 |
0.50 |
0.50 |
1.00 |
0.75 |
|
|
Mean |
0.20 |
0.38 |
0.75 |
0.92 |
1.23 |
1.42 |
|
|
Median |
0.13 |
0.30 |
0.67 |
1.00 |
1.25 |
1.50 |
|
|
Patient and Family Contacts plus Teaching |
High |
0.50 |
0.75 |
0.75 |
1.50 |
1.00 |
1.25 |
|
Low |
0.08 |
0.08 |
0.25 |
0.33 |
0.42 |
0.50 |
|
|
Mean |
0.27 |
0.33 |
0.45 |
0.58 |
0.72 |
0.87 |
|
|
Median |
0.20 |
0.25 |
0.42 |
0.50 |
0.75 |
0.87 |
|
|
Supervision and Teaching (Residents/Staff) |
High |
0.50 |
0.50 |
1.00 |
1.50 |
2.00 |
2.50 |
|
Low |
0.08 |
0.25 |
0.50 |
1.00 |
1.00 |
1.50 |
|
|
Mean |
0.30 |
0.43 |
0.87 |
1.25 |
1.50 |
1.92 |
|
|
Median |
0.33 |
0.50 |
0.87 |
1.25 |
1.50 |
2.00 |
|
|
Overall Mean Time |
1.08 |
2.00 |
3.00 |
4.08 |
5.25 |
6.38 |
|
|
Overall Median Time |
1.08 |
1.87 |
3.00 |
4.08 |
5.25 |
6.38 |
|
TIME PER INITIAL CONSULTATION OFF YOUR PCA
Fill in the average time in hours required by a staff physician in your service for each initial (new) consult on another service, noting the presence or absence of a resident in your own service. (When the resident is present, assume that he/she is performing the consult under the supervision of an attending physician.)
Chart 4
|
Time per Consult without Resident |
Time per Consult with Resident |
|||||||
|
Consultation off your PCA |
High |
Low |
Mean |
Median |
High |
Low |
Mean |
Median |
|
Medicine |
1.50 |
1.25 |
1.25 |
1.33 |
0.75 |
0.67 |
0.67 |
0.70 |
|
Surgery |
1.50 |
1.00 |
1.17 |
1.25 |
0.75 |
0.50 |
0.62 |
0.62 |
|
Nursing Home |
1.00 |
1.00 |
1.08 |
1.00 |
0.75 |
0.50 |
0.55 |
0.50 |
|
Intermediate Care |
1.00 |
0.83 |
1.00 |
1.92 |
0.75 |
0.42 |
0.53 |
0.50 |
|
Rehab Medicine |
1.00 |
0.83 |
1.00 |
1.92 |
0.75 |
0.42 |
0.53 |
0.50 |
|
Psychiatry |
1.00 |
1.25 |
1.25 |
1.33 |
0.75 |
0.67 |
0.67 |
0.70 |
TIME PER FOLLOW-UP VISIT OFF YOUR PCA
Fill in the average time in hours required by a staff physician in your service for each follow-up consultation visit on another service, noting the presence or absence of a resident from your service.
Chart 5
|
Time per Consult without Resident |
Time per Consult with Resident |
|||||||
|
Consultation off your PA |
High |
Low |
Mean |
Median |
High |
Low |
Mean |
Median |
|
Medicine |
0.33 |
0.25 |
0.28 |
0.28 |
0.42 |
0.17 |
0.25 |
0.22 |
|
Surgery |
0.33 |
0.25 |
0.28 |
0.28 |
0.42 |
0.17 |
0.25 |
0.22 |
|
Nursing Home |
0.33 |
0.17 |
0.28 |
0.28 |
0.42 |
0.08 |
0.23 |
0.22 |
|
Intermediate Care |
0.33 |
0.17 |
0.27 |
0.28 |
0.42 |
0.08 |
0.23 |
0.22 |
|
Rehab Medicine |
0.33 |
0.17 |
0.27 |
0.28 |
0.42 |
0.08 |
0.23 |
0.22 |
|
Psychiatry |
0.33 |
0.25 |
0.28 |
0.28 |
0.42 |
0.17 |
0.25 |
0.22 |
SPECIAL PROCEDURES
Please fill in the average time in hours required by a staff physician in your service for each of the special procedures listed on the left, noting the presence or absence of a resident.
Chart 6
|
Time per Test without Resident |
Time per Test with Resident |
|||||||
|
Special Procedures |
High |
Low |
Mean |
Median |
High |
Low |
Mean |
Median |
|
EEG |
0.83 |
0.33 |
0.47 |
0.42 |
1.00 |
0.25 |
0.52 |
0.42 |
|
Evoked Potential |
1.00 |
0.42 |
0.63 |
0.62 |
0.75 |
0.33 |
0.52 |
0.50 |
|
EMG |
2.00 |
1.00 |
1.37 |
1.50 |
2.00 |
0.50 |
1.50 |
1.75 |
|
Others (Specify) |
1.00 |
1.00 |
||||||
SECTION B: NON-PATIENT-CARE TIME
Part 1. The activities listed below generally do not occur every day, but may be time-consuming when looked at over a longer period, such as a week or month. List the time in hours that you would add to each physician's average workday to allow for the types of non-patient-care work listed below:
Chart 7
|
Assume the amount of research accomplished at this VAMC is: |
High1 |
Medium1 |
Low1 |
|
|
Education of Residents (didactic, classroom, not on the PCA) |
High |
1.00 |
1.67 |
1.00 |
|
Low |
1.00 |
1.00 |
0.50 |
|
|
Mean |
1.33 |
1.17 |
0.67 |
|
|
Median |
1.25 |
1.00 |
0.05 |
|
|
Administration by Chief (time required to manage your whole service by a Chief and/or Assistant Chief) |
High |
1.00 |
2.00 |
2.00 |
|
Low |
1.50 |
1.00 |
0.50 |
|
|
Mean |
1.75 |
1.50 |
0.67 |
|
|
Median |
1.75 |
1.50 |
0.50 |
|
|
Administration by Others (time required for individual physicians) |
High |
1.00 |
1.00 |
0.50 |
|
Low |
0.50 |
0.42 |
0.27 |
|
|
Mean |
0.67 |
0.60 |
0.50 |
|
|
Median |
0.58 |
0.50 |
0.37 |
|
|
Hospital-Related Activities (Mortality and Morbidity, quality assurance, staff meetings) |
High |
1.42 |
1.00 |
0.75 |
|
Low |
0.75 |
0.50 |
0.25 |
|
|
Mean |
0.87 |
0.68 |
0.53 |
|
|
Median |
0.87 |
0.63 |
0.58 |
|
|
1Examples of research level by total amount of funding (VA plus non-VA) in FY 1988. High: e.g.; VAMC I with $8.8 million in total funding; Medium: e.g.; VAMC II with $2.75 million in total funding; Low: e.g.; VAMC III with about $176,000 in total funding. |
||||
|
Assume the amount of research accomplished at this VAMC is: |
|||
|
Total Hours per Average Weekday: |
Overall Mean |
Overall Median |
|
|
For Chief2 |
High |
1.75 |
1.75 |
|
Medium |
1.50 |
1.50 |
|
|
Low |
1.25 |
1.33 |
|
|
For Non-Chief Physician |
High |
3.17 |
3.12 |
|
Medium |
2.42 |
2.42 |
|
|
Low |
1.67 |
1.78 |
|
|
1Examples of research level by total amount of funding (VA plus non-VA) in FY 1988. High: e.g.; VAMC I with $8.8 million in total funding; Medium: e.g.; VAMC II with $2.75 million in total funding; Low: e.g.; VAMC III with about $176,000 in total funding. 2Assume that Chief does not participate significantly in the Education of Residents and Hospital-Related Activities; SADI users may easily modify this assumption. |
|||
Part 2. In order to determine the actual staffing in this hospital, the number of FTEE must be adjusted to allow for CME, research, and any off-time required. What do you believe to be the appropriate percentage of time the “average” (typical) member of your service should devote to each of the following categories of non-patient-care-related activities?
Chart 8
|
Assume the amount of research accomplished at this VAMC is: |
High1 |
Medium1 |
Low1 |
|
|
Continuing Education |
High |
10.0 |
10.0 |
10.0 |
|
Low |
5.0 |
5.0 |
2.0 |
|
|
Mean |
9.5 |
7.5 |
6.0 |
|
|
Median |
8.0 |
8.0 |
7.0 |
|
|
Research (off the PCA) |
High |
60.0 |
40.0 |
10.0 |
|
Low |
25.0 |
20.0 |
5.0 |
|
|
Mean |
40.0 |
26.0 |
7.0 |
|
|
Median |
33.0 |
23.0 |
10.0 |
|
|
Vacation, Administrative Leave, Sick Leave, Other |
High |
25.0 |
23.0 |
20.0 |
|
Low |
8.0 |
8.0 |
8.0 |
|
|
Mean |
13.0 |
13.0 |
12.0 |
|
|
Median |
10.0 |
10.0 |
10.0 |
|
|
Total Percentage of Time |
||||
|
Overall Mean |
60.0 |
46.0 |
26.0 |
|
|
Overall Median |
62.0 |
46.0 |
23.0 |
|
|
1Examples of research level by total amount of funding (VA plus non-VA) in FY 1988. High: e.g.; VAMC I with $8.8 million in total funding; Medium: e.g.; VAMC II with $2.75 million in total funding; Low: e.g.; VAMC III with about $176,000 in total funding. |
||||
INSTITUTE OF MEDICINE
Committee to Develop Methods Useful to the Department of Veterans Affairs in Estimating Its Physician Requirements
Neurology Panel Roster
ROBERT J.JOYNT (Chair),*† Vice President and Vice Provost for Health Affairs, University of Rochester, Rochester, New York
|
†Member of the study committee. |
BENJAMIN R.BROOKS, Chief, Neurology Service, Madison VA Medical Center, Madison, Wisconsin
MARK DYKEN, Professor and Chairman, Department of Neurology, Indiana University Medical Center, Indianapolis
JOSEPH GREEN, Chairman, Department of Medical/Surgical Neurology, Texas Tech University, Lubbock
JOHN F.KURTZKE, Professor and Vice Chairman, Department of Neurology, Georgetown University Medical Center, Washington, D.C.
Nancy Kader, Staff Officer
|
*Member of the Institute of Medicine. |






























