
OTHER PHYSICIAN SPECIALTIES PANEL REPORT1
INTRODUCTION
The other physician specialties panel, organized in late 1989 to assist the IOM study committee in developing a VA physician staffing methodology, was charged with examining physician requirements for laboratory medicine, nuclear medicine, diagnostic radiology, and radiation oncology. The panel was composed of seven physicians—two specializing in laboratory medicine, three in nuclear medicine, one in diagnostic radiology, and one in radiation oncology. It met twice during 1990, and participated in other efforts to advise the study committee on appropriate staffing for these four physician specialties. The chairman of the panel was also a member of the study committee. The panel roster is attached.
This report will describe the panel's analyses, conducted in the framework of the “panel process” described in the “Overview” to this section of Volume II. Reported here are the results of these analyses, along with the panel's commentary and conclusions.
|
1 |
The initial draft of this report was prepared by Bobbie J.Alexander, Staff Associate to the Other Physician Specialties Panel during the conduct of the study. This final report was prepared by the editors of this volume. |
EXPERT JUDGMENT APPROACHES TO DETERMINING PHYSICIAN REQUIREMENTS IN THE OTHER PHYSICIAN SPECIALTIES
The Detailed Staffing Exercise (DSE) Approach
Initial Efforts
The first meeting of the other physician specialties panel was convened in April of 1990. The primary purpose was to determine whether the expert judgment panel process, as the study committee first conceived it, represented a viable means for determining physician staffing for these four physician specialties at individual VAMCs. This process required the development of staffing instruments that provide the panel with information about workload, about various nonphysician personnel that might be available to deliver care, and then, given that conditional information, to make judgments about what physician FTEE are appropriate to meet that workload, consistent with good-quality care. In preparation for the first panel meetings, staffing instruments were constructed for three actual VAMCs.
Focusing on the analysis of these instruments, study staff tested the feasibility of this process at the first meeting and found that it was generally acceptable, that panel members could render physician staffing judgments, but that they wished to have more detailed information about workload and other factors. The panel concluded that study staff should proceed with the expert judgment process, but that the staffing instruments should be modified in several specific ways:
-
subdivide workload into more homogeneous and exhaustive categories, distinguishing in greater detail the types of tests;
-
define workload in standardized terms whenever possible;
-
provide more descriptive detail about workload levels (e.g., number of patient admissions, number of patients, case mix, number of outpatient visits, as well as nursing and domiciliary patients);
-
specify relative incidence of new versus old patients;
-
for laboratory medicine, unweighted tests should be better defined (by noting the number in hematology, chemistry, microbiology, etc.) and the workload levels should reflect total tests performed in the facility, including not only the main but all satellite laboratories.
-
specify number and level of residents relative to each workload level. [In three of the four specialties, panel members felt that the time devoted to teaching and supervising residents was roughly counterbalanced by the residents' positive contribution to productivity, so that the net impact of residents on productivity was about zero. In laboratory medicine, the panel noted that residents require extensive supervision, so that the net impact of residents on productivity may be negative (all else equal).];
-
acknowledge more clearly the potential role of residents and fellows in working with staff physicians to provide “hands on” patient care in nuclear medicine;
-
provide greater specificity regarding the adequacy of nonphysician staffing, focusing on nurses, technicians (e.g., occupational pathologist assistant, cytology technician, etc.), and other support staff;
-
as background for determining FTEE, provide current distribution of VA and non-VA research dollars and FTEE by RAM group;
-
develop “external” staffing norms from standards published by professional societies and other health care organizations;
-
provide background information about the physical layout of the VA medical center and its patient care areas, including data on the sophistication and quality of equipment.
At the conclusion of the first round of all eight specialty and clinical program panel meetings, there was convened a major meeting (Joint Meeting I) involving the study committee (which includes all eight panel chairmen), the data and methodology panel, and the VA liaison committee. At this meeting, participants reviewed and evaluated the key concepts and assumptions underlying both the empirically based and expert judgment approaches to determining VA physician requirements.
The study staff emerged from Joint Meeting I with a set of recommendations from the committee on how to proceed with the panel process. Staff began to implement these recommendations on a panel-specific basis.
DSE: Overall Rationale
The next stage in the development of the expert judgment staffing methodology centered on the preparation for, and conduct of, the second panel meeting, held in August of 1990. Again, three actual VAMCs were selected for intensive analysis—in essence, to serve as “laboratories” for methodology
development. They were chosen to represent a range of geographic locations, sizes, staffing intensities, available services/programs, and affiliation status.
A revised staffing instrument, later termed the Detailed Staffing Exercise (DSE), was developed in response to the panel's recommendations. It provided a more specific description of the VAMC, including the types of patients, number of admissions, length of stay, and DRG mix of patients in each PCA. The intent is to describe the VAMC “in context” and in sufficient detail that the respondent can assess physician staffing requirements almost as if he/she were reviewing data at the facility.
Panel members were asked to complete DSE's for two of the VAMCs prior to the meeting. These results were tabulated and distributed at the meeting, along with data showing the actual staffing at these facilities. After review and discussion, panel members were given the opportunity to reevaluate staffing estimates. Then the panel, as a group, worked through an additional DSE constructed for VAMC III, a third facility; the members subsequently reflected on these results in light of the actual staffing for these four specialties at VAMC III.
DSE Instructions and Assumptions
To illustrate how the DSE works, a completed version of the instrument is presented as Exhibit 1 in the “Overview” to this section of Volume II.
This DSE is nearly identical structurally to those constructed for the four physician specialties analyzed by this panel.
In Section A of each DSE, the basic question is the same for each patient care area: In hours, how much time must be contributed by physicians in the relevant specialty (laboratory medicine, nuclear medicine, diagnostic radiology, or radiation oncology, as the case may be) to meet a specified workload level during an average weekday, under certain assumptions about patient mix and the availability of residents and support staff. These hours are then converted to FTEE, under the assumption that 40 hours per week translates into one FTEE.
In Section B of each DSE, panel members are asked to estimate the number of hours required for night call, weekend coverage, and non-patient-care-related activities: research off the patient care areas, educational activities not related to direct patient care, quality assurance, mortality and morbidity meetings or studies, administrative activities, and all other functions not directly related to patient care. These estimated hours are converted into FTEE, which are then added to those derived from Section A to yield total staff physician
requirements in that particular specialty. Also assessed in the DSE are the number of consulting and attending (C&A) and without-compensation (WOC) physicians desired from the community or neighboring medical school, given the completed assessment of VA staff physician requirements.
In general, the second meeting focused on the assumptions, thought processes, and algorithms underlying the panel's staffing estimates. From these discussions, the panel worked toward a consensus about the appropriate data, assumptions, and methodology required for expert judgment assessments of physician requirements. Strategies were discussed for reconciling the three major alternative approaches to deriving physician requirements: expert judgment, statistical modeling, and external (to the VA) staffing norms.
The Staffing Algorithm Development Instrument (SADI) Approach
SADI: Overall Rationale
At the conclusion of the second panel meeting, the committee implemented a sequence of postmeeting activities designed to promote the development of consensus positions regarding the appropriate methodology and accompanying data for determining VA physician requirements.
These postmeeting activities were formally initiated with the development of the Staffing Algorithm Development Instrument (SADI). The purpose of this new instrument was to test, build upon, and ultimately strengthen the algorithms and rules of thumb for staffing that emerged from the meetings of all eight specialty and clinical program panels. The instrument was designed on the premise that experts could be asked a set of generic staffing questions whose answers could then be applied to selected data from individual VAMCs to derive appropriate staffing levels for these facilities.
Instructions and Assumptions
Like the DSE, the SADI has two Sections, A and B, which focus on patient care and non-patient-care activities, respectively. Also like the DSE, the SADI is specialty specific. In Section A, the respondent is asked to estimate the amount of physician time in the designated specialty (e.g., nuclear medicine) required to complete a number of patient care functions and tasks under varying
assumptions about the availability of residents and nonphysician practitioners. These tasks include not only the performance of laboratory procedures and “hands on” patient care, but also incorporate the following activities, as appropriate: conferring with referring physicians, conferring with support services, charting, phone, paperwork, counseling patients and family, teaching and supervising residents, and rounds.
In Section B, the respondent must determine the total amount of physician time in that specialty that should be allocated to research, classroom instruction, continuing education, administration, and leaves of absence. To derive physician requirements in that specialty for a given VAMC, the estimated physician hours for patient care and non-patient-care activities are summed, then converted to FTEE under the 40 hours-per-week equivalency assumption.
Presented in Figure 1 of this report is a composite representation of the SADIs developed for the four specialties, complete with the panel members' median estimates for physician task times. Where multiple members estimated task time (i.e., for nuclear medicine), the high, low, median, and mean are reported; where only one panel member estimated times (e.g., for radiation oncology), those numbers are simply reported.
A detailed, self-contained illustration of how the SADI can be applied to determine the number of physicians required at a given VAMC is found in Exhibit 3 of the “Overview” to this section of Volume II. That example happens to focus on total internist requirements at VAMC I; for any of this panel's four specialties, the application of its SADI to determine physician FTEE at a given facility proceeds just as in the internist example. A careful study of that example reveals the type of facility-specific data needed to implement any SADI.
EMPIRICALLY BASED APPROACHES TO DETERMINING PHYSICIAN STAFFING FOR THE OTHER PHYSICIAN SPECIALTIES
In the course of the study, the committee proposed two alternative variants of the EBPSM, the production function (PF) and the inverse production function (IPF).
Under the PF approach, an input-output model (i.e., a “production function”) is estimated statistically for each of 14 patient care areas defined for the VAMC. The physician FTEE required for direct patient care in a given specialty or clinical program area at a given VAMC can be derived as the sum
of the FTEE required to meet the projected workload in each PCA (controlling for other factors). In principle, the PF approach is conceptually attractive in that physician requirements for a given specialty or program can be calculated as a function of the assumed availability of other labor inputs (e.g., support personnel) and nonlabor inputs (e.g., the quantity and vintage of equipment). In both of its meetings, the OPS panel examined alternative specifications of production function models; it became clear that the conceptual advantages of the PF approach were more than offset by several other factors:
-
The VA data used to estimate these models—particularly that relating to the allocation of physician FTEE across activities in the Cost Distribution Report (CDR) —were of questionable reliability;
-
Because data on nonlabor inputs were seriously lacking, the PF models focused largely on the relationship between labor inputs and workload production; and (most crucially)
-
The committee determined (and this panel is inclined to agree) that none of the four specialties under examination here is associated with a single dominant PCA; rather, physicians in these specialties tend to work in, and render services on behalf of, a number of PCAs. Hence, PCA-associated production functions cannot be estimated for these four specialties the way they can, say, for the medicine service (whose physicians are clearly the dominant specialty in the inpatient medicine and ambulatory medicine PCAs).
Following its two meetings, the OPS panel was asked to evaluate an alternative variant of the empirically based models, the inverse production function. Under the IPF approach, the physician FTEE in a given specialty required for direct patient care and resident education at a VAMC is modeled as a function of the inpatient, outpatient, and long-term care workload there, plus possibly other factors. Thus, IPFs can be estimated expressly for laboratory medicine, diagnostic radiology, nuclear medicine, and radiation oncology.
The final versions of these four IPFs, as derived by the study committee in consultation with both this panel and the data and methodology panel, are presented in Table 1. The statistical goodness of fit for the laboratory medicine and diagnostic radiology IPFs is considerably stronger than for the other two. However, an overriding concern about all such models relates, again, to the quality of the CDR data going into them. The panel regards this quality as variable at best across all physician specialties, and specifically suspect for the hospital-based specialties that are the focus here.
PHYSICIAN STAFFING RESULTS FROM THE APPLICATION OF EMPIRICALLY BASED AND EXPERT JUDGMENT MODELS
Summarized in Table 2 are alternative estimates of the physician FTEE required in the four specialties at VAMCs I, II, and III (three actual VA facilities) in FY 1989 as derived from: the VA's cost distribution report (CDR), the IPF variant of the EBPSM, the DSE (as analyzed at the second panel meeting), the SADI (both in its original and modified forms), and a mail survey of panel members just prior to Joint Meeting II (held September 7–9, 1990).
The principal purpose of analyzing physician requirements at these sites was model development—specifically, to test the feasibility and appropriateness of alternative staffing methodologies. It would be premature to conclude from these analyses, focusing on only three facilities, whether the VA as a whole is over- or understaffed in laboratory medicine, nuclear medicine, diagnostic radiology, or radiation oncology. In the latter three specialties, however, it is noteworthy that both of the expert judgment approaches tended to yield FTEE estimates that exceed those emerging from both the IPF and the CDR tally of actual staffing levels.
EXTERNAL (NON-VA) PHYSICIAN STAFFING NORMS
Data on physician staffing for the panel's four specialties were collected by study staff from several health care organizations external to the VA in order to determine whether there are staffing methodologies or productivity performance norms in the public or private sectors that could be usefully applied to calculate VA physician requirements. The complete list of organizations contacted is found in the “Overview” to this section of Volume II.
Each of the available external norms was applied experimentally to VAMCs I, II, and III in order to illustrate the staffing pattern which would emerge at the facility if the VA used the staffing guidelines implied by the external norm. In general, the number of physicians for a particular specialty was computed by dividing the actual workload at the VAMC by the workload standard for that specialty. In particular, for
Nuclear Medicine—Two separate, alternative FTEE estimates were computed by 1) dividing the actual number of imaging procedures at each VAMC by the workload standard of approximately 2000 imaging procedures per year per FTEE, and 2) dividing the operating bed level at each VAMC by the GMENAC-estimated optimal number of hospital beds per nuclear medicine physician.
The application of external norms to calculate physician requirements for the other three specialties proceeded similarly:
Laboratory—The required FTEE were based on an optimal bed size range for a given number of physicians, e.g., 6.0 FTEE for a hospital with more than 500 beds.
Diagnostic Radiology—Three alternative FTEE calculations emerge, from three alternative productivity standards: approximately 10,500 procedures per radiologist per year, or 11,240 per year, or 16,266 per year.
Radiation Oncology—The required FTEE were based on a productivity standard of approximately 225 patients per year.
Table 3 summarizes the physician workload standards and indicates the inferred staffing pattern for each VAMC for these four physician specialties.
In general, the panel found that comparing current VA staffing with that suggested by the application of such external norms was difficult because of differences in how workload and FTEE are measured, and also differences in the type of patient populations being served.
CONCLUSIONS
As a framework for determining physician requirements in the specialties of laboratory medicine, diagnostic radiology, nuclear medicine, and radiation oncology, the panel endorses the “disaggregated weighted-average ” approach to the Reconciliation Strategy (see Equation 6.1 of Volume I). Regarding the components of the strategy, the panel recommends the following:
Patient Care, Resident Education, and Administration
For these activities, FTEE should be derived from expert judgment methodologies. Although both the Staffing Algorithm Development Instrument (SADI) and the Detailed Staffing Exercise (DSE) are acceptable expert judgment approaches, the SADI is preferred. The focus of the SADI is on the time required by physicians to perform specific tasks and functions, making it suitable both for technologically based specialties, like laboratory medicine, and specialties that also have a strong component of physician-patient interaction, like nuclear medicine. The panel has made a first-cut effort to estimate these SADI task times.
On the basis of these results, the panel concludes that the SADI should be applied experimentally at a representative sample of VA medical centers to derive first-cut estimates of physician requirements in the four specialties. It would be possible to apply the DSE within the same representative sample, but the administrative burden would be considerably greater; in the judgment of the panel, that entire process would be inefficient since distinct DSE instruments would have to be developed for each VAMC.
Neither of the two empirically based approaches is acceptable at present. The production function (PF) variant could not be estimated for any of the four specialties; the PF is specific to PCAs, and there is no single “dominant” PCA defined in the overall methodology for any of the four specialties. The inverse production function (IPF) can be satisfactorily estimated for each of the specialties. But the IPF (like the PF) relies heavily on staffing data from the VA's cost distribution report (CDR), whose reliability the panel regards as variable at best, and specifically unreliable in these hospital-based specialties.2
Though the panel did not feel the need to adopt such an approach, it does see the merits of a version of the Reconciliation Strategy in which FTEE requirements are computed as a weighted average of expert judgment and statistical modeling results—especially for establishing reasonable initial increments, or decrements, in physician staffing relative to the status quo.
|
2 |
From a larger methodological perspective, the panel does find merit in the PF approach because, in principle, it permits physician requirements to be calculated as a function of both other labor inputs (e.g., support personnel) and nonlabor inputs (e.g., the quantity and vintage of equipment). The IPF models presented to the panel do not permit this. |
Research
An empirically based, rather than expert-judgment-based, approach should be adopted for determining FTEE allowances for research. The most straightforward reasonable procedure is to assign each specialty that amount of research FTEE allocated on the facility's CDR in the previous fiscal year. An alternative, and preferable, approach is to make these FTEE allocations dependent on quantitative measures of research productivity, such as grant funding levels and research publications.
Continuing Education
All VA physicians should be expected to receive some minimum amount of continuing education annually as an important part of an overall quality assurance program. This minimum FTEE commitment to continuing education should not vary by specialty or facility. The VA could base these FTEE allocations on standards established by the specialty boards for recertification, by the states for maintaining licensure, or by the American Medical Association for its Physician Recognition Award for Continuing Medical Education.
Leaves of Absence
The percentage of total FTEE earmarked for vacation, sick leave, administrative leave, and other authorized absences should be set globally, perhaps equated to an overall average computed across the VA system.
Purchased Coverage for Nights and Weekends
Assuming an adequate availability of residents, none is required. The panel notes, however, that this is a significant assumption and may not hold for all VAMCs, especially the smaller facilities.
Consulting & Attending and Without-Compensation Coverage
Assuming the VA is adequately staffed with VA physicians, there is no need for additional C&A and WOC FTEE to handle the present workload. However, these non-VA physicians can serve to enhance both the quality of patient care and educational opportunities for VA staff physicians and residents.
External Norms
In a strictly mechanical sense, non-VA staffing standards were successfully applied to determine the implied appropriate staffing at VAMCs I, II, and III for each of the four specialties. The overall result is that, although a given VAMC was sometimes understaffed according to a particular criterion, there was no significant pattern of understaffing or overstaffing.
But the validity of these comparisons is threatened by some fundamental problems. For each of the four specialties, there are national guidelines relating workload to physician staffing, but it is not clear whether these make proper allowance for all of the patient care and non-patient-care duties expected of the VA staff physician. With external norms derived from staffing behavior observed at non-VA facilities, there are several difficulties. The definition of workload for the four specialties varies across non-VA facilities. There is no universal definition of an FTEE, and virtually no other institution attempts to define it with the precision of the VA. Similarly, few private-sector facilities have data systems that keep track of the allocation of physician FTEE to specific types of activities. Since few hospitals routinely study the relationship between workload and physician FTEE, the non-VA staffing ratios that do emerge are often roughly estimated on an ad hoc basis.
Overall Adequacy of Physician Staffing in the VA
There was a general consensus among panel members that, for the three VAMCs studied in depth, there was a degree of understaffing (in FY 1989) in diagnostic radiology, nuclear medicine, and radiation oncology; laboratory medicine appeared neither significantly overstaffed nor understaffed in these facilities. However, the panel is unwilling at present to extend these conclusions to the VA system as whole. A sample of three is too small for valid inferences.
If the SADI were applied across the system, the question of overall staffing adequacy could be directly confronted. But a large caveat would remain, at least in the short term, because still lacking is quantitative information linking physician staffing intensity in these specialties to indicators of the quality of care. Evidence of such a linkage can be investigated only gradually over time, as quality of care indices are developed and their relationship to physician staffing levels investigated.
Other Points
Panel members differed on whether it is better to report physician staffing recommendations in the form of a range of alternative values or as a single point estimate. Some argued in favor of point estimates because budget pressures will inevitably lead the VA decision maker to the low end of whatever range is presented. Others pointed out that, first, a range allows one to reflect the genuine uncertainty that exists about “the” appropriate staffing level and, second, the VA decision maker may not invariably choose the lowest point on the range.
The panel was impressed by the ongoing work in the VA's pathology service to develop a methodology to account for how laboratory medicine physicians allocate their time that is more detailed than what is currently available from the CDR, the DSE, or the SADI. As the VA proceeds to refine the laboratory medicine SADI, it should investigate the development of time estimates at the level of task specificity found in the pathology service survey instruments.
Final Remarks
For determining physician requirements in laboratory medicine, diagnostic radiology, nuclear medicine, and radiation oncology, the panel endorses the variant of the Reconciliation Strategy described above.
The panel's estimates of physician requirements for three actual VAMCs, based on applications of the empirically based and expert judgment approaches discussed above, are summarized in Table 2.
TABLE 1 Estimated Inverse Production Functions for the Other Physician Specialties
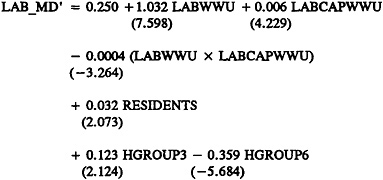
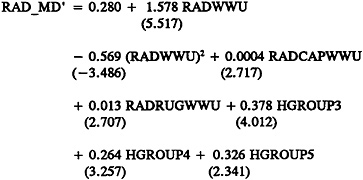
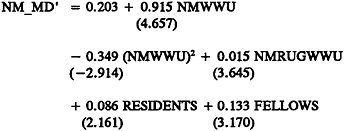
TABLE 2 Estimates of Physician Requirements in Other Physician Specialties at Three VAMCs
|
Source of FTEE Estimate |
VAMC I |
VAMC II |
VAMC III |
|
LABORATORY MEDICINE |
|||
|
CDR |
3.4 |
9.2 |
2.0 |
|
IPF |
5.9 |
9.8 |
3.5 |
|
DSE |
3.7 |
5.8 |
1.8 |
|
SADI |
2.9 |
5.2 |
1.8 |
|
SADI-Modified1 |
1.6 |
3.1 |
1.5 |
|
Survey2 |
3.9 |
8.0 |
2.0 |
|
NUCLEAR MEDICINE |
|||
|
CDR |
2.0 |
2.0 |
0.0 |
|
IPF |
2.2 |
2.0 |
0.6 |
|
DSE |
4.4 |
3.5 |
0.9 |
|
SADI |
6.7 |
3.1 |
1.8 |
|
SADI-Modified1 |
5.1 |
2.9 |
1.3 |
|
Survey2 |
5.0 |
3.5 |
1.5 |
|
1Derived by replacing the SADI-based estimates for non-patient-care activities with estimates based on the DSE; all FTEE for patient care and resident training in the PCAs continue to be derived from the SADI. 2Panel median response to the question, posed by mail survey in September 1990, of what is the overall preferred physician FTEE level at each VAMC. To provide a context for the response, each panel member was presented a summary of the physician FTEE level emerging, alternatively, from the CDR, from the IPF, and from both expert judgment approaches. |
|||
|
Source of FTEE Estimate |
VAMC I |
VAMC II |
VAMC III |
|
DIAGNOSTIC RADIOLOGY |
|||
|
CDR |
7.0 |
13.9 |
4.6 |
|
IPF |
8.5 |
10.4 |
11.3 |
|
DSE |
9.6 |
21.0 |
6.2 |
|
SADI |
12.3 |
25.0 |
7.7 |
|
SADI-Modified1 |
7.8 |
18.6 |
5.2 |
|
Survey2 |
7.8 |
18.6 |
5.2 |
|
RADIATION ONCOLOGY |
|||
|
CDR |
0.0 |
1.9 |
0.0 |
|
IPF |
1.5 |
3.5 |
1.4 |
|
DSE |
2.1 |
4.3 |
0.1 |
|
SADI |
2.2 |
3.1 |
0.4 |
|
SADI-Modified1 |
1.9 |
3.0 |
0.1 |
|
Survey2 |
2.0 |
4.0 |
0.2 |
|
1Derived by replacing the SADI-based estimates for non-patient-care activities with estimates based on the DSE; all FTEE for patient care and resident training in the PCAs continue to be derived from the SADI. 2Panel median response to the question, posed by mail survey in September 1990, of what is the overall preferred physician FTEE level at each VAMC. To provide a context for the response, each panel member was presented a summary of the physician FTEE level emerging, alternatively, from the CDR, from the IPF, and from both expert judgment approaches. |
|||
TABLE 3 Application of External Norms to Compute Other Physician Specialties Physician Requirements
|
Computed FTEE Requirements at: |
||||
|
Specialty/Source |
Workload/ FTEE |
VAMC I |
VAMC II |
VAMC III |
|
Nuclear Medicine |
||||
|
American College of Nuclear Physicians |
2000 procs |
1–2.01 |
1–2.01 |
1.0 |
|
GMENAC Delphi Survey |
177.5 beds |
2.1 |
5.5 |
6.1 |
|
Diagnostic Radiology |
||||
|
American College of Radiologists |
10,500 procs |
4.1 |
9.8 |
3.9 |
|
GMENAC Delphi Panel |
11,240 procs |
3.9 |
9.3 |
3.7 |
|
American Healthcare Radiology Administration |
16,266 procs |
2.7 |
6.4 |
2.6 |
|
Radiation Oncology |
||||
|
Inter-Society Council for Radiation Oncology |
226 patients |
02 |
4.3 |
0.02 |
|
Laboratory |
||||
|
GMENAC Delphi Panel |
Based on bed size ranges |
5.25 |
6 |
6 |
|
1Plus 1 optional FTEE for ultrasound and CT. 2Contracted out. However, for VAMC I and III, respectively, 1.5 and 0.1 FTEE would be required. |
||||
APPENDIX
A number of months before this IOM study began, the VA's Pathology Service at Central Office initiated its own inquiry into whether the “duties of a pathologist” —and the time required to perform each of them—could be determined in a detailed and comprehensive fashion. The survey instrument for eliciting both the per unit time and/or the total amount of time per week that the VA pathologist devotes to each duty is reproduced in its entirety in Figure A.1. Also shown there, for illustration, are the average performance times reported by one (representative) full-time anatomic pathologist in FY 1990.
Because this instrument focuses on the actual number of hours devoted to these duties, the time estimates that emerge—and the corresponding FTEE estimates that are implied—can be viewed functionally as (much more detailed) alternatives to the pathologist time allocation estimates reported in the VA' s Cost Distribution Report. As such, the time (and FTEE) estimates that are derivable from the survey, in its present form, differ in one crucial respect from those obtainable from either the DSE or SADI. The latter two are intended to reflect the expert's judgment about the amount of pathologist time that should be devoted to each duty, consistent with good patient care, while the survey examines the time actually devoted to each duty.
However, it would be relatively straightforward to modify the instrument in Figure A.1 so that experts could assess the pathologist time desired for each activity, consistent at once with both the DSE and SADI. Specifically, one would retain the level of task detail found in the current instrument, but include additional information required for evaluating physician requirements. As suggested in the construction of the DSE and SADI, the expert would need data on both the type of VAMC being staffed (e.g., degree of affiliation) and the “context of the production process” —that is, for each pathologist activity, the workload to be produced per period, and the availability of residents and relevant technical and support staff.
In such an augmented survey instrument, physician time estimates structurally similar to those derived from the DSE could be obtained directly from the column now labeled “Total Hours/Week.” Moreover, the per-unit time estimates emerging under the columns now labeled “Average Min[utes]/Compl[icated] Case” and “Average Min/Uncompl[icated] Case” could be used to develop a new, more detailed SADI for laboratory medicine.
Whether such fine-tuning would lead to physician FTEE estimates that are significantly different from—and superior to—those derivable from the present laboratory medicine SADI is strictly an empirical question. It is a question well worth examining if the VA elects to use expert judgment models as one basis for determining physician staffing requirements in laboratory medicine.
DEPARTMENT OF VETERANS AFFAIRS PATHOLOGY AND LABORATORY MEDICINE
A SYSTEMATIC APPROACH TO ASSESSING THE DUTIES OF A PATHOLOGIST
|
VAMC___________ YOUR NAME (Optional)________ |
|
|
Directions: |
Check the items that apply to your VA practice: |
|
SPECIALTY |
AP X CP__ NP__ EM__ |
|
POSITION |
Chief, Laboratory Service__Chief AP__Chief CP__ Chief, Other (enter specialty)_____ Staff Pathologist FT X Staff Pathologist PT (enter hrs/wk)__ Contract Pathologist (enter hrs/wk)__ |
|
Directions: |
Enter the requested data in the blanks that apply to your VA practice: |
|
I. |
Diagnosis and Interpretation |
Average Min/Compl Case |
Average Min/Uncompl Case |
Total Hours/ Week* |
Number of Residents Assisting by Performing Gross/ Screening |
|
AP |
Surgical Pathology |
||||
|
Routine |
45.0 |
20.0 |
18.0 |
25.0 |
|
|
Special |
60.0 |
30.0 |
2.0 |
0.0 |
|
|
DNA Probes |
0.0 |
0.0 |
0.0 |
0.0 |
|
|
AP |
Cytology |
40.0 |
10.0 |
8.0 |
0.5 |
|
Cytology Screening |
30.0 |
0.0 |
0.0 |
0.0 |
|
|
AP |
Hematopathology |
0.0 |
0.0 |
0.0 |
0.0 |
|
AP |
Immunopathology |
0.0 |
0.0 |
0.0 |
0.0 |
|
AP |
Neuropathology |
0.0 |
0.0 |
0.0 |
0.0 |
|
AP |
Electron Microscopy |
0.0 |
0.0 |
0.0 |
0.0 |
|
AP |
Other |
0.0 |
0.0 |
0.0 |
0.0 |
|
CP |
Clinical Chemistry |
0.0 |
0.0 |
0.0 |
0.0 |
|
CP |
Hematology |
0.0 |
0.0 |
0.0 |
0.0 |
|
CP |
Immunology |
0.0 |
0.0 |
0.0 |
0.0 |
|
CP |
Microbiology |
0.0 |
0.0 |
0.0 |
0.0 |
|
*Computed as total weekly hours reported by a participating full-time pathologist at VAMC II. |
|||||
|
I. |
Diagnosis and Interpretation (continued) |
Average Min/Compl Case |
Average Min/Uncompl Case |
Total Hours/ Week* |
Number of Residents Assisting by Performing Gross/ Screening |
|
CP |
Virology |
0 |
0 |
0 |
0 |
|
CP |
Immunohematology |
0 |
0 |
0 |
0 |
|
CP |
Transfusion |
||||
|
Medicine |
0 |
0 |
0 |
0 |
|
|
CP |
Urinalysis |
0 |
0 |
0 |
0 |
|
CP |
Other |
0 |
0 |
0 |
0 |
|
Usually Performed by: |
||||
|
II. Consultation |
Average Min/Case |
Hours/ Week |
Staff Pathologist |
Resident |
|
Immunopathology |
0 |
0 |
0 |
0 |
|
Bone Marrow |
0 |
0 |
0 |
0 |
|
Pharmacokinetics |
0 |
0 |
0 |
0 |
|
TPN |
0 |
0 |
0 |
0 |
|
Usually Performed by: |
|||
|
III. Medical Quality Assurance |
Hours/ Week |
Staff Pathologist |
Resident |
|
Autopsy |
10 |
0.75 |
0.25 |
|
Test Appropriateness |
0 |
0 |
0 |
|
Surgical Pathology Case Reviews, Peer Review |
3 |
0 |
0 |
|
Cytology Case Reviews, Peer Review |
0 |
0 |
0 |
|
Transfusion Committee |
0.5 |
1 |
0 |
|
Morbidity & Mortality Conferences |
0 |
0 |
0 |
|
Tumor Board |
1 |
0 |
0 |
|
Utilization Review Committee |
0 |
0 |
0 |
|
Other______ |
0 |
0 |
0 |
|
IV. Administration |
Hours/Week |
|
Administrative Paperwork, Meetings in Laboratory |
3 |
|
Administrative Meetings, Committees for VAMC |
2 |
|
Administrative Meetings (Personnel, Fiscal, etc.) |
0 |
|
Approve, Send Out Tests |
0 |
|
Test Development/Menus |
0 |
|
Reduction in Inappropriate Use of Tests |
0 |
|
Reduction in Inappropriate Use of Antibiotics and other Drugs |
0 |
|
Budget Planning/Formulation |
0 |
|
Strategic Planning |
0 |
|
Disciplinary/Counseling Sessions |
0 |
|
Other________ |
0 |
|
V. Education |
Hours/Week |
|
Medical Students, Path+A/O |
1 |
|
Residents, Path,+A/O |
3 |
|
Nurses |
0 |
|
Clinical Physicians |
2 |
|
QA Coordinators |
0 |
|
Committees/Meetings—Medical School |
0 |
|
Other____ |
0 |
|
VII. Research |
Hours/Week |
|
Clinical Pathology |
0 |
|
Anatomic Pathology |
4 |
|
Other_____ |
0 |
|
TOTAL* |
55 hours/week |
|
*Computed as total weekly hours reported by a participating full-time pathologist at VAMC II. |
|
FIGURE 1 The Staffing Algorithm Development Instrument (SADI) for the Other Physician Specialties Panel: Summary of Results1
The purpose of the SADI is to gather the data needed to construct, test, formalize, and enhance the algorithms and rules of thumb for staffing that emerged from prior meetings of each specialty and clinical program panel. The ultimate intention is to develop algorithms which could be applied by the project staff to estimate staffing requirements at VA medical centers (VAMCs), presumably duplicating the results specialty panelists themselves would have derived.
Your responses to the SADI will allow us not only to develop these algorithms but also to compare the relative efficacy of estimating physician requirements by disaggregated job activity versus estimating them more globally, e.g., by ward or Patient Care Area, as used in the original Detailed Staffing Exercises.
Section A of the SADI requests time estimates, in some cases by workload unit. In other cases, it requests time estimates by major job elements (tasks). We hope to infer from your numerical responses the implicit formulas you used to relate physician time to these variables as well as the nature of the relationship between workload and staffing, e.g., linear or nonlinear.
Section B seeks responses to a series of questions designed to allow us to explicitly account for the time spent in non-patient-care activities.
Instructions: In Section A, for each cell of each table, please estimate the number of physician hours required from your specialty to deliver good-quality care under the specified circumstances. Section B is self-explanatory.
|
1 |
These instructions were provided identically for the SADIs constructed for laboratory medicine, nuclear medicine, diagnostic radiology, and radiation oncology. |
LABORATORY MEDICINE
SECTION A: PATIENT CARE ACTIVITIES
I. LABORATORY MEDICINE—PATHOLOGY PROCEDURE TIME
Please fill in the average time in hours required by a staff physician in your service for the workload element listed on the left, noting the presence or absence of residents.
Times indicated below should incorporate the following activities, as appropriate:
-
Conferring with referring physicians
-
Conferring with support services
-
Charting, phone, paperwork
-
Counseling patients and families
-
Teaching and supervising residents
-
Rounds
Chart 1
|
Workload Element |
Average time required (in hours) for one procedure, of the type indicated |
|
|
With Resident |
Without Resident |
|
|
Autopsy |
1.00 |
2.50 |
|
Cytology Accession |
0.17 |
0.17 |
|
Electron Microscopy Accession |
1.00 |
1.00 |
|
Surgical Accession |
0.25 |
0.33 |
Chart 2
|
Average time required (in hours) for these numbers of procedures (in thousands). Assume no residents. |
||||||
|
1 |
10 |
100 |
200 |
500 |
1000 |
|
|
Blood Bank Review and Supervision |
0.00 |
0.25 |
0.50 |
1.00 |
N.A. |
N.A. |
|
Chemistry Lab Review and Supervision |
0.00 |
0.00 |
0.00 |
0.25 |
0.50 |
1.00 |
|
Hematology Lab Review and Supervision |
0.00 |
0.00 |
0.25 |
0.50 |
1.00 |
N.A. |
|
Microbiology Lab Review and Supervision |
0.00 |
0.00 |
0.25 |
0.50 |
1.00 |
N.A. |
SECTION B: NON-PATIENT-CARE TIME
Part 1. The activities listed below generally do not occur every day, but may be time-consuming when looked at over a longer period, such as a week or month. List the time in hours that you would add to each physician's average weekday to allow for the types of non-patient-care-related activites listed below:
Chart 3
|
Assume the amount of research accomplished at this VAMC is: |
High1 |
Medium1 |
Low1 |
|
Education of residents (didactic, classroom, not on the PCA) |
1.0 |
1.0 |
0.2 |
|
Administration by Chief (time required to manage your whole service by a Chief and/or Assistant Chief) |
2.0 |
2.0 |
2.0 |
|
Administration by Others (time required for individual—non-Chief-physicians) |
0.5 |
0.5 |
0.5 |
|
1Examples of research level as defined by total amount of research funding (VA plus non-VA) in FY 1988: High: e.g.; VAMC I with $8.8 million in total funding; Mediun: e.g.; VAMC II with $2.75 million in total funding; Low: e.g.; VAMC III with about $176,000 in total funding. |
|||
|
Assume the amount of research accomplished at this VAMC is: |
High1 |
Medium1 |
Low1 |
|
Hospital-Related Activities (Mortality and Morbidity, Q.A., Staff Meetings) |
0.5 |
0.5 |
0.5 |
|
Overall Median |
|||
|
For Chief2 |
2.0 |
2.0 |
2.0 |
|
For Non-Chief Physician |
2.0 |
2.0 |
1.2 |
|
1Examples of research level as defined by total amount of research funding (VA plus non-VA) in FY 1988: High: e.g.; VAMC I with $8.8 million in total funding; Medium e.g.; VAMC II with $2.75 million in total funding; Low: e.g.; VAMC III with about $176,000 in total funding. 2Assume that Chief does not participate significantly in the Education of Residents and Hospital-Related Activities; SADI users may easily modify this assumption. |
|||
Part 2. In order to determine the actual staffing at a VAMC, the number of FTEE must be adjusted to allow for CME, research, and any off-time required. What do you believe to be the appropriate percentage of time the “average” (typical) staff member of your service should devote to each of the following categories of non-patient-care-related activities?
Chart 4
|
Assume the amount of research accomplished at this VAMC is: |
High1 |
Medium1 |
Low1 |
|
Continuing Education |
12.5 |
12.5 |
8.0 |
|
Research (off the PCA) |
30.0 |
30.0 |
10.0 |
|
Vacation, Administrative Leave, Sick Time, Other |
14.0 |
14.0 |
14.0 |
|
Total Percentage of Time |
56.5 |
56.5 |
32.0 |
|
1Examples of research level as defined by total amount of research funding (VA plus non-VA) in FY 1988: High: e.g.; VAMC I with $8.8 million in total funding; Mediun: e.g.; VAMC II with $2.75 million in total funding; Low: e.g.; VAMC III with about $176,000 in total funding. |
|||
NUCLEAR MEDICINE
SECTION A: PATIENT CARE ACTIVITIES
I. NUCLEAR MEDICINE-PROCEDURE TIME
Please fill in the average time in hours required by a staff physician in your service for the workload element listed on the left, noting the presence or absence of residents.
Times indicated below should incorporate the following activities, as appropriate:
-
Conferring with referring physicians
-
Conferring with support services
-
Charting, phone, paperwork
-
Counseling patients and families
-
Teaching and supervising residents
-
Rounds
Chart 1
|
Workload Element |
Average time required (in hours) for one procedure of the type indicated |
|
|
With Resident |
Without Resident |
|
|
Scan |
1.00 |
1.13 |
|
Others: |
||
|
In Vitro |
0.25 |
0.25 |
|
Cardiology |
1.50 |
1.25 |
|
Therapy |
2.50 |
2.00 |
Part 1. The activities listed below generally do not occur every day, but may be time-consuming when looked at over a longer period, such as a week or month. List the time in hours that you would add to each physician's average weekday to allow for the types of non-patient-care-related activities listed below:
Chart 2
|
Assume the amount of research accomplished at this VAMC is: |
High1 |
Medium1 |
Low1 |
||||||
|
Hi |
Lo |
Med |
Hi |
Lo |
Med |
Hi |
Lo |
Med |
|
|
Education of residents (didactic, classroom, not on the PCA) |
5.0 |
1.0 |
2.4 |
5.0 |
0.5 |
2.0 |
1.6 |
0.0 |
0.1 |
|
Administration by Chief (time required to manage your whole service by a Chief and/or Assistant Chief) |
10.0 |
2.4 |
3.5 |
8.0 |
2.0 |
3.0 |
5.0 |
2.0 |
3.0 |
|
Administration by others: (time required for individual—non-Chief-physicians) |
5.0 |
0.5 |
0.6 |
4.0 |
0.0 |
0.6 |
1.0 |
0.0 |
0.6 |
|
1Examples of research level as defined by total amount of research funding (VA plus non-VA) in FY 1988: High: e.g.; VAMC I with $8.8 million in total funding; Medium: e.g.; VAMC II with $2.75 million in total funding; Low: e.g.; VAMC III with about $176,000 in total funding. |
|||||||||
|
Assume the amount of research accomplished at this VAMC is: |
High1 |
Medium1 |
Low1 |
||||||
|
Hi |
Lo |
Med |
Hi |
Lo |
Med |
Hi |
Lo |
Med |
|
|
Hospital-Related Activities (Mortality and Morbidity, Q.A., Staff Meetings) |
6.0 |
0.4 |
1.5 |
5.0 |
1.0 |
0.4 |
4.0 |
0.4 |
1.0 |
|
Overall Median |
|||||||||
|
For Chief2 |
10.0 |
2.4 |
3.5 |
8.0 |
2.0 |
3.0 |
5.0 |
2.0 |
3.0 |
|
For Non-Chief Physician |
16.0 |
3.0 |
3.4 |
14.0 |
3.0 |
1.5 |
5.0 |
1.1 |
2.6 |
|
1Examples of research level as defined by total amount of research funding (VA plus non-VA) in FY 1988: High: e.g.; VAMC I with $8.8 million in total funding; Mediun: e.g.; VAMC II with $2.75 million in total funding; Low: e.g.; VAMC III with about $176,000 in total funding. 2 Assume that Chief does not participate significantly in the Education of Residents and Hospital-Related Activities; SADI users may easily modify this assumption. |
|||||||||
Part 2. In order to determine the actual staffing in this hospital, the number of FTEE must be adjusted to allow for CME, research, and any off-time required. What do you believe to be the appropriate percentage of time the “average” (typical) staff member of your service should devote to each of the following categories of non-patient-care-related activities?
Chart 3
|
Assume the amount of research accomplished at this VAMC is: |
High1 |
Medium1 |
Low1 |
||||||
|
Hi |
Lo |
Med |
Hi |
Lo |
Med |
Hi |
Lo |
Med |
|
|
Continuing Education |
6.0 |
8.3 |
5.0 |
3.0 |
8.3 |
6.0 |
8.3 |
6.0 |
3.0 |
|
Research (off the PCA) |
32.0 |
15.0 |
25.0 |
15.0 |
10.0 |
16.0 |
0.0 |
0.0 |
0.0 |
|
Vacation, Administrative Leave, Sick Time, Other |
8.0 |
10.0 |
14.0 |
14.0 |
1.0 |
8.0 |
10.0 |
8.0 |
14.0 |
|
Total Percentage of Time |
46.0 |
33.3 |
44.0 |
32.0 |
28.3 |
30.0 |
18.3 |
14.0 |
17.0 |
|
1Examples of research level as defined by total amount of research funding (VA plus non-VA) in FY 1988: High: e.g.; VAMC I with $8.8 million in total funding; Mediun: e.g.; VAMC II with $2.75 million in total funding; Low: e.g.; VAMC III with about $176,000 in total funding. |
|||||||||
RADIATION ONCOLOGY
SECTION A: PATIENT CARE ACTIVITIES
I. RADIATION ONCOLOGY—PROCEDURE TIME
Please fill in the average time in hours required by a staff physician in your service for the workload elements listed on the left, noting the presence or absence of residents.
Times indicated below should incorporate the following activities, as appropriate:
-
Conferring with referring physicians
-
Conferring with support services
-
Charting, phone, paperwork
-
Counseling patients and families
-
Teaching and supervising residents
-
Rounds
Chart 1
|
Workload Element |
Average time required (in hours) for one procedure, of the type indicated |
|
|
With Resident |
Without Resident |
|
|
New Patient Examination |
2.00 |
2.00 |
|
Treatment visit |
0.13 |
0.13 |
|
Other: |
||
|
Treatment Planning and Simulation |
2.50 |
2.50 |
Part 1. The activities listed below generally do not occur every day, but may be time-consuming when looked at over a longer period, such as a week or month. List the time in hours that you would add to each physician's average weekday to allow for the types of non-patient-care-related activities listed below:
Chart 2
|
Assume the amount of research accomplished at this VAMC is: |
High1 |
Medium1 |
Low1 |
|
Education of residents (didactic, classroom, not on the PCA) |
1.00 |
1.00 |
0.00 |
|
Administration by Chief (time required to manage your whole service by a Chief and/or Assistant Chief) |
2.00 |
2.00 |
0.50 |
|
Administration by Others (time required for individual—non-Chief— physicians) |
|||
|
Hospital-Related Activities (Mortality and Morbidity, Q.A., Staff Meetings,) |
1.00 |
1.00 |
1.00 |
|
Overall Median |
|||
|
For Chief2 |
2.00 |
2.00 |
2.00 |
|
For Non-Chief Physician |
2.00 |
2.00 |
1.00 |
|
1Examples of research level as defined by total amount of research funding (VA plus non-VA) in FY 1988: High: e.g.; VAMC I with $8.8 million in total funding; Medium: e.g.; VAMC II with $2.75 million in total funding; Low: e.g.; VAMC III with about $176,000 in total funding. 2Assume that Chief does not participate significantly in the Education of Residents and Hospital-Related Activities; SADI users may easily modify this assumption. |
|||
Part 2. In order to determine the actual staffing in this hospital, the number of FTEE must be adjusted to allow for CME, research, and any off-time required. What do you believe to be the appropriate percentage of time the “average” (typical) staff member of your service should devote to each of the following categories of non-patient-care-related activities?
Chart 3
|
Assume the amount of research accomplished at this VAMC is: |
High1 |
Medium1 |
Low1 |
|
Continuing Education |
5.00 |
5.00 |
5.00 |
|
Research (off the PCA) |
10.00 |
5.00 |
0.00 |
|
Vacation, Administrative Leave, Sick Time, Other |
9.60 |
9.60 |
9.60 |
|
Total Percentage of Time |
24.60 |
19.60 |
14.60 |
|
1Examples of research level as defined by total amount of research funding (VA plus non-VA) in FY 1988: High: e.g.; VAMC I with $8.8 million in total funding; Medium: e.g.; VAMC II with $2.75 million in total funding; Low: e.g.; VAMC III with about $176,000 in total funding. |
|||
DIAGNOSTIC RADIOLOGY
SECTION A: PATIENT CARE ACTIVITIES
I. RADIOLOGY—PROCEDURE TIME
Please fill in the average time in hours required by a staff physician in your service for the workload elements listed on the left, noting the presence or absence of residents.
Times indicated below should incorporate the following activities, as appropriate:
-
Conferring with referring physicians
-
Conferring with support services
-
Charting, phone, paperwork
-
Counseling patients and family
-
Teaching and supervising residents
-
Rounds
Chart 1
|
Workload Element |
Average time required (in hours) for one procedure, of the type indicated |
|
|
With Resident |
Without Resident |
|
|
Diagnostic x-ray (chest film, skeletal, etc.) |
0.17 |
0.13 |
|
CT Scan |
0.50 |
0.50 |
|
Ultrasound |
0.50 |
0.50 |
|
Interventional Procedure (myelogram, angiogram, etc.) |
1.50 |
1.50 |
|
Others? Specify |
||
Part 1. The activities listed below generally do not occur every day, but may be time-consuming when looked at over a longer period, such as a week or month. List the time in hours that you would add to each physician's average weekday to allow for the types of non-patient-care-related activities listed below:
Chart 2
|
Assume the amount of research accomplished at this VAMC is: |
High1 |
Medium1 |
Low1 |
|
Education of residents (didactic, classroom, not on the PCA) |
1.00 |
1.00 |
1.00 |
|
Administration by Chief (time required to manage your whole service by a Chief and/or Assitant Chief) |
7.00 |
6.00 |
4.00 |
|
Administration by Others (time required for individual—non-Chief— physicians) |
0.50 |
0.50 |
0.50 |
|
Hospital-Related Activities (Mortality and Morbidity, Q.A., Staff Meetings) |
1.00 |
1.00 |
1.00 |
|
Overall Median |
|||
|
For Chief2 |
7.00 |
6.00 |
4.00 |
|
For Non-Chief Physician |
2.50 |
2.50 |
2.50 |
|
1Examples of research level as defined by total amount of research funding (VA plus non-VA) in FY 1988: High: e.g.; VAMC I with $8.8 million in total funding; Medium: e.g.; VAMC II with $2.75 million in total funding; Low: e.g.; VAMC III with about $176,000 in total funding. 2Assume that Chief does not participate significantly in the Education of Residents and Hospital-Related Activities; SADI users may easily modify this assumption. |
|||
Part 2. In order to determine the actual staffing in this hospital, the number of FTEE must be adjusted to allow for CME, research, and any off-time required. What do you believe to be the appropriate percentage of time the “average” (typical) staff member of your service should devote to each of the following categories of non-patient-care-related activities?
Chart 3
|
Assume the amount of research accomplished at this VAMC is: |
High1 |
Medium1 |
Low1 |
|
Continuing Education |
2.50 |
2.50 |
2.50 |
|
Research (off the PCA) |
20.00 |
10.00 |
10.00 |
|
Vacation, Administrative Leave, Sick Time, Other |
12.00 |
12.00 |
12.00 |
|
Total Percentage of Time |
34.50 |
24.50 |
14.50 |
|
1Examples of research level as defined by total amount of research funding (VA plus non-VA) in FY 1988: High: e.g.; VAMC I with $8.8 million in total funding; Medium: e.g.; VAMC II with $2.75 million in total funding; Low: e.g.; VAMC III with about $176,000 in total funding. |
|||
INSTITUTE OF MEDICINE
Committee to Develop Methods Useful to the Department of Veterans Affairs in Estimating Its Physician Requirements
OTHER PHYSICIAN SPECIALTIES PANEL ROSTER
ROBERT M.DONATI (Chair),† Executive Associate Vice President, St. Louis University Medical Center, St. Louis, Missouri
STANLEY J.GEYER, Chief of Staff, Seattle VA Medical Center, Seattle, Washington (through May 1990); Director, Laboratory Medicine, Georgetown University Hospital, Washington, D.C. (from June 1990)
RICHARD C.REBA, Professor of Radiology and Medicine and Director, Division of Nuclear Medicine, George Washington University Medical Center, Washington, D.C.
CHARLES C.ROGERS, Professor and Director, Division of Radiation Oncology and Biophysics, George Washington University Medical Center, Washington, D.C.
ROGER H.SHANNON, Director, Radiology Service, Department of Veterans Affairs, Washington, D.C., and Chief, Radiology, Durham VA Medical Center, Durham, North Carolina
ELEANOR M.TRAVERS, Director, Pathology Service, Department of Veterans Affairs, Washington, D.C.
HENRY N.WAGNER, Jr., Professor of Medicine, Radiology, and Environmental Health Sciences and Director, Divisions of Nuclear Medicine and Radiation Health Sciences, Johns Hopkins Medical Institutions, Baltimore, Maryland
Staff: Bobbie J.Alexander, Staff Associate
|
†Member of study committee. |









































