
AMBULATORY CARE PANEL REPORT1
INTRODUCTION
The ambulatory care panel, organized by the study committee in the winter of 1989, was charged with examining physician manpower requirements for the ambulatory care program at VA medical centers. The panel was composed of eight physicians—four with specialties in internal medicine, one in surgery, one in rehabilitation medicine, one in neurology, and one in psychiatry. The chairman of the panel was also a member of the study committee. The panel roster is attached.
This report will describe the ambulatory care panel's analyses, conducted in the framework of the “panel process” described in the “Overview” to this section of Volume II. Reported here will be the results of these analyses, along with the panel's commentary and conclusions.
EXPERT JUDGMENT APPROACHES TO DETERMINING PHYSICIAN REQUIREMENTS IN THE AMBULATORY CARE PROGRAM
The Detailed Staffing Exercise (DSE) Approach
Initial Efforts
The first meeting of the ambulatory care panel was convened in April 1990. The primary purpose was to determine whether the expert judgment panel process, as the study committee first conceived it, represented a viable means
|
1 |
The initial draft of this report was prepared by Bobbie J.Alexander, Staff Associate to the Ambulatory Care Panel during the conduct of the study. This final report was prepared by the editors of this Volume. |
for determining physician staffing for the entire ambulatory care program at individual VAMCs. This process required the development of staffing instruments that would provide the panel with information about workload, about various nonphysician personnel that might be available to deliver care, and then—given that conditional information —that would elicit judgments about the appropriate levels of physician FTEE to meet that workload. In preparation for the first panel meetings, staffing instruments were constructed for three actual VAMCs.
Focusing on the analysis of these instruments, study staff tested the feasibility of this process at the first meeting and found that it was generally acceptable, that panel members could render physician staffing judgments, but that they wished to have more detailed information about workload and other factors. The panel concluded that study staff should proceed with the expert judgment process, but that many of the underlying assumptions within the initial staffing exercises should be better defined in the next generation of the staffing instrument. In particular,
-
more detail was needed on clinic configuration and scheduling, defining the scope of each clinic listed—to include how frequently each is held, its length (in hours), and the number of patients seen.
-
emergency room activities should be treated separately from admitting and screening.
-
more specific detail was needed for psychiatry and surgery clinics.
-
the input of psychologists and psychiatric social workers should be acknowledged where appropriate, and the number of residents should be adjusted accordingly.
-
the postgraduate year of residents should be indicated.
-
compensation and pension exams need to be included—focusing on fee-for-service contracts as well as in-house services.
-
the administrative structure of the ambulatory care program should be defined: i.e., is it institutional administration or patient-focused administration?
-
the physician manpower required for direct patient contact and resident education should be distinguished from that required for research, continuing medical education, classroom teaching, administration, and leaves.
-
the next instruments should better separate out and define ambulatory surgery.
-
the next instruments should include at least one satellite clinic.
-
the length of the assumed workweek—30 hours, 40 hours, 50 hours or 60 hours—should be noted explicitly.
The proper role of the chief of the ambulatory care program was a significant topic of discussion at the first panel meeting. At some VAMCs, the chief may have direct control of a number of physicians, similar to the chief of a specialty service (e.g., medicine). At other VAMCs, the chief is primarily a program manager and oversees all aspects of ambulatory care across all disciplines, but does not directly supervise staff physicians from the specialty services. On balance, the panel thought that the second model is more appropriate, since it is consistent with the philosophy that each physician in the institution is assigned to a discipline (service) and the distribution of patient care workload determines the location of practice. Subsequent staffing exercises should be compatible with this viewpoint, the panel indicated.
At the conclusion of the first round of all eight specialty and clinical program panel meetings, there was convened a major meeting (Joint Meeting I) involving the study committee (which includes all eight panel chairmen), the data and methodology panel, and the VA liaison committee. At this meeting (held in May 1990), participants reviewed and evaluated the key concepts and assumptions underlying both the empirically based and expert judgment based approaches to determining VA physician requirements.
The study staff emerged from Joint Meeting I with a set of recommendations from the committee on how to proceed with the panel process. Staff began to implement these recommendations on a panel-specific basis.
DSE: Overall Rationale
The next stage in the development of expert judgment staffing methodology centered on the preparation for, and conduct of, the second panel meeting, held in August, 1990. Again, three actual VAMCs were selected for intensive analysis—in essence, to serve as “laboratories” for methodology development. They were chosen to represent a range of geographic locations, bed sizes, staffing intensities, available services/programs, and affiliation status.
A revised staffing instrument, later termed the Detailed Staffing Exercise (DSE), was developed in response to the panel's recommendations. It provided a more specific description of the VAMC, including the number of admissions, length of stay, and DRG mix of patients in each PCA. It was intended that all three VAMCs would be presented “in context” and described in sufficient detail that the respondent could assess physician staffing requirements almost as if he/she were reviewing data at the facility.
Panel members were asked to complete DSEs for two of the VAMCs prior to the meeting. These results were tabulated and distributed at the meeting, along with information on both the actual staffing and the statistically derived staffing at these facilities. After review and discussion, each panel member was given the opportunity to reevaluate his initial staffing estimates. Then the panel, as a group, worked through a third DSE constructed for VAMC III; the members subsequently reflected on these results in light of the actual and statistically derived staffing for ambulatory care at VAMC III.
Instructions and Assumptions
To illustrate how the DSE works, a completed version of the instrument is presented as Exhibit 1 of the “Overview” to this section of Volume II. This DSE is nearly identical structurally to the one constructed for ambulatory care (although the latter does focus only on physician requirements for the ambulatory care program per se).
In Section A of each exercise, the basic question was the same for each ambulatory patient care area: How much time (in hours) must be contributed by physicians in this VAMC's ambulatory care program to meet a specified workload level during an average weekday, under certain assumptions about patient mix, residents, and support staff availability. These hours were then converted to FTEE, using the 40-hour-per-week equivalency assumption.
In Section B of each DSE, panel members were asked to estimate the number of hours (and then to covert into FTEE) required from ambulatory care physicians for night call and weekend coverage, and for physician time spent in non-patient-care-related activities: research off the patient care area, educational activities not related to direct patient care, quality assurance, mortality and morbidity meetings or studies, administrative activities, and any other function not directly related to patient care areas. Also, panel members were asked to estimate how many consulting and attending (C&A) and without-compensation (WOC) physicians would be desired from the community or neighboring medical school (given the member's prior assessment of VA staff physician requirements).
In general, the second meeting focused on the assumptions, thought processes, and algorithms underlying the panel's staffing estimates. From these discussions, the panel worked toward a consensus about the appropriate data, assumptions, and methodology required for expert judgment assessments of physician requirements. Strategies were discussed for reconciling the alternative
approaches to deriving physician requirements: the expert panel approach, statistical models, and the application of external (to the VA) staffing norms.
The Staffing Algorithm Development Instrument (SADI) Approach
SADI: Overall Rationale
At the conclusion of the second panel meeting, the committee implemented a sequence of postmeeting activities designed to promote the development of consensus positions regarding the appropriate methodology and accompanying data for determining VA physician requirements.
This postmeeting process was formally initiated with the development of the Staffing Algorithm Development Instrument (SADI). The purpose of this new instrument was to test, build upon, and ultimately strengthen the algorithms and rules of thumb for staffing that emerged from the meetings of all eight specialty and clinical program panels. The instrument was designed to determine whether panel members could be asked a set of generic staffing questions whose answers would be applied to selected data from individual VAMCs to derive appropriate staffing levels for these facilities.
Instructions and Assumptions
Like the DSE, the SADI has two Sections, A and B, which focus on patient care and non-patient care activities, respectively. In Section A, the respondent is asked to estimate the amount of physician time required to complete a number of patient care functions and tasks under varying assumptions about the availability of residents and nonphysician practitioners. In Section B, the respondent must determine the amount of physician time that should be allocated to research, classroom instruction, continuing education, administration, and leaves of absence. To derive physician requirements for a given VAMC, the estimated physician hours for patient care and non-patient care activities are summed, then converted to FTEE under the assumption that 40 hours per week translates into one FTEE.
Section A was divided into three parts. In the first, all panel members were asked to estimate the average time in hours required by an ambulatory care program staff physician for the typical emergency/walk-in patient, or the typical
admitting & screening patient. In responding, panelists were requested to note the SADI's stated assumptions regarding the presence or absence of residents and nonphysician practitioners, and whether the visit was by a new or returning patient. In the second part, panel members were to estimate the average time in hours required by a staff physician in their service for a typical patient visit to one of their specialty clinics, noting the presence or absence of residents and nonphysician practitioners, and whether the visit is by a new or returning patient. The final part of Section A asked for estimates of the physician time (per test) required for ambulatory care-based special procedures, conditional on the presence or absence of a resident. The list of special procedures used was recommended by the panel during its second meeting. In Section B, panel members were asked to determine the amount of physician time that should be allocated to research, classroom instruction, continuing education, administration, and leaves of absence. To derive physician requirements for a given VAMC, the estimated physician hours for patient care and non-patient care activities are summed, then converted to FTEE under the assumption that 40 hours per week translates into one FTEE.
Presented in Figure 1 of this report is the ambulatory care SADI, complete with the the panel members' median estimates for physician task times. (Where multiple members estimated task time, the high, low, median, and mean are reported; where only one panel member estimated times, e.g., the neurology clinics, those numbers are simply reported.) A detailed, self-contained, illustration of how the SADI can be applied to determine the number of physicians required at a given VAMC is found in Exhibit 3 of the “Overview” to this section of Volume II. This example happens to focus on total internist requirements at VAMC I; the application of the ambulatory care SADI to determine physician FTEE at a given facility proceeds in a very similar fashion. A careful study of the example reveals the type of facility-specific data needed to implement any SADI.
EMPIRICALLY BASED APPROACHES TO DETERMINING PHYSICIAN STAFFING FOR THE AMBULATORY CARE PROGRAM
Six of the 14 VAMC patient care areas defined by the study committee are for ambulatory care: medicine, surgery, psychiatry, neurology, rehabilitation medicine, and other physician services. Each of the first five PCAs above is defined operationally as the set of clinic stops related to that specialty, e.g., the
ambulatory surgery PCA consists of all the designated surgery clinic stops. The other physician services PCA consists of all the remaining physician-related clinic stops, including the emergency room and admitting & screening. (For further discussion of how ambulatory care clinic stops were mapped into ambulatory PCAs, see chapter 4 of Volume I.)
Over the course of its two panel meetings and a follow-up conference call, the panel evaluated alternative specifications of production function models estimated for each of these six PCAs. The final versions of these equations, as derived in cooperation with the study's data and methodology panel, are presented in Table 2.
No inverse production function models have been estimated. As specified in this study, the IPF is specialty specific, and the facility, not the PCA, is the basic unit of observation. On the other hand, the ambulatory care program is multidisciplinary and encompasses only a portion of the VAMC. Nonetheless, the influence of ambulatory care workload on physician requirements is reflected in the IPF—specifically, as an independent variable that may be (and frequently was) a statistically significant factor “explaining” variations in physician FTEE devoted to direct care and resident education across the VAMC.
PHYSICIAN STAFFING RESULTS FROM APPLICATION OF EMPIRICALLY BASED AND EXPERT JUDGMENT APPROACHES
In Table 1 are alternative estimates of physician requirements for the ambulatory care program at VAMCs I, II, and III in FY 1989, as derived from: the VA's cost distribution report (CDR), the PF variant of the empirically based models, the DSE (from the second panel meeting), the SADI, and a mail survey of panel members conducted just prior to Joint Meeting II (held September 7–9, 1990).
Any conclusions drawn from the analysis of only three VAMCs must be treated cautiously, but several trends are suggested in Table 1. Both expert judgment approaches yield total FTEE estimates that noticeably exceed those derived from the PF and the actual physician count as inferred from the CDR. When the focus shifts to physician FTEE for direct care and resident education only, the DSE continues to yield the largest estimates but now there is no systematic tendency for the SADI results to exceed the PF.
By all criteria, the ambulatory care program at VAMC III appears to be significantly understaffed, in terms of both total physician FTEE and that allocated to direct care and resident education only. The expert judgment
approaches, but not the PF, indicate that VAMCs I and II have too few physicians in ambulatory care.
The approach yielding total FTEE estimates that are the closest overall to the panel's recommended levels, as indexed by the median of their responses to the Survey, is the SADI.
One possible explanation for these notable discrepancies between actual versus recommended physician staffing centers on the quality of the FTEE data available in the CDR for ambulatory care. In this FTEE accounting scheme, physicians in the different services (or their service chiefs) are asked to allocate their time across a range of activities that includes ambulatory care. But since a large component of physician time has traditionally been allocated to the inpatient side, these physicians may tend to underestimate the time spent in ambulatory care, as the latter has edged up in recent years.
Reflecting on the state of ambulatory care in the VA generally (and not just at these three facilities), the panel notes that many VA hospitals are not equipped (or constructed) for ambulatory care programs or services.
At many facilities, the number and quality of examining rooms, overall floor space, and support personnel are all inadequate. This, in turn, may have a dampening effect in many facilities on the amount of staff physician FTEE that can be usefully allocated to ambulatory care. (This, in turn, may account for some of the discrepancy between CDR-recorded physician FTEE for ambulatory care and the FTEE levels derived from the expert judgment models.)
The issue of unmet patient need was a major concern at both panel meetings. Traditionally, queues are regarded as more tolerable in ambulatory than in acute patient care; in many medical centers, there is a significant queueing process, with some patients waiting months for specific types of ambulatory care. Moreover, current eligibility criteria create situations in which many patients may be accepted for care (initial access) but referral to other ambulatory care and inpatient programs is limited because of limited resources.
EXTERNAL (NON-VA) PHYSICIAN STAFFING NORMS
Data on physician staffing for ambulatory care were collected from external (to the VA) health care organizations to determine whether methodologies or productivity performance norms that may exist in the public and private sectors could be applied successfully to the VA ambulatory care program.
Also acquired were some “internal” VA staffing guidelines, issued about 1965, which indicated it was appropriate to have one physician FTEE per 3500 visits per year.
Regarding the external staffing criteria, the Department of Defense (DoD) provided perhaps the most useful data since it utilizes full-time physician equivalents much like the VA; however, the DoD patient population is generally younger and includes a significant percentage of women and children. DoD defines physician performance levels in terms of the annual number of outpatient and inpatient visits rendered (the standard varies widely depending on the specialty and whether the facility has a teaching program). A different criterion applies if there are a significant number of residents, since it is assumed they need supervision regardless of workload.
From the Indian Health Service (IHS) came a simple staffing guideline: outpatient staffing is earned at the rate of 1.0 physician for every 5000 visits per year.
An interesting application was based on a 1987 survey conducted by the American Medical Association, “1987 AMA Socioeconomic Monitoring System Core Survey.” Only active, nonfederal, patient care physicians were sampled. By analyzing the reported rates with which surveyed physicians generated hospital and office visits, comparisons to the VA could be made.
The New York City Health and Hospitals Corporation (NYH&HC) provided data on physician FTEE per office visit.
Finally, data were obtained from a large, nationwide HMO on physician staffing in relation to outpatient visits (as well as inpatient workload). However, the patient population served by this HMO is substantially younger and contains more females than the VA population, with considerably different disease patterns.
Table 3 illustrates the computational approach, via dimensional analysis, used to derive each of these staffing standards. Summarized in Table 4 are the results from applying these norms to calculate the implied levels of physician staffing for the ambulatory care programs at VAMC I, II, and III. The logic behind these calculations is presented and illustrated in the “Overview” to this section of Volume II (see “External Norms”).
CONCLUSIONS
To determine the number of physicians required for the ambulatory care program at VAMCs, the panel endorses the study committee's proposed
Reconciliation Strategy. Regarding the components of the strategy, the panel recommends the following:
Patient Care, Resident Education, and Administration
To derive the level of physician FTEE required to care for a given patient workload, while residents are being trained and administrative duties are being handled, the panel recommends an expert-judgment-based methodology built around the SADI. The DSE is an acceptable alternative methodology, but the SADI is the better approach for ambulatory care for several reasons.
The time (and hence, FTEE) required to deliver ambulatory care can be usefully conceptualized as the time to manage a sequence of patient visits, of varying complexities. Some will be initial visits, others followup. Some will be handled with residents and various nonphysician practitioners; others may involve primarily the physician. Some will be emergency; others routine. Depending on the patient's problem, different specialties (or mixes of them) will be involved. The degree of physician involvement in a given visit will be influenced by all of these factors. Because it focuses on the physician time required per visit or per procedure, the SADI methodology is thus well suited for computing physician requirements in ambulatory care. Unlike the DSE instrument, which is facility specific, the SADI is a generic construct that can be applied directly to any VAMC (assuming adequate information about outpatient workload, residents, and support personnel).
The application of SADI to the ambulatory care program at VAMCs I, II, and III lead generally to plausible estimates of physician FTEE for patient care, resident education, and administration. The panel regards this as a fairly successful small-scale experiment; however, the validity and acceptability of the SADI methodology should be evaluated further through a much broader application involving a strategically chosen sample of VA ambulatory care programs.
Either form of the empirically based physician staffing model has problems at present. Conceptually, the PF does offer an attractive approach for analyzing physician requirements in ambulatory care. All of the VA's clinic stops are mapped into six mutually exclusive and exhaustive PCAs; and one can calculate alternative combinations of provider types that are consistent with meeting patient workload in each PCA. Given certain assumptions, physician FTEE required by specialty can be deduced from these statistical analyses. But a major concern is that the FTEE data used in estimating these models may be
significantly flawed at present. The panel believes that physician FTEE devoted to ambulatory care are consistently undercounted in the current data system. Despite efforts to improve data collection at many VAMCs, there is insufficient uniformity in the way facilities allocate physician FTEE between inpatient and ambulatory care and among activity categories within ambulatory care. Because the PF model requires FTEE broken out to this level of detail, the issue is important. Correspondingly, if CDR record keeping continues to improve over time, this objection to the PF model should dissipate.
The IPF model is plagued by these same data difficulties, but it presents a more fundamental problem. Because the IPF equations presented to the panel do not allow physician FTEE to be analyzed by PCA, there is no appropriate IPF for ambulatory care. (However, the effect of outpatient workload on physician requirements is recognized in each IPF.)
Research
Physician FTEE allocated to research should reflect a deliberate VA policy decision—not something determined mechanically from CDR data. The panel recommends that this determination be made by each facility with guidance from VA Central Office. Although a good research program will enhance the overall quality of ambulatory care at any VAMC, the panel acknowledges that the amount of FTEE allocated to research will—and should—vary significantly across facilities. In determining these FTEE, VA policymakers should be guided by measurable indicators of research productivity such as the level of VA and non-VA research funding. The strength of the VAMC's affiliation with a scientifically productive medical school is another potential indicator.
Continuing Education
As with research, the commitment to continuing education should not be dictated by the status quo, but rather be the result of a conscious VA policy decision on what continuing education is required to promote high-quality care. At a minimum, the FTEE allocated to continuing education should be commensurate with the commitment required to maintain board certification in the specialties concentrated in ambulatory care. The panel strongly recommends that the continuing education allowance be greater than this minimum and applied to all VAMCs, affiliated or not. Further, each VAMC should develop
a vigorous continuing education program of its own and ensure that all staff physicians participate to a specified extent
Leaves of Absence
The percentage of total FTEE earmarked for vacation, sick leave, administrative leave, and other authorized absences should be established on the basis of existing VA regulations.
Purchased Coverage for Nights and Weekends
When emergency, admitting & screening, and related ambulatory care clinic stops are open, one or more staff physicians should be available either to provide patient care or to supervise the provision of patient care by residents or others. When availability cannot be provided by existing staff physicians —for example, when extensive coverage is needed in smaller institutions with few staff physicians—then additional physician availability should be arranged for nights and weekends by purchasing coverage from other physicians. The amount of purchased coverage will depend on the total number of hours of coverage needed, the number of staff physicians available to provide coverage, and the distribution of staff physician effort between night or weekend coverage and other duties. (At some VAMCs, this “off hour” coverage is provided by residents hired specifically for the task. In the future, quality management concerns and other factors may serve to reduce the role of residents in this area.)
In general, decisions about the purchase of additional coverage should be made by each VAMC following guidelines provided by VA Central Office.
Consulting & Attending and Without-Compensation Coverage
These non-VA physicians enhance the quality of both patient care and resident education. Therefore, the need for these services may be higher in hospitals with more extensive teaching programs and in hospitals with limited types of specialists on its staff. Decisions about the acquisition of consulting and attending (C&A) and WOC services should be made at each facility following
guidelines provided by the VA. The panel notes also that compensation for C&A services has not been raised in many years; the fee remains $40/visit for attendings and $75/visit for consultants. The VA should strongly consider increasing these payment rates.
External Norms
The panel reviewed non-VA staffing ratios (visits/MD) from six sources and also VA guidelines for ambulatory care issued about 25 years ago. Each of these “norms” was applied, in turn, to VAMC I, II, and III to calculate the physician staffing level in ambulatory care consistent with the norm. The implied physician staffing level of each VAMC could then be compared with its actual staffing.
In sum, the panel found these analyses interesting, but counsels caution in drawing policy inferences from them. The overall trend from applying these norms was as follows: Two VAMCs (I and II) appeared neither significantly overstaffed nor understaffed, whereas VAMC III's CDR total for ambulatory care was significantly lower than any of the norms suggested that it should be.
The validity of these comparisons hinges on the validity of applying these externally derived visits/MD ratios to VA facilities, and the panel has several concerns in this regard. First, an outpatient “visit” is not a homogeneous concept but rather is defined specifically by the number, type, and severity of problems presented by the patient. In applying these norms (within the scope of this study), there was no way to control for this natural variability. Second, although the definition of a physician “FTEE” in the VA is relatively clear, this is not the case elsewhere. Hence, there will be some (unobserved, hard-to-correct) heterogeneity in the denominators of these staffing ratios, threatening the validity of the comparisons.
Overall Adequacy of Physician Staffing in the VA
For the three VAMCs studied at length, two (VAMC I and II) were found (in FY 1989) to be understaffed according to all modeling approaches except the PF; VAMC III was significantly understaffed by all approaches. In the panel's judgment, this general pattern of results would likely be replicated if these modeling approaches were applied across the VA system. Speaking
qualitatively, the panel feels that for the patient care that needs to be delivered, ambulatory care in the VA is presently understaffed. However, a sample of three is too small for drawing quantitative conclusions about the degree of understaffing systemwide. If a physician requirements methodology built around the SADI were to be applied to ambulatory care programs across the system, a quantitative assessment would be possible—and the panel's present judgment on staffing adequacy could be checked directly.
Other Points
Whatever physician staffing methodology the VA adopts should be reevaluated and updated on an ongoing basis. Given the anticipated changes in patient demographics, the technology of care, and physician practice patterns in the private sector, determining physician requirements in the VA cannot be a one-shot affair. A thorough reassessment of the methodology and required data should be undertaken at least every 5 years.
Final Remarks
For calculating physician requirements for the ambulatory care program at VAMCs, the panel supports the use of a Reconciliation Strategy whose FTEE components are analyzed as recommended above.
TABLE 1 Estimates of Physician Requirements in Ambulatory Care at Three VAMCs
|
A. Total FTEE |
|||||
|
VAMC |
CDR |
PF |
DSE |
SADI |
Survey1 |
|
VAMC I |
28.4 |
26.4 |
54.2 |
43.0 |
47.5 |
|
VAMC II |
51.3 |
41.0 |
95.7 |
52.8 |
67.0 |
|
VAMC III |
19.3 |
30.7 |
79.2 |
50.1 |
52.5 |
|
B. Direct Care Plus Resident Education FTEE Only |
|||||
|
VAMC |
CDR |
PF |
DSE |
SADI |
Survey1 |
|
VAMC I |
21.32 |
19.02 |
27.9 |
21.8 |
N.A. |
|
VAMC II |
47.83 |
37.53 |
52.9 |
29.9 |
N.A. |
|
VAMC III |
19.14 |
30.54 |
52.4 |
35.1 |
N.A. |
|
1Panel median response to the question, posed by mail survey in September 1990, of what is the overall preferred physician FTEE level at each VAMC. To provide a context for the response, each panel member was presented a summary of the physician FTEE level emerging, alternatively, from the CDR, from both empirically based approaches (as applicable), and from both expert judgment approaches. 2Based on systemwide averages for medicine services in RAM Group 3, these figures assume that 74 percent of total education FTEE in ambulatory care is for resident education. 3Based on systemwide average for medicine services in RAM Group 5, these figures assume that 67 percent of total education FTEE in ambulatory care is for resident education. 4Based on systemwide averages for medicine services in RAM Group 4, these figures assume that 61 percent of total education FTEE in ambulatory care is for resident education. |
|||||
TABLE 2 Estimated Production Functions for Ambulatory Care
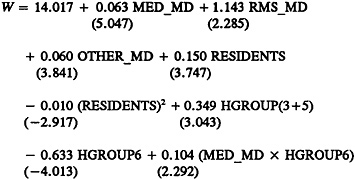
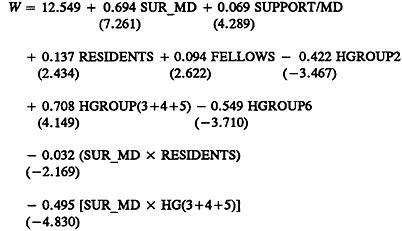
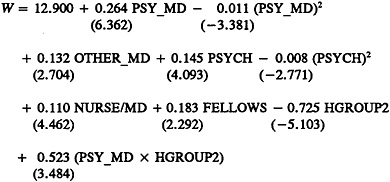
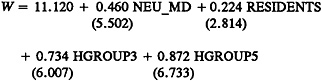
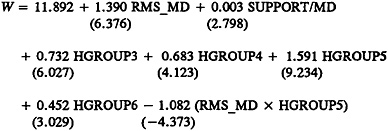

TABLE 3 External Norms—Ambulatory Care
|
Source, Results, and Derivation, if any: |
|
|
VA |
3,500 visits/MD/year |
|
IHS |
5,000 visits/MD/year |
|
AMA Core Survey Med=2.5 visits/hour×40 hour/week ×47.9 week/year×54/60.1 eff factor =4,300 visits/MD/year Sur=3.33 visits/hour×40 hour/week ×47.1 week/year×52.6/58.1 eff factor =5,700 visits/MD/year |
|
|
Overall weighted 2:1 med:surg= |
4,800 visits/MD/year |
|
NYH&HC |
|
|
Med=visits/attendings= |
4,270 visits/MD/year |
|
Sur=visits/attendings= |
6,420 visits/MD/year |
|
Overall weighted 2:1 med:surg= |
4,990 visits/MD/year |
|
Group Health Inc. of St. Paul |
|
|
90 visits/MD/week×45 weeks/year= |
4,050 visits/MD/year |
|
Large HMO Med=1,571 visits/k mem×5,436 k mem ×1/2,412 MD/0.9 OP factor ×40 hour/week/47 hour/week=3,350 visits/MD/year Sur=200 visits/mem×5,436 k mem ×1/883.5 MD/0.6 OP factor ×40 hour/week/47 hour/week=1,750 visits/MD/year |
|
|
Overall weighted 2:1 med:surg= |
2,820 visits/MD/year |
DoD
Standards for the number of visits per MD per year are specified separately by DoD for each of a number of specialists, e.g., internists, neurologists, general surgeons, orthopedic surgeons, neurosurgeons, etc. Further, different standards are specified for teaching versus nonteaching hospitals. Thus, the overall visit rate for a given hospital is a function of the type of hospital as well as the mix of outpatient clinics there. For example, if there were 25,000 general medicine visits annually at a teaching facility, the associated physician requirement would be
|
25,000 visits/year/(540 visits/month/MD ×12 month/year)= |
3.9 MD |
TABLE 4 Ambulatory Care External Norms Applied to Selected VAMCs
|
Computed FTEE1 at |
|||||
|
Source |
Statistic |
Workload/MD |
VAMC I |
VAMC II |
VAMC III |
|
DoD |
visit/MD |
weighted |
27.9 |
36.4 |
35.0 |
|
HMO |
visit/MD |
2,800 |
48.2 |
72.9 |
36.4 |
|
IHS |
visit/MD |
5,000 |
27.0 |
40.8 |
20.4 |
|
AMA |
visit/MD |
4,800 |
28.1 |
42.5 |
21.3 |
|
NYH&HC |
visit/MD |
5,000 |
27.0 |
40.8 |
20.4 |
|
GrHlthInc (St. Paul, Minn.) |
visit/MD |
4,050 |
33.3 |
50.4 |
25.2 |
|
VA Guidelines |
visit/MD |
3,500 |
38.6 |
58.3 |
29.1 |
|
1Excludes psychiatric workload. |
|||||
FIGURE 1 The Staffing Algorithm Development Instrument (SADI) for Ambulatory Care: The Complete Instrument with a Statistical Summary of the Panel's Assessments
INTRODUCTION AND INSTRUCTIONS (Abbreviated)
The purpose of the SADI is to gather the data needed to construct, test, formalize, and enhance the algorithms and rules of thumb for staffing that emerged from prior meetings of each specialty and clinical program panel. The ultimate intention is to develop algorithms which could be applied to estimate staffing requirements at VA medical centers (VAMCs), presumably duplicating the results specialty and clinical program panelists themselves would have derived.
Section A of the SADI requests time estimates, in some cases by workload unit. In other cases, it requests time estimates by major job elements (tasks). These elements had previously been indicated by some panel members as accounting for the bulk of the work of VA physicians in ambulatory care. We seek your estimates of how physician requirements vary with respect to such variables as the volume of patients and the availability of residents and nonphysician practitioners. By systematically varying the levels of workload and personnel, we hope to infer from your numerical responses the implicit formulas you used to relate physician time to these variables, as well as the nature of the relationship between workload and staffing, e.g., linear or nonlinear.
Section B seeks responses to a series of questions about the time spent in activities other than direct patient care.
Instructions: In Section A, for each cell of each table, please estimate the number of physician hours required from the ambulatory care program to deliver good-quality care under the specified circumstances. Section B is self-explanatory.
SECTION A: OUTPATIENT VISITS
EMERGENCY/WALK-INS
Please fill in the average time in hours required by an ambulatory care program staff physician for the typical emergency/walk-in patient or the typical admitting/receiving patient to your VAMC. In responding, please note the presence or absence of residents and nonphysician practitioners, and whether the visit is by a new or returning patient.
Chart 1
|
Physician Time per Visit |
||||
|
Type of Visit |
High |
Low |
Mean |
Median |
|
New Patient Visit No Resident |
1.50 |
0.25 |
0.80 |
0.75 |
|
New Patient Visit With Resident |
0.50 |
0.10 |
0.31 |
0.33 |
|
New Patient Visit With NP or PA |
1.00 |
0.16 |
0.42 |
0.33 |
ADMITTING & RECEIVING
Chart 2
|
Type of Visit |
Physician Time per Visit |
|||
|
High |
Low |
Mean |
Median |
|
|
New Patient Visit No Resident |
1.00 |
0.33 |
0.62 |
0.67 |
|
New Patient Visit With Resident |
0.83 |
0.10 |
0.33 |
0.25 |
|
New Patient Visit With NP or PA |
0.50 |
0.08 |
0.27 |
0.25 |
|
Follow-Up Visit No Resident |
0.75 |
0.25 |
0.36 |
0.33 |
|
Follow-Up Visit With Resident |
0.50 |
0.08 |
0.20 |
0.25 |
|
Follow-Up Visit With NP or PA |
0.50 |
0.08 |
0.20 |
0.16 |
SPECIALTY CLINIC VISITS—MEDICINE
Please estimate the average time in hours required by a staff physician for the typical ambulatory care specialty clinic visit. Note the presence or absence of residents and nonphysician practitioners, and whether the visit is by a new or returning patient.
Chart 3
|
Type of Visit |
Physician Time per Visit |
|||
|
High |
Low |
Mean |
Median |
|
|
New Patient Visit No Resident |
1.50 |
0.67 |
0.98 |
0.88 |
|
New Patient Visit With Resident |
0.50 |
0.08 |
0.25 |
0.22 |
|
New Patient Visit With NP or PA |
0.50 |
0.08 |
0.25 |
0.22 |
|
Follow-Up Visit No Resident |
0.50 |
0.25 |
0.40 |
0.42 |
|
Follow-Up Visit With Resident |
0.16 |
0.08 |
0.11 |
0.09 |
|
Follow-Up Visit With NP or PA |
0.16 |
0.08 |
0.11 |
0.09 |
SPECIALTY CLINIC VISITS—NEUROLOGY
Please estimate the average time in hours required by a staff physician for the typical ambulatory care specialty clinic visit. Note the presence or absence of residents and nonphysician practitioners, and whether the visit is by a new or returning patient.
Chart 4
|
Type of Visit |
Physician Time per Visit |
|
New Patient Visit No Resident |
0.75 |
|
New Patient Visit With Resident |
1.00 |
|
New Patient Visit With NP or PA |
0.58 |
|
Follow-Up Visit No Resident |
0.25 |
|
Follow-Up Visit With Resident |
0.33 |
|
Follow-Up Visit With NP or PA |
0.16 |
SPECIALTY CLINIC VISITS—REHABILITATION MEDICINE
Please estimate the average time in hours required by a staff physician for the typical ambulatory care specialty clinic visit. Note the presence or absence of residents and nonphysician practitioners, and whether the visit is by a new or returning patient.
Chart 5
|
Type of Visit |
Physician Time per Visit |
|
New Patient Visit No Resident |
1.00 |
|
New Patient Visit With Resident |
0.75 |
|
New Patient Visit With NP or PA |
0.50 |
|
Follow-Up Visit No Resident |
0.25 |
|
Follow-Up Visit With Resident |
0.16 |
|
Follow-Up Visit With NP or PA |
0.16 |
SPECIALTY CLINIC VISITS—PSYCHIATRY
Please estimate the average time in hours required by a staff physician for the typical ambulatory care specialty clinic visit. Note the presence or absence of residents and nonphysician practitioners, and whether the visit is by a new or returning patient.
Chart 6
|
Type of Visit |
Physician Time per Visit |
|
New Patient Visit Mental Hygiene No Resident |
1.00 |
|
New Patient Visit Mental Hygiene With Resident |
0.50 |
|
New Patient Visit Mental Hygiene With NP or PA |
0.50 |
|
New Patient Visit Substance Abuse No Resident |
1.00 |
|
New Patient Visit Substance Abuse With Resident |
0.50 |
SPECIALTY CLINIC VISITS—PSYCHIATRY
|
Type of Visit |
Physician Time per Visit |
|
|
New Patient Visit Substance Abuse With NP or PA |
0.50 |
|
|
Return Visit Mental Hygiene |
1.00 |
|
|
Return Visit Medicine Check |
0.50 |
|
|
Return Visit Substance Abuse |
1.00 |
|
|
Group Therapy Session |
0.25 |
(per patient in 2-hour session w/group of 8 patients) |
SPECIALTY CLINIC VISITS—SURGERY
Please estimate the average time in hours required by a staff physician for the typical ambulatory care specialty clinic visit. Note the presence or absence of residents and nonphysician practitioners, and whether the visit is by a new or returning patient.
Chart 7
|
Type of Visit |
Physician Time per Visit |
|
New Patient Visit No Resident |
0.33 |
|
New Patient Visit With Resident |
0.33 |
|
New Patient Visit With NP or PA |
0.25 |
|
Follow-Up Visit No Resident |
0.16 |
|
Follow-Up Visit With Resident |
0.16 |
|
Follow-Up Visit With NP or PA |
0.16 |
SPECIAL PROCEDURES—Within Medicine
We have listed the ambulatory care-based special procedures identified during the panel meeting which should be considered in estimating a staff physician's daily workload. Please estimate the physician time required, in hours, noting the presence or absence of a resident.
Chart 8
|
Special Procedure |
Time per Test Without Resident |
Time per Test with Resident |
||||||
|
High |
Low |
Mean |
Median |
High |
Low |
Mean |
Median |
|
|
Endoscopies |
1.00 |
0.33 |
0.67 |
0.67 |
1.00 |
0.50 |
0.75 |
0.75 |
|
Cardiac Stress Testing |
0.75 |
0.08 |
0.53 |
0.75 |
0.75 |
0.08 |
0.47 |
0.58 |
|
Pulmonary Bronchs |
0.33 |
0.30 |
0.32 |
0.32 |
0.58 |
0.42 |
0.50 |
0.50 |
|
Sigmoidoscopies |
0.75 |
0.13 |
0.38 |
0.25 |
0.58 |
0.22 |
0.43 |
0.50 |
|
Gastroscopies |
0.30 |
0.25 |
0.28 |
0.28 |
0.50 |
0.42 |
0.46 |
0.46 |
|
ECHOs |
0.50 |
0.17 |
0.34 |
0.34 |
0.75 |
0.17 |
0.46 |
0.46 |
|
EMGs |
0.75 |
0.75 |
0.75 |
0.75 |
1.00 |
1.00 |
1.00 |
1.00 |
|
Others: |
||||||||
|
Bone Marrow |
0.50 |
0.25 |
0.38 |
0.38 |
0.58 |
0.33 |
0.46 |
0.46 |
|
Arthrocentesis |
0.58 |
0.58 |
0.58 |
0.58 |
0.33 |
0.33 |
0.33 |
0.33 |
|
Thoracenthesis |
1.00 |
1.00 |
1.00 |
1.00 |
0.33 |
0.33 |
0.33 |
0.33 |
|
Lumbar Puncture |
1.00 |
1.00 |
1.00 |
1.00 |
0.33 |
0.33 |
0.33 |
0.33 |
|
Skeletal Biopsy |
0.50 |
0.50 |
0.50 |
0.50 |
0.25 |
0.25 |
0.25 |
0.25 |
Chart 9
|
SPECIAL PROCEDURES—Within Neurology |
||
|
Special Procedure |
Time per Test without Resident |
Time per Test with Resident |
|
EMGs |
0.75 |
1.00 |
|
Lumbar Puncture |
0.50 |
0.08 |
Chart 10
|
SPECIAL PROCEDURES—Within Surgery |
||
|
Special Procedure |
Time per Test without Resident |
Time per Test with Resident |
|
Endoscopies |
0.67 |
0.50 |
|
Cardiac Stress Testing |
0.33 |
0.25 |
|
Pulmonary Bronchs |
0.67 |
0.50 |
|
Sigmoidoscopies |
0.50 |
0.50 |
|
Gastroscopies |
0.50 |
0.33 |
|
ECHOs |
0.33 |
0.33 |
Chart 11
|
SPECIAL PROCEDURES—Within Psychiatry |
||
|
Special Procedure |
Time per Test without Resident |
Time per Test with Resident |
|
Hypnosis |
1.50 |
1.50 |
|
Amytal Interview |
1.50 |
1.50 |
SECTION B:
NON-PATIENT-CARE TIME
Part 1. The activities listed below generally do not occur every day, but may be time-consuming when looked at over a longer period, such as a week or month. List the time in hours that you would add to each physician's average weekday to allow for the types of non-patient-care-related activities listed below:
Chart 12
|
Assume the amount of research accomplished at this VAMC is: |
High1 |
Medium1 |
Low1 |
|
|
Education of Residents (didactic, classroom, not on the PCA) |
High |
1.00 |
0.50 |
0.50 |
|
Low |
0.25 |
0.17 |
0.00 |
|
|
Mean |
0.49 |
0.30 |
0.16 |
|
|
Median |
0.44 |
0.25 |
0.12 |
|
|
Administration by Chief (time required to manage your whole service by a chief and/or assistant chief) |
High |
4.00 |
4.00 |
4.00 |
|
Low |
1.00 |
0.50 |
0.17 |
|
|
Mean |
2.17 |
2.21 |
1.86 |
|
|
Median |
2.00 |
2.00 |
2.00 |
|
|
Administration by Others (time required per individual— non-chief— physician) |
High |
4.00 |
4.00 |
4.00 |
|
Low |
0.33 |
0.17 |
0.00 |
|
|
Mean |
1.10 |
0.87 |
0.88 |
|
|
Median |
0.75 |
0.50 |
0.38 |
|
|
1Examples of research level by total amount of funding (VA plus non-VA) in FY 1988: High: e.g., VAMC I with $8.8 million in total funding; Medium: e.g., VAMC II with $2.75 million in total funding; Low: e.g., VAMC III with about $176,000 in total funding, |
||||
|
Assume the amount of research accomplished at this VAMC is: |
High1 |
Medium1 |
Low1 |
|
|
Hospital-Related Activities: (mortality and morbidity, Q.A., staff meetings) |
High |
1.00 |
1.00 |
1.00 |
|
Low |
0.10 |
0.10 |
0.10 |
|
|
Mean |
0.60 |
0.63 |
0.55 |
|
|
Median |
0.50 |
0.50 |
0.50 |
|
|
Total Hours per Average Workday |
||||
|
Chief2 |
High |
4.00 |
4.00 |
4.00 |
|
Low |
1.00 |
0.50 |
0.17 |
|
|
Mean |
2.17 |
2.21 |
1.86 |
|
|
Median |
2.00 |
2.00 |
2.00 |
|
|
Other |
High |
6.00 |
5.25 |
5.15 |
|
Low |
1.88 |
1.00 |
0.34 |
|
|
Mean |
3.27 |
3.15 |
2.57 |
|
|
Median |
3.18 |
3.00 |
2.43 |
|
|
1Examples of research level by total amount of funding (VA plus non-VA) in FY 1988: High: e.g., VAMC I with $8.8 million in total funding; Medium: e.g., VAMC II with $2.75 million in total funding; Low: e.g., VAMC III with about $176,000 in total funding, 2Assumes that Chief does not participate significantly in the Education of Residents and Hospital-Related Activities; SADI users may easily modify this assumption. |
||||
Part 2. In order to determine the actual staffing in this hospital, the number of FTEE must be adjusted to allow for CME, research, and any off-time required. What do you believe to be the appropriate percentage of time the “average” (typical) staff (nonresident) member of your service should devote to each of the following categories of non-patient-care-related activities?
Chart 13
|
Assume the amount of research accomplished at this VAMC is: |
High1 |
Medium1 |
Low1 |
|
|
Continuing Education |
High |
10.0 |
10.0 |
15.0 |
|
Low |
3.8 |
2.0 |
5.0 |
|
|
Mean |
7.3 |
6.0 |
7.5 |
|
|
Median |
7.5 |
5.0 |
5.0 |
|
|
Research (off the PCA) |
High |
50.0 |
20.0 |
5.0 |
|
Low |
10.0 |
2.0 |
0.0 |
|
|
Mean |
23.3 |
10.6 |
1.8 |
|
|
Median |
17.5 |
10.0 |
1.0 |
|
|
Vacation, Administrative Leave, Sick Time Other |
10.02 |
10.02 |
10.02 |
|
|
Total Percentage of Time |
High |
70.0 |
40.0 |
28.8 |
|
Low |
28.8 |
17.0 |
15.0 |
|
|
Mean |
40.6 |
26.6 |
19.3 |
|
|
Median |
35.0 |
25.0 |
17.5 |
|
|
1Examples of research level by total amount of funding (VA plus non-VA) in FY 1988: High: e.g., VAMC I with $8.8 million in total funding' Medium: e.g., VAMC II with $2.75 million in total funding; Low: e.g., VAMC III with about $176,000 in total funding. 2The percentages noted for vacation, administrative leave, sick time, and other are based on system guidelines. |
||||
INSTITUTE OF MEDICINE
Committee to Develop Methods Useful to the Department of Veterans Affairs in Estimating Its Physician Requirements
AMBULATORY CARE PANEL
SANKEY V.WILLIAMS (Chair),† Professor of Medicine and Director of Clinical Scholars Program, University of Pennsylvania, Philadelphia
C.RODNEY BAKER, Associate Chief of Staff for Ambulatory Care, Little Rock VA Medical Center, Little Rock, Arkansas
JOHN R.CLARKE, Professor of Surgery and Director, Trauma Center, Medical College of Pennsylvania, Philadelphia
JOHN W.GOLDSCHMIDT, Medical Director (retired), National Rehabilitation Hospital, Washington, D.C.
ELWOOD J.HEADLEY, Deputy Associate Deputy Chief Medical Director for Ambulatory Care, Department of Veterans Affairs, Washington, D.C.
GAETANO F.MOLINARI, Professor and Chairman, Department of Neurology, George Washington University Medical Center, Washington, D.C.
DAVID A.NARDONE, Associate Chief of Staff for Ambulatory Care, Portland VA Medical Center, Portland, Oregon
LOUIS JOLYON WEST, Professor of Psychiatry and Biobehavioral Sciences, School of Medicine, University of California at Los Angeles
Staff: Bobbie J.Alexander, Staff Associate
|
†Member of the study committee. |








































