
LONG-TERM CARE PANEL REPORT1
INTRODUCTION
This panel was established in early 1990 to assist the IOM study committee in developing a VA physician requirements methodology that successfully incorporated the long-term care program at VA medical centers. The panel, consisting of five geriatricians, one orthopedic surgeon, and one nonphysician practitioner, met twice during 1990 and participated in other efforts to advise the study committee on appropriate physician staffing for this clinical program. The chairman of the panel was also a member of the study committee; the panel roster is attached. Additional details describing the analysis process followed by this and the other seven specialty and clinical program panels can be found in the “Overview” to this section of Volume II. The panel roster is attached.
This report summarizes the analyses conducted by the panel and its recommendations to the study committee.
EXPERT JUDGMENT APPROACHES TO DETERMINING PHYSICIAN REQUIREMENTS IN LONG-TERM CARE
The Detailed Staffing Exercise (DSE) Approach
Initial Efforts
A central purpose of the panel's first meeting, held in April 1990, was to help determine whether the expert judgment approach to staffing being developed by the study committee could be applied validly to long-term care.
|
1 |
The initial draft of this report was prepared by Judith L.Teich, Staff Officer to the Long-Term Care Panel during the conduct of the study. This final report was prepared by the editors of this Volume. |
The focus of this analysis was the initial draft of a physician staffing instrument, which required the expert to assess the time (and hence FTEE) required by geriatricians to render patient care, work with residents, and perform other tasks at the VA medical center (VAMC).
To test this approach, staffing instruments were constructed for three actual VAMCs. Each facility was portrayed as consisting of a set of patient care areas (PCAs), where direct patient care and resident training occur. Among these PCAs were two assumed to be focal points for geriatricians: the nursing home and the intermediate care ward(s).
For each PCA, data were presented on the volume of patient workload expected, the number of residents available, and the overall availability of nursing and support staff. The critical question with respect to every PCA was, how much geriatrician time is required, in total, to meet these VA mission-related demands in the course of a typical workday? Each PCA was analyzed, in turn, and total long-term care physician FTEE for the facility was computed. Additional questions at the end of the instrument elicited FTEE requirements for weekend coverage, special procedures, and non-VA physician consultants.
In the course of this first meeting, the panel reached several initial conclusions about the assumptions that should underlie the development of subsequent physician staffing instruments:
-
The instrument should be refined to capture more accurately the reality of staffing in the LTC PCAs. In particular, the overall accuracy of physician time assessments could be improved, it was suggested, if the instrument incorporated some type of algorithm for distinguishing among the specific tasks performed in the PCAs: admission work-up, rounds, discharge, etc.
-
More patient-specific information should be provided for each PCA: the average length of stay (LOS), the admission rate, the discharge rate, and the relative proportion of new patients in the total census.
-
Long-term care units should be staffed by numbers of physicians of different specialties; for example, in order to provide comprehensive care, physicians in rehabilitation medicine, surgery, gastroenterology, and psychiatry all should have input into the care of long-term patients. The amount of time contributed on long-term care units by physicians in each of these specialties needs to be addressed.
At this first meeting the panel also reviewed and evaluated the initial versions of the empirically based physician staffing model.
Following the first round of meetings for all eight specialty and clinical program panels, there was convened (in May 1990) Joint Meeting I involving the study committee, the data and methodology panel, and the VA liaison committee. Progress to date on both the expert judgment and empirically based model approaches was evaluated. After reviewing the reports submitted by each panel, the study committee recommended that work proceed on developing a more internally consistent and comprehensive instrument for determining physician requirements by expert judgment. A broadly similar approach should be adopted by each panel, but the instrument for each specialty or program area should be tailored to its specific characteristics.
DSE: Overall Rationale
For the long-term care panel's second meeting, held in August 1990, three additional VAMCs (denoted here and in the committee report [Volume I] as VAMCs I, II, and III) were analyzed using a revised version of the initial staffing instrument. This new instrument—later termed the Detailed Staffing Exercise (DSE) —was developed on the basis of the panel's critique delivered at the first meeting, plus general instructions from the study committee at the conclusion of Joint Meeting I. As before, each DSE was specific to an actual VAMC. This revised instrument described each PCA in greater detail than before, including more specific information on the VA patient population (e.g., admission rate, length of stay, and DRG mix).
In general, the underlying concept behind the DSE is to provide information in sufficient detail about the VAMC that the respondent can assess physician staffing requirements almost as if he/she were reviewing data at the facility.
Instructions and Assumptions
To illustrate how the DSE works, a completed version of the instrument is presented as Exhibit 1 of the “Overview” to this section of Volume II. This DSE is nearly identical structurally to the one constructed for long-term care.
As indicated in Exhibit 1 of the Overview, each DSE has an A and B section. Section A elicits the amount of time, in hours, required to provide quality care for individual PCAs of the VAMC. For each PCA, information is provided on the volume and DRG mix of workload, number of residents by postgraduate year, number of nonphysician practitioners (e.g., nurse practitioners, physician assistants), and general information about the adequacy
of nursing and support staff. Section B focuses on physician activities not addressed in Section A, such as night and weekend coverage, non-patient-care-related activities off the PCA, and leaves of absence.
The Panel Responds
Before the second meeting, panelists were mailed DSEs for VAMCs I and II; these were completed independently and returned prior to the meeting. The staff compiled these results on a spreadsheet showing the high, low, mean, and median responses.
At the second panel meeting, these DSEs were discussed thoroughly to determine whether panelists were using similar assumptions and to allow members to discuss the underlying reasoning behind these calculations.
Following this, the panelists were asked to reassess physician requirements in medicine at VAMCs I and II, again working independently.
Subsequently, a third exercise, constructed for VAMC III, was distributed and the panel worked as a group to estimate staffing requirements. Following the assessment, the actual CDR numbers for VAMCs I, II, and III were displayed for comparison. During the group discussion, the panel was asked to reflect on whether certain “rules of thumb ” were used (perhaps implicitly) to help quantify staffing requirements.
Interim Assessment of Expert Judgment Staffing Approaches
The panel, beginning at its first meeting, discussed alternative and more compact formats for obtaining estimates of the time required by LTC physicians to perform specific tasks in the PCAs. One of the panel's early proposals can be summarized as follows:
Possible Algorithm for Long-Term Care Physician Staffing
|
Type of Unit |
||||
|
Nursing Home Care Unit |
Geriatric Assessment |
Geriatric Psychiatry |
Domiciliary |
|
|
I. Direct Patient Care Activity |
||||
|
Admissions/ Evaluation |
(For each type of unit and activity combination, the respondent would estimate the required number of physician hours per week.) |
|||
|
Discharge Rounds Team Meetings Family Conferences |
||||
|
II. Non-Patient-Care Activity |
||||
|
Teaching/Research Administration |
||||
|
If Medical Director If not Medical Director |
||||
Also discussed at the panel meetings were possible questionnaire formats for estimating the amount of physician time from each VA specialty required for consultation on long-term care units. Panel members suggested a matrix (shown below) as one possible means of addressing this issue. It was also recommended that if such expert judgment-based estimates were obtained, they should be compared with the actual FTEE estimates for such consultations, as found in the VA's cost distribution report. In addition, estimates by other specialty panels of the amounts of time which they feel their physicians need to contribute to long-term care units might be usefully compared with what LTC physicians estimate to be the appropriate amount of consultation. Routine input from various specialties to long-term care should be considered an important part of any future model. How this data collection might proceed is illustrated in the following skeletal table:
Recommended Physician Input from Various Specialties
Number of MD Hours per Weekday Required from:
|
Med. |
Surg. |
Psych. |
Rehab. Med. |
Neuro. |
Other1 |
|
|
Illustrative LTC Unit: |
||||||
|
Geriatric Medicine Beds=22 ADC=19 LOS=27 |
||||||
|
Intermediate Care Unit Beds=33 ADC=27 LOS=27 |
||||||
|
NHCU (I) Beds=78 ADC=74 LOS=109 |
||||||
|
NHCU (II) Beds=25 ADC=22 LOS=109 |
||||||
|
1To be specified by the respondent. |
||||||
At its second meeting, the panel also developed a simple topology to help it analyze the time required by LTC physicians in PCAs other than the nursing home and intermediate care:
-
Geriatric consultations for management only
-
Without NPP
-
With NPP
-
-
Assessment/screening for long-term care admissions
-
Without NPP
-
With NPP
-
These activities constitute an important part of the long-term care physician's responsibilities. The amount of time needed for each type of activity should be considered in assessing overall physician requirements for long-term care.
In addition, it was emphasized that the nature of an intermediate care PCA may vary markedly from facility to facility. This PCA may consist, alternatively, of:
-
Distinct units where the LTC physician provides primary care; or
-
Distinct units where the LTC physician has a consultative role only; or
-
No distinct units (beds dispersed throughout other services) and the LTC physician has a consultative role.
Given these discussions, the LTC panel was subsequently pleased to see the study committee propose an expert judgment format such as SADI, which reflects the spirit of the panel's discussions.
The Staffing Algorithm Development Instrument (SADI) Approach
SADI: Overall Rationale
Following the second round of panel meetings, the study committee initiated a set of postmeeting activities to assist the specialty and clinical program panels in arriving at consensus positions regarding the most appropriate methodology for VA physician staffing. These recommendations would be regarded as advisory to the committee.
A central feature of these activities was the introduction of the Staffing Algorithm Development Instrument (SADI). The overall purpose of the SADI was to help test, build upon, and ultimately strengthen the rules of thumb for staffing that emerged from the second meetings of all eight panels. It represents an alternative, more compact means to derive physician requirements, by specialty or program, for any given VAMC.
Instructions and Assumptions
Like the DSE, the SADI has two sections, A and B, which focus on patient care and non-patient-care activities, respectively. In Section A, the respondent is asked to estimate the amount of physician time required to complete a number of patient care functions and tasks under varying assumptions about the availability of residents and nonphysician practitioners. In Section B, the respondent must determine the amount of physician time that should be allocated to research, classroom instruction, continuing education, administration, and leaves of absence. To derive physician requirements for a given VAMC, the estimated physician hours for patient care and non-patient-care activities are summed, then converted to FTEE under the assumption that 40 hours per week translates into one FTEE.
Presented in Figure 1 of this report is the long-term care SADI, complete with the panel 's median estimates for physician task times. A detailed and self-contained, illustration of how the SADI can be applied to determine the number of physicians required at a given VAMC is found in Exhibit 3 of the “Overview” to this section of Volume II. This example happens to focus on internist requirements at VAMC I; the application of SADI to determine long-term care FTEE at a given facility proceeds in a virtually identical fashion. A careful study of the example reveals the type of facility-specific data needed to implement any SADI. Although the information requirements of the DSE are greater, both of these expert judgment approaches require data (e.g., on frequency of consults across PCAs) not presently collected in the VA system.
EMPIRICALLY BASED APPROACHES TO DETERMINING PHYSICIAN STAFFING FOR THE LONG-TERM CARE PROGRAM
Of the 14 patient care areas defined by the study committee, two were specifically designated as “long-term care”: the nursing home and the intermediate care areas of the VAMC. In its two meetings and a follow-up conference call, the panel was presented alternative specifications of production function models estimated for each of these two PCAs.
Table 2 shows the final versions of these estimated models, as derived in cooperation with the study's data and methodology panel. Each PF model depicts the workload produced (per time period) in that LTC PCA as a function of the amount of specialty-specific physician FTEE and nonphysician FTEE
caring for patients in the PCA; in the intermediate care PCA, the VAMC's RAM Group status, reflecting both hospital size and degree of affiliation, is also an important factor in accounting for differences in workload productivity across the sample.
Workload in each PF is defined as the total Resource Utilization Group Weighted Work Units (RUGWWUs) generated in the PCA during the fiscal year. This output variable is based, as suggested, on the well-known Resource Utilization Group (RUG) methodology for indexing the expected amount of patient care (largely nursing care) required by a patient. In these statistical models, total RUGWWU is defined as the sum of the medicine, psychiatry, and rehabilitation medicine RUGWWUs generated in the PCA during the fiscal year.
As illustrated in chapter 4 of the committee report (Volume I), each PCA-specific model can be used to derive alternative combinations of specialty-specific physician FTEE that are consistent with meeting the patient workload expected in that PCA. However, neither the nursing home nor intermediate care model can be used to derive the amount of FTEE required by long-term care physicians in the VAMC 's 12 other patient care areas. Thus, for example, these PFs do not account for physician involvement in the geriatric evaluation units (which are, in fact, analyzed as part of the inpatient medicine PCA). Nor do they incorporate physician time spent in consultations on inpatient wards or in ambulatory clinics.
In sum, the PF models provide an in-depth look at workload production in the nursing home and intermediate care wards, but do not encompass all patient care activities that fall properly under the purview of the long-term care program at the VAMC (e.g., adult day health care).
No inverse production functions have been estimated for long-term care. As specified in this study, the IPF is specialty-specific (e.g., medicine, surgery, psychiatry); and the VAMC as a whole, not the PCA (in the VAMC), is the basic unit of observation. On the other hand, the long-term care program is multidisciplinary and concentrated largely in certain PCAs within the VAMC.
Nonetheless, the influence of long-term care workload on VA physician requirements is reflected in each IPF—to the extent the independent variable RUGWWU is contained in the equation as a (statistically significant) predictor of physician FTEE required for patient care and resident education in the associated specialty.
PHYSICIAN STAFFING RESULTS FROM APPLICATION OF EMPIRICALLY BASED AND EXPERT JUDGMENT APPROACHES
In Table 1 are alternative estimates of physician requirements for long-term care at VAMCs I, II, and III in FY 1989, as derived from: the VA 's cost distribution report (CDR), the PF variant of the empirically based physician staffing models, the DSE (from the second panel meeting), the SADI (in both its “pure” and modified formats), and a mail survey of panel members conducted just prior to Joint Meeting II (held September 7–9, 1990).
In interpreting these results, two important considerations must be kept in mind. First, because the sample of facilities is so small, one must be very cautious in drawing conclusions from the table about the appropriateness of current physician staffing in long-term care across the VA system. The main purpose of studying these VAMCs in detail was not to draw inferences about whether they were appropriately staffed, but to test the feasibility and appropriateness of alternative approaches for calculating physician requirements.
Second, the FTEE estimates derived from the CDR and the PF model are for total physician requirements for the two PCAs, nursing home and intermediate care, that the study defined early on as making up “long-term care. ” In particular, these estimates do not include physician FTEE for extended care and geriatric activity not occurring in these two PCAs. On the other hand, the four expert judgment-oriented estimates for each VAMC are for the total amount of FTEE for geriatricians at the facility (across all PCAs). Given the structure of both the long-term care DSE and SADI, these estimates do not include FTEE for consults by nongeriatricians to the nursing home and intermediate care PCAs. Hence, by definition, they are not comparable to those from the CDR and PF model.
Both the DSE and the SADI (not modified) yield total physician FTEE estimates that are relatively close to the median of panelist responses to a mail survey conducted in the fall of 1990. In fact, the DSE estimates are closer to these medians than are the SADI results. However, the panel believes that for application across the VA system, an expert judgment process based on the SADI would be less costly and more administratively efficient than one based on the DSE.
EXTERNAL NORMS
Data-Gathering Activities
Following the first panel meeting, a memo was sent to members requesting suggestions for specific non-VA long-term care facilities that could provide an appropriate “yardstick” for staffing. Private facilities that were suggested and then contacted by staff included:
-
North Shore University Hospital, Center for Extended Care and Rehabilitation, Manhasset, NY
-
Hebrew Home of Greater Washington, Washington, DC
-
Levindale Hebrew Geriatric Center and Hospital, Baltimore, MD
-
Bethesda Nursing Home, Minneapolis/St. Paul, MN
-
Northridge Nursing Home, Minneapolis/St. Paul, MN
-
Hennepin County Medical Center, Minneapolis/St. Paul, MN
-
Methodist Hospital, Hospital-Based Home Care Unit, Minneapolis/St. Paul, MN
-
Langton Lakes Nursing Home, Dementia Unit, Minneapolis/St. Paul, MN
Staff also contacted the American Association of Homes for the Aging, which provided information from the State Operations Manual on Provider Certification (U.S. Department of Health and Human Services, Health Care Financing Administration, September 1989) regarding regulations for Skilled Nursing Facilities (SNFs) and Intermediate Care Facilities (ICFs). With regard to physicians, the Interpretive Guidelines for Nursing Facilities and ICFs state that, “the resident must be seen by a physician at least once every 30 days for the first 90 days after admission, and at least once every 90 days thereafter.” For SNFs, the Guidelines indicate that, “the resident must be seen by a physician at least once every 30 days for the first 90 days after admission, and at least once every 60 days thereafter.”
Several of the facilities provided a comprehensive picture of their services and staffing, which could be used as a comparison with VA long-term care facilities. North Shore Hospital's Center for Extended Care and Rehabilitation, for example, has an average length of stay of 50 days and an average daily census of 186 patients. It is physically adjacent to the hospital, and in this way is more similar to most VA nursing home care units than most private community nursing homes, which are freestanding. The center has a medical director described as being full-time; however, he is also the chief of the
hospital's Division of Geriatric Medicine. There are four other physicians in the facility, also described as full-time, despite the fact that they may have some responsibilities in the hospital and in outpatient settings. The five MDs share coverage for nights and weekends at the center. The overall ratio of patients per physician would be 37.2; however, since these physicians may not actually be full-time, the ratio of patients to MD FTEE (when properly measured) may be somewhat higher.
The Hebrew Home of Greater Washington is a 548-bed comprehensive care facility; the facility description states explicitly that “ each full-time staff physician has responsibility for approximately 120 [nursing home] residents.” The Hebrew Home has an average of 260 admissions per year, indicating a significantly longer average length of stay than North Shore's Center, and, presumably, a patient population that requires a less intensive type of care.
A third facility, the Levindale Hebrew Geriatric Center and Hospital, has 283 beds and five FTEE geriatricians, plus one FTEE physiatrist. One physician is a full-time medical director; two are assigned to the 243 nursing home beds, and two are assigned to a 40-bed chronic hospital unit, which provides subacute (or higher than skilled nursing) care. Fifteen beds in the nursing home are allocated to short-stay rehabilitation, and 12 others are allocated to geropsychiatric rehabilitation. The beds-per-physician FTEE ratio for the nursing home is 121.5; for the chronic hospital unit, it is 20 beds per physician (excluding the rehabilitation physician). This facility, as well as the North Shore Center and the Hebrew Home, is affiliated with medical schools and trains medical students, residents in family medicine and rehabilitation, and geriatric fellows. A summary of information from these facilities is displayed in Table 3.
Attempts at gathering information from other long-term care facilities suggested by panel members were less successful. For example, five facilities in the Minneapolis area were contacted; of these, three were private nursing homes with no staff physicians except for either a full-time or part-time medical director. Patients in both facilities are cared for by private physicians from the community, making it very difficult to estimate the amount of physician FTEE available to patients. Another site suggested was a geriatric teaching unit run by the Department of Medicine at the Hennepin County Medical Center. This, however, is a short-term unit with an average length of stay of 5.2 days, and is run by the nursing service as a case management model. The extended care department of that hospital has no beds of its own, but is responsible for managing the care of approximately 1200 nursing home patients who reside in approximately 45 private nursing homes in the community. Contacts with these facilities did not, therefore, yield meaningful comparisons.
Information on one special type of unit—hospital-based home care (HBHC) —was also elicited from one private facility in Minneapolis. This program, which has an average daily census of 230 patients, is staffed totally by nurses, under the supervision of the patients' private physicians. There is a medical director, who contributes approximately 8–10 hours per month, in a strictly advisory capacity. In this instance, as well as in the case of the private nursing homes, the nature of the physician staffing does not allow for a meaningful comparison with VA extended care facilities, which have their own paid medical staffs; however, one useful piece of information was supplied by this HBHC program. The nursing administrator estimated that approximately 50% of the patients are seen by their private physicians once a month or once every two months, for a visit of about 30 minutes. Another 45 % of the patients, whose problems are more critical, are seen about two to three times per month by their physicians, for visits of similar duration. The remaining 5 % of patients are seen only about once a year by a physician, for monitoring only.
Internal Norms: Differences in Staffing among VA Facilities
The Detailed Staffing Exercises (DSEs) completed by panel members in conjunction with the two meetings of the long-term care panel served to highlight the fact that, in addition to possible differences in staffing patterns between the VA and private sector extended care facilities, there may be differences among VA facilities with regard to their long-term care physician staffing. For example, the following results emerged from a simple comparison of patients per total physician FTEE allocated to LTC in the nursing home care units, geriatric evaluation units, and intermediate medicine units, respectively, for the three facilities used in the staffing exercises at the second panel meeting:
|
VAMC I: (affiliated/ tertiary) |
Total LTC ADC |
= |
36.0 |
|
Intermed Med |
= |
7.0 |
|
|
NHCU |
= |
29.0 |
|
|
Long-term care FTEE (as reported by VAMC) |
= |
2.0 |
|
|
Inpts per LTC FTEE |
= |
18.0 |
|
|
Long-term care FTEE (from CDR) |
= |
0.7 |
|
|
Inpts per LTC FTEE |
= |
51.4 |
|
|
VAMC II: (affiliated/ tertiary) |
Total LTC ADC |
= |
142.0 |
|
Intermed Med |
= |
46.0 |
|
|
NHCU |
= |
96.0 |
|
|
Long-term care FTEE (as reported by VAMC) |
= |
3.0 |
|
|
Inpts per LTC FTEE |
= |
47.3 |
|
|
Long-term care FTEE (from CDR) |
= |
1.6 |
|
|
Inpts per LTC FTEE |
= |
88.8 |
|
|
VAMC III: (unaffiliated/ long term) |
Total LTC ADC |
= |
114.0 |
|
Intermed Med |
= |
73.0 |
|
|
NHCU |
= |
41.0 |
|
|
Long-term care FTEE (as reported by VAMC) |
= |
2.0 |
|
|
Inpts per LTC FTEE |
= |
57.0 |
|
|
Long-term care FTEE (from CDR) |
= |
3.3 |
|
|
Inpts per LTC FTEE |
= |
34.5 |
Panel members had also suggested that staff contact VAMCs (indicated here as VAMC A and B) that are generally recognized within the system to be well organized and well staffed with regard to their extended care services.
VAMC A reported a total of 5.75 physician FTEE for its geriatrics and extended care service. Of these, 2.0 FTEE are assigned to the 239-bed nursing home, yielding a ratio of 119.5 NHCU beds per FTEE. The service also has
an HBHC unit with an ADC of 55–65 patients; this unit is staffed by 0.25 physician FTEE, three full-time nurse practitioners, and one full-time nurse coordinator. There is a 40-bed intermediate care unit, staffed by 0.5 physician FTEE and 3.0 FTEE nurse practitioners, as well as a 16-bed geriatric evaluation unit; it has 0.3 physician FTEE assigned to it from the extended care service and is jointly administered with the medicine service of the hospital. The nursing home care unit is accredited by JCAHO and adheres to its minimum standard of one physician visit per patient per month.
VAMC B reported it has an HBHC unit with an ADC of 62 patients; this is staffed by a 0.5 FTEE medical director (a physician), and has input of approximately 10 hours per week from residents and fellows. The medical director and the trainees are directly involved in patient care and make home visits. The HBHC unit also has 4.0 FTEE in nursing, as well as 1.0 FTEE occupational therapist, 0.5 FTEE dietitian, 0.5 FTEE coordinator, and 0.5 FTEE social worker.
As can be seen in the staffing figures for VAMCs I, II, and III displayed in the text above, the ratio of inpatients per physician FTEE varies considerably across the VAMCs, as it does between similar facilities in the private sector. The reasons for this variation are not clear and may be related to differences between facilities; in the acuity and severity of illness of the patient population; with the definition of a physician FTEE; with the mix of other staffing, particularly nurse practitioners and physician assistants; or with other, as yet unidentified, factors.
It is interesting that VAMCs I, II, and III all have lower patient-to-physician ratios (i.e., more long-term care physicians per patient, as reported directly by the facilities) than, for example, VAMC A, which was specifically pointed out by VA panel members as being well staffed. The ratio of beds per physician FTEE in the nursing home care unit at VAMC A—120 beds/physician—was cited as an explicit standard by the Hebrew Home of Greater Washington. The VA's own staffing guidelines from 1965 use the figure of 100 beds per physician as an explicit standard for nursing home care units.
Comparisons of Nursing Home Staffing in VA and non-VA Facilities
Table 4 shows the results from applying the staffing ratios cited above (for North Shore, the Hebrew Home, Levindale, VAMC A, and the 1965 VA
standards) to derive the implied levels of physician FTEE required for the nursing home PCA at VAMCs I, II, and III. (Recall tha VAMC III's data pertained to HBHC.) These projected staffing figures are compared with the current physician staffing levels, as reported in the facilities' CDR.
Overall, the actual NHCV physician staffing at both VAMC I and II was roughly at the median of the five norms-based calculations. For VAMC III, four of the five norms lead to a lower required physician FTEE than reported at this VA facility in FY 1989; but this certainly does not suggest significant over-staffing.
The Utility and Limitations of External Norms
Several important caveats should be kept in mind when considering these external norm data. First, these numbers and the ratios derived from them might be better regarded as patterns rather than norms; that is, in most cases, they do not represent explicit standards consciously developed by an organization or agency, but rather reflect existing staffing as it has evolved over time.
Second, since there is no universally accepted operational definition of an FTEE, these external staffing numbers should not be taken to represent “hard” data, but rather rough approximations of levels of staffing. It is not clear, for example, to what extent so-called “full-time ” physicians in a given facility may have other, outside responsibilities (e.g., the full-time physicians at North Shore are also responsible to the Geriatric Service in the adjacent acute-care hospital). Further, while statistics on admissions, beds, outpatient visits, etc., are usually available, comprehensive staffing data rarely exist at these facilities in a written or computerized form. Rather, most of the data above were obtained from telephone conversations with one or more persons at each facility, increasing the risk of reporting error. For this reason, it would appear that they are subject to certain inaccuracies or ambiguities.
CONCLUSIONS
As a framework for determining VA physician requirements in long-term care, the panel endorses a specification of the Reconciliation Strategy that can assess the FTEE needed for all extended care and geriatric services, not simply for nursing home and intermediate care beds. Regarding the components of the strategy, the panel recommends the following:
Patient Care, Resident Education, and Administration
For these activities, FTEE should be derived from expert judgment approaches rather than the EBPSM, for several reasons.
First, the PF variant of the EBPSM allows one to infer physician requirements for the nursing home and intermediate PCAs, but those geriatric and extended care activities occurring on other PCAs are excluded from what the model calls “long-term care.” For example, geriatric evaluation units (GEUs) are analyzed as part of the inpatient medicine PCA.
Second, because the IPF is specialty specific and the long-term care (LTC) program is multidisciplinary, there is no IPF that applies to LTC. [However, the effect of nursing home and intermediate care workload on physician requirements is recognized in each IPF through the independent variable RUGWWU (Resource Utilization Group Weighted Work Units).]
Third, an expert judgment model built around the SADI offers a flexible approach for evaluating physician FTEE requirements for all extended care and geriatric services. The current LTC SADI is designed to capture the FTEE of physicians whose dominant commitment is to the VAMC's LTC “service.” But it would be straightforward to extend the SADI to include the FTEE of all physicians, regardless of specialty or dominant commitment, who devote time to extended care or geriatrics. Thus, the important role of psychiatrists and rehabilitation medicine physicians would be acknowledged.
Research
The amount of FTEE earmarked for research should be empirically driven, that is, based on a facility- or specialty-specific analysis of the existing relationship of research funding and other indicators of research activity to research FTEE. Hence, these research FTEE allocations would vary by facility and likely be a function of the facility' s affiliation status.
Continuing Education
The panel recommends that there be a minimum amount of FTEE set aside for continuing education, perhaps pegged to state medical licensure requirements. In addition to this baseline allocation, the panel recommends that additional FTEE for continuing education be allowed for physicians in highly
affiliated VA facilities or where significant research is ongoing. These physicians should be expected to present research findings and report on program developments at national meetings of the specialties in which they hold academic appointments. The effect of this allowance on total FTEE requirements should be estimated according to the level of affiliation and the amount of research funding at each facility.
Leaves of Absence
As a baseline across the system, the percentage of total FTEE allocated to leaves of all type should be set at a uniform level; the panel concurs with the committee that a reasonable benchmark is the amount of annual leave. However, there should be a mechanism to allow for leave days beyond this baseline for facilities that participate heavily in external research and education activities. An index for the latter would be the facility's affiliation status.
Purchased Coverage for Nights and Weekends
Assuming adequate support from medicine and the other services, no additional FTEE are required.
Consulting & Attending and Without-Compensation Coverage
Assuming the VAMC is appropriately staffed with VA physicians, there is, almost by definition, no need for additional C&A and WOC FTEE to meet basic needs. The panel notes, however, that these non-VA physicians can serve to improve the quality of patient care.
External Norms
For three VAMCs the panel computed what physician FTEE would have been had each been staffed with the same intensity, in turn, as three private sector nursing homes, another VA nursing service, and as suggested by the VA's own rough guidelines published in 1965. The overall finding was that
none of the three VAMCs was significantly overstaffed or understaffed (in FY 1989).
The panel believes that these analyses suggest that staffing norms can be usefully applied in LTC. But two caveats should be noted. First, except for the old VA guidelines noted, these “norms” are simply a reflection of the staffing behavior of LTC units as they have evolved over time. Second, there is no universally accepted operational definition of an FTEE, so that these workload/FTEE ratios computed for non-VA facilities must be carefully interpreted. It is not clear, for example, to what extent a “full-time” physician in a given private facility has other outside responsibilities occupying significant portions of the work week. In general, it appears that private LTC facilities collect good workload statistics (e.g., admissions, patient days), but physician staffing data are less likely to be recorded in a standardized fashion.
Overall Adequacy of Physician Staffing in the VA
Given the small number of VAMCs examined in detail, the panel could make no determination about the overall appropriateness of staffing for LTC in the VA. To make a global determination, it would be necessary to apply the SADI across the VA system. The panel urges that this be done, and in a way that is sensitive to particular concerns that arise in LTC. For example, the SADI must indicate the extent to which physicians assigned to LTC (rather than medicine) have primary responsibility on intermediate medicine units, since this would have a major effect on the amount of time that LTC physicians must spend on these units. Similarly, the SADI must specify clearly whether physicians have a primary-care role, or a consultative/advisory role, in the operation of VA-hospital-based home care (HBHC) units.
Other Points
The panel feels that there are at least seven issues requiring careful consideration as the VA continues to refine the proposed physician staffing methodology.
-
Physician staffing requirements were not reviewed for HBHC because, under the current VA system, the program is implemented by nursing with little direct physician involvement for patient care. In the non-VA home
-
care field, the push toward decreasing utilization of higher cost inpatient services has shifted the care of many patients to the community. This trend will be seen in the VA as well for the elderly, and perhaps, for AIDS patients. These veterans will have a higher acuity of illness than those currently being serviced by HBHC, and the rate of patient turnover will increase. Because of this, physicians will be more directly involved in the following activities: (a) screening for enrollment into HBHC, (b) patient care planning, (c) multidisciplinary care management, (d) periodic in-home assessment, and (e) evaluation of patient progress and potential for discharge from HBHC to other levels of care.
Rather than contenting itself with current levels of physician activity in HBHC, the VA should review external VA norms to determine requirements for physician involvement in the future. The American Academy of Home Care Physicians will be a significant resource for this endeavor.
-
Geriatric psychiatry is an area requiring particular attention. Although a high percentage of nursing home patients have secondary diagnoses involving mental disorders, psychiatrist time allocated to nursing home units appears to be disproportionately low. Additional analyses are required to determine whether this is merely a feature of the VA FTEE reporting system, or reflects a surprising lack of involvement of psychiatry in the treatment of these patients. (A similar question arises in other areas where geriatric psychiatry would be expected to play a significant role, e.g., HBHC, Adult Day Health Care, and Geriatric Evaluation and Management Units.)
-
Of the LTC workload measures available to the panel, the one most closely correlated with patient acuity appears to be the RUGWWU scores, which are derived from the well-known Resource Utilization Group (RUG) methodology. Nonetheless, the panel strongly recommends that the VA determine the degree to which RUGWWU scores are predictive of physician, rather than nursing, activity. If the correlation is deemed inadequate, the search for better workload variables should continue.
-
With regard to intermediate medicine units, the panel suggests that there are at least three different types of arrangements, and that the particular arrangement has an impact on the use of the physician and the amount of time that he or she may need to spend on the unit. These types of arrangements are:
-
Distinct, identified units where the LTC physician is responsible for providing primary care;
-
Distinct, identified units where the LTC physician has a consultative role only; and
-
Not an identified or distinct unit, but an arrangement in which intermediate care beds are dispersed throughout other services and in which the LTC physician has a consultative role only.
-
With regard to training issues, the panel suggests that the involvement of medical students on long-term care units be explored in detail. For example: What is the usual number of students doing clerkships on a long-term care unit at one time? How long do such clerkships usually last? In how many VA facilities, and how often, are such clerkships operational? What demands does this place on long-term care physicians with respect to teaching and supervision? Are house staff allocations based adequately on the LTC needs of the VAMC? These same questions may need to be explored in relation to residents in different postgraduate years. Further, it is important to clarify the actual average time involvement of fellows assigned to long-term care units; e.g., if a fellow is assigned “full-time” to a unit, how much time does this mean he or she generally spends per day on the unit?
-
Another concern of the long-term care panel is the importance of nonphysician practitioners (NPPs) in the provision of LTC services. There is a need to distinguish between different responsibilities and functions of nurse practitioners relative to physicians assistants, and the differential impact of each of these types of NPPs on physician time requirements. (The surveys conducted by the nonphysician practitioners panel, discussed elsewhere in Volume II, do shed some light on these questions.) The panel also stresses that all NPPs should have maximum flexibility in all long-term care activities, in order to ensure optimal use of physician time.
-
One final and major point: Further iterations of the LTC SADI should have the capability of assessing physician time requirements for all of the following activities, defined by the VA's Office of Geriatrics and Extended Care as falling within its purview:
Nursing home care (VA, community, state home)
Domiciliary care (VA, state home)
State home hospital care
Hospital-based home care
Community residential care
Adult day health care
Hospice/palliative care
Respite care
Geriatric Research, Education and Clinical Centers
-
-
Geriatric Evaluation and Management Units
Dementia and Alzheimer's disease initiatives
Information and referral services or activities.
Hence, the scope of “long-term care” activities in the overall physician requirements methodology would be operationally defined in an appropriate fashion and could encompass the growing role of physicians in such programs as HBHC.
It is important to distinguish between geriatrics and long-term care, and to articulate the relationship between the two—demand for long-term care is not generated exclusively by geriatric patients, and geriatricians have responsibility for patients outside the long-term care setting.
Final Remarks
The panel urges the VA to adopt a form of Reconciliation Strategy that uses expert judgment rather than statistical models to determine the amount of physician FTEE required for patient care, resident education, and administration within the LTC program of a VAMC. The remaining components of FTEE discussed above should be determined through a combination of empirically based and expert judgment based approaches, as indicated.
-
TABLE 1 Estimates of Physician Requirements in Long-Term Care at Three VAMCs
|
A. Total FTEE |
||||||
|
VAMC |
CDR1 |
PF1 |
DSE2 |
SADI2 |
||
|
VAMC I |
0.7 |
0.3 |
2.3 |
3.2 |
1.3 |
2.5 |
|
VAMC II |
1.6 |
1.3 |
2.7 |
3.1 |
2.4 |
2.5 |
|
VAMC III |
3.3 |
3.1 |
3.0 |
3.3 |
2.5 |
3.0 |
|
B. Direct Care Plus Resident Education FTEE Only |
||||||
|
VAMC |
CDR1 |
PF1 |
DSE2 |
SADI2 |
||
|
VAMC I |
0.6 |
0.2 |
1.5 |
0.5 |
0.5 |
N.A. |
|
VAMC II |
1.6 |
1.3 |
1.7 |
1.6 |
1.6 |
N.A. |
|
VAMC III |
3.3 |
3.1 |
1.2 |
2.1 |
2.1 |
N.A. |
|
1Does not include FTEE for consults by geriatricians to the non-LTC patient care areas, i.e., all PCAs except nursing home and intermediate care. 2Does not include FTEE for consults by nongeriatricians to nursing home and intermediate care PCAs. 3Derived by replacing the SADI-based estimates for non-patient-care activities with estimates based on the DSE; all FTEE for patient care and resident training in the PCAs continue to be derived from the SADI. 4Panel median response to the question, posed by mail survey in September 1990, of what is the overall preferred physician FTEE level at each VAMC. To provide a context for the response, each panel member was presented a summary of the physician FTEE level emerging, alternatively, from the CDR, from both empirically based approaches (as applicable), and from both expert judgment approaches. |
||||||
TABLE 2 Estimated Production Functions for Long-Term Care
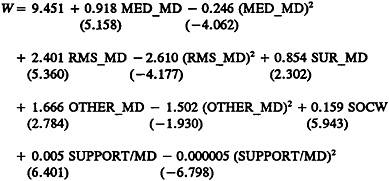
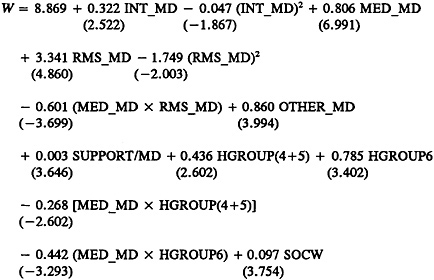
TABLE 3 External (Non-VA Staffing) Norms
|
North Shore Hospital Center for Extended Care |
Hebrew Home of Washington |
Levindale Geriatric Center |
|
ADC=186 Physician FTEE=5.01 |
Beds=548 Physician FTEE=4.5 |
Beds=243 (NH) Physician FTEE=3.0 (+1 rehab physician) |
|
Beds/ Physician FTEE=37.2 |
Beds/ Physician FTEE=121.8 |
Beds/ Physician FTEE=81.0 |
|
Hospital Unit: Beds=40 2 physician FTEE plus 1 PA |
||
|
Beds/physician FTEE=20.0 |
||
|
1Physicians also have responsibilities on the hospital inpatient's geriatrics service. |
||
TABLE 4 Required Physician Staffing in the Nursing Home PCAs of Three VAMCs According to Norms from Selected Sources
|
VAMC I NHCU Beds=30 NHCU1 FTEE=0.33 |
VAMC II NHCU Beds=103 NHCU1 FTEE=1.0 |
VAMC III NHCU Beds=62 NHCU1 FTEE=0.9 |
||
|
Source of Staffing Norms: |
||||
|
North Shore Hospital Center for Extended Care |
0.78 |
2.58 |
1.10 |
|
|
Hebrew Home of Washington |
0.24 |
0.79 |
0.34 |
|
|
Levindale Geriatric Center |
0.37 |
1.27 |
0.77 |
|
|
VAMC A |
0.24 |
0.80 |
0.34 |
|
|
VA Guidelines (circa 1965) |
0.30 |
1.03 |
0.62 |
|
|
1Based on FY 1989 CDR data; by definition, does not include FTEE allocated to intermediate care. |
||||
FIGURE 1 The Staffing Algorithm Development Instrument (SADI) for Long-Term Care: The Complete Instrument with a Statistical Summary of the Panel's Assessments
INTRODUCTION AND INSTRUCTIONS (Abbreviated)
The purpose of the SADI is to gather the data needed to construct, test, formalize, and enhance the algorithms and rules of thumb for staffing that emerged from prior meetings of each specialty and clinical program panel. The ultimate intention is to develop algorithms which could be applied to estimate staffing requirements at VA medical centers (VAMCs), presumably duplicating the results specialty and clinical program panelists themselves would have derived.
Section A of the SADI requests time estimates in some cases by workload unit. In other cases, it requests time estimates by major job elements (tasks). These elements had previously been indicated by some panel members as accounting for the bulk of the work of VA physicians. For the latter cases we seek your estimates of how physician requirements in your specialty vary with respect to such variables, as the volume of patients and the availability of residents and nonphysician practitioners. By systematically varying the levels of workload and personnel, we hope to infer from your numerical responses the implicit formulas you used to relate physician time to these variables, as well as the nature of the relationship between workload and staffing, e.g., linear or nonlinear.
Section B seeks responses to a series of questions for the time spent in activities other than direct patient care.
Instructions: In Section A, for each cell of each table, please estimate the number of physician hours required from the long-term care program at the VAMC to deliver good-quality care under the specified circumstances. Section B is self-explanatory.
SECTION A: PATIENT CARE ACTIVITIES
ADMISSIONS
Please fill in the average time, in hours, required by a staff physician in long-term care to accomplish an admission work-up, either with or without the assistance of a resident in your service.
Chart 1
|
Time per Admission Work-Up without Resident |
Time per Admission Work-Up with Resident |
|
|
High |
2.00 |
1.50 |
|
Low |
1.00 |
0.25 |
|
Mean |
1.60 |
0.61 |
|
Median |
2.00 |
0.50 |
ROUTINE DAILY PATIENT CARE
For each workload factor and alternative average daily census (ADC) level below, please fill in the average number of physician hours required from the long-term care program. Keep in mind that the daily rounds do not include new admission work-ups, since they are covered in Chart 1.
Chart 2
|
Nursing Home Ward Average LOS=115 days |
Assume No Residents |
||||||
|
ADC 1 |
ADC 10 |
ADC 20 |
ADC 30 |
ADC 40 |
ADC 50 |
||
|
Daily Rounds |
High |
0.05 |
0.30 |
0.60 |
1.00 |
1.50 |
2.00 |
|
Low |
0.02 |
0.16 |
0.30 |
0.48 |
0.64 |
0.80 |
|
|
Mean |
0.02 |
0.17 |
0.39 |
0.72 |
0.98 |
1.25 |
|
|
Median |
0.02 |
0.21 |
0.33 |
0.60 |
0.80 |
1.00 |
|
|
Nursing Home Ward Average LOS=115 days |
Assume No Residents |
||||||
|
ADC 1 |
ADC 10 |
ADC 20 |
ADC 30 |
ADC 40 |
ADC 50 |
||
|
Charting, Phone, and Paperwork |
High |
0.50 |
0.30 |
0.60 |
1.00 |
1.30 |
1.60 |
|
Low |
0.01 |
0.80 |
0.16 |
0.24 |
0.32 |
0.40 |
|
|
Mean |
0.20 |
0.17 |
0.38 |
0.58 |
0.73 |
0.90 |
|
|
Median |
0.20 |
0.17 |
0.40 |
0.60 |
0.75 |
1.00 |
|
|
Patient and Family Contacts plus Teaching |
High |
0.05 |
0.50 |
1.00 |
1.50 |
2.00 |
2.50 |
|
Low |
0.01 |
0.08 |
0.16 |
0.17 |
0.32 |
0.33 |
|
|
Mean |
0.03 |
0.16 |
0.40 |
0.58 |
0.75 |
0.93 |
|
|
Median |
0.04 |
0.08 |
0.17 |
0.25 |
0.33 |
0.41 |
|
|
Supervision and Teaching (Residents/Staff) |
High |
0.20 |
0.50 |
1.30 |
2.70 |
3.20 |
4.20 |
|
Low |
0.01 |
0.01 |
0.01 |
0.03 |
0.03 |
0.05 |
|
|
Mean |
0.08 |
0.29 |
0.68 |
1.12 |
1.43 |
1.78 |
|
|
Median |
0.06 |
0.35 |
0.92 |
1.17 |
1.67 |
1.83 |
|
|
TOTALS |
High |
0.20 |
1.40 |
2.80 |
4.20 |
5.60 |
7.00 |
|
Low |
0.00 |
0.33 |
0.65 |
0.99 |
1.31 |
1.65 |
|
|
Mean |
0.09 |
0.68 |
1.40 |
2.30 |
3.00 |
3.72 |
|
|
Median |
0.07 |
0.50 |
1.30 |
2.45 |
3.20 |
3.91 |
|
Chart 3
|
Nursing Home Ward Average LOS=115 days |
Assume 1 PGY 4-Level Resident |
||||||
|
ADC 1 |
ADC 10 |
ADC 20 |
ADC 30 |
ADC 40 |
ADC 50 |
||
|
Daily Rounds |
High |
0.03 |
0.15 |
0.30 |
0.60 |
0.80 |
1.00 |
|
Low |
0.00 |
0.00 |
0.08 |
0.12 |
0.16 |
0.20 |
|
|
Mean |
0.01 |
0.07 |
0.14 |
0.29 |
0.33 |
0.49 |
|
|
Median |
0.05 |
0.08 |
0.10 |
0.25 |
0.33 |
0.41 |
|
|
Charting, Phone, and Paperwork |
High |
0.01 |
0.01 |
0.16 |
0.30 |
0.40 |
0.50 |
|
Low |
0.00 |
0.00 |
0.00 |
0.00 |
0.00 |
0.00 |
|
|
Mean |
0.00 |
0.04 |
0.07 |
0.15 |
0.18 |
0.03 |
|
|
Median |
0.00 |
0.00 |
0.08 |
0.10 |
0.10 |
0.17 |
|
|
Patient and Family Contacts plus Teaching |
High |
0.05 |
0.50 |
1.00 |
1.50 |
2.00 |
2.50 |
|
Low |
0.00 |
0.00 |
0.05 |
0.08 |
0.08 |
0.17 |
|
|
Mean |
0.03 |
0.13 |
0.26 |
0.38 |
0.50 |
0.63 |
|
|
Median |
0.03 |
0.04 |
0.08 |
0.12 |
0.16 |
0.20 |
|
|
Supervision and Teaching (Residents/Staff) |
High |
0.25 |
0.60 |
1.21 |
1.80 |
2.80 |
3.00 |
|
Low |
0.01 |
0.08 |
0.16 |
0.20 |
0.20 |
0.20 |
|
|
Mean |
0.13 |
0.27 |
0.40 |
0.71 |
0.28 |
0.94 |
|
|
Median |
0.13 |
0.20 |
0.25 |
0.33 |
0.33 |
0.40 |
|
|
TOTALS |
High |
0.28 |
1.30 |
2.50 |
3.90 |
5.60 |
6.50 |
|
Low |
0.00 |
0.16 |
0.32 |
0.48 |
0.64 |
0.80 |
|
|
Mean |
0.14 |
0.50 |
0.93 |
1.45 |
2.0 |
2.30 |
|
|
Median |
0.13 |
0.40 |
0.55 |
1.00 |
1.20 |
1.40 |
|
Chart 4
|
Geriatric Evaluation Unit Average LOS=10 days |
Assume 1 PGY 4-Level Resident |
||||||
|
ADC 1 |
ADC 3 |
ADC 5 |
ADC 7 |
ADC 9 |
ADC 11 |
||
|
Daily Rounds |
High |
0.60 |
0.60 |
0.83 |
1.16 |
1.50 |
1.83 |
|
Low |
0.08 |
0.11 |
0.14 |
0.17 |
0.20 |
0.25 |
|
|
Mean |
0.44 |
0.34 |
0.44 |
0.53 |
0.71 |
0.79 |
|
|
Median |
0.17 |
0.25 |
0.33 |
0.42 |
0.60 |
0.60 |
|
|
Charting, Phone, and Paperwork |
High |
0.08 |
0.11 |
0.16 |
0.17 |
0.25 |
0.25 |
|
Low |
0.00 |
0.00 |
0.00 |
0.00 |
0.00 |
0.00 |
|
|
Mean |
0.04 |
0.05 |
0.08 |
0.08 |
0.12 |
0.13 |
|
|
Median |
0.02 |
0.08 |
0.08 |
0.08 |
0.17 |
0.17 |
|
|
Patient and Family Contacts plus Teaching |
High |
0.25 |
0.25 |
0.30 |
0.30 |
1.00 |
1.00 |
|
Low |
0.00 |
0.00 |
0.00 |
0.00 |
0.00 |
0.00 |
|
|
Mean |
0.08 |
0.11 |
0.13 |
0.15 |
0.32 |
0.34 |
|
|
Median |
0.04 |
0.08 |
0.12 |
0.16 |
0.20 |
0.25 |
|
|
Supervision and Teaching (Residents/Staff) |
High |
0.50 |
1.00 |
1.66 |
2.32 |
3.00 |
3.67 |
|
Low |
0.08 |
0.17 |
0.17 |
0.17 |
0.25 |
0.25 |
|
|
Mean |
0.30 |
0.48 |
0.69 |
0.86 |
1.10 |
1.26 |
|
|
Median |
0.34 |
0.40 |
0.48 |
0.64 |
0.83 |
1.00 |
|
|
TOTALS |
High |
1.08 |
1.55 |
2.57 |
3.60 |
4.65 |
6.29 |
|
Low |
0.30 |
0.52 |
0.75 |
0.83 |
1.00 |
1.00 |
|
|
Mean |
0.65 |
0.96 |
1.34 |
1.60 |
2.25 |
2.64 |
|
|
Median |
0.53 |
1.00 |
1.00 |
1.14 |
1.40 |
1.75 |
|
In some cases, the long-term care program may have the primary responsibility for managing the intermediate bed service. Please complete the following charts, again estimating the number of hours required per day from the long-term care program.
Chart 5
|
Intermediate Ward Average LOS=45 days |
Assume No Residents |
||||||
|
ADC 1 |
ADC 10 |
ADC 20 |
ADC 30 |
ADC 40 |
ADC 50 |
||
|
Daily Rounds |
High |
0.07 |
0.67 |
1.33 |
2.00 |
2.67 |
3.33 |
|
Low |
0.03 |
0.25 |
0.50 |
0.50 |
0.50 |
1.00 |
|
|
Mean |
0.05 |
0.48 |
0.96 |
1.38 |
1.79 |
2.33 |
|
|
Median |
0.05 |
0.50 |
1.00 |
1.50 |
2.00 |
2.50 |
|
|
Charting, Phone, and Paperwork |
High |
0.03 |
0.50 |
1.00 |
1.50 |
2.00 |
2.50 |
|
Low |
0.03 |
0.25 |
0.50 |
0.50 |
0.50 |
1.00 |
|
|
Mean |
0.03 |
0.35 |
0.69 |
0.98 |
1.26 |
1.71 |
|
|
Median |
0.03 |
0.32 |
0.63 |
0.95 |
1.27 |
1.67 |
|
|
Patient and Family Contacts plus Teaching |
High |
0.67 |
0.67 |
1.33 |
2.00 |
2.67 |
3.33 |
|
Low |
0.02 |
0.15 |
0.30 |
0.45 |
0.50 |
0.50 |
|
|
Mean |
0.24 |
0.34 |
1.18 |
0.96 |
1.24 |
1.70 |
|
|
Median |
0.03 |
0.28 |
0.55 |
0.70 |
0.90 |
1.21 |
|
|
Supervision and Teaching (Residents/Staff) |
High |
0.33 |
0.30 |
0.60 |
0.90 |
1.20 |
1.67 |
|
Low |
0.02 |
0.10 |
0.12 |
0.16 |
0.16 |
0.30 |
|
|
Mean |
0.13 |
0.19 |
0.26 |
0.36 |
0.45 |
0.69 |
|
|
Median |
0.03 |
0.19 |
0.16 |
0.19 |
0.21 |
0.40 |
|
|
TOTALS |
High |
0.20 |
1.79 |
3.45 |
5.16 |
6.83 |
8.63 |
|
Low |
0.00 |
0.83 |
1.67 |
1.67 |
1.67 |
3.00 |
|
|
Mean |
0.11 |
1.32 |
2.59 |
3.67 |
4.74 |
6.30 |
|
|
Median |
0.12 |
1.33 |
2.63 |
3.93 |
5.22 |
6.78 |
|
Chart 6
|
Intermediate Ward Average LOS=45 days |
Assume 1 PGY 4-Level Resident |
||||||
|
ADC 1 |
ADC 10 |
ADC 20 |
ADC 30 |
ADC 40 |
ADC 50 |
||
|
Daily Rounds |
High |
0.03 |
0.33 |
0.67 |
1.00 |
1.33 |
1.67 |
|
Low |
0.00 |
0.00 |
0.08 |
0.08 |
0.17 |
0.17 |
|
|
Mean |
0.02 |
0.20 |
0.39 |
0.57 |
0.78 |
1.00 |
|
|
Median |
0.03 |
0.20 |
0.40 |
0.60 |
0.80 |
1.09 |
|
|
Charting, Phone, and Paperwork |
High |
0.01 |
0.10 |
0.20 |
0.30 |
0.40 |
0.50 |
|
Low |
0.00 |
0.00 |
0.00 |
0.00 |
0.00 |
0.00 |
|
|
Mean |
0.00 |
0.05 |
0.10 |
0.15 |
0.20 |
0.25 |
|
|
Median |
0.00 |
0.05 |
0.10 |
0.15 |
0.20 |
0.25 |
|
|
Patient and Family Contacts plus Teaching |
High |
0.05 |
0.50 |
1.00 |
1.50 |
2.00 |
2.00 |
|
Low |
0.00 |
0.00 |
0.08 |
0.08 |
0.08 |
0.08 |
|
|
Mean |
0.02 |
0.20 |
0.40 |
0.58 |
0.77 |
0.83 |
|
|
Median |
0.02 |
0.12 |
0.25 |
0.38 |
0.50 |
0.63 |
|
|
Supervision and Teaching (Residents/Staff) |
High |
0.67 |
0.67 |
1.33 |
2.00 |
2.67 |
3.33 |
|
Low |
0.02 |
0.08 |
0.17 |
0.17 |
0.25 |
0.25 |
|
|
Mean |
0.25 |
0.39 |
0.78 |
1.17 |
1.56 |
1.80 |
|
|
Median |
0.05 |
0.40 |
0.80 |
1.25 |
1.65 |
1.80 |
|
|
TOTALS |
High |
0.14 |
1.40 |
2.80 |
4.20 |
5.60 |
6.17 |
|
Low |
0.00 |
0.08 |
0.33 |
0.33 |
0.50 |
0.50 |
|
|
Mean |
0.07 |
0.81 |
1.66 |
2.47 |
3.30 |
3.88 |
|
|
Median |
0.07 |
0.88 |
1.75 |
2.68 |
3.55 |
4.43 |
|
TIME PER INITIAL CONSULTATION OFF YOUR PCA
Fill in the average time in hours required by a staff physician in the long-term care program for each initial (new) consult on another service, noting the presence or absence of a nonphysician practitioner (NPP) in your own service. (When an NPP is present, assume that he/she is performing the consult under the supervision of an attending physician.)
Chart 7
|
Consultation in this PCA |
Time per Consult without NPP |
Time per Consult with Long-Term Care NPP |
||||||
|
High |
Low |
Mean |
Median |
High |
Low |
Mean |
Median |
|
|
Neurology |
2.00 |
0.50 |
1.30 |
1.50 |
0.50 |
0.08 |
0.38 |
0.50 |
|
Surgery |
2.00 |
0.25 |
1.25 |
1.50 |
0.50 |
0.08 |
0.38 |
0.50 |
|
Medicine |
2.00 |
0.25 |
1.10 |
1.00 |
0.50 |
0.08 |
0.38 |
0.50 |
|
Rehab. Med. |
2.00 |
0.50 |
1.15 |
1.00 |
0.50 |
0.08 |
0.38 |
0.50 |
|
Psychiatry |
2.00 |
0.50 |
1.25 |
1.50 |
0.50 |
0.08 |
0.38 |
0.50 |
TIME PER FOLLOW-UP VISIT (POST-CONSULTATION) OFF YOUR PCA
Fill in the average time in hours required by a staff physician in the long-term care program for each follow-up consultation visit on another service, noting the presence or absence of a nonphysician practitioner (NPP) from your service.
Chart 8
|
Consultation in this PCA |
Time per Visit without NPP |
Time per Visit with LTC NPP |
||||||
|
High |
Low |
Mean |
Median |
High |
Low |
Mean |
Median |
|
|
Neurology |
0.50 |
0.08 |
0.32 |
0.30 |
0.25 |
0.15 |
0.15 |
0.17 |
|
Surgery |
0.50 |
0.02 |
0.31 |
0.30 |
0.25 |
0.02 |
0.15 |
0.17 |
|
Medicine |
0.50 |
0.02 |
0.29 |
0.30 |
0.25 |
0.02 |
0.15 |
0.17 |
|
Rehab. Med. |
0.50 |
0.02 |
0.31 |
0.30 |
0.25 |
0.02 |
0.15 |
0.17 |
|
Psychiatry |
0.50 |
0.02 |
0.31 |
0.30 |
0.25 |
0.02 |
0.15 |
0.17 |
SPECIAL PROGRAMS
Fill in the average time, in hours, per week required by a staff physician in the long-term care program for any special program not previously accounted for, noting the presence or absence of a nonphysician practitioner (NPP).
Chart 9
|
Special Program |
Assume Physician Makes No Home Visits (Supervises NPP) |
Assume Physician Makes All Home Visits |
||||||
|
High |
Low |
Mean |
Median |
High |
Low |
Mean |
Median |
|
|
HBHC (Hospital-Based Home Care), with 60 Enrolled Patients |
5.00 |
1.00 |
4.17 |
3.75 |
22.00 |
8.00 |
13.10 |
9.20 |
SECTION B: NON-PATIENT-CARE TIME
Part 1. The activities listed below generally do not occur every day, but may be time consuming when looked at over a longer period, such as a week or month. List the time in hours that you would add to each physician's average workday to allow for the types of non-patient-care-related activities listed below:
Chart 10
|
Assume the amount of research accomplished at this VAMC is: |
High1 |
Medium1 |
Low1 |
|
|
Education of Residents (didactic, classroom, not on the PCA) |
High |
2.00 |
1.00 |
0.50 |
|
Low |
0.10 |
0.10 |
0.01 |
|
|
Mean |
1.05 |
0.50 |
0.20 |
|
|
Median |
1.00 |
0.50 |
0.30 |
|
|
Administration by Chief (time required to manage your whole program by a Chief and/or Assistant Chief) |
High |
4.00 |
3.00 |
3.00 |
|
Low |
1.00 |
0.50 |
0.25 |
|
|
Mean |
3.20 |
1.90 |
1.50 |
|
|
Median |
4.00 |
2.00 |
1.00 |
|
|
Administration by Other (non-Chief) Physicians |
High |
4.00 |
3.00 |
2.00 |
|
Low |
0.17 |
0.10 |
0.02 |
|
|
Mean |
1.40 |
1.00 |
0.70 |
|
|
Median |
1.00 |
0.50 |
0.25 |
|
|
1Examples of research level by total amount of funding (VA plus non-VA) in FY 1988. High: e.g., VAMC I with $8.8 million in total funding; Medium: e.g., VAMC II with $2.75 million in total funding; Low: e.g., VAMC III with about $176,000 in total funding. |
||||
|
Assume the amount of research accomplished at this VAMC is: |
High1 |
Medium1 |
Low1 |
|
|
Hospital-Related Activities (mortality and morbidity, Q.A., staff meetings) |
High |
1.00 |
0.50 |
0.50 |
|
Low |
0.20 |
0.10 |
0.10 |
|
|
Mean |
0.64 |
0.40 |
0.30 |
|
|
Median |
0.50 |
0.50 |
0.25 |
|
|
Total Hours per Average Weekday: |
||||
|
For Chief2 |
High |
4.00 |
3.00 |
3.00 |
|
Low |
1.00 |
0.50 |
0.25 |
|
|
Mean |
3.20 |
1.90 |
1.50 |
|
|
Median |
4.00 |
2.00 |
1.00 |
|
|
For Other (non-Chief) Physicians |
High |
5.50 |
4.00 |
2.50 |
|
Low |
0.50 |
0.40 |
0.20 |
|
|
Mean |
3.30 |
1.30 |
1.20 |
|
|
Median |
4.00 |
1.60 |
1.00 |
|
|
1Examples of research level by total amount of funding (VA plus non-VA) in FY 1988. High: e.g., VAMC I with $8.8 million in total funding; Medium: e.g., VAMC II with $2.75 million in total funding; Low: e.g., VAMC III with about $176,000 in total funding. 2Assume that Chief does not participate significantly in the Education of Residents and Hospital-Related Activities; SADI users may easily modify this assumption. |
||||
Part 2. In order to determine the actual staffing in this hospital, the number of FTEE must be adjusted to allow for CME, research, and any other requirements. What do you believe to be the appropriate percentage of time the “average” (typical) member of your program should devote to each of the following categories of non-patient-care-related activities?
Chart 11
|
Assume the amount of research accomplished at this VAMC is: |
High1 |
Medium1 |
Low1 |
|
|
Continuing Education |
High |
25 |
10 |
10 |
|
Low |
1 |
1 |
2 |
|
|
Mean |
13 |
5 |
5 |
|
|
Median |
13 |
5 |
5 |
|
|
Research (off the PCA) |
High |
40 |
20 |
10 |
|
Low |
30 |
10 |
3 |
|
|
Mean |
33 |
15 |
6 |
|
|
Median |
30 |
15 |
5 |
|
|
Vacation, Administrative Leave, Sick Time, Other |
High |
15 |
15 |
15 |
|
Low |
5 |
5 |
5 |
|
|
Mean |
11 |
11 |
10 |
|
|
Median |
13 |
11 |
10 |
|
|
Total Percentage of Time |
High |
60 |
34 |
25 |
|
Low |
46 |
28 |
15 |
|
|
Mean |
52 |
31 |
21 |
|
|
Median |
50 |
30 |
22 |
|
|
1Examples of research level by total amount of funding (VA plus non-VA) in FY 1988. High: e.g., VAMC I with $8.8 million in total funding; Medium: e.g., VAMC II with $2.75 million in total funding; Low: e.g., VAMC III with about $176,000 in total funding. |
||||
INSTITUTE OF MEDICINE
Committee to Develop Methods Useful to the Department of Veterans Affairs in Estimating Its Physician Requirements
LONG-TERM CARE PANEL
CHERYL E.WOODSON (Chair),† Director, Fellowship Program in Geriatric Medicine, Pritzker School of Medicine, University of Chicago, Chicago, Illinois
MARGARET GRIFFIN, Assistant Professor, Department of Internal Medicine, Loma Linda University School of Medicine, Loma Linda, California
ROBERT W.HUSSEY, Chief, Spinal Cord Injury Service, Richmond VA Medical Center, Richmond, Virginia
JOSEPH M.KEENAN, Assistant Professor of Family Medicine and Director of Geriatrics, Department of Family Practice and Community Medicine, University of Minnesota, Minneapolis
EDWIN J.OLSEN, Chief, Geriatric Psychiatry, Miami VA Medical Center, Miami, Florida
L.GREGORY PAWLSON, Chairman, Department of Health Care Sciences, George Washington University Medical Center, Washington, D.C.
ANN L.WHALL, Professor and Specialty Head, Gerontological Nursing, University of Michigan, Ann Arbor
Judith L.Teich, Staff Officer
|
†Member of the study committee. |









































