
7
Linkages Between Research and Services
How the two worlds of researchers and service providers interact is of great concern to all those involved in AIDS activities. With respect to AIDS prevention and intervention, research findings must be disseminated to the field as quickly and effectively as possible. At the same time, service providers often are in a unique position to discover new, researchable questions. To facilitate the exchange of ideas, federal agencies charged with missions for research and services must overcome differences and develop strategies for effective coordination and communication.
This chapter examines the relationship between the AIDS research programs of NIAAA, NIDA, and NIMH and the services programs at the Substance Abuse and Mental Health Services Administration (SAMHSA) and other PHS agencies. The following discussion begins with a description of the SAMHSA AIDS programs, and then looks at how service programs in general and SAMHSA programs in particular are linked with the AIDS research programs of NIAAA, NIDA, and NIMH. Attention is also paid to the issue of collaboration and coordination beyond NIH and SAMHSA in the larger arena of PHS and HHS.
AIDS PROGRAMS AT SAMHSA
SAMHSA was officially established in FY 1992 as the new incarnation of the services activities of the former ADAMHA.
SAMHSA's major components are the Center for Mental Health Services (CMHS), the Center for Substance Abuse Prevention (CSAP)—previously the Office of Substance Abuse Prevention (OSAP)—and the Center for Substance Abuse Treatment (CSAT)—previously the Office of Treatment Improvement (OTI). The Agency's comparable total budget increased from an appropriation of $794.7 million in FY 1988 to $2.1 billion in FY 1993. During the same period, specifically identified AIDS funding decreased from $42.5 million to $28 million (falling from 5 percent of the total budget to 1 percent) (Table 7.1).
AIDS constitutes a very small part of SAMHSA funding. To some degree, this is a legacy of the ADAMHA years, during which the vast majority of AIDS funding at the agency was allocated to research activities, as Figure 7.1 shows. Research represented 100 percent of the ADAMHA AIDS budget from FY 1983 to FY 1986, declined to 62 percent in FY 1988, and rose to 89 percent of the total AIDS budget in FY 1992.
As of FY 1994, only four programs are recognized in SAMHSA's formal budget as being AIDS related. Two of these programs—which constitute the bulk of the agency's AIDS-specific funds—are located in CSAT. The first, the Demonstrations and Training Program, has three components: Linkage, Training, and Outreach. The Linkage Program, which originated at NIDA in 1989, is a joint effort with the Health Resources and Services Administration (HRSA) to support demonstration projects that link community-based primary care and substance abuse, HIV/AIDS, and mental health treatment services. The program was funded at $7.8 million in FY 1993. The Training Program, which had a $2.8 million budget in FY 1993, trains health care workers, focusing on the relationship between substance abuse, HIV/AIDS, tuberculosis, and sexually transmitted diseases in the context of treatment services. The Outreach Program is the outgrowth of the NADR program that originated at NIDA and was later transferred to OTI (see Chapters 3 and 6). The current iteration still focuses on HIV prevention outreach to out-of-treatment drug users and their sexual partners, but now includes more complete medical assessments for tuberculosis and diagnostic screening for HIV. This program supports 25 to 30 projects for up to three years and had a total budget of $10 million in FY 1993.
The second CSAT AIDS program is the Treatment Improvement Demonstration Program, also known as the Comprehensive Community Treatment Program (CCTP). This program, funded at $791,000 in FY 1993, addresses the primary care needs of substance
TABLE 7.1 SAMHSA AIDS Program, 1986–1994 (Dollars in Millions)
|
|
1986 |
1987 |
1988 |
1989 |
1990 |
1991 |
1992 |
1993a |
1994b |
|
CMHSc |
0 |
0 |
0 |
0 |
4.4 |
3.1 |
3.0 |
3.0 |
4.4 |
|
CSAPd |
0 |
0 |
0 |
0 |
0 |
0 |
0 |
0 |
1.0 |
|
CSATe |
0 |
10.9 |
42.1 |
57.6 |
44. |
25.4 |
22.1 |
21.9 |
21.9 |
|
Prog. Mgt. |
0.2 |
0.2 |
0.4 |
0.5 |
0.7 |
1.6 |
0.9 |
0.7 |
0.7 |
|
AID |
0.2 |
11.1 |
42.5 |
58.1 |
49.8 |
30.1 |
26.0 |
25.6 |
28 |
|
Total |
533.3 |
851.5 |
794.7 |
1,108.0 |
1,664.5 |
1,871.5 |
1,950.7 |
2,038.5 |
2,150.2 |
|
% AIDS |
0 |
1 |
5 |
5 |
3 |
2 |
1 |
1 |
1 |
|
a Estimate. b Appropriations. c CMHS AIDS program includes AIDS Training and Demonstrations. d CSAP AIDS program includes HighRisk Youth Demonstrations. e CSAT AIDS program includes Treatment Demonstrations (including NADR). Source: SAMHSA Budget Office. |
|||||||||
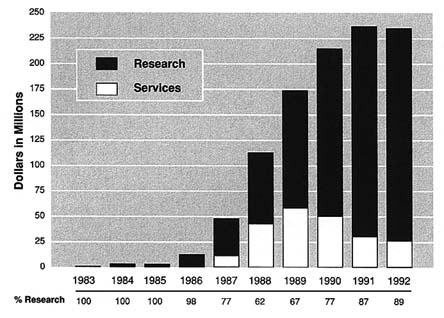
FIGURE 7.1 ADAMHA AIDS Budget Authority, 1983–1992. Note: "Research" includes former ADAMHA research activities currently with NIH (NIAAA, NIDA, NIMH, Office of Director, Buildings and Facilities); "Services" include former ADAMHA services activities currently with SAMHSA.Source: SAMHSA Budget Office.
abusers, including testing and prophylaxis for HIV, STDs, tuberculosis, and other illnesses, at drug treatment program entry. Overall, the CSAT AIDS program fell from $42.1 million in FY 1988 to $21.9 million in FY 1993, reflecting variations in the funding cycle of the outreach demonstration projects under the Demonstrations and Training line. The CMHS AIDS program includes Training and AIDS Training, which began at NIMH in FY 1990, and a new AIDS mental health services demonstration program, which was initiated in FY 1994. The Training Program, which was funded at $3.0 million in FY 1993, provides education and training for mental health care providers in the neuropsychiatric and psychosocial aspects of HIV infection. Eligible providers include psychiatrists, psychiatric nurses, psychiatric social workers, psychologists, and marriage and family counselors, as well as medical students, primary care residents, and nontraditional mental health care providers such as clergy, police, and alternative health care providers. The CMHS HIV/AIDS Mental Health Services Demonstration Program, developed in cooperation with HRSA and NIMH,
uses the cooperative agreement mechanism to develop and evaluate effective models for delivering mental health services to people with HIV/AIDS and their loved ones and caregivers. Its FY 1994 budget of $1.2 million is intended to fund 8 to 12 new projects for up to four years (CMHS is hoping to obtain the collaboration of other agencies to ensure an even larger budget in future years). Overall, AIDS funding at CMHS decreased from $4.4 million in FY 1990 to $2.9 million in FY 1993. With the addition of the demonstrations, it rose again to $4.4 million in FY 1994.
CSAP had no AIDS program until FY 1994, when it proposed providing supplements to the Prevention Demonstrations for HighRisk Youth Program to fund outreach and risk reduction activities related to HIV/AIDS, including skills building, pre-post HIV test counseling, outreach to resistant populations, and services to people who have lost friends and family members to AIDS. In FY 1994 this program was funded at $1 million, and it represents less than 1 percent of the total CSAP budget.
The goals of SAMHSA's AIDS program are fairly evident in the specific initiatives described above. First, the goal is to recognize that as AIDS becomes a chronic illness, more support will be needed from the substance abuse and mental health systems, which themselves will have to be strengthened to meet this challenge. Second, substance abuse and mental health treatment services will have to be further integrated into the primary care, general health care, and public health systems.
Indeed, the integration of substance abuse and mental health services into the general health care system is the primary goal of the SAMHSA AIDS office, which was created in 1992 by the ADAMHA reorganization bill. Currently, SAMHSA has an associate administrator for AIDS who is located in the office of the SAMHSA administrator. The associate administrator works with the three center offices on AIDS. These too were established by the ADAMHA reorganization bill, which mandated that each center have an AIDS office with an AIDS director or coordinator responsible for ensuring that HIV/AIDS issues are addressed and integrated into the overall programs of the center. The focus of the SAMHSA associate administrator for AIDS is coordination within and between the centers, SAMHSA, other federal agencies, and private organizations. An AIDS Work Group was in the planning stage at the time this report was written. This group will function under the aegis of the SAMHSA National Advisory Council and will provide a forum for discussion of planning and implementation of SAMHSA
AIDS activities. (This would be linked directly to the SAMHSA Committee for Women's Services.)
COLLABORATIONS BETWEEN RESEARCH AND SERVICES
When the ADAMHA Reorganization Act of 1992 was passed, some expressed concern that it would affect the relationship between research and services, with regard to the rapid, bidirectional transmission of information. Would research findings make their way quickly "from bench to bedside," and would observations and concerns from practitioners reach the research community in a timely manner? Those concerned about the splitting of the research and services programs of ADAMHA expressed fears that such separation could disrupt the linkages that existed within a single agency and impede the process of technology transfer. Those favoring the reorganization argued that separating the programs might well enhance relationships and thus improve linkages. This point was made in the report accompanying S-1306 the Senate bill to reorganize ADAMHA:
It might seem logical to keep research and services under the same roof to facilitate "technology transfer," the process by which research findings are applied in the field. In practice, however, the research and services enterprises are so different that they cannot be effectively administered in one agency. Researchers and service providers share a common goal, but they speak a different language and thrive in different professional cultures. Rather than collaboration between research and services, ADAMHA has been the setting for competition between these activities, a situation compounded by overlap and confusion with respect to the duties of the institutes and the agencies. (Senate Report 102–131, p. 3)
As the Senate report notes, the problem of a lack of collaboration between the research and services communities exists beyond the federal agencies, and is based in great part on different professional cultures. The two salient features of the research culture are the drive for "knowledge for knowledge's sake" and the existence of a reward system based on number and type of publications. The pursuit of knowledge involves the employment of a scientific method that emphasizes using controlled experiments, limiting the randomness of outcomes, and producing findings that can be replicated by other scientists. It involves sophisticated mathematical and statistical methodologies and advanced verbal and written skills, and it requires objectivity and limited
involvement with the subjects of the research (as much as possible) (Bailey, 1992a).
In contrast, the services world is driven by a desire to provide direct services to as many people as possible. Although the methods of service delivery are planned and evaluated, their internal integrity is often less important than the number of clients served. And while extensive reporting is often required by funding sources, this too is seen as less important to the mission of service providers than actually rendering the services—indeed, it is seen as a distraction. Furthermore, unlike researchers, service providers are trained to be subjective, to identify with and to advocate for their clients. Usually faced with funding and staffing inadequacies, and, in the case of HIV/AIDS service providers, daily experiences with severe illness and death, the services community easily can feel besieged (Bailey, 1992a).
These fundamental differences in culture and orientation between researchers and service providers result in significant barriers to collaboration. Service providers often feel that researchers are interested in their communities only for the sake of producing scientific results that will enhance the careers of individual researchers. Their experience is that, once that is accomplished, the researchers abandon the project and the client population on whom their research has been dependent. Moreover, service providers perceive researchers as coming from large, well-financed institutions that usually do not give anything back to the community they have studied once a research project is complete (Bailey, 1992a). As a result, they often feel that they and their clients are exploited by the scientific community.
At the same time, researchers often perceive service providers as unwilling to understand or appreciate the requirements of scientific research and the demand of their professional culture to get grants, teach, write, and publish. They encounter resistance to their efforts to refine or modify interventions in order to allow for rigorous scientific assessment, even though they explain to service providers the value of producing research results with scientific integrity. They often feel that service providers have unrealistic expectations about the potential applications of research findings to improved service delivery (Bailey, 1992a).
In addition to these differences in professional culture, there may be significant differences in the socioeconomic status of researchers and services providers—including their educational, racial/ethnic, and class status—that contribute to distrust and suspicion and get in the way of successful collaboration.
These kinds of conflicts are experienced at the federal level among agencies charged respectively with supporting research and services programs and are evidenced by the relatively limited collaborations between the AIDS research programs at NIAAA, NIDA, and NIMH and the AIDS services programs of SAMHSA, CDC, and HRSA, and the broader service-providing community. Even information exchange is limited. For example, each year the three research institutes sponsor many research exchange meetings, including research planning meetings, technical review meetings, workshops, and symposia. However, most of these meetings are designed to bring researchers together and very few reach beyond the research community to include service providers. Information about other linkages reported by the institutes in response to a committee request is provided below. (This is not an exhaustive review, but is meant to provide a sense of the range of existing activities.)
NIAAA
NIAAA identified only two AIDS research projects that it considers to have a direct relationship to the provision of services. The first is a longitudinal research program called The Native American Prevention Project on AIDS and Substance Abuse (NAPPASA), which developed rural school-based and community research partnerships that have produced positive outcome effects among southwestern Native American and other youth at risk. Community outreach programs were expanded to include reservation-wide, inter-reservation, statewide, regional, and national networking with Native American substance abuse and prevention groups. Workshops and conferences were cosponsored with the Navajo Tribe and with the Indian Health Service (a PHS agency). A community program coordinator representing the project has become integrated into the community and served as a member of the various prevention task forces.
The success of this continuing project is perceived to be a result of the ability of the principal investigator to form cooperative relationships between the research staff, schools, local public agencies, and the Native American Council. Staff members were hired from within the region, interventions were pretested with focus groups, and intervention materials were made available to additional school sites, which eventually requested partnerships with the research project. Both the Hopi Tribe and the Washington State Department of Indian Education have approached the principal
investigator to extend his work and to form new prevention research partnerships.
The second project identified by NIAAA as linking AIDS research and services provides alcohol and drug abuse counseling to gay men in the context of AIDS prevention activities. Here, too, the success of the linkages is attributed to the ability of the principal investigator to act as a credible liaison between the research, service provider, and constituency communities. Indeed, this research project is described by NIAAA as one that was prompted by service providers in the gay community who observed an increased rate of HIV infection among heavy drinkers and identified this as an important area of research.
NIDA
NIDA has engaged in a fairly wide range of activities with other federal agencies and nongovernmental service providers related to AIDS prevention and treatment among the drug-using population. These activities include collaboration in funding and planning projects and conferences, technical assistance in research planning, service delivery, education, and information dissemination. The following is a representative sample of activities:
NIDA/HRSA Program Linking Primary Health Care and Drug Abuse Treatment
This program, which was one of those transferred to CSAT with the ADAMHA reorganization, is designed to demonstrate the feasibility of various models for linking substance abuse treatment with primary health care services for drug abusers at risk for acquiring or spreading HIV. Of the original 21 grantees, about one-third were community health centers, one-third were city or county health departments, and the remainder were other institutions such as hospitals or state agencies. Now in its second round of funding, the program already has demonstrated success in reaching historically underserved populations, including women, Hispanics/Latinos, African Americans, adolescents, and HIV-infected individuals. This project found that clients first identified through primary care were much less advanced in their drug abuse career than those identified in drug abuse treatment programs. This important finding has implications for the design of integrated HIV, drug abuse, and primary medical care models.
National AIDS Demonstration Research Program (NADR)
The National AIDS Demonstration Research Program (NADR), which began at NIDA in 1987 and was transferred to OTI/CSAT in 1991, culminated in a program of technology transfer designed to facilitate the implementation of HIV prevention outreach and intervention initiatives throughout the country. NIDA's NADR program encompassed 41 individual projects conducting studies of the efficacy of community-based interventions in nearly 50 cities. Projects were focused on reaching out-of-treatment drug users and their sexual partners, and employed the use of indigenous leaders (ex-drug users) and other community members to recruit and retain people in the intervention programs. (See Chapters 3 and 6 for further details of NADR and its successor, the Cooperative Agreement for AIDS Community-Based Outreach/Intervention Research.) As a result of these efforts, alliances and linkages were formed between university or other research groups and community-based organizations in the implementation of the intervention research program.
During 1991, NIDA, the National Association of State Alcohol and Drug Abuse Directors (NASADAD), and the NADR grantees entered into a partnership to structure, organize, and facilitate implementation of effective AIDS prevention models from the NADR projects into training workshops. NIDA published manuals that documented the implementation of those models that were found to be the most effective, that is, that had resulted in reductions of risk-taking behavior. State-level training workshops were conducted with representatives from more than 300 organizations. Moreover, perhaps as a result of the NADR program, now all states are required by law to have HIV prevention outreach programs in order to quality for block grant dollars to provide drug abuse treatment. The regulations accompanying the relevant legislation prescribe the manuals developed by NIDA for use by the states in meeting this obligation. However, as of FY 1993, the funding for the training of state representatives in the implementation of these HIV prevention programs was cut at NIDA, which may hamper the states' ability to successfully adopt the programs.
NIDA/SAMHSA HIV Prevention/Intervention Training Courses
NIDA developed a series of HIV prevention/intervention training courses that are now housed in SAMHSA (CSAT). The curricula incorporated research findings, including intervention models
resulting from outreach research demonstration projects (e.g., NADR); research on the effects of drug use on immune system functioning; cofactors associated with disease progression; and relapse prevention methods used to help stabilize clients' functioning and thereby enhance their ability to practice prevention behaviors.
The contract under which the curricula were developed required dissemination to state agencies and community-based organizations. Numbers of ''Training of Trainers" and "Training of Service Providers" events were specified. Participants at all training events were informally encouraged to disseminate the material to colleagues in their geographic regions. The NIDA contractor was required to maintain a list of participants who successfully completed the training in order that these individuals could serve as technical resources to governments and other public and private agencies requesting technical assistance.
Success of this program is attributed to the use of the contract mechanism, which allowed NIDA to adequately monitor performance progress and to select a contract firm with appropriate experience and expertise in HIV training and community outreach. People from that firm had numerous links with individuals and agencies at the local level, which provided a valuable resource for various activities within the program.
Outreach and Bleach Distribution
NIDA's research on the effectiveness of bleach distribution for HIV prevention among injection drug users has been directly applied in community outreach projects, beginning in San Francisco in 1986. This kind of outreach project acts as a bridge to services because it refers drug users who are not in treatment for their addiction to such treatment, as well as to primary health care services.
Bleach distribution was an important HIV preventive intervention for NIDA while the institute was precluded (by Congress) from conducting or evaluating the effectiveness of needle and syringe exchange programs in reducing HIV transmission among injection drug users (see Chapters 3 and 6). Now that prohibition has been modified, NIDA is engaging in more direct research on needle exchange programs that also bridges services through drug treatment referral.
Other Collaborations
NIDA is providing technical assistance to SAMHSA in the development of quality assurance standards in methadone maintenance programs and on AIDS-related standards for drug treatment programs. It also is collaborating with CSAT and the District of Columbia in a research demonstration project testing the comparative efficacy of model programs that link drug abuse and HIV treatment and prevention.
NIMH
AIDS Research Centers
The AIDS Research Centers (see Chapter 6) supported by NIMH (and cofunded by NIDA from 1986 to 1988) are required to include an Information Exchange Core as a built-in mechanism for communicating with service providers in their communities. The HIV Center at Columbia University, for example, set up a community-wide board to advise on all aspects of the research and services program. This arrangement is seen as responsible for the success of the center's project targeting heterosexual, gay, and lesbian adolescents considered to be at risk for HIV transmission (e.g., runaway and homeless youth). In collaboration with other researchers and community-based service providers, the principal investigator developed a training manual entitled Adolescents Living Safely: AIDS Awareness, Attitudes, and Actions and tested it in a research study. The Information Exchange Core of the center was instrumental in disseminating the training manual to agencies in the services arena. The manual has been translated into Russian and has been used for the past year in the St. Petersburg school system. The United Nations translated the manuals into Spanish and is currently distributing them in South America.
The Columbia University AIDS Research Center also produced video and audio tapes in collaboration with an organization called The Media Group. Three of these videos: "AIDS, Me and My Baby," "AIDS is About Secrets," and "AIDS, Not Us,'' have been used widely by community-based organizations, drug treatment programs, health departments, and other entities involved in HIV prevention efforts throughout the United States and in other countries. These videos have received awards from both the medical education and the media communities, both nationally and internationally.
The San Francisco AIDS Research Center was funded to develop
effective prevention models and to form ongoing relationships with service organizations. An early study found that young gay men are at higher risk for HIV infection prior to confirmation with seroprevalence data. This study suggested that effective AIDS risk reduction programs should include issues concerning the meaning of life, coming out, and forming relationships. These findings were used by the San Francisco AIDS Foundation to develop a prevention campaign entitled "Life, Liberty, and the Pursuit of Happiness" targeted at young gay men.
AIDS Health Care Worker Training Program
Beginning in 1985, NIMH provided grants for training health care workers on different aspects of HIV/AIDS. Health care workers, including physicians, nurses, and social workers, were trained using the most current knowledge about AIDS, in particular HIV-related neuropsychiatric and cognitive problems. This program was one of those transferred to CMHS as part of the ADAMHA reorganization. In 1993, a book entitled AIDS, Health and Mental Health: A Primary Sourcebook was published as a direct outgrowth of the program and its evaluation, making possible even broader dissemination of the results.
NIMH (with CDC, HRSA, NIDA, NIAAA, and NICHD) Multisite Trial of Behavioral Strategies to Prevent the Further Spread of HIV Infection
In FY 1990, NIMH initiated a cooperative agreement to develop and test theory-driven behavior change interventions across multiple populations and sites. A major goal is to identify HIV prevention approaches that can be used readily by service providers in various communities. The cooperation of CDC and HRSA (along with NIDA, NIAAA, and NICHD) is intended to build in technology transfer and dissemination to the service provider community. This project is ongoing, and preliminary findings have not yet been released, so it is too early to measure its success in this regard.
HIV/AIDS Mental Health Services Demonstration Program
NIMH is a collaborating partner, along with HRSA, in the CMHS-sponsored demonstration program initiated in 1994 and described earlier in this chapter. NIMH will support certain aspects of the
program that relate to testing and evaluating models for mental health services for people with HIV/AIDS.
Other Collaborations
Since 1990 NIMH has sponsored an annual meeting in which AIDS prevention researchers from NIAAA, NIDA, and NIMH, colleagues from other PHS agencies such as CDC and HRSA, and representatives from community-based organizations actively participate in presentations and panel discussions. One outgrowth of such meetings has been the integration of NIMH-supported researchers into the AIDS prevention activities of CDC's Division of Adolescent and School Health as advisors, reviewers, and evaluators. Another product (from the 1992 meeting) is a handbook of guidelines for HIV prevention, directed toward highrisk populations, that will be printed and distributed to state and local community-based organizations.
BARRIERS TO COLLABORATION
All but one (the CMHS demonstrations) of the examples of collaborations between research and services cited above predate the reorganization of ADAMHA. Moreover, according to institute and agency staff, these collaborations came about as a result of informal communications between individual staff. No formal mechanism existed—or yet exists—to encourage interagency cooperation. Although within ADAMHA there had been tension between the research and services entities, some fear that the organizational separation of those entities will make collaboration even more difficult. In addition to cultural differences, legal and regulatory barriers also hinder collaboration between the institutes now at NIH and the services entities at SAMHSA (as well as at HRSA and CDC). In particular, the ADAMHA reorganization legislation made it eminently clear that SAMHSA centers were not to engage in anything called "research," and that the NIH institutes were not to engage in providing anything that could qualify as "services." In the realms of substance abuse and mental health, the dichotomization of research and services is not always possible nor helpful, especially in the context of AIDS, which requires rapid information exchange between research and services. The committee does not wish to take a position on the merits or defects of the ADAMHA reorganization, but it does wish to express concern over the potential for an even greater
divide between research and services. Such a divide should not be allowed to grow. Rather, the committee encourages the relaxation of cultural, legal, and regulatory barriers to collaboration between the research institutes and the service-providing agencies of the federal government.
In this regard, the committee takes heart from the new initiative sponsored by CMHS, in cooperation with NIMH and HRSA, designed to evaluate the efficacy of a range of mental health services provided to people with HIV/AIDS. The request for applications for this program was released in the spring of 1994, and applications were being submitted as this report was being written. Although it is unclear how successful this program will be, it is notable for having traversed significant organizational barriers to cooperation among the different research and services agencies, barriers made even more severe by the ADAMHA reorganization. The committee looks forward to its results.
COORDINATION OF AIDS ACTIVITIES WITHIN THE PUBLIC HEALTH SERVICE AND THE DEPARTMENT OF HEALTH AND HUMAN SERVICES
The possibility of collaborative activities between NIAAA, NIDA, and NIMH on the one hand and SAMHSA, CDC, and HRSA on the other is framed within the larger context of PHS and HHS AIDS activities. Coordination of PHS programs has resided for the past few years with the National AIDS Program Office (NAPO), and cross-agency coordination has been the function of the Federal Coordinating Committee on AIDS, chaired by PHS. In 1993, however, the Clinton administration elevated the status of federal AIDS coordination to a White House position with the appointment of a National AIDS Policy Coordinator responsible for all federal AIDS policy and programs. The activities of the newly titled Office of National AIDS Policy (ONAP) and the structures of organization and coordination within PHS and across federal agencies were still being determined at the time this report was written.
Rather than review activities of the past in this regard, the committee elected to reserve judgment about the overall coordination efforts at the PHS, HHS, and interdepartmental levels until the new organization and structures are in place. However, the committee does express its hope that mechanisms will emerge that make communication and cooperation between research and services entities more possible and collegial. Furthermore, the
committee hopes that the new coordination of AIDS activities and programs seeks to eliminate duplication of efforts and ensures the appropriate use of resources throughout the responsible federal agencies.
CONCLUSION AND RECOMMENDATIONS
CONCLUSION
The reorganization of ADAMHA was intended to separate research from services activities related to mental health and substance abuse. Although the decision to do so had nothing specifically to do with AIDS, it did have implications for how the disease would be addressed. While tensions already existed between the research and services programs at ADAMHA, their formal separation made collaboration and coordination even more difficult. This is evidenced by the small number of collaborative efforts between NIAAA, NIDA, and NIMH—now at NIH—and the newly named services entities at SAMHSA.
This tension between the worlds of researchers and service providers has historical roots. Nevertheless its persistence—both inside and outside of federal government agencies—poses a barrier to effective AIDS prevention and intervention. Research institutes and service-supporting agencies must find ways to overcome the cultural and institutional barriers to collaboration if they are to see a fruitful and productive exchange of knowledge necessary for intervening in—and ultimately eradicating—AIDS.
RECOMMENDATIONS FOR LINKAGES BETWEEN RESEARCH AND SERVICES
7.1 The committee recommends that NIAAA, NIDA, and NIMH ensure adequate follow-up time and money in their AIDS intervention research grants to accelerate information dissemination activities, including technical assistance.
7.2 The committee recommends that formal mechanisms be developed within the NIH institutes and other PHS agencies to foster linkages between AIDS research and services.
7.3 The committee recommends that NIAAA, NIDA, and NIMH sponsor regular research exchange meetings with services agencies and service providers, including local, regional, and national meetings.

















