

18 Carbon Tetrachloride Toxicity
|
Environmental ALERT…
|
This monograph is one in a series of self-instructional publications designed to increase the primary care provider’s knowledge of hazardous substances in the environment and to aid in the evaluation of potentially exposed patients. See page 18 for more information about continuing medical education credits and continuing education units.
|
Guest Contributor: |
Lora E.Fleming, MD, MPH, MSc |
|
Guest Editor: |
Michael Hodgson, MD |
|
Peer Reviewers: |
John Ambre, MD, PhD; Charles Becker, MD; Jonathan Borak, MD; Joseph Cannella, MD; Howard Kipen, MD, MPH; Richard J.Jackson, MD, MPH; Jonathan Rodnick, MD; Brian A.Wummer, MD |

U.S. DEPARTMENT OF HEALTH & HUMAN SERVICES
Public Health Service
Agency for Toxic Substances and Disease Registry
Case Study
A hazardous waste worker with delayed onset abdominal pain, nausea, vomiting, and diarrhea
As the physician on duty at a hospital emergency department (ED) in an urban community, you are notified that three hazardous waste workers—two men and a woman—are being transported from their worksite by ambulance. All three workers are complaining of headache, dizziness, and nausea.
You learn that the workers were handling several dozen barrels of a sweet-smelling hazardous waste liquid in a hot, unventilated room. Their work required taking samples from barrels, which were obtained from a defunct chlorofluorocarbon manufacturing plant. All three workers were initially wearing full-face respirators and protective clothing, but the younger man removed his respirator early in the day because he had a hangover and was nauseated; he felt it was more convenient to work without being hampered by the respirator. The other two workers continued in full protective gear. After 3 to 4 hours, the three workers began to experience symptoms.
Physical examinations of the workers are conducted in the ED. The older man’s and woman’s results are normal. Their symptoms subside within 2 hours, and they are discharged.
The younger man, however, has trouble concentrating and is mildly ataxic. His initial blood laboratory data are within normal limits, but he is kept under close observation. You learn from the young man that he is aged 25 and has been in good health with no history of similar problems. Last night, in celebration of his birthday, uncharacteristically he drank 9 to 12 beers, which accounts for his hangover this morning. He also mentions that this morning, while cleaning several wounds sustained in a fight the prior evening, he spilled a can of isopropyl alcohol on his hands and clothes but did not bother to change his clothing.
Six hours later, while still in the ED, the young man becomes acutely ill. He has abdominal pain, nausea, vomiting, and diarrhea. His rectal temperature is now 101°F, pulse 140/min, and he has become disoriented and drowsy. Two days after hospital admission he still has an elevated temperature and abnormal laboratory tests as follows: serum creatinine 2.0 mg/dL (normal 0.7 to 1.5); SGOT or AST 80 U/L (normal 7 to 45); total bilirubin 2.4 mg/dL (normal 0.1 to 1.4); PT 15 seconds (normal 10 to 13). Urinalysis reveals 2+ proteinurea, and urine output has decreased despite intravenous hydration.
![]()
(a) What is the possible clinical course for this young man?
_________________________________________________________________
(b) How will you identify the material to which the workers have been exposed?
_________________________________________________________________
(c) What treatment or antidote would you consider for the patient?
_________________________________________________________________
Answers to pretest questions may be found on page 15.
Exposure Pathways
❑ In the United States, most industrial CCl4is used in the synthesis of CFCs and chlorinated solvents. Production and usage is declining.
❑ Sources of environmental contamination include industrial and hazardous waste sites.
Carbon tetrachloride (CCl4) is a clear, nonflammable, heavy liquid that evaporates readily, producing a sweet odor. Although CCl4 does not occur naturally, it is ubiquitous in the environment. Its chemical stability results in an atmospheric half-life of 30 to 100 years. While CCl4 does not photodegrade in the ambient air, it may degrade in the presence of the shorter ultraviolet radiation found in the stratosphere. Synonyms for carbon tetrachloride include tetrachloromethane, carbon tet, carbona, tetrasol, and carbon chloride.
Acute CCl4 toxicity in the workplace was widely recognized by the 1950s. Since then, CCl4 manufacture and use have decreased. Today, most CCl4 is consumed in the synthesis of chlorofluorocarbons (CFCs), which are used as heat transfer agents in refrigerating equipment and as aerosol propellents. Because of recent international agreements to restrict the use of CFCs, which are thought to deplete the earth’s protective ozone layer, production of CCl4 will most likely continue to decline. Minor amounts of CCl4 are still used as an industrial solvent for oils, fats, lacquers, pesticides, varnishes, rubber, waxes, and resins. The largest source of CCl4 release has been from the fumigation of grains and other substances. In 1986, CCl4 fumigation was banned except for preserving museum artifacts.
In the United States, CCl4 has been used widely as an industrial and household cleaning fluid. In industry, it was an effective metal-degreaser, and in the home, it was used to remove spots from clothing, furniture, and carpets. CCl4 also has been used as an extracting solvent for flowers and seeds, as a component in fire extinguishers, as an anthelmintic and anesthetic, and until 1969, as a waterless shampoo. CCl4 is still used for many of these purposes in Europe and the third world.
The general population may be exposed to small amounts of CCl4 through ambient air. Sources producing concentrations that are above background levels include industrial locations where CCl4 is still used and chemical waste sites where emissions into air, water, or soil are not controlled properly. In 1983, the average atmospheric background level in rural areas was 0.13 parts per billion (ppb); average levels in suburban and urban areas were 0.19 ppb. The Environmental Protection Agency (EPA) has estimated that a lifetime exposure to 0.11 ppb CCl4 in air causes an excess risk of, at most, one additional cancer in a population of 100,000 people exposed. Before 1988, global atmospheric levels of CCl4 steadily increased by about 1.3% per year, but they will most likely decline in the future due to decreasing CCl4
production. Concentrations indoors are often higher than outdoors, indicating that building materials or products such as pesticides and cleaning agents inside the home may be a source of airborne CCl4.
Because of its moderate solubility in water and its relatively high rate of volatilization from water, only about 1% of the total CCl4 found in the environment is dissolved in surface waters and oceans. The results of surveys performed by the federal government show that about 99% of all groundwater supplies and about 95% of all surface water supplies contain less than 0.5 ppb of CCl4. The EPA maximum contaminant level (MCL) for drinking water is 5 ppb.
Who’s at Risk
❑ Workers using CCl4or CCl4-containing products are at greatest risk of exposure.
❑ Few cases of CCl4toxicity have occurred since the institution of industrial standards.
❑ Moderate to heavy drinkers and diabetics may be at increased risk of CCl4’s adverse effects.
Workers employed in industries that manufacture or use CCl4 are at greatest risk of exposure. According to a 1981–1983 survey, about 58,000 workers are exposed to CCl4 in the United States; however, phase-out of the solvent will most likely decrease the number of exposures. Although inhaled CCl4 has been associated with liver and kidney damage, exposure at current permissible airborne levels in the workplace is not linked to chronic disease. Workers who may be exposed to CCl4 include the following:
air transportation workers
automobile mechanics*
dry cleaners*
grain workers (inspection, storage, milling, processing)*
hazardous waste workers
museum workers
pesticide applicators*
pharmaceutical manufacturers
steel mill and blast furnace workers
telephone and telegraph equipment manufacturers
workers in tin-waste recovery operations
People living near chemical plants where fugitive emissions of CCl4 occur may be exposed to elevated levels of this chlorocarbon. Other populations at risk of exposure to CCl4 include people living near chemical waste sites where CCl4 is improperly stored.
The toxic metabolites of CCl4 are produced from reactions mediated by mixed function oxidase (MFO) enzymes occurring primarily in the liver and kidneys; therefore, persons with increased MFO enzyme activity may produce toxic CCl4 metabolites at a faster rate and may be more susceptible to CCl4-induced effects. These include persons taking certain medications (such as barbiturates), and persons exposed to chlorinated insecticides (such as DDT, chlordecone, or mirex) or halogenated industrial chemicals (such as polychlorinated biphenyls). Triamcinolone and progesterone may also potentiate the effects of relatively moderate CCl4 exposure.
Alcohols (methanol, ethanol, and isopropyl alcohol) and their ketone analogues are known MFO inducers; hence, persons with a history of moderate or heavy ethanol abuse and those with poorly controlled diabetes may be at increased risk of CCl4’s harmful effects. Even in nonhabitual drinkers, ethanol intake up to 12 hours before CCl4 exposure increases risk. Most occupational fatalities due to CCl4 inhalation involve alcohol abusers; fatal toxicity rarely occurs in nondrinking patients.
Animal studies have demonstrated that fasting or consuming diets low in antioxidants (such as vitamin E, selenium, or methionine) can lead to increased hepatotoxicity from CCl4 exposure although this effect has not been proven in humans. Persons with preexisting hepatic necrosis or cirrhosis or underlying renal disease appear to have increased susceptibility to CCl4-induced toxicity and are at increased risk of subsequent liver cancer.
Although CCl4 is not toxic to the fetus in most animal models, results of studies indicate that the human fetal MFO enzyme system may be operational in the later stages of development and can be induced by certain maternal exposures (e.g., cigarette smoke). Therefore, susceptibility of the human fetus to adverse effects of CCl4 may depend on developmental stage and on duration and concentration of exposure.
|
Information for the case study: You discuss the acute exposures with the workers’ company supervisor. He suspects that the waste barrels contain CCl4since that chemical is a starting material in the synthesis of chlorofluorocarbons, and it has a sweet odor. The older male worker in the case study is aged 40, has a full beard, and has a history of alcoholism, although he has been abstinent for several years. He also has a history of hepatitis B due to a blood transfusion more than 10 years ago. (1) If the material in the barrels is CCl4, is this worker at increased risk? _________________________________________________________________ (2) The female coworker later discovers she was almost 6 weeks pregnant at the time of this episode. Her obstetrician calls you to discuss the implications of the exposure to the fetus. What is your recommendation? Explain. _________________________________________________________________ _________________________________________________________________ |
Biologic Fate
❑ CCl4is absorbed readily by all exposure routes.
❑ Evidence indicates that CCl4metabolism occurs via a free-radical intermediate.
❑ Elimination of CCl4occurs in two phases. Some inhaled CCl4is rapidly exhaled unchanged. A small amount of inhaled CCl4temporarily enters fat tissue and later emerges and is excreted.
CCl4 readily enters the body by inhalation, ingestion, and dermal absorption. Inhalation is the primary route of exposure, with pulmonary absorption in humans estimated to be 60%. The rate of absorption through the gastrointestinal tract is rapid and greatly affected by diet (e.g., fat or alcohol in the gut enhances CCl4 absorption). CCl4 also is absorbed through the skin, though less readily than by the lungs. Dermally, the liquid is more rapidly absorbed than the vapor, and prolonged skin contact with the liquid can result in systemic effects.
Few quantitative studies of CCl4 absorption and distribution in humans have been reported. In experimental animals, CCl4 is dispersed to all organs and tissues proportionate to blood perfusion and lipid content; the brain has the highest levels after inhalation or oral administration. The rate of inhalation absorption in humans decreases as the duration of exposure or dose increases, indicating a saturable metabolic pathway.
In humans, approximately 50% to 80% of a dose absorbed by the lungs is exhaled unchanged. Some CCl4 temporarily enters fat tissue. After exposure ceases, CCl4 continues to emerge from fat and is removed by the lungs. About 4% of all metabolized CCl4 is converted directly to CO2 and is exhaled; the remainder forms adducts with proteins and other cellular molecules. The adducts are degraded (half-life about 24 hours) and their products excreted mainly in urine and feces.
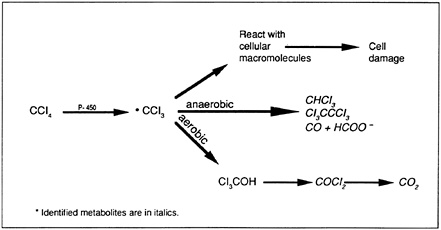
Bioactivation of CCl4 has become the model for chemical toxicity induced by free radicals—a mechanism of toxic injury similar to that associated with radiation and the aging process. The results of studies with experimental animals indicate that the first step in CCl4 metabolism may involve the formation of a trichloromethyl free radical (•CCl3) via the cytochrome P-450 enzyme system (Figure 1). The •CCl3 radical is postulated to bind directly to microsomal lipids and other cellular macromolecules, contributing to the breakdown of membrane structure and disrupting cell energy processes and protein synthesis. The •CCl3 radical also may undergo anaerobic reactions, resulting in the formation of a variety of toxins including chloroform (CHCl3), hexachloroethane (Cl3CCCl3), and carbon monoxide (CO). In aerobic metabolism, the •CCl3 radical can yield trichloromethanol (Cl3COH), a precursor to phosgene (COCl2), which is then hydrolyzed to form CO2.
Figure 1. Products of CCl4metabolism*
Physiologic Effects
The immediate effect of acute CCl4 exposure by all routes is central nervous system (CNS) depression. If the patient survives this immediate effect, death is usually due to hepatic or renal injury. Adverse effects to other organs are likely to be secondary to CNS, liver, or kidney damage. CCl4 is classified as a potential human carcinogen based on results of studies that indicate ingested CCl4 increases the frequency of liver tumors in experimental animals.
Neurologic Effects
❑ Acute exposure to CCl4may lead to rapid CNS depression.
CCl4 rapidly produces a narcotic effect on the brain. Immediate fatalities result either from respiratory depression (due to direct CNS effects) or from cardiac dysrhythmias. In severe cases, autopsy reveals permanent damage to nerve cells with focal areas of fatty degeneration and demyelination, Purkinje cell damage, and patchy pontine necrosis. Inhalation exposure can result in acute cerebellar dysfunction.
Hepatic and Renal Effects
❑ Hepatic and renal toxicity are due to biotransformation of CCl4to toxic metabolites.
❑ CCl4toxicity is potentiated by chemicals that activate the cytochrome P-450 system.
Carbon tetrachloride is a well-known hepatotoxic agent. In acute lethal CCl4 exposures, autopsy reveals marked hepatic steatosis (fatty degeneration) and centrilobar necrosis. The toxic metabolites of CCl4 block formation and release of low-density lipoproteins and deplete hepatic stores of glutathione. Centrilobular necrosis possibly results from reactions of initial free-radical intermediates. (See Biologic Fate, page 5.) In addition, a dramatic increase in calcium concentration occurs in hepatic mitochondria, accompanied by alterations in electrolyte distribution with swelling of hepatic cells and depletion of liver glycogen.
Hepatic injury, which usually manifests after CNS effects have subsided, typically occurs 1 to 4 days after acute exposure. Jaundice develops in about 50% of poisoning cases and typically evolves rapidly. Recovery from acute exposure is usually complete, with no long-term sequelae. Chronic exposure may result in fibrosis or cirrhosis. A decrease in clotting factors (due to acute liver damage) may predispose the patient to hemorrhage.
Exposure to CCl4 can result in nephritis, nephrosis, and renal failure. Within hours after manifestation of hepatic damage, renal failure may begin and typically reaches a peak in the second week after exposure. Oliguria or anuria may develop by the second to fourth day after exposure with concomitant edema, azotemia, proteinuria, hemoglobinuria, and glucosuria. Hypertension and acidosis may develop. Occasional moderate elevations in white cell counts occur, possibly in response to necrotic liver or kidney injury.
Fluid overload can lead to pulmonary congestion and edema. CCl4 also may have direct toxic effects on the lungs. Changes in blood pressure or heart rate are probably secondary to renal effects on fluid and electrolyte retention or to CNS effects on the heart or blood vessels. Kidney failure is the main cause of death in many patients with acute CCl4 exposure.
Carcinogenic Effects
Although data on the carcinogenic effects in humans are inconclusive, studies in experimental animals provide convincing evidence that ingestion of CCl4 increases the risk of liver cancer, in particular, hepatomas and hepatocellular carcinomas. It is speculated that highly reactive metabolic free radicals combine with hepatic macromolecules to cause these effects. The National Institute for Occupational Safety and Health (NIOSH) has identified CCl4 as a potential human carcinogen. The American Conference of Governmental Industrial Hygienists (ACGIH) considers CCl4 a suspected human carcinogen.
|
Additional information for the case study: Early that evening, the manager calls to inform you that the company has identified the hazardous waste as CCl4. (3) Knowing the exposure was to CCl4, do you consider the patient to be at increased risk of acute health effects? Why? _________________________________________________________________ _________________________________________________________________ |
Clinical Evaluation
No unique pattern characterizes acute or chronic CCl4-induced illness. Diagnosis is based on a history of exposure and the clinical signs including CNS depression, dysrhythmias, and hepatic necrosis.
History and Physical Examination
❑ The occupational and environmental history is essential to diagnosing CCl4toxicity.
❑ The physical examination should focus on the neurologic and gastrointestinal systems.
The patient’s occupational history is crucial. For each job held, the history should include the name and location of the company, job title, description of chemical processes employed, known toxic agents, and history of worker illness. Additional helpful information includes history of exposure to other known hepatotoxic agents (e.g., medications and ethanol), history of hepatic and renal disease, and an environmental history including type of water supply, location and duration of residence, proximity to industry, and patient’s hobbies.
In acute exposure, the initial physical examination should concentrate on the neurologic system. One to six days after an acute exposure, a patient may develop severe hepatic necrosis and renal failure, which can affect the cardiovascular and pulmonary systems. Toxic hepatitis, necrosis, and cirrhosis have been reported after chronic exposure to high levels of CCl4.
Signs and Symptoms
❑ Regardless of CCl4exposure route, CNS effects predominate initially; symptoms of hepatic and renal damage may manifest later.
Patients exposed to CCl4 by any route exhibit predominantly CNS depression. Common symptoms, which are dose-dependent, include headache, giddiness, weakness, ataxia, lethargy, stupor, and coma. Complaints of restricted peripheral vision have been reported. In less severe cases, effects usually disappear within a day or two after exposure is stopped. Persistence of neurologic symptoms beyond 24 hours is more common when severe hepatic and renal damage also have occurred.
Gastrointestinal symptoms of nausea, abdominal pain, vomiting, and diarrhea after acute exposure appear to be related to initial effects on the autonomic nervous system. Symptoms persisting beyond 24 hours may be the result of hepatic and renal injury. Signs may include hepatomegaly (right upper-quadrant pain), jaundice, oliguria, and anuria. Patients with hepatic and renal injury should be monitored for secondary signs of cardiac dysrythmias, pulmonary edema, and bleeding disorders.
Symptoms from chronic CCl4 exposure are similar to those from acute exposure. Workers chronically exposed to CCl4 have complained of headache, decreased peripheral vision, inability to think clearly, and dizziness; visual effects have been evaluated in many clinical studies without conclusive results. Persistent nausea should prompt an evaluation of the liver for toxic hepatitis.
Laboratory Tests
Direct Biologic Indicators
❑ Any detectable amount of CCl4in the blood indicates exposure, although not necessarily adverse effects.
Carbon tetrachloride can be detected by gas chromatography in blood, serum, and adipose tissue, as well as other biologic and environmental materials. Even though refrigeration of blood samples in sealed tubes conserves the CCl4 level, analysis should be performed within 24 hours. Any detectable blood level indicates exposure, although detectable levels are not necessarily indicative of adverse health effects. CCl4 and other chlorinated hydrocarbons are radiopaque and may appear on abdominal X ray.
Indirect Biologic Indicators
❑ Liver and kidney function tests, chest X ray, and electrocardiogram are advised for persons exposed to CCl4.
For persons exposed to CCl4, baseline liver function tests (including SGOT [AST], SGPT [ALT], alkaline phosphatase, and bilirubin) and liver injury tests (levels of serum bile acids and indocyanine green [ICG] clearance rates) may be helpful in assessing liver status. Renal function tests (creatinine, BUN, electrolytes, and urinalysis) should be performed, and urine output and fluid balance should be
monitored carefully. In persons with high exposures, clotting studies (i.e., PT and PTT), chest X ray, and electrocardiogram are warranted for baseline and monitoring purposes. If liver or renal injury is severe, patients should be evaluated for spontaneous bleeding with serial hematocrits and tests for stool occult blood.
|
(4) Exposure to CCl4is confirmed. What are your immediate concerns regarding the prognosis of the acutely ill patient in the case study? _________________________________________________________________ _________________________________________________________________ (5) What initial action should be taken in the emergency department for patients exposed to any volatile solvent (CCl4included)? What laboratory work-up is advised? _________________________________________________________________ _________________________________________________________________ |
Treatment and Management
❑ N-acetylcysteine may reduce complications in patients with severe CCl4exposure.
❑ Other than removal from the source of exposure and avoidance of other hepatotoxicants, no treatment for effects of chronic CCl4exposure exists.
Liquid CCl4 is absorbed through the skin; therefore, clothing should be removed from exposed persons and the skin cleansed with copious amounts of water and soap (or mild detergent). Because CCl4 is somewhat irritating to mucous membranes, exposed eyes should be irrigated with water for at least 15 minutes. Gastric lavage and administration of activated charcoal are appropriate measures for patients who have ingested CCl4. Do not induce emesis because pulmonary aspiration is a risk.
Case reports from Europe, where antioxidants such as methionine, cysteine, and N-acetylcysteine (NAC or MucoMyst®*) are used, suggest that when these free-radical scavengers are given intravenously within 12 to 15 hours after high-level, acute CCl4 exposure, they may prevent or decrease hepatic and renal damage. Recommended intravenous use of NAC, which is currently investigational in the United States, is based on its success in the treatment of acetominophen overdose. The oral form of NAC, which is commercially available in the United States, also may prove useful. The clinician should consult with an experienced medical toxicologist or a regional poison control center.
Because of the suspected free-radical nature of a toxic intermediate in CCl4 metabolism, the use of hyperbaric oxygen is contraindicated. Hemodialysis has been used to treat renal failure, but it has not proved successful in reversing CCl4 pathology. Epinephrine should be used cautiously since it may induce or aggravate cardiac dysrhythmias.
Patients should be observed for onset of hepatic and renal effects up to 2 weeks after exposure. To a large extent, survival depends upon the patient’s nutritional status and underlying condition of the hepatorenal system. Future hepatocellular carcinoma in persons with residual liver damage is a possibility. Exposed patients should be instructed to avoid stimulants and other hepatotoxicants including ethanol. Administration of the hepatitis B vaccine should be considered.
|
(6) What treatment would you recommend for the patient in the case study? _________________________________________________________________ _________________________________________________________________ _________________________________________________________________ (7) What follow-up would you recommend for this patient? For his potentially exposed coworkers? _________________________________________________________________ _________________________________________________________________ |
Standards and Regulations
NIOSH considers CCl4 a probable human carcinogen and ACGIH considers CCl4 a suspected human carcinogen. ACGIH also gives CCl4 a “skin” designation, which indicates potential for dermal absorption. CCl4 has an odor threshold of 10 parts per million (ppm), which does not provide adequate warning of harmful exposure. The regulations and guidelines pertaining to CCl4 are summarized in Table 1.
Workplace
Air
The workroom standard for CCl4, mandated by the Occupational Safety and Health Administration (OSHA), is a time-weighted average (TWA) of 2 ppm. NIOSH recommends a 60-minute ceiling limit of 2 ppm. The air level considered by NIOSH to be immediately dangerous to life and health (IDLH) is 300 ppm.
Environment
Air
Currently, there are no federal regulations for CCl4 emissions into air; however, several state agencies have established maximum levels. CCl4 is on the list of 190 hazardous air pollutants listed in the Clean Air Act, which was signed into law November 15, 1990. EPA is scheduled to issue CCl4 emission standards by November 1992.
Table 1. Standards and regulations for carbon tetrachloride
|
Agency* |
Focus |
Level |
Comments |
|
ACGIH |
Air-workplace |
5 ppm (30 mg/m3) |
Advisory; TLV-TWA† (Skin) |
|
NIOSH |
Air-workplace |
2 ppm (12.6 mg/m3) |
Advisory; Ceiling (60 minutes) |
|
OSHA |
Air-workplace |
2 ppm (12.6 mg/m3) |
Regulation; PEL§ as TWA |
|
EPA |
Drinking water |
5ppb (0.005 mg/L) |
MCL¶ |
|
|
|
0 |
MCLG** |
|
*ACGIH=American Conference of Governmental Industrial Hygienists; EPA=Environmental Protection Agency; NIOSH=National Institute for Occupational Safety and Health; OSHA=Occupational Safety and Health Administration †TLV-TWA (Threshold Limit Value-Time Weighted Average)=time-weighted average concentration for a normal workday and a 40-hour workweek to which nearly all workers may be repeatedly exposed. §PEL (Permissible Exposure Limit)=highest level of CCl4 in air to which a worker may be exposed, averaged over an 8-hour workday ¶MCL (Maximum Contaminant Level)=enforceable level for drinking water **MCLG (Maximum Contaminant Level Goal) |
|||
Water
The EPA maximum contaminant level for CCl4 in drinking water is 5 parts per billion (ppb). States have established maximum levels as low as 0.5 ppb (proposed for California).
Other
Federal regulations have banned the use of all pesticide products containing CCl4; an exception is the use of CCl4 on encased museum specimens.
|
Additional information for the case study: You are requested to consult with the hazardous waste management company regarding the effect of CCl4exposure on employee health. (8) What will you stress with management concerning this incident? _________________________________________________________________ _________________________________________________________________ |
Suggested Reading List
General
Dossing M, Skinhoj P. Occupational liver injury. Present state of knowledge and future perspective. Int Arch Occup Environ Health 1985;56:1–21.
Guzelian PS. Hepatic injury due to environmental agents. Clin Lab Med 1984;4(3):483–8.
Hardin BL. Carbon tetrachloride poisoning—a review. Ind Med Surg 1954;23:93–105.
Louria DB, Bogden JD. The dangers from limited exposure to carbon tetrachloride. Crit Rev Toxicol 1980:7(2);177–88.
Zimmerman HJ. Effects of alcohol on other hepatotoxins. Alcohol Clin Exp Res 1986;10(1):3–15.
Treatment and Management
Meredith TJ, Ruprah M, Liddle A, Flanagan RJ. Diagnosis and treatment of acute poisoning with volatile substances. Hum Toxicol 1989;8(4):277–86.
Pond SM. Effects on the liver of chemicals encountered in the workplace. West J Med 1982;137(6):506–14.
Ruprah M, Mant TGK, Flanagan RJ. Acute carbon tetrachloride poisoning in 19 patients: implications for diagnosis and treatment. Lancet 1985;8436:1027–9.
Government Documents
Agency for Toxic Substances and Disease Registry. Toxicological profile for carbon tetrachloride. Atlanta: US Department of Health and Human Services, Public Health Service, 1989.
Environmental Protection Agency. Health effects assessment for carbon tetrachloride. Cincinnati: US Environmental Protection Agency, Office of Environmental Criteria and Assessment, 1989. Report no. EPA/600/8–89/088; NTIS report no. PB90–142407.
Sources of Information
More information on the adverse effects of carbon tetrachloride and treating and managing cases of exposure to carbon tetrachloride can be obtained from ATSDR, your state and local health departments, and university medical centers. Case Studies in Environmental Medicine: Carbon Tetrachloride Toxicity is one of a series. For other publications in this series, please use the order form on the back cover. For clinical inquiries, contact ATSDR, Division of Health Education, Office of the Director, at (404) 639–6204.
Answers to Pretest and Challenge Questions
Pretest
Pretest questions begin on page 1.
-
Acute hepatic necrosis and renal impairment can occur up to 2 weeks after a CCl4 exposure. Other secondary health effects reported include coagulation disorders, cardiac dysrhythmias, and pulmonary edema; these effects are not likely to resolve without improvement in the intercurrent kidney and liver disorders. Because of the patient’s multiple exposures to hepatotoxic agents (i.e., recent heavy consumption of ethanol and potential occupational exposure), acute treatment should begin as soon as possible as a preventive measure.
(NOTE: It is unclear whether the isopropyl alcohol spilled on the patient’s clothing will affect the patient’s medical condition. Reports of isopropyl alcohol’s ability to potentiate the harmful effects of CCl4 are based on inhalation studies in experimental animals. Significant inhalation of isopropyl alcohol in this case is unlikely since the solvent does not volatilize readily. Isopropyl alcohol also is not absorbed readily by intact skin.)
Most cases of fatal CCl4-induced hepatotoxicity involve persons with a history of heavy ethanol abuse. Although our patient consumed ethanol the night before the incident, he says he rarely imbibes, and most likely he has a healthy liver. Nevertheless, exposure to ethanol within 12 hours before CCl4 exposure will potentiate CCl4’s toxicity. If the patient survives the first 2 weeks, the prognosis is good for complete recovery or for only mildly compromised liver and kidney function.
-
Since samples were taken for analysis by the hazardous waste company, you should urge the company to complete this analysis as soon as possible. The history of the source plant as a chlorofluorocarbon manufacturer is suggestive of CCl4 use. When the company identifies the material, you may request a Material Safety Data Sheet (MSDS). MSDSs often do not adequately meet the clinician’s needs, however. More extensive documents, such as those in the Suggested Reading List, page 14, or the NIOSH Current Intelligence Bulletin for CCl4 may be more helpful.
-
Based on reports of treatment of patients with acetaminophen overdose, NAC given within approximately 12 hours after exposure may decrease the severity of both liver and kidney damage. Hemodialysis has been used in treating patients acutely exposed to CCl4, but its success in reversing the pathology of CCl4 has not been proven. Maintenance of normal hydration and a high protein diet (the latter only if tolerated) is suggested. Consultation with a gastroenterologist is indicated.
Challenge
Challenge questions begin on page 5.
-
The older man’s history of alcoholism and hepatitis B could put him at increased risk of CCl4’s adverse effects. Underlying liver damage would increase risk of acute effects and subsequent hepatocellular carcinoma. Although he was working in an appropriate protective suit and full-face respirator, it is unclear whether he has been exposed. His beard may have prevented proper fit of the respirator face piece. However, his symptoms could be due to working in a hot, enclosed space, or they may be psychophysiologic.
-
It is not clear that this woman has been exposed to CCl4. Her symptoms may be morning sickness associated with her pregnancy. However, it is important that she discuss this possible exposure with her obstetrician.
Although CCl4 is lipophilic and may readily pass through the placenta to the fetus after maternal exposure, CCl4 does not appear to be teratogenic in either animals or humans in the early stages of pregnancy. The human fetus typically develops the enzyme system necessary for the (toxic) metabolism of CCl4 in the later months of pregnancy. Although it would be important to know if the mother is exposed to other exogenous MFO-inducing agents, it is doubtful that the 6-week-old fetus has been significantly affected. Nevertheless, it would be prudent to inform the parents and medical-care provider of the possible consequence of in utero exposure.
-
Because the young man removed his respirator and presumably breathed the solvent for a prolonged time, he is at high risk. The odor was characterized as sweet smelling, which indicates that the air level was above 10 ppm (the CCl4 odor threshold). His prior ethanol intake and possibly his concurrent exposure to isopropyl alcohol increase his risk. Alcohols can induce production of MFO enzymes, thereby potentiating the formation of CCl4 toxic intermediates and metabolites.
-
See answer to Pretest question (a).
-
Initial actions include removing all contaminated clothing (since dermal absorption of some solvents is high) and cleansing the skin with mild soap and water. Care should be taken to prevent exposure of ED personnel to fumes from contaminated clothing; if possible, the patient should be decontaminated before entering the ED.
The following laboratory work-up is recommended for patients exposed to volatile solvents: baseline hepatic and renal function tests (i.e., SGOT [AST], SGPT [ALT], bilirubin, alkaline phosphatase, BUN, creatinine, electrolytes, and urinalysis), as well as PT, PTT, and CBC. Some solvents may cause dysrhythmias and pulmonary edema (probably secondary to renal toxicity); thus, a baseline electrocardiogram and chest X ray should be obtained. These tests should be repeated periodically to monitor the patient’s condition.
You may wish to send blood and urine for a toxic substance screen concentrating on hepatotoxic agents such as acetaminophen and ethanol. If a laboratory is available that performs head space analysis by gas chromatography, a sealed, refrigerated blood sample can be analyzed for volatile solvents. The likelihood of confirming a patient’s solvent exposure depends on the dose of solvent received, the time of sampling in relation to the time of exposure, and precautions taken during the collection and storage of the sample. Generally, analysis is most effective if performed within 24 hours after the exposure.
Appropriate public or occupational health reports should be filed. Some states may require that a doctor’s first report of illness be filed with the state health department. These reports are often overlooked by ED physicians.
-
See answer to Pretest question (c).
-
Immediate follow-up for the acutely ill patient consists of monitoring liver and kidney functions for up to 2 weeks. The patient’s cardiac and pulmonary systems and clotting ability should also be evaluated periodically since abnormalities can occur secondary to hepatic and renal damage. If the patient shows no improvement, liver biopsy may be considered since liver enzyme levels are not always reliable predictors of liver damage. Liver biopsy is contraindicated in patients with coagulation disorders.
Persons exposed to CCl4 who have survived without permanent physiologic damage have experienced nausea, dizziness, vision changes, abdominal pain, or delirium up to 24 hours after exposure. The patient’s two coworkers, however, may suffer effects because of their unique circumstances. See answers to Challenge questions 1 and 2.
All three persons (the patient and his two coworkers) should be counseled to avoid other hepatotoxic agents such as ethanol, drugs, solvents, and chlorinated compounds. The 40-year-old worker (with possible liver injury as a result of alcoholism and hepatitis B), who was discharged the morning after the incident, and the acutely ill 25-year-old patient may be at increased risk for hepatocellular carcinoma; they should be monitored periodically. It may be advisable for the 25-year-old patient to get the hepatitis B vaccine as a preventive measure. The 30-year-old woman, who used full protective gear and whose symptoms disappeared quickly, is probably at minimal risk. See Challenge question and answer 2.
-
It is important that the company establish a protocol for periodic health examinations of all employees. A complete exposure history for each employee should be maintained and made available to the physician. Under the OSHA Hazard Communication regulation (right-to-know provisions), MSDSs for hazardous chemicals in the workplace must be made available to the workers, their physician, and designated worker representative. All employees using a respirator should be fit-tested and all should be properly trained before entering a hazardous environment. Proper supervision is necessary at all times. Employees who are ill should not be allowed to remain at work, nor should employees be permitted to work without the requisite protective gear.


















