

30 Ethylene/Propylene Glycol Toxicity
|
Environmental ALERT…
|
This monograph is one in a series of self-instructional publications designed to increase the primary care provider’s knowledge of hazardous substances in the environment and to aid in the evaluation of potentially exposed patients. See page 23 for more information about continuing medical education credits and continuing education units.
|
Guest Contributor: |
Gary Pasternak, MD, MPH |
|
Guest Editor: |
Lewis Goldfrank, MD |
|
Peer Reviewers: |
John Ambre, MD, PhD; Charles Becker, MD; Jonathan Borak, MD; Alan Hall, MD; Richard J.Jackson, MD, MPH; Jonathan Rodnick, MD |
|
Air Force Peer Reviewers: |
Terence Lyons, MD, MPH; Bruce Poitrast, MD, MPH |

U.S. DEPARTMENT OF HEALTH & HUMAN SERVICES
Public Health Service
Agency for Toxic Substances and Disease Registry
Case Study
Disorientation, ataxia, and abdominal symptoms in visitors to a municipal airport
A 67-year-old man is brought to the Emergency Department (ED) of a small community hospital where you are the family physician on call. The patient is experiencing ataxia, dizziness, and vomiting. He is hyperventilating. On physical examination, the patient appears well nourished, agitated, and disoriented. There is no odor of ethanol on his breath. His vital signs include blood pressure, 120/80 mm Hg; temperature, 98.5°F; pulse, 80 beats/minute; and respirations, 40 breaths/minute. Neurologic examination is normal, and there is no nystagmus. Abdominal and cardiorespiratory examinations are also normal.
The patient was brought to the ED by his friend, who relates that the patient said he felt dizzy and began vomiting late last night. This morning he was hyperventilating and continued to vomit. Both men are retired pilots who teach at the ground school at the local airport. Because two other people had collapsed at the airport that morning and were taken by ambulance to another hospital, the friend wonders if the food at the airport cafeteria is responsible. Both he and the patient had hot dogs and coleslaw; yet the friend states that he feels fine.
Although the friend insists that the patient drank only water all day, you order a blood ethanol level, as well as a drug screen, arterial blood gases (ABG), serum electrolytes, BUN, creatinine, and glucose. Blood ethanol and drug screen are negative, and ABG results reveal pH 7.10; Paco21 20 mm Hg; and Pao2 95 mm Hg. Other test results are sodium, 145 mEq/L; potassium, 3.8 mEq/L; chloride, 105 mEq/L; bicarbonate, 8 mEq/L; BUN, 20 mg/dL; creatinine, 1.0 mg/dL; and glucose, 80 mg/dL. The calculated anion gap is 32 (normal 12 to 16).
Less than 30 minutes later, a 4-year-old boy is brought to the ED. On examination, you find a sleepy but arousable child. There is no evidence of trauma or focal neurologic signs. Abdominal and cardiorespiratory examinations are normal. Vital signs include rectal temperature, 97.8°F; respirations, 12 breaths/minute; pulse, 78 beats/minute; BP, 94/76 mm Hg. The parents tell you that they were attending a local fliers’ club luncheon at the airport. When they found the child staggering and incoherent, they rushed him to the ED; the child vomited in the car. You order the same laboratory tests for the child that you ordered for the 67-year-old patient. From the results of the child’s tests, you note that the child is hypoglycemic and slightly acidotic. You calculate an anion gap of 13.
You contact the local health department and are told that they are investigating the earlier incidents at the airport. They suspect that the airport’s water supply is contaminated, but they have not identified the contaminant.
![]()
(a) What would you include in each patient’s problem list? What is the differential diagnosis for an anion gap metabolic acidosis?
_________________________________________________________________
_________________________________________________________________
_________________________________________________________________
(b) What additional tests, if any, will you order for these patients?
_________________________________________________________________
(c) How will you initially treat these patients?
_________________________________________________________________
_________________________________________________________________
Answers to the Pretest questions are on page 21.
Glycol Properties
Ethylene glycol and propylene glycol are manufactured chemicals that have similar physical properties and uses. Their chemical structures differ by only one methyl group (ethylene glycol, HOCH2CH2OH; propylene glycol, CH3CH[OH]CH2OH). Both chemicals are clear, colorless, odorless, sweet-tasting, highly viscous liquids. They have low vapor pressures at room temperature, indicating low potential for inhalation exposure.
Despite similarities in physical properties and chemical structure, ethylene glycol and propylene glycol have vastly different toxicities. Ethylene glycol is acutely toxic to humans, whereas propylene glycol is a safe additive for foods and medications. Propylene glycol causes poisoning only rarely and under unusual circumstances. These glycols should not be confused with glycol ethers (e.g., ethylene glycol monomethyl ether, also known as methyl cellosolve, and ethylene glycol monoethyl ether), which are suspected reproductive and developmental toxicants. A discussion of ethylene glycol follows; discussion of propylene glycol begins on page 18.
Ethylene Glycol Exposure Pathways
❑ Antifreeze, which can contain up to 95% ethylene glycol, is the most common source of ethylene glycol overexposure.
Ethylene glycol is used in many industries because it has the ability to absorb water and to prevent overheating or freezing. It is used extensively in automotive fluids such as antifreeze, coolants, and hydraulic fluids. Antifreeze, which typically consists of 95% ethylene glycol, accounts for about 65% of the ethylene glycol produced. Ethylene glycol is also used in cosmetics, fat extractants, and as a chemical intermediate. As a solvent, it is found in inks, stains, pesticides, fire extinguishers, foams, polishes, and adhesives. Its heat-regulation properties are employed in air conditioning units and solar energy systems.
Synonyms for ethylene glycol include ethylene alcohol, glycol alcohol, glycol, 1,2-dihydroxyethane, and 1,2-ethanediol. Commercial products containing high concentrations of ethylene glycol include Dowtherm SR1*, Lutrol-9, Norkool, Tescol, and UCAR-17.
Waste streams produced when ethylene glycol is manufactured or used account for the most significant releases of this compound into
❑ Because of its low vapor pressure and poor skin absorption, ethylene glycol poisonings normally occur by ingestion.
the environment. In military and commercial aviation, large amounts of ethylene glycol are used for deicing. It is sprayed as an aerosol or mist onto airplane wings to prevent ice buildup. Used in this manner, ethylene glycol can contaminate groundwater near airports through runoff and may expose workers to air levels ranging from <0.05 milligrams per cubic meter (mg/m3) to 10.4 mg/m3 (i.e., <0.02 parts per million [ppm] to 4.2 ppm). The Occupational Safety and Health Administration (OSHA) ceiling limit (15-minute sample) for ethylene glycol is 125 mg/m3 or 50 ppm. Ethylene glycol is also used in coolant loops in spacecraft and in aviator protective clothing; both applications present potential for exposure if leaks occur.
❑ Ethylene glycol rapidly degrades in the environment.
Ethylene glycol does not persist in ambient air in large amounts because breakdown is rapid (half-life in air is 24 to 50 hours). Its low vapor pressure precludes substantial inhalation exposure at ambient temperatures, and its poor skin absorption prevents significant absorption after dermal contact. Ethylene glycol is miscible with water and adheres to soil (half-life in water and soil is several days). Because it is not fat-soluble, bioconcentration and bioaccumulation are insignificant.
|
(1) What questions would health department investigators ask airport visitors and employees to establish the exposure source? _________________________________________________________________ _________________________________________________________________ _________________________________________________________________ |
Who’s at Risk
❑ Workers in industries producing or using products that contain ethylene glycol are at greatest risk of exposure.
Workers in industries that manufacture or use products containing ethylene glycol, particularly operations involving automobile maintenance and aircraft deicing, are at greatest risk of exposure. Although dermal contact is the main route of occupational exposure, vapors or mists can be inhaled when the chemical is heated, agitated, or sprayed.
❑ The general population has risk of exposure to ethylene glycol primarily through contact with automobile antifreezes and coolants.
There have been no reports of adverse health effects from chronic environmental exposures to ethylene glycol, and few data exist to evaluate such effects from these exposure scenarios. In the general population, ethylene glycol exposure occurs most commonly through accidental or intentional ingestion of antifreeze. During 1990, 3,242 cases of ethylene glycol exposure were reported to the 72 poison centers participating in the National Data Collection System of the American Association of Poison Control Centers. Of these, 1,451 patients (45%) were examined in health care facilities, 1,147 (35%) became symptomatic, 62 (2%) developed major symptoms, and 5 (0.2%) died. The remainder (577[17.8%]) suffered no ill effects. The general population can also be exposed to ethylene glycol by dermal contact while handling automotive antifreezes, coolants, and brake fluids; however, such exposure is not likely to cause adverse health effects under normal conditions.
Biologic Fate
❑ Absorption of ethylene glycol by the gastrointestinal tract is rapid; dermal absorption is slow. Inhalation is not an important route of exposure under normal conditions of use.
Ethylene glycol is rapidly absorbed by the gastrointestinal tract, less rapidly by the lungs, and slowly through the skin. Because of ethylene glycol’s low vapor pressure, inhalation is generally not associated with toxicity, although neurologic symptoms including nystagmus and syncope were reported in factory workers chronically exposed to vapor from heated ethylene glycol.
Because it is highly water-soluble, ethylene glycol is evenly distributed throughout the body. It reaches peak tissue levels 1 to 4 hours after ingestion. Approximately 24 hours later, no unchanged ethylene glycol is detected in urine or tissues, indicating rapid biotransformation. The normal serum half-life of ethylene glycol is approximately 2.5 hours.
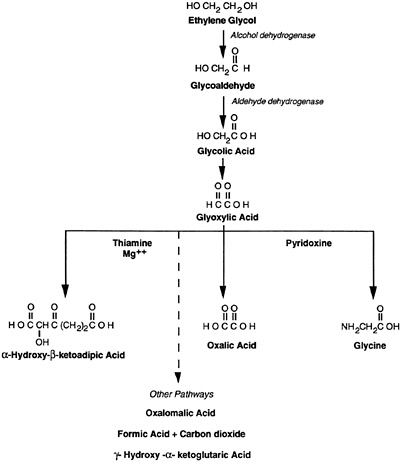
❑ Ethylene glycol is metabolized in the liver to a variety of more toxic compounds.
Although ethylene glycol itself has relatively low toxicity, it is metabolized in the liver to a variety of toxic compounds (Figure 1), some of which have elimination half-lives of up to 12 hours. The rate-limiting step in this metabolic process is the conversion of ethylene glycol to glycoaldehyde. Generally, only a small fraction of ethylene glycol (less than 20% in low-dose ingestions) is excreted unchanged in the urine. However, coadministration of ethanol, which inhibits ethylene glycol metabolism by preferentially reacting with alcohol dehydrogenase, can extend the serum half-life of ethylene glycol to 17 hours and increase the percentage of ethylene glycol that is ultimately excreted unchanged. This mechanism is the basis for the antidotal use of ethanol in ethylene glycol-poisoned patients.
❑ Only a small fraction of absorbed ethylene glycol is normally excreted unchanged in the urine.
Persons who have impaired liver or kidney function, and children, who have immature hepatic detoxification systems, may be at greater risk of ethylene glycol’s initial central nervous system (CNS) effects. However, the clinical courses of illness in such patients may be less severe because of decreased abilities to form toxic metabolites.
|
Additional information for the case study: The health department identifies the water contaminant as ethylene glycol. When construction crews at the airport were repairing the water supply system, they inadvertently connected the water from the heating system to the drinking water system. The concentration of ethylene glycol measured at the cafeteria’s water source was 9%, or 90,000 ppm. The Environmental Protection Agency (EPA) has a drinking water quality guideline of 7 ppm for ethylene glycol. The lethal dose of 95% ethylene glycol is about 100 mL. (2) Who in the case study may be at risk of adverse health effects? Explain. _________________________________________________________________ _________________________________________________________________ _________________________________________________________________ _________________________________________________________________ |
Physiologic Effects
Neurobehavioral Effects
❑ Unmetabolized ethylene glycol contributes to CNS depression.
The aldehyde metabolites of ethylene glycol are the cause of many of ethylene glycol’s delayed toxic effects. These metabolites inhibit oxidative phosphorylation; cellular respiration; and glucose, protein, and serotonin metabolism. In addition, accumulation of glycolic acid, glyoxylic acid, and, to a lesser extent, oxalic acid, results in metabolic acidosis. (Lactic acid formed during the metabolism of ethylene glycol to oxalic acid also contributes to the metabolic acidosis in patients poisoned by this glycol.)
❑ Delayed clinical toxicity results from the conversion of ethylene glycol to more toxic metabolites.
Ethylene glycol poisoning typically has three phases (Table 1). Phase 1, which begins 30 minutes to 12 hours after ingestion, includes signs of inebriation and CNS depression from unmetabolized ethylene glycol and from aldehyde metabolites that peak 6 to 12 hours after ingestion. In some cases, cerebral edema develops. Signs of metabolic acidosis may become apparent late in Phase 1.
Table 1. Clinical course in acute ethylene glycol intoxication
|
Phase |
Onset After Ingestion |
Primary Systems Affected |
Signs and Symptoms |
|
1 |
30 minutes to 12 hours |
CNS |
Ataxia, nystagmus, coma, myoclonus, seizures |
|
|
|
Gastrointestinal |
Nausea, vomiting |
|
2 |
12 to 24 hours |
Cardiovascular |
Mild hypertension, tachycardia, shock |
|
Pulmonary |
Tachypnea, adult respiratory distress syndrome, pulmonary edema, pneumonitis |
||
|
Metabolic |
Metabolic acidosis with elevated anion and osmolal gaps, possible tetany from hypocalcemia, and hyperventilation |
||
|
3 |
24 to 72 hours |
Renal |
Flank pain, costovertebral angle tenderness, oliguric renal failure, hyperkalemia |
Phase 2, the cardiopulmonary toxicity phase, begins 12 to 24 hours after ingestion. Deposition of calcium oxalate crystals can cause tissue injury in various sites including the meninges of the brain, vascular tree, myocardium, and lung parenchyma. Hypocalcemia may occur secondary to the precipitation of calcium by the oxalate metabolite.
Phase 3, which begins 24 to 72 hours after ingestion, can be manifested by a profound metabolic acidosis. Deposition of calcium oxalate crystals in the kidneys can lead to acute renal failure (irreversible in some cases) and hyperkalemia.
The minimum lethal ingested dose of antifreeze (95% ethylene glycol) for adults is approximately 1.4 mL/kg body weight or about 100 mL of antifreeze for a 70-kg person, although persons who attempted suicide by ingesting 1 to 2 liters of the 95% solution and were treated within 1 hour have survived.
Neurologic Effects
❑ Signs of inebriation are among the first to appear after ethylene glycol ingestion. Any delay in initiating supportive and specific treatment may cause increased severity of adverse effects.
The initial phase of ethylene glycol poisoning is characterized by inebriation caused by unmetabolized ethylene glycol. In acute poisoning, ataxia, slurred speech, and somnolence are common, as are irritation, restlessness, and disorientation. Cerebral edema and crystalline deposits of calcium oxalate in the walls of small blood vessels in the brain may increase CNS depression. In severe poisonings, myoclonic jerks, convulsions, and coma can occur.
Several case reports of acute ethylene glycol poisoning have described effects on cranial nerves (e.g., facial paralysis, hearing loss, and bilateral visual disturbances) that occurred 5 or more days after ingestion. These sequelae, however, are not seen often; delay in instituting treatment may contribute to their development.
Respiratory Effects
❑ Ingestion of ethylene glycol can cause noncardiogenic pulmonary edema.
Pulmonary effects typically occur 12 to 72 hours after ingestion and may include hyperventilation, respiratory distress syndrome, pneumonitis, and noncardiogenic pulmonary edema. Oxalate crystals in lung parenchyma have been found at autopsy in some ethylene glycol-poisoned patients.
In one study, volunteers who inhaled aerosolized ethylene glycol at a mean concentration of 31 mg/m3 (12.4 ppm) for 20 to 22 hours per day for 4 weeks experienced throat and upper respiratory-tract irritation. Potential for long-term exposure to ethylene glycol exists in spacecraft if cooling systems leak.
Cardiovascular Effects
❑ Ethylene glycol ingestion can produce conduction disturbances and cardiac dysrhythmias.
Cardiovascular effects occur most often in conjunction with respiratory compromise. Deposition of calcium oxalate crystals in the vascular tree and in cardiac tissue may cause the mild hypertension or hypotension and dysrhythmias experienced by patients severely poisoned with ethylene glycol.
Metabolic Effects
❑ Patients who have ethylene glycol poisoning characteristically have an elevated anion gap and osmolal gap.
If large doses of ethylene glycol are ingested, poisoning is accompanied by metabolic acidosis, with onset occurring within 24 hours after ingestion. This acidosis is caused primarily by the accumulation of glycolic and glyoxylic acids, although oxalic acid and excess lactic acid may be contributing factors. These acidic metabolites release hydrogen ions, which react with bicarbonate, decreasing the pH in serum and other body fluids. An elevated anion gap results. In addition, ethylene glycol is osmotically active, thereby causing an increased measured osmolal gap. (Osmolality is the osmotic concentration, defined as the moles of solute divided by the number of particles into which it dissociates per kilogram of solvent.)
Tetany can sometimes occur due to hypocalcemia. Hypocalcemia results from precipitation of calcium by the oxalate formed during ethylene glycol metabolism.
Renal Effects
❑ Nephrotoxicity is the dominant effect of serious ethylene glycol poisoning.
Nephrotoxicity manifests about 24 to 72 hours after substantial ingestion of ethylene glycol. It results from precipitation of calcium oxalate crystals in renal tubules and from the direct cytotoxic action of ethylene glycol metabolites (e.g., oxalic and glycolic acids). Interstitial changes in the kidney are accompanied by acute tubular necrosis. In most cases, the renal injury resolves after recovery; however, it can be irreversible.
Other Effects
❑ Ethylene glycol is a skin and mucous membrane irritant.
Ethylene glycol is only a minor skin irritant, although a few cases of allergic contact dermatitis have been documented. Acute iridocyclitis has been reported after accidental eye contact with the liquid.
No studies in experimental animals have linked ethylene glycol to cancer. One epidemiologic study found an elevated odds ratio for renal cancer in workers exposed to ethylene glycol; however, these workers may have been exposed to other chemicals also.
❑ Data are inadequate to determine whether ethylene glycol is a carcinogen or a reproductive hazard in humans.
Studies in experimental animals do not indicate that ethylene glycol causes developmental effects. Although studies in humans have not specifically addressed effects on the fetus, adverse reproductive or developmental outcomes in humans have not been reported.
|
(3) A week after the water contamination incident, a patient comes to your office. He deices airplanes at the airport and was involved in a major spill yesterday when he was drenched with deicing fluid. He knows that deicing agents contain large amounts of ethylene glycol. He immediately showered and changed clothes after the incident, but he is worried about possible adverse health effects; he wonders if cancer could develop. What will you tell him? _________________________________________________________________ _________________________________________________________________ _________________________________________________________________ (4) A pregnant worker at the airport consults you because she drank tea made with the contaminated water. Although she consumed only a small amount of tea and had no ill effects, she is worried that her fetus will be adversely affected. How will you counsel her? _________________________________________________________________ _________________________________________________________________ _________________________________________________________________ |
Clinical Evaluation
History and Physical Examination
❑ A detailed history is important in diagnosing ethylene glycol poisoning.
Ethylene glycol ingestion is a medical emergency requiring prompt recognition and aggressive treatment for a good outcome. The clinical picture in ethylene glycol poisoning varies based upon the amount ingested, the time elapsed since ingestion, and the concurrent ingestion of large amounts of ethanol. Making a correct decision regarding treatment requires a reliable history of the time, route, and magnitude of exposure. However, a detailed history can be difficult to obtain because patients often have an altered mental state. If ethylene glycol poisoning is strongly suspected, supportive and specific treatment should be instituted pending confirmatory laboratory results.
❑ Prompt recognition and early therapeutic intervention are essential to preventing latent effects and potential sequelae of ethylene glycol poisoning.
Although there is concern about environmental exposures to ethylene glycol, nearly all cases of ethylene glycol poisoning are due to ingestions. A history of alcohol abuse may suggest ingestion of ethylene glycol as an ethanol substitute. A meticulous search in the home for ethylene glycol-containing compounds should be made in all suspected poisonings. If a product label does not list the chemical ingredients, the regional poison control center may be able to assist. Inquiring about similar symptoms in family members, friends, and coworkers may be helpful in identifying a common source of exposure.
The patient’s vital signs should be monitored. Although not specific for ethylene glycol intoxication, hypertension, tachycardia, and low-grade fever have been associated with moderate or severe poisoning. A complete neurologic examination should be performed with special attention directed to gait and balance.
Numerous exogenous toxic substances are associated with an elevated anion gap (Table 2). Only four conditions will cause metabolic acidosis and elevate both the anion and osmolal gaps— methanol poisoning, ethylene glycol poisoning, alcoholic ketoacidosis, and diabetic coma. However, when large quantities of ethanol are ingested concomitantly with ethylene glycol, enzymatic conversion to toxic metabolites that produce metabolic acidosis will be inhibited. Inhibiting metabolism also increases the amount of unchanged ethylene glycol circulating in the body. Hence, a patient who has concomitantly ingested ethanol could have an elevated osmolal gap without an elevated anion gap early in the clinical course. The presence of metabolic acidosis and either an anion or osmolal gap should alert the clinician to the possibility of ethylene glycol poisoning.
Table 2. Common toxic agents associated with an elevated anion gap
|
Substance |
CNS Depression |
Metabolic Acidosis |
Ketosis |
Increased Osmolality |
Characteristic Findings |
|
Methanol |
+ |
++ |
− |
+ |
Blindness, pink edematous optic disk |
|
Ethanol |
+ |
+ |
+ |
+ |
Alcoholic ketoacidosis |
|
Ethylene glycol |
+ |
++ |
− |
+ |
Renal failure, calcium oxalate and hippurate crystals, noncardiogenic pulmonary edema |
|
Isopropanol |
+ |
− |
++ |
+ |
Hemorrhagic tracheobronchitis and gastritis |
|
Salicylates |
+ |
+ |
+ |
− |
Vomiting, tinnitus, hyperthermia |
|
Adapted from Goldfrank LR. Goldfrank’s toxicologic emergencies. 4th ed. Norwalk, Connecticut: Appleton and Lange, 1990:483. |
|||||
Signs and Symptoms
❑ Patients with ethylene glycol poisoning may initially appear inebriated and may lack severe toxic manifestations.
Patients who have ingested ethylene glycol often progress through three clinical phases. These phases represent a continuum, and an individual patient may have any combination of organ or systemic effects (Table 1, page 7). The time course for each phase, as well as the severity of illness, is dependent on the amount of ethylene glycol ingested and whether ethanol was ingested concurrently.
CNS signs and symptoms predominate during the first 12 hours, including headache, slurred speech, dizziness, ataxia, myoclonic jerks, convulsions, coma, and death. In mild cases, the patient may appear inebriated but have no ethanol odor on the breath. Abdominal pain with nausea and vomiting is common.
❑ After a characteristic latent period, metabolites of ethylene glycol can cause potentially life-threatening illness.
Phase 2 begins 12 to 24 hours after ingestion and is caused by the products of ethylene glycol metabolism. The primary manifestations are cardiopulmonary with tachypnea, tachycardia, dysrhythmias, hypertension or hypotension, respiratory distress syndrome, and pulmonary edema. Profound metabolic acidosis may be present.
Phase 3 occurs 24 to 72 hours after ingestion if the condition is not treated or is treated unsuccessfully. Acute renal dysfunction secondary to acute tubular or cortical necrosis is seen. Renal dysfunction varies from mild elevation in BUN to overt oliguric renal failure. The renal failure usually resolves but may be irreversible in some cases. Myopathy and bone marrow suppression have also been reported.
In some cases, facial paralysis and other cranial-nerve abnormalities may occur several days after ingestion. These neurologic sequelae are usually found when treatment is delayed or inadequate.
Laboratory Tests
❑ An elevated anion-gap metabolic acidosis and an elevated osmolal gap combined with urinary crystals suggest ethylene glycol poisoning.
❑ Measurement of serum ethylene glycol levels can confirm poisoning.
The abnormal laboratory findings in ethylene glycol poisoning include an elevated anion-gap metabolic acidosis, an increased osmolal gap, elevated serum ethylene glycol level, calcium oxalate or hippurate crystalluria, and sometimes, hypocalcemia. Arterial blood gases, blood glucose, serum electrolytes, and blood ethanol should be measured in all patients with histories of ethylene glycol ingestion or in whom poisoning is suspected. Results of these laboratory tests will confirm the presence and degree of metabolic acidosis and allow calculation of the anion and osmolal gaps (Table 3). A blood ethanol level will establish whether initial CNS symptoms are due to ethanol. The presence of ethanol will also have a substantial impact on metabolism and therapy.
Table 3. Formulas for calculating anion and osmolal gaps
|
The serum anion gap (AG) is determined from serum electrolytes measured in mEq/L and may be defined by the formula AG=(Na++K+)−(Cl−+HCO3−) (Normal anion gap: 12 to 16) The serum osmolal gap (OG) is most commonly approximated by the formula OG=Osmolality(measured)*−2Na++[BUN÷2.8]+[Glucoses÷18] (Normal osmolal gap: <10) |
|
*In this formula, Osmolality(measured) is obtained by the freezing-point-depression method and expressed in milliosmoles per liter (mOsm/L); Na+ in mEq/L; BUN and glucose in mg/dL. |
The presence of calcium oxalate or hippurate crystals in the urine, together with an elevated anion gap or osmolal gap, strongly suggests ethylene glycol poisoning. Urinary crystals result from the precipitation of calcium by the oxalic acid metabolite of ethylene glycol or from the reaction of the glycine metabolite with benzoic acid, which forms hippuric acid. The crystals can take many forms including dumbbells, envelopes, or most commonly, needles. Absence of urinary crystals, however, does not rule out poisoning. Because some antifreeze products contain fluorescein, the urine may fluoresce under a Wood’s lamp.
An elevated serum level of ethylene glycol confirms ethylene glycol poisoning; significant toxicity is associated with levels greater than 50 mg/dL. Communication with the laboratory is critical in poisoning cases because 2,3-butanediol often found in the plasma of alcoholics can be mistakenly identified as ethylene glycol when the analysis is performed by gas chromatography. Furthermore, propylene glycol may interfere with some assays for ethylene glycol.
|
(5) What additional laboratory tests will you order for the man and child described in the case study on page 1? _________________________________________________________________ _________________________________________________________________ _________________________________________________________________ |
Treatment and Management
❑ Correction of metabolic acidosis is an important part of treatment in ethylene glycol poisoning.
Treatment should not be delayed pending results of ethylene glycol serum levels if the clinical picture is severe or if the history suggests such poisoning. Treatment advice can be obtained from a regional poison control center or medical toxicologist
Initial management of suspected poisoning includes basic life support with intubation and mechanical ventilation if required. When the ingestion is recent, measures to prevent ethylene glycol absorption
should be taken if the patient’s level of consciousness permits. Induced emesis or gastric lavage may be useful if ingestion occurred within 1 to 2 hours. Activated charcoal is not likely to be effective because it does not adsorb ethylene glycol well.
❑ Specific treatments for ethylene glycol poisoning are ethanol therapy and hemodialysis.
Specific treatment for ethylene glycol poisoning consists of sodium bicarbonate to correct the metabolic acidosis, ethanol to competitively inhibit conversion of ethylene glycol to its more toxic metabolites, and hemodialysis to remove ethylene glycol and glycolic acid. Although this treatment regimen is effective in most cases, renal failure and death can occur if treatment is delayed.
Ethanol is used to saturate the alcohol dehydrogenase enzyme so that ethylene glycol is maintained in an unmetabolized form and excreted unchanged in the urine. Ethanol therapy should be considered when ethylene glycol levels are greater than 20 mg/dL or when ethylene glycol poisoning is strongly suspected. Patients who have a history of concurrent ethanol ingestion, or who are undergoing hemodialysis, require dosage modification (Table 4). Ethanol can cause hypoglycemia, particularly in children; therefore, blood glucose should be monitored closely. The hypoglycemia that develops in adults is often overlooked because the impairment of mental status is attributed to the ethanol.
Table 4. Intravenous administration of ethanol in ethylene glycol and methanol poisoning
|
Goal of ethanol therapy: Maintain blood ethanol level between 100 and 150 mg/dL |
||
|
Loading dose |
mg/kg |
mL of 10% ethanol/kg |
|
600 to 800 |
7.6 to 10 |
|
|
Maintenance dose |
mg/kg/hr |
mL of 10% ethanol/kg/hr |
|
Chronic alcoholic |
154 |
1.95 |
|
Social drinker |
110 |
1.39 |
|
Nondrinker |
66 |
0.83 |
|
During hemodialysis* |
mg/kg/hr |
mL of 10% ethanol/kg/hr |
|
Chronic alcoholic |
304 |
3.85 |
|
Social drinker |
256 |
3.29 |
|
Nondrinker |
216 |
2.73 |
|
*Assuming no ethanol is added to dialysis bath. Adapted from Hall AH. Ethylene glycol and methanol: poisons with toxic metabolic activation. Emergency medicine reports 1992;13(4):29–38. |
||
The loading dose and the maintenance dose should be infused over the first hour of therapy. Decrease to only the maintenance dose in the second hour. If the drinking habits of a patient cannot be determined from the history, assume the patient is in the category of “social drinker,” then adjust the dose to achieve a blood ethanol level that remains between 100 and 150 mg/dL.
To prepare 1 liter of 10% ethanol in 5% dextrose in distilled water (D5W) for intravenous infusion, perform either of the following steps:
-
Remove 100 mL of fluid from 1 liter of D5W; replace with 100 mL of absolute ethanol, or
-
Remove 50 mL of fluid from 1 liter of commercially available 5% ethanol in D5W solution; replace with 50 mL of absolute ethanol.
Blood ethanol and serum glucose levels should be monitored at the end of the loading dose and hourly until the maintenance dose is adjusted. Both should then be monitored two to three times daily, but more frequently during dialysis.
Hemodialysis should be considered if serum ethylene glycol levels exceed 50 mg/dL, if severe acid/base or fluid/electrolyte disturbances persist despite decontamination and ethanol therapy, or if renal failure develops. Hemodialysis should be continued until acidosis is controlled and the serum ethylene glycol level is in the 10 to 15 mg/dL range. Ethanol therapy can be discontinued when the serum ethylene glycol level is below this range.
Thiamine and pyridoxine, two water-soluble B complex vitamins that act as metabolic cofactors, are commonly administered to patients who have ethylene glycol toxicity. Pyridoxine is administered intravenously (100 mg or 1 mg/kg daily until intoxication is resolved). If the vitamins are administered before dialysis, the dose should be repeated after dialysis because they are highly water-soluble and are likely to be removed by the procedure. Thiamine is administered intravenously (100 mg or 1 mg/kg daily) until intoxication is resolved. These cofactors help convert ethylene glycol to less toxic metabolites and may decrease the formation of oxalate.
4-Methylpyrazole is a specific inhibitor of the alcohol dehydrogenase enzyme. It has low toxicity and may replace ethanol in the treatment of ethylene glycol poisoning. At present, 4-methylpyrazole is undergoing clinical trials and is available in the United States only for investigational use.
|
Additional information for the case study: It was later determined that during dinner at the cafeteria, the 67-year-old man had consumed several cups of coffee, while his friend, who did not become ill, drank only soda from a can. The serum ethylene glycol level for the 67-year-old patient is 55 mg/dL; the anion gap is 35. (6) How will you treat the 67-year-old patient? _________________________________________________________________ _________________________________________________________________ _________________________________________________________________ Additional information for the case study: The child’s ethanol level is 85 mg/dL. You repeat the ethanol test, and again the result is high. The parents are incredulous but admit that the child was not supervised closely during the luncheon, where wine and cocktails were served. Potential ethylene glycol exposure sources for the child could not be identified. (7) How will you treat the child? _________________________________________________________________ _________________________________________________________________ _________________________________________________________________ |
Standards and Regulations
Workplace
OSHA has recognized the respiratory irritation potential of ethylene glycol vapors by setting an exposure limit of 50 ppm (125 mg/m3) as a ceiling (15-minute sample). The American Conference of Governmental Industrial Hygienists (ACGIH) recommends the same occupational exposure limit.
Environment
Water
The U.S. Environmental Protection Agency (EPA) has an advisory of 7 mg/L or 7 ppm ethylene glycol in drinking water.
Food
The Food and Drug Administration (FDA) has approved ethylene glycol as a component of adhesives used in packaging.
State Guidelines
Some states have defined acceptable ambient air concentrations for ethylene glycol ranging from zero for California to the Texas standard of 1.4 ppm (3.9 mg/m3) for 30 minutes. Arizona has a drinking water quality guideline of 5,500 µg/L (5.5 ppm); Connecticut has a drinking water quality standard of 100 µg/L (0.1 ppm). Vermont has an enforcement standard of 7.0 mg/L (7.0 ppm) for groundwater.
|
Additional information: The community is worried that the deicing fluid spilled at the airport will contaminate the groundwater supply. They call a town meeting and ask you to speak on the health hazards of ethylene glycol and the regulations governing its presence in air and water. (8) Where can you find more information on ethylene glycol, and what will you tell the community? _________________________________________________________________ _________________________________________________________________ _________________________________________________________________ |
Propylene Glycol Exposure Pathways
❑ Propylene glycol is used in various foods, cosmetics, and pharmaceutical products.
FDA classifies propylene glycol as a Generally Recognized as Safe (GRAS) additive. Propylene glycol acts as an emulsifying agent, humectant, surfactant, and solvent in certain medicines, cosmetics, and food products. Concentrations in foods range from <0.001% in eggs and soups to about 15% in some seasonings and flavorings. The largest amounts of propylene glycol are used in the textile industry, where it is an intermediate in polyester fiber production. Synonyms for propylene glycol include 1,2-propanediol, 1,2-dihydroxypropane, methyl glycol, and trimethyl glycol.
The military uses aerosolized propylene glycol as a smoke screen on the battlefield to conceal the movement of troops. Because it can provide dense smoke without flames, it is also a smoke simulator in various types of fire-training materials. Propylene glycol is sometimes used as a deicing agent; however, ethylene glycol is used more often because it costs less. Propylene glycol is an FDA-approved additive for military dietary rations.
In the general population, propylene glycol exposure occurs primarily through ingestion of food and medications and through dermal contact with cosmetics or topical medications. No adverse health effects are likely to occur from normal use of these products.
Who’s at Risk
❑ Propylene glycol toxicity is not expected in normal environmental or occupational exposures.
Propylene glycol toxicity has been reported only rarely and in unusual circumstances involving medical applications such as intravenous injection or prolonged dermal contact during treatment of burns. (See Physiologic Effects, page 19.)
Biologic Fate
❑ Propylene glycol is metabolized to compounds that are normal constituents of the citric acid cycle.
Absorption of propylene glycol from the gastrointestinal tract is rapid, with maximal plasma concentrations in humans occurring within 1 hour after ingestion. Propylene glycol is metabolized in the liver by alcohol dehydrogenase to lactic acid, then to pyruvic acid. Both of these metabolites are normal constituents of the citric acid cycle and are further metabolized to carbon dioxide and water. About 45% of an absorbed propylene glycol dose is excreted by the kidneys unchanged or as the glucuronide conjugate. The elimination half-life of propylene glycol is about 4 hours.
Physiologic Effects
❑ Large doses and unusual circumstances are necessary for the development of propylene glycol toxicity.
CNS depression is the primary manifestation of acute propylene glycol poisoning. Metabolic conversion of propylene glycol to lactic and pyruvic acids can contribute to metabolic acidosis with an abnormal anion gap. Unchanged propylene glycol circulating in the body causes hyperosmolality.
❑ Propylene glycol poisoning is marked initially by CNS depression and an elevated osmolal gap, and later by an increased anion gap.
Although propylene glycol is nontoxic under normal conditions, it can cause poisoning in rare and unusual circumstances. In one case, an 8-month-old infant with large surface area second- and third-degree burns was treated for many days with topical silver sulfadiazine containing a large amount of propylene glycol. The infant developed acute metabolic acidosis and cardiorespiratory arrest. The dose of propylene glycol was 9,000 mg/kg/day. Serum propylene glycol levels were highest on day 14 (1,059 mg/dL) when the osmolal gap was 75 mOsm/L (normal: <10 mOsm/L).
❑ Unlike ethylene glycol, propylene glycol does not produce nephrotoxicity in humans.
Propylene glycol is a common diluent for injectable medications and constitutes 40% of the intravenous form of phenytoin. This high concentration is necessary to maintain a stable preparation and to prevent precipitation of phenytoin crystals. In some patients given intravenous phenytoin, propylene glycol was reported to cause hypotension, cardiac conduction disturbances, and cardiac dysrhythmias; fatal cardiac and respiratory arrests have been reported.
Propylene glycol has not been associated with nephrotoxicity in humans. Unlike ethylene glycol, propylene glycol is not metabolized to oxalic acid with subsequent deposition of calcium oxalate in the kidneys.
Clinical Evaluation, Treatment, and Management
❑ Treatment for propylene glycol poisoning is supportive and involves hemodialysis and correction of metabolic acidosis using sodium bicarbonate therapy.
Although the toxicity of propylene glycol is low, if large amounts are absorbed, an elevated osmolal gap may result. Because propylene glycol is metabolized to lactic acid, ingestion of massive doses of propylene glycol can cause severe metabolic acidosis. Coma, seizures, and hypoglycemia rarely develop in patients with propylene glycol intoxication. Cardiac monitoring is needed if other symptoms are present.
Metabolic acidosis caused by ingestion of large amounts of propylene glycol can be corrected with sodium bicarbonate therapy. Hemodialysis is effective in correcting hyperosmolality by removing propylene glycol from the blood. Ethanol therapy, as described for ethylene glycol-poisoned patients, is unnecessary for patients with propylene glycol poisoning.
Standards and Regulations
There are no workplace or environmental standards for propylene glycol. FDA considers an average daily dietary intake of 23 mg/kg of body weight to be safe for persons 2 to 65 years of age.
Suggested Reading List
General
Gabow PA, Clay K, Sullivan JB, et al. Organic acids in ethylene glycol intoxication. Ann Intern Med 1986;105(1):16–20.
Miller W. Ethylene glycol toxicity. Del Med J 1990;62(10):1267–72.
Factor SA, Lava NS. Ethylene glycol intoxication: a new stage in the clinical syndrome. NY State J Med 1987;87(3):179–80.
Ford M, Goldfrank LR. Alcohols and glycols. In: Rippe JM, Irwin RS, Alpert JS, Fink MP, eds. Intensive care medicine. 2nd ed. Boston: Little, Brown and Co., 1991:1160–73.
Jacobsen D, Dewlett TO, Webb R, et al. Ethylene glycol intoxication: evaluation of kinetics and crystalluria. Am J Med 1988;94(1):145–52.
Jacobsen D, McMartin KE. Methanol and ethylene glycol poisonings: mechanisms of toxicity, clinical course, diagnosis and treatment . Med Toxicol 1986;1(5):309–34.
Momont SL, Dahlberg PJ. Ethylene glycol poisoning. Wis Med J 1989;88(9):16–20.
Winek CI, Shingleton DP, Shanor SP. Ethylene and diethylene glycol toxicity. J Toxicol Clin Toxicol 1978;13(2):297–324.
Treatment
Baud FJ, Galliot M, Astier A, et al. Treatment of ethylene glycol poisoning with intravenous 4-methylpyrazole. N Engl J Med 1988;319:97–110.
Cheng JT, Beysolow TD, Kaul G, et al. Clearance of ethylene glycol by kidneys and hemodialysis. J Toxicol Clin Toxicol 1987;25(1&2):95–108.
Malmlund HO, Berg A, Karlman G, et al. Considerations for the treatment of ethylene glycol poisoning based on analysis of two cases. J Toxicol Clin Toxicol 1991;29(2):231–40.
Stokes JB III, Aueron F. Prevention of organ damage in massive ethylene glycol ingestion. JAMA 1980;243:2065–6.
Government Publications
Agency for Toxic Substances and Disease Registry. Technical report for ethylene glycol/propylene glycol [draft]. Atlanta: US Department of Health and Human Services, Public Health Service, 1992.
Sources of Information
More information on the adverse effects of ethylene glycol and propylene glycol and treating cases of exposure to these glycols can be obtained from ATSDR, your state and local health departments, and university medical centers. Case Studies in Environmental Medicine: Ethylene/Propylene Glycol Toxicity is one of a series. To obtain other publications in this series, please use the order form on the inside back cover. For clinical inquiries, contact ATSDR, Division of Health Education, Office of the Director, at (404) 639–6204.
Answers to Pretest and Challenge Questions
Pretest questions are on page 1. Challenge questions begin on page 3.
Pretest
-
The man’s problem list includes ataxia, vomiting, agitation, disorientation, hyperventilation, and an elevated anion-gap metabolic acidosis. The child’s problem list includes somnolence, ataxia, mental status changes, vomiting, hypoglycemia, low body temperature, and an anion-gap metabolic acidosis.
Common toxic agents associated with an elevated anion gap are shown in Table 2 on page 11.
-
Additional testing of these patients should include urinalysis, complete blood count, serum osmolality measured by the freezing-point-depression technique, ethylene glycol and methanol levels, and liver function tests.
-
Treatment for the 67-year-old man is found in Challenge answer 6 on page 22. Additional information on the condition of the child is in Additional Information for Challenge question 7, page 16. Treatment for the child is discussed in Challenge answer 7 below.
Challenge
-
The most common sources in epidemic poisonings include contaminated food, beverages, and water supplies. The investigators would inquire about types of food and drink available at the airport. They would take a detailed history of food and beverage intake from the patients and all others at the airport, in an attempt to find a common factor that would include those who were ill and exclude those who did not become ill. By gathering such data from a large number of people and statistically analyzing the data, the exposure source can usually be identified or possibilities restricted.
-
The lethal dose of antifreeze (95% ethylene glycol) is about 100 mL, although there is wide variation among reported cases. A cup (240 mL) of the contaminated water would contain about 22 mL of ethylene glycol. This dose could cause significant toxicity. Even mild symptoms of ethylene glycol poisoning would be a concern for air traffic controllers and other airport personnel responsible for judgments affecting many lives. All employees and visitors who consumed beverages or food prepared using water at the airport should be examined.
-
Absorption of ethylene glycol is slow through intact skin. Because the patient showered and changed clothes immediately, it is unlikely that he will experience toxic effects from the spill. In the case of chronic exposure during the deicing process, few particles from a spraying device are likely to be respirable, so inhalation of ethylene glycol would be minimal. Contact during the deicing process would not contribute substantially to toxicity, especially if protective clothing and respiratory protection were used. There is no evidence that ethylene glycol causes cancer in humans.
-
You can inform the patient that although no studies in humans specifically assess the effects of ethylene glycol on fetal development, no reports in humans suggest adverse outcomes. In addition, studies in experimental animals indicate that ethylene glycol does not cause developmental effects.
-
See Pretest answer (b) above. No test for methanol is necessary if it is established that the water was contaminated with ethylene glycol.
-
Several hours have passed since the ingestion, and emesis or gastric lavage will be of little value. Activated charcoal is likely to be ineffective. However, it is important to act promptly to correct the metabolic acidosis and to prevent further conversion of the remaining ethylene glycol to its toxic metabolites. The acidosis can be corrected with sodium bicarbonate therapy. Intravenous administration of ethanol as described on page 14 will inhibit further metabolism of ethylene glycol. At serum ethylene glycol levels of 50 mg/dL or greater, hemodialysis should be instituted to remove ethylene glycol and its metabolites from the blood. Pyroxidine and thiamine should also be administered.
-
It is possible that the child is intoxicated with only ethanol or with both ethanol and ethylene glycol. If intoxication is due to ethanol alone, careful monitoring of blood glucose and ethanol should be carried out until intoxication resolves. However, you must consider that ethylene glycol poisoning may be a complication. Because ethanol competitively inhibits ethylene glycol metabolism, you may choose to let the ethanol level decrease naturally to 70 mg/dL, then administer ethanol intravenously to maintain that level. The child should be transferred immediately to a pediatric unit where hemodialysis can be instituted if laboratory results indicate that ingestion of ethylene glycol occurred.
-
Information about health effects and standards and regulations can be obtained from the Technical Report for Ethylene/Propylene Glycol available from the Agency for Toxic Substances and Disease Registry (ATSDR). (For the address and telephone number of this agency, see Sources of Information, page 20.) The air and water standards vary with each state. A search of EPA’s Hazardous Substance Data Bank may provide information about the criteria for establishing these standards.























