

1 Lead Toxicity
|
Environmental ALERT…
|
This monograph is one in a series of self-instructional publications designed to increase the primary care provider’s knowledge of hazardous substances in the environment and to aid in the evaluation of potentially exposed patients. See page 27 for more information about continuing medical education credits and continuing education units.
|
Guest Contributor: |
Sarah E.Royce, MD, MPH |
|
Guest Editor: |
Herbert L.Needleman, MD |
|
Peer Reviewers: |
Charles Becker, MD; Jonathan Borak, MD; Joseph Cannella, MD; Robert Fried, MD; Bernard Goldstein, MD; Alan Hall, MD; Richard J.Jackson, MD, MPH; Jonathan Rodnick, MD; Linda Rosenstock, MD, MPH; Robert Wheater, MS; Brian Wummer, MD |

U.S. DEPARTMENT OF HEALTH & HUMAN SERVICES
Public Health Service
Agency for Toxic Substances and Disease Registry
Case Study
A hyperactive 5-year-old with disturbed hearing and hypochromic anemia
A 5-year-old boy is brought to your office by his mother, who is concerned that her child is hyperactive. At a parent-teacher conference last week, the kindergarten teacher said that the boy seems impulsive and has trouble concentrating, and recommended evaluation by a physician as well as by the school psychologist. The mother states that he has always seemed restless and easily distracted, but that these first 6 months in kindergarten have been especially trying.
Family history reveals that the boy lives with his sister, mother, and maternal grandparents in an older suburb of your community. The child’s monthly weekend visits to his father’s house are working out fine. However, he seems to be fighting more with his sister, who has an attention-deficit disorder and is repeating first grade. Since the mother moved in with her parents after her divorce 4 years ago, she has worked with the grandfather in an automobile radiator repair shop, where her children often come to play after school. She was just laid off, however, and expressed worry about increasing financial dependence on her parents. She also worries that the grandfather, who has gout and complains increasingly of abdominal pain, may become even more irritable when he learns that she is pregnant. Her third child is due in 4 months.
On chart review, you see that the boy was last seen in your clinic for his preschool physical 1 year ago, results of which were normal. A note describes a very active 4-year-old who could dress himself without help but could not correctly name the primary colors. His vision was normal, but hearing acuity was below normal, and speech and language were slightly delayed. Immunizations are up to date.
Further history on that visit indicated adequate diet, with no previous pica. Spun hematocrit was diminished at 30%. Peripheral blood smear showed hypochromia and microcytosis. There was no evidence of blood loss, and stool examination was negative for occult blood. The diagnosis was “mild iron deficiency anemia,” and iron therapy was prescribed. The family failed to keep several follow-up appointments, but the child did apparently complete the prescribed 3-month course of iron supplements. He receives no medications at this time and has no known allergies.
On physical examination today, you note that the boy is in the tenth percentile for height and weight. His attention span is very short, making him appear restless, and he has difficulty following simple instructions. Except for language and social skills, he has reached most important developmental milestones.
![]()
(a) What should be included in this boy’s problem list?
_________________________________________________________________
(b) List several possible causes for the anemia.
_________________________________________________________________
(c) What tests would you order to confirm or rule out your diagnosis?
_________________________________________________________________
Answers are incorporated in Challenge answers (11) through (14) on page 25.
Who’s at Risk
❑ Young children have a great potential for lead exposure and are especially susceptible to its toxic effects.
❑ Since blood lead readily crosses the placenta, lead poses a substantial threat to the developing fetus.
❑ Workers may bring lead dust home on skin and clothes and unknowingly expose family members.
By and large, children show a greater sensitivity to lead’s effects than adults do. The incomplete development of the blood-brain barrier in very young children (up to 36 months of age) increases the risk of lead’s entry into the developing nervous system, which can result in prolonged neurobehavioral disorders. Children absorb and retain more lead in proportion to their weight than do adults. Young children also show a greater prevalence of iron deficiency, a condition that can increase gastrointestinal absorption of lead.
No economic or racial subgroup of children is free from the risk of having blood lead levels high enough to cause adverse health effects. In 1984, approximately 17% of children in the United States were estimated to be at risk of lead poisoning. Sizable numbers of children from families with incomes well above the poverty line have been reported to have elevated blood lead levels. The prevalence of elevated levels, nevertheless, remains highest among inner-city, underprivileged children who live in deteriorating pre-1970s housing containing leaded-paint surfaces. Lead in paint and lead in soil and dust are the principal sources of exposure.
The percentage of African-American children affected by lead is disproportionate to their number in the U.S. population. In 1984 African-American children constituted 46% of the children at risk. The family income categories of these children show that the higher percentage is related to economic factors. African-American children are over represented in the poor and low-income groups as well as in inner-city areas. Other minorities are similarly affected; 15% of Mexican-Americans and 20% of Puerto Rican-Americans exceed a blood lead cutoff of 15 µg/dL As blood lead levels in the general population are declining because of restrictions on leaded gasoline use, race and income will become better indicators of the likelihood of exposure to leaded paint and, consequently, elevated blood lead levels.
Since lead readily crosses the placenta, the fetus is at risk. Fetal exposure can cause potentially adverse neurologic effects in utero and during postnatal development. According to the Public Health Service, in 1984, more than 400,000 fetuses were exposed to lead through maternal blood lead concentrations associated with early developmental effects.
More than 1 million workers in over 100 different occupations may be exposed to lead. In lead-related industries, workers not only may inhale lead dust and lead oxide fumes, but may eat, drink, and smoke in or near contaminated areas, increasing the probability of lead ingestion. If showers and changes of clothing are not provided, workers can bring lead dust home on their skin, shoes, and clothing, thus inadvertently exposing family members.
|
(1) Who else in the family or community discussed in the case study is at risk of lead poisoning? _________________________________________________________________ (2) Evaluate the exposure potential and risk to the fetus mentioned in the case study. _________________________________________________________________ |
Exposure Pathways
❑ The primary sources of environmental exposure to lead are leaded paint, auto emissions, and drinking water.
Lead is a naturally occurring element that has been used almost since the beginning of civilization. Because of the many industrial activities that have brought about its wide distribution, lead is ubiquitous in the environment today. All humans have lead in their bodies, primarily as a result of exposure to manmade sources.
Today, the major environmental sources of metallic lead and its salts are paint, auto exhaust, food, and water. For children, the most important pathways are ingestion of chips from lead-painted surfaces, inhalation of lead from automobile emissions, food from lead-soldered cans, drinking water from lead-soldered plumbing, and medications in the form of folk remedies.
❑ A wide variety of workers, hobbyists, and substance abusers may encounter potentially high levels of lead. Certain folk remedies may also cause lead poisoning.
Automobile emissions have been an important source of lead exposure for urban residents, particularly in areas with congested traffic. Although inhalation of lead from gasoline is no longer considered a public health problem, the lead from dust in automobile emissions has been deposited in the soil. Children playing near roads and freeways may come in contact with contaminated soil.
The lead content of paint was not regulated until 1977. Many older structures, residential and commercial, have leaded paint that is peeling, flaking, and chipping. Children can ingest loose paint as a result of pica (compulsive eating of nonfood items) and through mouthing of items contaminated with lead from paint, dust, and soil. High levels of lead in soil and house dust have been associated with increased blood lead levels in children.
❑ Lead enters the body primarily through ingestion and inhalation.
Food may contain lead from the environment or from containers. Agricultural vehicles are not required to use unleaded gasoline; consequently, lead can be deposited on and retained by crops, particularly leafy vegetables. Acidic foods have been found to leach lead from lead solder in cans and lead glazes used in making pottery and ceramicware. Water from leaded pipes, soldered plumbing, or water coolers is another potential source of lead exposure. Stationary or point sources of lead include mines and smelters.
Several folk remedies used in this country have been shown to contain large amounts of lead. Two Mexican folk remedies are azarcon and greta, which are used to treat “empacho,” a colic-like illness. Azarcon and greta are also known as liga, Maria Luisa, alarcon, coral, and rueda. Lead-containing remedies and cosmetics used by some Asian communities are chuifong tokuwan, pay-looah, ghasard, bali goli, and kandu. Middle Eastern remedies and cosmetics include alkohl, kohl, surma, saoott, and cebagin.
In addition to these environmental sources, many occupations, hobbies, and other activities result in potential exposures to high levels of lead and can put the entire family at risk of lead poisoning. Sources of lead exposure are listed below. Lead-glazed pottery, particularly if it is imported, is a potential source of exposure that is often overlooked. Even “safe” ceramicware can become harmful; dishwashing may chip or wear off the protective glaze and expose lead-containing pigments.
Inorganic lead enters the body primarily through inhalation and ingestion and does not undergo biologic transformation. In contrast, organic lead, found primarily in gasoline as tetraethyl lead, enters the body through inhalation and skin contact and is metabolized in the liver. In 1976 and in 1984, federal regulation drastically reduced the amount of lead in gasoline, and today organic lead in gasoline is not as great an environmental concern in the United States as it is in other countries, where it remains a serious hazard.
Sources of lead exposure
Occupational
Plumbers, pipe fitters
Lead miners
Auto repairers
Glass manufacturers
Shipbuilders
Printers
Plastic manufacturers
Lead smelters and refiners
Police officers
Steel welders or cutters
Construction workers
Rubber product manufacturers
Gas station attendants
Battery manufacturers
Bridge reconstruction workers
Firing range instructors
Environmental
Lead-containing paint
Soil/dust near lead industries, roadways, lead-painted homes
Plumbing leachate
Ceramicware
Leaded gasoline
Hobbies and Related Activities
Glazed pottery making
Target shooting at firing ranges
Lead soldering (e.g., electronics)
Painting
Preparing lead shot, fishing sinkers
Stained-glass making
Car or boat repair
Home remodeling
Substance Use
Folk remedies
“Health foods”
Cosmetics
Moonshine whiskey
Gasoline “huffing”
|
(3) The case study suggests several sources of lead in the boy’s life. What are these sources? What questions will you ask to gauge the extent of the boy’s exposure to each of these sources? _________________________________________________________________ _________________________________________________________________ (4) What questions will you ask the family to evaluate less obvious, but possible, sources of lead exposure? _________________________________________________________________ |
Biologic Fate
❑ Once in the bloodstream, lead is primarily distributed among three compartments—blood, soft tissue, and mineralizing tissue. The bones and teeth of adults contain more than 95% of total lead in the body.
❑ In times of stress, the body can mobilize lead stores, thereby increasing the level of lead in the blood.
❑ The body accumulates lead over a lifetime and normally releases it very slowly.
In the human body, inorganic lead is not metabolized but is directly absorbed, distributed, and excreted. The rate at which lead is absorbed depends on its chemical and physical form and on the physiologic characteristics of the exposed person (e.g., nutritional status and age). Inhaled lead deposited in the lower respiratory tract is completely absorbed. The amount of lead absorbed from the GI tract of adults is typically 10% to 15% of the ingested quantity; for pregnant women and children, the amount absorbed can increase to as much as 50%. The quantity absorbed increases significantly under fasting conditions and with iron or calcium deficiency.
Once in the blood, lead is distributed primarily among three compartments—blood, soft tissue (kidney, bone marrow, liver, and brain), and mineralizing tissue (bones and teeth). Mineralizing tissue contains about 95% of the total body burden of lead in adults.
The lead in mineralizing tissues accumulates in subcompartments that differ in the rate at which lead is resorbed. In bone, there is both a labile component, which readily exchanges lead with the blood, and an inert pool. The lead in the inert pool poses a special risk because it is a potential endogenous source of lead. When the body is under physiologic stress such as pregnancy, lactation, or chronic disease, this normally inert lead can be mobilized, increasing the lead level in blood. Because of these mobile lead stores, significant drops in a person’s blood lead level can take several months or sometimes years, even after complete removal from the source of lead exposure.
Of the lead in the blood, 99% is associated with erythrocytes; the remaining 1% is in the plasma, where it is available for transport to the tissues. The blood lead not retained is either excreted by the kidneys or through biliary clearance into the gastrointestinal tract. In single-exposure studies with adults, lead has a half-life, in blood, of approximately 25 days; in soft tissue, about 40 days; and in the non-labile portion of bone, more than 25 years. Consequently, after a single exposure a person’s blood lead level may begin to return to normal; the total body burden, however, may still be elevated.
For lead poisoning to develop, major acute exposures to lead need not occur. The body accumulates this metal over a lifetime and releases it slowly, so even small doses, over time, can cause lead poisoning. It is the total body burden of lead that is related to the risk of adverse effects.
|
(5) What would likely be revealed by an X ray of the abdomen or long bones of a lead-exposed child? _________________________________________________________________ (6) Why does the blood lead level fail to drop within a few days, even with complete removal from the source of exposure? _________________________________________________________________ _________________________________________________________________ (7) Several weeks after chelation therapy and removal from the source of exposure, in some cases the patient’s blood lead level is found to have increased again. What is the cause of this rebound phenomenon? _________________________________________________________________ _________________________________________________________________ _________________________________________________________________ |
Physiologic Effects
❑ Lead affects primarily the peripheral and central nervous systems, the blood cells, and metabolism of vitamin D and calcium. Lead also causes reproductive toxicity.
Whether lead enters the body through inhalation or ingestion, the biologic effects are the same; there is interference with normal cell function and with a number of physiologic processes. The lowest observable blood lead levels associated with specific health effects in chronically exposed children and adults are shown in Figure 1.
Neurologic Effects
❑ Neurologic deficits, as well as other effects caused by lead poisoning, may be irreversible.
The most sensitive target of lead poisoning is the nervous system. In children, neurologic deficits have been documented at exposure levels once thought to cause no harmful effects. In addition to the lack of a precise threshold, childhood lead toxicity may have permanent effects. One study showed that damage to the central nervous system (CNS) that occurred as a result of lead exposure at age 2 resulted in continued deficits in neurologic development, such as
❑ Effects in children generally occur at lower blood lead levels than in adults.
❑ The developing nervous system in children can be affected adversely at blood lead levels of less than 10 µg/dL.
Figure 1. Effects of inorganic lead on children and adults— lowest observable adverse effect levels
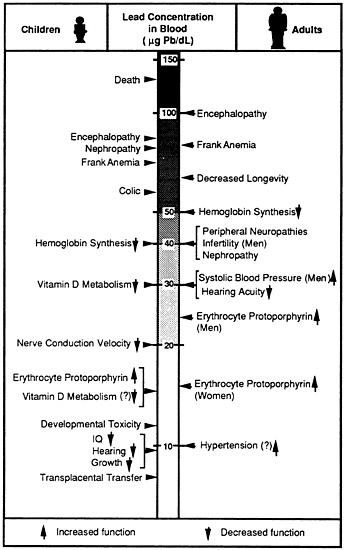
Adapted from ATSDR, Toxicological Profile for Lead (1989)
lower IQ scores and cognitive deficits, at age 5. In another study that measured total body burden, primary school children with high tooth lead levels but with no known history of lead poisoning had larger deficits in psychometric intelligence scores, speech and language processing, attention, and classroom performance than children
with lower levels of lead. A 1990 follow-up report of children with elevated lead levels in their teeth noted a sevenfold increase in the odds of failure to graduate from high school, lower class standing, greater absenteeism, more reading disabilities, and deficits in vocabulary, fine motor skills, reaction time, and hand-eye coordination 11 years later. The reported effects are more likely caused by the enduring toxicity of lead than by recent excessive exposures because the blood lead levels found in the young adults were low (less than 10 micrograms per deciliter [µg/dL]).
Hearing acuity, particularly at higher frequencies, has been found to decrease with increasing blood lead levels. Hearing loss may contribute to the apparent learning disabilities or poor classroom behavior exhibited by children with lead intoxication.
Adults also experience CNS effects at relatively low blood lead levels, manifested by subtle behavioral changes, fatigue, and impaired concentration. Peripheral nervous system damage, primarily motor, is seen mainly in adults. Peripheral neuropathy with mild slowing of nerve conduction velocity has been reported in asymptomatic lead workers. Lead neuropathy is believed to be a motor neuron, anterior horn cell disease with peripheral dying-back of the axons. Frank wrist drop occurs only as a late sign of lead intoxication.
Hematologic Effects
❑ Lead inhibits several enzymes that are critical to the synthesis of heme.
❑ Lead poisoning in children only rarely results in anemia.
Lead inhibits the body’s ability to make hemoglobin by interfering with several enzymatic steps in the heme pathway. Ferrochelatase, which catalyzes the insertion of iron into protoporphyrin IX, is quite sensitive to lead. A decrease in the activity of this enzyme results in an increase of the substrate, erythrocyte protoporphyrin (EP), in the red blood cells. Recent data indicate that the EP level, which has been used to screen for lead toxicity in the past, is not sufficiently sensitive at lower levels of blood lead and is therefore not as use ful a screening test for lead poisoning as previously thought. (See Laboratory Evaluation for further discussion of EP testing.)
Lead can induce two types of anemia. Acute high-level lead poisoning has been associated with hemolytic anemia. In chronic lead poisoning, lead induces anemia by both interfering with erythropoiesis and by diminishing red blood cell survival. It should be emphasized, however, that anemia is not an early manifestation of lead poisoning and is evident only when the blood lead level is significantly elevated for prolonged periods.
Endocrine Effects
❑ Lead interferes with a hormonal form of vitamin D, which affects multiple processes in the body, including cell maturation and skeletal growth.
A strong inverse correlation exists between blood lead levels and levels of vitamin D. Because the vitamin D-endocrine system is responsible in large part for the maintenance of extra- and intracellular calcium homeostasis, it is likely that lead impairs cell growth and maturation and tooth and bone development.
Renal Effects
❑ Lead-induced chronic renal insufficiency may result in gout.
A direct effect on the kidney of long-term lead exposure is nephropathy. Impairment of proximal tubular function manifests in aminoaciduria, glycosuria, and hyperphosphaturia (a Fanconi-like syndrome). There is also evidence of an association between lead exposure and hypertension, an effect that maybe mediated through renal mechanisms. Gout may develop as a result of lead-induced hyperuricemia, with selective decreases in the fractional excretion of uric acid before a decline in creatinine clearance. Renal failure accounts for 10% of deaths in patients with gout.
Reproductive and Developmental Effects
❑ Maternal lead stores readily cross the placenta, placing the fetus at risk.
An increased frequency of miscarriages and stillbirths among women working in the lead trades was reported as early as the turn of the century. Although the data concerning exposure levels are incomplete, these effects were probably a result of far greater exposures than are currently found in lead industries. Reliable dose-effect data for reproductive effects in women are still lacking today.
Increasing evidence indicates that lead not only affects the viability of the fetus, but development as well. Developmental consequences of prenatal exposure to low levels of lead include reduced birth weight and premature birth. Lead is an animal teratogen; however, most studies in humans have failed to show a relationship between lead levels and congenital malformations.
The effects of lead on the male reproductive system in humans have not been well characterized. The available data support a tentative conclusion that testicular effects, including reduced sperm counts and motility, may result from chronic exposure to lead.
Carcinogenic Effects
❑ EPA’s Science Advisory Board has recommended that lead be considered a probable human carcinogen.
Case reports have implicated lead as a potential renal carcinogen in humans, but the association remains uncertain. Soluble salts, such as lead acetate and lead phosphate, have been reported to cause kidney tumors in rats.
|
(8) What are the major effects of lead on the human body? _________________________________________________________________ _________________________________________________________________ (9) How do lead’s effects differ in children and adults? _________________________________________________________________ _________________________________________________________________ |
Clinical Evaluation
History and Physical Examination
❑ The first signs of lead poisoning in children are often subtle neurobehavioral problems that adversely affect classroom behavior and social interaction.
❑ Speech or hearing impairments, or both, are not uncommon in lead-exposed children.
Medical evaluation of a patient with suspected lead exposure includes a full workup and medical history. Clues to potential exposure are often obtained by discussing the following with the family:
occupational history of all home occupants
family history, including use of unusual medicines
location, age, and physical condition of residence, school, day-care center, etc.
home remodeling activities
condition of household pets
hobbies of all family members
use of imported or glazed ceramics
drinking water source and type of pipe
nutritional status
proximity to industrial facilities and hazardous waste sites
The physical examination should include special attention to the hematologic, cardiovascular, gastrointestinal, and renal systems. The nervous system, including behavioral changes, should be carefully evaluated. A purplish line on the gums (lead line) is rarely seen today, but if present, usually indicates severe and prolonged lead poisoning.
For children, hearing, speech, and other developmental milestones should be carefully evaluated and documented. In certain geographic areas, iron deficiency is common in children 9 to 24 months of age. Since iron and calcium deficiencies are known to enhance the absorption of lead and to aggravate pica, it is especially important to assess the nutritional status of young children.
Signs and Symptoms
❑ Most persons with lead toxicity are not overtly symptomatic.
Because of differences in individual susceptibility, symptoms of lead intoxication and their onset may vary. With increasing exposure, the severity of symptoms can be expected to increase. Those symptoms most often associated with varying degrees of lead toxicity are listed below. In symptomatic lead intoxication, blood lead levels generally range from 35 to 50 µg/dL in children and 40 to 60 µg/dL in adults. Severe toxicity is frequently found in association with blood lead levels of 70 µg/dL or more in children and 100 µg/dL or more in adults.
Continuum of signs and symptoms associated with lead toxicity
Mild Toxicity
Myalgia or paresthesia
Mild fatigue
Irritability
Lethargy
Occasional abdominal discomfort
Moderate Toxicity
Arthralgia
General fatigue
Difficulty concentrating
Muscular exhaustibility
Tremor
Headache
Diffuse abdominal pain
Vomiting
Weight loss
Constipation
Severe Toxicity
Paresis or paralysis
Encephalopathy-may abruptly lead to seizures, changes in consciousness, coma, and death
Lead line (blue-black) on gingival tissue
Colic (intermittent, severe abdominal cramps)
Some of the hematologic signs of lead poisoning mimic other diseases or conditions. In the differential diagnosis of microcytic anemia, lead poisoning can usually be ruled out by obtaining a venous blood lead concentration; if the blood lead level is less than 25 µg/dL, the anemia usually reflects iron deficiency or hemoglobinopathy. Two rare diseases, acute intermittent porphyria and coproporphyria, also result in heme abnormalities similar to those of lead poisoning.
Other effects of lead poisoning can be misleading. Patients exhibiting neurologic signs due to lead poisoning have been treated only for peripheral neuropathy or carpal tunnel syndrome, delaying treatment for lead intoxication. Failure to correctly diagnose lead-induced gastrointestinal distress has led to inappropriate abdominal surgery.
Laboratory Evaluation
If pica or accidental ingestion of lead-containing objects (such as curtain weights or fishing sinkers) is suspected, an abdominal radiograph should be taken. Hair analysis is not usually an appropriate assay for lead toxicity because no correlation has been found between the amount of lead in the hair and the exposure level. The probability of environmental lead contamination of a laboratory specimen and inconsistent sample preparation make the results of hair analysis difficult to interpret. Suggested laboratory tests to evaluate lead intoxication include the following:
CBC with peripheral smear
Blood lead level
Erythrocyte protoporphyrin level
BUN and creatinine level
Urinalysis
❑ Basophilic stippling is not always seen in lead-poisoned patients.
CBC with Peripheral Smear. In a lead-poisoned patient, the hematocrit and hemoglobin values may be slightly to moderately low. The differential and total white count may appear normal. The peripheral smear may be either normochromic and normocytic or hypochromic and microcytic. Basophilic stippling is usually seen only in patients who have been significantly poisoned for a prolonged period. Eosinophilia may appear in patients with lead toxicity but does not show a clear dose-response effect.
❑ The best screening and diagnostic test for lead poisoning is a blood lead level.
Blood Lead Level. A blood lead level is the most useful screening and diagnostic test for lead exposure. A blood lead level reflects lead’s dynamic equilibrium between absorption, excretion, and deposition in soft- and hard-tissue compartments. For chronic exposures, blood lead levels often underrepresent the total body burden; nevertheless, it is the most widely accepted and commonly used measure of lead exposure. Blood lead levels respond relatively rapidly to abrupt or intermittent changes in lead intake (for example, ingestion of lead paint chips by children) and, within a limited range, bear a linear relationship to those intake levels.
Lead is most harmful to children under 6 years of age. Every child who has a developmental delay, behavioral disorder, or speech impairment, or who may have been lead-exposed, should be considered for a blood lead test. Equally important, siblings, housemates, and playmates of children with suspected lead toxicity probably have similar exposures to lead and should be promptly screened. For occupationally exposed adults, consult the federal lead standard for the mandated type and frequency of lead screening (p. 20, Workplace, Air).
Today, the average blood lead level in the U.S. population is below 10 µg/dL, down from an average of 16 µg/dL (in the 1970s), the level before the legislated removal of lead from gasoline. A blood lead level of 10 µg/dL is about 3 times higher than the average level found in some remote populations.
The levels defining lead poisoning have been progressively declining. (See Biologic Guidelines in Standards and Regulations.) Currently, the consensus level of concern for children is 10 to 14 µg/dL (see Table 1). Effects on stature have been reported to begin at levels as low as 4 µg/dL, the present limit for accurate blood lead measurement. Taken together, effects occur over a wide range of blood lead concentrations, with no indication of a threshold. No safe level has yet been found for children. Even in adults, effects are being discovered at lower and lower levels as more sensitive analyses and measures are developed.
❑ Using an EP or ZPP assay to screen children for lead poisoning is not as useful as once thought.
EP and ZPP Levels. Until recently, the test of choice for screening asymptomatic children and other populations at risk was erythrocyte protoporphyrin (EP), commonly assayed as zinc protoporphyrin (ZPP). An elevated level of protoporphyrin in the blood is a result of accumulation secondary to enzyme dysfunction in the erythrocytes. It reaches a steady state in the blood only after the entire population of circulating erythrocytes has turned over, about 120 days. Consequently, it lags behind blood lead levels and is an indirect measure of long-term lead exposure.
Table 1. Interpretation of blood lead test results and follow-up activities: class of child based on blood lead concentration
|
Class |
Blood lead concentration (µg/dL) |
Comment |
|
I |
≤9 |
A child in Class I is not considered to be lead-poisoned. |
|
IIA |
10–14 |
The presence of many children (or a large proportion of children) with blood lead levels in this range should trigger communitywide childhood lead poisoning prevention activities. Children in this range may need to be rescreened frequently. |
|
IIB |
15–19 |
A child in Class IIB should receive nutritional and educational interventions and more frequent screening. If the blood lead level persists in this range, environmental investigation and intervention should be done. |
|
III |
20–44 |
A child in Class III should receive environmental evaluation and remediation and a medical evaluation. Such a child may need pharmacologic treatment of lead poisoning. |
|
IV |
45–69 |
A child in Class IV will need both medical and environmental interventions, including chelation therapy. |
|
V |
≥70 |
A child with Class V lead poisoning is a medical emergency. Medical and environmental management must begin immediately. |
The major disadvantage of using EP (ZPP) testing as a method for lead screening is that it is not sensitive at the lower levels of lead poisoning. Data from the second National Health and Nutrition Examination Survey (NHANES II) indicate that 58% of 118 children with blood lead levels above 30 µg/dL had EP levels within normal limits. This finding shows that a significant number of children with lead toxicity would be missed by reliance on EP (ZPP) testing alone as the screening tool. An EP (ZPP) level is still useful in screening patients for iron deficiency anemia.
Normal values of ZPP are usually below 35 µg/dL. Hyperbilirubinernia (jaundice) will cause falsely elevated readings when the hematofluorometer is used. EP is elevated in iron deficiency anemia and in sickle cell and other hemolytic anemias. In erythropoietic protoporphyria, an extremely rare disease, EP is markedly elevated (usually above 300 µg/dL).
❑ Renal function may be impaired in lead-exposed persons.
BUN, Creatinine, and Urinalysis. These parameters may reveal only late, significant effects of lead on renal function. Renal function in adults can also be assessed by measuring the fractional excretion of uric acid (normal range 5% to 10%; less than 5% in saturnine gout; greater than 10% in Fanconi syndrome).
|
(10) What should be included in the problem list for the patient described in the case study? _________________________________________________________________ (11) List several possible causes of the boy’s anemia. _________________________________________________________________ (12) You have just learned from the laboratory that the boy has a ZPP level of 350 µg/dL. What are the possible causes of this elevated value? _________________________________________________________________ (13) What other laboratory tests will you now order to confirm or rule out your diagnosis? _________________________________________________________________ |
Treatment and Management
❑ All therapeutic chelating agents have potentially adverse side effects and should be used cautiously.
❑ The type of therapy required will normally depend on the patient’s blood lead level. Asymptomatic patients with blood lead levels below 25 µg/dL usually require only separation from the source of exposure.
It is not sufficient to provide treatment only; the patient and lead source must be permanently separated. After diagnosing lead poisoning, the physician should call upon the resources of the local health authority to determine the lead source (e.g., home, workplace). If the lead poisoning is caused by leaded paint in the home, the patient and all other family members should be rehoused until the home has undergone safe and satisfactory lead abatement. Family members and other persons likely to have been exposed should be tested for lead poisoning. Steps should be taken to identify and correct dietary deficiencies, particularly of calcium and iron, and to educate family members on the preventable hazards of lead.
The most reliable index of exposure is a measurement of blood lead concentration. In those asymptomatic children having blood lead levels below 25 µg/dL, treatment is probably not indicated, and removal from the source is the most important action. Patient followup to confirm a decreasing blood lead level is needed, however.
❑ Children with blood lead levels of 45 µg/dL or greater should be referred for appropriate chelation therapy immediately.
The Centers for Disease Control (CDC) recommends that children with blood lead levels of 45 µg/dL or greater should be referred for appropriate chelation therapy immediately. Some practitioners routinely treat children with blood lead levels between 25 and 44 µg/dL with chelation therapy and some do not use chelating agents for children with blood lead levels in this range. Other practitioners base this decision on the results of a provocative EDTA test. Only very minimal data exist about chelation therapy for children with blood lead levels below 25 µg/dL, and such children should not be chelated except in the context of approved clinical trials.
❑ The EDTA challenge test will indicate the extent of lead stores in the body. Some practitioners use this test when deciding whether to institute chelation therapy for a patient with a blood lead level between 25 and 44 µg/dL.
Several drugs (see Table 2) are used in the treatment of lead poisoning. These drugs, capable of binding or chelating lead, deplete the soft and hard (skeletal) tissues of lead and thus reduce its acute toxicity. All drugs have potential side effects and must be used with caution. In rare cases, the chelating agent, calcium disodium ethylenediaminetetraaceate acid (CaNa2EDTA) has caused proteinuria, microscopic hematuria, proximal tubule damage, hypercalcemia, and fever. Before instituting this therapy or using the chelation challenge test, the patient should be hospitalized and a physician experienced in chelation should be consulted. Such physicians can be identified by contacting an accredited regional poison control center, university medical center, or state or local health department.
Table 2. Chelating agents used in treating children who have lead poisoning
|
Product Name |
Generic Name |
Chemical Name |
Abbreviation |
|
Calcium Disodium Versenate |
Edetate disodium calcium |
Calcium disodium ethylenediaminetetraacetate |
CaNa2EDTA |
|
BAL* in Oil |
Dimercaprol |
2,3-dimercapto-1-propanol |
BAL* |
|
Cuprimine |
D-penicillamine |
3-mercapto-D-valine |
D-penicillamine |
|
Chemet |
Succimer |
Meso-2,3-dimercaptosuccinic acid |
DMSA |
|
*British anti-Lewisite |
|||
|
(14) The laboratory results indicate that the blood lead level of the child in the case study is 50 µg/dL. What treatment and follow-up activities will you recommend? _________________________________________________________________ (15) Who could you contact for medical consultation regarding this boy’s case? _________________________________________________________________ (16) What can you as a physician do to prevent exposure to lead? _________________________________________________________________ |
Standards and Regulations
The number of federal standards and regulations reflect the extent to which lead is considered a public health problem. In some cases, the lead levels are mandated; in others, they are only recommended standards (Table 3).
Table 3. Summary of standards and regulations for lead
|
Agency* |
Focus |
Level |
Comments |
|
CDC |
Blood |
10 µg/dL |
Advisory; level of concern for children† |
|
OSHA |
Blood |
50 µg/dL |
Regulation; medical removal from exposure (See p. 20, Workplace, Air) |
|
OSHA |
Air |
50 µg/m3 30 µg/m3 |
Regulation; PEL§ (General industry) Action level |
|
ACGIH |
Air |
150 µg/m3 |
Advisory; TLV/TWA¶ (Under revision) |
|
EPA |
Air |
1.5 µg/m3 |
Regulation; 3-month average |
|
CDC (NIOSH) |
Air |
100 µg/m3 |
REL** |
|
EPA |
Water |
15 µg/L |
Action level; (See p. 20, Environment, Water) |
|
FDA |
Food |
100 µg/day |
Advisory |
|
CPSC |
Paint |
600 ppm (0.06%) |
Regulation; by dry weight |
|
*ACGIH=American Conference of Governmental Industrial Hygienists; CDC=Centers for Disease Control; CPSC=Consumer Product Safety Commission; EPA=Environmental Protection Agency; FDA=Food and Drug Administration; NIOSH=National Institute for Occupational Safety and Health; OSHA=Occupational Safety and Health Administration †If many children in the community have blood lead levels ≥10 µg/dL, communitywide interventions (primary prevention activities) should be considered by appropriate agencies. §PEL(Permissible Exposure Limit): The employer shall assure that no employee is exposed to lead at concentrations >50 µg/m3 of air averaged over an 8-hour period. ¶TLV/TWA (Threshold Limit Value/Time Weighted Average): The time-weighted average concentration for a normal 8-hour workday and a 40-hour workweek, to which nearly all workers may be repeatedly exposed, day after day, without adverse effect. **REL (Recommended Exposure Limit): Air concentration to be maintained so that worker blood lead remains <0.060 mg/100g of whole blood. |
|||
Biologic Guidelines
❑ CDC lowered the recommended action level for lead poisoning in children in 1991.
Lead levels that in the past were considered safe are now considered hazardous. As new information has emerged about the neurologic, reproductive, and possible hypertensive toxicity of lead, and as more sensitive parameters are developed, the levels defining lead poisoning have been progressively lowered. Between 1986 and 1988, several studies demonstrated neurobehavioral impairment in lead-exposed children with blood lead levels as low as 10 to 14 µg/dL. As more data become available, the definition of lead toxicity level will likely continue to be lowered (Figure 2).
Figure 2. CDC’s action level for blood lead in children has steadily declined.
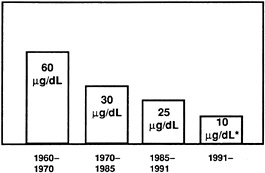
*Emphasis is on primary prevention efforts (i.e., elimination of lead hazards before children are poisoned).
❑ Several states require primary care physicians to report cases of lead poisoning.
Physician Reporting Requirements. Several states require primary care physicians and persons in charge of screening programs to report both presumptive and confirmed cases of lead toxicity to the appropriate health agency so that abatement of the lead source, education of the patient, and remediation steps can be undertaken. In many states, laboratories performing blood lead or EP (ZPP) tests are also required to report abnormal results to the appropriate health agency.
Workplace
Air
❑ OSHA has set required standards for the amount of lead allowed in workroom air at 50 µg/m3averaged over an 8-hour workday.
The federal lead standard specifies the permissible exposure limit (PEL) of lead in the workplace, the frequency and extent of medical monitoring, and other responsibilities of the employer. The Occupational Safety and Health Administration (OSHA) has set a PEL of lead in workroom air at 50 µg/m3 averaged over an 8-hour workday for workers in general industry. For those exposed to air concentrations at or above the action level of 30 µg/m3 for more than 30 days per year, OSHA mandates periodic determination of blood lead levels. If a blood lead level is found to be greater than 40 µg/dL, the worker must be notified in writing and provided with medical examination. If a worker’s blood lead level reaches 60 µg/dL (or averages 50 µg/dL or more), the employer is obligated to remove the employee from excessive exposure, with maintenance of seniority and pay, until the employee’s blood lead level falls below 40 µg/dL (29 CFR §1910.1025). A copy of the lead standard can be obtained by calling your regional office of OSHA.
Environment
Air
❑ EPA will probably lower its present ambient air standard for lead.
Occupational exposure limits are generally set to accommodate 8-hour workdays and healthy persons; they bear little relation to environmental limits, which are set to protect the most susceptible persons in the general population. EPA requires that the concentration of lead in air the general public may breathe shall not exceed 1.5 µg/m3 averaged over a calendar quarter. This standard will probably be lowered. To reduce the amount of lead released into the environment, EPA regulations now limit the level of lead in unleaded gasoline to 0.05 grams per gallon.
Drinking Water
❑ EPA’s proposed goal for lead in drinking water after treatment is zero.
EPA estimates that about 20% of the U.S. population (including 3.8 million children) consumes drinking water with lead levels above 20 µg/dL. EPA is required to set drinking water standards with two levels of protection. The primary standards define contaminant levels in drinking water as levels above which the water source requires treatment. These maximum contaminant levels (MCLs) are limits enforceable by law and are set as close as possible to the maximum contaminant level goals (MCLGs), the levels determined to be safe by toxicologic and biomedical considerations, independent of feasibility. EPA has promulgated a final rule for lead in drinking water: this rule does not establish an MCL; the MCLG is zero and the action level is set at 15 µg/L. If more than 10% of targeted tap water samples exceed the action level, certain actions are required of water system administrators. For further information, call the U.S. EPA Safe Drinking Water Hotline toll-free at 1–800–426–4791.
The use of lead solder and other lead-containing materials in connecting household plumbing to public water supplies was banned by EPA as of June 1988. Many older structures, however, still have lead pipe or lead-soldered plumbing internally, which may substantially increase the lead content of water at the tap. Regulations controlling the lead content of drinking-water coolers in schools went into effect in 1989.
Food
❑ Most lead in food comes from solder in cans or glazes on ceramicware.
Regulating lead contamination in foods is the responsibility of the Food and Drug Administration (FDA). FDA has set a goal of less than 100 µg/day as the total lead intake by children 1 to 5 years of age. Lead in food and beverages is encountered by virtually this entire age group in the United States.
According to a 1988 ATSDR report, FDA has estimated that about 20% of all dietary lead comes from canned food; about two-thirds of that amount results from lead solder in cans. The number of food cans that are lead-soldered continues to decline. In 1979, over 90% of all food cans were lead soldered; in 1986, this figure was 20%, or less than about 2 million cans. It is important to note that imported canned foods are not included in these figures and may still contain lead. Imported glazed ceramics and lead-containing pottery are also potential sources of dangerously high levels of lead.
Paint
❑ Today, paint intended for residential use is limited to 0.06% lead content.
Since 1977, the Consumer Product Safety Commission has limited the lead in most paints to 0.06% (600 ppm by dry weight). Paint for bridges and marine use may contain greater amounts of lead.
|
(17) Regarding the facts reported in the case study, should public health authorities or regulatory agencies be notified? Why? _________________________________________________________________ (18) You learn from the boy’s mother that her place of employment had poor ventilation and no provision for respiratory protection, shower facilities, or work clothes. She ate lunch and smoked in the repair shop. “In fact,” she says, “I wonder if my layoff has anything to do with the blood test the company had me get.” The company’s test indicated that her blood lead level was 62 µg/dL. What advice could you give the boy’s mother regarding her former employment? _________________________________________________________________ |
Suggested Reading List
General
Cullen MR, Robins JM, Eskenazi B. Adult inorganic lead intoxication: presentation of 31 new cases and a review of recent advances in the literature. Medicine (Baltimore) 1983;62:221–47.
Gerber GB, Leonard IA, Jacquet P. Toxicity, mutagenicity and teratogenicity of lead. Mutat Res 1980;76:115–41.
Kehoe RA. Occupational lead poisoning: clinical types. J Occup Med 1972;14:298–300.
Piomelli S, Needleman HL, Rosen JF. Lead poisoning. American Academy of Pediatrics Update (audiotape available) 1988;9(4):1–9.
Putnam RD. Review of toxicology of inorganic lead. Am Ind Hyg Assoc J 1986;47:700–3.
Chelation Therapy
Chisolm JJ Jr, Kaplan E. Lead poisoning in childhood—comprehensive management and prevention. J Pediatr 1968;73(6):942–50.
Chisolm JJ Jr. The use of chelating agents in the treatment of acute and chronic lead intoxication in childhood. J Pediatr 1968;73(1):1–38.
Markowitz ME, Rosen JF. Assessment of lead stores in children: validation of an 8-hour CaNa2EDTA provocative test. J Pediatr 1984;104(3):337–41.
Markowitz ME, Rosen JF. Need for the lead mobilization test in children with lead poisoning. J Pediatr 1991;119(2):305–10.
Piomelli S, Rosen JF, Chisolm JJ Jr, Graef JW. Management of childhood lead poisoning. J Pediatr 1984;105(4):523– 32.
Rosen JF, Markowitz ME, Bijur PE, et al. Sequential measurements of bone lead content by L X-ray fluorescence in CaNa2EDTA-treated lead-toxic children. Environ Health Perspect 1991;93:271–7.
Rosen JF, Markowitz ME, Bijur PE, et al. Sequential measurements of bone lead content by L X-ray fluorescence in CaNa2EDTA-treated lead-toxic children [published erratum appears in Environ Health Perspect 1991;92:181]. Environ Health Perspect 1991;91:57–62.
Neurobehavioral Development
Bellinger D, Leviton A, Waternaux C, Needleman H, Rabinowitz M. Longitudinal analyses of prenatal and postnatal lead exposure and early cognitive development. N Eng J Med 1987;316:1037–43.
Needleman HL, Gunnor C, Leviton A, et al. Deficits in psychologic and classroom performance of children with elevated dentine lead levels. N Engl J Med 1979;300:689–95.
Needleman HL, Schell A, Bellinger D, Leviton A, Allred EN. The long-term effects of exposure to lead in childhood. An 11-year follow-up report. N Engl J Med 1990;322:83–8.
Schwartz J, Otto D. Blood lead, hearing thresholds, and neurobehavioral development in children and youth. Arch Environ Health 1987;42:153–9.
Hematologic Effects
Moore MR, Goldberg A, Yeung-Laiwah AC. Lead effects on the heme biosynthetic pathway. Ann NY Acad Sci 1985;191–202.
Nephropathy
Lurakis MF, Pitone JM. Occupational lead exposure, acute intoxication, and chronic nephropathy: report of a case and review of the literature. J Am Osteopath Assoc 1984;83:361–6.
Reproductive Effects
Mitchell JW, ed. Occupational medicine forum: lead toxicity and reproduction. J Occup Med 1987;29:397–9.
Uzych L. Teratogenesis and mutagenesis associated with the exposure of human males to lead: a review. Yale J Biol Med 1985;58:9–17.
Sources of lead exposure
Kunkel DB. The toxic emergency. Emergency Medicine 1986;18(Mar):207–17.
Drinking Water
Marcus WL. Lead health effects in drinking water. Toxicol Ind Health 1986;2:363–400.
Related Government Documents
Agency for Toxic Substances and Disease Registry. The nature and extent of lead poisoning in children in the United States: A report to Congress. Atlanta: US Department of Health and Human Services, Public Health Service, 1988. DHHS report no. 99–2966.
Agency for Toxic Substances and Disease Registry. Toxicological profile for lead—draft. Atlanta: US Department of Health and Human Services, Public Health Service, 1992.
Centers for Disease Control. Preventing lead poisoning in young children: a statement by the Centers for Disease Control, January 1985. Atlanta: US Department of Health and Human Services, Public Health Service, 1985. DHHS report no. 99–2230. Revised October 1991.
Centers for Disease Control. Criteria for a recommended standard: occupational exposure to inorganic lead revised criteria. Atlanta: US Department of Health, Education, and Welfare, Public Health Service, 1978. Report no. (NIOSH) 78–158.
Centers for Disease Control. Lead poisoning following ingestion of homemade beverage stored in a ceramic jug-New York. Atlanta: US Department of Health and Human Services. MMWR 1989;38(21):379–80.
Centers for Disease Control. Occupational and environmental lead poisoning associated with battery repair shops-Jamaica. Atlanta: US Department of Health and Human Services. MMWR 1989;38(27):474–81.
Centers for Disease Control. Cadmium and lead exposure associated with pharmaceuticals imported from Asia-Texas. Atlanta: US Department of Health and Human Services. MMWR 1989;38(35):612–4.
Centers for Disease Control. Surveillance for occupational lead exposure-United States, 1987. Atlanta: US Department of Health and Human Services. MMWR 1989;38(37):642–6.
Centers for Disease Control. Lead poisoning in bridge demolition workers-Massachusetts. Atlanta: US Department of Health and Human Services. MMWR 1989;38(40):687–94.
Environmental Protection Agency. Air quality criteria for lead, Vol 2. Research Triangle Park, North Carolina: US Environmental Protection Agency, Office of Health and Environmental Assessment. Report no. EPA-600/ 8–83/028bF.
Environmental Protection Agency. Maximum Contaminant Level Goals and National Primary Drinking Water Regulations for Lead and Copper. Federal Register 1991;56:26460, 26477.
Office of the Federal Register. Code of federal regulations; occupational safety and health standards. Appendix C-Medical surveillance guidelines. Washington, DC: Office of the Federal Register, National Archives and Records Administration, 1988. (29 CFR §1910.1025).
Answers to Pretest and Challenge Questions
Pretest questions are found on page 1. Challenge questions begin on page 3.
-
All members of the family are at risk; they should be promptly evaluated and, if necessary, treated. The mother’s unborn child is also at risk. Workers in the radiator repair shop and their families, and any of the children’s playmates who have accompanied them to the repair shop after school, should also be screened.
-
The boy’s mother is 5 months pregnant. Since the placenta presents no barrier to lead, the fetus’ blood lead level is likely to be similar to that of the mother. It is during the initial weeks of pregnancy that the neurologic system of the conceptus is formed; therefore, damage to the fetus may have already occurred. The mother is no longer working at the repair shop, but you should alert her and the family to the possibility of continued lead exposure via the grandfather, who may be bringing lead dust home on his skin, shoes, or clothes.
-
Two of the obvious sources of lead suggested in the case study are leaded paint at home (paint flakes, household dust, and soil) and fumes and dust from solder at the radiator repair shop. You should determine if the boy ever had pica (a compulsive eating of nonfood items, to be distinguished from normal hand-to-mouth behavior of children). Pica is more common in children aged 2 to 5, so it is unlikely that this is a present behavior. Exposure to high levels of lead at the radiator repair shop is very possible, and you need to ascertain the type and length of the boy’s play at the shop.
-
To evaluate less obvious, but possible, sources of lead exposure, you might inquire about the proximity of the child’s home and play areas to freeways, hazardous waste sites, and industry. The occupations of all adults in the household are important; children of lead-exposed workers have been shown to have higher lead levels than control groups. Do any of the boy’s associates or does the father have hobbies involving lead, such as those mentioned on page 4? You might also inquire whether the home is undergoing remodeling, whether any home or folk remedies are used, if glazed ceramicware is used for food, or if there are lead or lead-soldered pipes in the house that could contaminate the drinking water.
-
If a child does not have pica and there is nothing to suggest that a lead-containing object has recently been ingested, an abdominal X ray will likely be negative. On long-bone radiograms, opacities in the metaphysial plates may be seen after 4–8 weeks or more of lead exposure. These “lead lines” (which are due to dense zones of calcium and not deposited lead) are more likely to be found in larger bones (e.g., radius and tibia) than in smaller bones (e.g., ulna and fibula). Lead lines seen in the smaller bones may be indicative of a longer exposure, usually several months. Radiographs are helpful only in the rare circumstances that they are positive. Negative X rays do not rule out lead poisoning.
-
Even with complete removal from the source of exposure, the blood lead level will drop only gradually because, without chelation, lead is only slowly excreted. In addition, even as it is excreted, it may be replaced by lead currently stored in bones and teeth.
-
This rebound phenomenon is due to the mobilization of lead from the body’s stores in bones and teeth.
-
The major effects of lead on the human body are damage to the neurologic, hematologic, renal, and reproductive systems.
-
Because of an incompletely developed blood-brain barrier, children under 36 months of age are particularly susceptible to neurologic damage at very low blood lead levels. Since children (to age 7) are more sensitive to lead’s effects, most adverse effects of lead are often manifested at lower blood lead levels in children than in adults.
-
History suggests delayed language ability, slightly impaired hearing, short stature, possible attention deficit disorder, and anemia. The child is also experiencing passive exposure to his mother’s cigarette smoke and family disruption related to his parents’ divorce.
-
Three of the most common causes of microcytic anemia are iron deficiency, hemoglobinopathy, and lead poisoning. In lead-poisoned patients, anemia is usually evident only when the blood lead level is significantly elevated for prolonged periods. It manifests in only a relatively small number of children with chronic lead poisoning. It is possible for a patient to be both lead-poisoned and to have anemia due to some other cause. The relative rarity of nutritional iron deficiency in this boy’s age group and the absence of evidence for blood loss suggest consideration of other etiologies to explain the anemia.
-
An elevated ZPP level is most often due to iron deficiency anemia, hemolytic anemias, or lead poisoning. A rare disease that may cause the ZPP level to be markedly elevated is erythropoietic protoporphyria.
-
To confirm lead poisoning, the best test is a venous blood lead level. If the blood lead level is below 25 µg/dl, then a serum ferritin level and other iron studies can be used to determine if iron deficiency anemia exists.
-
With an elevated blood lead level of 50 µg/dL, the conclusion is that the boy is lead-poisoned. In this case, the child should be referred for appropriate chelation therapy immediately. It is important to immediately identify and eliminate all sources of lead exposure for both the boy and his family. Environmental evaluation, intervention, and remediation should begin immediately. All household members should be screened for lead exposure (See Table 1, page 15). Adequate diet for the family should be stressed.
-
You should consult with a physician experienced in treating lead-poisoned patients. To identify such physicians, contact your state or local health department, a university medical center, or a certified regional poison control center.
-
Knowing the subgroups at greatest risk of lead exposure, you should take every opportunity to educate these subpopulations, your colleagues, and the community about the hazards of lead poisoning and the steps to prevent its occurrence. Those children and members of the community whom you suspect may be in danger of lead poisoning should be promptly screened.
-
In certain states, public health authorities must be notified if a patient’s blood lead level and ZPP level exceed certain limits. In any case, you should contact your state or local health department so all sources of lead in the home can be identified and abated. You should also notify OSHA so the radiator repair shop can be brought, if required, into compliance with the federal lead standard. A NIOSH health hazard evaluation could also be requested. The reason for notifying these agencies is to prevent lead exposure in others.
-
The federal lead standard mandates that a worker with a blood lead level of 60 µg/dl or higher (or an average of 50 µg/dL)undergo medical removal from the lead hazard and be reassigned with retention of job seniority and pay. In addition to referring her for obstetrical evaluation, you should recommend that the mother talk to her employer, employee representative, and OSHA to clarify her work status under the lead standard and possible reinstatement procedures.
Sources of Information
More information on the adverse effects of lead and the treatment and management of lead-exposed persons can be obtained from ATSDR, your state and local health departments, and university medical centers. Case Studies in Environmental Medicine: Lead Toxicity is one of a series. For other publications in this series, please use the order form on the back cover. For clinical inquiries, contact ATSDR, Division of Health Education, Office of the Director, at (404) 639–6204.


























