
Behavioral and Audiological Manifestations of Noise-Induced Hearing Loss
Sufficiently intense sounds have the potential of disrupting all parts of the peripheral and central auditory system. Noise can have direct mechanical effects on the middle ear, such as ossicular and discontinuity, tympanic membrane perforation, or fistula of the oval window, and on cochlear structures. The outer hair cells are particularly vulnerable to the effects of excessive noise exposure, followed in vulnerability by the inner hair cells. The cochlea, once damaged, cannot be repaired; the subsequent loss of sensory cells and neural changes produces an auditory pathology that represents the morphologic substrate for the loss of hearing threshold, referred to as a noise-induced sensorineural hearing loss, or simply a noise-induced hearing loss (NIHL). A similar set of cochlear changes can be induced by lower levels of noise that continuously stress the metabolic processes of the cochlea. While these changes may initially produce a temporary loss of threshold, with repeated exposures they may lead to permanent changes.
Hearing loss resulting from noise exposure can be separated into three distinct categories: acoustic trauma, temporary threshold shift (TTS), and permanent threshold shift (PTS). A single, relatively intense noise exposure is referred to as an acoustic trauma and is usually followed by tinnitus and a change in hearing threshold. While hearing may improve slightly over time, if the exposure is sufficiently intense a PTS will result. One or both ears may be involved. Those who experience an acoustic trauma may also suffer from tympanic membrane perforation(s) and disarticulated or fractured ossicles. Such middle-ear disorders are more likely to appear, if at all, once the peak noise exposure level exceeds approximately 160 dB SPL. In general, however, any acute sound exposure that causes any of the following symptoms represents a hazard to the auditory system and could result in an acute acoustic trauma: immediate pain, a tickling sensation in the ears often occurring if the SPL exceeds approximately 120 dB, vertigo, tinnitus, hearing loss, or reduced communication skills.
Lower levels of noise (<85 dB[A]) are potentially hazardous and may result in an NIHL if, following exposure, there is a transient shift in the threshold of hearing that recovers gradually (a TTS). While the onset of hearing loss in acute acoustic trauma is instantaneous, the onset and progression of NIHL is far more insidious since it accumulates, usually unnoticed, over a period of many years of exposure to noise on a daily basis. During the initial stages of NIHL, the temporary hearing loss recovers within a few hours or days following removal from the noise. However, if the exposure to this noise is repeated often enough, the hearing loss may not recover completely (that is, permanent sensorineural hearing impairment will begin).
Reprinted with permission from Occupational Health: Recognizing and Preventing Work-Related Disease, Levy and Wegman (eds.), 328–31, Copyright 1995, Little, Brown and Company.
The following is a typical case history of an history individual with permanent NIHL:
A 48-year-old man had chief complaints of constant, high-pitched tinnitus and progressive hearing loss in both ears over the previous 2 years. He reported some difficulty hearing in quiet surroundings but noticed marked difficulty understanding speech in noisy environments. He did not report any previous serious illnesses, accidents, atypical drug use, or problems with his ears. For the past 8 years, he had worked in a noisy textile mill, where he said that he “occasionally” wore hearing protective devices. The patient had not been exposed to other hazardous noises off the job, such as gunfire or motorbikes.
The diagnosis of NIHL comes under the domain of the audiologist, whose primary responsibility is the identification and measurement of hearing loss and the rehabilitation of those with hearing impairment. By measuring auditory thresholds in decibels (relative to a normal hearing level or 0 dB HL) for pure tones as a function of frequency, an audiogram (a frequency-intensity graph) is generated. Hearing level (HL) is a term used to designate an individual’s hearing threshold at a given test frequency, referenced to an audiometric zero level. The audiogram will help answer the following questions: (1) Is there evidence of hearing loss? (2) If so, what is the severity of the loss? (3) What is the nature of the loss (conductive, sensorineural, or mixed)? and (4) Can the use of a hearing aid(s) benefit the hearing-impaired individual? A typical normal audiogram and an audiogram from an individual with an NIHL are shown in Fig. 16–5.
Hearing loss induced by most industrial noise characteristically produces a bilateral symmetrical loss that is progressive in nature so long as the individual is continuously exposed to hazardous noise levels (Fig. 16–5). In the initial stages of development, the loss usually occurs at frequencies lying between 3,000 and 6,000 Hz. The maximum loss is usually centered at 4,000 Hz. The audiometric configuration, therefore, is characterized by a downward slope with greater loss in the high-frequency region (3,000–6,000 Hz) than in the low- and mid-frequency regions (250–2,000 Hz). As the NIHL accumulates following further exposure, the 4,000-Hz loss increases in magnitude and the adjacent (higher and lower) frequencies also become increasingly affected. The progressive nature of NIHL may eventually result in a moderate to severe impairment across most of the usable hearing frequency range (250–8000 Hz) unless preventive measures are taken to reduce the degree of hazard imposed by the noise.
Although the diagnosis of a permanent NIHL may be indicated by the audiometric configuration of the hearing loss (the 4,000-Hz notch), it would be premature to make a definitive diagnosis unless additional factors are considered, such as: (1) What is the duration, type, and time-weighted average of the individual’s noise exposure? (2) What is the individual’s hearing both before and after exposure? (3) What is the age and general health of the individual? (4) Are there any other disorders that may result in
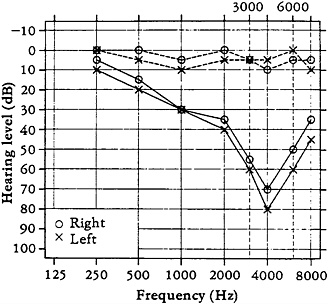
Fig. 16–5. An example of a typical audiogram from a normal individual (dashed lines) and an individual with a bilateral sensorineural hearing loss resulting from excessive noise exposure. Note the maximum loss at 4,000 Hz and the spread of loss to the lower frequencies.
hearing impairment (such as middle-ear disorders, congenital factors, Meniere’s disease, an eighth cranial nerve lesion, ototoxicity, and presbycusis)? Consideration of these questions provides important information as to whether the cause and degree of impairment can be solely attributable to noise exposure. Two major diagnostic problems are distinguishing NIHL from hearing loss associated with presbycusis or ototoxic agents and determining the degree of impairment attributed to the aging process. A reported history of tinnitus or “muffled” hearing occurring immediately after any noise exposure or after leaving the work environment and a characteristic 4,000-Hz notch on the audiogram strongly suggest an occupational NIHL hearing loss. Complaints of vertigo are also common.
People usually do not report any difficulty in hearing until a hearing loss of more than 25 dB HL occurs at a frequency at or below 4,000 Hz. Difficulty in hearing the high-frequency sounds of speech (such as s, f, k, t, and sh) may provide the only clue to the individual of an NIHL. Performance on speech intelligibility tasks varies considerably depending on the magnitude of the loss and the affected frequencies. If the hearing loss is confined to frequencies above 3,000 Hz, speech intelligibility measured in quiet surroundings is usually within normal limits. As the frequencies below 3,000 Hz become involved, intelligibility decreases in relation to the degree of impairment. Given that approximately 95 percent of the frequency components in speech lie between 300 and 3,000 Hz, it should not be surprising to find a deterioration in speech intelligibility performance once the NIHL extends into this range of frequencies. Also, individuals with sensorineural hearing loss, due either to noise exposure or other factors, usually have greater difficulty understanding speech against a competing background noise environment than in a quiet environment. This common complaint may be minor if the hearing loss is restricted to frequencies at or above 3,000 Hz but may present market difficulty for those with losses below 3,000 Hz. Since the usual pattern of progressive NIHL is one in which the speech frequencies are affected last, it is important to identify NIHL during its initial stages to help prevent future deterioration of hearing sensitivity and speech discrimination abilities.
Occupational health nurses and physicians involved in assessing and monitoring hearing status in hearing conservation programs should refer the worker to an audiologist if a significant change in hearing level (≥10 dB at any frequency in either ear) is observed after the worker has had a minimum of 48 hours to recover from environmental noise exposure. Audiological management of the individual with NIHL may include the use of hearing aids, aural rehabilitation, and assistive listening devices to help improve some of the communication dysfunction experienced in certain listening situation. What, if any, strategies are implemented depends largely on the severity of the communication handicap produced by the noise exposure and the listening needs of the individual.




