
APPENDIX A Waste Management
The Low Level Radioactive Waste Policy Act of 1980 (Public Law 96-573) and its amendment in 1985 (Public Law 99-240, Title I) carry serious implications for any new isotope facility, regardless of its form or location. As succeeding paragraphs will make clear, this legislation puts the onus of disposal of mildly radioactive materials squarely on the states in which they are generated. No new disposal sites have opened since 1980, however, and access to the only two remaining disposal sites in the United States will become severely restricted as of July 1994. One problem for a new facility, thus, is simply ensuring access to a disposal site for the low-level radioactive waste (LLRW) that it generates. A second issue for a facility making and selling radioisotopes and associated equipment, services, or materials arises from the needs of its customers for this same access.
NATURE AND SOURCES OF LOW-LEVEL RADIOACTIVE WASTE (LLRW)
The Low Level Radioactive Waste Policy Act defines LLRW by exclusion in an attempt to distinguish mildly radioactive materials with relatively short half-lives from high level radioactive wastes that must be effectively isolated for many centuries to prevent serious harm to the biosphere. Included in the high level radioactive waste category are spent fuel elements from nuclear reactors, residues from the reprocessing of irradiated uranium to separate out plutonium for weapons production, significant concentrations of radionuclides of transuranic elements (e.g., plutonium), and by-products of reactor operations. LLRW then consists of all other (mildly) radioactive waste, including such things as depleted uranium, activated beam line components; target materials, contami-
nated paper, rags, rubber gloves, and protective clothing; hardware and tools; laboratory glass and plastic; syringes; filters; animal excreta, parts, and carcasses; cleanup materials and irradiated components from nuclear power plants, and even sealed sources that have outlived their utility. An important exclusion from the provisions of the act is radioactive waste generated by the U.S. Department of Energy. The national laboratories are not dependent on the state in which they are located for disposal of radioactive waste. Sixty-five percent of all LLRW is produced and disposed of at the federal level (Coates et al., 1992).
In 1992 waste disposal operators reported receiving over 1,700,000 ft3 (48,000 m3)of LLRW, generating a shade over 1 million curies (Ci) of activity (Fuchs and McDonald, 1993). In the United States, such LLRW accounts for about 85 percent of all radioactive waste by volume but only about 1 percent by activity (Hendee, 1993). Table A-1 and Figure A-1 (adapted from Fuchs and McDonald, 1993) break out those totals by the type of generator: academic, which includes university hospitals and research facilities of all types; government; industrial, including pharmaceutical manufacturers; medical, which encompasses hospitals and clinics, nonuniversity research facilities, and private offices; and utility, which primarily includes the 76 active commercial nuclear power reactors. Industrial sources provided over half of the waste by volume, and utilities contributed over 85 percent of the radioactivity. Medical and academic sources generated less than one-half of one percent of the radioactivity and only 4 percent of the total volume.
The U.S. Nuclear Regulatory Commission (U.S. NRC) has subclassified LLRW into classes A, B, and C for the purposes of setting disposal standards (10 CFR 61). On the basis of concentration, half-life, and stability of the waste form, the regulations demand increasing levels of physical security as the radionuclides become longer-lived or more concentrated. Ninety-five percent of all LLRW and nearly all medical LLRW fall in Class A, the lowest level of security. Even at that
TABLE A-1 LLRW Received at Commercial Disposal Sites in the United States in 1992
|
Generator Category |
Volume (ft3) |
Activity (Ci) |
|
Academic |
44,322 |
1,724 |
|
Government |
158,186 |
40,780 |
|
Industrial |
908,452 |
100,090 |
|
Medical |
26,251 |
398 |
|
Utility |
606,067 |
857,110 |
|
Total |
1,743,279 |
1,000,102 |
|
SOURCE: Fuchs and McDonald, 1993. |
||
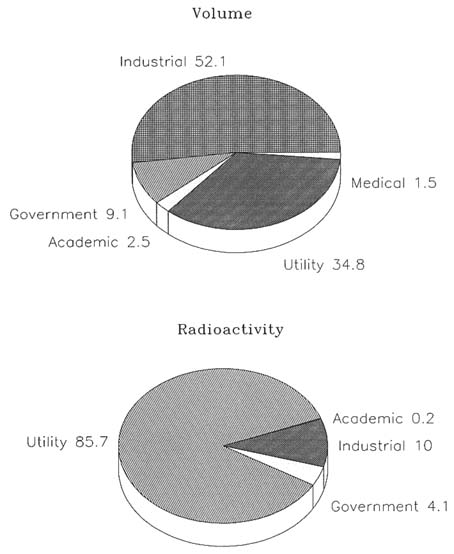
FIGURE A-1 Percentages of volume and radioactivity of low-level radioactive waste by source.
level, however, disposal sites must be designed to protect both humans and the environment for 100 years. For example, institutional control of the site for a century is required, including measures to preclude inadvertent disturbance. The site must be a suitable distance from groundwater and surface waters and located in a region where earthquakes and volcanic activity are very low probability
events. All present U.S. sites employ shallow land burial, the simplest and cheapest method that is allowable under these regulations. Metal containers containing waste are placed in long trenches at least 7.5 m deep and are covered with a clay cap suitably contoured for drainage and erosion control. Future sites are likely to be much more elaborate structures of concrete and steel, because a number of states have already banned the shallow land burial method of disposal.
RISK FROM LLRW
Radiation is very poorly understood by the general public and, as a result, seems to generate fears out of proportion to objective risk. The fact that some radiation injuries become apparent only years after exposure no doubt contributes to this wariness of the public, but radiation standards have been promulgated by various national and international groups for more than 50 years. In the present case, the U.S. NRC has decreed that releases of radiation from any artificial source, including LLRW disposal sites, should not exceed 0.25 milliSieverts (mSv; 25 mrem) per year to the whole body or any organ other than the thyroid, which is given a limit of 0.75 mSv (75 mrem) per year. Eisenbud (1980) estimated that LLRW from isotope use in biology and medicine contributes less than 0.01 mSv (1 mrem) to each person's annual radiation exposure, and the U.S. Environmental Protection Agency estimates that the annual exposures of people living near a disposal facility would be something under 0.1 mSv (10 mrem) (Council on Scientific Affairs, 1989).
Although scientists working with radiation have traditionally taken a very conservative no-threshold view of safety, that is, all radiation is assumed to be injurious, it might be well to put these exposure limits in perspective by considering some of the other sources of radiation to which the general public is exposed. As Table A-2 illustrates the average person in the United States today receives about 3.6 mSv (360 mrem) of radiation annually, of which roughly 3.0 mSv (300 mrem) comes from natural and largely unavoidable sources (National Council on Radiation Protection and Measurements, 1987). Radon gas from radium in the soil is an example of such sources. Cosmic rays are another. Internal radionuclides carried naturally in the body include potassium-40, lead/polonium-210, carbon-14, and radium-228/224. Subsamples of the population can be exposed to much higher doses. Denver residents, who have less atmosphere above them than those who live at sea level, get close to twice the average dose of 0.27 mSv/year (27 mrem/yr) from cosmic rays. Smokers' lungs are thought to absorb as much as 160 to 200 mSv/yr (16,000–20,000 mrems/yr) from polonium in tobacco smoke. Artificial sources of radiation other than from waste may vary greatly as well. Diagnostic radiology is estimated to contribute about 0.5 mSv (50 mrem) to each person's annual exposure, but this obviously could be much greater in those with poor health or many injuries. The LLRW contribution, even for people living near disposal sites and the current exposure standards, are thus
TABLE A-2 Average Annual Dose Equivalents from Sources of Radiation Exposure in the United States
|
|
Dose Equivalenta (mSv) |
Effective Dose Equivalent |
|
||
|
Source |
|
mrem |
mSv |
% |
|
|
Natural |
Radonb |
24 |
2,400 |
2.0 |
55> |
|
Cosmic |
0.27 |
27 |
0.27 |
8 |
|
|
Terrestrial |
0.28 |
28 |
0.28 |
8 |
|
|
Internal to human body |
0.39 |
39 |
0.39 |
11 |
|
|
Total natural |
— |
— |
3.0 |
82 |
|
|
Artificial |
Medical |
|
|||
|
|
X-ray diagnosis |
0.39 |
39 |
0.39 |
11 |
|
|
Nuclear medicine |
0.14 |
14 |
0.14 |
4 |
|
|
Consumer products |
0.10 |
10 |
0.10 |
3 |
|
Other |
Occupational |
0.009 |
0.9 |
<0.01 |
<0.3 |
|
Nuclear fuel cycle |
<0.01 |
<1.0 |
<0.01 |
<0.03 |
|
|
Fallout |
<0.01 |
<1.0 |
<0.01 |
<0.03 |
|
|
Miscellaneousc |
<0.01 |
<1.0 |
<0.01 |
<0.03 |
|
|
Total artificial |
— |
— |
0.63 |
18 |
|
|
Total natural and artificial |
|
— |
— |
3.6 |
100 |
|
a To soft tissues. b Dose equivalent to bronchi from radon daughter products. The assumed weighting factor for the effective dose equivalent relative to whole-body exposure is 0.08. c U.S. Department of Energy facilities, smelters, transportation, etc. SOURCE: National Council on Radiation Protection and Measurements (1987). |
|||||
extremely low. Public resistance to new disposal sites has nevertheless been formidable and has produced a gridlock that could easily become a crisis for nuclear medicine in the next few years.
DISPOSAL SITES
In the early days of atomic energy shortly after World War II, the Atomic Energy Commission was in charge of all aspects of atomic energy, including waste disposal. This generally meant burial on federal lands or, especially for LLRW, dumping in the oceans or large waterways. The Atomic Energy Act Amendments of 1959 opened the door to state administration of their own radiation safety programs, and by 1971 New York, Kentucky, Illinois, Washington, South Carolina, and Nevada owned LLRW disposal sites and had them operated by commercial contractors. By the late 1970s the first three of these had closed, one because it was full and two because of management problems and increased environmental concerns by state governments (and the public). The three remaining sites took in increased volumes from all over the country, and political opposition to serving as dump sites for the rest of the nation grew quickly. In 1979, the governors of Washington, Nevada, and South Carolina threatened to close the sites unless some more equitable plan for sharing this burden was devised.
The result was the Low Level Radioactive Waste Policy Act of 1980. In it, the U.S. Congress decreed that each state would be responsible, by January 1, 1986, for disposing of the LLRW generated within its borders. It also suggests that the best way to do this would be through regional compacts, or agreements to share a disposal facility. The third key provision was that such compacts would be allowed, after January 1, 1986, to exclude waste generated outside the compact states (without such permission attempts to exclude waste would be prohibited by the commerce clause of the Constitution forbidding the states from impeding the free flow of interstate commerce). In 1985 Congress amended the act because no compacts had been ratified and no new sites had been selected. The amendments extended the deadline until January 1, 1993, but provided a series of planning milestones that states without sites would have to meet to maintain access to existing disposal sites. A very important provision designed to exert additional pressure for site development by state governments was the ''take title" provision, which required states that had not arranged for disposal for its in-state LLRW generators by January 1, 1996, to take title to the waste and assume liability for any damages. Even though the "take title" clause of the 1985 amendments was ruled unconstitutional by the U.S. Supreme Court in 1991, effectively shifting the disposal burden from the state governments back to the waste generators themselves, some progress has occurred. All but a few states have joined compacts, four applications for LLRW disposal licenses are under review by the U.S. NRC and seven other states have begun siting studies. On the other hand, no new sites have opened or are likely to open before 1996, the proposed new sites
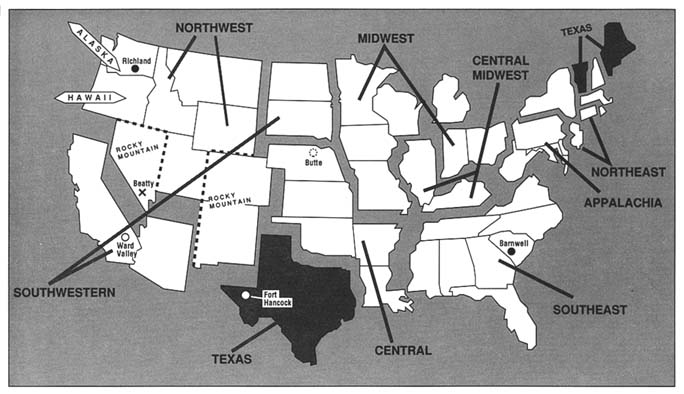
are still not fully clear of all legal and political hurdles, the Nevada site has shut down completely, and the Washington site has closed to waste generators outside the Northwest and Rocky Mountain compacts. The South Carolina legislature, after fierce debate, voted to restrict access to its disposal site at Barnwell to Southeast compact states as of July 1994, and on January 1, 1996, that facility will be closed to all wastes. As of that date, LLRW generators in the following states will have access to a disposal site: Alaska, Hawaii, Washington, Oregon, Idaho, Montana, Wyoming, Utah, Nevada, Colorado, and New Mexico. Generators in California, Arizona, the Dakotas, Texas, Vermont, and Maine will probably have to store their wastes on-site for 1 to 2 years; those in the Central and Southeast compacts may have a disposal site before 2000; but the remaining states, mostly in the Midwest and the Northeast, will very likely be without sites at least until the turn of the century. Figure A-2 summarizes the current organization of compacts and their access to disposal sites.
IMPLICATIONS FOR ISOTOPE PRODUCTION AND USE
Although numerous critics (e.g., Coates et al., 1992) have called for still further revisions of federal law to speed the process of providing safe, economical, and equitable disposal of LLRW for all U.S. generators, members of the relevant U.S. House and U.S. Senate committees did not revisit the topic in the 103rd Congress (Nuclear Waste News, 1993). Thus, both current and future (e.g., National Biomedical Tracer Facility [NBTF]) LLRW generators will have to deal with this problem of access to disposal sites. To estimate the possible volume and costs of waste disposal by an accelerator facility of the sort proposed for NBTF, data were collected from the Tri-University Meson Facility cyclotron in Vancouver, British Columbia, Canada. This facility typically has two disposal shipments per year. In 1992 the two combined shipments consisted of 11.7 gigabecquerels (GBq) of radioactivity, and weighed 15,940 kg. Each of the two shipments cost about $5,000 (Canadian) for shipping, and about $60,000 (Canadian) for disposal. Isotope production facilities will be affected not merely by their own waste generation but also by problems encountered by their research, medical, and commercial customers. Over the next 5 years at least, regardless of the location or nature of any NBTF, a substantial portion of its potential customers are likely to be faced with on-site LLRW storage as their only option. All users of radioisotopes are limited by the terms of their license to specified quantities of each radionuclide. If forced to store waste on-site, an increasing portion of the allowable amounts of some isotopes could be tied up in wastes. Many of the radionuclides used in clinical medicine have relatively short half-lives and may be stored until they have decayed to background levels (10 half-lives is commonly taken as the rule of thumb in estimating the required storage time) and then disposed of as ordinary trash, albeit still in conformity with regulations governing hazardous chemical or biological waste. Some of the longer-lived
isotopes, such as cobalt-60, molybdenum-99/technetium-99m generators, and gadolinium-153 bone densitometry sources, are shipped back to the manufacturer for disposal, but others in wide use have half-lives ranging from months (iron-125, xenon-127, strontium-89, iridium-192) to years (hydrogen-3) or even centuries (carbon-14). Storage requirements will no doubt vary widely. A 1989 paper reports that the Mayo Clinic in Rochester, Minn. generates 6,000 ft3 (170 m3) of LLRW annually, and the University of Cincinnati's 1987 waste was 1,755 ft3 (50 m3), even though two small hospitals in Illinois found the disposal problem to be negligible (Council on Scientific Affairs, 1989). Much has been done in the way of volume reduction since 1980, despite steadily rising activity levels, as generators correctly anticipated rising prices and dwindling access. Conscientious segregation of nonradioactive and radioactive waste, compaction, evaporation, decontamination, and incineration have reduced the total volume of LLRW sent to commercial dump sites from over 3.5 million ft3 (99,000 m3) in 1980, to 1.7 million ft3 (48,000 m3) in 1993. It is probably safe to assume that most of the cost-effective volume reduction techniques are already in use for on-site storage as well as for shipment to disposal sites.
New York is one of the states that will be left without access to a disposal site after July 1994, and although the state has begun the process of developing a site of its own, one of its first steps was a survey of its current LLRW generators' on-site storage capacities, their abilities to expand those capacities, and the economic viability of establishing a separate centralized storage site solely for Class A LLRW from medical and academic sources. The recently completed study (New York State Energy Research and Development Authority, 1993) reported that 142 facilities will have to store LLRW on-site for extended periods if New York is denied access to existing disposal sites. These facilities currently expect to produce approximately 50,000 ft3 (1,400 m3) of LLRW each year. Forty-eight of these facilities have less than 1 year of storage capacity, and 27 will be able to store LLRW for 6 months or less. This assumes that many of the generators will be able to amend their licenses to accommodate the increases in the amounts of on-site material. Making some further assumptions about the ability of these facilities to expand their storage capacity, the study still finds that 16 facilities will have less than 2 years' capability. Fifteen of those 16 are medical and academic institutions, accounting for about 70 percent of the expected medical and academic LLRW.
The final piece of the New York study attempted to assess the economic viability (i.e., the ability to pay capital and operating costs from revenue) of a hypothetical central storage facility for Class A medical and academic LLRW. It found that generators were extremely sensitive to prices. At the lowest hypothetical storage fee ($25/ft3), such generators reported that they would only send about 25 percent of their anticipated volume, opting instead for on-site storage or treatment or ceasing activities that generate LLRW. This would leave the facility well short of the break-even point, even in the unrealistic capital cost of $10
million. (North Carolina expects to have spent $80 million by the time that it completes siting and licensing, before ever turning over a spade of soil.)
REFERENCES
Blake, E. M. 1993. Twenty Nagging Questions and Not-Necessarily-Satisfying Answers About LLW Management in the United States. Nuclear News (December):42–45.
Coates, D., V. Heid, and M. Munger. 1992. The Disposal of Low-Level Radioactive Waste in America: Gridlock in the States. St. Louis: Center for the Study of American Business.
Council on Scientific Affairs, American Medical Association. 1989. Low-Level Radioactive Wastes. Journal of the American Medical Association 262:669–674.
Eisenbud, M. 1980. Radioactive Wastes from Biomedical Institutions. Science 207:1299.
Fuchs, R. L., and S. D. McDonald. 1993. 1992 State-by-State Assessment of Low-Level Radioactive Wastes Received at Commercial Disposal Sites. Prepared for the U.S. Department of Energy by EG&G Idaho, Inc. Idaho Falls, Idaho.
Hendee, W. R. 1993. Disposal of Low-Level Radioactive Waste. J. American Medical Association 269:2403–2406.
National Council on Radiation Protection and Measurements. 1987. Ionizing Radiation Exposure of the Population of the United States. NCRP Report 93:15, 40, 53. Bethesda, Md.
New York State Energy Research and Development Authority. 1993. Low-Level Radioactive Waste Storage Study. Albany, N.Y.: New York State Energy Research and Development Authority.
Nuclear Waste News. January 21, 1993. Not with a 10-foot pole. Nuclear Waste News 13(3):21.










