
APPENDIX E
Guidelines for Adolescent Preventive Services
INTRODUCTION
Changes in adolescent morbidity and mortality during the past several decades have created a health crisis for today's youth. Unintended pregnancy, STDs [sexually transmitted diseases] including HIV [human immunodeficiency virus], alcohol and drug abuse, and eating disorders are just some of the health problems faced by an increasing number of adolescents from all sectors of society. This health crisis requires a fundamental change in the emphasis of adolescent services—a change whereby a greater number of services are directed at the primary and secondary prevention of major health threats facing today's youth. School and community organizations have responded to the need for change by increasing health education programming. Primary care physicians and other health providers must respond by making preventive services a greater component of their clinical practice.
Guidelines for Adolescent Preventive Services (GAPS) can direct providers in how to deliver these services.
GAPS is a comprehensive set of recommendations that provides a framework for the organization and content of preventive health services.
Reprinted with permission from the American Medical Association, copyright, 1995, 2nd Edition.
GAPS recommendations are organized into four types of services that address 14 separate topics or health conditions.
-
Three recommendations pertain to the delivery of health care services.
-
Seven recommendations pertain to the use of health guidance to promote the health and well-being of adolescents and their parents or guardians.
-
Thirteen recommendations describe the need to screen for specific conditions that are relatively common to adolescents and that cause significant suffering either during adolescence or later in life.
-
One recommendation pertains to the use of immunizations for the primary prevention of selected infectious diseases.
The topics or health conditions addressed by GAPS are:
-
promoting parents' ability to respond to the health needs of their adolescents;
-
promoting adjustment to puberty and adolescence;
-
promoting safety and injury prevention;
-
promoting physical fitness;
-
promoting healthy dietary habits and preventing eating disorders and obesity;
-
promoting healthy psychosocial adjustment and preventing the negative health consequences of sexual behaviors;
-
preventing hypertension;
-
preventing hyperlipidemia;
-
preventing the use of tobacco products;
-
preventing the use and abuse of alcohol and other drugs;
-
preventing severe or recurrent depression and suicide;
-
preventing physical, sexual, and emotional abuse;
-
preventing learning problems; and
-
preventing infectious diseases.
A complete description of how GAPS recommendations were developed, the clinical approach to a comprehensive preventive services visit, and the scientific justification for each recommendation are contained in Guidelines for Adolescent Preventive Services, by Arthur B. Elster, M.D., and Naomi J. Kuznets, Ph.D. (1994), William and Wilkins: Baltimore.
GAPS recommendations are designed to be delivered ideally as a preventive service package during a series of annual health visits between the ages of 11 and 21. The recommended frequency of specific GAPS preventive services are presented in Table E-1. Annual visits offer
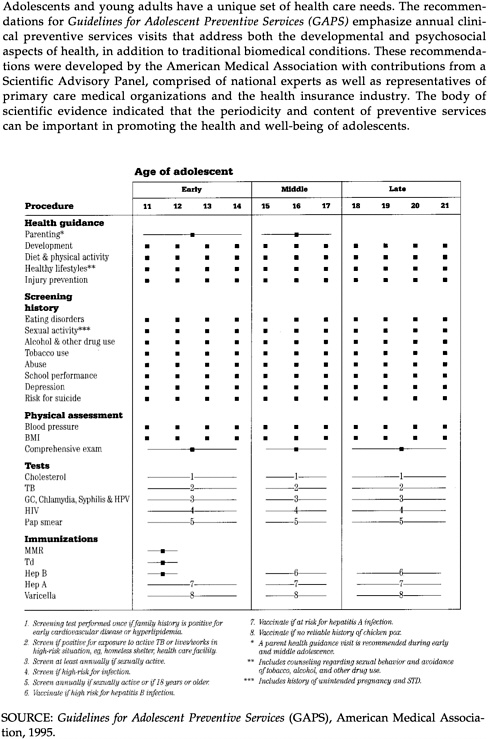
the opportunity to reinforce health promotion messages for both adolescents and their parents, identify adolescents who have initiated health risk behaviors or who are at early stages of physical or emotional disorders, provide immunizations, and develop relationships with the adolescents that will foster an open disclosure of future health information.
RECOMMENDATIONS FOR DELIVERY OF HEALTH SERVICES
The periodicity and manner in which services are delivered to adolescents can be important determinants of the effectiveness of preventive services. The rapid behavioral changes that occur during adolescence require frequent visits to screen for health risk behaviors and to provide health guidance. To ensure that providers obtain accurate information and deliver health guidance appropriate for each adolescent, GAPS recommends that services be tailored to the individual and that information shared by the adolescent during the medical visit remain confidential.
Recommendation 1: From ages 11 to 21, all adolescents should have an annual preventive services visit.
-
These visits should address both the biomedical and psychosocial aspects of health, and should focus on preventive services.
-
Adolescents should have a complete physical examination during three of these preventive services visits. One should be performed during early adolescence (age 11 to 14), one during middle adolescence (age 15 to 17), and one during late adolescence (age 18 to 21), unless more frequent exams are warranted by clinical signs or symptoms.
Recommendation 2: Preventive services should be age and developmentally appropriate, and should be sensitive to individual and sociocultural differences.
Recommendation 3: Physicians should establish office policies regarding confidential care for adolescents and how parents will be involved in that care. These policies should be made clear to adolescents and their parents.
RECOMMENDATIONS FOR HEALTH GUIDANCE
Adolescence is a time of experimentation and risk taking. Developmentally, adolescents are at a crossroads of health. Emerging cognitive abilities and social experiences lead adolescents to question adult values and experiment with health risk behaviors. Some behaviors threaten cur-
rent health, while other behaviors may have long-term health consequences. The changes in cognitive abilities, however, also offer an opportunity to develop attitudes and lifestyles that enhance health and well-being. GAPS recommends that adolescents receive health guidance annually to help them cope with developmental challenges, develop and maintain healthy lifestyles, improve diet and fitness, and prevent injury. In addition, GAPS recommends health guidance be given to parents and guardians of adolescents to help them respond appropriately to the health needs of their adolescent.
Recommendation 4: Parents or other adult caregivers should receive health guidance at least once during their child's early adolescence, once during middle adolescence and, preferably, once during late adolescence.
This includes providing information about:
-
normative adolescent development, including information about physical, sexual, and emotional development;
-
signs and symptoms of disease and emotional distress;
-
parenting behaviors that promote healthy adolescent adjustment;
-
why parents should discuss health-related behaviors with their adolescents, plan family activities, and act as role models for health-related behaviors;
-
methods for helping their adolescent avoid potentially harmful behaviors, such as:
-
monitoring and managing the adolescent's use of motor vehicles, especially for new drivers;
-
avoiding having weapons in the home. Parents who have weapons in the home should be advised to make them inaccessible to adolescents. If adolescents have weapons, parents and other adult caregivers should ensure that adolescents follow weapon safety procedures.
-
removing weapons and potentially lethal medications from the homes of adolescents who have suicidal intent;
-
monitoring their adolescent's social and recreational activities for the use of tobacco, alcohol and other drugs, and sexual behavior.
-
Recommendation 5: All adolescents should receive health guidance annually to promote a better understanding of their physical growth, psychosocial and psychosexual development, and the importance of becoming actively involved in decisions regarding their health care.
Recommendation 6: All adolescents should receive health guidance annually to promote reduction of injuries.
Health guidance for injury prevention includes the following:
-
counseling to avoid the use of alcohol or other substances while using motor or recreational vehicles, or where impaired judgment may lead to injury;
-
counseling to use safety devices, including seat belts, motorcycle and bicycle helmets, and appropriate athletic protective devices;
-
counseling to resolve interpersonal conflicts without violence;
-
counseling to avoid the use of weapons and/or promote weapon safety;
-
counseling to promote appropriate physical conditioning before exercise.
Recommendation 7: All adolescents should receive health guidance annually about dietary habits, including the benefits of a healthy diet, and ways to achieve a healthy diet and safe weight management.
Recommendation 8: All adolescents should receive health guidance annually about the benefits of physical activity and should be encouraged to engage in safe physical activities on a regular basis.
Recommendation 9: All adolescents should receive health guidance annually regarding responsible sexual behaviors, including abstinence. Latex condoms to prevent STDs, including HIV infection, and appropriate methods of birth control should be made available, as should instructions on how to use them effectively.
Health guidance for sexual responsibility includes the following:
-
counseling that abstinence from sexual intercourse is the most effective way to prevent pregnancy and sexually transmissible diseases (STDs), including HIV infection;
-
counseling on how HIV infection is transmitted, the dangers of the disease, and the fact that latex condoms are effective in preventing STDs, including HIV infection;
-
reinforcement of responsible sexual behavior for adolescents who are not currently sexually active and for those who are using birth control and condoms appropriately;
-
counseling on the need to protect themselves and their partners from pregnancy; STDs, including HIV infection; and sexual exploitation.
Recommendation 10: All adolescents should receive health guidance annually to promote avoidance of tobacco, alcohol, and other abusable substances, and anabolic steroids.
RECOMMENDATIONS FOR SCREENING
GAPS includes recommendations for the screening of biomedical, behavioral, and emotional conditions. Some GAPS recommendations lead to a definitive diagnosis (e.g., cervical culture in females to diagnose gonorrhea). Other recommendations lead to a presumptive diagnosis (e.g., urine test for leukocyte esterase in males to screen for gonorrhea or asking about use of alcohol or other drugs during the past six months to screen for substance use) that must be confirmed with additional assessment. Physicians can use information from the initial screening to decide whether to continue the assessment themselves or to refer the adolescent elsewhere. Health risk behaviors may, in some adolescents, be interrelated and co-occur. Adolescents who are found to engage in one health risk behavior, therefore, should be asked about involvement in others.
Recommendation 11: All adolescents should be screened annually for hypertension according to the protocol developed by the National Heart, Lung, and Blood Institute Second Task Force on Blood Pressure Control in Children.
-
Adolescents with either systolic or diastolic pressures at or above the 90th percentile for gender and age should have blood pressure (BP) measurements repeated at three different times within one month, under similar physical conditions, to confirm baseline values.
-
Adolescents with baseline BP values greater than the 95th percentile for gender and age should have a complete biomedical evaluation to establish treatment options. Adolescents with BP values between the 90th and 95th percentiles should be assessed for obesity and their blood pressure monitored every six months.
Recommendation 12: Selected adolescents should be screened to determine their risk of developing hyperlipidemia and adult coronary heart disease, following the protocol developed by the Expert Panel on Blood Cholesterol Levels in Children and Adolescents.
-
Adolescents whose parents have a serum cholesterol level greater than 240 mg/dl and adolescents who are over 19 years of age should be screened for total blood cholesterol level (nonfasting) at least once.
-
Adolescents with an unknown family history or who have multiple
-
risk factors for future cardiovascular disease (e.g., smoking, hypertension, obesity, diabetes mellitus, excessive consumption of dietary saturated fats and cholesterol) may be screened for total serum cholesterol level (nonfasting) at least once at the discretion of the physician.
-
Adolescents with blood cholesterol values less than 170 mg/dl should have the test repeated within five years. Those with values between 170 and 199 mg/dl should have a repeated test. If the average of the two tests is below 170 mg/dl, total blood cholesterol level should be reassessed within five years. A lipoprotein analysis should be done if the average cholesterol value of the two tests if 170 mg/dl or higher, or if the result of the initial test was 200 mg/dl or greater.
-
Adolescents who have a parent or grandparent with coronary artery disease, peripheral vascular disease, cerebrovascular disease, or sudden cardiac death at age 55 or younger should be screened with a fasting lipoprotein analysis.
-
Treatment options are based on the average of two assessments of low-density lipoprotein cholesterol. Values below 110 mg/dl are acceptable; values between 110 and 129 mg/dl are borderline, and the lipoprotein status should be reevaluated in one year. Adolescents with values of 130 mg/dl or greater should be referred for medical evaluation and treatment.
Recommendation 13: All adolescents should be screened annually for eating disorders and obesity by determining weight and stature, asking about body image and dieting patterns.
-
Adolescents should be assessed for organic disease, anorexia nervosa, or bulimia if any of the following are found: weight loss greater than 10 percent of the previous weight; recurrent dieting when not overweight, use of self-induced emesis, laxatives, starvation, or diuretics to lose weight; distorted body image; or body mass index (weight/height 2) below the fifth percentile.
-
Adolescents with a body mass index (BMI) equal to or greater than the 95th percentile for age and gender are overweight and should have an in-depth dietary and health assessment to determine psychosocial morbidity and risk for future cardiovascular disease.
-
Adolescents with a BMI between the 85th and 94th percentiles are at risk for becoming overweight. A dietary and health assessment to determine psychosocial morbidity and risk for future cardiovascular disease should be performed on these youth if:
-
their BMI has increased by two or more units during the previous 12 months;
-
-
there is a family history of premature heart disease, obesity, hypertension, or diabetes mellitus;
-
they express concern about their weight;
-
they have elevated serum cholesterol levels or blood pressure.
If this assessment is negative, these adolescents should be provided general dietary and exercise counseling and should be monitored annually.
Recommendation 14: All adolescents should be asked annually about their use of tobacco products, including cigarettes and smokeless tobacco.
-
Adolescents who use tobacco products should be assessed further to determine their patterns of use.
-
A cessation plan should be provided for adolescents who use tobacco products.
Recommendation 15: All adolescents should be asked annually about their use of alcohol and other abusable substances and about their use of over-the-counter or prescription drugs for nonmedical purposes, including anabolic steroids.
-
Adolescents who report any use of alcohol or other drugs or inappropriate use of medicines during the past year should be assessed further regarding family history; circumstances surrounding use; amount and frequency of use; attitudes and motivation about use; use of drugs; and the adequacy of physical, psychosocial, and school functioning.
-
Adolescents whose substance use endangers their health should receive counseling and mental health treatment, as appropriate.
-
Adolescents who use anabolic steroids should be counseled to stop.
-
The use of urine toxicology for the routine screening of adolescents is not recommended.
-
Adolescents who use alcohol and other drugs should also be asked about their sexual behavior and their use of birth control products.
Recommendation 16: All adolescents should be asked annually about involvement in sexual behaviors that may result in unintended pregnancy and STDs, including HIV infection.
-
Sexually active adolescents should be asked about their use and motivation to use condoms and contraceptive methods, their sexual orientation, the number of sexual partners they have had in the past six
-
months, if they have exchanged sex for money or drugs, and their history of prior pregnancy or STDs.
-
Adolescents at risk for pregnancy, STDs (including HIV), or sexual exploitation should be counseled on how to reduce this risk.
-
Sexually active adolescents should also be asked about their use of tobacco products, alcohol, and other drugs.
Recommendation 17: Sexually active adolescents should be screened for STDs.
STD screening includes the following:
-
a cervical culture (females) or urine leukocyte esterase analysis (males) to screen for gonorrhea;
-
an immunologic test of cervical fluid (female) or urine leukocyte esterase analysis (male) to screen for genital chlamydia;
-
a serologic test for syphilis if they have lived in an area endemic for syphilis, have had other STDs, have had more than one sexual partner within the last six months, have exchanged sex for drugs or money, or are males who have engaged in sex with other males;
-
evaluation for human papilloma virus by visual inspection (males and females) and by Pap test.
-
If a presumptive test for STDs is positive, tests to make a definitive diagnosis should be performed, a treatment plan instituted according to guidelines developed by the Centers for Disease Control, and the use of condoms encouraged.
-
The frequency of screening for STDs depends on the sexual practices of the individual and the history of previous STDs.
Recommendation 18: Adolescents at risk for HIV infection should be offered confidential HIV screening with the ELISA [enzyme-linked immunosorbent assay] or confirmatory test.
-
Risk status includes having used intravenous drugs, having had other STD infections, having lived in an area with a high prevalence of STDs and HIV infection, having had more than one sexual partner in the last six months, having exchanged sex for drugs or money, being male and having engaged in sex with other males, or having had a sexual partner who is at risk for HIV infection.
-
Testing should be performed only after informed consent is obtained from the adolescent.
-
Testing should be performed only in conjunction with both pre-and post-test counseling.
-
The frequency of screening for HIV infection should be determined by the risk factors of the individual.
Recommendation 19: Female adolescents who are sexually active or any female 18 or older should be screened annually for cervical cancer by use of a Pap test.
Adolescents with a positive Pap test should be referred for further diagnostic assessment and management.
Recommendation 20: All adolescents should be asked annually about behaviors or emotions that indicate recurrent or severe depression or risk of suicide.
-
Screening for depression or suicidal risk should be performed on adolescents who exhibit cumulative risk as determined by declining school grades, chronic melancholy, family dysfunction, homosexual orientation, physical or sexual abuse, alcohol or drug use, previous suicide attempt, or suicidal plans.
-
If suicidal risk is suspected, adolescents should be evaluated immediately and referred to a psychiatrist or other mental health professional, or else should be hospitalized.
-
Nonsuicidal adolescents with symptoms of severe or recurring depression should be evaluated and referred to a psychiatrist or other mental health professional for treatment.
Recommendation 21: All adolescents should be asked annually about a history of emotional, physical, or sexual abuse.
-
If abuse is suspected, adolescents should be assessed to determine the circumstances surrounding abuse and the presence of physical, emotional, and psychosocial consequences, including involvement in health risk behavior.
-
Health providers should be aware of local laws about the reporting of abuse to appropriate state officials, in addition to ethical and legal issues regarding how to protect the confidentiality of the adolescent patient.
-
Adolescents who report emotional or psychosocial sequelae should be referred to a psychiatrist or other mental health professional for evaluation and treatment.
Recommendation 22: All adolescents should be asked annually about learning or school problems.
-
Adolescents with a history of truancy, repeated absences, or poor or declining performance should be assessed for the presence of conditions that could interfere with school success. These include learning disability, attention deficit hyperactivity disorder, medical problems, abuse, family dysfunction, mental disorder, or alcohol or other drug use.
-
This assessment, and the subsequent management plan, should be coordinated with school personnel and with the adolescent's parents or caregivers.
Recommendation 23: Adolescents should receive a tuberculin skin test if they have been exposed to active tuberculosis, have lived in a homeless shelter, have been incarcerated, have lived in or come from an area with a high prevalence of tuberculosis, or currently work in a health care setting.
-
Adolescents with a positive tuberculin skin test should be treated according to CDC [Centers for Disease Control and Prevention] treatment guidelines.
-
The frequency of testing depends on risk factors of the individual adolescent.
RECOMMENDATIONS FOR IMMUNIZATIONS
The fourth set of recommendations involves the use of vaccinations to prevent infectious disease. National immunization policies have changed recently with the development of the vaccination against Hepatitis B virus and the resurgence of measles and rubella among adolescent and adult populations. Providers will need to determine the number and type of previous vaccinations to assess the immunization needs of the adolescent.
Recommendation 24: All adolescents should receive prophylactic immunizations according to the guidelines established by the federally convened Advisory Committee on Immunization Practices.
-
Adolescents should receive a bivalent Td [tetanus and diphtheria toxoid] vaccine booster at the 11–12 year visit if not previously vaccinated within 5 years. With the exception of the Td booster at 11–12 years, routine boosters should be administered every 10 years.
-
Adolescents should receive a second dose of MMR [measles–
-
mumps–rubella] at age 11–12 years, unless there is documentation of two vaccinations earlier during childhood. MMR should not be administered to pregnant adolescents.
-
Adolescents 11–12 years of age who have not been immunized as part of a routine childhood schedule and who do not have a reliable history of chickenpox should be offered varicella vaccine.
-
Hepatitis B immunizations should be initiated at 11–12 years of age. Older unvaccinated adolescents with identified risk factors for HBV [Hepatitis B virus] infection should also be vaccinated. Major risk factors for acquisition of HBV infection in adolescents include multiple sex partners, intravenous drug abuse, living in areas with increased rates of parenteral drug abuse, teenage pregnancy, and/or sexually transmitted diseases. Widespread use of Hepatitis B vaccination is encouraged because risk factors are not always easily identifiable among adolescents.
-
Hepatitis A immunizations should be given to adolescents who are traveling or living in countries with high or intermediate endemicity of Hepatitis A virus (HAV), live in communities with high endemic rates of HAV, have chronic liver disease, are injecting drug users or are males who have sex with males.
-
Ideally all vaccinations should be administered at the scheduled 11–12 year visit.
CLINICAL APPLICATIONS
GAPS provides a strategy to organize the content and delivery of care within a clinical setting to address the health issues of adolescents. Most primary care providers offer some preventive services to adolescents but GAPS suggests a comprehensive approach that includes screening and health guidance on an annual basis. All adolescents should be scheduled for an initial GAPS visit at the 11–12 year visit.
DIFFERENCES BETWEEN GAPS AND TRADITIONAL APPROACHES TO HEALTH CARE
The major differences between GAPS services and the traditional approaches to health care are the emphasis on comprehensive rather than categorical services for adolescents, visits for their parents or guardians, and the orientation to preventive care. These differences are summarized in the following table.
GAPS Recommendations Compared with Traditional Approaches to Adolescent Health Care
|
GAPS Recommendations |
Traditional Health Care |
|
Provider plays an important role in coordinating adolescent health promotion. This role complements health guidance that adolescents receive from their family, school, and community. |
Provider role is considered to be independent of health education programs offered by schools, family, and the community. |
|
Preventive interventions target social morbidities such as alcohol and other drug use, suicide, STDs, (including HIV), unintended pregnancy, and eating disorders. |
Emphasis is on biomedical problems alone, such as the medical consequences of health risk behaviors (e.g., STDs, unintended pregnancy). |
|
Provider emphasizes screening of comorbidities; i.e., adolescent participation in clusters of specific health risk behaviors. |
Emphasis is on the diagnosis and treatment of categorical health conditions. |
|
Annual visits permit early detection of health problems and offer an opportunity to provide health education and develop a therapeutic relationship. |
Visits are scheduled only as needed for acute care episodes or for other specific purposes (e.g., immunizations or an examination prior to participating in sports). |
|
Provider performs three comprehensive physical examinations: one during early, middle, and late adolescence. |
Current standards vary from as necessary to examinations every two years during adolescence. |
|
It is recommended that all parents receive education about adolescent health care at least twice during the child's adolescence. |
Parents are included in the health care of the adolescent solely at the discretion of the provider, who also serves as the sole decision maker of what health education topics should be addressed with parents. |














