
4
Intended Births
The nations that signed the Programme of Action of the International Conference on Population and Development (ICPD) committed to try "… by the year 2015, … to provide universal access to a full range of safe and reliable family-planning methods and to related reproductive health services which are not against the law" (United Nations, 1994:sect 9.1). Family planning programs contribute to reproductive health in two main ways: by allowing women and men to exercise the "freedom to decide if, when and how often" to have children (as included in the ICPD definition of reproductive health) and by reducing the number of times that a woman is exposed to the risks of unsafe pregnancy and delivery. In addition to these direct effects, there is evidence for a long-term impact as well: families that are not burdened by excess fertility can and do invest more in the nutrition, schooling, and health care of their wanted children. This investment, in turn, can be expected to improve the reproductive health of the next generation, among other benefits.
In this chapter we first discuss the evidence that unintended pregnancies and births are common. We next summarize the evidence that unintended pregnancies are harmful for the health and well-being women and their families. The bulk of this chapter then deals with some of the main problems confronting family planning programs and provision of safe abortions, which are the primary means through which public policy facilitates achievement of the goal of intended births. The final section deals with the broader policy environment.
DEFINING AND MEASURING INTENDED FERTILITY
There is no unambiguous definition of ''intended birth" that would apply to the different societies covered by this report, nor to all families within any society. "Intentions" fit actual decisions and behavior only imperfectly: the answers to standardized questions used in household surveys cannot fully capture the complexity of the process by which intentions are formed or their intensity. However, some measures, even imprecise ones, are needed to gauge the extent of the problem of unintended pregnancy, and survey data on fertility intentions have been found to predict subsequent fertility behavior well, at least at a population level (Westoff, 1990).1
The best recent source of comparable data for large populations in developing countries is the Demographic and Health Surveys (DHS). Using different items in the standard DHS questionnaires, there are two broad approaches to measuring intentions. One approach relies on answers to direct questions about the last birth or current pregnancy. In most DHS surveys, women are asked, for each live birth that occurred less than 5 years before the interview: "At the time you became pregnant with [Name], did you want to become pregnant then, did you want to wait until later, or did you want no more children at all?" Women who are pregnant at the time of the interview are asked analogous questions about their current pregnancy.
We use the term "unwanted" to refer to a pregnancy or birth to a woman who reports that she did not want any more children; "mistimed" for a pregnancy or birth to woman who wants more children, but not in the near future, and "unintended" to cover both.2
The second approach relies on hypothetical questions about all children. Most DHS surveys include this question: "If you could go back to the time when you did not have any children and could choose exactly the number of children to have in your whole life, how many would that be?" The answers can be averaged for a population, or a desired total
fertility rate can be estimated by deleting recent births to women who report an ideal family size lower than their actual number of living children (Cochrane and Sai, 1993; Bongaarts, 1990). An alternative is to construct a "synthetic estimate" of desired total fertility rates, summarizing estimates of proportions of women at each parity who report that they want no more children. These indirect methods do not allow estimation of mistimed (as opposed to entirely unwanted) pregnancies, and they require a hypothetical recasting of respondents' lives that may not be especially meaningful. But they avoid one weakness of the direct questions about specific pregnancies: "[U]nderreporting is apparently common and is presumably caused by a reluctance of women to classify their offspring as unwanted" (Bongaarts, 1991:223).
Since desired family size has fallen in almost all developing countries for which it has been measured, it has been conventional to focus on only one aspect of failure to achieve reproductive goals, namely, unwanted childbearing. Yet as Kingsley Davis (1967) noted three decades ago, "family planning" literally construed should include the notion of couples planning to have a family. Infertility can lead to loss of social status, divorce, and other negative consequences, as well as being a cause of tremendous unhappiness.
Larsen and Menken (1989) provide useful evidence on the prevalence of infertility from a combination of demographic surveys and microsimulation of populations with varying amounts of deliberate fertility control. Larsen (1994) estimates that the proportion of women sterile by age 34 in 17 sub-Saharan African countries varied from a low of 11 percent in Burundi to a high of 31 percent in Cameroon. She concluded that "the true prevalence of sterility in sub-Saharan Africa is so substantial that it ceases to be a merely individual problem and has become a public health issue" (Larsen, 1994:469). As in previous reviews, Larsen found great geographic variation in apparent infertility, which she plausibly ascribes to geographic variation in the incidence of reproductive tract infections. In Chapter 3 we discuss the needs for programs to control sexually transmitted diseases (STDs), which is the most effective way to prevent infertility in the countries most affected.
Whose Intentions?
A crucial question in all societies is whose fertility intentions count in deciding if a birth is "intended." The potential mother is obviously most directly affected, and any definition of intention that did not include her wishes and interests would be unacceptable. Potential fathers also have, or are expected to have, a lot at stake in fertility decisions. A widely shared ideal would call for good spousal communication and socially
approved methods of reconciling disagreements that respect the rights of all involved.
A recent review of published studies, based on both surveys and qualitative research, showed (Mason and Taj, 1987:632;631) "more often than not … women's and men's fertility goals are very similar. When gender differences do occur … they usually are small and are of both types (men more pronatalist than women and vice versa)." These are population averages, which could be consistent with some degree of offsetting disagreement between spouses. More importantly, general agreement on preferences for the number of children does not imply agreement among spouses about the desirability of particular behaviors (modern contraception, periodic abstinence, or induced abortion) to implement those goals. Husbands' disapproval is one of the most common reasons for women's not using contraception reported in surveys by women at risk of an unwanted pregnancy. As Bongaarts and Bruce (1995) point out, more than one-half of such women in most African countries also report that they have never discussed contraception with their husbands, suggesting that they may feel powerless to influence the decision or even raise the topic. Casterline, Perez, and Biddlecom (1996) report similar results from more intensive interviews in the Philippines.
Intergenerational differences in family size goals may be more pronounced than interspousal differences. It is commonly believed by family planning program managers in South Asia, for example, that the chief opponents of small families are domineering mothers-in-law. Caldwell (1986) has argued that the patriarchs in West African lineage systems have a strong interest in seeing their sons have many children who can perform economic and religious services and generate prestige for their grandfathers. We know of no studies directly comparing the stated preferences of older people for grandchildren with the fertility goals of their adult children. The notion of a couple as the only decision makers whose preferences should count is probably a minority view in the world as a whole, and a recent development even where it is now the dominant view. Marriage and fertility decisions are widely regarded as too important to leave solely to prospective spouses and parents, particularly young ones. In practice, methods for estimating the extent of unwanted fertility and unmet needs for family planning implicitly take the woman's (potential mother's) stated intentions as paramount. The justification is that a woman is the person whose physical health is directly at risk in pregnancy and delivery; in all societies women, on average, bear the major share of responsibilities for child care.
Unwanted Pregnancies and Births
Direct Measures
Figure 4-1 shows the proportions of recent births and current pregnancies reported as unwanted in the most recent DHS survey in 34 countries, grouped by region.3 The proportion varies widely among countries within regions, but it is clearly lowest in sub-Saharan Africa, where large desired family sizes are still reported, and generally highest in Latin America, the Middle East, and North Africa. Outside Africa, the proportion of births unwanted ranges in most countries from 12 to 34 percent.
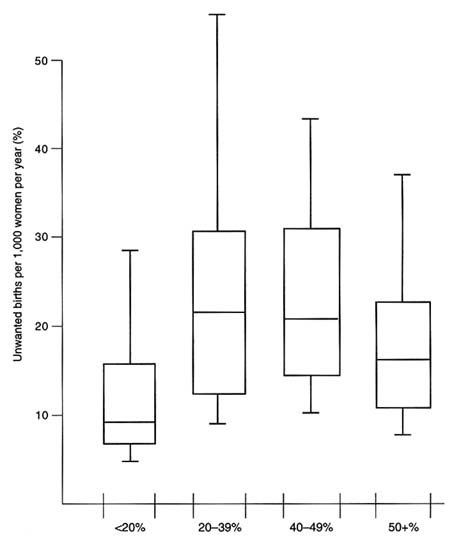
Figure 4-2 shows the proportion of unwanted births in the same countries, grouped by the percentages of married women aged 15-49 currently using any form of contraception (the contraceptive prevalence rate). The countries with the lowest contraceptive prevalence (most of which are in sub-Saharan Africa) have low proportions of unwanted births. The median is 18 percent among the nine countries with contraceptive prevalence of more than 50 percent, considerably higher than the median of 5 percent among the ten countries with contraceptive prevalence of less than 20 percent. This difference does not necessarily mean that women in the highest contraceptive prevalence countries are more likely to have an unwanted birth in a particular year. Precisely because they use contraception more, they are less likely to have a baby than are women in countries where contraceptive use is uncommon. This can be seen in Figure 4-3, showing the range of values for the unwanted birth rate (unwanted births per 1,000 women per year) for countries in the same contraceptive prevalence categories as in Figure 4-2.4 Countries with contraceptive prevalence above 50 percent tend to have lower unwanted birth rates than countries with contraceptive prevalence between 20 and 30 percent, despite having higher proportions of unwanted births, because they have much lower overall birth rates. Women are most at risk of unwanted births in countries where contraceptive use is in the range 20-40 percent, presumably because contraceptive behavior and fertility are lagging behind the more rapid change in fertility preferences.
The proportion of unwanted births is the appropriate measure for discussing the consequences of unwantedness for children. It highlights
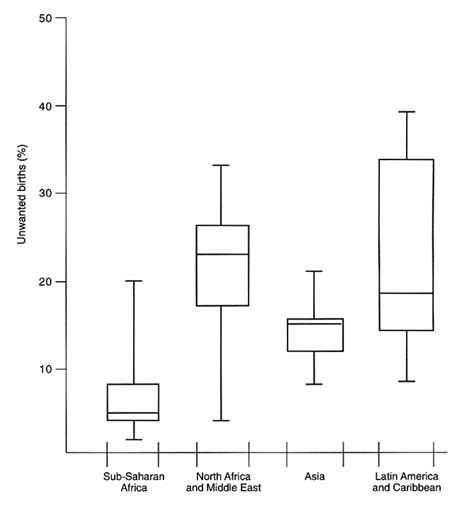
FIGURE 4-1 Percentage of most recent births or current pregnancies unwanted in countries with recent DHS surveys, by region. Wide bars show 25th centile, median, and 75th centile for countries in each category; narrow bars show lowest and highest values. SOURCE: Demographic and Health Surveys.
the situation in many low-fertility societies where contraception and safe abortions are already widely available and well known. The second measure, the unwanted birth rate, is appropriate for gauging the effects of unwanted fertility on women's lives. It shows that women in low-fertility societies are less likely than those in societies with higher fertility rates to be affected by the consequences of unintended pregnancies and births.
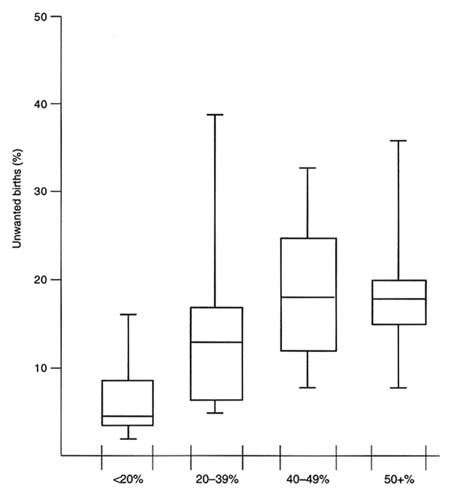
FIGURE 4-2 Percentage of most recent births or current pregnancies unwanted in countries with recent DHS surveys, by contraceptive prevalence. Data are for married women aged 15-49. Wide bars show 25th centile, median, and 75th centile for countries in each category; narrow bars show lowest and highest values. SOURCE: Demographic and Health Surveys.
Indirect Measures
The indirect approaches to measurement also produces high aggregate estimates of the extent of unwanted fertility. Cochrane and Sai (1993) estimate that in developing countries outside China, 30 percent of fertility is unwanted. Bongaarts' aggregate estimates (also based on comparison of ideal with actual family size) show that in countries with high fertility (total fertility rates [TFR] above six births per women), only 16 percent of births appear unwanted. The highest percentages of unwanted births are found in countries in the middle range of fertility rates (between four and six births per woman), where nearly one-third of births are inferred to be unwanted. In low-fertility countries (TFRs below four births per woman), 25 percent of births appear unwanted.
Figure 4-4 shows the proportion of recent births or current pregnancies reported as mistimed in DHS surveys, with countries grouped according to contraceptive prevalence rates.5 These data show no consistent association: the median proportion of mistimed births is just above one-fifth for all countries, across the range of contraceptive prevalence rates. This evidence suggests that the potential demand for family planning for purposes of spacing births can be high even when desired fertility is high. Country-level analyses of DHS data by Westoff and Bankole (1995) confirm that much of the unmet need for contraception inferred from women's replies, especially in sub-Saharan Africa, is motivated by the desire to delay first pregnancies or to space pregnancies, rather than by a desire to stop childbearing.
Determinants
The determinants of unintended fertility are complex, not easily reduced to factors such as lack of education, unfamiliarity with contraception and abortion, or unavailability of services. In Indonesia, for example, Weller et al. (1991) found no significant association between women's education and the wantedness of their most recent child born within the last 5 years. The researchers ascribed this lack of an association to the offsetting effects of education on preferences for lower fertility and on ability to control fertility.
Data for the United States—a country where nearly all adults are literate, publicly funded family planning clinics have existed across the
|
5 |
The percentages shown in Figure 4-4 do not include the births and current pregnancies reported as unwanted (shown in Figure 4-2). |

FIGURE 4-4 Percentage of most recent births or current pregnancies mistimed in countries with recent DHS surveys, by contraceptive prevalence. Wide bars show 25th centile, median, and 75th centile for countries in each category; narrow bars show lowest and highest values. SOURCE: Demographic and Health Surveys.
country since the late 1960s, private outlets for contraceptive supplies and advice are widespread and costs of contraception are very low in relation to incomes (by international standards), and abortion is safe and common (about 30 percent of all pregnancies not ending in miscarriage are terminated by induced abortion)—are revealing. In the United States, nearly one-half of all births in 1988 were unintended (Kost and Forrest, 1995): more than one-quarter of births to women with 16 or more years of schooling
were unintended, and births to women with three or more previous births were more likely to be unintended than were first births. The evidence demonstrates that making contraception and abortion safe and widely available and ensuring that women have high levels of education do not, by themselves, reduce the proportions of unintended pregnancies and births.
Thus, despite the increased use of effective contraception, the proportion of births that are unwanted or mistimed may rise in the early stages of the fertility transition before leveling off or falling. Changes in fertility preferences that accompany the fertility transition make the goal of eliminating unintended births a moving target. There is good evidence that fertility intentions change during the course of the transition to low fertility. Desired family size has fallen in almost every country where trend data are available from DHS and the World Fertility Survey, and the decline has sometimes been dramatic: in Kenya, the average fell by more than three children per woman in 20 years (Rutstein, 1995). Desired family size has fallen quite consistently for almost all birth cohorts of women, and for both educated and uneducated women, in 28 countries for which two or three comparable surveys are available (Rutstein, 1995).
Lloyd (1994:191) argues that "the emergence of 'unwanted fertility' is symptomatic of parents' rising aspirations and their increasing awareness of alternatives to their own and their children's current condition." This gap between intentions and experience appears to grow in the early stages of the demographic transition, when declining mortality, particularly for infants and children, results in larger numbers of children growing up for given numbers of live births. As actual fertility declines, wanted fertility may decline even faster, so that the proportion of births that are unintended may actually grow even while fertility control is becoming more prevalent.
Induced Abortions
The evidence about the prevalence of unintended pregnancy discussed so far is based on women's reports about their intentions and contraceptive behavior. Further evidence that large proportions of pregnancies are unintended comes from the limited available data on the prevalence of induced abortion. The most authoritative estimates are that in 1987, worldwide, there were between 26 and 31 million legal abortions and 10 to 22 million illegal abortions (Henshaw and Morrow, 1990).
By combining direct reports with incomplete data on treatment of abortion complications, Henshaw estimated that in 1990, there were total of 20 million "unsafe abortions," that is, those "not provided through approved facilities and/or persons" (World Health Organization, 1994:2).
These 20 million unsafe abortions are estimated to have resulted in 70,000 deaths of women, of which 69,000 are in developing countries, one-third of them in Africa (World Health Organization, 1994:Table 3). Although some abortions result from pregnancies that were desired at the time of conception, the great majority are likely to have been unintended from the outset.
Abortion complications are not uniquely problems of the young and the unmarried, whose sexual activity may not be considered legitimate. For example, in low-income urban communities in Kenya, women who had recently had abortions were typically in their 20s and had previously given birth (Baker and Khasiani, 1991). ''While not denying that induced abortion is a growing problem among young, educated women [in Africa], evidence suggests that the problem is not limited to them" (Coeytaux, 1988:187).
CONSEQUENCES OF UNWANTED PREGNANCIES AND BIRTHS
Unwanted pregnancies and births can have a variety of negative consequences, for the children themselves, their siblings, their parents, and society as a whole. Unwanted births impose psychological and financial costs to the family, and high fertility, much of it unintended, imposes costs on society as well.
Unwanted pregnancies expose women, especially poor women, to health risks simply by increasing the number of pregnancies and deliveries in their lifetimes. The lifetime risk of complications is determined in great part by the number of pregnancies a woman has. The lifetime risk of maternal mortality is a function of the number of pregnancies and the quality and likelihood of utilization of available health care. For a given level of access and utilization of effective health care, a reduction in the number of pregnancies will bring about lower maternal mortality rates (Koenig et al., 1988).
In adequate medical settings, abortions are not dangerous procedures, yet most abortions in developing countries are carried out in inadequate settings, and the procedure can be dangerous (World Health Organization, 1994; Mashalaba, 1989). Incomplete and septic abortions are one of the four leading causes of pregnancy-related mortality and also account for a huge number of nonfatal injuries (see Chapter 5). Since most induced abortions result from unwanted pregnancies, and safe and effective methods of preventing pregnancies exist and are acceptable in most societies, the morbidity and mortality caused by unsafe abortion are preventable. Contraception can be regarded as primary prevention of complications
of abortion; ensuring medically adequate abortions and postabortion care are secondary and tertiary prevention.
Unintended births are disproportionately risky for the infant. Tables 4-1, 4-2, and 4-3 show, respectively, the proportions of most recent births (or current pregnancies) reported as unintended in six recent DHS surveys, by age of mother; by birth order, and (for second or subsequent pregnancies) by the time since previous (most recent) birth. In every country, births to women over age 35 and fifth- or higher order births are most likely to be reported as unintended.
Similar results have been found in analyses using the ideal family size questions. In 27 countries covered by the DHS surveys in the late 1980s, the majority of women who had given birth to more than five children reported an ideal of fewer children than the number they actually had in every country outside sub-Saharan Africa (except Guatemala). For the African countries, the cutoff for excess fertility was usually eight children—although in all countries, substantial numbers of women with five children (four, in much of Latin America) also reported that they had more children than their ideal number.
Births or pregnancies coming after intervals of 24 months or less are more likely to be reported as unintended, although the differences are less stark than are those associated with high parity and older maternal age.
Since older maternal age, high parity, and short pregnancy intervals are all associated with the risk of infant mortality (Working Group on the Health Consequences of Contraceptive Use and Controlled Fertility, 1989), delaying mistimed pregnancies or eliminating unwanted ones could improve
TABLE 4-1 Most Recent Birth or Current Pregnancy Unintended in Selected Countries, by Mother's Age: in percent
|
Country (Year) |
Mother's Age |
|
|
|
|
<20 |
20-34 |
35+ |
|
Bolivia (1993) |
41.5 |
53.9 |
74.0 |
|
Colombia (1986) |
34.9 |
48.3 |
60.5 |
|
Egypt (1988) |
13.9 |
41.3 |
75.0 |
|
Kenya (1993) |
61.2 |
55.3 |
65.4 |
|
Nigeria (1990) |
13.7 |
12.5 |
21.6 |
|
Philippines (1993) |
37.6 |
46.4 |
58.2 |
|
Tanzania (1991) |
22.7 |
26.1 |
31.7 |
|
Thailand (1987) |
28.3 |
38.4 |
47.2 |
|
SOURCE: Data from Demographic and Health Surveys, unpublished tabulations. |
|||
TABLE 4-2 Most Recent Birth or Current Pregnancy Unintended in Selected Countries, by Birth Order: in percent
|
Country (Year) |
Birth Order |
|
|
|
|
1 |
2-4 |
5+ |
|
Bolivia (1993) |
32.7 |
50.1 |
78.6 |
|
Colombia (1986) |
25.0 |
50.7 |
68.8 |
|
Egypt (1988) |
3.8 |
39.5 |
67.2 |
|
Kenya (1993) |
52.1 |
52.1 |
66.2 |
|
Nigeria (1990) |
11.2 |
9.9 |
22.7 |
|
Philippines (1993) |
22.3 |
47.4 |
63.6 |
|
Tanzania (1991) |
18.7 |
25.0 |
39.5 |
|
Thailand (1987) |
20.7 |
36.3 |
64.4 |
|
SOURCE: Data from Demographic and Health Surveys, unpublished tabulations. |
|||
TABLE 4-3 Recent Higher Order Birth or Current Pregnancy Unintended in Selected Countries, by Interval from Prior Birth to Conception: in percent
|
Country (Year) |
Interval |
|
|
|
|
Less than 24 months |
24 or more months |
|
|
Bolivia (1993) |
68.4 |
60.1 |
|
|
Colombia (1986) |
67.6 |
49.2 |
|
|
Egypt (1988) |
54.0 |
50.2 |
|
|
Kenya (1993) |
67.2 |
56.1 |
|
|
Nigeria (1990) |
21.1 |
13.0 |
|
|
Philippines (1993) |
62.1 |
49.3 |
|
|
Tanzania (1991) |
33.5 |
27.5 |
|
|
Thailand (1987) |
53.4 |
36.7 |
|
|
SOURCE: Data from Demographic and Health Surveys, unpublished tabulations. |
|||
infant and child health simply by reducing disproportionately the number of pregnancies defined as high risk.6
A few studies have shown higher mortality risks for unwanted children
(e.g., Frenzen and Hogan, 1982, for Thailand), especially for unwanted girls (Muhuri and Preston, 1991, for Bangladesh). It would be a mistake to limit consideration of the consequences of unintended fertility to the relatively easily measured effects of morbidity and mortality. Particularly as increasing numbers of young women remain unmarried into their 20s and seek more formal schooling to prepare for new roles, unintended fertility can become more burdensome. In West Africa, for example, it has been argued that adolescent fertility, once expected and welcomed, is increasingly a problem since unmarried girls have to quit school and have diminished chances of good jobs and marriages if they become pregnant (Bledsoe and Cohen, 1993).
The threat as well as the actuality of unintended pregnancy can cause considerable suffering. Dixon-Mueller (1989:145) argues:
An unwanted pregnancy or birth can drive women to attempt a dangerous self-induced abortion; to infanticide; or to prolonged hostility, depression, and despair. [We] must include under women's health not only reported rates of maternal mortality and morbidity associated with contraceptive use and childbirth but also—and perhaps more importantly—women's fears of such conditions or events; the fear of getting pregnant accidentally, for example, or of not getting pregnant at all; the fear of potentially debilitating contraceptive side effects; and the fear of trauma or death in abortion or childbirth.
Deleterious impacts of unintended births on siblings result from the dilution of parental resources, including time and attention as well as material resources. Numerous studies have shown that children in large families receive less schooling and less health care and have poorer nutritional status than children from small families (Lloyd, 1994; Desai, 1995). In Ghana, Lloyd and Gage-Brandon (1994) found that girls are at a particular disadvantage: the more younger siblings they have, the less likely to enroll in secondary school and the more likely to drop out. Crosssectional associations are insufficient evidence of causation, of course, since there is also abundant evidence that parents make conscious decisions to balance the number of children they have with the costs of such investments in child "quality" (e.g., Knodel, Chamratrithirong, and Debavalya, 1987). But there is also some evidence—for example, from an intensive family planning program with a quasi-experimental design (Foster
and Roy, 1996)—showing that the associations are partly causal. Helping people implement their preference for fewer children should result in better schooling and health care for the wanted children. The ICPD Programme of Action emphasized the contribution that increased education of girls could make to lowering fertility rates, and, thus, population growth rates. A similar program of action with increased education of girls as its goal could reciprocally emphasize the contribution that family planning programs could make toward that end.
The effects of unintended births on siblings and parents can be mitigated by institutions and customs that share the economic burden with a wide circle of kin or fellow citizens. Child fosterage in West Africa, for example, "breaks down household economic boundaries and spreads the impact of additional children on family resources across a wider kin network" (Lloyd, 1994:188). However, when social institutions, whether traditional or modern, mitigate the impact of an unwanted birth on the immediate family, however, they are spreading costs of unintended pregnancy more widely within society, not eliminating them.
ROLE OF FAMILY PLANNING AND ABORTION SERVICES
There is a large literature on the design, management, financing, and evaluation of family planning programs, and there have been some very useful recent reviews (Simmons and Lapham, 1987; Phillips and Ross, 1992; Buckner et al., 1995), so this report does not attempt to cover the field in a comprehensive fashion. Rather, we focus on some of the major challenges that face family planning programs in the next decade or two, with an emphasis on those that are shared with other aspects of comprehensive reproductive health services.
Unmet Need for Contraception
A measure of "unmet need" for contraception in developing countries can be formed by cross-classification of responses to survey items on the wantedness of current pregnancies, intentions for childbearing in the near future, and current contraceptive use. Westoff and Bankole (1995), using data from 1990-1994 DHS surveys in 27 countries, calculate unmet need as the sum of currently pregnant women who report that their pregnancy is unintended and nonpregnant currently married women who believe themselves fecund and want no more children (or none within the next 2 years), but are not currently practicing any contraceptive method. The proportions of unmet need vary greatly, from between 10 and 15 percent of women in Turkey, Colombia, and Indonesia (countries with
high contraceptive prevalence) to more than 35 percent of women in 4 of 14 sub-Saharan African countries (Westoff and Bankole, 1995).
Such estimates have taken on new importance for policy makers since they provide a way to reconcile an emphasis on reproductive rights and client needs with the aggregate goals of fertility reduction that nearly all developing countries have officially adopted. Sinding, Ross, and Rosenfield (1994) note that meeting existing unmet need would by itself fulfill for most countries their official targets for contraceptive prevalence or lowered fertility rates. In this report, we consider individual intentions as paramount in defining reproductive health: "Every birth wanted and safe" means wanted by the parents, not wanted by the state. Helping individuals achieve their reproductive goals should also result in lower fertility rates in the aggregate if desired fertility rates continue to fall in most places. This congruence provides an additional rationale for family planning programs to help women achieve their fertility goals.
Definitions of unmet need have been criticized on several grounds (Pritchett, 1994; Germain and Dixon-Mueller, 1992; Bongaarts, 1991). One is that the surveys on which they are based typically do not include sexually active nonmarried women or women currently using some method of contraception they should not be using for health reasons, using it ineffectively, or suffering needless side effects. Thus, "unmet need" as conventionally measured might be very low, despite the existence of many sexually active women who do not use contraceptives and so are at risk of unintended pregnancies and many dissatisfied users. The available survey indices also do not measure the intensity of women's preferences or why nonusers are not practicing contraception even though they do not want pregnancies. Despite the importance of these questions for scientists trying to explain and predict fertility behavior and to policy makers trying to achieve reproductive health goals, there is surprisingly little indepth research on these issues.
Casterline, Perez, and Biddlecom (1996) used a combination of survey, in-depth, and focus group interviews in the Philippines to examine the reasons for high rates of unmet need. Their findings confirm the conclusions of Bongaarts and Bruce (1995), who argue that lack of access to services and cost are relatively unimportant barriers. There was a tendency for women in the unmet need category in the Philippines study to believe themselves less likely to conceive. More important, however, were the women's perceptions of their husbands' fertility preferences (though communications among spouses were typically poor), concerns about the acceptability of contraception, and concerns about the health risks though to be possed by contraceptive methods. (Health risks were important to contraceptive users as well.) These results, which need to be replicated in other countries, tend to reinforce the view that unmet need
will not be met solely by an expansion of services. Rather, they point to a need for better counseling, informed choice, and higher quality services that will build trust and create effective demand for family planning.
Need for New Contraceptive Methods
In the early 1960s, the "contraceptive revolution, ushered in by the pill, was thought to be just beginning, and it was widely predicted that a host of new methods would soon be available—a pregnancy vaccine, a pill for men, a menses inducer and a reversible sterilant for men and women" (Lincoln and Kaeser, 1988:20). But the major advances in the last three decades have been in new ways to deliver synthetic hormonal contraceptives for women (injectable and implantable contraceptives and the Levonorgestrel intrauterine device [IUD]). A recent estimate is that it will take at least a decade for injectable hormonal contraception for men to be available in the United States, and 20 years for the availability of contraceptive vaccines for men and women (Alexander, 1995).
New versions of synthetic hormone-releasing IUDs and new plastic condoms are likely to become more widely available in the near future. The experience with contraceptive introduction in the past has shown a need for evaluation of the capabilities of the delivery system as a whole, not just use-effectiveness trials among small numbers of users. Research and development of new contraceptives are not currently receiving funding commensurate with the needs for new methods of low-cost, safe, and effective contraception and control over STD transmission (Harrison and Rosenfield, 1996).
Emergency Contraception
Emergency contraception—prevention of pregnancy through use of contraceptive methods after unprotected sex—could prove a simple and effective back-up to regular contraceptive use, and it may be particularly important for women who are victims of coercive sex. Emergency contraceptives include combinations of regular oral contraceptive pills (containing estrogen and progestin), progestin-only pills, and the copper-T IUD (Trussell, Ellertson, and Stewart, 1996; Trussell and Ellertson, 1995). Combined oral contraceptives that are available in most countries have been shown to be safe and effective for use as emergency contraceptives, with fewer and less severe side effects than older high-estrogen regimens (Trussell, Ellertson, and Stewart, 1996).
Affiliates of the International Planned Parenthood Federation provided emergency contraceptive information and services to some 40,000 women in 1993, mostly in a few developed countries (Senanayake, 1996).
The main reason that emergency contraception is not more widely used in developing countries is a lack of knowledge on the part of both health care providers and women at risk of unwanted pregnancies (International Planned Parenthood Federation, 1995). More operational research, better education of family planning caregivers, and communication to the public are all needed before emergency contraception can become a significant option for women in developing countries.
Quality Issues in Family Planning Services
The promotion of higher quality services in family planning has been pervasive in the last decade. The need for quality improvements has been revealed by studies of services in a wide variety of settings.
The framework proposed by Bruce (1990) has proved useful both for conceptualizing quality of care in assessments and as a checklist for efforts to improve quality. She found six aspects of services that clients view as critical: choice of methods, information given to clients, technical competence, interpersonal relations, mechanisms to encourage continuity of care, and an appropriate constellation of services (Bruce, 1990). We deal here with the first four of these; we do not consider continuity of care, and the appropriate constellation of services is discussed in Chapter 6.
Modern contraceptive methods are now widely available in developing countries; about one-third of married couples in developing countries outside China use some form of effective contraception (Robey, Rutstein, and Morris, 1992). But this availability does not mean that most women and men have safe access to a variety of contraceptive methods so that they can choose one appropriate to their needs at a particular time of their lives. It is difficult to measure access independent of use, but Ross and Mauldin (1996) have used the pooled judgment of experts in a large number of countries to quantify several dimensions of family planning program effort, including safe availability of multiple methods and services. Their study is one of a series of comparable studies dating back to 1972, so it is particularly useful in showing trends over time. In every region of the developing world except East Asia (where scores were already high in 1982), the safe availability of methods and services was greater in 1994 than it had been 12 years earlier. But sub-Saharan Africa still lagged well behind the rest of the world in availability of methods, and little progress had been made there, or in other parts of the developing world, in improving availability between 1989 and 1994. The rapid progress of the 1970s and 1980s in expanding choices in the developing countries appears to have stalled. At the same time that many people are calling for a "second contraceptive revolution" to better meet the needs for safe and reversible contraception and protection from STDs, large parts of the
world have not fully profited from the "first contraceptive revolution" (Harrison and Rosenfield, 1996).
Situation analyses conducted by the Population Council in family planning service delivery points in several African countries showed that counseling dealt far more often with information about resupply than with information on how to use contraceptives effectively. Clinic-based providers did not typically ask whether potential clients were breast-feeding, which should affect the choice and sequence of methods (Winikoff, Elias, and Beattie, 1994). Observations at clinics have shown a widespread tendency for providers neither to elicit information about clients' needs nor to listen carefully when it is offered. This lack greatly reduces the value of the interaction (Winikoff, Elias, and Beattie, 1994; Huntington and Schuler, 1993).
Efforts to improve quality have often been regarded by senior managers as inappropriate demands for luxury services. For decades, the ministries of health in developing countries were criticized for spending most of their resources on tertiary care of relatively high quality for urban elites while short-changing basic services for the much larger poor population. For international agencies and women's health advocates to demand greater attention to quality may seem now like a retrograde step. Yet the analogy with curative health services and the quantity-quality tradeoff could be misleading.
First, many of the problems with technical quality of care revealed by the situation analyses and similar studies could as well be seen as barriers to an adequate quantity of services: missing equipment and supplies, clinics left shut or clients turned away because poorly supervised providers do not work when they are supposed to; untrained or poorly supervised workers turning clients away (or never seeing any) because they themselves are unfamiliar with procedures. The steps that are needed to improve quality—attention to logistics, adequate supervision, motivation for workers at every level, real feedback to supervisors and managers, accountability for supplies and money—are then same that would be needed to increase service quantity. The advantage of dealing with these problems under the rubric of quality assurance is that emphasis on quality could focus the attention of managers on factors over which they have some control, rather than dissipating their attention onto the external factors for which they cannot be held accountable.
Second, the service that family planning provides is inseparable from provision of information. For resupply methods (e.g., pills), the continuous active participation of individual clients is required. High discontinuation rates are likely to indicate a poor quality program. There are always some clients who wish to conceive after spacing, or whose needs have changed, and who therefore should be discontinuing a particular
contraceptive method. But if large numbers of contraceptive users are discontinuing use of any method, rather than switching to one that better meets their needs, it probably indicates that the program is not meeting their needs (Jain and Bruce, 1994).
Lastly, the measures taken to improve quality of services provided by existing providers in existing facilities may result in great efficiency—more output for a given level of resources—than would the deployment of new workers or building of new facilities. The argument that improved quality will lead to greater demand for services and operation at more efficient scales is still largely untested. In a situation analyses of clinics and other family planning service sites in the same clusters included in the 1991-1992 DHS in Peru, Mensch, Arends-Kuenning, and Jain (1994) found that the quality of local services affected the likelihood of contraceptive use more in the rural than in the urban areas (because, the authors suggest, urban residents had access to a choice of clinics). Extreme differences in the quality index they constructed were associated with a predicted increase in contraceptive use from 33 percent to 38 percent of women; in this sample, that difference is comparable to the differences between uneducated women and women with postsecondary education (although less than the estimated effects of exposure to mass media).
Quality control in health care in most developing countries is typically achieved through routine monitoring or periodic assessments. There is a great need for simple and replicable monitoring techniques, including self-assessments and peer review. The client-oriented program evaluation devised by the Association for Voluntary Surgical Contraception is a form of self-assessment that has proved useful in several countries. Peer review has been tried with some success, for example, by midwives in Indonesia (MacDonald et al., 1995). Quality assurance should be considered primarily as a management responsibility in current programs, rather than simply as a topic for research and pilot programs. But there is a need for more operations research and dissemination of experience on replicable methods of quality improvement.
The type of programmatic linkages between family planning and other reproductive health services, especially infectious disease control and antenatal and delivery care, will vary among settings depending on such factors as whether free-standing services are already developed and patterns of utilization. Family planning programs in many countries reach large numbers of young women and thus are particularly well suited as sources of information about sources of prenatal care and emergency care for obstetric complications (see Chapter 5).
As discussed in Chapter 3, family planning programs have an important role in controlling reproductive tract infections (RTIs). At a minimum,
clinical contraceptive services, like other clinical services, should be included in measures to prevent iatrogenic infections. Both clinical and community-based programs need to incorporate into guidelines for counseling some realistic assessment, and discussion, of clients' exposure to STDs, including HIV. Latex condoms and nonoxnynol-9 reduce the risk of STD transmission as well as unwanted pregnancy. As we argue in Chapter 3, family planning clinics providing insertion of IUDs should be able to supply standardized case management of symptomatic infections (using the World Health Organization algorithms) and selected screening efforts.
Information, Education, and Communication
The diffusion of information about modern contraception throughout the world in the last three decades has been a remarkable achievement. In 13 of the 22 countries where DHS surveys were conducted in 1990-1993, more than 90 percent of women said they had heard of one or more modern contraceptive methods. In all countries except Nigeria, more than one-half of the women had heard of one or more modern methods (Curtis and Neitzel, 1996). In every country except 4 of the 11 sub-Saharan African countries, more than one-half of the women had heard of the contraceptive pill, the best-known method worldwide. These survey questions have sometimes been criticized on the grounds that respondents claim knowledge out of politeness or so as not to appear ignorant (e.g., by Bongaarts and Bruce, 1995), but even without prompting, the majority of women in all but five countries could name at least one modern contraceptive method (Curtis and Neitzel, 1996). Men are even more likely than women to know at least one contraceptive method: in 15 countries where men were interviewed in DHS surveys, more than one-half of the men reported that they had heard of at least one modern contraceptive method (Ezeh, Seroussi, and Raggers, 1996).
Of course, knowledge that an option exists is not enough. Informed choice and effective use of contraceptives require basic knowledge of how a method works, what noncontraceptive effects it might have, and how to use it. There is evidence both from standardized survey questions and from more intensive interviews and observations that many women and men do not know such things, even in countries where family planning programs are well established. For example, in the DHS in Egypt in 1992, women who reported using the contraceptive pill were asked to show their packet of pills. Interviewers inspected the packets for evidence that the pills had been taken out of sequence, and they asked the women whether they had missed days and what they would do if they did miss a day. Thirty-seven percent of the women had missed taking at least one
pill during the month preceding the interview. Only one-third of those who missed a day knew that they should take two pills on the following day or switch methods temporarily. The lack of information may well be due to inadequate services. Findings from multivariate analysis indicate that women whose source of supply was the government clinics were four times as likely as those with other sources to have taken pills out of sequence or missed days (Trottier et al., 1994).
Bongaarts and Bruce (1995) created an index of contraceptive knowledge using data from 12 DHS surveys. It shows that the percentage of women who could name a contraceptive method spontaneously, knew where to get supplies or services, and had an opinion (either positive or negative) about side effects of the method was less than 50 percent, often well below, in 6 of the 12 countries. To explore reasons for not using contraception, Bongaarts and Bruce (1995) used the DHS data, supplemented by results from intensive studies from women respondents who reported that they did not want to get pregnant but were not currently using contraception. The researchers argue that most unmet need is associated with women's lack of knowledge, concerns about health, side effects, the behavior required to use contraception, and objections from their husbands. Bongaarts and Bruce (1995:64) conclude:
As a combined consequence of poor community information levels, inadequate services, and low literacy, a large proportion of women may not be sufficiently knowledgeable about the health effects of methods to make an informed and comfortable decision about contraception. In such an environment, the impact of unknowns, unfounded rumors, or negative perceptions … will depend largely on the adequacy of the program communication strategies and client-provider exchanges.
Such results show a continuing, important role for information, education, and communication campaigns and face-to-face counseling by providers, especially where nonprogram channels of information about contraception are weak. High rates of method failure likely indicate insufficient knowledge about contraceptive use (though the fact that failure rates are higher for couples who want more children some time in the future indicates that motivation also plays a part). Concerns for health effects can be based either on an accurate appraisal of the risks and benefits of a method, in which case the availability of alternatives is particularly important, or on inaccurate information, in which case family planning programs can be considered to have failed in their most fundamental role. Improving knowledge about the side effects of contraception can make an important contribution to women's health. As Casterline, Perez, and Biddlecom (1996) show, both contraceptive users and women with unmet need (as conventionally defined) in their Philippine samples reported a great deal of worry about health effects in in-depth interviews.
Mass communication, social marketing7, and community-based distribution of contraceptive information and supplies are all strategies that have proved successful in spreading two basic messages—the existence of safe and effective contraceptive methods and the small family norm—even in countries like Bangladesh where the weight of tradition worked against them (Cleland et al., 1994; Lissance and Schellstede, 1993; Piotrow et al., 1994). Now, family planning programs face a new challenge in trying to convey subtler messages about the advantages and disadvantages of different methods and about effective use. There have been some successes in using proven strategies to convey information beyond the basic messages: for example, experiments with adapting the ''training and visit" system of agricultural extension to health and family planning in several Indian states.
Abortions
Access to Safe Abortion
In the past three decades, more than 70 countries have changed their laws to remove criminal prohibitions of abortions or to expand the scope of provisions under which abortion had previously been legalized (Cook, 1989). More than 50 percent of all women in developing countries live in countries where induced abortion is legal under most circumstances, 27 percent live in countries where abortions are legal under various medical or social criteria, and 15 percent live in countries where induced abortion is either always illegal or legal only when a woman's life is threatened if she carries the pregnancy to term. These figures are heavily affected by China and India, however: excluding these countries, the figures are 19 percent (almost always legal), 52 percent (legal under specified criteria), and 28 percent (almost always illegal) (Population Reference Bureau, 1995; Henshaw and Morrow, 1990). The current legal status of induced abortion varies widely across regions: 174 million women live in developing countries where abortion is usually illegal, most of them in Central and West Africa, South Asia apart from India, the Middle East, and South America.
The legal status of abortion is without doubt important in determining whether women have access to safe abortions, but it is not the only
determinant. In many countries where abortions are legal, large numbers of women have little access to safe services. In some countries where abortions are meant to be legal under specified criteria, there are in fact few provisions for referring women who meet those criteria to abortion providers, and abortions are treated by the health services as though they were illegal under most circumstances. Conversely, there are countries where most abortions are illegal, but where women can find clinics that provide services with relative impunity, as in Colombia.
The problems of access, interpersonal relations, and technical quality of care may well be linked for abortion and emergency treatment of the sequelae of abortion. Even legal and mandated services can be abusive and accusatory (McLaurin, Hord, and Wolf, 1990). Studies in Brazil show poor technical quality of care—the wrong intravenous fluids used and wrong decisions about procedures (Costa and Vessey, 1993). In many countries, including India, induced abortion is legal under various circumstances, but many hospitals have no provisions for referrals or for performing the procedure: For many women in many countries, the right to a safe abortion exists only de jure, not de facto.
In many developing countries, the most common technique used for abortions in hospitals is still uterine evacuation through dilatation and curettage, although the World Health Organization recommends vacuum aspiration in most cases (World Health Organization, 1986). Dilatation and curettage needlessly exposes women to risks of uterine perforation and the risks associated with general anesthesia. Manual vacuum aspiration can be safely delivered in nonhospital settings (McLaurin, Hord, and Wolf, 1990).
Abortions will likely become more common in developing countries in the next few decades. There is very little information about how the necessary medical or paramedical supervision for medical abortions can be assured in practice, and how these services would best be linked with family planning. When providers are properly trained, manual vacuum aspiration should make early abortion safer and less expensive than the dilation and curettage procedure. For both provision of abortions where legal and treatment of incomplete abortions, the equipment and training for manual vacuum aspiration should be made widely available.
Sex-Selective Abortions
Prenatal diagnostic techniques, even those using sophisticated equipment, have spread to some developing countries, so that deformed or unhealthy—or female—fetuses can be identified. There has been a good deal of speculation about the use of such techniques to identify and abort female fetuses. There are three ways of determining the sex of a fetus:
chorionic villi sampling, amnioscentesis, and ultrasound imaging. Ultrasound imaging is very unreliable before the second trimester of a pregnancy, but it is the safest and cheapest of the methods and the most widely available in Asia, so there is some concern that the number of difficult late abortions may increase as a result of increased use of ultrasound imaging. Ultrasound equipment is available in hundreds of clinics and hospitals in India, no longer confined to the large, modern cities where the problem was first described.
Much of the evidence for widespread prenatal screening followed by sex-selective abortion is indirect, based on sex ratios of reported births. In South Korea, China, and Taiwan, the ratio of male births to female births has been steadily increasing since about 1980. In China, the ratio of male births to female births increases steeply with parity, up to parity four, and this difference increased over time during the 1980s (Westley, 1995). Sex-selective abortion illustrates the problems entailed in adopting a simple policy of goal maximization of individual reproductive choice. The definitions agreed at the ICPD lead to a salutary presumption that individual choices are paramount, but they do not solve all potential disputes about exactly which services are part of "reproductive health." India, Korea, and China have all adopted measures prohibiting fetal screening for sex and sex-selective abortion, but enforcement is likely to be difficult.
The Policy Environment
Fulfilling the goal of "every child wanted" will require changes of behavior on the part of public-sector bureaucracies (national and international), private-sector service providers, and current and potential users of services. In studying family planning programs it has sometimes proven useful to classify the needed changes as supply-side or demandside factors, but the distinction between the two is artificial (Koenig and Simmons, 1992). New services are provided, or their quality and accessibility increased, or policies made more supportive, in part because political leaders and bureaucratic officials decide that these changes are beneficial for the country and conducive to their own continued rule, and in part because an educated and informed public pressures for changes. Organizations in both public and private sectors create their microenvironment, but are also creatures of the larger policy environment.
As we discuss in Chapters 6 and 7, family planning programs in developing countries are typically subsidized: contraceptive supplies, counseling, and clinical services are distributed either free of charge or at prices well below full cost recovery by government agencies and nongovernmental organizations (NGOs). Because of the large numbers of couples now entering peak ages for childbearing and the increasing reliance on
modern contraception for fertility control, the demand for subsidized services could rise rapidly.
Countries with subsidized services that face increasing demand have a limited number of options: they can devote more public funds to subsidizing family planning; they can ration services; or they can reduce the average level of subsidy per contraceptive user. The latter can be done either by making services more efficient or by mobilizing private funds, for example, through user fees. In Chapter 7 we discuss the rationale for public-sector financing and some of the experience with user fees.
Recent discussions of population policy have returned to an issue that dominated much of the debate during the early years of international assistance to family planning in developing countries: whether the provision of contraceptive supplies and information suffice or a wide range of other incentives for fertility control and disincentives for large families (measures "beyond family planning") would be required to create effective demand for contraception. In large measure, this debate was overtaken by events in the 1970s and 1980s as individual demand for contraception proved strong in most countries even without incentives and disincentives. Once fertility declines began in Asian and Latin American countries, they proceeded with such rapidity that they seemed to have their own momentum; few stalled because of a lack of continued efforts to stimulate demand (Cleland and Wilson, 1987; Knodel, Chamratrithirong, and Debavalya, 1987; for a counter example, see Hirschman, 1986).
There is little information on which to base estimates of the likely effects on fertility intentions and behavior of policies in other sectors, such as education and social policies to improve women's status. Most current proposals are based on observations of associations (e.g., of women's education and fertility) rather than evaluations of actual interventions. Increasing girls' schooling is likely to produce a range of benefits for women, their families, and society at large.
In the discussions surrounding the ICPD in 1994, the demand-side proponents were not arguing for top-down incentives and disincentives aimed solely at fertility reduction, but for measures to improve education and literacy of women and to raise women's economic and legal status more generally. The argument is that when women have more decision-making power in their households, communities, and society, they will use it in ways that promote reproductive health in the largest sense. Conversely, where women are powerless, efforts to introduce reproductive health programs as isolated interventions will not achieve much.
When the client environment is supportive, programs are effective. Programs are forced to achieve more by a demanding public, as Nag (1983) has shown with useful comparisons of South Asian health services and Caldwell (1986) has argued with historical examples concerning child
health. But there are also examples of family planning programs serving (as opposed to coercing) large numbers of women even in unpropitious circumstances, as in Bangladesh (Cleland et al., 1994). Where women are illiterate, poor, and powerless, an ability to limit fertility may be an important (though not in itself sufficient) precondition for change in their status. This argument can be made not only with examples from what are now poor countries, but with historical examples from what are now rich countries, where improvements in the legal and political status of women typically followed by decades the onset of fertility declines.
The education of girls and the improvement of the legal, economic, and political status of women have much broader effects on society than just their impact on fertility and reproductive health. But in the narrow sectoral perspective of a report on reproductive health, they might be seen as the long-term measures that would ensure the sustainability of all short-term programs targeted directly at improving reproductive health. These are complementary investments working on different time scales and through different organizations in society, rather than substitutes.
In the short run, there are several relatively low-cost ways in which policy reforms can support the goal of intended births. Kenney (1993) provides a convenient "checklist" of laws and administrative regulations that limit the availability of safe contraception: health and safety regulations that restrict the choice of methods or of providers; taxes and barriers to trade; regulation of advertising; and restrictions affecting the private sector (both commercial and nonprofit institutions).
Though it is likely that improved access and quality of family planning services would reduce high rates of abortion in many countries, even widespread and high-quality family planning services will not eliminate the demand for abortions. In practice, the effectiveness of reversible contraception is always well short of 100 percent, and coerced or simply unplanned sexual relations remain common.
It is beyond the scope of this report to assess the arguments about whether abortion is morally justified, and under what circumstances, or whether public financing and provision of abortions is justified in a society where a significant minority believe induced abortion to be immoral. But there are many countries where early abortions, in particular, are completely legal, yet unsafe abortions are common, and complications are a major health problem (World Health Organization, 1994). Even where abortions are largely or entirely illegal, medical care for complications is still provided. Thus, regardless of the legal status of induced abortion, improved care for incomplete abortions and complications must be seen as a part of reproductive health services.
TECHNICAL NOTE: Problems with Measurement of Fertility Intentions and Abortion
Much of the available evidence about fertility intentions comes from verbal reports of respondents' mental states at some time in the past or about hypothetical chances to make decisions all over again in response to standardized questions. It is imprecise, at best, to summarize intentions formed more or less unclearly and desires felt more or less intensely into simple dichotomies (wanted or unwanted; correctly timed or mistimed). Verbal reports can be inconsistent over time or with the subsequent behavior, or they may be too consistent, as when people rationalize whatever they did or come to terms with whatever happened to them by claiming that what happened is what was intended.
Estimates based on survey items like those used in the Demographic and Health Surveys (DHS) have been criticized by Pritchett (1994) and others on several grounds: preferences are unstable (though unstable individual preferences would not invalidate conclusions based on population averages; they are analogous to any type of measurement error in this respect), too hypothetical to be used as definitions of unmet need for contraception, and too much influenced by respondents' knowledge of what the interviewers would consider the "correct" answer. This last concern might diminish the usefulness of these survey items for predicting individual fertility without diminishing their usefulness for examining changes in norms or predicting fertility in a population.
Westoff (1990) has argued that data on fertility intentions are meaningful because in the aggregate they predict behavior: the proportion of women who reported in early surveys of the World Fertility Survey (WFS) or DHS that they want no more children was a good predictor of subsequent contraceptive use. However, this work tests only one of the survey items needed to construct measures of unwanted fertility. It could be that the forward-looking survey item ("Do you now want more children?") is an accurate predictor of behavior, at least in the aggregate, but the recall items ("Did you want your last pregnancy?") or explicitly hypothetical items ("If you could start over, how many children would you have?") are not valid or reliable. For example, we know of no direct attempts to validate the recall data by comparing prospective data gathered around the time of conceptions with data gathered later in pregnancies or after the outcomes. Answers to different questions in the same DHS interview can appear inconsistent, as for example, when women report that their last pregnancy was entirely unwanted (rather than mistimed) yet that they now want another child. (However, Westoff and Bankole [1995]
report that removing such women does not much change aggregate estimates of unmet need for contraception.)
For this report, we rely most on the direct measure, for two reasons: the direct items allow consideration of mistiming as well as a desire for complete cessation of childbearing; and the major objection to the direct measure of wantedness is that it produces underreporting. But if significant percentages of pregnancies appear unwanted using a measure that is probably biased then the argument that unwantedness is a big problem is strengthened.
We need to distinguish between the wantedness of conceptions and of births. It is likely that many women change their minds about the impending birth during the course of the pregnancy, either becoming reconciled to the birth or regretting an initially wanted conception. Rosenzweig and Wolpin (1993), using data from a survey in the United States for which women were interviewed by random assignment either before or after a birth, found an 8 percent decrease in wantedness after the birth, which suggests that at least in this population regret may be more common than rationalization. In an extreme case, a woman may not have intended the sexual intercourse that produced the conception, or the conception, but report as pregnancy goes on that she wants the birth, perhaps not seeing any acceptable alternative. Such an "intended birth" would not be regarded as an indicator of good reproductive health. Conversely, a change of intentions about an initially wanted pregnancy could come about because of a change in circumstances during a pregnancy—abandonment or abuse by the father, for example. It has been argued that conceptions are intended even when births are not; this may be the case, for example, in cultures where a new or potential wife's proof of fecundity is highly valued.
Data on abortions provide evidence both of the extent of unintended pregnancy and of one of its major potentially harmful consequences in developing countries. But existing data are very incomplete. Direct estimates based on household surveys produce implausibly low estimates of the prevalence of induced abortion. In the United States, for example, where most states had liberalized abortion laws even before laws against first-trimester abortions were ruled unconstitutional in 1973, confidential surveys of providers suggest that induced abortions are more than twice as common as is reported in household surveys (Jones and Forrest, 1992). There has been some recent experimentation with survey methods in both developed and developing countries, and survey researchers may have given up too easily on the prospect of measuring abortion with direct questions (see Huntington, Mensch, and Miller, 1996; Laumann et al., 1994:457). The estimates produced by the Alan Guttmacher Institute and the World Health Organization (which we use in the text) are based
on a combination of sources, including reports of abortion complications treated in hospitals and clinics which are then extrapolated to the community (see discussion in World Health Organization, 1994:5-9). The estimates, especially of clandestine abortions, should be considered approximate at best.































