
Summary
BACKGROUND AND HISTORY
This report on calcium and related nutrients1 is the first in a series of reports that presents dietary reference values for the intake of nutrients by Americans and Canadians. The overall project is a comprehensive effort undertaken by the Standing Committee on the Scientific Evaluation of Dietary Reference Intakes (DRI Committee) of the Food and Nutrition Board, Institute of Medicine, National Academy of Sciences, with the involvement of Health Canada. (See Appendix A for a description of the overall process and its origins.) This initial study was requested by the National Institute of Health' s National Heart, Lung and Blood Institute; the U.S. Food and Drug Administration; and the Agricultural Research Service of the U.S. Department of Agriculture. Additional support was received by the U. S. Army Medical Research and Materiel Command,
|
1 |
As this report was the first in the series intended to provide both quantitative recommendations for dietary reference intakes and guidance in how they should be used, changes in the prepublication version of this report have been made to increase the readability and clarity of the information provided. Improvements in format and descriptions are included in order to be consistent with the second report released in the series (DRIs for B vitamins and choline). Additionally, due to concerns raised about the statistical approach used in determining maximal calcium retention (see Appendix E), changes have been made with regard to the methodology for estimating calcium retention which were subsequently used in determining recommended intakes for calcium. See calcium discussion which follows in this summary. |
Department of Defense and the Office of Disease Prevention and Health Promotion, U.S. Department of Health and Human Services.
WHAT ARE DIETARY REFERENCE INTAKES?
Dietary Reference Intakes (DRIs) are reference values that can be used for planning and assessing diets for healthy populations and for many other purposes. The DRIs replace the periodic revisions of the Recommended Dietary Allowances (RDAs), which have been published since 1941 by the National Academy of Sciences. DRIs encompass the Estimated Average Requirement (EAR), the Recommended Dietary Allowance (RDA), the Adequate Intake (AI), and the Tolerable Upper Intake Level (UL).
As has been the practice with dietary recommendations in the past from the Food and Nutrition Board (NRC, 1980, 1989a, 1989b) and Health Canada (1990), the DRIs included in this report apply to the healthy general population. In the case of RDAs and AIs, they are nutrient levels that should decrease the risk of developing a condition related to a nutrient and associated with a negative functional outcome. Intake at the level of the RDA or AI would not necessarily be expected to replete individuals previously undernourished, nor would it be adequate for disease states marked by increased requirements. Although at times these reference intakes may serve as the basis for recommendations for these other purposes, each situation calls for adaptation by qualified professionals.
For this report, consideration of the dietary practices associated with intakes of calcium and related nutrients has been limited to observations within U.S. and Canadian populations. The recommendations for the DRIs may not be generalizable globally, especially where food intake and indigent dietary practices may result in very different bioavailability of mineral elements from sources not considered in traditional diets of Canadians and Americans.
Estimated Average2 Requirement
The Estimated Average Requirement (EAR) is the nutrient intake value that is estimated to meet the requirement defined by a specified indicator of adequacy in 50 percent of the individuals in a life stage
|
2 |
It is recognized that the definition of EAR implies a median as opposed to a mean or average. The median and average would be the same if the distribution of requirements followed a symmetrical distribution, and would diverge as a distribution became skewed. Three considerations prompted the choice of the term estimated average requirement: (1) data are rarely adequate to determine the distribution of requirements, (2) precedent has been set by other countries that have used the same term for reference values similarly derived (COMA, 1991), and (3) the impreciseness of the data evaluated makes the determination of a statistically reliable median extremely unlikely. |
and gender group. At this level of intake, the remaining 50 percent of the specified group would not meet their nutrient needs. For some life stage or gender groups, data had to be extrapolated to estimate this value. In deriving the EARs, contemporary concepts of the reduction of disease risk were among the factors considered, rather than basing reference values solely upon the prevention of nutrient deficiencies.
The EAR is expressed as a daily value averaged over time, for most nutrients at least one week. Because the EAR is a dietary intake value, it includes an adjustment for an assumed bioavailability of the nutrient. The EAR is used in setting the RDA, and it may be used as one factor for assessing the adequacy of intake of groups and for planning adequate intakes by groups.
Recommended Dietary Allowances
The Recommended Dietary Allowance (RDA) is the average daily dietary intake level that is sufficient to meet the nutrient requirements of nearly all (97 to 98 percent) individuals in a life stage and gender group. The RDA applies to individuals, not to groups. The EAR serves as the foundation for setting the RDA. If the standard deviation (SD) of the EAR is available and the requirement for the nutrient is normally distributed, the RDA is set at 2 SDs above the EAR:
RDA = EAR + 2 SDEAR.
If data about variability in requirements are insufficient to calculate a standard deviation, a coefficient of variation (CVEAR) of 10 percent is assumed in this report, and the resulting equation for the RDA is
RDA = EAR + 2 (EAR × 0.1)
RDA = EAR (1.2).
If the estimated CV is 15 percent, the formula would be
RDA = EAR (1.3).
If the nutrient requirement is known to be skewed for a population, other approaches are used to find the ninety-seventh to ninety-eighth percentile to set the RDA.
If data are insufficient for a specific life stage group to set an EAR, then no RDA will be set. An AI will be developed based on the data available (see below).
The RDA for a nutrient is a value to be used as a goal for dietary intake by healthy individuals. It is not intended to be used for assessing the diets of either individuals or groups or to plan diets for groups.
Adequate Intakes
The Adequate Intake (AI) is set instead of an RDA if sufficient scientific evidence is not available to calculate an EAR. The AI is based on observed or experimentally determined estimates of average nutrient intake by a group (or groups) of healthy people. For example, the AI for young infants, for whom human milk is the recommended sole source of food for the first 4 to 6 months, is based on the estimated daily mean nutrient intake supplied by human milk for healthy, full-term infants who are exclusively breastfed. The main intended use of the AI is as a goal for the nutrient intake of individuals. Other possible uses of the AIs will be considered by another expert group.
Tolerable Upper Intake Levels
The Tolerable Upper Intake Level (UL) is the highest level of daily nutrient intake that is likely to pose no risks of adverse health effects to almost all individuals in the general population. As intake increases above the UL, the risk of adverse effects increases. The term tolerable intake was chosen to avoid implying a possible beneficial effect. Instead, the term is intended to connote a level of intake that can, with high probability, be tolerated biologically. The UL is not intended to be a recommended level of intake. There is no established benefit for healthy individuals associated with nutrient intakes above the RDA or AI.
ULs are useful because of the increased interest in and availability of fortified foods and the increased use of dietary supplements. ULs are based on total intake of a nutrient from food, water, and supplements if adverse effects have been associated with total intake. However, if adverse effects have been associated with intake
from supplements or food fortificants only, the UL is based on nutrient intake from those sources only, not on total intake. The UL applies to chronic daily use.
For some nutrients, there may be insufficient data on which to develop a UL. This does not mean that there is no potential for adverse effects resulting from high intake. When data about adverse effects are extremely limited, extra caution may be warranted.
COMPARISON OF RECOMMENDED DIETARY ALLOWANCES AND ADEQUATE INTAKES
Although the RDA and AI are used for the same purpose—setting goals for intake by individuals—the RDA differs from the AI. Intake of the RDA for a nutrient is expected to meet the needs of 97 to 98 percent of the individuals in a life stage and gender group. If the EAR is not known, as is the case when an AI is set, it is not known what percentage of individuals are covered by the AI. The AI for a nutrient is expected to exceed the average requirement for that nutrient, and it should cover the needs of more than 98 percent of the individuals, but it might cover the needs of far fewer (see Figure S-1). The degree to which an AI exceeds the average requirement is likely to differ among nutrients and population groups.
For people with diseases that increase requirements or who have other special health needs, the RDA and AI may each serve as the basis for adjusting individual recommendations; qualified health professionals should adapt the recommended intake to cover higher or lower needs.
In this report, AIs rather than EARs and RDAs are being proposed for all nutrients for infants to age 1 year, and for calcium, vitamin D, and fluoride for all life stages. The method used to derive the AI differs for each nutrient and for infants as follows.
Infants: Ages 0 through 6 Months
The AI is the intake by healthy breastfed infants as obtained from average human milk nutrient composition and average milk volume. Since infants self-regulate milk intake from the breast, it is presumed that larger infants, who may require more milk than the average population intake, will achieve this by increasing milk intake volume.
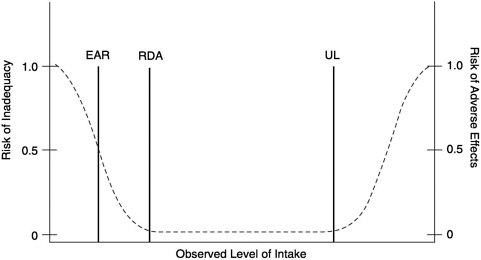
FIGURE S-1 Dietary reference intakes. This figure shows that the Estimated Average Requirement (EAR) is the intake at which the risk of inadequacy is 0.5 (50%) to an individual. The Recommended Dietary Allowance (RDA) is the intake at which the risk of inadequacy is very small—only 0.02 to 0.03 (2 to 3%). The Adequate Intake (AI) does not bear a consistent relationship to the EAR or the RDA because it is set without being able to estimate the average requirement. It is assumed that the AI is at or above the RDA if one could be calculated. At intakes between the RDA and the Tolerable Upper Intake Level (UL), the risks of inadequacy and of excess are both close to 0. At intakes above the UL, the risk of adverse effect may increase.
Calcium
In this report, three major approaches were considered in deriving the AIs for calcium—calcium balance studies of subjects consuming variable amounts of calcium, a factorial model using calcium accretion based on bone mineral accretion data, and clinical trials which investigated the response of change in bone mineral content/density or fracture rate to varying calcium intakes. The prepublication version of this report estimated per cent maximal calcium retention derived from calcium balance data as one of the three major approaches considered to develop the recommended intakes for calcium. Subsequent comments received following the report's release in prepublication form indicated concerns with the statistical methodology used to obtain such estimates from the available balance data. In response to the technical issues raised, the DRI Committee determined for this final printed version that it would estimate desirable calcium retention in place of estimating the
per cent of maximal retention, using the same data and statistical methodology as was included in the prepublication version (see Appendix E).
Where sufficient data were available, values from balance studies for individual subjects within specific age groups were applied to a nonlinear mathematical model recently used by Jackman et al. (1997) which describes the relationship between varying calcium intakes and retention. The equation derived from this model was then solved to determine the calcium intake required to achieve retention of the desirable amount of calcium. The desirable retention varied by age group but for the most part reflected accretion of calcium in bone based on bone mineral accretion data available for some of the age groups.
Another major approach considered by the DRI Committee to estimate intake needed to maintain calcium adequacy was the factorial method. This is based on combining estimates of losses of calcium via various routes by apparently healthy individuals and then assuming that these represent the degree to which calcium intake, as corrected by estimated absorption, will balance these losses. The weakness of using this approach alone is that the data come from different studies, in different subjects, and the variation in absorption, particularly depending on previous intake, may be significant. The third approach derives calcium requirements from the few available clinical trials in which additional calcium was given and changes in bone mineral content or density or in fracture rate were measured over time.
Comparison of the intakes needed to achieve desirable calcium retention or maintain minimal calcium loss using each of these three methods gave reasonable confidence and concordance to the levels of intake recommended as AIs.
The decision to set AIs rather than EARs for calcium was based on the following concerns: (1) uncertainties in the methods inherent in and the precise nutritional significance of values obtained from the balance studies that form the basis of the desirable retention model described in the previous paragraph, (2) the lack of concordance between observational and experimental data (mean calcium intakes in the United States and Canada are much lower than are the experimentally derived values required to achieve desirable calcium retention), and (3) the lack of longitudinal data that could be used to verify the association of the experimentally derived calcium intakes for achieving a pre-determining calcium retention with the rate and extent of long-term bone loss and its clinical sequelae, such as fracture. Taking all of these factors into consideration it
was determined that an EAR for calcium could not be established at the present time. The recommended AI represents an approximation of the calcium intake that, in the opinion of the DRI Committee and its Panel on Calcium and Related Nutrients, would appear to be sufficient to maintain calcium nutriture while recognizing that lower intakes may be adequate for many; however, this evaluation will have to await additional studies on calcium balance over broad ranges of intakes and/or of long-term measures of calcium sufficiency.
Vitamin D
The AI is the intake value that appears to be needed to maintain, in a defined group of individuals with limited but uncertain sun exposure and stores, serum 25-hydroxyvitamin D concentrations above a defined amount. The latter is that concentration below which vitamin D deficiency rickets or osteomalacia occurs. The intake value was rounded to the nearest 50 IU, and then doubled as a safety factor to cover the needs of all, regardless of exposure to the sun.
Fluoride
The AI is the intake value that reduces the occurrence of dental caries maximally in a group of individuals without causing unwanted side effects. With fluoride, the data are strong on risk reduction, but the evidence upon which to base an actual requirement is scant, thus driving the decision to adopt an AI as the reference value.
INDICATOR OF NUTRIENT ADEQUACY
The DRIs represent a new paradigm for the nutrition community: three of the reference values are defined by a specific indicator of nutrient adequacy, which may relate to the reduction of the risk of chronic disease or disorders; the fourth is defined by a specific indicator of excess where one is available. In the previous paradigm, the indicator of adequacy was usually limited to a classical deficiency state. Since the publication of the last revision of the Recommended Dietary Allowances in the United States (NRC, 1989a), the Canadian Recommended Nutrient Intakes (Health Canada, 1990), and the report on Diet and Health (NRC, 1989b), the research base related to the role of diet in chronic disease has expanded sufficiently to permit moving beyond deficiency indicators to other indicators with
broader significance. Examples of such indicators are those related to decreasing the risk of chronic diseases such as osteoporosis, heart disease, or hypertension. However, there is insufficient scientific evidence to relate every nutrient to chronic disease. This is the case for phosphorus and magnesium. Thus, EARs and RDAs for these two nutrients are based on traditional indicators (for example, balance studies or circulating nutrient concentrations).
For calcium, it was initially planned to estimate calcium intakes which are thought to lead to the fewest diet-related osteoporotic fractures late in life; unfortunately, the available evidence does not presently exist to establish the precise relationship. Observational data linking calcium intake to fracture risk were considered, although the role of calcium intake at any single life stage in the etiology of osteoporosis is still unclear. Moreover, the long latency period for the development of osteoporosis complicates interpretation of both the epidemiological and experimental data. Epidemiological data are of limited use until more is known about the relationships between calcium intakes by individuals and the phenotypic expression of a specific risk of osteoporosis.
The approach taken was to consider information obtained from several types of studies, that could serve as a basis for setting an AI for each age group. The information reviewed came primarily from published calcium balance studies and calcium accretion data. These data were combined with information on bone mineral content and density using the new dual-energy x-ray absorptiometry technology adding new insights into calcium needs at various stages of the lifespan.
CRITERIA FOR DIETARY REFERENCE INTAKES
The scientific data for developing DRIs were obtained from clinical trials; dose-response, balance, depletion/repletion, prospective observational, and case-control studies; and clinical observations in humans. Studies that measured actual dietary and supplement intake were given more weight than studies that depended on self-reported food and supplement intake. Studies published in peerreviewed journals were the principal source of data. The data were considered by life stage and gender to the extent possible. This allowed examination of possible physiologic differences in nutrient requirements and utilization. For some nutrients, the available data did not provide a basis for proposing different requirements for various life stage and gender groups. After careful review and analysis of the evidence, scientific judgment was used to determine what
indicator of function or other criterion would be used as the basis of the requirement in establishing the EAR, AI, or UL.
For each nutrient, the strengths and weaknesses of relevant studies were assessed. The rationale for the inclusion or exclusion of evidence is given in Chapter 4, Chapter 5, Chapter 6, Chapter 7 through Chapter 8. Where applicable, the strength, consistency, and preponderance of the data and the degree of concordance in epidemiological, clinical, and laboratory evidence influenced the selection of the indicators and the derivation of the EARs, AIs, or ULs.
USES OF DIETARY REFERENCE INTAKES
Uses of the DRIs are summarized in the following Box S–1:
For statistical reasons that will be addressed in a future report, the EAR is greatly preferred over the RDA for use in assessing the nutrient intake of groups.
International Uses of Dietary Reference Intakes
Until more is known about the prevalence of chronic disease risk and habitual nutrient intakes in other countries, the implications of these DRIs should be used with caution outside the United States and Canada. When requirements are estimated to decrease risk of disease, particularly chronic disease, associations may not be easily identified in short-term studies. Further, the AIs developed in this report may be at the upper range of intakes typically found in nationwide surveys if the criterion or outcome chosen involves chronic disease. The implication would be that it might be desirable to achieve an increase in the mean intake of the population in order to lower risk. However, the quantitative aspect is uncertain because of the approximate nature of the AI and limitations of the epidemiological and experimental data.
How to Meet Recommended Dietary Allowances or Adequate Intakes
A primary question that must be answered is “How can individuals consume the RDA or AI if surveys indicate that typical diets contain lower amounts?” This becomes a policy issue with regard to choosing methods to increase consumption of that nutrient in order to decrease the number of individuals at risk due to inadequate dietary intakes. Such methods include educating consumers to change their food consumption behavior, fortifying foodstuffs with
|
BOX S-1 Uses of Dietary Reference Intakes for Healthy Individuals and Groups
EAR = Estimated Average Requirement RDA = Recommended Dietary Allowance AI = Adequate Intake UL = Tolerable Upper Intake Level aRequires statistically valid approximation of usual intake. |
the nutrient, providing dietary supplements, or a combination of the three methods. It is not the function of this report, given the scope of work outlined, to provide an analysis of the impact of using these three methods.
Obtaining recommended intakes from unfortified foodstuffs has the advantage of providing intakes of other beneficial nutrients and
of food components for which RDAs and AIs may not be determined, and of the potential enhancement of nutrient utilization through interactions with other nutrients simultaneously. It is recognized, however, that the low energy intakes reported in recent national surveys may mean that it would be unusual to see changes in food habits to the extent necessary to maintain intakes by all individuals at levels recommended in this report. Eating fortified food products represents one method by which individuals can increase or maintain intakes without major changes in food habits. For some individuals at higher risk, use of nutrient supplements may be desirable in order to meet recommended intakes.
It is not the function of this report, given the scope of work (see Appendix A, Origin and Framework of the Development of Dietary Reference Intakes), to address in detail applications of the DRIs, including considerations necessary for the assessment of adequacy of intakes of various population groups and for planning for intakes of populations or for groups with special needs. However, some uses for the different types of DRIs are described briefly in Chapter 9. A subsequent report is expected to focus on the uses of DRIs in various settings.
CRITERIA AND PROPOSED VALUES FOR EARs, RDAs, AND AIs
Table S-1, Table S-2, Table S-3, Table S-4 through Table S-5 present the criteria used for deriving the age-group specific EARs and AIs, as well as the values for EARs, AIs, and RDAs. For vitamin D, the same criterion was used for all the life stage groups; however, for calcium, phosphorus, and magnesium, different criteria were used for some of the life stage groups. For calcium for those ages one year and older, three lines of evidence were considered as described previously, yet due to a lack of experimental evidence for ages 1 through 3 and greater than 70 years, estimates of the AI were extrapolated from other age groups.
The DRIs presented in these tables do not differ by gender except for magnesium and fluoride (because of the gender difference in average body weight). For the other nutrients, differences by gender were not apparent. For calcium, vitamin D, and fluoride, AIs have been estimated. For calcium, phosphorus, vitamin D, and fluoride, the evidence indicated that the AIs or EARs for pregnant and lactating women were no different from those for adolescents and adults of the same age. For magnesium, there was a slight increase in the EARs during pregnancy, but not during lactation.
It is important to recognize that the major focus in the develop-
ment of EARs and AIs has been the determination of the most appropriate indicator of adequacy, and then, from data available, the derivation of the EAR or AI. A key question is “adequate for what?” The value derived for the EAR, for example, would differ depending on the outcome criterion of nutrient adequacy that was judged to be the most relevant based on the scientific data available. Each EAR and AI is described in terms of the criterion(a) or outcome chosen.
CRITERIA AND PROPOSED VALUES FOR ULs
The model for deriving ULs is described in detail in Chapter 3 of the report. This is a risk assessment model that consists of a systematic series of scientific considerations and judgments to be used in deriving a UL. The hallmark of the risk assessment model is the requirement to be explicit in all the evaluations and judgments that must be made to document conclusions. Primarily due to limitations of the database, ULs are set for very broad age groups.
ULs for calcium, phosphorus, magnesium, vitamin D, and fluoride are presented in Chapter 4, Chapter 5, Chapter 6, Chapter 7 through Chapter 8 and summarized in Table S-6. These UL values have been set to protect the most sensitive individuals in the healthy general population (such as elderly individuals who tend to have a decreased glomerular filtration rate). They are likely to be too high for persons with certain illnesses (such as renal glomerular disease) or genetic abnormalities that affect the utilization or decrease the elimination of the nutrient.
RESEARCH RECOMMENDATIONS
Nutrient-specific recommendations for future research needs are provided in detail at the end of each nutrient chapter. The following major research areas are considered the highest priority in order to more accurately determine the DRIs for calcium, phosphorus, magnesium, vitamin D, and fluoride in future reports:
-
Epidemiological research that evaluates the impact of habitual (lifetime) nutrient intake on functional outcomes related to specific diseases is urgently needed in order to optimize nutrient recommendations. Examples of such research include:
-
dietary calcium, peak bone mass and fracture risk
-
dietary calcium and prostate cancer
-
dietary calcium and renal stones
-
-
exposure to fluoride from all sources with prevention of dental caries and risk of fluorosis
-
role of dietary magnesium in the development of hypertension, cardiovascular disease and diabetes.
-
Research is needed to assess methods for determining individual risk of chronic disease outcomes. For example, the potential relationship between allelic variation in the vitamin D receptor (VDR), bone mineral density, and osteoporosis within and between population groups requires further elucidation in order to determine if VDR polymorphisms are a variable influencing life-long calcium intake needs.
-
For children ages 1 through 18 years, research is needed to evaluate the dietary intakes of calcium, phosphorus, magnesium, and vitamin D required to optimize bone mineral accretion, especially in relation to changing age ranges for the onset of puberty and growth spurts.
-
With respect to dietary intake needs for vitamin D, information is required by geographical and racial variables that reflect the mix of the Canadian and United States populations and the influence of sunscreens on intake requirements.
TABLE S-1 Criteria and Dietary Reference Intake Values for Calcium by Life Stage Group
|
Life Stage Groupa |
Criterion b |
AI (mg/day) c |
|
0 through 6 months |
Human milk content |
210 |
|
7 through 12 months |
Human milk + solid food |
270 |
|
1 through 3 years |
Extrapolation of desirable calcium retention from 4 through 8 years |
500 |
|
4 through 8 years |
Calcium accretion/∆ BMC/calcium balance |
800 |
|
9 through 13 years |
Desirable calcium retention/factorial/∆ BMC |
1,300 |
|
14 through 18 years |
Desirable calcium retention/factorial/∆ BMC |
1,300 |
|
19 through 30 years |
Desirable calcium retention/factorial |
1,000 |
|
31 through 50 years |
Calcium balance |
1,000 |
|
51 through 70 years |
Desirable calcium retention/factorial/∆ BMD |
1,200 |
|
> 70 years |
Extrapolation of desirable calcium retention from 51 through 70 year age group/∆ BMD/fracture rate |
1,200 |
|
Pregnancy |
||
|
≤ 18 years |
Bone mineral mass |
1,300 |
|
19 through 50 years |
Bone mineral mass |
1,000 |
|
Lactation |
||
|
≤ 18 years |
Bone mineral mass |
1,300 |
|
19 through 50 years |
Bone mineral mass |
1,000 |
|
a All groups except Pregnancy and Lactation are males and females. b Criteria upon which the AI was based vary between life stage groups depending on the data available in the literature that were judged to be appropriate. The value for the AI reflects an approximation of the calcium intake that is judged to maintain calcium nutriture based upon all of the information examined. See Table 4-5 for a detailed summary of the specific approaches and data considered for each life stage group. ∆ BMC is the change in bone mineral content. ∆ BMD is the change in bone mineral density. c AI = Adequate Intake. The experimentally determined estimate of nutrient intake by a defined group of healthy people. AI is used if the scientific evidence is not available to derive an EAR. For healthy infants fed human milk, AI is an estimated mean intake. Some seemingly healthy individuals may require higher calcium intakes to minimize risk of osteopenia and some individuals may be at low risk on even lower intakes. The AI is believed to cover their needs, but lack of data or uncertainty in the data prevent being able to specify with confidence the percentage of individuals covered by this intake. |
||
TABLE S-2 Criteria and Dietary Reference Intake Values for Phosphorus by Life Stage Group
|
Life Stage Group a |
Criterion |
EAR (mg/day) b |
RDA (mg/day) c |
AI (mg/day) d |
|
0 through 6 months |
Human milk content |
— |
— |
100 |
|
7 through 12 months |
Human milk + solid food |
— |
— |
275 |
|
1 through 3 years |
Factorial approach |
380 |
460 |
— |
|
4 through 8 years |
Factorial approach |
405 |
500 |
— |
|
9 through 13 years |
Factorial approach |
1,055 |
1,250 |
— |
|
14 through 18 years |
Factorial approach |
1,055 |
1,250 |
— |
|
19 through 30 years |
Serum Pie |
580 |
700 |
— |
|
31 through 50 years |
Serum Pi |
580 |
700 |
— |
|
51 through 70 years |
Extrapolation of serum Pi from 19 through 50 years |
580 |
700 |
— |
|
> 70 years |
Extrapolation of serum Pi from 19 through 50 years |
580 |
700 |
— |
|
Pregnancy |
||||
|
≤ 18 years |
Factorial approach |
1,055 |
1,250 |
— |
|
19 through 50 years |
Serum Pi |
580 |
700 |
— |
|
Lactation |
||||
|
≤ 18 years |
Factorial approach |
1,055 |
1,250 |
— |
|
19 through 50 years |
Serum Pi |
580 |
700 |
— |
|
a All groups except Pregnancy and Lactation are males and females. bEAR = Estimated Average Requirement. The intake that meets the estimated nutrient needs of 50 percent of the individuals in a group. c RDA = Recommended Dietary Allowance. The intake that meets the nutrient need of almost all (97 to 98 percent) of individuals in a group. dAI = Adequate Intake. For healthy infants fed human milk, AI is the estimated mean intake. e Pi = Serum inorganic phosphate concentration. |
||||
TABLE S-3 Criteria and Dietary Reference Intake Values for Magnesium by Life Stage Group
|
EAR (mg/day) a |
RDA (mg/day) b |
AI (mg/day) c |
|||||
|
Life Stage Group |
Criterion |
Male |
Female |
Male |
Female |
Male |
Female |
|
0 through 6 months |
Human milk content |
— |
— |
— |
— |
30 |
30 |
|
7 through 12 months |
Human milk + solid food |
— |
— |
— |
— |
75 |
75 |
|
1 through 3 years |
Extrapolation of balance from older children |
65 |
65 |
80 |
80 |
||
|
4 through 8 years |
Extrapolation of balance from older children |
110 |
110 |
130 |
130 |
||
|
9 through 13 years |
Balance studies |
200 |
200 |
240 |
240 |
||
|
14 through 18 years |
Balance studies |
340 |
300 |
410 |
360 |
||
|
19 through 30 years |
Balance studies |
330 |
255 |
400 |
310 |
||
|
31 through 50 years |
Balance studies |
350 |
265 |
420 |
320 |
||
|
51 through 70 years |
Balance studies |
350 |
265 |
420 |
320 |
||
|
> 70 years |
Intracellular studies; decreases in absorption |
350 |
265 |
420 |
320 |
||
|
Pregnancy |
|||||||
|
≤ 18 years |
Gain in lean mass |
335 |
400 |
||||
|
19 through 30 years |
Gain in lean mass |
290 |
350 |
||||
|
31 through 50 years |
Gain in lean mass |
300 |
360 |
||||
|
Lactation |
|||||||
|
≤ 18 years |
Balance studies |
300 |
360 |
||||
|
19 through 30 years |
Balance studies |
255 |
310 |
||||
|
31 through 50 years |
Balance studies |
265 |
320 |
||||
|
a EAR = Estimated Average Requirement. The intake that meets the estimated nutrient needs of 50 percent of the individuals in a group. b RDA = Recommended Dietary Allowance. The intake that meets the nutrient need of almost all (97–98 percent) individuals in a group. c AI = Adequate Intake. For healthy infants fed human milk, AI is the estimated mean intake. |
|||||||
TABLE S-4 Criteria and Dietary Reference Intake Values for Vitamin D by Life Stage Group
|
Life Stage Groupa |
Criterion |
|
|
0 through 6 months |
Serum 25(OH)D |
5 |
|
7 through 12 months |
Serum 25(OH)D |
5 |
|
1 through 3 years |
Serum 25(OH)D |
5 |
|
4 through 8 years |
Serum 25(OH)D |
5 |
|
9 through 13 years |
Serum 25(OH)D |
5 |
|
14 through 18 years |
Serum 25(OH)D |
5 |
|
19 through 30 years |
Serum 25(OH)D |
5 |
|
31 through 50 years |
Serum 25(OH)D |
5 |
|
51 through 70 years |
Serum 25(OH)D |
10 |
|
> 70 years |
Serum 25(OH)D |
15 |
|
Pregnancy |
||
|
≤ 18 years |
Serum 25(OH)D |
5 |
|
19 through 50 years |
Serum 25(OH)D |
5 |
|
Lactation |
||
|
≤ 18 years |
Serum 25(OH)D |
5 |
|
19 through 50 years |
Serum 25(OH)D |
5 |
|
aAll groups except Pregnancy and Lactation are males and females. bAs cholecalciferol. 1 µg cholecalciferol = 40 IU vitamin D. cAI = Adequate Intake. The experimentally determined estimate of nutrient intake by a defined group of healthy people. AI is used if the scientific evidence is not available to derive an EAR. For healthy infants fed human milk, AI is the estimated mean intake. Some seemingly healthy individuals may require higher vitamin D intakes to minimize risk of low serum 25(OH)D levels and some individuals may be at low risk on lower dietary intakes of vitamin D. The AI is believed to cover their needs, but lack of data or uncertainty in the data prevent being able to specify with confidence the percentage of individuals covered by this intake. d In the absence of adequate exposure to sunlight. |
||
TABLE S-5 Criteria and Dietary Reference Intake Values for Fluoride by Life Stage Group
|
AI (mg/day) a |
|||
|
Life Stage Group |
Criterion |
Male |
Female |
|
0 through 6 months |
Human milk content |
0.01 |
0.01 |
|
7 through 12 months |
Caries prevention |
0.5 |
0.5 |
|
1 through 3 years |
Caries prevention |
0.7 |
0.7 |
|
4 through 8 years |
Caries prevention |
1 |
1 |
|
9 through 13 years |
Caries prevention |
2 |
2 |
|
14 through 18 years |
Caries prevention |
3 |
3 |
|
19 through 30 years |
Caries prevention |
4 |
3 |
|
31 through 50 years |
Caries prevention |
4 |
3 |
|
51 through 70 years |
Caries prevention |
4 |
3 |
|
> 70 years |
Caries prevention |
4 |
3 |
|
Pregnancy |
|||
|
≤ 18 years |
Caries prevention |
— |
3 |
|
19 through 50 years |
Caries prevention |
— |
3 |
|
Lactation |
|||
|
≤ 18 years |
Caries prevention |
— |
3 |
|
19 through 50 years |
Caries prevention |
— |
3 |
|
a AI = Adequate Intake. For healthy infants fed human milk, AI is the mean intake. The observed estimate of nutrient intake that reduces the incidence of dental caries maximally in a group of healthy people. The AI is used if the scientific evidence is not available to derive an EAR. The AI is believed to cover their needs, but lack of data or uncertainty in the data prevent being able to specify with confidence the percentage of individuals covered by this intake. |
|||
TABLE S-6 Tolerable Upper Intake Levels (ULa), by Life Stage Group
|
Life Stage Group |
Calcium (g/day) |
Phosphorus (g/day) |
Magnesium (mg/day) b |
Vitamin D (µg/day) c |
Fluoride (mg/day) |
|
0 through 6 months |
NDd |
ND |
ND |
25 |
0.7 |
|
7 through 12 months |
ND |
ND |
ND |
25 |
0.9 |
|
1 through 3 years |
2.5 |
3 |
65 |
50 |
1.3 |
|
4 through 8 years |
2.5 |
3 |
110 |
50 |
2.2 |
|
9 through 18 years |
2.5 |
4 |
350 |
50 |
10 |
|
19 through 70 years |
2.5 |
4 |
350 |
50 |
10 |
|
> 70 years |
2.5 |
3 |
350 |
50 |
10 |
|
Pregnancy |
|||||
|
≤ 18 years |
2.5 |
3.5 |
350 |
50 |
10 |
|
19 through 50 years |
2.5 |
3.5 |
350 |
50 |
10 |
|
Lactation |
|||||
|
≤ 18 years |
2.5 |
4 |
350 |
50 |
10 |
|
19 through 50 years |
2.5 |
4 |
350 |
50 |
10 |
|
a UL = the maximum level of daily nutrient intake that is likely to pose no risk of adverse effects to members of the healthy general population, Unless specified otherwise, the UL represents total intake from food, water, and supplements. b The UL for magnesium represents intake from pharmacological agents only and does not include intake from food and water. c As cholecalciferol. 1 µg cholecalciferol = 40 IU vitamin D. d ND. Not determinable due to lack of data of adverse effects in this age group and concern with regard to lack of ability to handle excess amounts. Source of intake should be from food only in order to prevent high levels of intake. |
|||||




















