
7
Resources Needed for Young Investigators
This chapter briefly examines the funding structures and levels for advanced training in addiction research in the context of more general pressures confronting young investigators. In addition, the chapter explores some special problems for clinical researchers, particularly physician scientists, and outlines some examples of nonfederal funding strategies. Recommendations directed toward a variety of agencies and foundations are made in this chapter.
Young investigators trained in the disciplines relevant to addiction research seek postdoctoral fellowships or salaried positions in universities, academic medical centers, or pharmaceutical companies. Those who seek academic careers usually apply for positions where the salary is at least partly secure, but their ability to conduct research is often dependent on research funding that has been obtained by a colleague (such as a senior researcher in charge of the postdoctoral training program) or funding that they must obtain by writing or helping to write a successful research grant application. The launching of a research career or the sustained development of a career thus depends upon the availability of fellowship programs, research grants, and other mechanisms.
The effectiveness of individual fellowships, institutional traineeships, grant-funded research assistantships, and other programs is currently under review by both the National Institutes of Health (NIH) and the National Science Foundation (NSF) (Mervis, 1996). Large national surveys, however, rarely identify trends specific to addiction research. Thus, it is useful to examine the funding streams specific to this area of research in the context of the overall funding structure for postgraduate training.
Federally supported research career paths often include efforts to obtain the National Research Service Awards (NRSA) predoctoral and postdoctoral training fellowships (e.g., T32, F31, F32), followed by career development awards (e.g., K01, K02, K08, etc.), and general research grant funding mechanisms (e.g., R29, R01, R37). These are available through NIH; two institutes, the National Institute on Drug Abuse (NIDA) and the National Institute on Alcohol Abuse and Alcoholism (NIAAA), use these awards for addiction researchers. Each program has its own set of requirements, duration of support, and funding (see Box 7.1).
|
BOX 7.1 Description of Awards F30 (Individual Predoctoral National Research Service Awards for M.D./Ph.D. Fellowships)—The fellowship provides support for both medical school and predoctoral Ph.D. training. The maximum duration is 6 years (4 years if being used to cover tuition). A stipend of $10,008 is provided to cover living expenses. F31 (Individual Predoctoral National Research Service Awards for Fellows)—The fellowship award provides up to 5 years' support for predoctoral students enrolled in a doctoral degree program. A stipend of $10,008 to cover living expenses is included. The fellowship also requires that the awardee work with an approved mentor or sponsor actively doing research in the area. F32 (Individual Postdoctoral National Research Service Awards for Fellows)—The award provides up to 3 years of aggregate support for scientists who have completed a degree with the goal of broadening their background or extending their research potential. In FY 1994, the average NIH F32 was $24,500 with the duration depending on the number of years of relevant postdoctoral experience possessed by the candidate. Awardees must pursue their research training on a full-time basis (40 hours/week) with research clinicians confining clinical duties within the training experience. Furthermore, fellows incur a service obligation of 1 month for each month of support in the first 12 months of postdoctoral NSRA support. T32 (National Research Service Award Institutional Research Training Grant)—The grant provides up to 5 years of renewable support to institutions for various levels of training, including predoctoral research training, postdoctoral research training, clinical research training, and short-term research training for health professional students. T35 (National Research Service Award Short-Term Institutional Research Training Grant)—The grant provides support to institutions offering research training opportunities to individuals or students during off-quarters or summers |
|
to continue or initiate their research experience. The positions should last longer than 2 but less than 3 months. K01 (Mentored Research Scientist Development Award)—The award provides 3 to 5 years of support for an intensive, supervised career development experience in one of the biomedical, behavioral, or clinical sciences. The program should focus on novel or highly promising multidisciplinary approaches to the problem. The applicant must identify an experienced mentor willing to provide 75 percent support for the duration of the award. K02 (Independent Scientist Award)—This award provides up to 5 years of support for newly independent scientists who can demonstrate the need for a period of intensive research focus as a means of enhancing their research careers. The applicant must have a doctoral degree and peer-reviewed, independent, research support at the time the award is made and be willing to spend at least 75 percent time on research and research career development. K05 (Senior Scientist Award)—The 5-year award provides stability of support to outstanding scientists who have demonstrated a sustained, high level of productivity and whose expertise, research accomplishments, and contributions to the field have been and will continue to be critical to the mission of the particular NIH center or institute. The candidate must have long-term support from an institute or center and peer-reviewed grant support at the time of the award. K07 (Academic Career Award)—The award is used to provide support for individuals interested in introducing or improving curriculum in a particular scientific field as a means of improving the educational or research capacity at the grantee institution. The support may be of two types: (1) leadership—a 5-year award for more senior individuals; and (2) development—a 2- to 5-year mentored award for more junior candidates. Candidates for the leadership award must be willing to devote at least 25 percent effort to the program and development candidates 75 percent time. K08 (Mentored Clinical Scientist Development Award)—The 3- to 5-year award supports the development of outstanding clinician research scientists through a period of supervised research experience that may integrate didactic studies with laboratory or clinically based research. The applicant must have a clinical degree or equivalent, have initiated postgraduate clinical training, and be willing to devote at least 75 percent effort to the program. R01 (Research Project)—Research project grants are awarded to institutions on behalf of a principal investigator to facilitate pursuit of a scientific focus objective. Institutional sponsorship assures NIH that the institution will provide facilities and be accountable for the grant funds. |
|
R03 (Small Grant)—The awards provide research support, specifically limited in time and amount, for various activities such as pilot projects, testing of new techniques, or feasibility studies of innovative, high-risk research, which would provide a basis for more extended research. R21 (Exploratory/Developmental Grant)—A small, limited time award to encourage the development of new research activities in categorical program areas. R29 (First Independent Research Support and Transition [FIRST] Award) —The award is designed to assist newly independent researchers. The award, usually for 5 years, provides an opportunity for a research scientist who has completed training to become an independent investigator. R37 (Method to Extend Research in Time [MERIT] Award)—The award provides long-term grant support to investigators whose research competence and productivity are distinctly superior and who are highly likely to continue to perform in an outstanding manner. Investigators may not apply for a MERIT award. Program staff and/or members of the cognizant National Advisory Council/Board will identify candidates for the award during review of competing research grant applications. SOURCE: NIH (1996c). |
At the committee's workshop, new investigators and senior investigators expressed their perceptions that obtaining initial research funding from NIDA and NIAAA is difficult because of the instability of these funds and the competition for them. To assess the accuracy of these perceptions, the committee examined trends in overall funding, the number of applications and awards, and application success rates for the various mechanisms. Comparative data across several institutes are shown to provide a useful context for understanding the career development issues involved in addiction research. Information is provided for NIDA, NIAAA, the National Institute of Mental Health (NIMH), the National Cancer Institute (NCI), and the National Heart, Lung, and Blood Institute (NHLBI). The latter were selected because they represent chronic and prevalent medical diseases (see Chapter 2 and Table 7.1 for a discussion of the comparative costs to society for cancer, mental disorders, and other chronic diseases).
TABLE 7.1 Total Costs to Society and NIH Training and Research Support for Specific Diseases (millions of dollars)
|
Disease |
Year |
Total Costsa to Society |
1995 Research Budget |
1995 Training Budget |
Training Budget Percent of Research Budget |
|
Drug Addictionb |
1990 |
$256,800 |
$472.1 |
$14.5 |
3.1 |
|
Cancer (all sites)c |
1990 |
96,100 |
1,215.5 |
38.6 |
3.2 |
|
Heart Diseasesc |
1991 |
125,800 |
982.6 |
48.0 |
4.9 |
|
Mental Disorders |
1990 |
147,800 |
454.2 |
30.9 |
6.8 |
|
NOTE: Research and training figures taken from budgets of related NIH institutes (i.e., drug addiction: NIDA, NIAAA; cancer: NCI; heart diseases: NHLBI; mental disorders: NIMH). 1990 is used as the base year because it is the most recent date for which the total costs to society of substance addiction and mental disorders have been estimated. For comparison, total cost estimates for cancer and heart diseases are based on the years listed closest to 1990. However, given that the cost estimates were calculated by different sources, the numbers may not be directly comparable and serve only to provide an overview of the estimated cost of each illness to society. a Includes direct and indirect costs. b Total for alcohol, illicit drugs, and nicotine (includes costs of AIDS and fetal alcohol syndrome). c Includes costs of adverse health effects of drugs, particularly nicotine. SOURCE: IOM (1995), NHLBI (1994), NIH (1996a, 1997), Rice (1995), Varmus (1995), and see Table 2.3. |
|||||
FUNDING LEVELS
Total institute budgets, research grant budgets, and training grant budgets for the past 10 years are shown in Figures 7.1 through 7.3. Although there have been increases in total budgets in actual dollars, when inflation is taken into consideration the growth has been more limited, except for NCI and NIDA.1 Since FY 1990, research grant budgets have increased between 18 percent to 30 percent, with NIDA increasing by 24 percent and NIAAA by 21 percent. Although training budgets show a different trend—in the direction of convergence for NIDA and NIAAA with the other three institutes—both NIDA's and
NIAAA's training budgets are significantly lower than the others when measured as the percentage of training dollars to total research dollars.
THE PIPELINE
Comparative data on the total numbers of applicants and awardees for training and fellowship awards (T32, F31, and F32) and for career development research awards (R29 and R01) show that there are fewer investigators at all stages of the pipeline for both NIDA and NIAAA than for the other institutes (Figures 7.4 through 7.7). In fact, between 1975 and 1992 only a small proportion (3 percent) of the National Research Service Awards (NRSA) trainees and fellows were supported by NIAAA (327 individuals) and NIDA (310 individuals). In recent years, the number of awards for traineeships and fellowships has been increasing overall for both NIDA and NIAAA, but they are still far fewer than at the other three institutes (Pion, 1996). There has been considerable growth over the past 10 years in the number of applicants for NIDA and NIAAA career development awards (R29 and R01). The number of awards doubled for NIDA, but has fluctuated rather than consistently increased for NIAAA.
Vulnerable Junctures and Lack of Research Training
Investigators at early stages of their research careers frequently progress from an extended period of postdoctoral research training support to the First Independent Research Support and Transition (FIRST) award (i.e., R29 support). This 5-year award is designed to provide an opportunity for a research scientist who has completed training to become an independent investigator. The committee learned, however, that this is a particularly vulnerable time, making attrition from the pipeline a serious problem at this juncture. Many of the young investigators at the workshop expressed concern about this difficult transition and the low prospects for receiving support. Because of the reduced number of available tenure track positions in many fields, young investigators are increasingly finding themselves in postdoctoral positions or nontenure track, semi-dependent positions for extended periods of time. There is increased concern that there are few permanent jobs available following completion of post-doctoral training fellowships. Some junior and senior investigators stated that they had chosen to leave the field, or research altogether, as a result in part of their frustration about obtaining subsequent career development awards. The vulnerability during this interval is considerable, however, for all young investigators. The delay between training fellowship and career development grant for NIAAA has increased from less than 1.4 years before FY 1990 to just less than 3 years in 1995; for NIH in general the increase has been from 1.7 to 2.4 years.
A second point of vulnerability in the pipeline is the R01 award, which is a research project grant awarded to institutions on behalf of a principal investigator. Although data demonstrate that investigators trained through the NRSA awards are more successful in obtaining subsequent career development awards (Pion, 1996), investigators at the workshop reported finding it increasingly difficult to obtain an R01 award. The data, although partially supporting their concerns in terms of overall success rates, do not support the notion that success rates for drug abuse research differ greatly from general NIH-wide success rates. In fact, NIDA success rates, but not NIAAA, averaged higher than the overall NIH rates. Success rates for funding the R01 research project grants are declining across all NIH institutes, including NIAAA. R01 success rates for NIAAA varied between 17 percent and 32 percent between FYs 1991 and 1995, compared to 25 percent to 37 percent between FYs 1986 and 1990. At NIDA, although reduced from success rates during FY 1986–1987 (36.3 percent and 43.2 percent) and FY 1989–1990 (36.3 percent and 39.8 percent), success rates for R01 awards have stabilized around 30 percent since FY 1991 (Table 7.2).
The low number of research training and research awards made by NIDA and NIAAA is in part a result of their lower total budget for research training support (Figure 7.3); also, it is partly offset by the smaller number of applicants. Increasing research training support without increasing the availability of research project grant funding creates a frustrating discontinuity; newly trained researchers are unable to find the research support needed for career success. For example, although funding for research training at NIAAA substantially increased in 1994 and 1995, the instability of research funding in terms of R01 success rates over the past 5 years has evoked caution among promising young researchers in alcohol research (Table 7.2). The committee is concerned that further decreases in funding would prevent many scientists from going into the field or fail to sustain researchers currently employed in addiction research.
The committee found that the training budgets for NIDA and NIAAA, either as a percentage of the extramural research budget or in dollars, are low compared to other NIH institutes. NIDA's $9.3 million and NIAAA's $5.2 million training budget in FY 1995 were 2.5 percent and 2.8 percent, respectively, of their extramural research funding (Tables 7.3 and 7.4). In contrast, NHLBI spent 5 percent on training grants (the NIH average is 5 percent) and the NIMH spent 7 percent. These differences were even more pronounced before the mid-1990s, when research training funds at several of the NIH institutes were substantially increased (e.g., NIDA and NCI) from earlier levels, primarily because of mandated increases, such as support for HIV/AIDS research and research training, rather than increases in the general budget.
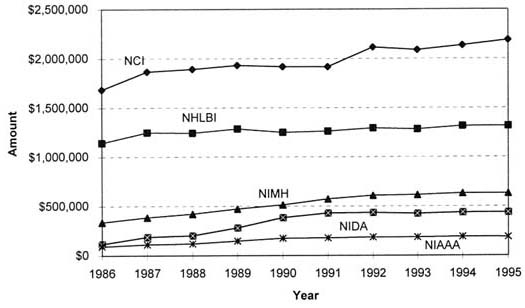
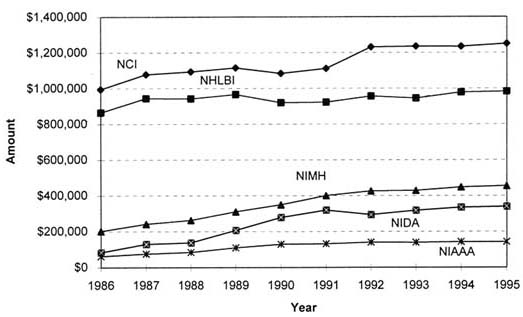
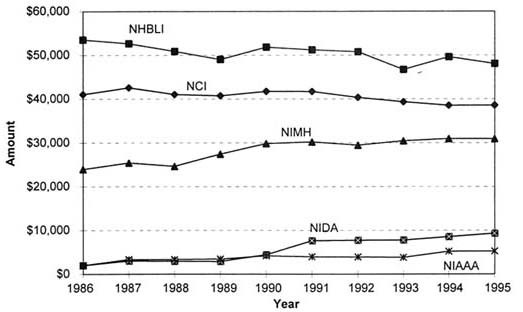
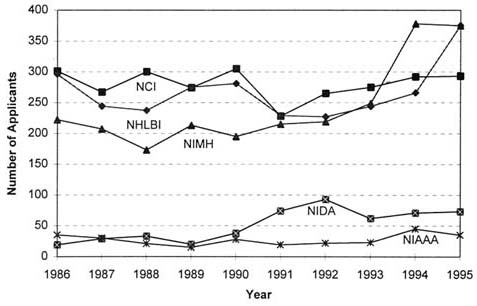
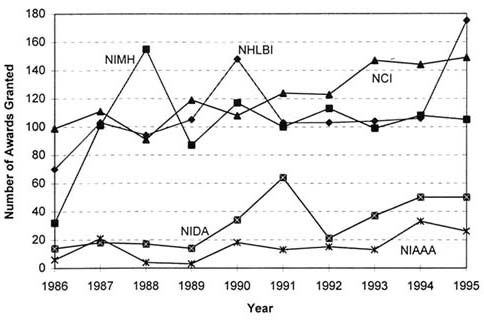
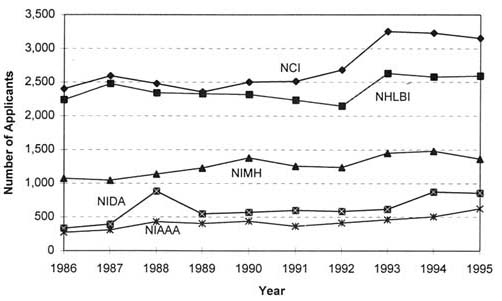
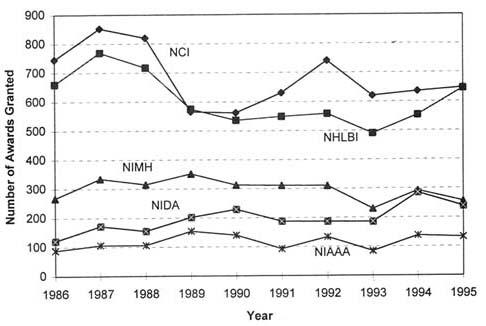
TABLE 7.2 R01 Success Rates
|
|
NIH |
NIAAA |
NIDA |
||||||
|
Fiscal Year |
Applicants (Awards) |
Average Size |
Success Rate |
Applicants (Awards) |
Average Size |
Success Rate |
Applicants (Awards) |
Average Size |
Success Rate |
|
1986 |
17,212 (5,408) |
$135,650 |
31.4% |
272 (88) |
$116,318 |
32.4% |
333 (121) |
$142,182 |
36.3% |
|
1987 |
15,825 (5,608) |
$154,816 |
35.4% |
282 (103) |
$138,262 |
36.5% |
387 (167) |
$158,216 |
43.2% |
|
1988 |
16,814 (5,170) |
$157,707 |
30.7% |
379 (94) |
$161,564 |
24.8% |
851 (145) |
$167,614 |
17.0% |
|
1989 |
17,257 (4,607) |
$173,956 |
26.7% |
369 (137) |
$161,920 |
37.1% |
523 (190) |
$181,053 |
36.3% |
|
1990 |
17,898 (4,112) |
$186,797 |
23.0% |
418 (134) |
$215,112 |
32.1% |
548 (218) |
$211,986 |
39.8% |
|
1986–1990 Total |
85,006 (24,905) |
$160,075 |
29.3% |
1,720 (556) |
$163,079 |
32.3% |
2,642 (841) |
$176,627 |
31.8% |
|
1991 |
17,203 (4,709) |
$198,123 |
27.4% |
339 (85) |
$239,024 |
25.1% |
570 (172) |
$236,878 |
30.2% |
|
1992 |
17,579 (4,769) |
$203,701 |
27.1% |
394 (124) |
$220,960 |
31.5% |
551 (167) |
$256,030 |
30.3% |
|
1993 |
19,314 (4,121) |
$205,394 |
21.3% |
436 (76) |
$211,342 |
17.4% |
584 (174) |
$256,580 |
29.8% |
|
1994 |
20,573 (4,821) |
$212,756 |
23.4% |
472 (127) |
$223,299 |
27.0% |
831 (267) |
$261,603 |
32.1% |
|
1995 |
20,100 (5,001) |
$228,508 |
24.9% |
577 (119) |
$239,303 |
20.6% |
813 (220) |
$274,486 |
27.0% |
|
1991–1995 Total |
94,769 (23,421) |
$210,038 |
24.7% |
2,218 (531) |
$227,145 |
23.9% |
3,349 (1,000) |
$258,380 |
29.9% |
|
SOURCE: OER (1996a). |
|||||||||
TABLE 7.3 NIDA Research Training Funding as a Percentage of Total Extramural Research Funding (millions of dollars)
|
|
Research Training |
Percentage of Total Extramural Research |
|||||
|
|
Individual |
Institutional |
Total |
||||
|
Year |
No. |
Amount |
No. |
Amount |
No. |
Amount |
|
|
1986 |
24 |
0.40 |
55 |
1.03 |
79 |
1.43 |
2.2 |
|
1987 |
36 |
0.67 |
78 |
1.58 |
114 |
2.25 |
2.0 |
|
1988 |
31 |
0.57 |
83 |
1.73 |
114 |
2.30 |
1.9 |
|
1989 |
34 |
0.64 |
80 |
1.73 |
174 |
2.37 |
1.5 |
|
1990 |
44 |
0.83 |
130 |
2.98 |
174 |
3.81 |
1.4 |
|
1991 |
73 |
1.26 |
203 |
5.55 |
276 |
6.81 |
2.1 |
|
1992 |
61 |
1.11 |
236 |
6.01 |
297 |
7.12 |
2.1 |
|
1993 |
65 |
1.26 |
237 |
6.11 |
302 |
7.37 |
2.2 |
|
1994 |
79 |
1.43 |
266 |
6.90 |
345 |
8.33 |
2.3 |
|
1995 |
63 |
1.67 |
291 |
7.54 |
374 |
9.31 |
2.5 |
|
SOURCE: IOM (1995), NIDA (1994, 1996), and OER (1996b). |
|||||||
TABLE 7.4 NIAAA Research Training Funding as a Percentage of Total Extramural Research Funding (millions of dollars)
|
|
Research Training |
Percentage of Total Extramural Research |
|||||
|
|
Individual |
Institutional |
Total |
||||
|
Year |
No. |
Amount |
No. |
Amount |
No. |
Amount |
|
|
1986 |
10 |
0.20 |
61 |
1.23 |
71 |
1.4 |
2.2 |
|
1987 |
10 |
0.18 |
113 |
2.32 |
123 |
2.5 |
3.0 |
|
1988 |
10 |
0.19 |
119 |
2.40 |
129 |
2.6 |
2.8 |
|
1989 |
7 |
0.14 |
113 |
2.65 |
120 |
2.8 |
2.3 |
|
1990 |
15 |
0.31 |
132 |
3.27 |
147 |
3.6 |
2.4 |
|
1991 |
23 |
0.45 |
137 |
3.10 |
160 |
3.5 |
2.2 |
|
1992 |
18 |
0.37 |
123 |
3.23 |
141 |
3.6 |
2.1 |
|
1993 |
19 |
0.39 |
130 |
3.22 |
149 |
3.6 |
2.1 |
|
1994 |
36 |
0.73 |
147 |
4.31 |
183 |
5.0 |
2.7 |
|
1995 |
45 |
0.85 |
167 |
4.39 |
212 |
5.2 |
2.8 |
|
SOURCE: NIAAA (1996) and OER (1996b). |
|||||||
Alternatives to Federal Funding
Academic researchers rely heavily on federal funding to succeed in their careers. Another route for the young investigator pursuing a career in addiction research is through industry. The opportunity to earn higher salaries, to conduct research with large budgets, and to have ready-made collaborations attracts many young researchers who have completed their graduate or postdoctoral training. A research career in industry, however, offers a different set of career incentives and institutional environments from NIH-funded research careers in academic institutions.
Foundations provide an additional, and often innovative, pathway of support for the career development of research scientists (Box 7.2). However, there are few awards to new investigators (NRC, 1994). Foundation funding of addiction research increased from $4.4 million in 1980 to $26.4 million in 1987 (The Foundation Center, 1989), although those increases have not continued.2 One exception is the Robert Wood Johnson Foundation (RWJF), which continues to support addiction research, primarily in the health services area. However, RWJF currently does not have any programs to recruit young investigators into addiction research. Several other foundations have supported addiction research in the past, but no longer do so, largely owing to stigma, lack of outcome measures, absence of a clear definition of their role, a belief that such funding is the responsibility of government, and changing priorities (The Foundation Center, 1989). Recently, a few foundations have begun to support young investigators in addiction research through seed money for new projects, funds to travel to conferences, or through initiatives that foster careers for young investigators. However, these programs benefit relatively few addiction researchers.
Competition with Senior Researchers
As in other fields, there is the perception in addiction research that funding favors more established researchers. A recent study of the National Research Council (NRC) (1994) found that success rates are dropping for grant applications
|
BOX 7.2 Foundation-Funded Research: A Model Program The ''Great Neglected Diseases of Mankind" Program was established in 1978 by the Rockefeller Foundation and focused on the development of young investigators and international collaborative research. The goal of that program was to create a network of high-quality investigators who would constitute a critical mass in the field of infectious disease. The research ranged from basic through clinical investigation and field epidemiology. Support was provided for 8 years and annual meetings were held to foster communication and collaboration. The program resulted in 14 research laboratories working on the health problems of the developing world, involved 161 scientists and clinicians and 360 trainees, and resulted in publication of 1,280 articles. The total cost to the Rockefeller Foundation was $15 million. (Lancet, 1994; Warren and Jimenez, 1988). |
submitted by younger investigators. This suggests stiffer competition with more senior researchers and lends some credence to young investigators' complaints that their research careers are constrained by "fiefdoms," where they are always in the shadow of an established senior researcher in the addiction field. However, there are no objective analyses to determine whether this field is any more, or less, driven by experienced researchers than other areas.
To meet the challenges for developing careers in addiction research, the committee recommends that:
-
The number of research career development awards should be increased, greater flexibility in duration and time-to-start of awards should be provided, and the funding priority of such awards should be advanced;
-
The use of the B/START (Behavioral Science Track Award for Rapid Transition) mechanism now at NIMH and NIDA to provide seed money for young investigators should be expanded;
-
Programs for student-directed summer research should be established by NIDA and NIAAA;
-
Industry and private foundations should cooperate with universities to provide supplemental funds for career development and research support of young investigators, especially during transition periods between awards, or to provide partial salary support for clinical researchers;
-
Increases should be made in the percentage of NIDA and NIAAA extramural research funding spend on training programs to reach the NIH institute average (currently 5 percent to 6 percent), funds for which should not be redirected from the research budgets of these institutes;
-
Jointly sponsored programs (e.g., government, industry, private foundations, academia) to support research training should be established
-
with clear roles and responsibilities for the participation of each institution; and
-
NIDA and NIAAA should explore the possibility of providing bridging support for promising young investigators to assist in the transition from K01 and R29 to R10 funding.
Special Problems for Clinical Investigators
The problem of attracting M.D.s, M.D./Ph.D.s, and Ph.D.s into a research career has been noted in other studies (IOM, 1994; IOM, 1995; NRC, 1994; Pincus et al., 1995). In drug addiction research, attracting clinical researchers and sustaining their careers is even more difficult (IOM, 1995). Although both NIDA and NIAAA have implemented efforts to use the K20 awards to attract more M.D.s and M.D./Ph.D.s into the field, very few have been awarded. NIDA increased the number of M.D./Ph.D. clinical research awards from 3 in FY 1990 to 10 in FY 1995, while NIAAA has continued to fund only 1 or 2 M.D./Ph.D. clinical researchers a year.
Level Of Stipends
As with all federally funded pre- and postdoctoral training awards, the level of the stipends poses another type of barrier for young investigators. Recent increases in stipends for NIH predoctoral researchers and junior postodoctoral researchers have brought such awards more in line with other federal and non-federal programs; stipends rose from $8,800 to $10,008 per year for predoctoral researchers, and from $19,700 to $20,700 for those with at least 1 full year of postodoctoral experience (NIH, 1992, 1996b). Despite these increases, these stipends are extremely low compared to salaries for individuals of comparable ages in other careers.
The low funding level of awards is often a particular barrier for attracting physicians who want to be clinical investigators. The maximum salary for a fourth- or fifth-year postgraduate M.D. investigator in basic research is about $30,000, while an M.D. taking a junior faculty position may earn between $70,000 to $80,000 (AAMC, 1995). Basic health insurance and other benefits are also very limited. Under the current system, payback of education-related debt must begin in the third year of postgraduate training, and most graduate and postgraduates have significant debt (AAMC, 1995).3 To alleviate the debt burden, research training is sometimes eliminated to allow earlier entry into practice, and many M.D. investigators moonlight to supplement the low salaries
of research positions (NRC, 1994). This is also a problem for Ph.D.-trained clinical researchers (IOM, 1994). These financial pressures may detract from their enthusiasm for a research career.
Competing Demands
Another barrier for many clinical researchers is trying to balance teaching, clinical, and research responsibilities. Academic departments have exerted added pressure for many investigators to increase their clinical efforts, impairing their ability to pursue research. Combined with shifts in health care funding and in support by the federal and state governments, excessively heavy clinical workloads are likely to have significant consequences for future research careers. As one young M.D./Ph.D. investigator stated, "There is always tension between the need to deliver services for my department while at the same time trying to keep my research going." Another commented on "the challenge of protecting the time for research through grant dollars that is becoming increasingly difficult due to grant funding limitations." The demands of clinical practice place enormous pressure on the clinical researcher's schedule.
To encourage excellence in clinical research on the problems of addiction, the committee recommends that:
-
The federal government should establish a debt deferral or forgiveness program for scientists conducting clinical research in drug addiction or treating persons with drug abuse in publicly funded settings; and
-
Federal funds should be made available from NIH, SAMSHA, HRSA, or AHCPR to provide training for primary care physicians (e.g., obstetricians, family physicians, and internists) to recognize, treat effectively, or refer patients with drug abuse problems.
Integration and Collaboration
In recent years, there has been increasing recognition that the behavioral sciences and neurosciences have advanced the field of addiction research and treatment (IOM, 1996). The behavioral sciences have contributed to our understanding of the complex behaviors of initiation, maintenance, cessation, and relapse to addiction, while the neurosciences have described neural mechanisms and common reward pathways responsible for addictive behaviors. That research may illuminate the underlying causes of addiction and provide theory-guided direction for the development of treatment and prevention strategies. Integration and collaboration of these research perspectives will benefit all types of research, basic and applied.
Unfortunately, integrative and collaborative research tends to be the exception rather than the standard. For example, agencies tend to be oriented toward funding research programs that are drug-or issue-specific. Requests for proposals (RFPs) and grants reflect the interests of the funding agency and are often focused on a specific problem and/or are discipline-specific. Study sections tend to be comprised of individuals knowledgeable about one discipline or field of research, and awards are granted to studies that are based on criteria that do not include or give priority to interdisciplinary research. In addition, the organization of most universities into disciplinary departments makes interdisciplinary research difficult to conduct and manage (NAS, 1995). Collaborative efforts within institutes or agencies are often impeded by proprietary concerns, conceptual differences, funding conflicts, and competition. Although those traditional mechanisms are important for funding research in any area, it would appear that in some instances a break with tradition is necessary to deal with interdisciplinary and collaborative research.
Effective and productive multidisciplinary collaboration is difficult to achieve, but is possible when there is a commitment by scientists and clinicians in the field to support collaborative efforts involving basic, clinical, and behavioral science. In light of the recent advances in the field and the importance of collaborative and integrative research efforts to address the problems of addiction and relapse, the committee recommends that:
-
Funding institutions, such as the government and private foundations, should develop program funding mechanisms (e.g., Requests for Applications [RFAs], annual conferences, symposia) to foster collaborative exchanges of information and research, such as the scientific breakthroughs that occur during drug development;
-
Universities with faculty engaged in addiction research should undertake a comprehensive review of the support and resources available for collaborative efforts within and outside the university, particularly those collaborative efforts which involve multiple disciplines; administrators should develop a plan to share resources and facilities both within and across institutions and specify criteria for access;
-
Funding agencies, such as the government and private foundations, should focus on new integrative opportunities (e.g., drug addiction etiology and medications) through using the combined strengths of participating institutions, including government, industry, private foundations, multidisciplinary centers, and Academic Centers of Excellence;
-
NIH should review the composition of Initial Review Groups (IRGs) to ensure that there is appropriate representation across necessary disciplines;
-
NIDA and NIAAA should consider establishing additional mechanisms or expanding R03 awards for individual investigator awards that support innovative, high-risk, interdisciplinary research; and
-
Additional sources of resources to increase and support integrative and collaborative efforts in addiction research should be considered by Congress; for example, the percentage of the budget of the White House Office of National Drug Control Policy earmarked for research should be increased substantially as part of coordinated strategy to make drug abuse and addiction research a national priority.
REFERENCES
AAMC (Association of American Medical Colleges). 1995. Minority Students in Medical Education: Facts and Figures IX. Washington, DC: Association of American Medical Colleges.
BLS (Bureau of Labor Statistics). 1996. Consumer Price Index: All Urban Consumers, U.S. City Average, All Items—1913–1995. Washington, DC: Bureau of Labor Statistics.
The Foundation Center. 1989. Alcohol and Drug Abuse Funding: An Analysis of Foundation Grants 1983–1987. New York: The Foundation Center.
The Foundation Center. 1995. Grants for Alcohol and Drug Abuse, 1995–1996 . New York: The Foundation Center.
The Foundation Center. 1996. Personal communication with S Qureshi. The Foundation Center. July 8.
IOM (Institute of Medicine). 1994. Careers in Clinical Research: Obstacles and Opportunities. Washington, DC: National Academy Press.
IOM. 1995. The Development of Medications for the Treatment of Opiate and Cocaine Addictions. Washington, DC: National Academy Press.
IOM. 1996. Pathways of Addiction: Opportunities in Drug Abuse Research . Washington, DC: National Academy Press.
Lancet. 1994. Proposal quality or product quality? Lancet 344:488–489.
Mervis J. 1996. NSF to take closer look at how support shapes careers. Science 272:806.
NAS (National Academy of Sciences). 1995. Allocating Federal Funds for Science and Technology. Washington, DC: National Academy Press.
NHLBI (National Heart, Lung, and Blood Institute). 1994. Morbidity and Mortality: Chartbook on Cardiovascular, Lung, and Blood Diseases . Washington, DC: National Heart, Lung, and Blood Institute.
NIAAA (National Institute on Alcoholism and Alcohol Abuse). 1996. National Institute on Alcohol Abuse and Alcoholism Funding History, 1986–1995. Rockville, MD: National Institute on Alcohol Abuse and Alcoholism.
NIDA (National Institute on Drug Abuse). 1994. National Institute on Drug Abuse 1995 Budget Estimate. Rockville, MD: National Institute on Drug Abuse.
NIDA. 1996. NIDA Research Training History, 1986–1995. Rockville, MD: National Institute on Drug Abuse.
NIH (National Institutes of Health). 1992. National research service award—Institutional grants. Request for Applications (RFA) HS-93-02. NIH Guide 21(38):October 23.
NIH. 1996a. Personal communication with Kimberly Garr. Office of Financial Management. June 4.
NIH. 1996b. NIH national research service awards for individual postdoctoral fellows guidelines. NIH Guide 25(31):September 20.
NIH. 1996c. National Institutes of Health: Grants and Contracts. [http://www.nih.gov/grants]. September.
NIH. 1997. Personal communication with Robert Feaga. Office of Financial Management. May 27.
NRC (National Research Council). 1994. The Funding of Young Investigators in the Biological and Biomedical Sciences. Washington, DC: National Academy Press.
OER (Office of Extramural Research, National Institutes of Health). 1996a. NIH Competing Research Project Applications: Number of Applicants and Awardees for Each Award by Year and Institute, 1970–1995. Prepared for the Committee to Identify Strategies to Raise the Profile of Substance Abuse and Alcoholism Research. Rockville, MD: Division of Computer Research and Technology, Office of Extramural Research, National Institutes of Health. May.
OER. 1996b. Institute and Center Research Training Budgets as a Percentage of Their Budgets for NIH Extramural Research and Development Grants, FY 1995. Rockville, MD: Office of Extramural Research, National Institutes of Health.
Pincus HA, Haviland MG, Dial TH, Hendryx MS. 1995. The relationship of postdoctoral research training to current research activities of faculty in academic departments of psychiatry. The American Journal of Psychiatry 152(4):596–601.
Pion G. 1996. Analysis of Characteristics and Outcomes for NRSA Trainees and Fellows Supported by NIAAA and NIDA. Nashville, TN: Vanderbilt University and Office of Research Training, National Institutes of Health.
Rice DP. 1995. Personal communication to the Institute of Medicine. University of California at San Francisco. February.
Varmus H. 1995. Disease-Specific Estimates of Direct and Indirect Costs of Illness and NIH Support. Bethesda, MD: Office of the Director, National Institutes of Health.
Warren KS, Jimenez C. 1988. The Great Neglected Diseases of Mankind Biomedical Research Network. New York: The Rockefeller Foundation.
























