
Summary
This report on folate, other B vitamins, and choline is one of a series that presents dietary reference values for the intake of nutrients by Americans and Canadians. The overall project is a comprehensive effort undertaken by the Standing Committee on the Scientific Evaluation of Dietary Reference Intakes (DRI Committee) of the Food and Nutrition Board, Institute of Medicine, National Academy of Sciences, with active involvement of Health Canada. (See Appendix A for a description of the overall process and its origins.) This study was requested by the U.S. Federal Steering Committee for Dietary Reference Intakes and coordinated by the U.S. Department of Health and Human Services Office of Disease Prevention and Health Promotion; with funding from the Office of Dietary Supplements, National Institutes of Health; Division of Nutrition and Physical Activity, National Center for Chronic Disease Prevention and Health Promotion, Centers for Disease Control and Prevention; the Agricultural Research Service, U.S. Department of Agriculture; and Health Canada. Additional funding was provided by contributors to the DRI Corporate Donors Fund.
Major new recommendations in this report include the following:
-
The use of dietary folate equivalents (DFEs) for estimating folate requirements, recommending daily folate intake, and assessing intake. This adjusts for the greater degree of absorption of folic acid (free form) compared with folate naturally found in foods (1 µg of food folate equals 0.6 µg of folate added to foods or taken with food or 0.5 µg of folate supplements taken on an empty stomach).
-
A Recommended Dietary Allowance (RDA) for folate that is the same for men and women; however, for women who are capable of becoming pregnant, a special recommendation is made for intake of folate from fortified food or supplements.
-
For adults over age 50, the use of food fortified with vitamin B12, or B12 supplements to meet most of the RDA for B12.
-
Recommendations for choline intake (recommendations for all the B vitamins had been made previously).
-
Suggested maximum intakes of niacin, vitamin B6, folate from supplements and fortified foods, and choline.
-
A research agenda that focuses primarily on folate and vitamin B12.
WHAT ARE DIETARY REFERENCE INTAKES?
Dietary Reference Intakes (DRIs) are reference values that are quantitative estimates of nutrient intakes to be used for planning and assessing diets for healthy people. They include RDAs but also three other types of reference values (see Box S-1). Although the reference values are based on data, the data were often scanty or drawn from studies that had limitations in addressing the question. Thus, scientific judgment was required in setting the reference values.
|
BOX S-1 Dietary Reference Intakes Recommended Dietary Allowance (RDA): the average daily dietary intake level that is sufficient to meet the nutrient requirement of nearly all (97 to 98 percent) healthy individuals in a particular life stage and gender group. Adequate Intake (AI): a recommended daily intake value based on observed or experimentally determined approximations of nutrient intake by a group (or groups) of healthy people that are assumed to be adequate—used when an RDA cannot be determined. Tolerable Upper Intake Level (UL): the highest level of daily nutrient intake that is likely to pose no risk of adverse health effects to almost all individuals in the general population. As intake increases above the UL, the risk of adverse effects increases. Estimated Average Requirement (EAR): a daily nutrient intake value that is estimated to meet the requirement of half the healthy individuals in a group. |
The reasoning used is described for each nutrient in Chapters 4 through 12.
The development of DRIs expands on the periodic reports called Recommended Dietary Allowances, which have been published since 1941 by the National Academy of Sciences. The chart on the inside back cover gives the recommended intake levels, whether RDAs or AIs, for the B vitamins and choline by life stage and gender group. Uses of DRIs appear in Box S-2. The transition from using RDAs alone to using all the DRIs appropriately will require time and effort by health professionals and others.
Recommended Dietary Allowances
The Recommended Dietary Allowance (RDA) is the average daily dietary intake level that is sufficient to meet the nutrient requirement of nearly all (97 to 98 percent) healthy individuals in a particular life stage (life stage considers age and, when applicable, pregnancy or lactation) and gender group.
Process for Setting the RDA
The process for setting the RDA depends on being able to set an Estimated Average Requirement (EAR). That is, the RDA is derived from the nutrient requirement; therefore, if an EAR cannot be set, no RDA will be set. The EAR is the daily intake value of a nutrient that is estimated to meet the nutrient requirement of half the healthy individuals in a life stage and gender group. Before setting the EAR, a specific criterion of adequacy is selected based on a careful review of the literature. When selecting the criterion, contemporary concepts of the reduction of disease risk are considered along with many other health parameters.
If the standard deviation (SD) of the EAR is available and the requirement for the nutrient is normally distributed, the RDA is set at 2 SDs above the EAR:
RDA = EAR + 2 SDEAR.
If data about variability in requirements are insufficient to calculate an SD, a coefficient of variation for the EAR of 10 percent is ordinarily assumed in this report.
The resulting equation for the RDA is then
RDA = 1.2 × EAR.
|
BOX S-2 Uses of Dietary Reference Intakes for Healthy Individuals and Groups
|
||||||||||||||||||
If the estimated coefficient of variation is 15 percent, the formula would be
RDA = 1.3 × EAR.
If the nutrient requirement is known to be skewed for a population, other approaches are used to find the ninety-seventh to ninety-eighth percentile to set the RDA.
The RDA for a nutrient is a value to be used as a goal for dietary intake by healthy individuals. As discussed in Chapter 13 of the report, the RDA is not intended to be used to assess the diets of either individuals or groups or to plan diets for groups.
Adequate Intakes
The Adequate Intake (AI) is set instead of an RDA if sufficient scientific evidence is not available for calculating an EAR. The AI is based on observed or experimentally determined estimates of nutrient intake by a group (or groups) of healthy people. For example, the AI for young infants, for whom human milk is the recommended sole source of food for the first 4 to 6 months, is based on the daily mean nutrient intake supplied by human milk for healthy, full-term infants who are exclusively breastfed. The main intended use of the AI is as a goal for the nutrient intake of individuals. Other possible uses of AIs will be considered by another expert group.
Tolerable Upper Intake Levels
The Tolerable Upper Intake Level (UL) is the highest level of daily nutrient intake that is likely to pose no risk of adverse health effects to almost all individuals in the general population. As intake increases above the UL, the risk of adverse effects increases. The term tolerable intake was chosen to avoid implying a possible beneficial effect. Instead, the term is intended to connote a level of intake that can, with high probability, be tolerated biologically. The UL is not intended to be a recommended level of intake. There is no established benefit for healthy individuals if they consume nutrient intakes above the RDA or AI.
ULs are useful because of the increased interest in and availability of fortified foods and the increased use of dietary supplements. ULs are based on total intake of a nutrient from food, water, and supplements if adverse effects have been associated with total intake. How-
ever, if adverse effects have been associated with intake from supplements or food fortificants only, the UL is based on nutrient intake from those sources only, not on total intake. The UL applies to chronic daily use.
For some nutrients, there are insufficient data on which to develop a UL. This does not mean that there is no potential for adverse effects resulting from high intake. When data about adverse effects are extremely limited, extra caution may be warranted.
COMPARISON OF RECOMMENDED DIETARY ALLOWANCES AND ADEQUATE INTAKES
Although the Recommended Dietary Allowance (RDA) and Adequate Intake (AI) are used for the same purpose—setting goals for intake by individuals—the RDA differs from the AI. Intake of the RDA for a nutrient is expected to meet the needs of 97 to 98 percent of the individuals in a life stage and gender group. If the EAR is not known, as is the case when an AI is set, it is not known what percentage of the individuals are covered by the AI. The AI for a nutrient is expected to exceed the average requirement for that nutrient, and it might even cover the needs of more than 98 percent of the individuals, but it might cover the needs of far fewer (see Figure S-1). The degree to which an AI exceeds the average requirement is likely to differ among nutrients and population groups.
For people with diseases that increase requirements or who have other special health needs, the RDA and AI may each serve as the basis for adjusting individual recommendations; qualified health professionals should adapt the recommended intake to cover higher or lower needs.
In this report, AIs rather than RDAs are being proposed for all nutrients for infants to age 1 year and for pantothenic acid, biotin, and choline for persons of all ages (see Table S-1).
APPROACH FOR SETTING DIETARY REFERENCE INTAKES
The scientific data used to develop DRIs have come from observational and experimental studies. Studies published in peer-reviewed journals were the principal source of data. Life stage and gender were considered to the extent possible, but for some nutrients the data did not provide a basis for proposing different requirements for men and women or for adults in different age groups.
Three of the categories of reference values (Estimated Average Requirement [EAR], Recommended Dietary Allowance [RDA], and
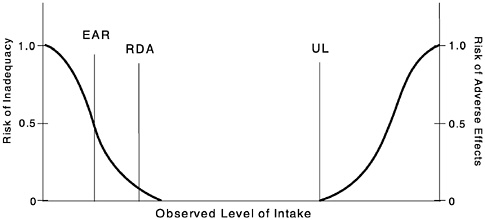
FIGURE S-1 Dietary reference intakes. This figure shows that the Estimated Average Requirement (EAR) is the intake at which the risk of inadequacy is 0.5 (50%) to an individual. The Recommended Dietary Allowance (RDA) is the intake at which the risk of inadequacy is very small—only 0.02 to 0.03 (2% to 3%). The Adequate Intake (AI) does not bear a consistent relationship to the EAR or the RDA because it is set without being able to estimate the average requirement. It is assumed that the AI is at or above the RDA if one could be calculated. At intakes between the RDA and the Tolerable Upper Intake Level (UL), the risks of inadequacy and of excess are both close to 0. At intakes above the UL, the risk of adverse effects may increase.
Adequate Intake [AI]) are defined by specific criteria of nutrient adequacy; the fourth (Tolerable Upper Intake Level [UL]) is defined by a specific indicator of excess if one is available. In all cases, data are examined closely to determine whether reduction of risk of a chronic degenerative disease or developmental abnormality could be used as a criterion of adequacy. The quality of studies was examined by considering study design; methods used for measuring intake and indicators of adequacy; and biases, interactions, and confounding factors. After careful review and analysis of the evidence, including examination of the extent of congruence of findings, scientific judgment was used to determine the basis for establishing the values. In this report, the scientific evidence was judged to be too weak to use the prevention of chronic degenerative disease as the basis for setting any of the recommended levels of intake. Thus, for the B vitamins and choline, EARs and RDAs, or AIs if applicable, are based on criteria related to their general func-
TABLE S-1 Estimated Average Requirements (EARs) and Reported Dietary Intakes of Six B Complex Vitamins by Gender for Young (19–30 years) and Older (> 70 years) Adults
|
Life Stage Group |
Thiamin (mg/d) |
Riboflavin (mg/d) |
|
Males |
|
|
|
19–30 y |
|
|
|
EAR |
1.0 |
1.1 |
|
CSFII Median Dietary Intakeb |
1.95 |
2.33 |
|
Range (5th–95th percentiles) |
1.16–3.14 |
1.32–4.00 |
|
NHANES III Median Dietary Intakec |
1.78 |
2.09 |
|
Range (5th–95th percentiles) |
1.07–3.41 |
1.18–3.90 |
|
>70y |
|
|
|
EAR |
1.0 |
1.1 |
|
CSFII Median Dietary Intake |
1.64 |
1.97 |
|
Range (5th–95th percentiles) |
0.97–2.62 |
1.09–3.30 |
|
NHANES III Median Dietary Intake |
1.56 |
1.84 |
|
Range (5th–95th percentiles) |
1.03–2.68 |
1.13–3.28 |
|
Females |
|
|
|
19–30 y |
|
|
|
EAR |
0.9 |
0.9 |
|
CSFII Median Dietary Intake |
1.22 |
1.49 |
|
Range (5th–95th percentiles) |
0.80–1.99 |
0.80–2.55 |
|
NHANES III Median Dietary Intake |
1.45 |
1.63 |
|
Range (5th–95th percentiles) |
0.94–2.49 |
0.99–2.85 |
|
>70y |
|
|
|
EAR |
0.9 |
0.9 |
|
CSFII Median Dietary Intake |
1.18 |
1.40 |
|
Range (5th–95th percentiles) |
0.68–1.86 |
0.83–2.34 |
|
NHANES III Median Dietary Intake |
1.38 |
1.60 |
|
Range (5th–95th percentiles) |
0.94–2.21 |
1.01–2.71 |
|
NOTE: The EAR can be used to assess the adequacy of nutrient intakes by groups. To do this, one determines the percentage of individuals whose usual intakes are less than the EAR. From this table it can be seen that less than 5 percent of young men have thiamin intakes less than the EAR, but more than half of young women have reported folate intakes less than the EAR. Appendixes G and H allow more accurate estimates of percentages for all age groups than does this excerpted table. a Dietary folate equivalents for the EAR but not for reported dietary intakes. Reported intakes are likely to underestimate true intakes because of limitations of the methods used to analyze the folate content of food (see Chapter 8) and because adjustment has not been made for the higher bioavailability of the folic acid consumed in fortified |
||
|
Niacin (mg/d) |
B6 (mg/d) |
Folate (µg/d)a |
B12 (µg/d) |
|
12 |
1.1 |
320 |
2.0 |
|
30.5 |
2.31 |
297 |
5.60 |
|
17.60–50.60 |
1.25–4.01 |
148–584 |
2.90–13.10 |
|
25.30 |
2.02 |
277 |
5.22 |
|
15.00–45.60 |
1.16–3.91 |
163–564 |
4.42–7.56 |
|
12 |
1.4 |
320 |
2.0 |
|
21.7 |
1.89 |
276 |
5.10 |
|
12.60–35.30 |
1.01–3.29 |
137–527 |
2.40–10.30 |
|
20.8 |
1.72 |
269 |
4.99 |
|
13.84–35.67 |
1.02–3.22 |
163–542 |
4.45–6.81 |
|
11 |
1.1 |
320 |
2.0 |
|
17.5 |
1.38 |
200 |
3.45 |
|
9.50–29.10 |
0.76–2.31 |
100–374 |
1.67–6.47 |
|
19.69 |
1.54 |
223 |
4.77 |
|
13.23–33.56 |
0.93–2.77 |
145–497 |
4.27–6.23 |
|
11 |
1.3 |
320 |
2.0 |
|
16.8 |
1.41 |
212 |
3.32 |
|
9.70–26.60 |
0.76–2.35 |
105–383 |
1.49–11.63 |
|
18.78 |
1.53 |
252 |
4.74 |
|
12.74–30.30 |
0.92–2.76 |
152–474 |
4.37–5.99 |
|
foods and supplements: 1 dietary folate equivalent = 1 µg food folate = 0.6 µg of folate from fortified food or as a supplement consumed with food = 0.5 µg of a supplement taken on an empty stomach. b SOURCE: Continuing Survey of Food Intakes by Individuals (CSFII) data on B vitamin intake from food, unpublished data, A.Carriquiry, Iowa State University, 1997. c SOURCE: Third National Health and Nutrition Examination Survey (NHANES III), 1988–1994, unpublished data on B vitamin intake from food, C.L.Johnson and J.D. Wright, National Center for Health Statistics, Centers for Disease Control and Prevention, 1997. |
|||
tions. For the B vitamins the EAR is some what higher than the amount needed to prevent deficiency disease (allowing a moderate safety margin) and there is laboratory evidence of sufficiency, but there is no observable health benefit beyond the prevention of signs and symptoms of deficiency. However, a special recommendation is included to address reduction of the risk of neural tube defects. The indicators used in deriving the RDAs and AIs are described below.
Nutrient Functions and the Indicators Used to Estimate the Requirements for the B Vitamins
Thiamin functions as a coenzyme in the metabolism of carbohydrates and branched-chain amino acids. Estimations of the requirement are based on the amount of thiamin needed to achieve and maintain normal erythrocyte transketolase activity while avoiding excessive thiamin excretion.
Riboflavin functions as a coenzyme in numerous oxidation-reduction reactions. Intake in relation to a combination of indicators is used to estimate the requirement for riboflavin. These indicators include the excretion of riboflavin and its metabolites, blood values for riboflavin, and the erythrocyte glutathione reductase activity coefficient.
Niacin functions as a cosubstrate or coenzyme with numerous dehydrogenases for the transfer of the hydride ion. The primary method used to estimate the requirement for niacin relates intake to the urinary excretion of niacin metabolites. The requirement is expressed in niacin equivalents, allowing for some conversion of the amino acid tryptophan to niacin.
Vitamin B6 functions as a coenzyme in the metabolism of amino acids, glycogen, and sphingoid bases. To estimate the requirement, many types of biochemical data were examined; however, when possible, priority was given to the amount of B6 consistent with maintenance of an adequate plasma pyridoxal phosphate concentration.
Folate functions as a coenzyme in single-carbon transfers in the metabolism of nucleic and amino acids. Folate is a generic term used to cover both the naturally occurring form of the vitamin (food folate) and the monoglutamate form (folic acid), which is used in fortified foods and supplements. To estimate the requirement the primary focus for all adults was on the amount of Dietary Folate Equivalents (DFEs) (values adjusted for differences in the absorption of food folate and folic acid) needed to maintain erythrocyte
folate, but ancillary data on plasma homocysteine and plasma folate concentrations were also considered.
Vitamin B12 functions as a coenzyme in the metabolism of fatty acids of odd-chain length and in methyl transfer. To estimate the requirement, the primary focus was on the amount of B12 needed for the maintenance of hematological status and serum B12 values.
Pantothenic acid functions as a component of coenzyme A and phosphopantetheine, which are involved in fatty acid metabolism. The AI is based on data on pantothenic acid intake sufficient to replace urinary excretion.
Biotin functions as a coenzyme in bicarbonate-dependent carboxylations. The AI is based on limited intake data.
Choline functions as a precursor for acetylcholine, phospholipids, and the methyl donor betaine. The AI is based on the intake required to maintain liver function as assessed by measuring serum alanine aminotransferase levels. Although AIs have been set for choline, there are few data to assess whether a dietary supply of choline is needed at all stages of the life cycle, and it may be that the choline requirement can be met by endogenous synthesis at some of these stages.
Consideration of the Risk of Developmental Abnormalities and Chronic Degenerative Disease
Close attention was given to evidence relating intake of B vitamins and choline to reduction of the risk of developmental disability and chronic disease. Conclusions on four of these relationships follow.
Neural Tube Defects
Because pregnancy affected by a neural tube defect (NTD) occurs in only a very small fraction of the population of women in their childbearing years, reduction of the risk of NTDs is not considered compatible with the setting of the RDA for folate. That is, by definition, the EAR would need to prevent fetal NTD in 50 percent of all women in the age group and the RDA would need to prevent it in 97 to 98 percent of the women, but NTD occurrence is already much lower than this—less than 1 percent of all pregnancies.
The RDA for folate recommended in this report for women ages 19 through 50 years (400 µg/day of dietary folate equivalents) is consistent with some recommendations for the prevention of NTDs. However, the amount and form of folate demonstrated in currently available studies to minimize NTD risk is 400 µg/day of folic acid in
addition to food folate. Therefore, the recommendation for women capable of becoming pregnant is to take 400 µg/day of folate from fortified foods and/or a supplement as well as food folate from a varied diet. It is not known whether the same level of protection could be achieved by using food that is naturally rich in folate. Neither is it known whether lower intakes would be protective or whether there is a threshold below which no protection occurs.
Vascular Disease and Thrombosis
Elevated homocysteine values have been associated with increased risk of vascular disease, and intakes of folate and vitamins B6 and B12 have been inversely related to homocysteine values. However, conflicting evidence exists and it is premature to conclude that increasing the intake of these B vitamins could reduce the risk of vascular disease and thrombosis. Randomized trials among high-risk, healthy individuals and among patients with vascular disease are expected to provide evidence useful in resolving this matter.
Cancer
Many studies have investigated relationships between folate status and carcinogenesis. The data suggesting an inverse relationship between folate status and the occurrence of colorectal cancer are stronger than for other forms of cancer (e.g., cancer of the cervix, esophagus, stomach, and lung) but are not conclusive.
Neuropsychiatric Disorders
Although available information suggests that a link may exist between folate deficiency and abnormal mental function, more than three decades of research have not produced a definitive connection. Other than for relatively rare inborn errors of metabolism, it is not known whether low folate or vitamin B6 status increases the risk of neuropsychiatric disorders or results from them. Neither is it known definitively how vitamin B12 status above that usually presumed to be adequate relates to psychiatric disturbances.
CRITERIA AND PROPOSED VALUES FOR TOLERABLE UPPER INTAKE LEVELS
A risk assessment model is used to derive the Tolerable Upper Intake Levels (ULs). The model consists of a systematic series of
scientific considerations and judgments. The hallmark of the risk assessment model is the requirement to be explicit in all the evaluations and judgments made. Primarily as a result of database limitations, ULs are set for very broad age groups.
The UL values in Table S-2 for niacin, vitamin B6, folate, and choline were set to protect the most sensitive individuals in the general population (such as those light in weight).
The ULs for folate and niacin apply to forms obtained from supplements, fortified foods, or a combination of the two. As described in Chapter 8, the UL for folate is based on examination of case studies of progression of neurological effects in vitamin B12-deficient patients taking folate supplements.
Because of lack of suitable data, ULs could not be established for infants or for thiamin, riboflavin, vitamin B12, pantothenic acid, or biotin. This signifies a need for data. It does not signify that people can tolerate chronic intakes of these vitamins at levels exceeding the Recommended Dietary Allowance (RDA) or Adequate Intake
TABLE S-2 Tolerable Upper Intake Levels (ULsa), by Life Stage Group
|
Life Stage Group |
Niacinb (mg/d) |
Vitamin B6 (mg/d) |
Folateb (µg/d) |
Choline (g/d) |
|
0 through 12 mo |
NDc |
ND |
ND |
ND |
|
1 through 3 y |
10 |
30 |
300 |
1.0 |
|
4 through 8 y |
15 |
40 |
400 |
1.0 |
|
9 through 13 y |
20 |
60 |
600 |
2.0 |
|
14 through 18 y |
30 |
80 |
800 |
3.0 |
|
≥ 19 years |
35 |
100 |
1,000 |
3.5 |
|
Pregnancy, ≤ 18 y |
30 |
80 |
800 |
3.0 |
|
Pregnancy, ≥ 19 y |
35 |
100 |
1,000 |
3.5 |
|
Lactation, ≤ 18 y |
30 |
80 |
800 |
3.0 |
|
Lactation, ≥ 19 y |
35 |
100 |
1,000 |
3.5 |
|
a UL = maximum level of daily nutrient intake that is likely to pose no risk of adverse effects. Unless otherwise specified, the UL represents total intake from food, water, and supplements. Because of the lack of suitable data, ULs could not be established for thiamin, riboflavin, vitamin B12, pantothenic acid, or biotin. In the absence of ULs, extra caution may be warranted in consuming levels above recommended intakes. b The ULs for niacin and folate apply to forms obtained from supplements, fortified foods, or a combination of the two. c ND: Not determinable because of lack of data for adverse effects in this age group and concern with regard to lack of ability to handle excess amounts. Source of intake to prevent high levels of intake should be from formula and food only. |
||||
(AI). Like all chemical agents, nutrients can produce adverse effects if intakes are excessive. Therefore, when data are extremely limited, extra caution may be warranted.
USING DIETARY REFERENCE INTAKES TO ASSESS THE NUTRIENT INTAKE OF GROUPS
For statistical reasons that will be addressed in a future report, the Estimated Average Requirement (EAR) is greatly preferred over the Recommended Dietary Allowance (RDA) for use in assessing the nutrient intake of groups. Table S-1 shows, for example, that fewer than 5 percent of young men have dietary intakes of thiamin, riboflavin, niacin, or vitamin B12 that are less than the EARs for these nutrients. This indicates that dietary intake of these five B vitamins by young men has a high probability of being sufficient to meet their needs. A large proportion of the individuals in the population, especially women, reportedly has a total folate intake less than the EAR. However, because the reported folate content of foods is considered to be substantially underestimated (in part because of methodological problems, content not being reported in dietary folate equivalents, and data being obtained before the fortification of cereal grains was required), it is not known to what extent this discrepancy between the EAR and intake represents a problem.
The determination of ways to increase dietary intake of a nutrient should include examination of the foods that are the major contributors of the nutrient to the U.S. or Canadian diet and the specific foods that are rich in the nutrient. U.S. data on both are provided in this report.
HOW TO MEET RECOMMENDED DIETARY ALLOWANCES OR ADEQUATE INTAKES
A primary question that must be answered is How can individuals consume the Recommended Dietary Allowance (RDA) or Adequate Intake (AI) if surveys indicate that typical diets contain lower amounts? This becomes a policy issue with regard to choosing methods to increase consumption of that nutrient in order to decrease the number of individuals at risk because of inadequate dietary intakes. Such methods include educating consumers to change their food consumption behavior, fortifying foodstuffs with the nutrient, providing dietary supplements, or a combination of the three methods. It is not the function of this report, given the scope of work outlined, to provide an analysis of the impact of using these three methods.
Obtaining recommended intakes from unfortified foodstuffs has the advantage of providing intakes of other beneficial nutrients and of food components for which RDAs and AIs may not be determined. Another advantage is the potential enhancement of nutrient utilization through simultaneous interactions with other nutrients. It is recognized, however, that the low energy intakes reported in recent national surveys may mean that it would be unusual to see changes in food habits to the extent necessary to maintain intakes by all individuals at levels recommended in this report. Eating fortified food products represents one method by which individuals can increase or maintain intakes without major changes in food habits. For some individuals at higher risk, use of nutrient supplements may be desirable in order to meet reference intakes.
It is not the function of this report (see Appendix A, Origin and Framework of the Development of Dietary Reference Intakes) to address in detail the applications of the DRIs, including considerations necessary for the assessment of adequacy of intakes of various population groups and for planning for intakes of populations or for groups with special needs. However, some uses for the different types of DRIs are described briefly in Chapter 13. A subsequent report is expected to focus on the uses of DRIs in various settings.
RECOMMENDATIONS
Reporting Data
Because of the difference in the bioavailability of food folate and the monoglutamate form of folate, it is recommended that both food folate and folic acid be included in tables of food composition and in reports of intake. That is, the content or intake of naturally occurring food folate should be reported separately from that of folate provided by fortified foods and supplements.
Research
Four major types of information gaps were noted: (1) a dearth of studies designed specifically to estimate average requirements; (2) a nearly complete lack of usable data on the nutrient needs of infants, children, and adolescents; (3) a lack of appropriately designed studies to determine the role of selected B vitamins and choline in reducing the risk of certain chronic diseases; and (4) a lack of studies designed to detect adverse effects of chronic high intakes of some B vitamins.
In the judgment of the DRI Committee and its panel and subcommittees, highest priority should be given to research that has potential to prevent or retard human disease processes and to prevent deficiencies with functional consequences, as follows:
-
Studies to provide the basic data for constructing risk curves and benefit curves across the exposures to food folate and folic acid. Such studies would provide estimates of the risk of developing neural tube defects, vascular disease, and neurological complications in susceptible individuals consuming different amounts of folate.
-
Investigations of the size of the effect of folate, vitamin B6, vitamin B12, and related nutrients for preventing vascular disease and of possible mechanisms for the influence of genetic variation.
-
Studies to overcome the methodological problems in the analysis of folate, including the development of sensitive and specific deficiency indicators and of practical, improved methods for analyzing the folate content of foods and determining its bioavailability.
-
Studies to develop economical, sensitive, and specific methods to assess the prevalence, causes, and consequences of vitamin B12 malabsorption and deficiency and to prevent and treat these conditions.
-
Investigation of how folate and related nutrients influence normal cellular differentiation and development, including embryogenesis and neoplastic transformation.
The requirements that appear to be the most productive to study are vitamin B12 requirements of the elderly and how they may be met; folate requirements, by trimester of pregnancy; and indicators on which to base vitamin B6 requirements.
















