
13
Uses of Dietary Reference Intakes
OVERVIEW
In the past, Recommended Dietary Allowances (RDAs) were the primary values available to health professionals for planning and assessing the diets of individuals and groups and for making judgments about excessive intake. However, the RDAs were not ideally suited for many of these purposes (IOM, 1994). The Dietary Reference Intakes (DRIs) developed in this report—RDAs, Adequate Intakes (AIs), Tolerable Upper Intake Levels (ULs), and Estimated Average Requirements (EARs) —are a more complete set of reference values. Each type of DRI has specific uses. The transition from using RDAs alone to using all the DRIs appropriately will require time and effort by health professionals and others.
The most widespread uses of DRIs—diet assessment and planning—are described briefly in this chapter. Also included are two specific applications to the nutrients discussed in this report: using dietary folate equivalents and selecting sources of vitamin B12 for the elderly.
Three of the DRIs—the RDA, AI, and EAR—are set with reference to a specific criterion of adequacy. With few exceptions the criterion of adequacy chosen for each of the B vitamins is the same for each life stage and gender group. Each nutrient chapter identifies the primary criterion that defines adequacy for the specific life stage and gender group.
|
Dietary Reference Intakes (DRIs) RDA (Recommended Dietary Allowance): the intake level that is sufficient to meet the nutrient requirement of nearly all (97 to 98 percent) healthy individuals in a group. AI (Adequate Intake): a value based on observed or experimentally determined approximations of nutrient intake by a group (or groups) of healthy people—used when an RDA cannot be determined. UL (Tolerable Upper Intake Level): the highest level of daily nutrient intake that is likely to pose no risk of adverse health effects to almost all individuals in the general population. As intake increases above the UL, the risk of adverse effects increases. EAR (Estimated Average Requirement): a nutrient intake value that is estimated to meet the requirement of half the healthy individuals in a group. NOTE: DRIs are expressed as intakes per day but they are meant to represent intakes averaged over time. |
USING RECOMMENDED DIETARY ALLOWANCES
Nutrient Recommendations for Individuals
The Recommended Dietary Allowance (RDA) is the value to be used in guiding healthy individuals to achieve adequate nutrient intake. It is a goal for average intake over time; day-to-day variation is to be expected. RDAs are set separately for specified life stage groups and sometimes they differ for males and females. The RDAs are not intended to be used for planning diets for groups or assessing the nutrient intakes of free-living groups (Beaton, 1994). Rather, the RDAs are intended to ensure the adequacy of nutrient intake. If a healthy person meets the RDA for a nutrient, there is only a very slight chance that the intake is inadequate for this person.
The RDA is expressed as a single absolute value. For example, from Chapter 6, the RDA and thus the recommended daily intake of niacin for women ages 19 through 30 years is 16 mg/day of niacin equivalents. This would be the case for a woman in this age
range weighing 50 kg (110 lb), 55 kg (121 lb), or 70 kg (154 lb) despite the differences in size and energy expenditure.
Reference weights are provided (Chapter 1, Table 1-2) to allow a calculation, when necessary, of the amount of nutrient per unit of body weight for individuals who are greatly outside the typical range of body size. These weights may also be useful for infants and children, whose average weights change substantially with age. Ordinarily, adjusting values for the nutrients included in this report based on reported energy intake has not been recommended; little justification for this practice could be found in the literature for individuals eating typical diets.
Assessing the Adequacy of Nutrient Intakes of an Individual
Although RDAs have been used to assess the adequacy of an individual’s nutrient intake in the past, this practice has serious limitations if a person’s intake is less than the RDA. An individual’s nutrient requirement is never known with certainty; only the approximate distribution of requirements for the life stage group may be known. If the individual’s intake on average meets or exceeds the RDA, there is good assurance that the intake is adequate for the specified criterion. If an individual’s average intake over time is less than the RDA, it can be inferred only that there is some increased likelihood that the intake is inadequate. The likelihood increases the further the intake falls below the RDA. For a requirement that is normally distributed, when the usual intake is less than 2 standard deviations below the Estimated Average Requirement (EAR), the likelihood that the individual’s requirement would be met would be small (NRC, 1986). A usual intake that is well below the RDA may indicate the need for further assessment of nutritional status by biochemical tests or clinical examination.
USING ADEQUATE INTAKES
As is true for the Recommended Dietary Allowance (RDA), healthy individuals with an average daily intake at or above the Adequate Intake (AI) are assumed to be at low risk of intake inadequate for a defined state of nutrition. This is its most important use. Similarly, if an individual’s average intake over time is less than the AI, it can be inferred only that there is some likelihood that the intake is inadequate. The likelihood increases the further the intake falls below the AI. Just as with the RDA, a usual intake that is well below
the AI may indicate the need for further assessment of nutritional status by biochemical tests or clinical examination.
The inherent limitations of the AI must always be taken into account in its application. The AI depends on a greater degree of judgment than is applied in estimating the Estimated Average Requirement (EAR) and subsequently deriving an RDA. Therefore, the AI provides a more imprecise basis for the planning and assessment of nutrient intakes for individuals than would an RDA. For example, when an AI is used, it is less clear at what point it would be nearly certain that the individual’s requirement would not be met. The AI might deviate significantly from the RDA if it could be determined, and might be numerically higher than the RDA would be if it were known. For this reason, AIs must be applied with greater care than is the case for RDAs.
When applying an AI to the nutrition of individuals, professionals should first assess particular risk factors and other characteristics of apparently healthy individuals that are relevant to the specific nutrient or food component. In most circumstances AIs are useful only as surrogates for RDAs for individuals. In the absence of EARs and depending on how the AIs are derived, it may be possible for an AI to be taken into account when nutritionally adequate diets are planned for populations or the diets of population groups are assessed. The extent to which AIs can be used in population planning and assessment will be addressed further in subsequent reports.
USING TOLERABLE UPPER INTAKE LEVELS
The Tolerable Upper Intake Level (UL) may be used to examine the possibility of overconsumption of a nutrient. The evaluation of true status requires clinical, biochemical, and anthropometrie data. If an individual’s usual nutrient intake remains below the UL, it is unlikely that there would be an increased risk of adverse effects from excessive intake. The risk of adverse effects increases as intakes above the UL are continued over time. However, the intake at which a given individual will develop adverse effects as a result of taking large amounts of a nutrient cannot be known with certainty. There is no established benefit for healthy individuals from consuming amounts of nutrients that exceed the Recommended Dietary Allowance (RDA) or Adequate Intake (AI).
The UL may also be used to determine the prevalence of intakes that pose a risk of adverse effects. For the B vitamins the form of the vitamin may need to be considered when intake data are examined, and this may be impossible with current survey data (see “Specific
Applications”). For example, the UL for folate applies only to folic acid, not to folate naturally found in foods, and the UL for niacin applies only to niacin in supplements, not to the niacin in food either added or found naturally or to the niacin equivalents from its precursor, tryptophan.
USING ESTIMATED AVERAGE REQUIREMENTS
Assessing the Adequacy of Nutrient Intake of Groups
The Estimated Average Requirement (EAR) (Table 13-1) may be used to estimate the prevalence of inadequate nutrient intake for a life stage group. To do so, one determines the percentage of the
TABLE 13-1 Estimated Average Requirements for B Vitamins
|
Life Stage and Gender Group |
Thiamin (mg/d) |
Riboflavin (mg/d) |
Niacin (mg/d)a |
Vitamin B6 (mg/d) |
Folate (µg/d)b |
Vitamin B12 (µg/d) |
|
Children |
||||||
|
1–3 y |
0.4 |
0.4 |
5 |
0.4 |
120 |
0.7 |
|
4–8 y |
0.5 |
0.5 |
6 |
0.5 |
160 |
1.0 |
|
Males |
||||||
|
9–13 y |
0.7 |
0.8 |
9 |
0.8 |
250 |
1.5 |
|
14–18 y |
1.0 |
1.1 |
12 |
1.1 |
330 |
2.0 |
|
19–30 y |
1.0 |
1.1 |
12 |
1.1 |
320 |
2.0 |
|
31–50 y |
1.0 |
1.1 |
12 |
1.1 |
320 |
2.0 |
|
51–70 y |
1.0 |
1.1 |
12 |
1.4 |
320 |
2.0 |
|
> 70 y |
1.0 |
1.1 |
12 |
1.4 |
320 |
2.0 |
|
Females |
||||||
|
9–13 y |
0.7 |
0.8 |
9 |
0.8 |
250 |
1.5 |
|
14–18 y |
0.9 |
0.9 |
11 |
1.0 |
330 |
2.0 |
|
19–30 y |
0.9 |
0.9 |
11 |
1.1 |
320 |
2.0 |
|
31–50 y |
0.9 |
0.9 |
11 |
1.1 |
320 |
2.0 |
|
51–70 y |
0.9 |
0.9 |
11 |
1.3 |
320 |
2.0 |
|
> 70 y |
0.9 |
0.9 |
11 |
1.3 |
320 |
2.0 |
|
Pregnancy (all ages) |
1.2 |
1.2 |
14 |
1.6 |
520 |
2.2 |
|
Lactation (all ages) |
1.2 |
1.3 |
13 |
1.7 |
450 |
2.4 |
|
NOTE: Estimated Average Requirements (EARs) have not been set for infants or for pantothenic acid, biotin, or choline. a As niacin equivalents. 1 mg of niacin = 60 mg of tryptophan. b As dietary folate equivalents. 1 dietary folate equivalent = 1 µg food folate = 0.7 µg of folate added to food or as a supplement consumed with food = 0.5 µg of folate taken as a supplement on an empty stomach. |
||||||
individuals in the group whose usual intakes are less than the EAR (Beaton, 1994) (Figure 13-1). The estimate is most accurate if the variability of intakes is at least twice as large as the variability of requirements. Before intake is compared with the EAR, methods should be used to remove the day-to-day variation in intake (Nusser et al., 1996) so that the intake data better reflect usual intakes. The adjustment narrows the intake distribution and thus gives a better estimate of the percentage of the group with intakes below the EAR (Figure 13-2).
Examples of estimating the prevalence of inadequate intake appear in Figures 13-3 and 13-4, which use adjusted data from the Third National Health and Nutrition Examination Survey. A large percentage of adults reportedly have a total folate intake less than the EAR (Figure 13-3), and this percentage is greater for women than for men. However, because the reported folate intake is considered to be substantially underestimated (partly because of methodological problems, partly because adjustment has not been made for the better bioavailability of folate in fortified cereals, and partly because these data were obtained before the fortification of cereal grains with folate was required), it is not known to what extent this
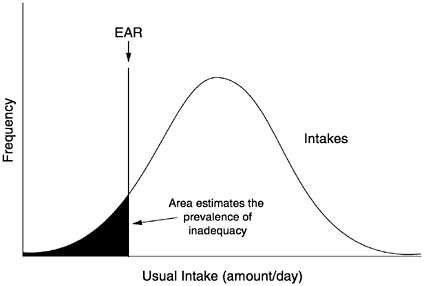
FIGURE 13-1 Estimation of the population prevalence of inadequate intakes. For this method to apply, the variance of intakes must be greater than the variance of requirements, and the requirement distribution must be symmetrical. EAR = Estimated Average Requirement.
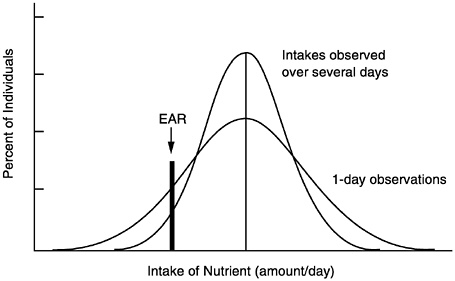
FIGURE 13-2 Effect of multiple days of observation on the apparent distribution of nutrient intake. The mean is the same for both, but the percentage of individuals with intakes less than the Estimated Average Requirement (EAR) is overestimated by the 1-day observations. Adapted from NRC (1986); originally from Hegsted (1972).
discrepancy between the EAR and intake represents a true concern. In contrast, Figure 13-4 reveals that nearly all adults have intakes of vitamin B12 that exceed the EAR. This graph does not provide any perspective on the problem of vitamin B12 absorption by many elderly, however, because the EAR assumes that adequate absorption of food-bound vitamin B12 occurs.
Overestimates of the prevalence of inadequate intakes could result from the underreporting of food intake; underestimates of the prevalence of inadequate intake are also possible. (See Chapter 2 for a discussion of many of the potential sources of error in self-reported dietary data.)
As suggested above, several questions need to be considered when assessing the intake of populations:
-
What kinds of adjustments can be made, if any, for biases in the food intake data?
-
What factors should be considered in interpreting the findings in different populations?
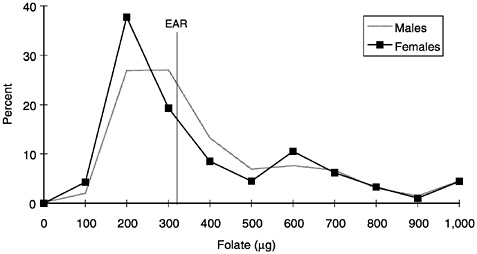
FIGURE 13-3 Distribution of reported total folate intake for men and women aged 19 years and older, Third National Health and Nutrition Examination Survey, 1988–1994. The area under each curve represents 100 percent of that population. More than 50 percent of young women have reported folate intakes (diet plus supplements) below the Estimated Average Requirement (EAR). However, these data are not adjusted for the higher bioavailability of folate as consumed in fortified foods and supplements as was done in determining the EAR. Furthermore, the reported intakes are likely to be underestimates of the actual intake because of limitations in the methods used to analyze food folate. Data have been adjusted for within-person variability using the method of Nusser et al. (1996). Folate intake values were rounded to the nearest 100 µg and all values greater than 1,000 µg were recorded as 1,000 µg. Data points are from unpublished data on percentiles of B vitamin intake from food and supplements, J.D.Wright, National Center for Health Statistics, Centers for Disease Control and Prevention, 1998.
-
At what level of intake should concern be raised for a population?
Planning Nutrient Intakes of Groups
The EAR also may be used as a basis for planning or making recommendations for the nutrient intakes of free-living groups. A group mean intake that would be associated with a low prevalence of inadequate intakes can be based on the EAR and the variance of intake. This can be done by using the same principles that were used in the estimation of the prevalence of inadequate nutrient intakes above (Figure 13-5). A detailed explanation of the method is
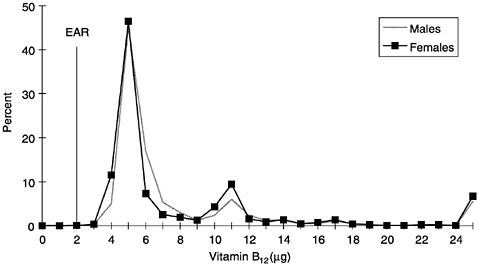
FIGURE 13-4 Distribution of reported total vitamin B12 intake for men and women aged 19 years and older, Third National Health and Nutrition Examination Survey, 1988–1994. Reported intakes of vitamin B12 (diet plus supplements) are well above the Estimated Average Requirement (EAR) for young men and women. Data were adjusted for within-person variability. Vitamin B12 intake values were rounded to the nearest 1.0 µg and all values greater than 25 µg were recorded as 25 µg. Data points are from unpublished data on percentiles of B vitamin intake from food and supplements, J.D.Wright, National Center for Health Statistics, Centers for Disease Control and Prevention, 1998.
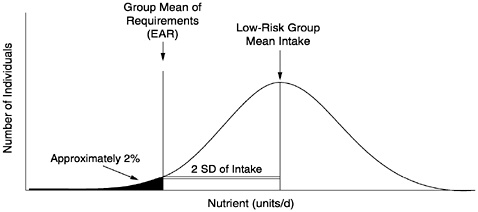
FIGURE 13-5 Derivation of a low-risk group mean intake. If the variation of intake is smaller than depicted, a lower group mean intake would also be low risk. SD = standard deviation. Adapted from WHO (1996).
presented by Beaton (1994), and an example of the application of the method is found in Trace Elements in Human Nutrition and Health (WHO, 1996).
Using the EAR in planning intakes of groups involves a number of key decisions and the analysis of questions such as the following:
-
Should actual or ideal distributions of populations intakes be used to calculate recommendations for groups? (Actual distributions are seldom normally distributed.)
-
What factors should influence the selection of the degree of risk that can be tolerated when planning for groups?
-
Do the results point to a need to take concrete steps to increase the intake of those at risk or of the entire group?
It is anticipated that methods of using the EAR for assessment and planning will be addressed in future reports.
OTHER USES OF DIETARY REFERENCE INTAKES
For many years, the Recommended Dietary Allowances in the United States and the Canadian Recommended Nutrient Intakes have been used by many national and federal agencies for a variety of purposes. For example, they have been considered in setting regulations for feeding programs, setting standards for feeding in group facilities (nursing homes, school cafeterias, and correctional facilities), developing recommended intakes for the military, and setting reference values for food labels. They have been used for comparative purposes in many computer programs for nutrient analysis and by dietitians as a basis when modifying diets of patients. Guidance for using Dietary Reference Intakes (DRIs) for many purposes will be addressed in future reports. The development of this guidance is an important component of the overall DRI project.
SPECIFIC APPLICATIONS
Dietary Folate Equivalents and Folate Sources
Diet Assessment
Individuals. Currently, nutrient databases and nutrition labels do not distinguish between sources of folate (food folate and folic acid) or express the folate content of food in dietary folate equivalents
(DFEs), which takes into account the different bioavailabilities of folate sources. DFEs and types of folate are related as follows:
|
1 µg of DFEs |
= 1.0 µg of food folate = 0.6 µg of folate added to foods (as a fortificant or folate supplement with food) = 0.5 µg of folate taken as a supplement (without food). |
|
1 µg of food folate |
= 1.0 µg of DFEs |
|
1 µg of folate added as a fortificant or as a supplement consumed with meals |
= 1.7 µg of DFEs |
|
1 µg of folate supplement taken without food |
= 2.0 µg of DFEs. |
When intakes of folate in the diet of an individual are assessed, it is possible to approximate the DFE intake by estimating the amount present added in fortification and the amount present naturally as food folate by using the relationship 1 µg of folate added as a fortificant = 1.7 µg of DFEs (the reciprocal of 1 µg of DFEs = 0.6 µg folate added to food).
The following four-step method is proposed to approximate DFEs when estimating the dietary intake of an individual:
-
Group foods into (a) fortified cereal grain foods and specially fortified foods and (b) all others.
-
If other current data are not available for cereal grains, assume the following levels of fortification (read the label of the product to determine whether folate has been added in amounts greater than the required fortification level; this primarily refers to cereals):
one slice of bread provides 20 µg of added folate;
one serving (about 1 cup) of cooked pasta provides 60 µg of added folate; and
one serving (about 1 cup) of cooked cereal or rice provides 60 µg of added folate.
Moderately fortified ready-to-eat cereals provide approximately 25 percent of the daily value per serving according to the product label, which is currently equivalent to 100 µg of added folate (25 percent of 400 µg). Highly fortified ready-to-eat cereals provide 100 percent of the daily value per serving, or 400 µg of added folate. Serving sizes of ready-to-eat cereals vary widely.
-
Combine the folate contributed by all the fortified cereal grains and multiply the result by 1.7 to obtain DFEs from folate added to foods.
-
Add DFEs from cereal grains to the folate content (in µg) from all other foods obtained from existing nutrient databases to obtain the total folate content in DFEs. For example, if the fortified cereal grains consumed were
8 slices of bread at 20 µg of added folate per slice (160 µg of total folate),
1 serving of moderately fortified ready-to-eat cereal (100 µg of folate), and
1 one-cup serving of pasta (60 µg of folate),
the total content would be 320 µg of added folate. The other foods in the diet—fruits, vegetables, meats, legumes, and milk products— provide 250 µg of food folate as determined by food composition data.
Therefore, total folate intake in DFEs = (1.7 × 320) + 250 = 794 µg of DFEs.
Populations. If dietary folate intake has been reported for groups without adjusting for DFEs and if members of the group have consumed foods fortified with folate, the amount of available folate will be higher than reported for those group members. Adjustments can be made only at the individual level, not at the group level.
Recommendation
Because of the difference in the bioavailability of food folate and folate added to foods or taken as supplements, it is recommended that both food folate and added folate be included in tables of food composition and in reports of intake. In other words, the content or intake of naturally occurring food folate should be reported separately from that of added folate in fortified foods and supplements. This allows the computation of DFEs for the assessment of intake and for diet planning, the computation of added folate intake for comparison with the Tolerable Upper Intake Level (UL), and analysis of the relative contributions of the two forms to total intake.
Diet Planning for Individuals
As can be inferred from the example above, individuals who wish
to increase their folate consumption to the Recommended Dietary Allowance (RDA) level (400 µg/day of DFEs) could readily do so by consuming fortified cereal grains. They could also increase intake of foods that are naturally high in folate, such as orange juice and cooked dried peas and beans, eat more foods that are good sources of folate, and eat fewer foods that contain none (such as soft drinks and most candy). For women capable of becoming pregnant, taking 400 µg/day of folate from fortified food, supplements, or a combination of the two is recommended to reduce the risk of neural tube defects.
One combination of fortified foods that would provide 400 µg of added folate is
2 servings of moderately fortified ready-to-eat cereal (200 µg of folate),
7 slices of bread or alternate (140 µg of folate), and
1 cup of rice or pasta (60 µg of added folate).
According to the serving sizes specified in the Food Guide Pyramid (USDA, 1992), this would be 11 servings of cereal grains— much more than that consumed by many women. It is the upper limit of the recommendation to consume 6 to 11 servings made in the Food Guide Pyramid.
Obtaining Synthetic Vitamin B12from Food
It is recommended that adults over age 50 obtain their vitamin B12 mainly as synthetic B12 from fortified foods or supplements because absorption of food-bound B12 may be limited (see Chapter 9). The main food sources of synthetic vitamin B12 are fortified ready-to-eat cereals and soy-based meat substitutes (see Table 9-10). If these foods provide 25 percent of the current daily value designated on the product label, they provide 1.5 µg of synthetic B12 (more than half the RDA for B12 for older adults of 2.4 µg/day).
SUMMARY
Each reference value should be used for its intended purpose. The Recommended Dietary Allowance (RDA) and the Adequate Intake (AI) are intended for use primarily as goals for intake by individuals. Special attention to the form of folate and vitamin B12 is often warranted.
REFERENCES
Beaton GH. 1994. Criteria of an adequate diet. In: Shils ME, Olson JA, Shike M, eds. Modern Nutrition in Health and Disease, 8th ed. Philadelphia: Lea & Febiger. Pp. 1491–1505.
Hegsted DM. 1972. Problems in the use and interpretation of the Recommended Dietary Allowances. Ecol Food Nutr 1:255–265.
IOM (Institute of Medicine). 1994. How Should the Recommended Dietary Allowances Be Revised? Washington, DC: National Academy Press.
NRC (National Research Council). 1986. Nutrient Adequacy. Assessment Using Food Consumption Surveys. Washington, DC: National Academy Press.
Nusser SM, Carriquiry AL, Dodd KW, Fuller WA. 1996. A semiparametric transformation approach to estimating usual daily intake distributions. J Am Stat Assoc 91:1440–1449.
USDA (U.S. Department of Agriculture). 1992. The Food Guide Pyramid. Home and Garden Bulletin Number 252. Washington, DC: US Government Printing Office.
WHO (World Health Organization). 1996. Trace Elements in Human Nutrition and Health. Prepared in collaboration with the Food and Agriculture Organization of the United Nations and the International Atomic Energy Agency. Geneva: WHO.














