
(DHHS), are intended to encourage the design of summary measures that are readily understood and helpful and to promote use of these measures in ways that are accountable and credible. The committee recommends that DHHS do the following:
-
Initiate a process of analysis and public discussion to (a) clarify the ethical assumptions and value judgments embedded in different measures of population health and (b) assess the critical ethical and policy implications of differing designs, implementation approaches, and uses of these measures.
-
Create a process to establish standards for population health metrics and to investigate the value and practicality of a compatible set of summary measures of population health that could be used for different descriptive and decisionmaking purposes.
-
Invest in the education and training of public health and medical professionals to promote their understanding of the interpretation and appropriate use of summary measures of population health.
BACKGROUND
Origin of the Report
This brief report is the product of a short-term IOM project that was funded by DHHS to provide guidance on future directions for the development and application of summary measures. To meet this charge and prepare this report, the IOM established a seven-member committee of experts in public health, ethics, policy analysis, and measurement development and use.
At the request of DHHS, the committee, which was appointed in September 1997, convened a workshop that would bring together a carefully balanced group of methodologists, ethicists, and policymakers to discuss the design and use of summary measures of population health and to provide guidance on steps that would strengthen the credibility and utility of the measures. The December 1997 workshop included one day of presentations from national and international experts and a second day devoted to small-group discussion of issues and directions. The workshop agenda, list of participants, and background papers prepared for the workshop are included here as appendixes.
The IOM committee met immediately following the workshop to consider its conclusions and recommendations and to outline a short report. In addition to the committee’s own expertise and perspectives, the report draws on the workshop presentations and small-group discussion as well as on the background papers drafted for the workshop by Marthe Gold, Dennis Fryback, Norman Daniels, and Daniel Brock. The focus is on the United States, but the committee benefited from the international expertise and experience represented by participants from Canada, the Netherlands, the United Kingdom, Mexico, and the Organization for Economic Cooperation and Development as well as others who advise international groups such as the World Health Organization and the World Bank.
Terminology
One problem facing the committee was that the nomenclature for concepts and measures of population health derives from a number of literature streams, and the committee found itself at a confluence of these streams, where the same names were being applied to quite different things. For purposes of this report, a measure of population health can involve mortality data (e.g., age-adjusted mortality rates for a given year, life expectancy at birth or age 65) or morbidity data (e.g., disability rates or quality of life indices) or both. The focus of the report is on summary measures of population health that combine both mortality and morbidity data to represent overall population health in a single number (e.g., a health-adjusted life year or health-adjusted life expectancy).
Figure 1 depicts how mortality and morbidity measures—as partial measures of population health—combine to form an integrative measure. The background paper by Fryback describes the process in more detail.
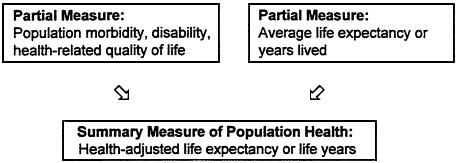
FIGURE 1 Building a summary measure from partial measures of health.
Because measures of health-related quality of life (HRQL) are important building blocks of these integrated measures and generate much of the controversy about these measures, such measures are also considered in this report and the background papers. To depict an individual’s overall health at a particular time, these measures generate a single number on a scale anchored by 0 (state of being dead) and 1 (state of optimal health) that represents the degree or strength of preferences for one health state over another. For some purposes including cost-effectiveness analysis, measures of health-related quality of life must be based on utilities or preferences for health states that meet the conditions of welfare economics, which assumes that individuals seek to maximize utilities (preferences for particular outcomes) and that overall societal welfare is some function of these individual utilities.
A variety of other measures of health status have been developed. One broad category of measures constructs profiles of people’s health along one or more dimensions. The measures include the SF-36, the 36-item short-form of the Medical Outcomes Study survey created from the Rand General Health Survey (Brook et al., 1979) and the Sickness Impact Profile (Bergner, 1981). Because such profiles do not yield a single summary number from, for example, scores representing physical or mental functioning, these measures of health status have not been combined with life expectancy measures to form an integrative summary measure of population


