
3
SUBPOPULATIONS SENSITIVE TO AIR CONTAMINATION
THIS chapter presents the subcommittee's evaluation of the Air Force's definition of sensitive subpopulations. The subcommittee investigated whether some population subgroups are likely to be more sensitive to the rocket-emission toxicants than the general population and, if some are, (1) how much more sensitive they are and (2) how they can be identified.
This chapter is divided into six sections. The first section presents the subcommittee's evaluation of the literature reviews on populations sensitive to air pollutants published in recent years. In the second section, the subcommittee reviews the available qualitative and quantitative data on the variation in human sensitivity to specific air pollutants, including the three major rocket-emission toxicants discussed in this report. In the third section, the subcommittee identifies several limitations of those studies for purposes of risk assessment. In the fourth section, the subcommittee describes common practices for accounting for sensitive subpopulations in human health risk assessments when data on sensitivity are lacking. In the fifth section, the subcommittee evaluates the Air Force criteria for defining sensitive subpopulations. In the sixth section, the subcommittee presents its conclusions and recommendations.
LITERATURE REVIEW FOR SENSITIVE SUBPOPULATIONS
The subcommittee consulted several recent reviews focusing on varia-
tions in individual susceptibility (i.e., sensitivity) to pollutants (Brain et al. 1988; WHO 1992; NRC 1993; ATS 1996a,b).
The NRC (1993) report concluded that profound differences exist between children and adults. Because infants and children are growing and developing, they are different from adults in composition and in certain metabolic, physiological, and biochemical processes. Before full maturation, damage to a specific organ or organ system might permanently prevent normal physical maturation and increase the incidence of a variety of diseases. That possibility has been demonstrated in studies showing children's sensitivity to the irreversible effects of lead and mercury (Calabrese 1986; Klaassen et al. 1996), enhanced susceptibility to certain radiation-induced cancers (Calabrese 1978), and enhanced risk from a number of carcinogens, e.g., vinyl chloride-induced angiosarcoma (Drew et al. 1983; Calabrese 1986). In addition, certain populations of children might be more sensitive than other children to the effects of chemical agents because of physiological and biochemical factors, such as genetic predisposition, general health status, low socioeconomic status, and possible interactions with certain medications. For certain types of toxicity, children might be more resistant to certain chemical agents, and in such cases, adults might be at greater risk.
Brain et al. (1988) provided a comprehensive analysis of the general principles for variations in human sensitivity to inhaled air pollutants. In that review, Brain et al. (1988) focused primarily on the effects of genetic factors, age and nutrition, gender, smoking, and pre-existing disease states on sensitivity. Non-neoplastic and neoplastic pulmonary diseases were discussed. The analysis was limited, however, to the effects of comparatively low-concentration, long-term exposures to common air pollutants and did not provide substantial guidance relevant to short-term exposures or to the specific compounds—HCl, NO2, and HNO3—examined in this report.
In 1992, the World Health Organization (WHO) reviewed human health effects caused by brief episodes of air pollution and provided some information on the special needs of sensitive populations (WHO 1992). WHO stated that people with pre-existing lung disease or circulation problems usually are more affected by episodes of increased “winter-type” (sulfur dioxide and particulates) pollution than are healthy individuals. On the other hand, for “summer-type” pollution (mostly nitrogen oxides and ozone), WHO could not identify any spe-
cific group of individuals that is more likely to be affected than other groups, although some individuals might suffer more severe responses than others.
The American Thoracic Society (ATS) analyzed the human health effects caused by air pollutants in general, including ozone, nitrogen oxides, carbon monoxide, lead, particulates, sulfur oxides, and acid aerosols (ATS 1996a,b). On balance, thorough evaluation of available epidemiological and controlled-chamber studies did not provide much evidence that adverse health effects caused by exposure to common air pollutants would be substantially more serious in potentially sensitive subpopulations (i.e., asthmatic individuals, children, and the elderly) than in the remainder of the general population.
In summary, the Brain et al. (1988), WHO (1992), and ATS (1996a,b) reports do not offer much guidance on possible safety factors or considerations that should be incorporated in exposure scenarios and risk assessments to ensure protection of sensitive subgroups. In the NRC (1993) report Pesticides in the Diets of Infants and Children, it was recommended that an uncertainty factor up to 10 be considered when evidence of postnatal developmental toxicity exists and when toxicity data relevant to children are incomplete.
CHEMICAL-SPECIFIC VARIATION IN HUMAN SENSITIVITY
To evaluate the potential for variation in human sensitivity to the rocket emission toxicants specifically, the subcommittee examined data for HCl, NO2, and HNO3 and for two additional compounds for which extensive data on variation in human sensitivity are available—ozone and sulfur dioxide (SO2). Data for these compounds were evaluated because the human studies allow a comparison between responses in selected groups of sensitive populations and in healthy individuals. However, the subcommittee recognizes that ozone and SO2 are not specifically of concern to the Air Force, and the conclusions drawn from the effects of those agents cannot be assumed to apply to HCl, NO2, or HNO3, for which no similar data are available.
HYDROGEN CHLORIDE
Humans with respiratory problems have been presumed to be more
sensitive to HCl; however, no data are available on HCl that directly support that hypothesis. Data presented in Appendix D suggest that 2 and 5 ppm might represent no-observed-effect levels (NOELs) for sensitive and healthy populations, respectively.1 On the basis of the work of Stevens et al. (1992)—who showed that a 1.8-ppm HCl exposure to young asthmatic adults for 45 min, including two 15-min exercise periods, was without effect—2 ppm can represent a NOEL for sensitive individuals for a 45-min exposure. On the basis of general occupational experiences, industrial hygienists suggest that slight symptoms might occur at exposure concentrations around 5 ppm (see Appendix D). Thus, the human data on HCl suggest that if individuals with asthma are more sensitive, the exposure concentration associated with a threshold for response in sensitive individuals is perhaps only 2- to 3-fold lower than the concentration associated with a threshold for response in healthy individuals.
NITROGEN DIOXIDE
The data available to judge the potential impact of NO2 on particularly sensitive subgroups are not consistent (see Appendix E). NO2 is emitted in the home environment by gas cooking and has been reported to increase susceptibility to respiratory-tract infections in young children (Melia et al. 1979; Hasselblad et al. 1992; EPA 1993). However, that effect is believed to result from long-term exposures, which are not applicable to rocket-launch situations. Short-term exposures of human volunteers to NO2 have generally provided conflicting results. The ATS (1996b) compiled a list of nine controlled NO2-exposure studies of asthmatic subjects published since 1980. For seven of the studies, no changes in pulmonary function or airway responsiveness were reported. One study (Bauer et al. 1986) showed that exposure of asthmatic subjects to NO2 at a concentration of 0.3 ppm potentiated exercise-induced bronchospasm and airway hyperactivity after cold-air provocation. By
|
1 |
In this report, the phrase no-observed-effect level (NOEL) is used instead of no-observed-adverse-effect level (NOAEL) throughout because mild effects of concern to the Air Force often would not be considered adverse. Definitions of mild and adverse effects are presented in Chapter 4. |
comparison, exposure of healthy humans at concentrations up to 4 ppm usually failed to affect pulmonary function (ATS 1996b). However, in another study, no significant lung-function alterations could be found in asthmatic subjects exposed at 0.3 ppm NO2 for 1 hr (Morrow and Utell 1989). Mohsenin (1987) found heightened airway reactivity in asthmatic subjects exposed to NO2 at 0.5 ppm for 1 hr. However, Linn et al. (1985) observed no effects in asthmatic or healthy individuals exposed to NO2 at concentrations up to 4 ppm for 1.25 hr; that observation was attributed to potential adaptation of the subjects who lived in an area with frequent increases in common air pollutants. Morrow et al. (1992) found responsiveness to a 4-hr exposure to NO2 at 0.3 ppm to be slightly greater in patients with chronic obstructive pulmonary disease (COPD) than in elderly healthy subjects. Interindividual variation in responsiveness also was substantially greater in elderly subjects than in the other groups (Morrow et al. 1992). Thus, some study comparisons suggest that the NO2 concentrations at which individuals begin to respond are approximately 10-fold lower in those with asthma or COPD than in healthy individuals; other comparisons suggest no difference in the exposure concentration representing a threshold for effects in the two subgroups.
NITRIC ACID
There are few human studies available for HNO3 (Appendix F). A study by Aris et al. (1993) identified a NOEL for exposure of healthy humans to HNO3 at 0.2 ppm for a period of 4 hr. The studies with human asthmatic subjects have shown that this portion of the population might be more sensitive to HNO3 than healthy individuals, but the data are equivocal. Two studies by Koenig et al. (1989a,b) provide somewhat different results but suggest that some asthmatic individuals under some conditions might experience a mild, reversible increase in respiratory resistance when exposed to HNO3 at concentrations as low as 0.05 ppm for 40 to 45 min. Applying Haber's rule to the 4-hr NOEL of 0.2 ppm for healthy adults would yield a 1-hr NOEL of 0.8 ppm, or a 45-min NOEL of 1 ppm. Comparing that NOEL with the LOEL of 0.05 ppm for individuals with asthma, both for 45 min, suggests that individuals with asthma might begin to respond at doses as much as 20-fold lower than healthy adults.
OZONE
Data are conflicting concerning the relative sensitivity of healthy adults and individuals with asthma or COPD to ozone. Several epidemiological studies strongly suggest that individuals with asthma are more sensitive to episodes of increased ozone air pollution than individuals without asthma. In controlled chamber studies, however, exposure to ozone generally resulted in only small changes or no changes in the lung function of subjects with asthma as compared with controls (Kreit et al. 1989; ATS 1996a). Similarly, the effects were not more severe in people with COPD than in people without (Linn et al. 1982; Solic et al. 1982).
SULFUR DIOXIDE
SO2 (and sulfuric acid aerosols) can elicit more severe responses in individuals with asthma than in healthy individuals. A controlled-exposure study has shown that asthmatic subjects begin to show responses at concentrations of SO2 (1 ppm) that are 5-fold lower than the concentrations at which healthy individuals respond (5 ppm) (Sheppard et al. 1980). In another study (Linn et al. 1987), healthy and atopic subjects showed practically no changes in pulmonary function when exposed to SO2 at 0.6 ppm, whereas some moderately to severely asthmatic subjects responded even at 0.2 ppm, a 3-fold difference. Those asthmatic subjects responded with an increase in specific airway resistance up to 20 times higher than the healthy subjects. Those with asthma also have been found to be more sensitive to the effects of inhaled H2SO4 aerosols, and exposure to those aerosols is linked to increased nonspecific airway hyperactivity (Linn et al. 1989). Another function affected by inhalation of H2SO4 is mucociliary clearance, which usually slows in response to exposure to SO2 (Spektor et al. 1989). That effect could be more detrimental to people with respiratory-tract infections or immunodeficiencies than to healthy individuals.
LIMITATIONS OF EXISTING STUDIES
Several limitations of the available data make it difficult to evaluate the degree to which specific human subpopulations might be more sensitive
to air contaminants than healthy adults. One limitation is that most studies report only the mean values for pulmonary-function measurements; however, interindividual variation might be considerable. For example, Linn et al. (1987) reported a difference in total symptom scores of up to 10-fold or higher among moderately to severely asthmatic individuals exposed to SO2. In fact, in an in-depth analysis of the effects of NO2 in humans, Morrow and Utell (1989) found that among those with asthma, there appeared to be an even more-sensitive (hyperasthmatic) subpopulation.
A second limitation is that sensitive members of the population cannot be studied in a controlled setting. It is neither feasible or ethical to recruit people with severe cardiac or pulmonary disease or severe asthma into controlled exposure experiments, particularly those involving exercise. Thus, although controlled-exposure studies might confirm the suspicion derived from epidemiological studies that a more-sensitive subpopulation exists, they do not include the extremes in sensitivity that might in fact exist. It is also not feasible or ethical to conduct controlled exposure studies using infants or small children. The few epidemiological studies in which effects in children were compared with effects in adults failed to show differences (i.e., in response to acute exposures to ozone; Spektor et al. 1988; Berry et al. 1991).
A third important limitation is that studies involving human volunteers would necessarily involve exposures to comparatively low concentrations of pollutants. Because clinical studies cannot be conducted using high exposure concentrations, reliable data are lacking on the magnitude of such differences in the proportion of people affected and in the severity of response at high exposure concentrations. At higher exposure concentrations, such as those that might occur during a catastrophic abort of a rocket launch, young children or elderly people with compromised pulmonary and cardiovascular health might be disproportionately more affected than healthy individuals and show more severe responses.
Finally, experimental studies on humans measure only a few aspects of the effects of air pollution: pulmonary-function-test changes and, on occasion, minor signs of inflammatory events in airways and lung parenchyma. Such effects are considered minor and certainly not a serious threat to health, in contrast to the serious problems observed during episodes of high air pollution (i.e., increased hospital admissions and increased morbidity and mortality).
COMMON RISK-ASSESSMENT PRACTICES FOR SENSITIVE SUBPOPULATIONS
The specific issue of how to estimate risks for sensitive subpopulations was the topic of a recent symposium (Mattie 1996). An entire session was devoted to presentations discussing how to incorporate variations in human sensitivity in risk assessments. In particular, Grassman (1996) emphasized that failure to consider differences in susceptibility could result in the propagation of standards that are not protective for highly susceptible segments of the population. The subcommittee agrees in principle with that conclusion. However, Grassman (1996) used examples that cover a wide variety of disease states, from cancer to neurotoxicity, and that cover numerous individual agents. Most of those toxicants illustrate the importance of interindividual variations in metabolism and pharmacokinetics. Although the subcommittee found the information discussed in the symposium to be useful in general, it did not find any specific data relevant to the three rocket-emission compounds under consideration or to acute inhalation exposures.
In developing guidelines for setting community emergency exposure levels (CEELs) for hazardous substances, the NRC (1993) recommended consideration of the criteria for identifying sensitive subpopulations set by EPA. EPA (1994) noted that human populations, as opposed to experimental animals, react more heterogeneously to toxic agents, and defined sensitive individuals as those who experience an adverse health effect earlier or at a lower dose than the average individual. EPA (1994) recommended the use of an uncertainty factor to account for variation in sensitivity among individuals when calculating inhalation reference concentrations, intended to be safe for the general population, on the basis of data from healthy humans or animals. Specifically, the exposure concentration identified as a no-observed-adverse-effect level (NOAEL) for effects in healthy adult populations is divided by an uncertainty factor of 10 to estimate a NOAEL for potentially more-sensitive subgroups. The NRC has previously concluded that this practice is reasonable (NRC 1986,1993, 1997). That uncertainty factor applied to a NOAEL, however, is intended to derive a ''safe" exposure level (or concentration) below which adverse health effects are not expected even in sensitive subpopulations; it has no meaning for the shape or slope of the exposure-response curve. The default value of 10
is used for a wide variety of noncancer toxic end points and exposure routes, as described by Grassman (1996), not just respiratory effects resulting from an inhalation exposure.
DEFINING SENSITIVE POPULATIONS
As described in Chapter 2, the Air Force considers the sensitive subgroup to include children (less than 15 years of age), the elderly (more than 64 years of age), and all people with bronchitis, asthma, or other physiological stress, especially upper-respiratory ailments (Gene Killan, U.S. Air Force Space Command, personal commun., May 6,1996). The subcommittee finds the phrase "physiological stress" to be too vague to be useful, is not aware of data supporting the particular age cutoffs specified, and does not support the use of age cutoffs in general for identifying sensitive subgroups. The subcommittee believes that disease state should be the principal attribute used to define sensitive subgroups. Age should be used as an attribute only to the extent that it correlates with disease states or other physiological conditions that could give rise to greater sensitivity. Selection of the exact ages for the cutoff is arbitrary and difficult to defend against claims that the age was adjusted to influence the size of the sensitive subgroup. Instead, site-and age-specific prevalence of cardiopulmonary diseases, such as asthma and COPD, together with the age distribution of the population should be used to define the sensitive subgroups; that is, in each age group (less than 15,15 to 64, more than 64), the number of individuals estimated from U.S. Census data to be in the population near the launch site should be multiplied by the prevalence of relevant cardiopulmonary disease. The sum of those products over all age categories provides a less arbitrary (although still quite uncertain) estimate of the number of individuals in the sensitive subgroups. Where site-specific data are not available, a default prevalence from a relevant data set could be used. If it is not feasible to provide a more rigorous justification and definition of sensitive subgroups, the subcommittee questions the need for separate ERFs for sensitive and normal subgroups.
The U.S. Bureau of Census has been compiling national health data continuously since 1957. The National Health Interview Survey (NHIS) multistage probability design is intended to provide estimates of the health status of the civilian, noninstitutionalized population of the Unit-
ed States (Kovar and Poe 1985). Demographic and personal data collected for each survey subject include household composition, date of birth, age, sex, service in armed forces, education, race, origin, current occupation or industry, marital status, income, hospitalization history, limitation of activity, disability days, 12-month bed days, doctor contacts, general health status, height, and weight. Participants are asked questions regarding chronic health conditions of various body systems, including the skin (since 1969), the respiratory system (since 1970), and the cardiovascular system (since 1972). Conditions identified in questions concerning the respiratory-system include bronchitis, bronchiectasis, asthma, hay fever, sinus trouble, emphysema, pleurisy, tuberculosis, lung abscess, and work-related respiratory conditions. Conditions identified in questions about the cardiovascular-system include rheumatic fever, rheumatic heart disease, arteriosclerosis, congenital heart disease, coronary heart disease, hypertension, stroke or cardiovascular accident, brain hemorrhage, angina pectoris, myocardial infarction, other heart attacks, damaged heart valves, tachycardia, heart murmur, other heart trouble, and aneurysm. The subcommittee considers any of the cardiovascular and pulmonary conditions listed above as likely to render an individual more sensitive to the effects of rocket-emission toxicants than members of the population without those conditions.
CONCLUSIONS AND RECOMMENDATIONS
DEFINING SENSITIVE SUBGROUPS
Epidemiological studies strongly suggest that some individuals within any given population might be more sensitive to some air pollutants, such as NO2, ozone, or SO2. During episodes of heavy air pollution, most of those who seek or should get medical attention are those with asthma or the elderly suffering from COPD or other cardiopulmonary problems (ATS 1996a,b). The subcommittee recommends that disease status be used as the principal attribute for identifying sensitive subgroups rather than age cutoffs. The subcommittee believes that a more accurate assessment of the number of potentially sensitive individuals in the populations near the launch sites can be obtained by basing sensitivity on the estimated prevalence of health conditions likely to render a person sensitive rather than by basing sensitivity on indirect measure-
ments such as age. An extensive database created by the NHIS could be used to characterize the population near launch sites by identifying the proportion of individuals in specific age categories with specific conditions that might render them more sensitive. The U.S. Census data can be used by the Air Force to obtain the age structure of the communities near launch sites.
QUANTIFYING THE DEGREE OF DIFFERENCE IN SENSITIVITY BETWEEN SENSITIVE AND NORMAL SUBGROUPS
Figure 3-1 illustrates three ways in which an exposure-versus-incidence curve for HCl, NO2, and HNO3 for nonimmunologically mediated effects might differ between sensitive and normal populations: (1) the threshold for response for the sensitive subgroups might be lower, but the slope of the curve is similar to that for the normal population; (2) both subgroups exhibit the same threshold, but the slope of the curve for the sensitive subgroup is steeper than that for the normal population; and (3) a combination of relationships 1 and 2 also is possible. The ERFs included in LATRA assume that case 3 applies; in other words, sensitive subgroups begin to respond at lower concentrations than the normal population, and the slope of the exposure-versus-incidence curve is steeper for the sensitive subgroup than for the normal population.
Although a lower threshold and steeper slope of the exposure-versus-incidence curve for the sensitive subgroup seems reasonable, as described above, data that would allow quantifying a difference in both intercept (threshold) and slope between sensitive and normal populations are limited. There is no information for any of these toxicants relevant to the slope of an incidence-versus-exposure dose-response curve. The number of subjects included in the studies is too small, and the controlled experiments are not designed to determine how the proportion of individuals responding increases with increasing exposure concentration. There are some data relevant to the threshold for response, however. For NO2, the data are equivocal. Some studies, but not others, suggest that individuals with asthma might begin to respond at an exposure concentration up to 10-fold lower than do normal healthy individuals. For HCl, young children or people suffering from asthma or COPD might respond at lower concentrations, but only 3-fold lower, than healthy adults. For HNO3, the data from the few studies available
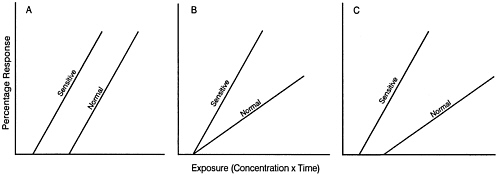
FIGURE 3-1 Hypothetical exposure-response "curves" for populations of sensitive and normal individuals. (A) Curves have a different intercept (threshold) but the same slope. (B) Curves have the same intercept (threshold) but different slopes. (C) Curves have a different intercept (threshold) and different slopes
are equivocal as to whether individuals with asthma respond at lower total exposures than healthy individuals, but the difference in threshold might be as high as 20-fold.
Data from SO2 and ozone do not show dramatic differences in sensitivity between individuals suffering from pre-existing lung diseases such as asthma or COPD and those without. Clinical studies with controlled SO2 exposure suggest that moderately to severely asthmatic individuals might show functional changes, on average, up to 20-fold more severe than those seen in controls but that asthmatic individuals begin to respond at a concentration no more than 5-fold lower than healthy individuals. For ozone, no similar data are available, and the few studies with people suffering from COPD have shown no differences either in the threshold or severity of response.
Data for all the inhalation toxicants discussed above, however, are for comparatively low exposure concentrations. Conceivably, at higher exposure concentrations, young children or individuals with compromised pulmonary or cardiovascular health might be more severely affected than healthy individuals. The subcommittee concludes that, in the general population, some individuals have pre-existing conditions that are likely to make them more sensitive to NO2, HCl, and HNO3 than healthy individuals both in the severity of response at a given exposure concentration and in the exposure concentration and duration required to initiate a response. Given that in the general population surrounding the launch sites, individuals are likely to be found who are more sensitive to the rocket-emission toxicants than healthy adults, the subcommittee believes that provisions should be made to ensure their protection. Where the data are equivocal, the subcommittee believes that the worst case possibility should be employed. Thus, the subcommittee recommends using the assumption that for short exposure durations (i.e., 1 hr or less), sensitive individuals begin to respond at lower concentrations than normal individuals by a factor of 10 for NO2, a factor of 3 for HCl, and a factor of 20 for HNO3.













