
2
The Future Burden of Cardiovascular Diseases in Developing Countries
Cardiovascular disease (CVD) is currently a substantial cause of death and disability in many low- and middle-income countries, and this burden will be higher in the future. Three factors will determine the increase in death and disability from this disease. First, as populations age, more people will reach ages at which CVD becomes common. Second, older populations will be more exposed to risk factors including tobacco, high blood pressure, diets high in saturated fat, obesity, and a sedentary life-style. Third, populations may change their use of preventive and curative health services.
Aging populations are the result of declining fertility and declining mortality in earlier years. The probability of death before age 5 is expected to decrease by half in demographically developing countries—from 11 percent in 1990 to 5 percent in 2020—for both males and females. The probability of death between ages 15 and 60 is expected to decline from 20 to 12 percent for women and to remain close to 24 percent for men over the same period. Estimates suggest that the proportion of adults (both young and older) will rise sharply. Developing countries will have a 108 percent increase in the number of adults aged 30-69 from 1990 to 2020 (Murray and Lopez, 1996; UN, 1995). The number of deaths before age 30 is expected to decline by 41 percent between 1990 and 2020. In contrast, the numbers of deaths between ages 30 and 69 and at age 70 and above are expected to increase by 149 percent and 53 percent, respectively.
PROJECTIONS OF THE FUTURE BURDEN
Projections of the future burden of CVD rely on models because there are few prospective studies in developing countries. Some projections are based solely on current demographic trends (Bulatao and Stephens, 1992), whereas
others rely on extrapolation of past trends and population projections. Aging of the population is the only predictive variable in projection models. Murray and Lopez (1996) had the most comprehensive projections for the years 1990 to 2020, and these include estimates for different causes of mortality. The projections rely on an econometric model that has four variables: (1) per capita income, (2) human capital (average number of years of schooling in a population), (3) smoking intensity, and (4) time. They have three levels for future growth—baseline, optimistic, and pessimistic—based on standard, higher, and lower growths in per capita income. The model is applied to each disease and injury group by age group and by sex.
Table 2-1 summarizes the results for CVD using this model for the years 1990 and 2020. Most of the increase in total CVD deaths is due to ischemic heart disease and cerebrovascular disease. The ratio of CVD deaths to total deaths is stable across the baseline (34 percent), optimistic (36 percent), and pessimistic (31 percent) scenarios. In contrast, the contribution of all communicable diseases will differ greatly between baseline (18 percent) and pessimistic (25 percent) scenarios. This reflects the fact that income growth has large impacts on early, but not middle-age, mortality (World Bank, 1993). In rank order of disability-adjusted life years (DALYs), ischemic heart disease and cerebrovascular disease, respectively, will change from being the eighth and tenth largest contributors of disease burden in 1990, to the third and fifth largest contributors in 2020 (Murray and Lopez, 1996).
The increase in CVD mortality projected in Table 2-1 is likely to be conservative. First, the model does not take into account the possible interaction of increases in key risk factors such as tobacco, hypertension, and saturated fat intake. Data from a study of U.S. males suggest that the combination of these three risk factors elevates risk severalfold compared with any single risk factor. Second, the model does not consider the 20 percent increased risk of CVD caused by childhood deprivation, as measured by low birthweight or poor nutritional status (Rich-Edwards et al., 1997). Low birthweight (defined as less than 2,500 grams) is more common in low-income countries, where it averages 16 percent, than in high-income countries, where it averages 6 percent. The highest levels of low birthweight are in South Asia and Sub-Saharan Africa (33 and 16 percent, respectively).
When considering projections for the global burden of CVD, recent trends in the United States show that the long-standing decline in stroke mortality has stopped or even reversed and the decline in mortality from coronary heart disease appears to have stopped. There are also persistent or growing disparities in CVD mortality between white and minority populations, with minority populations at greater risk (AHA, 1998; Labarthe, 1998). Thus, the challenges of controlling CVD continue in the developed countries. There is much yet to be learned through application of R&D to the CVD epidemic in developing countries.
TABLE 2-1 Deaths from Cardiovascular Diseases in 1990 and 2020, by Region (thousands)
|
|
|
|
Deaths at All Ages |
Percentage of Deaths at All Ages |
Deaths at Age 30-69 |
Percentage of Deaths at Age 30-69 |
||||
|
Region |
Cause |
Sex |
1990 |
2020 |
1990 |
2020 |
1990 |
2020 |
1990 |
2020 |
|
Developing country |
Ischemic heart disease |
Males |
1,828 |
4,347 |
9 |
14 |
899 |
2,355 |
12 |
14 |
|
|
|
Females |
1,737 |
3,501 |
9 |
15 |
651 |
947 |
12 |
12 |
|
|
Cerebrovascular disease |
Males |
1,461 |
3,218 |
7 |
10 |
679 |
1,696 |
9 |
10 |
|
|
|
Females |
1,492 |
2,775 |
8 |
12 |
582 |
782 |
11 |
10 |
|
|
Inflammatory and rheumatic heart disease |
Males |
319 |
591 |
2 |
2 |
149 |
370 |
2 |
2 |
|
|
|
Females |
368 |
448 |
2 |
2 |
162 |
199 |
3 |
2 |
|
World |
Ischemic heart disease |
Males |
3,126 |
6,077 |
12 |
16 |
1,427 |
3,014 |
15 |
16 |
|
|
|
Females |
3,134 |
5,030 |
13 |
17 |
904 |
1,080 |
14 |
12 |
|
|
Cerebrovascular disease |
Males |
2,022 |
3,977 |
8 |
10 |
862 |
1,927 |
9 |
10 |
|
|
|
Females |
2,359 |
3,721 |
10 |
13 |
729 |
867 |
11 |
10 |
|
|
Inflammatory and rheumatic heart disease |
Males |
388 |
677 |
2 |
2 |
222 |
414 |
2 |
2 |
|
|
|
Females |
448 |
544 |
2 |
2 |
192 |
214 |
3 |
2 |
|
SOURCE: Murray and Lopez, 1996. |
||||||||||
Future Impact of Tobacco
Age-specific mortality and morbidity rates will increasingly be determined by current and future exposure to risks such as tobacco. The relative lack of large, standardized, prospective epidemiologic data in most developing populations makes it difficult to predict trends in tobacco use, high blood pressure, high-fat diets, and obesity. There is enough evidence, however, to suggest that these risks are increasing in many low- and middle-income countries (WHO, 1997).
Currently, only the impact of tobacco can be predicted with some confidence. The contribution of tobacco to the global burden of disease is predicted to increase to about 8.3 million deaths and 124 million DALYs by 2020, with more than 70 percent of these occurring in developing countries. This amounts to a doubling of the percentage of current deaths and a tripling of current DALYs due to tobacco use worldwide (Ad Hoc Committee, 1996). Peto and colleagues (1994) estimated that there will be 10 million tobacco-related deaths annually by 2030-or a total of 100 million deaths over the next 20 years-with half of these occurring in the productive years of middle age (35-69) and causing a 20- to 25-year loss in life expectancy for smokers. These projections are limited by the uncertainty of the impact of past and current smoking patterns. Although current trends predict with some assurance that deaths due to tobacco use will reach 10 million per year, the more difficult prediction is when this will happen.
Tobacco has the highest impact in populations with high underlying cardiovascular mortality. South Asian males, for example, have high (and largely unexplained) levels of CVD. Thus, in India, tobacco-attributable mortality is expected to increase from 1 percent of total mortality in 1990 to 13 percent in 2020. Similarly, in males in the former socialist economies (FSEs) tobacco-attributable mortality is expected to increase from 14 percent of total mortality in 1990 to 23 percent in 2020 (Ad Hoc Committee, 1996). A study in the United Kingdom suggested that among cigarette smokers aged 30-49 years, 80 percent of myocardial infarctions were caused by their tobacco use, among those aged 50-59 years, the figure was 67 percent, and among those aged 60-79 years, it was 50 percent.
TABLE 2-2 Estimated Number of CVD Deaths (in millions) Worldwide Attributable to Cigarette Smoking and Percentage of Total Estimated Global Deaths—1990, 2000, 2010, and 2020
|
|
1990 |
2000 |
2010 |
2020 |
|
CVD deaths attributable to cigarette smoking |
0.96 |
1.40 |
1.93 |
2.61 |
|
Percentage of total deaths |
1.9 |
2.5 |
3.2 |
3.8 |
|
SOURCE: Ad Hoc Committee, 1996. |
||||
Future Effects of Other CVD Risk Factors
There are few reliable cross-sectional or prospective data on the contribution of most risk factors to CVD in developing countries. Thus, the projection of such risks into the future is not possible. For developing countries in 1990, Murray and Lopez (1996) estimated that hypertension contributed to 3.8 percent of total deaths and 0.9 percent of total DALYs. Alcohol use contributed to 1.6 percent of total deaths and 2.7 percent of total DALYs. Physical inactivity contributed to 2.3 percent of total deaths and 0.6 percent of total DALYs.
Elevated blood pressure is a significant cause of ischemic heart disease and stroke worldwide and may have greater effects in East Asian countries (MacMahon et al., 1990). The determinants of elevated blood pressure appear to be similar for different populations. The INTERSALT study of 52 populations (including 17 in developing countries and 5 in FSEs) revealed that urinary sodium (a proxy for sodium intake), body mass index, and high alcohol intake are correlated with high blood pressure. In Western countries, processed foods are the main source of sodium, which contributes significantly to hypertension (INTERSALT, 1988; Law et al., 1991). Consumption of processed foods is increasing in developing countries (WHO, 1992).
Levels of saturated fat intake and blood cholesterol appear to be rising in FSEs and developing countries. With increasing affluence, the consumption of meat and saturated fat rises, and this trend is likely to occur globally (WHO, 1992), particularly where subsidies are given to meat and dairy producers. In urban China, mean body mass index, blood pressure, and cholesterol rose over a three-year period in the late 1980s (Keil and Kuulasmaa, 1989). A study in rural and urban India found values of body mass index, blood pressure, fasting blood cholesterol, and diabetes approaching those of Indian populations in the West.
Evidence is emerging to suggest that obesity is increasing rapidly in developing as well as developed countries. Moreover, since it appears to be escalating in children as well as adults, the health consequences may continue into the distant future. Reliable data are available for only a few developing countries to show increasing obesity over time. In African and Asian countries, obesity is still relatively uncommon, but more prevalent in urban than rural populations (Mbanya et al., 1997).
Diabetes is another independent risk factor for CVD. Its prevalence in adults worldwide was 4 percent in 1995 and is projected to rise to 35 percent or more by the year 2025 (King et al., forthcoming). Although the prevalence of diabetes is higher in developed than in developing countries, the number of adults with diabetes worldwide will rise from 135 million in 1995 to 300 million in the year 2025. The major part of this increase will occur in developing countries: by the year 2025, more than 75 percent of persons with diabetes will reside in these countries. In absolute terms, the countries having the greatest number of people with diabetes are—and will continue to be in the year 2025—India, China, and the United States. Diabetes is more common in women than men, especially in
Latin America and the Caribbean, China, and developed countries. In India, more men than women have diabetes. Diabetes will become increasingly concentrated in urban areas. In developing countries, the majority of persons with diabetes are 45-64 years of age, whereas in developed countries, they are 65 years and over. This pattern is predicted to persist to the year 2025.
CAN DEVELOPING COUNTRIES AVOID THE FUTURE BURDEN?
Changes in coronary heart disease mortality in different populations over periods of only a few years demonstrate the strength of environmental determinants of risk regardless of the underlying genetic composition of those populations. The challenge is to address these environmental determinants effectively, even before research identifies specific subgroups with exceptional genetic risk (Breslow, 1997; Labarthe, 1998). Although CVD mortality early in the epidemiologic transition tends to be highest among the well educated and affluent, most countries that have undergone the epidemiologic transition also observe CVD mortality to be high in population groups with low levels of income and education. Epidemiologic studies in upper- and middle-income countries provide strong evidence for the preventability of CVD (Blackburn, 1997; Dowse et al., 1995). This evidence includes differences in CVD incidence among populations; trends in CVD incidence over time; CVD incidence among migrants; trends of CVD incidence with changes in exposure to risk factors; correlations between risk factor exposure and disease in individuals and populations; estimates of risk reduction due to changing distributions of risk factors in populations; results of clinical trials with risk factor modification; and results of public health trials of population-based risk factor modification (Pearson and Stone, 1997). Together these form a strong rationale to support the CVD risk factor paradigm, which states that controlling major CVD risk factors should control the disease itself.
Although death in middle age need not be common in any population, death in old age is unavoidable, and in some cultures, attempts to avoid it are not acceptable. In the 1880s, 50 percent of U.K. residents died before age 40, and 77 percent before age 70. By 1980, only 3 percent of U.K. residents died before age 40, and 30 percent died before age 70. In both periods, nearly all died before age 100. Evidence that CVD can be avoided also comes from the wide divergence of CVD mortality across populations (Thom, 1989), from international and internal migration studies (Reed and MacLean, 1989), and from changes over time. Analyses from Norway suggest that the scarcity of saturated fat, cigarettes, and alcohol during the Second World War contributed to marked declines in certain chronic diseases (Thelle, 1985).
Second, certain middle-income countries in Latin America (Chile, Argentina, Uruguay, and Cuba) have shown a marked decline in CVD mortality. Mauritius showed marked declines in serum cholesterol, hypertension, and
smoking from 1987 to 1992 (Dowse, 1995). In Poland there was a one-third decline in mortality due to CVD in men and women aged 20—40 between 1991 and 1993. This appears to be attributable in large part to a declining dietary intake of saturated fats—the ratio of polyunsaturated to saturated fats increased from 0.2 to 0.4 in a short time. Declines in saturated fat intake and increases in vegetable fats are consistent with the end of government subsidies to meat and dairy producers (Zatonski, 1996).
Several FSEs have shown marked increases in CVD mortality rates, but the reasons have not been well studied. In many countries, increases follow recent declines. Underlying reasons appear to be the maturing tobacco epidemic, increased saturated fat intake, elevated blood pressure, and poor access to primary and secondary preventive care. The role of risk factors remains poorly understood but offers opportunities for research. Rising incomes may increase tobacco use, use of processed food with high salt content, diets high in saturated fat, and obesity. These effects depend also on the level of information available. For example, in 1970, tobacco use increased with increasing income for males in developed countries. By 1990, however, tobacco use was decreasing with rising income, due partly to better and more available information on its hazards.
Developed countries have shown a remarkable decline in CVD mortality. Canada, for example, has about 40 percent fewer CVD deaths than predicted by 1970 age-standardized rates (Second International Heart Health Conference, 1995). Most declines appear to be driven by gradual life-style changes, declining tobacco consumption, improved diets, and other less understood factors. The rapid declines in Poland, Estonia, and Norway are due to marked socioeconomic changes. The continuing experience in many FSEs may provide new understanding.
Finally, clinical treatments have contributed to the decline of CVD in developed countries, largely by offering wide access to low-cost medical treatment rather than high-technology clinical or surgical treatment. For example, the improved survival from acute myocardial infarction after 1980 is due largely to increasing use of aspirin, low-cost beta-blockers, and to a lesser extent, newer and more expensive clot-dissolving drugs (Forrester et al., 1996).
Cardiovascular Disease Prevention Strategies
Two strategies might be employed for CVD prevention: one that focuses on high-risk individuals and one that focuses on a public health approach (Figure 2-1) (Carleton et al., 1991). The first approach identifies those with high exposure to CVD risk factors and intensively treats them to reduce that risk. Although it is effective for individuals, this approach has limited impact on the population-wide burden of disease, since most cases are not at high risk. The public health approach is to shift the entire distribution of CVD risk factors to a lower level. In reality, many populations use a combination of the two strategies.
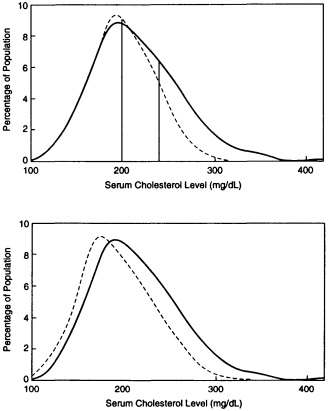
FIGURE 2-1 Cholesterol distribution in the U.S. population aged 20-74 years from the National Health and Nutrition Examination Survey II (1976-1980) and potential changes in this distribution. Top: Expected shift in population distribution of serum cholesterol values with application of high-risk approach (Adult Treatment Panel Guidelines of National Cholesterol Education Program). Dashed line shows effect of the recommendations. Bottom: Expected shift in population distribution of serum cholesterol values with application of public health approach (Population Panel of the National Cholesterol Education Program). Dashed line shows effect of the recommendations. SOURCE: Carleton et al., 1991. Copyright 1991 by the American Heart Association; reprinted with permission.
Efficacy of Current Interventions
The remarkable reduction in CVD mortality documented in the populations of Western Europe, North America, Australia, and New Zealand since 1970 suggests that population-wide efforts are effective in lowering the disease bur-
den. More controlled studies of interventions in schools, work sites, and entire communities have had less certain results but are successful when the intervention is more intense (Pearson and Stone, 1997).
Primary prevention of CVD has been effective in randomized trials that lower CVD risks such as elevated low-density lipoprotein (LDL) cholesterol, high-fat or high-cholesterol diets, hypertension, and cigarette smoking (Forrester et al., 1996; Pasternak et al., 1996). The efficacy of these interventions in the United States has lead to the development of guidelines (Grundy et al., 1997). In general, persons at low risk are encouraged to develop healthier life-styles, and pharmacologic therapies are reserved for high-risk individuals. Primary preventive interventions can be relatively cost-effective, especially for low-cost interventions and subgroups of the population at high risk (Goldman et al., 1996).
Case management strategies have been investigated extensively for patients with both acute and chronic manifestations of coronary heart disease and cerebrovascular disease. Interventions range from relatively inexpensive steps such as the control of high-risk behavior (e.g., smoking cessation, lipid-lowering diet, physical activity, weight reduction) to the use of inexpensive technologies (e.g., lipid-lowering drugs, aspirin, beta-blockers, estrogens) to sophisticated, expensive technologies (e.g., thrombolytic therapies, automated internal defibrillation, coronary angiography with or without angioplasty and/or stent placement, coronary bypass surgery, cardiac transplantation). Guidelines for the management of acute myocardial infarction (Ryan et al., 1996) and secondary prevention strategies (Smith et al., 1995) have been published for the United States. In case management, behavioral changes and inexpensive technologies are highly cost-effective (Goldman et al., 1996).
Although little information is available from developing countries about the feasibility and cost-effectiveness of such management strategies, the committee believes that increasing the use of one or several effective, low-cost medications (aspirin and/or beta-blockers) in survivors of acute myocardial infarction could dramatically reduce CVD deaths in developing countries. As indicated in Table 2-3, the relatively low-cost combination of aspirin and beta-blockers after acute myocardial infarction could avoid about 300,000 deaths due to ischemic heart disease (IHD) and stroke in low- and middle-income countries in the year 2020, if coverage is increased from 30-40 percent to 85 percent of the patient population. If more people with acute myocardial infarction are treated and if the use
of aspirin and beta-blockers is equally high, it is estimated that 400,000 deaths could be avoided in developing countries.
It has been shown in developed countries that when survivors of myocardial infarction stop smoking, there is a profound reduction of mortality. Research on ways to promote smoking cessation deserves support.
ECONCOMIC CONSEQUENCES
The economic consequences of the increasing CVD burden include household health and composition, lost production and earnings, and lost investment and consumption (Over et al., 1994). Few studies exist in developing or developed countries to document these economic losses.
The death of an adult family member can have a devastating impact on the household. In Bangladesh, the probability of death between ages 15 and 60 is 29 percent for females and 31 percent for males. When there is an adult death—most often from CVD—a child of less than 2 years has a 12-fold higher probability of death (Over et al., 1994).
In developing country populations, CVD occurs at an earlier age than in developed country populations. There is a greater loss of productivity and a greater impact on the household. In India, mortality, years of life lost discounted at 3 percent, and productivity-weighted years of life lost (YLL) (productivity weight maximal at age 24) show different patterns (see Table 2-4). In the productivity-weighted years of life lost the greatest loss is during the productive years of middle age.
Data from the United States suggest that reduced productivity and lost output due to CVD cost about $17.6 billion in 1993, or 15 percent of the total economic costs of CVD (including facilities, services, and drugs; AHA, 1993). Total costs for CVD were about 2 percent of the gross domestic product (GDP), while reduced productivity and lost output due to CVD amounted to about 0.3 percent of the GDP. In Canada, CVD accounts for 21 percent of total disease-classifiable costs of illness or a total of U.S. $12 billion per year (HSF, 1994). These costs include treatment, care, and indirect costs, such as the loss of income from mortality and disability. CVD costs are followed by those from injuries (16 percent of the total) and cancer ( I percent). CVD is responsible for the highest proportion (32 percent) of earnings lost due to premature death and is followed by cancer (27 percent); CVD accounts for 17 percent of lost productivity due to disability.
TABLE 2-3 2020: Number and Percentage of Total IHD and Stroke Deaths Avoided by Use of Aspirin, Beta-Blockers, and Increased Treatment
|
|
Aspirin and Beta-Blockers (85% use of aspirin and beta-blockers) |
Aspirin, Beta-Blockers, and Treatment(10% increase in treatment) |
||
|
Age |
Developing Countries |
FSEs |
Developing Countries |
FSEs |
|
30-69 |
72,000 (2%) |
38,000 (3%) |
96,000 (3%) |
45,000 (3.5%) |
|
All ages |
211,000 (2.5%) |
102,000 (3.5%) |
281,000 (3.5%) |
122,000 (4%) |
|
SOURCE: Ad Hoc Committee, 1996. |
||||
TABLE 2-4 Estimates of Mortality in India by Age Group Using Different Weighting Scales—1992
|
Age |
Percentage of Deaths |
YLL at 3% Discount Rate |
Productivity-Weighted YLL |
|
<30 |
41.6 |
59.1 |
29.0 |
|
30-69 |
32.8 |
29.6 |
45.0 |
|
≥70 |
25.5 |
11.3 |
26.0 |
|
NOTE: World Bank estimates of mortality differ from the Global Burden of Disease Study results presented due to the different populations studied. SOURCE: Jha et al., forthcoming. |
|||
As has been noted, developing countries are likely in two to three decades to have a CVD burden comparable to that of developed countries today. However, economic projections suggest that developing countries will not be able to afford expensive cardiovascular procedures and specialists' services (Jha et al., forthcoming). Western-based technologies have increased rapidly in the urban settings of many developing countries, often spurred by inappropriate government incentives.
Control of rising CVD costs will have to rely on the following guidelines: (1) public policies that subsidize prevention and low-cost clinical care ahead of more expensive curative interventions; (2) the use of appropriate technology assessment for new devices; and (3) alignment of health finance and delivery systems to ensure a focus on prevention and low-cost clinical care.
COST-EFFECTIVENESS OF PREVENTION AND TREATMENT
Identifying appropriate public policies for the financing and delivery of cardiovascular care relies partly on analyses of cost-effectiveness. These analyses demonstrate that massive policy-based tobacco control campaigns are cost-effective at U.S. $20-$70 per year of life saved (Jha et al., forthcoming). The cost-effectiveness of treatment, on the other hand, depends largely on the cost and use of medications, given that the effectiveness of most treatments ranges from 20 to 30 percent. Thus, a large impact on the population may be possible only if these drugs are widely accessible and low cost. Aspirin and beta-blockers can be cost-effective in emerging market economies and in many low- and middle-income countries. Cholesterol-lowering statin drugs are expensive in developed countries; thus, their cost-effectiveness is currently unfavorable compared with aspirin or beta-blockers (Goldman et al., 1988). However, such statins are less expensive in developing countries, and most of their patents will expire within 5 years. Thus, there is good reason for introducing them into an essential













