
PREVALENCE OF EXPOSURE AND DATA QUALITY OF LEAD CONTAMINATION IN LATIN AMERICA AND THE CARIBBEAN
ISABELLE ROMIEU/MARINA LACASANA*
The rapid industrial development that the American region has experienced has brought an accumulation of distinct, potentially toxic elements —of which lead is one—into the environment. We have compiled existing information on the magnitude of the problem in Latin America and the Caribbean in order to evaluate: (1) the major sources of exposure to lead in the region, (2) the impact of this exposure as measured by blood lead levels on specific population groups, and (3) the effectiveness of actions by national governments to prevent and control lead exposure. These actions include legislation to protect the environment and occupationally exposed populations.
METHODS
A survey was undertaken with the help of national representatives of the Pan American Health Organization (PAHO). The survey requested information on: (1) production, export, and import of lead (tons/year); (2) industrial use of lead; (3) sources of lead emission in the air; (4) other principal sources of lead exposure; (5) measurement studies of lead in the environment; (6) results of studies that measured blood lead levels in specific populations; and (7) the nature of existing regulations and rules for the control of lead contamination.
RESULTS
Of the national PAHO representatives surveyed, 57 percent (16/28) responded. While the rate of Latin American countries answering the survey, excluding the Caribbean, was 83 percent (15/18 countries), the rate of response from the Caribbean Basin was only 30 percent (3/10 countries).
|
* |
Pan American Center for Human Ecology and Health, Metepec, Mexico |
Latin America and the Caribbean contribute 14 percent of the world production of lead. Peru and Mexico are the leading producers in the hemisphere. In Latin America, the principal lead mines are located in Peru, Mexico, and Argentina; the primary smelters are in Peru, Mexico, Brazil, Argentina, and Nicaragua; and the secondary smelters are in Mexico, Brazil, Colombia, Venezuela, and Trinidad (see Figure 3-4). Several additional Latin American and Caribbean countries also produce lead or import it for industrial use.
Lead, in different forms and compounds, is used in numerous industries and activities, but numbers and intensity of lead use are not well known in Latin America and the Caribbean. In countries such as Mexico, Peru, and Honduras, for example, lead varnishes are commonly used as glazes for ceramicware, although the extent of production and distribution of lead-glazed ceramicware is not precisely known.
The survey data also suggest that for the majority of Latin American and Caribbean countries (excluding Brazil, Guatemala, and Mexico), one of the more important uses of lead is as an antiknocking agent in gasoline. In the last 14 years, however, the lead content in gasoline has actually been reduced in Bolivia, Brazil, Chile, Mexico, Guatemala, Uruguay, and Venezuela. Currently lead levels in gasoline vary from 4.99 grams a gallon (g/gal) in Suriname to 0.70 g/gal in Argentina, Colombia, and E1 Salvador, and 0.19 g/gal in Mexico. According to the survey, 36 percent of the countries in the region that responded have introduced unleaded gasoline. These include Argentina, Bolivia, Brazil, Chile, Colombia, El Salvador, Mexico, Peru, Costa Rica, Guatemala, Honduras, and Uruguay in Latin America and the Dominican Republic and Trinidad in the Caribbean Basin. The survey also assessed the proportion of unleaded gasoline used for automotive purposes because this may provide a good indicator of the success of the national programs to reduce lead contamination of air. Of the countries responding to this question, Brazil, Guatemala, and Mexico reported the greatest proportion of unleaded gasoline used (100, 80, and 46 percent, respectively). They were followed by the Dominican Republic, Chile, Colombia, and Argentina, which reported proportions of 28.6, 13, 10, and 6 percent, respectively. The use of unleaded gasoline in Peru was reported to be minimal (0.2 percent). In other countries, including El Salvador, Costa Rica, and Honduras, information regarding the proportion of unleaded gasoline use was not reported.
The estimates above provide the only measure, albeit an indirect one, of lead levels in air for most of the Latin American and Caribbean countries

responding to the survey. The exceptions are Brazil and Mexico, which have recorded data on air pollutants, including lead. In Brazil, the “national program of alcohol” was initiated in 1975 to bring to the forefront the nation's dependence on imported petroleum. Since the widespread introduction of lead-free gasoline throughout Brazil in 1975, the level of lead in the air in urban zones has diminished by approximately 72 percent. In Mexico, a less extensive program to reduce atmospheric lead was introduced in the 1980s. The Metropolitan Zone of Mexico City, which has monitored air pollutants since 1988, reported significant decreases in atmospheric lead levels, from an annual average of 1.95 µg/m3 in 1988 to 0.28 µg/m3 in 1994. Paralleling this decrease has been an observed lowering of blood lead levels in the residential population in the Metropolitan Zone of Mexico City.
Lead exposures related to use of leaded gasoline are highest in urban environments. Residents of intense vehicular traffic areas generally have blood lead levels much higher than populations exposed to less vehicular traffic. The populations of Latin American and the Caribbean are primarily urban—75 percent of all people in the region live in urban zones, and this percentage is expected to increase in the coming years. This fact, coupled with the observation that 30 percent of the population of the region is less than 15 years of age (corresponding to more than 110 million people), signifies that a great proportion of children in the region are, and will continue to be, subject to high levels of lead exposure attributed to vehicular emissions. Continued attention should, therefore, be given to reducing the lead content of gasoline, because this will markedly reduce the lead exposure of a significant proportion of the population in Latin America and the Caribbean.
Besides lead from vehicular emissions, other sources of lead exposure in Latin America require consideration. Based on the data from our survey, the local authorities in 87 percent of respondent countries recognized that lead emitted into the air also derives from fixed industrial sources, including smelting, petrochemical processing, and mining. The reutilization and recycling of batteries was recognized as an important source of occupational lead exposure. Of total respondents, 75 percent consider paint to represent an important source of lead exposure in the region, 55.3 percent believed that lead contamination of food represents an additional important source of lead exposure, and 25 percent referred to the contamination of water as a potential source of lead exposure.
Data on the content of lead in different items in the environment were reported to have been analyzed by some of the countries responding. Samples of air; sediment and dust; food, particularly fish, shellfish, and vegetables; and water were the items most frequently analyzed. Lead levels in some samples surpassed the norms of the World Health Organization. Unfortunately, sufficient data were not available to determine the importance of these sources of exposure to human health in the region. It is also important to remember that few certified laboratories exist in the area with control of internal and external qualities for measuring lead. This limits the interpretation of the research results that are available.
Measurements of lead in the general population of children and adults were reported for several of the countries responding. In Table 3-3, one can observe that the levels of lead in the blood are higher in populations that live near fixed sources of lead emissions. Average blood lead levels in children varied from 3.4 µg/dl to 39.0 µg/dl, and the proportion of children having lead in their blood above 10 µg/dl varied from zero to 100 percent. Also, it is important to note that potential exposure of different populations through wastes from battery recycling is very high.
In urban populations, lead levels observed in infants ranged from 3.0 µg/dl in Tobago to 28.8 µg/dl in Ecuador. The proportion of young children with lead levels above 10 µg/dl varied between zero and 60 percent. In adult populations, the levels observed are similar, although generally a little higher. In the Metropolitan Zone in Mexico City, blood lead levels have decreased since 1991. Approximately 30 to 50 percent of children are considered to have blood lead levels exceeding 10 µg/dl. This decrease is probably related to the drop in the lead content of leaded gasoline and the introduction of unleaded gasoline in Mexico. In adults, this proportion was slightly greater. One of the factors that could explain this difference is the use of lead-glazed ceramicware, which is still widely used by the adult population.
In occupational populations, the levels of lead in the blood were observed to be uniformly high, and these varied by an average of 21.4 to 48.8 µg/dl, with a range of 4.1 to 104 µg/dl. The data collected, however, were insufficient to determine the magnitude of the lead poisoning in these populations.
Finally, it is important to determine the government's perceptions regarding the problem of lead, and to know if a given country is taking action to prevent or control lead poisoning. Of the countries responding to this survey, 75 percent indicated that their governments identify lead as a
TABLE 3-3
Blood Lead Levels in Different Population Groups by Country (in µg/dl)
|
Country |
Population |
Location |
n |
Age (years) |
Average |
Range |
>10 µg/dl (percent) |
|
Argentina |
Children |
Fixed source |
424 |
5–15 |
22.1±7.5 |
7.0–42 |
75a |
|
Brazil |
Adults |
Urban |
156 |
15–49 |
11.8±5.2 |
2.8–27.2 |
45 a |
|
Adults |
Fixed source |
71 |
15–63 |
27.2±5.7 |
9.2–42 |
100 |
|
|
Children |
Urban industrial |
199 |
4–5 |
9.58±4.6 |
0.6–35.7 |
30 a |
|
|
Children |
Fixedsource |
6 |
2–7 |
39.0±5.0 |
34–45 |
100 |
|
|
Chile |
Nursing infants |
Urban |
200 |
12 months |
4.3±1.8 |
0.5–18 |
5 a |
|
Ecuador |
Children |
Urban |
64 |
7 |
28.8 |
17–54 |
100 |
|
Children |
Urban |
27 |
Infants |
14.4 |
6.0–20 |
60 |
|
|
Adults |
Urban |
83 |
Pregnant women |
18.4 |
— |
60 a |
|
|
Mexico |
Children |
Urban |
200 |
< 5 |
9.0±5.77 |
1–31 |
27.8 |
|
Adults |
Urban |
200 |
15–55 |
9.74±6.19 |
1–39 |
36.5 |
|
|
Adults |
Urban |
3,309 |
15–45 |
10.55 |
.5–62.2 |
42 |
|
|
Children |
Rural |
46 |
6–8 |
7.3 |
2.7–15.2 |
17.4 |
|
|
Adults |
Rural |
92 |
15–62 |
12±7.2 |
1.6–3.9 |
50 |
|
|
Uruguay |
Children |
Urban |
48 |
2–14 |
9.5 |
1–31 |
30 a |
|
Nicaragua |
Children |
Fixed source |
50 |
1–6 |
11.5±3.7 |
8.3–53.6 |
45 |
|
Trinidad |
Mothers |
Urban |
94 |
— |
4.8±2.03 |
1.2–14.4 |
2.12 |
|
Tobago |
Children |
Urban |
94 |
Infants |
3.4±1.6 |
0–8.7 |
0 |
|
Children |
Battery recycling |
20 |
3–19months |
72.1 |
17–235 |
100 |
|
|
a Estimated Source: Compiled by Isabelle Romieu. |
|||||||
public health problem. In 50 percent of these countries, legislation exists to regulate the content of lead in different sectors. Only 19 percent of the countries with existing legislation, however, reported that it was routinely enforced. Enforcement, when it does occur, tends to be sporadic and inconsistently applied.
CONCLUSIONS
This survey demonstrated that there is a lack of data available to evaluate the extent of the problem of lead exposure in the Americas and the Caribbean. Perhaps the data exist, but are not routinely published. It is more likely, however, that the data do not exist. If so, it is imperative that they be collected.
The partial results of this survey suggest that lead poisoning is a very important health problem in the region. The principal sources of exposure are related to vehicular emissions, coming from automobiles that use leaded gasoline; industrial use, in particular in paints and batteries; and food. The majority of governments in the region know that lead is a serious health problem, but the actions they have taken to confront the problem have been limited thus far. Based on our survey, 13 countries (36 percent) have realized or initiated changes to introduce nonleaded gasolines, but the use of lead-free gasolines remains limited in the region.
Drs. Romieu and Lacasana wish to thank the following individuals for their valuable contributions: Henri Jouval, Isaias Daniel Guti érrez, Arend Van de Kork, Philippe Lamy, Manuel Nasif Issa, Armando López Scavino, Celia Castelló, Mauricio Habaca Marileo, Raúl Penna Melo, Franciso José Mardones, Antonio Romero Hernández, Carlos Hilburg, Carlos Alfonso Osorio, Javier Hernán Paiga Coca, Germán Giraldo Salinas, Ramón José Zapata Giraldo, Luis Edilberto Blandon Palomino, Merlin Fernández, Luis A. Leal, Gustavo Mora, Ricardo Núñez, Yamara F. Hernández F., Mauricio Pardón, Gonzalo A. Ordoñez, César Hermida, Carlos A. Linger, Carlos Morales, Fernando Meneses González, Jorge Jenkins, Juan Antonio Casas, Rocio Espinoza Laín, Habib Latiri, Guy Felix, Paul Ellis, Juan Carlos Veronelli, Roberto Solvetella, Jorge W. Bruschem, and Jorge Baso.
NATURE AND EXTENT OF LEAD EXPOSURES AND TOXICITY IN THE AMERICAS
ELLEN K. SILBERGELD*
Lead exposures, both chronic and acute, contribute to the incidence of lead poisoning in many populations in the Americas. While local conditions and source terms are extremely important for understanding the nature of specific risks within communities, there are sufficient similarities among exposures that valuable information can be generalized for purposes of preventive health policy. For purposes of developing hemisphere-specific strategies for prevention, both the local and international aspects of lead exposure are important. Lead is an international problem because of transnational movement of lead released into the air from stationary and mobile sources; because of trade in products containing lead, such as food and painted objects; and because of the movement of lead-containing discards (Silbergeld, 1995). Lead sources may be considered in terms of mass balance; because of the elemental nature of lead, anthropogenic activity that shifts lead from crustal deposits to the human environment increases the likelihood of human exposure. In addition, many lead sources contribute to multiple pathways, complicating exposure assessment.
Mexico, Canada, Peru, and the United States are major world lead producers and exporters. Since early European settlement, lead mining and production have been economically important in the hemisphere. Over the past 20 years, lead production and consumption have continued to grow; the largest and fastest growing use of lead is in storage batteries. Lead exemplifies the paraoccupational nature of chemical exposure problems: mining, smelting, and production expose both workers and nearby communities to lead releases; moreover, workers may bring lead dusts home. “Fouling the nest” occurs when lead industries are located near or even conducted in homes, or when parents or children work in lead-using industries and bring the contaminant home with them.
|
* |
University of Maryland Medical School, Baltimore, Maryland |
The complexity of lead source/pathway relationships is demonstrated by analysis of lead in air. As shown in Figure 3-5, lead released from cars first enters the air, where it may be an immediate source of lead exposure by inhalation. Most lead from this source is deposited close to roadways, where it contaminates dusts and soils. This contamination may affect the food supply, particularly foods grown exposed to air; drinking water; and dusts and soils in houses, schools, and other environments. Because of its pervasiveness, lead in gasoline rapidly contributes to human exposure. In the period 1976–1992, the use of lead in gasoline accounted for about 30 percent of median blood lead levels in the United States.
While reducing lead levels in gasoline immediately reduces ambient air concentrations of lead (and crop deposition, with a lag time associated with the harvest cycle), lead deposits in soils and dusts remain for decades, offering significant potential sources for exposure. Moreover, actions to reduce lead in gasoline (grams/liter) may not affect overall lead use or air lead concentrations if total gasoline consumption continues to grow, and leaded fuels retain a substantial market share.
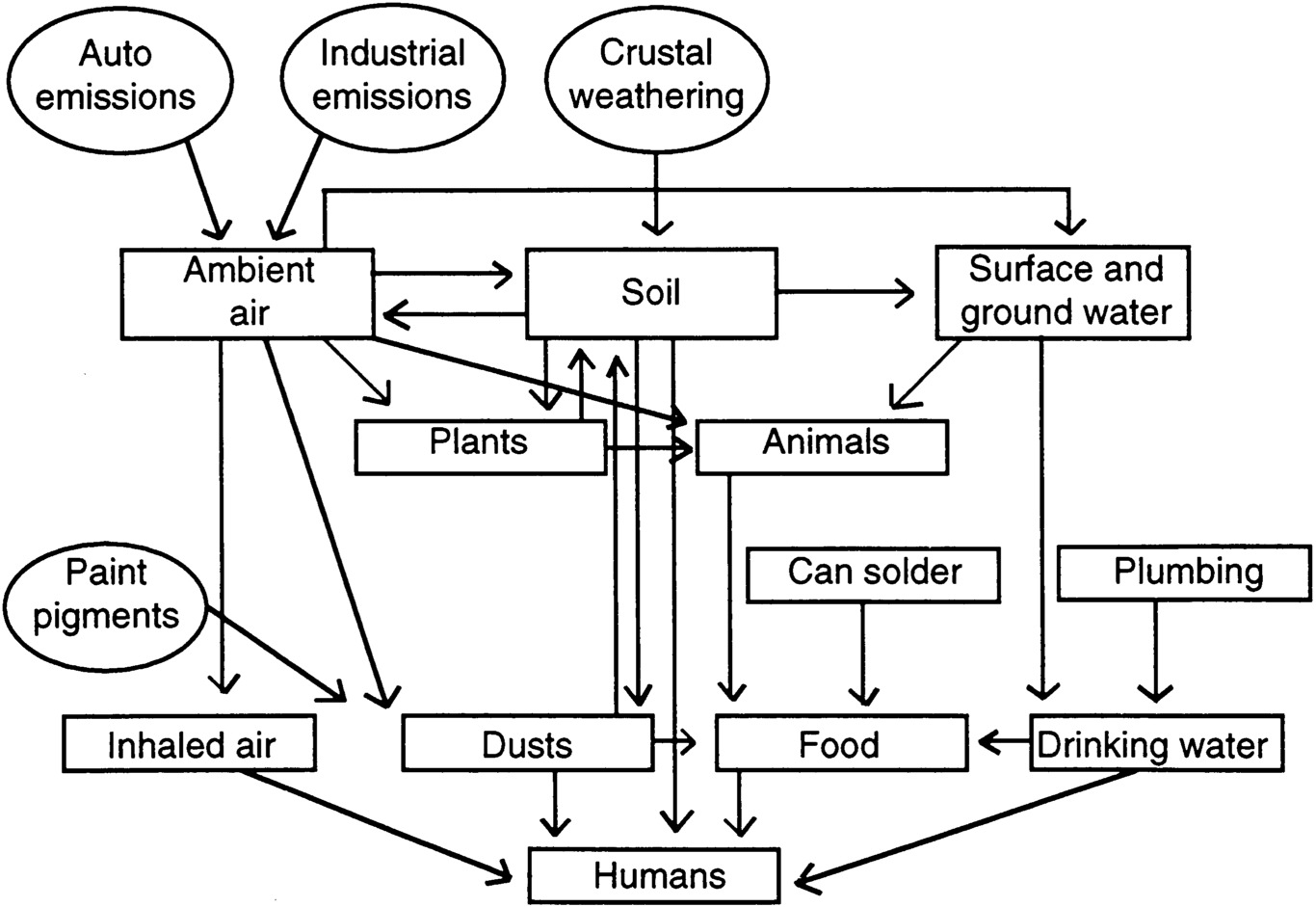
Figure 3-5. Sources and pathways of lead from environment to humans. Source: Adapted from EPA, 1986.
The problem of lead in gasoline and its residuals is similar to the problem of lead in paint. Despite the International Labor Organization convention in the early 1920s against white lead, to which several countries in the Americas are signatory, and despite bans on use of lead-based paint in residences in the United States, millions of tons of lead in paint remain on building surfaces. For example, in the United States this reservoir of past lead use constitutes one of the most intense sources of lead exposure, particularly to young children. Exposure to lead paint and to other sources are often most intense in populations at economic and other disadvantage. In the United States, current (1988-1992) rates of increased lead exposure (blood lead concentrations >10 µg/dl) are five times greater in African American children, and twice as high in poor children, than in affluent white children.
The complexity of lead sources can be studied using careful analysis of pathways, and also by stable isotopic techniques. These methods (NRC, 1993) exploit the geochemical differences in lead deposits on Earth. If different sources utilize lead from geochemically distinct sources (such as, for instance, the United States and Australia), then the relative contribution of each source in environmental media and in blood can be defined, using sensitive ultraclean mass spectrometry. Stable isotopic analyses have also demonstrated the importance of bone lead stores as sources of internal exposure during major physiological stages in humans. During pregnancy, lactation, and aging, bone lead may be mobilized back to the circulation and present an opportunity for (re)exposure of the host, or for additive exposure to the fetus during pregnancy.
Concerns over the prevalence of lead exposure have focused on the young child, although lead is also recognized as a major health problem for adults, particularly in industry. Children are at risk for three reasons: their exploratory behaviors and hand-to-mouth activity places them at risk of lead exposure, if it is present in their environments; children absorb lead from the gut with 5–10 times the efficiency of adults; and certain cellular targets for lead toxicity may be more sensitive in the young child than the adult. Several major epidemiologic studies, some of them prospective in design, have associated relatively small increases in body lead burden with persistent problems in learning and school attainment. In addition, prenatal lead exposures are associated with decreased growth in stature and delays in neurobehavioral development.
As shown in Figure 3-6, increases in body lead burden (as measured by dentine lead levels in teeth) were associated with decreased attainment on
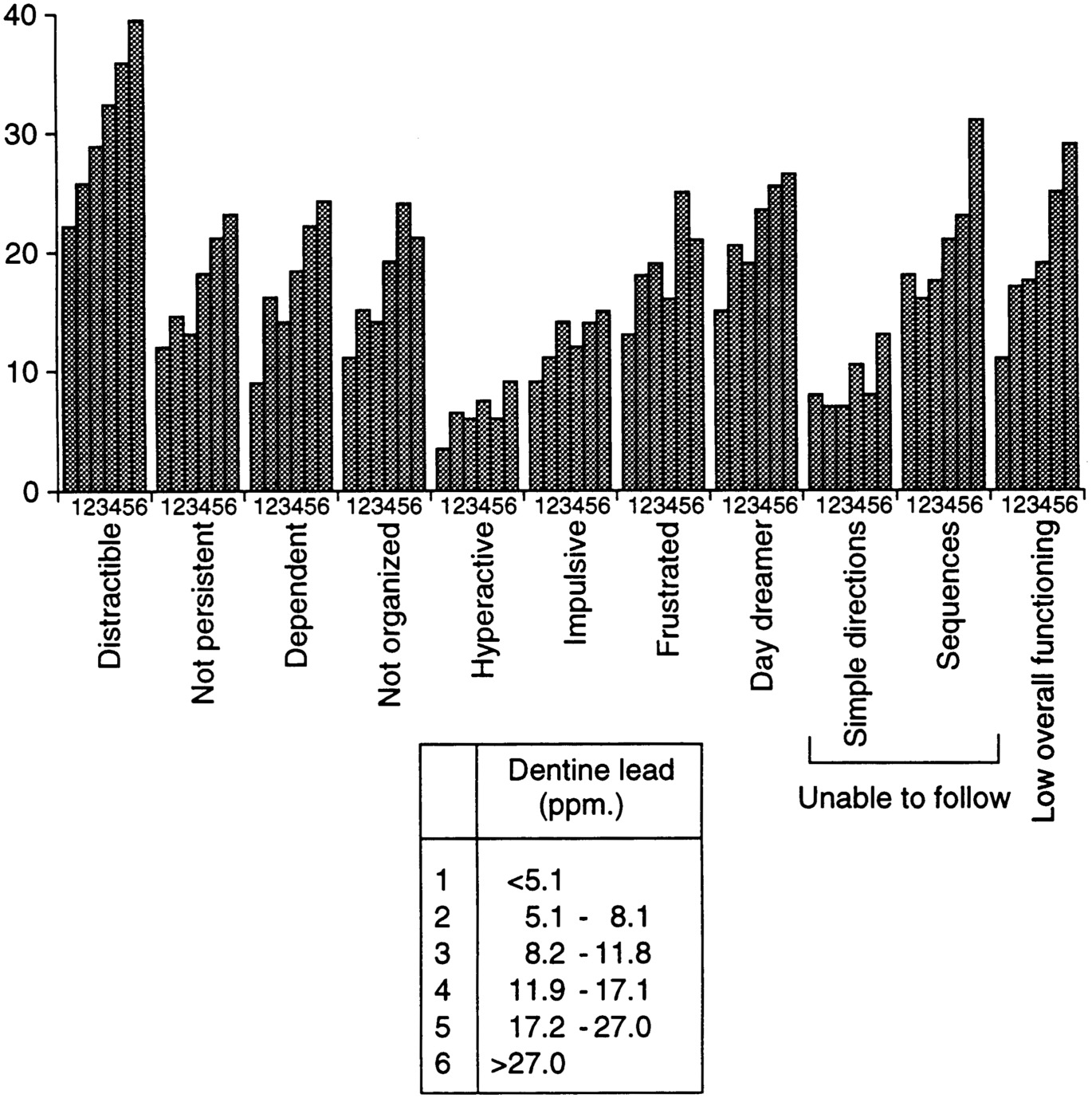
Figure 3-6. Deficits in psychologic and classroom performance of children with elevated dentine lead levels. Source: Reprinted, with permission, from Needleman, H.L., et al. “Deficits in psychologic and classroom performance of children with elevated dentine lead levels,” The New England Journal & Medicine 300(13):689-695. ©1979 by the Massachusetts Medical Society.
Note: The distribution of Negative Ratings by Teachers on 11 Classroom Behaviors is provided in relation to dentine lead concentration. The group boundaries were chosen to obtain symmetrical cell sizes for the median (Groups 1 and 6=6.8 percent; Groups 2 and 5= 17.6 percent; and Groups 3 and 4= 25.6 percent).
neurocognitive tests and unfavorable assessments of learning and behavior by teachers. No “threshold” for these effects was discernible. Basic research on lead toxicity supports these associations, as well as the conclusion that lead neurotoxicity may be largely irreversible.
As shown in Figure 3-7, lead can penetrate inside neurons in the central nervous system (CNS) and, once inside, it cannot be removed even by strong chelators (such as dithiothreitol) in vitro. In the CNS, lead can disrupt neuronal communication and memory storage through actions at several molecular targets: ion regulation by Na-K ATPase and conductance channels; neurotransmitter receptor and transporter binding; intracellular calcium storage and release; and intraneuronal second messenger proteins such as adenyl cyclase and protein kinase C. These effects occur at lead concentrations as low as 1 pM. During development, some of these actions may have persistent if not permanent sequelae, because neurotransmitters play a trophic role in “hardwiring ” the CNS during early perinatal stages. By impeding cell:cell communication at these stages, lead exposure may permanently prevent appropriate development of regional and interregional connectivity. The possibility that lead exposure
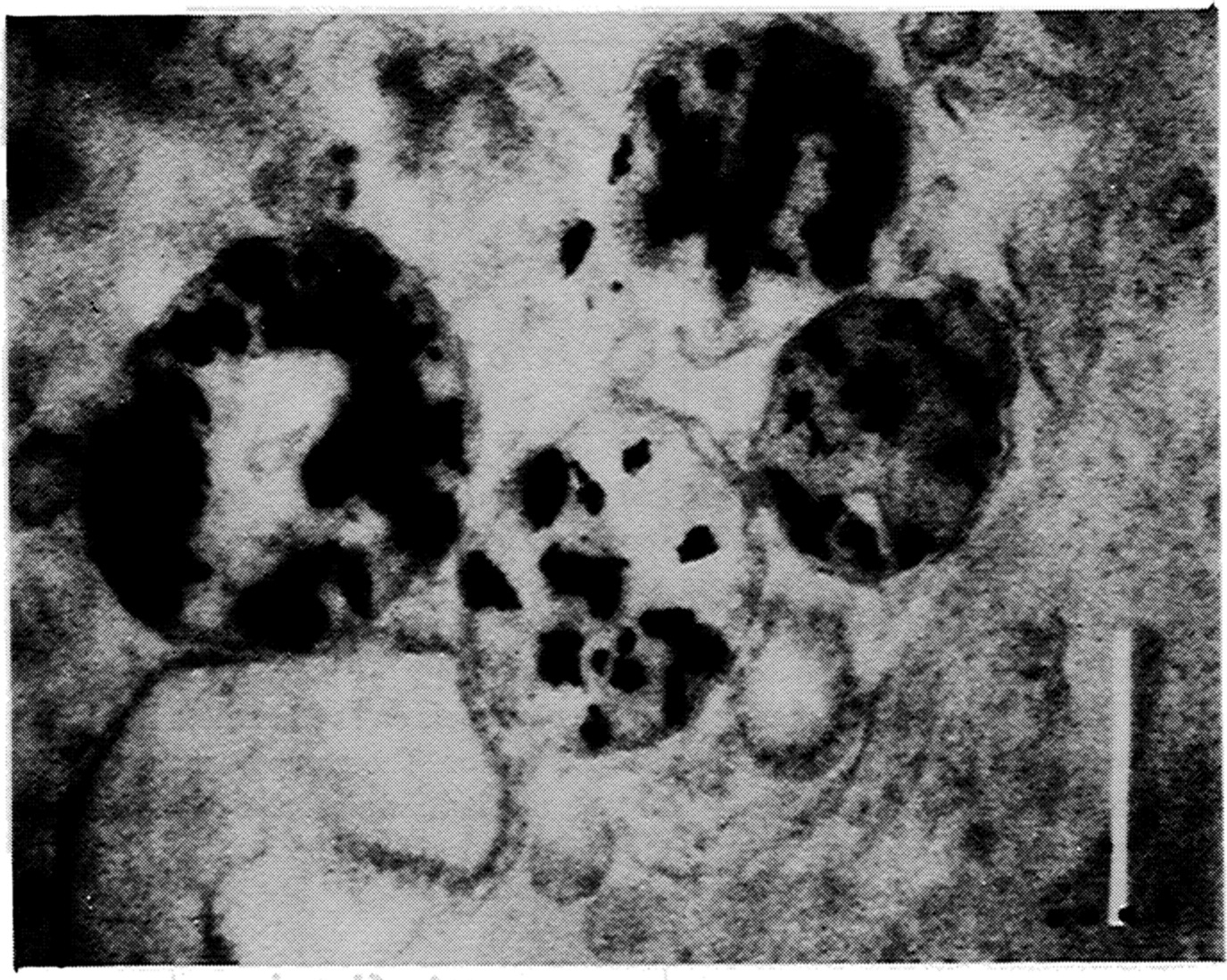
Figure 3-7. Subcellular localization of lead I synaptosomes. Source: Silbergeld, 1992.
during aging may also have neurotoxic effects is only now being studied, specifically in the context of new information on the alterations in lead storage and toxicokinetics that occur during aging and after the menopause in women.
These data demonstrate that in order to fully eradicate lead poisoning, it is necessary to control both ongoing sources of lead into the environment and to evaluate the risks of existing reservoirs from past uses. In addition, understanding the range of lead toxicity is required to develop focused public health programs of surveillance and intervention. Experience demonstrates that the most effective means of lead exposure reduction are bans or substitutions on uses of lead in products such as gasoline, food cans, and paints. The continued prevalence of lead poisoning attests to the need to continue to reduce human exposure.
















