
European Health Care Reform and Primary Care
Jo Ivey Boufford
BACKGROUND
It is common wisdom that very few models of anything used in one country travel well—primarily because most have evolved from different historical and cultural traditions. This is probably true, but in my own experience of the last 3 years in Europe, models from other countries can certainly help you reflect on your own system and perhaps develop new ideas about ways around or through apparent obstacles. I always start these comparisons with a favorite word of caution from Robert Evans, the Canadian health economist, to anyone working in health care: “When you think your health care system has got it right, that's when you're really in trouble.”
With that, it may be useful to start with a brief overview of the U.S. health care system as seen from the macrolevel by a foreign audience.
The predominant characteristic of the U.S. system is its heterogeneity. There is no central planning for facilities, services, or health personnel. There is no uniform central financing of the service delivery function. The U.S. Surgeon General's report of 1979,1Healthy People, did, however, articulate a set of central health promotion and disease prevention goals for the nation.
Health insurance in the United States has tended to be largely an employment-based system, with other programs developed by the federal government to fill in the gaps for special population groups—most notably, Medicare, a federally funded health insurance program for elderly and disabled individuals, and Medicaid, a health insurance program
for certain categories of the poor financed jointly by the federal and state governments, with eligibility levels and benefit packages varying by state.
Health care financing programs have tended to focus on institutional acute care and, more recently, institutional long-term care rather than on community-based services. The result is a delivery system that is badly out of balance (dominated by acute-care hospitals and technology) and very expensive. It is estimated that 30 million to 35 million Americans have no health insurance, and there may be up to 70 million to 75 million with inadequate insurance. Individuals are more likely to be insured for inpatient or emergency care than ambulatory or primary care and are almost never insured for preventive services.
Finally, with over 13 percent of the gross national product going to health care costs, the major U.S. health policy for the past decade has been cost containment. As a result, there is an alphabet soup of financing and organizational models—PROs, DRGs, HMOs, PPOs, and IPAs—aimed at lowering costs and, to some degree, promoting quality control through regulatory frameworks and financial disallowances for unnecessary services. The primary focus of all these efforts has been the reduction of acute-care hospitalization.
Although scores of changes have been proposed to address some of the obvious problems in the U.S. system and some incremental progress is being made, large-scale change still seems very difficult.
The British government, on the other hand, under Margaret Thatcher, was not convinced that it was getting value for its money for health care expenditures that were slightly under 6 percent of the gross domestic product, and in December 1989 it launched a full-scale reform of the National Health Service (NHS), with only marginal new resources added. The goal of the reform was to introduce an internal market to an increasingly decentralized state-managed health care system to increase efficiency and consumer responsiveness.
When complete on April 1, 1994, in a little less than 4 years, government policy changes will have been largely implemented to alter the following:
-
the basis for health service financial allocations for the NHS;
-
the organizational structure and management of hospital and community nursing care;
-
primary care and general practitioner (GP) services to increase incentives for prevention and shift power to GPs who act as fundholders and buy an array of hospital services on behalf of their patients; and
-
the funding and delivery of community care for elderly, mentally ill, and learning-disabled individuals to increase deinstitutionalization and transfer management responsibility from the NHS to local government.
Because a picture is worth a thousand words, the biggest differences between the U.S. and U.K. health systems can be captured by a sequence of three diagrams comparing the “participants” in the U.S. health care system and those in the British system (Figure 1, Figure 2, Figure 3).
Figure 1 shows the basic transaction between a provider (a doctor) and a patient who pays for his or her own care. In the prereform NHS, the state was the dominant provider, with the NHS administered centrally through 14 regions and about 200 districts and with GPs on contract to the government. Patients paid taxes in exchange for universal financial entitlement to services.
Figure 2 shows a postreform NHS in which the government has delegated its purchasing authority to 177 (and this number is decreasing) defined district commissioning agencies that buy services on behalf of the population in a defined geographic area. These services are purchased through contracts with providers who were previously managed by districts but who can now apply for quasi-independent status as NHS “trusts ” and who will compete for contracts.
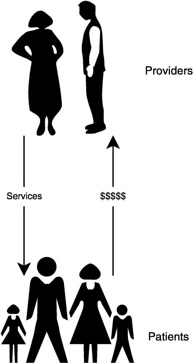
FIGURE 1 Health care financing in the United Kingdom before reform of the National Health Service.

FIGURE 2 Health care financing in the United Kingdom after reform of the National Health Service (NHS).
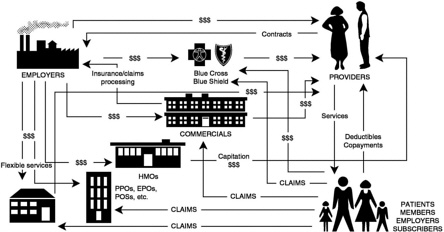
FIGURE 3 Health care financing in the United States. Competition in the U.S. health system is based on cost of administration, cost of care, channeling of patients, access to providers, range of benefits, incentives to providers, cost to patients, and advertising.
Patients are now, in a sense, the beneficiaries of the district-based purchasing agency for acute care and are registered on a list with GPs or GP fundholders for primary care. There is now a single intermediary in the system in the United Kingdom. By contrast, one might characterize the current mature or postmature market in the U.S. system by the images in Figure 3. When you see the different number of players involved, you begin to understand why differences in cost and in the pace of change are possible.
Two additional features of the system in the United Kingdom are worth noting mainly because they were not changed in the reform. They are crucial strengths of their system and crucial weaknesses in ours: universal financial access to health services and the general practice service as a primary care referral system.
A final feature, and perhaps the most radical one, is described in a recent report called Health of the Nation,2 issued in July 1992, which calls for a renewal of the original goal of the NHS, which is to serve as an instrument for improving the health of the entire population, not just the provision of individual patient care.
WHAT IS PRIMARY CARE?
One of the big problems in discussing primary care is defining what it is. Without this it is very difficult to decide who provides it, how to teach it, and ultimately how to strengthen it. Albert and Charney's functional definition,3 which is complemented by that of the Insitute of Medicine,4 covers the key characteristics of a definition. Primary care involves the provision of the following:
-
first-contact care at the patient's point of entry into the health care system;
-
comprehensive care to the patient (including preventive, curative, and rehabilitative care);
-
continuous care, in which the patient has an on-going, personalized relationship with a primary care provider or team for his or her health care;
-
coordinated care, in which the primary care provider serves as the coordinator of all patient care, including hospitalization and necessary referrals to specialists, including mental health specialists, and related health and social services. The primary care provider acts as the patient's advocate to ensure that the care received is appropriate to the patient's needs and that the patient is an informed participant in decision-making about the overall care plan and is educated as to the appropriate use of the health care systems;
-
ensuring access for the patient to needed health services (barriers to access can include operating hours, geography, finances, culture, and language); and
-
ensuring accountability of professional and administrative staff for the quality of services rendered, the ways in which they are provided, and the outcome of care. This involves accountability to internal and external review criteria as well as to the patient.
In revisiting this definition today, one might add the concept of “community-oriented” primary care, with primary care providers assuming some role, if not direct responsibility, for improving the health of the community they serve.5 When trying to develop health policy mechanisms to support primary care service delivery and education, it is important that definition be clear so you can test the models you are developing.
HOW IMPORTANT IS PRIMARY CARE?
Primary care is very important. My favorite example is shown in an often-quoted study conducted in the 1960s by Kerr White.6 In a classic paper in which he used data from the “Survey of Sickness in England and Wales” and the U.S. National Health Survey, he analyzed the sickness behaviors of 1,000 adults over 16 years of age during 1 month. He found that of these 1,000 adults, 750 experienced some health complaint, of which 250 sought medical attention; 9 of these were admitted to a community hospital, 5 were referred to another physician, and 1 was admitted to a teaching hospital. Applying these findings to our evaluation of the relative role of the components of health services, we realize that the hospital, clearly the focal point of the traditional delivery system and medical education system, is actually needed by less than 4 percent of individuals who enter the formal health care system. Most are treated in an ambulatory-care or primary care setting. A similar review in 1983 showed even less initial use of the physician and, once the patient enters the service system, less use of the hospital, a trend that is likely to continue.
WHAT'S SO DIFFERENT ABOUT PRIMARY CARE?
What key issue distinguishes primary care from the traditional dominant and, by virtually all external criteria, outstanding U.S. system for acute-care service delivery and medical education? Why are so many different structural, financial and educational models needed? A few of the examples presented may provide a sense of the enormous differences that must be addressed.
Given the differences outlined in Table 1, what kind of progress has been made in the United States to date in supporting the development of primary care service delivery and education, and what are some of the key issues remaining on which the British experience might shed some light?
PRIMARY CARE: THE U.S. EXPERIENCE
In many ways my professional career mirrors the recent era of primary care development in the United States, and because we now may be moving, however tentatively, beyond the “demonstration program” or “special project” phase of primary care education and service, it is important to reflect on the history of such efforts so that we do not find ourselves yet again “rediscovering” primary care a decade from now .
While my experience is largely in New York City, the principles apply more broadly; the examples of what has been done there are not unique but exist, and are sometimes better developed, all over the country.
In many ways I “grew up” professionally in primary care in innercity New York. I arrived from Michigan as a pediatric resident in the Social Medicine Program at Montefiore Hospital in the Bronx in 1971. It was the end of the golden age of the federal community health center movement, in which interdisciplinary teams of doctors, nurses, and community health workers with legal aid, social, and mental health services worked out of a neighborhood health center to serve a geographically defined community. I received much of my training in one of these centers, which was affiliated with a teaching hospital. There were several such models in New York City. These were based on a program run by George Silver in New York City in the 1950s and models in New York in the 1930s described by George Rosen.7,8
In the 1970s and 1980s, this system, largely designed for the poor, grew to a network of nearly 800 primary care centers throughout the country. Considerable research on their effectiveness showed them to be models for comprehensive continuing care: accessible geographically and by time, and capable of lowering rates of hospitalization and emergency room use, and state Medicaid bills. Much of the richness of the multiservice center concept was lost with the cost-containment pressures of the 1970s, but it is still a vital network and is now being targeted for reinvestment. During this same period the HMO movement was being launched as a primary care model for working people.
The mid- to late 1970s also saw the initial federal investment in innovative models for primary care undergraduate and graduate medical education in general internal medicine, general pediatrics, and family prac-
TABLE 1 Major Differences Between an Acute-Care Hospital and Primary Care
|
Acute Care |
Primary Care |
|
1. Site and pace of work: |
|
|
Hospital-based ward medicine is major use of time; patients are seen intensively for short periods of time |
Outpatient setting is a major focus; patients are seen intermittently over long periods of time |
|
2. Goals: |
|
|
Disease-centered problem-solving, disease classification, and death prevention |
Disease prevention; problem mangement; reduction of discomfort, dissatisfaction, and worry; health promotion |
|
3. Role models: |
|
|
Faculty “stars” in clinical research and high-prestige areas of surgery, and subspecialty medicine |
Primary care physician in pediatrics, general internal medicine, family practice (not always on the faculty, therefore low prestige in medical school) |
|
4. Knowledge and skills: |
|
|
Knowledge, skills, technology in medical “science” are the intervention central focus of training |
Knowledge and skills in general medicine; psychosocial and problem management are central |
|
5. Diagnosis and treatment: |
|
|
Inpatient diagnosis is deterministic and treatment is controlled and closely observed |
Ambulatory diagnosis relies on probability derived from clinical experience and epidemiology. Treatment is frequently a “clinical trial,” with many unknown variables |
|
6. Doctor–patient relationship: |
|
|
Hospital relationship is time limited, and the ward ritual assures a “safe” distance between doctor and patient |
Relationship between doctor and patient is one-to-one, continuous, close, and extended over time |
|
The doctor is in total control of the enviroment (e.g., medicine taking, information giving, degree of patient contact with family) while the patient is in hospital |
Doctor has little control over patient's environment; must deal with patient in a complex social network |
|
An assumption is made that any doctor can be replaced by any other at any time provided that he or she has similar skills and experience (e.g., ward rotations) |
The nature of care creates one-to-one relationships; the individual healing abilities of the doctor are critical |
|
Physicians are specialists but are rarely in a position to be criticized since they are solving “problem cases” referred by other physicians |
Physicians are first-in-line contacts by the nature of the referral system and are also in a position to be criticized by specialists |
|
The patient is acutely ill and totally dependent on physician |
Ambulatory patients are “functioning” at some level; are more self-reliant; may not comply with treatment regimen; and are subject to outside influences |
|
Gratification is immediate: that is, patient survives a cardiac arrest; an acute infection is cured; or a surgical problem is treated |
Gratification is often delayed: chronic disease with long-term management, psychosocial problems with ambiguous outcomes |
|
Major need is in scientific technology, so the doctor is the key figure, a solo performer who autonomously manages medical problems |
Because of the complex nature of the medical problems, the doctor works on a team and makes decisions collaboratively |
tice as part of the Health Professions Educational Assistance Act. Since that time, thousands of primary care residents have graduated from many such programs throughout the country, and many are now in leadership roles in major health care institutions.
The National Health Service Corps is another program of that era. It provided mechanisms for financially supporting young doctors and other health professionals to work in medically underserved communities. Also cut deeply during the 1980s, the corps is receiving renewed attention.
In the early 1980s, as president of New York City's Health and Hospitals Corporation, I assembled a team charged with putting primary care on the corporation's agenda. Ironically, this often meant rebuilding and expanding health care centers and programs that had existed in the 1970s but that had been dismantled during the city's fiscal crisis. It also meant that the city had to assume financial responsibility for investment in capital and staffing costs, because there was no other source of financial support due to the inadequacy of outpatient reimbursement and the number of uninsured patients.
Between 1986 and 1989 eight new primary care and community mental health centers were opened and a new series of hospital-linked pri-
mary care networks were established around most hospitals that were a part of the Health and Hospitals Corporation. Other academic medical centers around the country were doing the same thing. Some provided community services and some provided good marketing mechanisms to ensure full beds.
I have seen some enormous successes and some frustrating loss of ground over the last 15 years. What have we learned from these experiences?
-
U.S. health professionals know how to set up excellent primary care models that can deliver comprehensive services to a defined community. These include the following: group practices, hospital-based primary care services, neighborhood health centers, primary care networks linked to hospitals, physician homesteading, and managed-care programs of all kinds. They have all been tried, and those that have received sufficient resources (human and financial) over a sufficiently long period have succeeded in delivering quality care, reducing hospitalization, and providing effective services to some of the most medically deprived communities in the country as well as to groups with private insurance.
-
We know how to train residents and medical students in primary care settings both in a hospital base and in the community. Since the mid-1970s, graduates of primary care residency programs in general internal medicine and general pediatrics with significantly more primary care and ambulatory-care experience and often with significantly less inhospital experience than their traditional counterparts have performed well on their board exams and as clinicians and faculty in teaching hospitals, medical schools, and the community. Family practice residents are trained in excellent primary care “teaching health centers” and have been increasingly important primary care service providers all over the country. Similar teaching models have been developed in HMOs and large group practices.
-
We know that the primary care service and training programs that work are all long-term partnerships. These partnerships are between the primary care systems, the community served, and in urban or isolated rural settings especially, a backup hospital or medical center that can offer specialty support for clinical care and academic continuing education support, including academic appointments for physicians and nursing staff. It has been hard to sustain such partnerships because of the historical priorities of medical education and tertiary-care hospitals.
-
We know that primary care programs are a financial liability because of the lack of health insurance for large segments of the population in need, inadequate financing of primary care services relative to their cost—especially when provided by individual primary care physicians —
-
the expense of capital infrastructure for primary care in urban environments, and inadequate financing of graduate medical education in primary care settings. Those institutions with a commitment to such efforts have subsidized them directly or have lived off grants and special program funds for years, trying to fill the gaps and keep the programs running. Some states are beginning to develop financing mechanisms within existing public insurance frameworks to address these issues.
Some of the most talented and committed primary care experts in service and education in the world are in the United States and, interestingly, are very involved as consulting experts in health reform projects in Western, Eastern and Central Europe, and the former Soviet Union. All of these countries see a strong primary care system as the foundation on which to build reformed health care delivery systems. To achieve this in the United States we need mechanisms to ensure that the kind of ongoing financial support enjoyed by hospital-based secondary-and tertiary-care services and graduate medical education in past years is extended to community-based primary care. Service and education efforts must be institutionalized as part of “the way we do business ” if things are to really change.
REFLECTIONS FROM THE BRITISH EXPERIENCE
So what are a few of the key issues important to strengthening primary care in the United States and how could the British experience help us think about them differently? I have selected four issues for special focus.
-
There is a lack of consensus on a single universal paradigm for primarycare.
This was the major problem cited in the final report of a recent National Primary Care Conference sponsored by the Health Resources and Services Administration.9 The definition of primary care I cited earlier would probably satisfy most people as to what it is. The real issue is who provides it? This is especially an issue in the United States, because on the answer rests the issue of who gets paid and how much.
The nominees for primary care providers are family practitioners, general internists, general pediatricians, or specialists. In the United States, a debate for funding educational programs has been resolved by the very useful federal definition that distinguishes general internal medicine and general pediatric graduate medical education programs from those traditional internal medicine and pediatric programs that most often lead to specialty training and practice. Family practice was accepted as a primary care specialty without debate.
An ongoing debate on the role of specialists in providing primary care, especially in the face of the diminishing number of medical school graduates entering these primary care specialties, is best captured by Gordon Moore of Harvard in his review article “The Case of the Disappearing Generalists.”10 He examines the arguments for just letting the specialists do primary care because we do not seem to be able to attract students to it, and there are already more than enough specialists and they do primary care anyway. His analysis of the data on the quality and adequacy of comparative practice seems to favor the argument for the primary care physician, but he does raise the need for strengthening training and practice in primary care to realize its full potential.
This debate is a nonissue in most European countries and certainly in the United Kingdom, where there is very clear differentiation between specialists, who are hospital based, and GPs, who are community based. In actual fact, many specialists have office-based private practices, and GPs in some parts of the United Kingdom do follow patients into the hospital. The key to the distinction, however, is the clarity of the so-called referral system (a less pejorative and economically driven label than the often used term gatekeeper).
GPs are the first-contact doctor provider, and patients get to specialists and hospitals only through referrals. GPs also control access to most of the social welfare benefits of society, for example, disability and sickness funds.
This distinction has an interesting history in the United Kingdom, as recounted by Rosemary Stevens.11 In 1518, the Royal College of Physicians was established to regulate medical practice within 7 miles of London. The “physicians” were the elite, served royalty, and were rich. Surgeons and apothecaries were restricted to practicing outside urban areas. In the 1700s, a hospital system started; physicians made all the decisions, but the surgeons and apothecaries did the work. Bed control in the more established hospitals was restricted to physicians, so surgeons and medical specialists (eye, ear, and other) began to set up their own hospitals and increasingly began to see outpatients. As the size of the middle class increased and demand soared, surgeons and apothecaries also started seeing outpatients and keen competition led to an agreement. The Medical Practice Law of 1858 determined that the physician and surgeon consultant specialists “got the hospital” and the apothecaries, who later became GPs, “got the patient.” With the 1915 National Insurance System, the GP list began, and shortly after that, hospital doctors became salaried.
The burgeoning number of GPs was not a threat to specialists because they were mutually dependent for referrals. In the current reform, the creation of GP fundholders has strengthened this interdependence through their increased purchasing power.
In Canada in the 1970s, the Royal College of Physicians and Surgeons decreed that specialists function as consultants and designated family practitioners as responsible for primary care. This was further reflected in the payment system under which consultants were paid less for “non-referred” patients.
A further issue in defining the “who” in primary care is that of nondoctors. By the earlier criteria for primary care, nondoctors, especially nurses, can do significant amounts of primary care. Expanded roles for nonphysicians such as nurse practitioners (NPs) and physician's assistants (PAs) are much more developed in the United States, but there is a lively debate over the scope of practice and payment. By contrast, in the United Kingdom there is a much more extensive service infrastructure in community nursing and allied health linked to acute and primary care. More recently, practice nurses and other health professionals can be hired by GPs and included in the practice allowance. Because all are salaried through the NHS, there is no competition for financing. There is some difficulty in coordination, but the general focus is on patient needs and how to develop the teams to meet them.
In the United States, the simplest mechanism that could be used to start developing a primary care sector would be to designate recognized primary care providers, including nondoctors. They would be eligible for enhanced payment for primary care, and one would need to create financial disincentives for specialists who do the same work. Because of pluralistic financing, we may need a uniform definition of service to do this, and all providers would be paid the same. Current payment systems, including RBRVS, still seem to be procedure rather than transaction oriented. Finally, we may not be ready to develop a full referral system, but clearly, HMOs and other managed care approaches provide the beginnings of the model. If managed competition seems a favored approach, there are real opportunities to reinforce the role of primary care.
-
There is a need for medical education and personnel planning for primary care.
As noted earlier, the United States has no central planning system for health personnel. There is some self-regulation by specialists, who limit the numbers of residency slots they will approve, but this has most often been market driven. Generally, medical students are free to select their specialty, and hospitals or academic medical centers can train the numbers and types of students they wish, subject to quality review. The subsequent location of a new specialist's practice is similarly open.
In the 1970s, there was a national awareness of medical specialty and geographic distribution problems, and it was decided that a market approach would be taken: double the number of medical school graduates and they would “trickle down” into the needed specialties and locations.
This theory worked about as well as trickle-down economics, and there are still major problems of excess specialists; more than 70 percent of U.S. graduates in the recent National Resident Matching Program chose non-primary care specialties, and 64 percent of practicing physicians identify themselves as specialists. Persistent geographic maldistribution led to a recent Fortune magazine article describing “a national physician shortage” and blaming the protectionist attitudes of physicians for the maldistributions. 12
Although financial incentives for practice are obviously a problem (and one we have not been prepared to address), we have tended to believe that an educational strategy might work: the proper experiences in primary care during medical school would increase the numbers of primary care physicians.
In his classic study of medical school graduates between 1958 and 1976, D. Funkenstein concluded that the greatest influences on career choice were economic incentives and ideology (the social value of the time). The reason for the upsurge in primary care in the 1970s was, he believed, a perceived excess of specialists and federal government interest and investment in primary care.13
Another body of research shows the clear influence of new primary care medical schools and special programs geared toward primary care on proportionately increasing the percentage of graduates selecting and remaining in primary care fields. Special graduate medical education programs in primary care have even more compelling results.
Although federal investment has been a critical incentive, it has been variable and most medical institutions have not picked it up as part of their mainstream funding. There is also confusion between giving students more ambulatory-care experiences—in emergency rooms and specialty outpatient clinics—and primary care experiences that meet the definitional criteria outlined above.
Interestingly, in the United Kingdom, where over 60 percent of physicians are GPs, undergraduate medical education is, by U.S. standards, rather traditional and rarely involves out-of-hospital experiences. Graduate medical education (GME) is even more hospital biased, and GP specialty certification began only in 1982. Clearly, the major influence on specialty distribution and geographic practice in the United Kingdom and other European countries is national or regional systems of personnel control.
For specialists in the United Kingdom, the central Department of Health controls financing of all training funds (GME positions). They are allocated to regions in line with the number of consulting posts that will be needed. Previously, the districts—and now the new trusts—bid to regions for posts. An advisory committee (the Joint Consultants Commit-
tee), with membership from the British Medical Association, the Royal Colleges, and Department of Health officials, act on applications, shaping the system but not planning the distributions or numbers of specialists. Occasional problem areas where requests are not properly balanced lead to intervention.
For British GPs, there is a national system through the Medical Practice Committees in which agreed population and practice size limits are used as benchmarks for self-regulation of practice location, which is monitored by the Department of Health.
In Canada, with about 50 percent family practitioners, provincial governments fund the majority of GME positions and influence the mix of the numbers and types of GME positions offered. New York State recently began a policy of “up-weighting” primary care residencies under a state methodology for funding the indirect costs of GME. Using the federal definitions, residency positions in general internal medicine, general pediatrics, and family practice received a weight of 1.5 and the others received a weight of 1. The plan next year is to phase out support for fellowships and weight all non-primary care residency slots at 0.9.
The specialty choice and the geographic distribution of doctors are areas in which years of effort at self-regulation have failed. It is time to revisit national or state physician personnel planning or “shaping” mechanisms. Medical education is a necessary, but not sufficient, strategy for achieving the goals of primary care development.
-
A third issue is the increasing voice of the patient and the public and their roles in relation to those of health professionals and for those managing the health care system.
In the United States, we have always had high patient demand and high expectations, and in a litigious environment, the response has been, “when in doubt, treat” (with the patient often referred to the specialist).
In the United Kingdom, patients have historically been relatively passive and reliant on the doctor's advice and have lower expectations from the system because of an acceptance of resource limitations. The tendency has been, “when in doubt, do not treat.”
With the introduction of the internal market in the British reforms, patients are becoming more engaged, sometimes around more superficial amenities, which is the first tendency in the market, but again, the reform has set a framework for citizen involvement and performance standards for guiding expectations for all public services. For the NHS, this is called the Patient's Charter. It lays out service expectations on waiting times that would not be particular advances for U.S. health consumers, but direct patient access to one's medical chart is certainly one of the more radical changes included. The point is that there is a national effort to raise the level of citizen involvement.
Purchasing authorities are also charged with implementing ambitious goals for public participation in making choices about how money should be spent. As patients become increasingly well informed, they begin to ask substantive questions about the effectiveness of procedures and the quality of doctors and hospitals. This is obviously a long-term process, but the approach is an interesting example of a large-scale policy initiative to involve and empower individual citizens to hold doctors accountable for their one-to-one care and to hold purchasers accountable for decisions on resource use for the larger community.
It seems very different in style from U.S. proposals to set up yet another third-party entity like Health Insurance Purchasing Cooperatives to represent the aggregate of patients in the financial transaction. The U.S. Public Health Service's Healthy Community initiative uses more of a community development approach to citizen activation around health issues in general.
An obvious issue is the distinction between a public health care system like that in the United Kingdom, which is by its nature accountable if the level of public awareness is raised, and mixed or predominantly private systems like those in the United States, which may need “organizational forces” to have an effect. It does raise the question in the United States about the proper role for government as an advocate or proxy for the citizen or the patient in a system in which public funds are already paying in excess of 50 percent of health care costs.
-
The final issue to be analyzed is the question of a vision for what a healthservice could be.
Again, from across the Atlantic, the only vision that seems to be articulated for the U.S. health care system is that it must provide everything to those who can pay and it must cost less.
One British observer marvels at U.S. information systems, utilization review techniques, and protocols for care, but sees these as tools for the micromanagement of processes that are used to compensate for the failure to “macromanage” the system by a global budget mechanism or a clear policy framework.
The initial vision for the NHS was to guarantee universal financial access and distribute the available health care resources as equitably as possible. As such, and especially in the post-Thatcher era, the NHS has enormous symbolic value as one of the few, if not the only, remaining public service that is available to all citizens regardless of their income and that is publicly accountable to them for its performance.
This is seen by policy analysts to be a critical feature of most well-supported state welfare programs: the extent to which the middle class benefits from it.
This reality is now appearing in the United States. As increasing numbers of middle-class citizens are beginning to be affected by the costs of health care and problems in health care delivery systems, there are increasingly serious demands for change and increasing activity by politicians in response.
Responding to cost control in a zero-sum game by definition means taking something away, imposing limitations, and loss. Reactions to these negatives lead to entrenched institutional or public resistance.
Alternatively, the development of a vision of what the health care delivery system is supposed to do can at least provide a framework for tough decisions taken toward a purpose.
The postreform NHS has revitalized an additional feature of the initial vision for it, that it should be an instrument for improving the population's health, which is a responsibility that goes beyond caring for and curing the individual patient.
There is considerable debate about the appropriateness of such a goal in the United Kingdom. Some see it as a cynical attempt to deflect attention from the problems of a health service that is underfunded for its current responsibilities; others see it as unrealistic because health care exerts only a small influence on overall health. But it has become a framework for a series of policy decisions that have shaped the reforms and is giving health services managers a clearer sense of direction.
Figure 4 represents a way of thinking about improving a population's health. It identifies the types of interventions needed to promote a community's health; the potential targets of the intervention, individuals, the community, or institutions; and the impacts of these interventions, the continuum from illness to health. Institutional and individual purchasers and providers can act at each of these levels if they are aware of that potential and if they are provided with the proper incentives—financial, regulatory, or political—to do so.
If we provide only traditional clinical medical care, even if we ensure the effectiveness of each intervention, we limit our ability to significantly influence the health of the larger community, although we may save enormous amounts of resources.
If we can begin to unlock the financing of primary care and the use of primary care practices as a base for health promotion and disease prevention as well as treatment, then we can reach out into the larger community and take better advantage of the power of the health care system as a broader instrument for improving community health.
U.K. government health policy reinforces this vision by further strengthening the historically strong role of primary care in reform. Part of the reason for doing this is very pragmatic. With limited resources, the government needs the GP to minimize unnecessary use of services (only
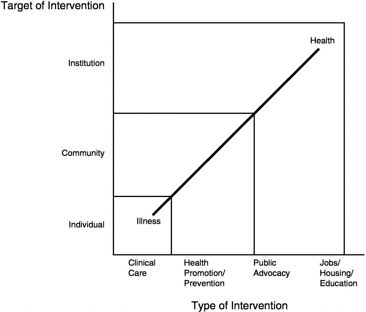
FIGURE 4 This diagram represents a way of thinking about improving a population 's health. It identifies the types of interventions needed, the potential targets of the interventions, and their impacts—the continuum from illness to health. Institutional and individual purchasers and providers can act at each of these levels, if they are aware of that potential and are provided with the proper incentives—financial, regulatory, or political—to do so.
about 1/10th of all visits to a GP result in a referral for speciality care). But elements of the importance vested in primary care have been in the system for some time.
Overall physician income scales in the United Kingdom in 1990–1991 show an estimated net income of £42,000 (about US$65,000) for GPs and £45,000 (about US$70,000) for specialists without merit awards, although two-thirds of consultants eventually receive merit awards and this disparity is under negotiation in the new GP contract.14
When the number of GPs was declining in the 1960s, a new Family Doctor Charter was written to change the basic financing of general practice and address premises costs, staffing costs, and targeting incentives for night calls and home care. The recent reforms have added incentives for prevention activities, and the GP fundholder initiative shifts even more power into the hands of certain GPs so that they can purchase an array of services for their patients. Once primary services can be adequately financed, the next challenge is bringing the services provided
more in line with the health needs of the community rather than with pure market demands. In a resource-restricted environment, we must achieve the closest match possible and perhaps make some hard choices.
The experiment with health care rationing in Oregon, with all of its flaws, has caught the imagination of health policy leaders throughout Europe because they understand financial limitations and see it as an effort to involve the public in an open debate about what the health care system should do. However, the real challenge for the future is the need to provide incentives for health service providers to use their institutional resources and influence to improve community health in its broadest sense and to help the community to think more carefully about issues related to the allocation of scarce resources.
In the United Kingdom, the Secretary of State for Health is charged with working with other government ministries to assess the health impacts of various policies for education, housing, environment, and trade. An example of a volatile issue now facing the minister is whether to permit tobacco advertising.
A number of U.S. providers have seen that it is in their self-interest to take on more of a responsibility for the health of the people in the communities they serve. With a new administration, there is an opportunity for a new vision. A statement explaining the goals for health services in the United States could provide a framework within which states, insurers, and providers could shape their behaviors to be consistent with the policies of the national leadership and facilitate the process and a mechanism to monitor it.
Even if a vision that sought to address the health needs of the community could be developed, it would still be a challenge to implement such a vision. Such changes confront long-standing vested interests in the health care delivery system. Often these interests involve medical politics within powerful institutions or organized medicine. For example, a community health needs assessment that demonstrates a greater need for maternal child services, perhaps at the expense of specialty surgery, places the decisionmaker squarely at odds with traditional interests and ways of doing things.
Another problem is that primary care and other efforts to achieve improved community health are interdisciplinary undertakings. They require collaboration across professional disciplines (medicine, nursing, social services, etc.), across sectors (acute, primary, and community care), and across units of government and within the public. It is hard to work at interfaces; it is lonely and there are few rewards. Traditional treatment and care services are a little neater; they would be more effective if there was more collaboration, but the patient can still get the services from a series of relatively independent sources.
Leadership for primary care and community health improvement is about building systems of care, not institutions. This is perhaps the most difficult and threatening step of all. The necessary interdependence, fluid boundaries between levels of care, and collaborative focus on patient and community needs—rather than control and institutional survival—are very difficult to realize.
Finally, there is a more acute risk for the public-sector policymaker and manager: running out of time. Politicians' attention spans tend to run in electoral cycles, usually of 2 to 4 years. It is very hard to make fundamental institutional changes in such a time frame, especially in the face of resistance and constrained resources. The advice one often gets is not to do any strategic thinking or acting.
Health systems change will be one of the major challenges to the Clinton Administration, but the time is never better than at the beginning. Eli Ginsberg's recent article in the New England Journal of Medicine indicates that we have little choice because we cannot sustain the costs of our current health care system to the end of the century. 15
CONCLUSION
Finally, I have a few reflections on the feasibility of this task when viewed from the perspective of another country. First, viewing the U.S. system from the European perspective, in sharp contrast to the other systems in the world, health care in the United States is not seen as a public service or right of citizenship. It is profoundly embarrassing that the United States spends 30 to 50 percent more on health care than any other country in the world but cannot assure access to health care for all of its citizens.
This is not a money issue, it is a values issue, because costs keep going up as we delay. If there was, in fact, a developing consensus that all U.S. citizens should have access to health care, then that would become a linchpin in a new vision for health care delivery systems of the future, and a key element in ensuring the appropriate use of services will be effective primary care development.
Second, no matter how difficult the financial situation, the United States has enormous resources in its health care system that are unheard of in other countries. The issues are how we use them and, as always, our will to make changes. Institutions must sometimes reinvent themselves. A sense of history can be important in that effort. St. Bartholomew's Hospital in the United Kingdom was founded in the tenth century and was potentially hard hit by the recent NHS reforms, which will cause its traditional referral base for tertiary care to shrink dramatically. Although most are fighting the change, one consultant physician said thoughtfully,
“Well, you know we've only been a tertiary care hospital for the last 30 to 40 years; maybe we should consider what we need to be for the future.” There must be a vision of the future in the United States to make health care change easier rather than a reflex “digging in of heels” to resist the loss of something we have had.
Finally, the energy and action orientation of Americans is incredibly unique. Many other countries struggling to make changes in their health care systems know what they want to achieve, but they do not have the managerial or organizational skills or resources required to make those changes. We do, if we have the will and the vision. That is one of our gifts as a people. We must use this gift to begin and sustain a process of change that can ensure the best health care delivery system and the best health for all of our citizens.
REFERENCES
1. U.S. Public Health Service, Surgeon General of the United States. 1979. Healthy People. Washington, DC: U.S. Government Printing Office.
2. Alpert, J., and Charney E. 1973. The Education of Physicians for Primary Care. DHEW Pub. No. (HRA), 74-3113. Washington, DC: U.S. Department of Health, Education, and Welfare.
3. Secretary of State for Health. 1992. The Health of the Nation. London: Her Majesty's Stationery Office.
4. Institute of Medicine. 1978. A Manpower Policy for Primary Health Care. Washington, DC: National Academy of Sciences.
5. Nutting, P. 1987. Community-Oriented Primary Care: From Principles to Practice. Washington, DC: U.S. Department of Health and Human Services.
6. White, K., Williams, T.F., and Greenberg, B.G.. 1961. The ecology of medical care. New England Medical Journal 265:885–892.
7. Silver, G. 1974. Family Medical Care: A Design for Health Maintenance. Cambridge, MA: Ballinger.
8. Rosen, G. 1949. A History of Public Health. New York: MD Publications.
9. The National Primary Care Conference. 1992. The National Primary Care Conference Executive Summary. Washington, DC: U.S. Department of Health and Human Services.
10. Moore, G. 1992. The case of the disappearing generalist. Milbank Quarterly 70(2): 361–379.
11. Stevens, R. 1966. Medical Practice in Modern England. New Haven, CT: Yale University Press.
12. Tully, S. 1992. America's painful doctor shortage. Fortune 16:68–72.
13. Funkenstein, D. 1978. Medical Students, Medical Schools and Society During Five Eras: Factors Affecting Career Choices of Physicians 1958–1976. Cambridge, MA: Ballinger.
14. Bowles, R. 1992. Understanding the pay structure of GPs. Primary Health Care Management 2(12):2–5.
15. Ginsburg, E. 1992. Health care reform—where are we and where should we be going? New England Journal of Medicine 327(18):1310–1312.





















