
Information for Women About the Safety of Silicone Breast Implants
A REPORT OF A STUDY BY THE INSTITUTE OF MEDICINE
More than 1.5 million American women currently have silicone breast implants.
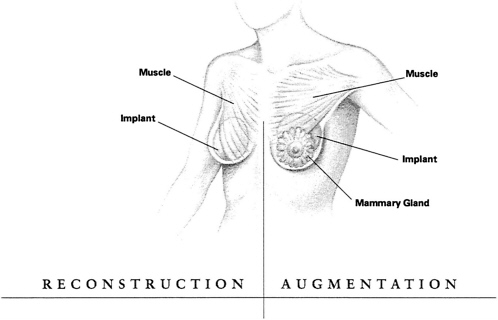
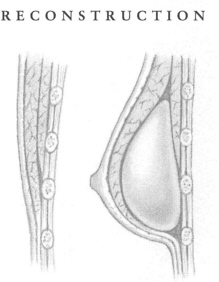
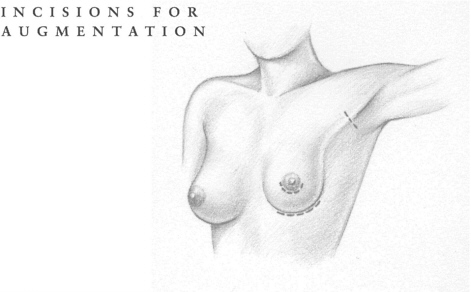
More than two-thirds of these women received implants because they wanted to improve their appearance by changing the size or shape of their breasts, a process called “augmentation.” This number is not surprising, since a 1998 study showed 34% of American women were dissatisfied with their breasts. Most of the remaining women in the implant group had a very different reason for considering implants: They had lost one or sometimes both breasts to mastectomy, an operation for breast cancer that removes the breast. The breast is then “reconstructed ” by the insertion of an implant.
Some women who are, or feel they are, at high risk for breast cancer have had prophylactic mastectomies to remove their breasts, followed by reconstruction with implants. Other women opted for reconstruction after noncancerous but troublesome breast problems.
Implants today are soft sacs, usually inflated with a saline, or saltwater, solution. The implant has a shell made of silicone, a rubber-like substance that the body tolerates comparatively well.
Until the 1990s, most implants contained a synthetic silicone gel that often had a more pleasing feel and look than today's saline-filled implants. But this same silicone gel has caused controversy because of fears that it produces ill effects in women receiving breast implants.
As many as two-thirds of women say they are very satisfied with their implants, even those who experienced postoperative problems. For some women with breast implants, the psychological benefits of the procedure may outweigh such problems.
But other women have experienced upsetting complications that require surgery or even removal of the implant, such as:
-
implant rupture, which can cause the silicone gel to leak out into neighboring tissue and even into other parts of the body;
-
capsular contracture, an often painful distortion and shrinkage of fibrous tissue surrounding the implant;
-
saline-filled implants that deflate, spilling the harmless solution into the body; or
-
pain, from many causes, including postoperative muscular spasms and severe capsular contracture.
Some women have claimed even more potentially serious problems, alleging that the silicone in implants, particularly the silicone gel inside the implant sac, can cause connective tissue or other autoimmune diseases such as rheumatoid arthritis and lupus, neurological disorders, cancer, and even new silicone-related diseases. As a result of this belief, many lawsuits were filed against implant manufacturers by women claiming they were harmed by silicone breast implants.
Silicone: What Is It?
Silicone is derived from silicon, a semimetallic or metal-like element that in nature combines with oxygen to form silicon dioxide, or silica. Beach sand, crystals, and quartz are silica. In fact, silica is the most common substance on earth.
Silicon can be produced by heating silica with carbon at a high temperature. Further processing can convert the silicon into a long chemical chain, or polymer, called silicone—which can be a liquid, a gel, or a rubbery substance.
Various silicones are used in lubricants and oils, as well as in silicone rubber. Silicone can be found in many common household items, such as polishes, suntan and hand lotion, antiperspirants, soaps, processed foods, waterproof coatings, and chewing gum. Because silicone is relatively compatible with human tissue, it has been used in many types of implants, including those for the breast.
Several processes have been used in treating and making ready silicone for implants. The most common product of these processes is platinum-cured gel or liquid rubber, which was used in early implants. Other processes prepare the silicone for use in implants; however, all of these procedures require a final oven bake to ensure their purity and stability.
Noncrystalline silica is amorphous (shapeless) and is less toxic than the crystalline form. Amorphous silica powder is used in most silicone shells (elastomers). Although concerns have been raised that the silica in these shells can travel to breast tissue, experimental studies have not found amorphous silica in tissues near implants. Another worry voiced is that the amorphous silica could convert to sand (crystalline silica) within the body, but this is a chemical impossibility. No crystalline silica has been found in women with implants.
HOW THIS STUDY CAME ABOUT
Until 1976, when the “Medical Devices” law was passed, there was no federal regulation of implants. Although the 1976 law gave the Food and Drug Administration (FDA) jurisdiction over such devices, breast implants were “grandfathered,” meaning that manufacturers were not required to provide the FDA with scientific evidence of product safety unless questions arose about the safety and effectiveness of these already marketed devices.
Questions did arise about implants. In 1988, the FDA categorized silicone breast implants as requiring stringent safety and effectiveness standards and later required premarket approval applications from manufacturers. On April 10, 1991, the FDA issued a regulation requiring manufacturers of silicone-gel-filled implants to submit information on their safety and effectiveness in order for the devices to continue to be marketed. In 1992, the FDA banned most uses of silicone-filled implants because the manufacturers had not proved their safety. In 1993, the agency notified saline implant manufacturers that they, too, must submit safety and effectiveness data, although these implants were allowed to stay on the market.
For many years, women had complained about the lack of information they received before implant surgery. Many said they had received no data on possible complications, pain, and the chance that the implant would not last forever. This lack of information was due, in part, to the fact that silicone breast implants were widely used before there was any requirement for research and documentation of the safety and effectiveness of medical devices.
In 1997, the U.S. House of Representatives asked the federal Department of Health and Human Services to sponsor an extensive study of silicone breast implants. This comprehensive evaluation would include
-
a scientific look at the components of implants, including an analysis of silicone chemistry, toxicology, and immunology;
-
a history of breast implants and a description of their modern “generations,” or the many forms they have taken over time;
-
a review of complications occurring during or after breast implant surgery;
-
an analysis of studies examining whether breast implants are related to connective tissue, rheumatic, and neurological diseases and cancer;
-
an assessment of whether there are any effects of silicone implants on pregnancy, breast-feeding, and children; and
-
an evaluation of how mammography and other breast imaging techniques are affected by silicone implants.
The Institute of Medicine (IOM), part of the National Academy of Sciences, was selected to perform this important work.
To accomplish its task, the IOM set up a 13-member committee—6 of them women—made up of distinguished members of the medical, scientific, and educational communities, with experience in radiology, women's health, neurology, oncology, silicone chemistry, rheumatology, immunology, epidemiology, internal medicine, and plastic surgery (see list on inside back cover). This was a group of volunteers, without conflicts of interest, and with no prior or current relationship with any implant lawsuits.
An important task of the committee was to study and review thousands of published scientific reports. The committee also studied selected industry research reports on silicone breast implants and heard presentations from the public, including representatives of consumer groups, researchers, and women with silicone breast implants.
The committee's goals were to produce recommendations regarding the need for further research on the safety of silicone breast implants and to provide information to women with breast implants or who were considering breast implant surgery.
WHAT THE IOM COMMITTEE FOUND
The committee's work resulted in a 440-page report covering all aspects of silicone breast implants. An important goal of the committee was to provide to women all the known information about silicone breast implants. What follows are highlights from the committee's report, which it hopes will be of help not only to women considering breast implants but also to those who already have them.
Positive Findings
The committee focused on several issues of major concern to women regarding the safety of silicone breast implants, including their
-
potential for causing major disease,
-
effect on breast-feeding,
-
effect on unborn children,
-
implications for radiation therapy,
-
impact on the use of mammography to detect cancer,
-
health effects given recent improvements in design and implantation procedures, and
-
effect on the body's immune system.
In addition, the committee reviewed available data about the safety of silicone when implanted in the body. Some of the committee's major findings are summarized below.
Silicone Implants Do Not Cause Major Disease
Evidence clearly shows that silicone breast implants do not cause breast cancer or the recurrence of breast cancer. In fact, some studies suggest that women with breast implants have fewer new or recurring cancers. For example, a large, 14-year study of 3,182 women with cosmetic implants (augmentation) actually showed fewer cases of cancer (31) than would be expected (43) in a group of that size. The explanation for this lower-than-expected number of cancers is not clear. More studies should be conducted to determine whether or not the observation is valid and, if so, what might be contributing to the phenomenon.
Originally, concerns about cancer arose from studies that linked implant-formulated silicone with the development of cancerous tumors in rats. Such tumors can be induced if the implants are of a certain size, shape, and surface type and are made of a wide variety of substances, including glass and metal—not just silicone. No studies have demonstrated that such tumors ever develop in humans.
In addition, there is no evidence that silicone breast implants contribute to an increase in autoimmune (connective tissue) diseases. These diseases cause the immune system, which fights any invasion into the
body, to produce antibodies that attack the body's own tissues. Examples of autoimmune diseases are lupus, Raynaud 's phenomenon (a painful response of the hands and feet to cold), rheumatoid arthritis, and scleroderma, a disease that involves thickening of the skin.
A report from the long-term Nurses' Health Study involving 87,505 women showed no link between implants and connective tissue disease or rheumatic conditions.
A review of 17 separate studies of the occurrence of connective tissue disease in the population was remarkable for the consistent finding of no elevated risk or no indication of an association of implants with disease.
Moreover, the committee found no proof or significant evidence of the existence of a “novel” systemic disease, as some researchers have claimed, caused by the presence of silicone implants.
Although symptoms found in neurological diseases such as multiple sclerosis, neuritis, Lou Gehrig's disease, or Ménière's disease (a disorder of the inner ear) have been reported by some to be associated with breast implants, two large studies failed to find an increased incidence of these, or any other neurological diseases, in women with implants.
Nor do animal studies support the idea of silicone-gel deposits as a cause of neurological disease. (The committee did find that if an implant ruptures, localized problems such as scarring and nerve compression can occur in the breast or arm areas.)
The committee also concluded that because there are more than 1.5 million American women with silicone breast implants, it would be expected that some of these women would develop connective tissue diseases, cancer, neurological diseases, or other systemic complaints or conditions during their life. Evidence suggests that such diseases are no more common in women with breast implants than in women without them.
Breast-Feeding Is Okay
A major concern about implants has been the possible adverse effects of silicone on breast-fed infants. It is important to note that much higher levels of silicon—from which silicone is derived—have been found in cows' milk and commercially available infant formula than are found in
the breast milk of women with implants. In fact, there is no evidence of elevated silicone levels in breast milk or any other substance that would be harmful to infants, nor are there any differences in silicone levels in the milk and blood of nursing mothers with implants and those without them.
Although some mothers with implants may find it difficult to produce an adequate milk supply, the committee urges that all mothers try breast-feeding, because it is beneficial to babies and is not harmful to mothers.
Silicone Implants Do Not Harm the Developing Fetus
Concerns have been raised about the possible harmful effects of silicone crossing the placenta to the developing fetus. The committee found no evidence of increased levels of disease or birth defects in children born to women with implants.
Radiation Does Not Hurt Implants, and Vice Versa
Contrary to some published reports, the committee found no significant evidence that implants interfere with radiation therapy. The implants showed good stability in reaction to any necessary radiation doses, and they did not interfere with radiation beams. Evidence is limited that radiation therapy can cause capsular contracture (shrinkage and distortion of the implant area) and somewhat less pleasing cosmetic results, but there is the potential for concern.
Breast Implants Have Improved Over Time, Reducing Some Health Risks
There have been many changes—and improvements—in silicone implants since they were first introduced in 1963.
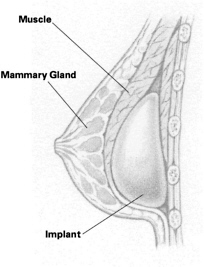
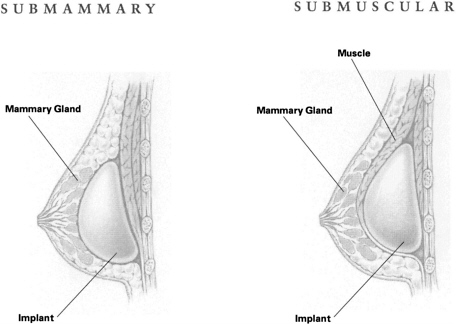
Although the time frame involved is relatively short, early results have caused many to believe that the implants of today offer greater protection from rupture or painful capsular contracture. The majority of implants are now inserted behind instead of on top of the chest wall muscles that cover the breast area. Putting the implants behind the muscles lessens the chance of severe contracture, that is, shrinking and hardening of the tissue around the implant, and allows a better view of breast tissue when a woman has a mammogram.
The outside of the implant shell (the elastomer) is usually textured, also offering greater protection against contracture. The shell itself today is stronger, often with an additional inner barrier layer that helps guard against seepage.
Saline implants were not very popular when they were first introduced. Not only did they often “deflate,” but also the cosmetic result was generally not as good as with the silicone-gel models. Patients complained about the “slosh effect,” a fluid wave from within the implant that sometimes they could actually hear. Another negative factor was the implant039;s thin consistency, with wrinkling visible through the skin.
But today's saline implants are much improved. The high rate of deflation has been corrected, and better cosmetic effects have been achieved by slightly overfilling the implant and placing it behind, or deep into, the chest muscles.
Some saline implants used in reconstruction have valves, designed to be inflated gradually after surgery as new tissue forms around the pocket created. Early valves often leaked, resulting in deflation or possible bacterial contamination of the saline. These problems, too, have been corrected.
Recent studies indicate that a majority of women are satisfied with their implants. Complaints to the FDA dropped sharply in 1995, after peaking in the period from 1992 to 1994, a time flame marked by numerous lawsuits and much negative publicity.
Implants Do Not Weaken the Immune System
A foreign protein in the body is called an antigen, and many antigens are found in bacteria and viruses. The body reacts to the presence of an antigen by producing an antibody. T cells, a type of white blood cell, play an important part in defending the body against disease. When these defenders malfunction, the result is an autoimmune disorder—such as rheumatoid arthritis—in which the body's own cells and tissues are attacked.
These disorders can be brought about by toxins that provoke the body into producing antibodies against itself. There is no evidence, however, that silicone implants cause such a reaction.
Antibodies are the body's normal way of dealing with foreign substances, and their presence doesn't necessarily indicate disease.
The Independent Review Group, organized in the United Kingdom in response to women's concerns about silicone breast implants, concluded that, overall, silicones found in breast implants were bland substances with little toxicity and no adverse effect on the body's immune system.
In General, Silicone Is “Safe”
The committee studied and evaluated multiple documents on the history, chemistry, and toxicology of silicone implants. It noted that the wide use of silicone—in foods, cosmetics, lubricants, and a variety of consumer products—has resulted in extensive exposure to it by individuals in all developed countries.
Almost all studies agree that there are baseline levels of silicon, an indicator for silicone, in normal breast and other tissue. Silicon is found in moderately higher than baseline levels around saline implants and in the capsules around silicone-gel implants. Silicon levels are particularly high around ruptured implants. This silicon apparently does not travel to other parts of the body. The committee found that exposure of women to silicone from the breast implant is limited almost entirely to the implant, its capsule, and the tissue and lymph nodes immediately surrounding the area. The IOM committee concluded that the silicon found in distant tissues most likely reflects human exposure to the widespread presence of silicon and silicone in the environment. At the end of its investigation, the IOM committee concluded that the silicones found in breast implants do not provide a basis for concern at doses reasonably to be expected.
Negative Findings
The committee also reported on its findings regarding the health problems that can occur in women with implants. These included
-
the need to replace implants,
-
local complications, and
-
the need for additional surgery or other medical interventions.
The most serious of these problems are “local” complications, meaning those that occur in or near the implant. Although generally not life threatening, such complications can cause discomfort and, in some cases, pose considerable risk. The IOM committee believes these local complications—
which occur often and may themselves prompt additional medical procedures, including operations—are the primary safety issue with silicone breast implants. The committee also recognizes that many of the reports reviewed in conducting this study were based on silicone-gel implants that were largely replaced by saline-filled implants in the early 1990s, and the risk of local complications is likely even lower with saline-filled implants.
Finally, although breast surgery has a low risk of death, many complications can occur when implants are removed, revised, or replaced.
Some of the problems the committee found follow.
Breast Implants Do Not Last Forever
The chances are great that most women will outlive their implants. The odds of having at least one replacement implant are high, and some women have had many more. A study of women receiving reconstruction over an average of 6 years showed that 16% of those with saline implants required replacements. Another study reported an 18% implant loss in women reconstructed with gel implants or submuscular expanders. A smaller study of women with implant troubles showed that, on average, over 12 years there were about three implants performed per woman.
The risks of having a local complication—such as a replacement operation—continue to accumulate over time.
Local Complications Are Frequent with Gel-Filled Silicone Implants
Women with gel-filled silicone implants and those undergoing reconstructive surgery appear to have a greater chance of complications than do women who have saline implants or implants for augmentation. The operation for immediate reconstruction is more serious because it involves a significant surgical procedure (mastectomy or removal of the breast) followed by the implant procedure. Some studies have suggested that from 30 to 40% of these patients could expect complications.
This percentage may rise when an expander is used to help generate tissue growth in the breast area, and complications are probably more frequent when the woman has previously undergone radiation therapy. The possibility of more frequent and serious side effects following immediate reconstruction must be weighed against the psychological benefits of such a procedure.
Women undergoing augmentation have fewer complications, especially if they have had modern “RTV” (room temperature vulcanized, or strengthened) saline implants. Still, the frequencies are high. A study of 2,855 women with modern saline implants showed 18% of augmented women and 36% of those with reconstruction had complications—within a year of receiving their implants—in one of four categories: infection, severe contracture, deflation, and implant removal.
The IOM committee found that a large number of women with implants could expect to have an additional procedure within the first 5 years after the original implant.
In addition, several studies indicate that removal of implants because of health fears is of little psychological value in relieving distress, depression, or anxiety.
Frequent Complications Mean Frequent Procedures
Frequent local complications include the rupture of silicone-gel-filled implants, the deflation of saline-filled implants, severe contracture of fibrous tissue around the implant, infections, hematoma (a pooling of clotted blood), pain, and implant displacement. The end result of these problems may be more surgery or other medical interventions.
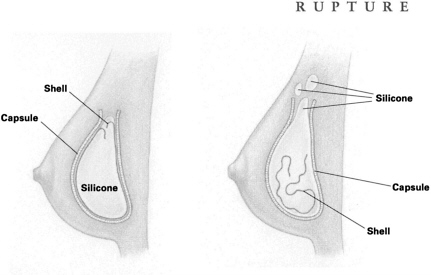
RUPTURE Rupture occurs when silicone gel escapes the implant shell. Such a rupture may be caused by tiny flaws in the shell or by inadvertent needle pricks while the incision is being stitched up. Ruptures can also happen after a needle insertion (a biopsy, for example) or when the breast is severely squeezed or compressed either during procedures to break up fibrous tissue (capsular contracture) around the implant, or because of trauma caused by an automobile accident or even, some say, a too-tight hug. The implant shell may also weaken with time; in fact, this can be expected with older models.
With the rupture of a silicone-gel implant, the gel and fluid can sometimes escape into other tissues and even form an unwanted lump somewhere else on the body, such as the arm, armpit, or chest area. Often, however, the space between the fibrous capsule (which forms around all implant shells) and the implant can actually contain the gel, keeping it from spreading into surrounding tissue, so that the rupture goes unnoticed. This type of rupture is called “intracapsular. ”
One of the questions the IOM committee hopes will be explored is whether screening measures should be undertaken to find these “hidden ” ruptures or whether diagnosis is necessary in women who have no symptoms (e.g., pain or leakage).
When both the implant shell and the capsule of a gel implant rupture or leak, the result is an “extracapsular” rupture that allows silicone to spill out or leak into body tissues. Most surgeons believe this condition should be corrected.
Surgery for extracapsular rupture consists of removal of the implant (explantation) as well as the capsule surrounding the implant (capsulectomy). These operations will require anesthesia, incisions, and stitches. And, of course, the surgical procedure may include a new implant as well.
The frequency of implant rupture is unknown. The IOM committee found studies reporting that the frequency of gel-filled implant ruptures varied from 0.3 to 77% of implanted women. The extreme variability of these percentages is due to the type and model of the implants, their length of implantation, the types of groups of women studied, and many other factors. Other investigators found no ruptures in late-model (“third-generation”) gel implants, but more time is needed to observe these implants. Some reasons for the confusing statistics about ruptures are (1) ruptures are not always detected, (2) the composition of implants has undergone many changes over the years, and (3) the time interval varies and is not long enough to pick up late ruptures. Because of such conflicting information, the committee recommends further studies.
Further, the IOM committee concluded that it is unclear whether implants in current use will need replacement in 10 or 15 years, as some older models did, or will last longer.
DEFLATION It is usually very easy to spot a saline implant that has ruptured—within 2 or 3 days the harmless saltwater solution spills out into the surrounding tissue and the implant collapses, or deflates. Only occasionally does a “slow leak” (partial deflation) take from 1 to 2 years to become noticeable.
Although early saline implant models had frequent deflations, later models are less likely to do so—a 5 to 10% frequency after 10 years, according to one study. Ruptures, leaks, and deflations may be more common in gel-filled implants than in current saline-filled models, although one team of investigators showed that only 67% of saline implants were still in place at the end of 10 years, causing the researchers to comment that their study “confirms the obvious: Inflatable breast implants deflate with time.”
The IOM committee concluded that deflation of modern first-year saline implants might run from 1 to 3% and that this percentage would rise steadily with time. The report strongly recommends that more studies be conducted to answer questions about today's implant rupture and deflation rates.
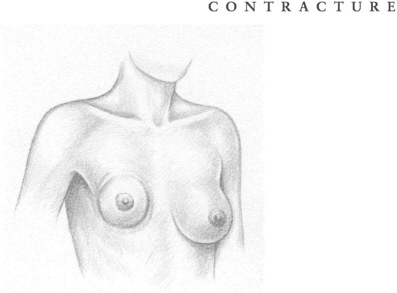
CAPSULAR CONTRACTURE The human body considers a breast implant—or any implant—to be a foreign agent and forms a protective capsule of fibrous tissue around the intruder, resembling the immature scar formed after a severe burn. This buildup of tissue is called a capsular contracture. If severe, it can cause painful and disfiguring squeezing as well as distortion of both the implant and the overlying tissue. The ensuing complications can be serious, including additional medical procedures to break down the overgrowth of protective tissue, or to remove it, or even to replace the implant itself. Additional surgery comes with its own risks, including infection, possible ruptures, and the hazards of anesthesia.
Some of these medical procedures—particularly “closed capsulotomy,” where strong pressure is applied to the outside of the breast to help break up the fibrous capsule—are performed repeatedly on the same women. Problems with capsular contracture made up 28% of secondary procedures done on women with breast augmentation and 14% of those with reconstruction. A recent study showed that contracture was the reason for 73% of implant removals.
The severity of contracture is often measured using the Baker Classification, which has four categories:
|
Class I |
The augmented breast is as soft as a nonaugmented one. |
|
Class II |
The breast is less soft and the implant can be palpated (felt) but is not visible. |
|
Class III |
The breast is firmer and the implant can be palpated easily and can be seen (or a distortion can be seen). |
|
Class IV |
The breast is firm, hard, tender, painful, and cold. Distortion is marked. |
Most surgeons consider the first two classes satisfactory but not the last two. Women, however, have often tolerated Class III and IV contractures either by not seeking any medical help or by indicating, when asked, that they are satisfied with their implants. A 1990 study reported that 85% of women appeared satisfied with their implants even though 35% had experienced severe contracture.
A 1997 report on 186 implants showed Class III and IV contractures continuing to occur, “reaching 100% around silicone-gel-filled implants at 25 years.”
Treatments for contracture other than closed capsulotomy include “open capsulotomy,” in which an incision is made into the body to break up the capsule, and a “capsulectomy” or surgical removal of the capsule itself. This operation may also involve removal and replacement of the implant as well as loss of breast tissue. Replacement and capsulectomy also involve as much as an hour or more of operating time. The IOM committee reports an excess use of some procedures, particularly the closed capsulotomy, in treating contracture. Repeated capsulotomy, open or closed, has progressively less chance of success. Contracture with its treatment is an important and incompletely resolved issue in breast surgery. It is likely that contracture is a progressive phenomenon, slowly increasing with time.
Scientists and doctors do not know for sure why severe contracture happens. Some have suggested that trauma to the breast during the implant surgery itself or at another time may bring about thickening and constriction of the capsule. The silicone used in implants has also been named as a culprit in contracture capsules formed around gel implants. The IOM committee noted that most studies agree that baseline levels of silicon are found in all normal breast and other tissue. Definite proof of a relationship between the presence of silicone in the tissue and contracture is lacking, but silicone fluid injected directly into the breasts (an early and improper practice) does cause fibrosis, or hardening of tissue.
Although definitive studies are limited, evidence suggests that saline-filled implants have a reduced rate of contracture compared to
implants filled with silicone. Fewer cases of severe contracture are also reported in studies of textured-surface implants compared to those with smooth surfaces. Both patients and doctors in a 1997 study preferred the textured surface.
In one clinical study, women undergoing immediate reconstruction after mastectomy also showed fewer cases of contracture than did women having later reconstruction. And, after 5 years, contracture among reconstructed women in the study was less frequent than that among augmented women. However, the women with reconstruction had a much higher proportion of textured-surface implants and implants placed behind the chest muscles than did the women with augmentation. This probably explains this unexpected result and suggests how effective texturing and placement can be in reducing contracture.
Placement of the implant behind the chest muscles seems to lower the chance of contracture. One study demonstrated that the rate of contracture is 30% with submammary implants versus 10% with submuscular implants. The lower incidence of severe contracture with submuscular implant placement is important. The IOM committee believes patients and surgeons should consider this factor when discussing implant surgery options.
Despite the possibility of contracture, some plastic surgeons still put the implant just beneath the skin or breast or glands in 32% of augmentation implants, probably because the procedure can have a better cosmetic effect and cause less long-term pain than the submuscular procedure.
The use of steroids to reduce capsular contracture is not recommended. Steroids placed inside saline implants may carry other health risks and are not approved for use by the FDA. In addition, steroids may weaken the implant shell. The IOM committee recommends that any use of steroids should be postponed until carefully designed studies can be conducted to determine the risks and benefits of such use.
INFECTION Infection can cause serious complications. Sometimes an infection can develop in the area where the surgery was performed, requiring medical treatment, additional surgery, and possibly removal or replacement of the implant.
Most local infections—those due to bacteria such as staph, for example—may be treated with antibiotics. These infections are reported most often in women who have had reconstruction, particularly immediate reconstruction after mastectomy. Sometimes infection can lodge in the expander used in some reconstructions. The ducts of breasts also collect some normal bacterial inhabitants of the skin area, and occasionally these may cause infection.
Infection may even contribute to the development of severe capsular contracture. The very medical procedures used to correct the condition may expose the area to more bacteria. One of the problems is that slightly abnormal and not easily detected infectious conditions can exist in a “slime” layer around the implant where the infectious agents are protected from the effects of antibiotics. According to some studies, these “subclinical” infections may also contribute to such symptoms as fatigue, muscle or joint pain, and diarrhea.
In one study of various implant devices, 93% of the women who reported pain also had an infection. When patients were given antibiotics (usually for staph) and implant devices were replaced by sterile models, 90% of the new implants were reported to be pain free.
The evidence that the presence of bacteria around an implant might contribute to contracture is not conclusive, but certainly suggestive.
HEMATOMA Sometimes blood or tissue fluid collects around an implant, causing pain, infection, or other complications. In a small number of cases, repeat operations have been necessary to correct the problem. Plastic surgeons often use drains after implant surgery to manage bleeding and the collection of blood (hematoma) or fluid around implants, and some surgeons claim such drains help prevent contracture.
Hematomas may occur, rarely, many years after the implant operation in association with contracture, perhaps because a stiff capsule has developed tiny fractures. The committee concluded that there is insufficient evidence pointing to more frequent contractures and subsequent complications around hematomas.
PAIN Pain is one of the significant reasons for implant removal and replacement, although few studies dealing with local implant problems have involved information about pain.
Some studies have reported that a majority of women do experience pain after implant surgery, and this pain may be long lasting.
Patients also reported more pain with implants after mastectomies compared with mastectomies alone and with implants placed under the chest muscles instead of under the skin and breast glands.
A questionnaire returned to one study group reported substantial local pain after reconstruction (up to 50%) and up to 38% after augmentation. As with other studies, pain was also more common after submuscular (50%) implants compared to submammary implants (21%), and with saline implants (33%) compared to gel-filled ones (22%).
About 20 to 29% of patients with pain required pain-control medication. Formation of the implant capsule, especially when the implant is under the chest muscles, may cause nerve compression resulting in considerable pain that may require additional treatment.
The committee recognized that pain following surgery is not surprising given the damage that occurs to the nerves to the breast during implantation and reconstructive surgery, which in some cases occurs after injury to the nerves following mastectomy and, in some cases, lymph node surgery.
Pain may also be an indicator of trouble ahead. Sometimes the implant has to be removed, or a capsule forming under the chest muscles may result in more compression and pain and lead to more surgical procedures. Much of the pain with a late onset is caused by capsular contracture, but it can also be indicative of bacterial infections or rupture.



















