
5
HEALTH EFFECTS OF METHYLMERCURY
THIS chapter begins with a brief review of the carcinogenicity of MeHg and its immunological, reproductive, renal, cardiovascular and hematopoietic toxicity. Because the central nervous system is widely viewed as the organ system most sensitive to MeHg, the remainder of this chapter focuses on the adverse effects of MeHg on neurological function. Neurological effects in infants, children, and adults are discussed. Studies carried out in populations exposed to high concentrations of MeHg are described, followed by a discussion of epidemiological data on populations exposed chronically to low concentrations of MeHg. Animal data following in utero, early postnatal, and adult exposure are also discussed.
The information available on the human health effects of MeHg are derived from studies of various designs. Each type of design has strengths and weaknesses and might be the most appropriate choice for a given set of circumstances. The methodology, strengths, and weaknesses of environmental epidemiological studies have been discussed in previous NRC reports (NRC 1991, 1997). The data on the Minamata and Iraqi episodes, the collection of which were initiated in response to the occurrence of recognizable illness in the population, are derived from case reports, descriptive studies of convenience samples, and ecological studies of rates. A major advantage of such studies is that the end points assessed are often of clear clinical significance. The inferences permitted from such studies, as described in greater detail in the following sec-
tions, can be limited by methodological weaknesses, such as the absence of detailed information on the sampling frame or referral patterns that generated the study sample, the degree to which the study sample is representative of the population from which it was drawn, exposure histories of the subjects, detailed assessments of health status, and the nature of severity of possible confounding biases.
Case-control studies, in which the exposure status (or history) of individuals with a certain health outcome (case) is compared with the exposure status of individuals without the health outcome (controls), can provide a much stronger basis for drawing inferences about exposure-disease associations. Among the challenges of such studies, however, are assembling a representative group of cases and a comparable group of controls, collecting adequate information on critical aspects of exposure history (which, in the case of long-latency diseases, might mean exposures that occurred decades before), and identifying the critical potential confounding biases. A case-control design, however, might be the only efficient way to study rare health outcomes.
Cohort designs (e.g., cross-sectional, retrospective, and prospective) provide a number of advantages. Instead of being selected on the basis of outcome status, as in case-control studies, study subjects are either randomly selected from the target population or selected on the basis of particular exposure characteristics (e.g., over-sampling of extremes of exposure distribution). The former strategy might be used if the goal is to enhance the generalizability of the study inferences to the target population, and the latter might be used if the goal is to estimate, with the greatest precision, the nature of the dose-response relationship within a certain region of the dose distribution. Another advantage of a cohort design is that multiple health outcomes can be measured and related to the index of exposure. A cohort study that incorporates prospective assessments of the study sample generally provides opportunities to assemble more-comprehensive exposure histories of the study subjects and to examine the natural history of a dose-response relationship, including factors that modify risk. As with all epidemiological studies, the methodological challenges of cohort studies include accurate classification of exposure and outcome status and the assessment and control of confounding bias.
CARCINOGENICITY
None of the epidemiological studies found an association between Hg exposure and overall cancer rates; however, two studies found an association between exposure to Hg and acute leukemia. The interpretation of those results is difficult due to the small study populations, the problem of assessing historical exposures to Hg, and the inability of investigators to control for other risk factors. In animals, chronic exposure to MeHg increased the incidence of renal tumors in male mice in some of the studies; however, the increase was observed only at doses that were toxic to the kidneys. Therefore, the tumorigenic effect is thought to be secondary to cell damage and repair. MeHg did not cause tumors in female mice or in rats of either sex. Therefore, in the absence of a tumor initiator, long-term exposure to subtoxic doses of MeHg does not appear to increase tumor formation.
On the basis of the available human and animal data, the International Agency for Research on Cancer (IARC) and the U.S. Environmental Protection Agency (EPA) have classified MeHg as a “possible” human carcinogen.
Human Studies
Four epidemiological studies examined the effect of Hg exposure on cancer incidence or cancer death rate. Those studies are summarized in Table 5-1. Tamashiro et al. (1984) carried out a cohort study that evaluated the causes of death of 334 individuals who had survived Minamata disease (MD) and died between 1970 and 1980. Control cases were selected from deaths that occurred in the same city or town as the MD cases and were matched for sex, age and year of death. No significant difference in cancer death rates was observed between the subjects and the controls, suggesting that the risk of dying from cancer was not correlated with patient history of MeHg poisoning. Specific types of cancer, however, were not evaluated.
Tamashiro et al. (1986) compared the death rates among residents of the Fukuro and Tsukinoura districts with those of age-matched residents of Minamata City. Residents of the two districts were assumed to have a higher intake of local seafood and higher Hg exposure than residents
TABLE 5-1 Summary of Cancer Studies in Humans
|
Type of Study |
Size of Study |
Finding |
Reference |
|
Retrospective cohort |
334 deaths in high-exposure cohort; 668 in low-exposure cohort |
No increase in cancer death rate; site-specific rates not analyzed |
Tamashiro et al. 1984 |
|
Retrospective cohort |
416 deaths in high-exposure cohort; 2,325 deaths in low-exposure cohort |
Increased liver-cancer death rate among males in high-exposure cohort |
Tamashiro et al. 1986 |
|
Case-control study of hair Hg concentrations in leukemia patients |
47 cases; 79 controls |
Increased hair Hg concentrations in acute leukemia patients |
Janicki et al. 1987 |
|
Retrospective cohort study of Minamata-disease (MD) survivors |
1,351 MD survivors; 5,667 referents |
Increased leukemia death rate among MD survivors; relative risk, 8.35 |
Kinjo et al. 1996 |
of Minimata City. No statistically significant increase in the overall cancer mortality was observed. However, an increase in liver- cancer death rates was observed among males who resided in the areas thought to have high Hg exposure (standardized mortality ratio (SMR1), 250.5; 95% confidence interval (CI), 133.4-428.4). Males also had significantly higher mortality due to chronic liver disease and cirrhosis in those areas than in Minamata City. The investigators indicated that the increases could not be attributed solely to MeHg, because the alcohol consumption rates and the prevalence of hepatitis B infection were higher in the Fukuro and Tsukinoura districts than in Minamata City. The study is also limited by its failure to fully characterize Hg concentrations in subjects in each cohort.
In a case-control study in Poland, Janicki et al. (1987) found a statisti-
|
1 |
The SMR is the ratio of the number of deaths observed in a study group divided by the number expected (based on age- or sex-specific rates in the general population) and multiplied by 100. An SMR greater than 100 indicates that the death rate was higher than would be expected. |
cally significant increase in the Hg content in hair collected from 47 patients with leukemia compared with 52 healthy unrelated subjects (mean 1.24 versus 0.49 ppm). The Hg content in hair from a subgroup of 19 leukemia patients was also significantly greater than that from 52 healthy relatives who had shared the same home for at least 3 years (0.69 versus 0.43 ppm). When those data were analyzed for specific types of leukemia, only patients with acute leukemia had significantly higher hair Hg concentrations. No significant difference was seen in the Hg content in hair collected from nine patients with chronic granulocytic leukemia or from 15 patients with chronic lymphocytic leukemia compared with the healthy unrelated subjects. The study is limited by the small study population, inadequate description of case and control populations, uncertainty about the source of Hg exposure, and lack of adjustment for other leukemia risk factors. In addition, all the hair Hg concentrations were within normal limits.
Kinjo et al. (1996) compared cancer death rates for a cohort (1,351 cases) of MD survivors with those of a referent population (5,667 subjects) who lived in the same region of Japan and consumed fish daily. After adjusting for age, gender, and length of follow-up period, they found no excess relative risk (RR) for overall mortality, all cancer deaths combined, or all noncancer deaths combined. Analysis of site-specific cancers found that Minamata survivors were less likely to die of stomach cancer than the referent population (RR, 0.49; 95% confidence interval (CI), 0.26-0.94). However, on the basis of five observed deaths, survivors were eight times more likely than the referent population to have died from leukemia (RR, 8.35; 95% CI, 1.61-43.3).
Animal Studies
The carcinogenic potential of MeHg was examined in several chronic exposure animal studies. Those studies are summarized in Table 5-2.
Newberne et al. (1972) carried out a 2-year multigeneration study in which Sprague-Dawley rats (30 per sex) were fed diets with MeHg doses of 0 or 0.008 mg/kg per day. Tumor incidence was similar in both groups; however, the maximum tolerated dose (MTD) was not achieved.
A 2-year feeding study conducted by Verschuuren et al. (1976) also failed to provide evidence of carcinogenic effects. Rats (25 per sex per
TABLE 5-2 Summary of Cancer Studies in Animals
|
Animal |
Dose (mg/kg/d) |
Tumor response |
Study Duration (wk) |
Reference |
|
Sprague-Dawley rat |
0, 0.008 |
None |
104 |
Newberne et al. 1972 |
|
Rats, unspecified strain |
0, 0.004, 0.02, 0.1 |
None |
104 |
Verschuuren et al. 1976 |
|
Sprague-Dawley rats |
130 |
Mitsumori et al. 1983, 1984 |
||
|
Males |
0, 0.01, 0.05, 0.28 |
None |
||
|
Females |
0, 0.01, 0.06, 0.34 |
None |
||
|
Swiss Albino mice |
0, 0.19, 0.95a |
None |
Weaning to death |
Schroeder and Mitchener 1975 |
|
ICR mice |
78 |
Mitsumori et al. 1981 |
||
|
Males |
0, 1.6, 3.1 |
0/37, 11/16, NA |
||
|
Females |
0, 1.6, 3.1 |
0, 0, NA |
||
|
Swiss mice |
0, 0.03, 0.07, 0.27 |
Increased tumor response to urethane |
15 |
Blakley 1984 |
|
ICR mice |
104 |
Hirano et al. 1986 |
||
|
Male |
0, 0.03, 0.15, 0.73 |
1/32, 0/25, |
||
|
Female |
0, 0.02, 0.11, 0.60 |
0/29, 13/26 |
||
|
None in any group |
||||
|
B6C3F1 mice |
0, 0.03, 0.14, 0.69 |
0/60, 0/60, |
104 |
Mitsumori et al. 1990 |
|
Male |
0, 0.03, 0.13, 0.60 |
0/60, 13/60 |
||
|
Female |
0/60, 0/60, |
|||
|
0/60, 1/60 |
||||
|
a0.95 mg/kg per day for 70 days and then 0.19 mg/kg per day thereafter due to high mortality at 0.95 mg/kg per day. Abbreviation: NA, not available. Mitsumori et al. (1983, 1984) also exposed Sprague-Dawley rats to MeHg chloride in feed (males, 0, 0.011, 0.05, or 0.28 mg/kg per day; group) were exposed to MeHg chloride at 0, 0.004, 0.020, or 0.10 mg/kg per day for 2 years. Survival decreased in the mid- and high-dose groups, and kidney weights increased in the high-dose group. However, tumors occurred at similar rates in all the groups. |
||||
females, 0, 0.014, 0.064, or 0.34 mg/kg per day) for up to 130 weeks. Effects were seen in the central nervous system, kidney, arterial wall, and spleen. The MTD was achieved in males in the mid-dose group and exceeded in males and females in the high-dose group. No increase in tumor incidence was observed.
A lifetime study conducted in Swiss albino mice failed to detect a tumorigenic response (Schroeder and Mitchener 1975). Groups of mice (54 per sex per group) were exposed from weaning until death to methylmercuric acetate in drinking water at two doses. The low-dose group received 1 ppm (0.19 mg/kg per day) and the high dose group received 5 ppm (0.95 mg/kg/day) for the first 70 days and then 1 ppm thereafter due to high mortality at the higher dose. Although no increase in tumors was noted, interpretation of the study is limited because of cessation of the high-dose exposure and failure to conduct complete histological examinations.
The incidence of renal tumors was increased in males in a study of ICR mice (60 per sex) fed diets containing MeHg chloride (0, 1.6, or 3.1 mg/kg per day) for 78 weeks (Mitsumori et al. 1981). The majority of mice in the high-dose group died by week 26 of the study. Males in the low-dose group had significantly higher numbers of renal epithelial adenocarcinomas (0 of 37 in control group; 11 of 16 in low-dose group) and renal adenomas (1 of 37 in control group; 5 of 16 in low-dose group) than controls. No renal tumors were observed in females in any group.
Blakley (1984) exposed female Swiss mice to MeHg chloride (approximately 0, 0.03, 0.07, or 0.27 mg/kg per day) in drinking water for 15 weeks. After 3 weeks of exposure, mice were given urethane in a single intraperitonal dose of 1.5 mg/kg. No more than one tumor per mouse was seen in the absence of urethane. With urethane, a statistically significant trend was seen for an increase in the size (0.7, 0.73, 0.76, and 0.76 millimeters (mm) at 0, 0.03, 0.07, and 0.27 mg/kg per day, respectively) and number of tumors per mouse (21.5, 19.4, 19.4, and 33.1 at 0, 0.03, 0.07, and 0.27 mg/kg per day, respectively). These findings suggest that MeHg may act as a tumor promoter.
In a follow-up study to Mitsumori et al. (1981), Hirano et al. (1986) fed MeHg chloride to ICR mice (60 per sex) at lower doses (males, 0, 0.03, 0.15, or 0.73 mg/kg per day; females, 0, 0.02, 0.11, or 0.6 mg/kg per day) for 104 weeks. Kidney and reproductive-system effects indicated that
the MTD was exceeded at the highest dose. An increased incidence of renal epithelial tumors (adenomas and adenocarcinomas) occurred in males. In males in the high-dose group, 10 of the 13 tumors were adenocarcinomas; the incidence of renal epithelial adenomas was not increased. No renal tumors were seen in females.
The incidence of renal tumors was also increased in male B6C3F1 mice following chronic exposure to MeHg chloride. Mitsumori et al. (1990) fed B6C3F1 mice (60 per sex) MeHg chloride (males, 0, 0.03, 0.14, or 0.69 mg/kg per day; females, 0, 0.03, 0.13, or 0.60 mg/kg per day). Following 104 weeks of exposure, adverse effects were seen in the central nervous system, kidney, and testis. The MTD was achieved in males in the mid-dose group and in females in the high-dose group. The MTD was exceeded in males in the high-dose group. The incidence of renal epithelial carcinomas and renal adenomas was significantly increased in males in the high-dose group.
Although chronic exposure to MeHg increased the incidence of renal tumors in male mice in some studies, that effect was observed only at doses that were toxic to the kidneys and is thought to be secondary to cell damage and repair. Exposure to MeHg did not increase tumor rates in female mice or in rats of either sex.
GENOTOXICITY
Human Studies
Evidence that human exposure to Hg causes genetic damage is inconclusive. Several investigators have reported higher rates of chromosomal aberrations among workers who were exposed to elemental or inorganic forms of Hg (Popescu et al. 1979; Verschaeve et al. 1976; Barregard et al. 1991). However, questions have been raised regarding the influence of possible confounders, such as age or simultaneous exposure to other toxicants on these findings. In a recent occupational study, Queiroz et al. (1999) reported a significant increase in the percentage of micronuclei in Hg-exposed workers when compared with unexposed controls.
Skerfving et al. (1970, 1974) reported a positive correlation between blood Hg concentrations and chromosomal aberrations in the lympho-
cytes of 23 people who consumed Hg-contaminated fish. However, their findings have been questioned because of experimental problems, such as failure to identify smokers. In addition, significant effects were found only from lymphocyte cultures that were set up several days after collection, and the incidence of aneuploidy in the control and exposed groups was lower than expected. Wulf et al. (1986) reported an increased incidence of sister chromatid exchange in humans who ate Hg-contaminated seal meat. However, information on smoking status and exposure to other heavy metals was not provided for those individuals, making interpretation of the study difficult. More recently, Franchi et al. (1994) reported a correlation between the incidence of micronuclei in peripheral lymphocytes and blood Hg concentrations in a population of fishermen who had eaten Hg-contaminated seafood.
Animal Studies
A single dose of Hg chloride (HgCl) to male Swiss mice (2.2, 4.4, or 8.9 mg/kg) induced a dose-related increase in the frequency of chromosomal aberrations and the percentage of aberrant cells in bone marrow (Ghosh et al. 1991). Chronic exposure of cats to MeHg at doses of 0.0084, 0.02, or 0.046 mg/kg per day for 39 months produced a significant increase in the number of nuclear abnormalities in bone-marrow cells and inhibited DNA repair (Miller et al. 1979). The response, however, was not dose related.
In Vitro Studies
MeHg has been shown to cause DNA damage in cultured Bacillus subtilis (Kanematsu et al. 1980); chromosomal aberrations and aneuploidy in human lymphocytes (Betti et al. 1992); and DNA damage in cultured human nerve and lung cells, Chinese hamster V-79 cells, and rat glioblastoma cells (Fiskesjo 1979; Costa et al. 1991). Inorganic Hg concentrations greater than 10 µM have been shown to inhibit mammalian DNA polymerase activity in whole-cell extracts and in purified enzyme preparations (Williams et al. 1987; Robison et al. 1984). Sekow-
ski et al. (1997) demonstrated the ability of mercuric ion to impair the fidelity of synthesome-mediated DNA replication at HgCl concentrations as low as 1 µM.
IMMUNOTOXICITY
The immune system appears to be sensitive to Hg. Although there are no data on the effect of MeHg on immune function in humans, occupational studies indicate that Hg compounds can affect the immune system. Animal studies have demonstrated MeHg effects on immune-cell ratios, cellular responses, and the developing immune system. Autoimmune effects have also been associated with exposure to elemental Hg.
Human Studies
The effect of MeHg on the human immune system has not been studied. However, occupational exposure to elemental Hg has been found to alter certain immune parameters. Queiroz and Dantas (1997a, b) evaluated B- and T-lymphocyte populations among 33 workers in a Brazilian Hg production facility. At the time of the study, all the workers had urinary Hg concentrations below 50 µg/g of creatinine. Analysis of T-cell populations found a reverse CD4+-to-CD8+ ratio that was haracterized by a reduction in the number of CD4+ lymphocytes. That alteration was significantly correlated with urinary Hg concentrations. B-lymphocyte counts were also significantly reduced in this cohort; however, that effect was not correlated with urinary Hg concentrations. Analysis of serum antibody levels found increased immunoglobulin E levels but did not detect anti-DNA or anti-nucleolar antibodies. The researchers reported a moderate negative correlation between length of exposure to Hg and IgE levels (Dantas and Queiroz 1997).
Moszczynski et al. (1995) studied lymphocyte subpopulations (T cells, T-helper cells, T-suppressor cells, and natural killer cells) in the peripheral blood of 81 men occupationally exposed to metallic Hg vapors and 36 unexposed men. The average Hg concentration in the workplace air was 0.0028 mg/m3. Urinary Hg concentrations ranged from 0 to 240
µg/L, and concentrations in the blood varied from 0 to 30 µg/L. Stimulation of T-lymphocytes — manifested by an increased number of T cells, T-helper cells, and T-suppressor cells — was observed.
Animal Studies
Effects on the Adult Immune System
Work in animals has demonstrated that Hg can effect immune function (see Table 5-3). Ilbäck (1991) found that oral exposure to MeHg altered the ratio of lymphocyte subpopulations, enhanced lymphoproliferation in response to B- and T-cell mitogens, and depressed natural-killer-cell activity in mice. Exposure of female Balb/c mice to MeHg (3.9 ppm) in the diet (equivalent to 0.5 mg/kg per day) for 12 weeks significantly decreased thymus weight (22%) and cell number (50%). Lymphoproliferation in response to T- and B-cell mitogens was increased, and natural-killer-cell activity was decreased in exposed mice. Red- blood-cell counts were slightly higher in exposed mice than in unexposed mice, and white-blood-cell counts were unaffected.
Thompson et al. (1998) evaluated the effects of low-dose MeHg exposure in mice. Mice were exposed to MeHg at 0, 3, or 10 ppm in the drinking water for 4 weeks. MeHg altered the proportion of splenocyte and thymocyte subpopulations and caused dose-dependent decreases in splenocyte glutathione concentrations and mitogen-stimulated calcium flux.
Rats were exposed to MeHg (chloride or sulfide; concentrations of 5 or 500 µg/L) in drinking water for 8 or 16 weeks (Ortega et al. 1997). An 8-week exposure to both concentrations of MeHg sulfide enhanced the lymphocyte response to conconavalin A. However, only the 54-µg/L concentration of MeHg chloride had that effect. At 16 weeks, lymphocyte proliferation decreased in the rats exposed to MeHg chloride but increased in those exposed to MeHg sulfide. Those data indicate that the effects of MeHg on T-cell proliferation are dependent upon the dose, duration, and chemical form of the MeHg exposure.
Prolonged exposure to MeHg increased the susceptibility of mice to
TABLE 5-3 Summary of Immunological Studies in Animals
|
Species |
NOAEL |
LOAEL |
Effect |
Reference |
|
Rat |
None |
3.9 ppm in diet of dams |
Reduced NK cell activity in pups |
Ilbäck et al. 1991 |
|
Rat |
None |
5 ppb in water |
Altered mitogen response |
Ortega et al. 1997 |
|
Rat |
None |
5 ppb in water of dams |
Increased thymic weight in pups |
Wild et al. 1997 |
|
Mouse |
None |
1 ppm in diet |
Increased mortality when infected with encephalitis virus |
Koller 1975 |
|
Mouse |
None 3.9 ppm in diet |
(0.5 mg/kg/d) |
Reduced NK cell activity; decreased thymus weight. |
Ilbäck 1991 |
|
Mouse |
None |
3.69 ppm in diet of dams |
Reduced resistance to Coxsackie B3 |
Ilbäck et al. 1996 |
|
Mouse |
None |
0.5 ppm in diet of dams |
Altered immune effects in pups |
Thuvander et al. 1996 |
|
Mouse |
None |
3 ppm in water |
Altered B-cell and T-cell subtypes; decreased GSH concentrations in splenocytes |
Thompson et al. 1998 |
|
Mouse |
None |
0.3 mg/kg/d |
Antinucleolar antibody production |
Hultman and Hansson-Georgiadis 1999 |
|
Abbreviations: NOAEL, no-observed-adverse-effect level; LOAEL, lowest-observed-adverse-effect level; NK, natural killer; GSH, glutathione. |
||||
viral infections. Koller (1975) fed mice subtoxic doses of MeHg chloride(1 or 10 mg/kg) for 84 days and saw significantly higher mortality after inoculation with encephalomyocarditis virus in exposed mice than in unexposed mice. In the same report, MeHg exposure did not alter the course of neoplasia in mice inoculated with Rauscher leukemia virus. MeHg (3.69 mg/g of diet) also did not alter the lethality of myocarditic coxsackie virus B3 in Balb/c mice but did increase heart tissue damage and viral persistence (Ilbäck et al. 1996).
Effects on the Developing Immune System
Prenatal and perinatal exposure to MeHg has long-term effects on the developing immune system. Ilbäck et al. (1991) reported alterations in white-blood-cell counts, natural-killer-cell activity, and the response of thymocytes and splenocytes to T-cell mitogen in Sprague-Dawley rats following prenatal and postnatal exposure of rat pups to MeHg. Wild et al. (1997) exposed rats, in utero and during the nursing period to MeHg (maternal drinking-water concentrations of MeHg chloride at 5 or 500 µg/L, or MeHg sulfide at 5 µg/L). At 6 weeks of age, total body and splenic weights were significantly increased in both MeHg-chloride-exposed groups. Rats exposed to MeHg sulfide had a significant increase in thymic weight at 6 weeks of age. Splenocyte response to pokeweed mitogen was enhanced at 6 and 12 weeks in both MeHg-chloride-exposed groups but was unaffected by MeHg sulfide. Natural-killer-cell activity was not affected in any exposure group at 6 weeks of age but was decreased by 57% in both groups exposed to MeHg chloride at age 12 weeks.
Similar effects have been demonstrated in mice. Female Balb/c mice were fed diets containing MeHg (0, 0.5 or 5 mg/kg) for 10 weeks before mating, throughout gestation, and up to day 15 of lactation (Thuvander et al. 1996). Blood Hg concentrations in the offspring were increased on day 22 (0.5-mg/kg group) and on days 22 and 50 (5-mg/kg group). The number of splenocytes and thymocytes increased, and the antibody response to a viral antigen was stimulated in the offspring of the 0.5-mg/kg group. The response of splenocytes to B-cell mitogen increased in offspring of the 5-mg/kg group. Lymphocyte subpopulations in the thymus were altered at both doses.
In Vitro Studies
The effects of MeHg on lymphocyte function have been studied in cell-culture systems in an attempt to elucidate the mechanisms involved in its ability to modulate immune function. Exposure of cultured lymphocytes to MeHg has been shown to inhibit mitogen-induced DNA synthesis, cell proliferation, and antibody synthesis. Electron micro-
scopic analysis of MeHg-exposed lymphocytes revealed nuclear changes characterized by hyperchromaticity and fragmentation. MeHg exposure also induced a rapid and sustained increase in intracellular calcium levels (Nakatsuru et al. 1985; Shenker et al. 1993). Shenker et al. (1999) investigated the mechanism by which MeHg chloride induces human T-cell apoptosis. They reported that the earliest detectable event following MeHg exposure was at the level of the mitochondria. Exposure of T-cells to MeHg chloride caused a decrease in the overall size of mitochondria and changes in the structure of the cristae. Cellular thiol reserves were depleted and mitochondrial cytochrome c was translocated to the cytosol.
Autoimmune Response
Human Studies
There is some evidence that human exposure to metallic Hg can induce an autoimmune response. Renal biopsies of two Hg-exposed workers who had developed proteinuria revealed deposits of IgG and complement C3 in the glomeruli (Tubbs et al. 1982). Examination of 10 patients who complained of illnesses after they received dental amalgams found that 3 of them had antiglomerular basement membrane antibodies, and 2 had elevated antinucleolar antibodies (Anneroth et al. 1992). In addition to those reports, Cardenas et al. (1993) reported high anti-DNA antibody titers in 8 of 44 workers from a chloralkali plant. No studies were located that evaluated autoimmunity in humans following exposure to organic forms of Hg.
Animal Studies
Hg is one of the few chemicals which is able to induce loss of tolerance to self-antigens in animals. This effect is human leukocyte antigen (HLA) dependent and has been demonstrated in genetically susceptible strains of rats and mice. Brown-Norway rats injected with Hg chloride (HgCl2) produce antilaminin antibodies, which attack the kidneys, causing an autoimmune glomerulonephritis (Druet et al. 1994). The
autoimmune response observed following Hg exposure has been linked to a T-cell dependent polyclonal B-cell activation (Hua et al. 1993). Hu et al. (1999) found that Hg exposure induced an autoimmune response in C57BL/6(H-2b) wild-type and interlukin-4 (IL-4)-deficient mice. Antibodies of all classes were induced by Hg treatment, except that in the IL-4-deficient mice, no immunoglobulin E (IgE) and very little IgG1 were produced.
REPRODUCTIVE EFFECTS
Human Studies
In occupational exposure studies, paternal exposure to metallic Hg does not appear to cause infertility or malformations (Alcser et al. 1989; Lauwerys et al. 1985). However, a study of pregnancy outcomes among the wives of 152 Hg-exposed men revealed an increased incidence of spontaneous abortions (Cordier et al. 1991). Preconception paternal urinary Hg concentrations above 50 µg/L were associated with a doubling of the spontaneous abortion risk.
The effect of elemental Hg on fertility and reproductive success has also been examined among occupationally exposed women. The results of various studies are conflicting but are suggestive of an effect on fertility. Elghany et al. (1997) compared the pregnancy outcomes of 46 Hg-exposed workers to those of 19 women who worked in nonproduction areas of the same factory. Among cases and controls during the study period (1948-1977), 104 pregnancies were recorded. Women exposed to inorganic Hg had a higher rate of congenital anomalies. Concentrations were up to 0.6 mg/m3. No significant differences in stillbirth or miscarriage rates were noted between the two groups of women. Rowland et al. (1994) found that the probability of conception among female dental hygienists who prepared more than 30 amalgams per week and had at least five poor hygiene practices when handling Hg was only 63% of that among unexposed controls. Women with lower exposures, however, were more fertile than unexposed controls. A large study conducted in Norway compared reproductive success rates among 558 female dental surgeons with those of 450 high-school teachers (Dahl et al. 1999). They concluded that exposure to Hg, benzene, and
chloroform was not associated with decreased fertility except for a possible Hg effect on the last pregnancy of multiparous dental surgeons.
No studies were identified that specifically evaluated human reproductive success following exposure to MeHg. However, in a study that described the clinical symptoms and outcomes of more than 6,000 Iraqi citizens who were severely poisoned by bread that had been prepared with MeHg-treated wheat, Bakir et al. (1973) commented on the low number of pregnant women in the cohort. Their report states, in part, that “The admissions frequency of affected pregnant females was remarkably low. One would expect to find approximately 150 pregnant females with diagnosable poisoning in the 6350 cases admitted to hospitals, yet only 31 such females were reported.” Although no explanation was offered for the small number of pregnancies among the exposed population, the report provides evidence of a possible effect of MeHg on human fertility.
Animal Studies
The reproductive effects of MeHg exposure in animals are summarized in Table 5-4. Abortion and decreased litter size are the most commonly reported reproductive effects of MeHg in animal studies. Pre- and post-implantation losses have been experimentally induced in rats, mice, guinea pigs, and monkeys exposed to MeHg.
In rats, an oral dose of MeHg at 7.5 mg/kg on gestational days 7-14 resulted in increased fetal deaths and an increased incidence of malformations. A dose of 5 mg/kg was also associated with an increased incidence of malformations as well as reduced fetal weight (Fuyuta et al. 1978).
In Fischer 344 rats, oral doses of MeHg chloride at 10, 20, or 30 mg/kg administered on day 7 of gestation decreased fetal survival by 19.1%, 41.4%, and 91.1%, respectively (Lee and Han 1995). Compared with control animals, implantation sites in the three groups were decreased by 5.9%, 13.7% and 22.5%, respectively. The median lethal dose for fetuses was 16.5 mg/kg.
Oral doses of MeHg hydroxide at 3, 5, or 10 mg/kg on day 8 of gestation in mice caused a significant dose-related decrease in litter size. No effects were seen at 2 mg/kg (Hughes and Annau 1976).
TABLE 5-4 Summary of Reproductive Studies in Animals
|
Species |
NOAEL (mg/kg/d) |
LOAEL (mg/kg/d) |
Effect |
Reference |
|
Monkey |
None |
0.05 |
Abnormal sperm |
Mohamed et al. 1987 |
|
Monkey |
0.05 |
0.07 |
Low conception rate |
Burbacher et al. 1988 |
|
Rat |
2.5 |
5 (males) |
Reduced litter size |
Khera 1973a |
|
Rat |
None |
10 on GD 7 |
Decreased fetal survival |
Lee and Han 1995 |
|
Mouse |
2 |
3 on GD 8 |
Decreased fetal survival |
Hughes and Annau 1976 |
|
Mouse |
None |
5 on GD 6-13 |
Fetal malformations |
Fuyuta et al. 1978 |
|
Mouse |
None |
10 on GD 10 |
Embryo resorption |
Fuyuta et al. 1979 |
|
Mouse |
None |
0.73 |
Low sperm counts Tubular atrophy of testes |
Hirano et al. 1986 Mitsumori et al. 1990 |
|
Guinea pig |
None |
11.5 on GD 21, 28, 35, or 42 |
Fetal abortions |
Inouye and Kajiwara 1988 |
|
Abbreviations: NOAEL, no-observed-adverse-effect level; LOAEL, lowest-observed-adverse-effect level; GD, gestation day. |
||||
Fuyuta et al. (1978) reported that an oral dose of MeHg chloride at 7.5 mg/kg on gestational days 6-13 in mice was embryocidal, and doses of 5 or 6 mg/kg reduced fetal weights and increased the incidence of malformations (cleft palate and fused thoracic vertebrae).
Fuyata et al. (1979) also dosed mice with a single oral dose of MeHg at 10,15, 20, or 25 mg/kg on gestational day 10. An increase in resorbed embryos occurred at 25 mg/kg. At the doses of 15, 20, and 25 mg/kg, fetuses weighed less than controls and had an increase in malformations.
A single dose of MeHg chloride at 11.5 mg/kg administered to pregnant guinea pigs on day 21, 28, 35, or 42 of gestation caused half of the litters to be aborted (Inouye and Kajiwara 1988).
Reproductive problems, including decreased conception rates, early abortions, and stillbirths were seen following exposure of female Macaca fascicularis monkeys to MeHg hydroxide at 50, 70, or 90 µg/kg per day for 4 months (Burbacher et al. 1988). Although no effects were observed on the menstrual cycle, the number of conceptions decreased with
increasing dose (93% for controls, 81% for group at 50 µg/kg per day, 71% for group at 70 µg/kg per day, and 57% for group at 90 µg/kg per day). A significant reduction in the percentage of viable offspring was observed for the groups at 70 and 90 µg/kg per day (83% for controls, 69% for group at 50 µg/kg per day and 29% for groups at 70 or 90 µg/kg per day). The effects on reproduction were observed at a maternal blood concentration greater than 1.5 ppm. Maternal toxicity was also observed in the doses of 70 and 90 µg/kg per day following prolonged MeHg exposure (½ year to over 1 year), typically at maternal blood concentrations greater than 2 ppm. Maternal toxicity was not seen in monkeys exposed at 50 µg/kg per day.
Effects on reproduction have also been seen following paternal exposure to MeHg. Exposure of male rats to high doses of MeHg chloride (5 to 7 daily doses of 1, 2.5, or 5 mg/kg) before mating with unexposed females produced a dose-related increase in post-implantation losses and reduced litter size (Khera 1973a). Exposure of male mice to those doses had no effect on reproductive success (Khera 1973a). Mohamed et al. (1987) examined the testicular functions of male Macaca fascicularis following oral exposure to MeHg hydroxide at 50 or 70 µg/kg per day for 20 weeks. Although there was no significant decrease in sperm counts, MeHg exposure was associated with a decrease in the percentage of motile sperm, a reduction in sperm speed, and an increase in the number of abnormal sperm (primarily bent or kinked tails). No effects were observed on serum testosterone concentrations, and no histological abnormalities were detected in testicular biopsies. Sperm motility returned to normal soon after the cessation of MeHg exposure, and sperm morphology remained abnormal. Chronic exposure to MeHg chloride at 0.73 mg/kg per day decreased spermatogenesis and produced tubular atrophy of the testis in mice (Hirano et al. 1986; Mitsumori et al. 1990). That dose caused renal damage, indicating that it exceeded the MTD.
RENAL TOXICITY
Human Studies
The kidney is sensitive to metallic Hg following inhalation exposure, possibly due to accumulation of Hg. High exposures have resulted in
mild transient proteinuria, gross proteinuria, hematuria, and oliguria. Kidney biopsies from workers with proteinuria revealed proximal tubular and glomerular changes (Kazantzis et al. 1962). Several investigations have found renal changes in workers chronically exposed to Hg vapor (Danziger and Possick 1973; Buchet et al. 1980; Barregard et al. 1988; Cardenas et al. 1993).
However, renal toxicity has rarely been reported following human exposure to organic forms of Hg (see Table 5-5). All cases in which renal damage was confirmed following exposure to organic Hg involved severe poisonings in which neurological symptoms were also present. An autopsy of a man who died following an acute exposure to alkyl Hg vapor revealed necrosis of the tubule epithelium, swollen granular protoplasm, and nonstainable nuclei in the kidneys (Höök et al. 1954). Jalili and Abbasi (1961) described the clinical course of several victims of the Iraqi poisoning incident who displayed symptoms of renal damage, including polyuria, polydypsia, and albuminuria. Similar symptoms were observed in two children who had consumed ethyl-Hg-contaminated pork over a period of several weeks (Cinca et al. 1979). Laboratory analyses conducted shortly after their illnesses began indicated elevated blood urea, urinary protein, and urinary sediment. Both children died of cardiac arrest, and their autopsies revealed severe nephritis and myocarditis.
The only evidence of a renal effect following ingestion of Hg-contaminated fish comes from a death-certificate review conducted by Tamashiro et al. (1986). They evaluated causes of death among residents of a small area of Minamata City that had the highest prevalence of MD using age-specific rates for the entire city as a standard. Between 1970 and 1981, the number of deaths attributed to nephritic diseases was higher than expected among women who resided in that region (SMR, 276.5) but was within the expected range (0.80) among men who resided in this region.
Animal Studies
Although it is well known that the kidney is the target organ for inorganic Hg (Samuels et al. 1982), several reports from animal studies have also described MeHg- induced renal toxicity (see Table 5-6). A
TABLE 5-5 Summary of Renal Studies in Humans Exposed to Various Organic Mercurials
|
Exposure source |
Effects |
Reference |
|
Occupational exposure to alkyl Hg vapors |
Necrosis of renal tubules |
Höök et al. 1954 |
|
Occupational exposure to Hg vapors |
Albuminuria, tubular changes |
Kazantzis et al. 1962 |
|
Occupational exposure to Hg vapors |
Proteinuria |
Danziger and Possick 1973 |
|
Occupational exposure to Hg vapors (urinary > 50 µg/g creatinine) |
Albuminuria |
Buchet et al. 1980 |
|
Occupational exposure to Hg vapors |
Increased N-acetyl-B-glucosaminidase |
Barregard et al. 1988 |
|
Occupational exposure to Hg vapors |
Tamm-Horsfall protein, tubular antigen |
Cardenas et al. 1993 |
|
Ingestion of mercuric chloride (30 mg/kg) |
Oliguria, proteinuria |
Afonso and deAlvariz 1960 |
|
Ingestion of mercuric chloride |
Fatal acute renal failure |
Murphy et al. 1979 |
|
Dermal application of mercuric ammonium chloride |
Impaired renal function |
Barr et al. 1972 |
|
Dermal application of mercuric ammonium chloride |
Impaired renal function |
Dyall-Smith and Scurry 1990 |
|
Ingestion of ethyl-Hg-contaminated pork |
Elevated blood urea, urinary protein, urinary sediment |
Cinca et al. 1979 |
|
Ingestion of MeHg-treated wheat |
Polyuria, albuminuria |
Jalili and Abbasi 1961 |
|
Ingestion of MeHg-contaminated fish |
Increase in deaths due to nephritic diseases among women |
Tamashiro et al. 1986 |
report by Fowler (1972) described the presence of large numbers of spherical masses containing bundles of smooth endoplasmic reticulum in the pars recta of the kidney proximal tubules in rats following a 12-week exposure to MeHg at 2 ppm (0.08 mg/kg per day). Those effects were observed in female rats only. The authors indicated that the sex-specific effects were most likely due to sex differences known to exist in the activity of kidney enzymes associated with MeHg metabolism. In
TABLE 5-6 Summary of Renal Studies in Animals
|
Species |
Duration |
NOAEL (mg/kg/d) |
LOAEL (mg/kg/d) |
Effect |
Reference |
|
Rat |
3-12 wk |
None |
0.84 |
Fibrosis, inflammation, large foci in renal cortex |
Magos and Butler 1972 |
|
Rat |
12 wk |
0.08 |
Cytoplasmic masses in proximal tubules |
Fowler 1972 |
|
|
Rat |
2 yr |
0.02 |
0.1 |
Increased renal weights Decreased renal enzymes |
Verschuuren et al. 1976 |
|
Rat |
0-21 days of age |
None |
1 |
Altered renal function and renal hypertrophy |
Slotkin et al. 1985 |
|
Rat |
2 yr |
0.4 |
Nephrosis |
Solecki et al. 1991 |
|
|
Mouse |
26 wk |
0.15 |
0.6 |
Degeneration of proximal tubules |
Hirano et al. 1986 |
|
Mouse |
0.03 (males) 0.13 (females) |
0.14 (males) 0.6 (females) |
Chronic nephropathy, interstitial fibrosis |
Mitsumori et al. 1990 |
|
|
Mouse |
Once |
8 (males) 24 (females) |
16 (males) 32 (females) |
Decreased phenolsulfonphthalein excretion, increased serum creatinine, swollen tubuler epithelium |
Yasutake et at. 1991 |
|
Abbreviations: NOAEL, no-observed-adverse-effect level; LOAEL, lowest-observed-adverse-effect level. |
|||||
a similar study, Magos and Butler (1972) reported fibrosis in the renal cortex of female rats following 12 weeks of MeHg exposure at the lowest dose studied (0.84 mg/kg per day). Increased kidney weight and decreased proximal convoluted tubule enzymes were seen in rats given MeHg chloride in the diet (0.1 mg/kg per day) for 2 years. No histopathological changes were observed (Verschuuren et al. 1976). Subsequent studies of rats and mice reported nephrosis following long-term exposure to MeHg (Mitsumori et al. 1983, 1984, 1990; Solecki et al. 1991). Nephrosis was also observed in rats exposed to phenylmercuric acid in drinking water for 2 years (Solecki et al. 1991).
Degeneration of the proximal tubules was observed in mice given MeHg chloride in the diet (0.11 mg/kg per day) for 2 years (Hirano et al. 1986). Epithelial degeneration and regeneration of the proximal tubules and interstitial fibrosis were noted in both male and female mice following almost 2 years of exposure to MeHg in the diet (estimated
dose associated with effects was approximately 0.2 mg/kg per day) (Mitsumori et al. 1990). Yasutake et al. (1991) showed in mice that a single oral dose of MeHg (16 mg/kg) impaired renal function, causing increased plasma creatinine concentrations and swelling of tubular epithelium with exfoliation of cells into the tubular lumen. No effects were observed after a single gavage dose of Hg at 8 mg/kg.
A study by Slotkin et al. (1985) examined the renal effects of MeHg exposure during the neonatal period. Rats exposed to daily doses of 1 or 2.5 mg/kg per day from birth to 21 days of age (weaning) exhibited renal hypertrophy and altered renal function (elevated fractional excretions of water, glucose, sodium, chloride, osmotic particles), which peaked at approximately 20 days of age. The authors indicated that the results reflected effects on tubular function and that tests conducted in conjunction with physiological challenge might reveal even greater impairment.
CARDIOVASCULAR EFFECTS
Numerous studies have examined fish consumption and cardiovascular disease risk, and there are strong indications of protective effects of fish. These effects could be due to a number of components in fish, such as omega-3 fatty acids and selenium and might also indicate a different style of eating (diets lower in red meats).
Although inclusion of fish in the diet is generally beneficial, some fish contain agents such as MeHg and PCBs that have been associated with adverse cardiovascular effects. Therefore, future studies should control for co-exposure to these common contaminants in their analyses of the beneficial effects of fish intake.
Hg accumulates in the heart, and exposures to organic and inorganic forms of this metal have been associated with blood-pressure alterations and abnormal cardiac function. Numerous reports of human poisonings have described marked hypertension and abnormal heart rate among victims. Autopsies of two boys who died of cardiac arrest after they were fed ethylmercury-contaminated pork over a period of several weeks revealed myocarditis. Two recent epidemiological studies have found associations between dietary exposure to very low levels of MeHg
and cardiovascular effects. One of those studies found evidence of an effect of prenatal MeHg exposure on heart function at age 7. Additional studies are needed to better characterize the effect of MeHg exposure on blood pressure and cardiovascular function at various stages of life.
Human Studies
The cardiovascular effects of Hg exposure in humans are summarized in Table 5-7. Warkany and Hubbard (1953) reported several cases in which children developed tachycardia and elevated blood pressure after they were treated with mercurous chloride-containing medications for worms or teething discomfort. Increases in blood pressure and heart rate have also been reported following inhalation of high concentrations of metallic Hg (Hallee 1969; Soni et al. 1992; Bluhm et al. 1992). In one of the cases, the increase in heart rate was described as a sinus tachycardia (Soni et al. 1992). Marked hypertension (160/120 mm Hg) and tachycardia (120 beats per minute) were also described in an 11-year old girl who was hospitalized with a diagnosis of acute Hg intoxication (Wössmann et al. 1999). Vroom and Greer (1972) reported a high incidence (five of nine workers) of hypertension among workers in a thermometer plant.
Exposure to organic Hg has also been associated with cardiovascular changes. Three clinical case reports and two epidemiological investigations have reported similar effects. The first evidence of cardiovascular abnormalities following exposure to organic Hg was provided by Jalili and Abbasi's (1961) description of patients who were hospitalized during the Iraqi grain poisoning epidemic. Abnormalities seen in severely poisoned patients included irregular pulse and electrocardiograms showing ventricular ectopic beats, prolongation of the Q-T interval, depression of the S-T segment and T inversion. Electrocardiograms of four family members who consumed ethylmercury-contaminated pork revealed similar findings, including abnormal heart rhythms with S-T segment depression and T-wave inversion (Cinca et al 1979). Deaths of two children in this family were attributed to cardiac arrest, and their autopsies revealed myocarditis. A child who was diagnosed with acrodynia following exposure to vapors from a paint that contained
Table 5-7 Summary of Cardiovascular Studies in Humans
|
Exposure source |
Effects |
Reference |
|
Mercurous Chloride medications |
Tachycardia and increased blood pressure in children |
Warkany and Hubbard 1953 |
|
Occupational exposure to alkyl Hg vapors |
Increased blood pressure |
Höök et al. 1954 |
|
Alkyl Hg-contaminated wheat |
Irregular heart rate |
Jalili and Abbasi 1961 |
|
Ethylmercury-contaminated meat |
Irregular heart rate, cardiac arrest, myocarditis |
Cinca et al. 1979 |
|
Phenylmercuric acetate vapors |
Hypertension and rapid heart rate |
Aronow et al. 1990 |
|
Metallic Hg vapors |
Increased blood pressure and heart rate |
Hallee 1969, Bluhm et al. 1992, Soni et al. 1992, Vroom and Greer 1972 |
|
Dental amalgams |
Increased blood pressure |
Siblerud 1990 |
|
Frequent fish consumption |
Higher cardiovascular death rates |
Salonen et al. 1995 |
|
Hg intoxication (source unspecified) |
Marked hypertension in child |
Wössmann et al. 1999 |
|
Unspecified |
High Hg concentrations in myocardium of IDCM patients |
Frustaci et al. 1999 |
|
Prenatal exposure |
Increased blood pressure and decreased heart rate variability at age 7 |
Sørensen et al. 1999 |
phenylmercuric acetate exhibited a rapid heart beat and hypertension (Aronow et al. 1990).
Two recent epidemiological investigations have found associations between exposure to low levels of MeHg and adverse cardiovascular effects. A recent study by Sørensen et al. (1999) showed an association between prenatal exposure to MeHg and cardiovascular function at age 7. The study of 1,000 children from the Faroe Islands found that diastolic and systolic blood pressures increased by 13.9 and 14.6 mm Hg, respectively, as cord-blood Hg concentrations rose from 1 to 10 µg/L. In boys, heart-rate variability, a marker of cardiac autonomic control,
decreased by 47% as cord-blood Hg concentrations increased from 1 to 10 µg/L.
Salonen et al. (1995) compared dietary intake of fish and Hg, and compared Hg concentrations in hair and urine with the prevalence of acute myocardial infarction (AMI) and death from coronary heart disease or cardiovascular disease in a cohort of 1,833 Finnish men. All study participants were free of clinical heart disease, stroke, claudication, and cancer at the beginning of the study. Daily fish intake ranged from 0 to 619.2 g (mean = 46.5 g per day) and hair Hg concentrations ranged from 0 to 15.67 ppm (mean = 1.92 ppm). Dietary Hg intake ranged from 1.1 to 95.3 µg per day (mean = 7.6 µg per day). Over a 7-year observation period, men in the highest tertile (at or more than 2 ppm) of hair Hg content had a 2.0-fold higher risk of AMI than men in the two lowest tertiles. The relative risk was similar for coronary deaths and cardiovascular deaths, although the difference for coronary deaths did not reach statistical significance due to small numbers. Men who consumed at least 30 g of fish a day had a 2.1-fold higher risk of AMI. For each additional 10 g of fish consumed, there was an increment of 5% in the 5-year risk of AMI.
Trace elements were measured in myocardial and muscle-tissue samples from 13 patients diagnosed with idiopathic dilated cardiomyopathy (IDCM). The subjects had no history of Hg exposure. Findings were compared with Hg concentrations measured in myocardial and muscle biopsies from age-matched patients with valvular (12 patients) or ischemic heart disease (13 patients), papillary and skeletal-muscle biopsies from 10 patients with mitral stenosis, and left-ventricle endomyocardial biopsies from 4 normal subjects. Hg concentrations in myocardial samples collected from patients with IDCM were 22,000 times higher than those in control samples. Antimony, gold, chromium, and cobalt concentrations were also higher in IDCM patients, but the greatest differences were for Hg (178,400 ng/g versus 8 ng/g) and antimony (19,260 ng/g versus 1.5 ng/g). The investigators concluded that the increased concentration of trace elements found in patients with IDCM might adversely affect mitochondrial activity and myocardial metabolism and worsen cellular function (Frustaci et al. 1999). Matsuo et al. (1989) analyzed Hg concentrations in human autopsy tissues collected from 46 cadavers. The subjects (32 males and 14 females aged
4 months to 82 years) were residents of metropolitan Tokyo and had no known exposure to Hg. The average total Hg content in heart tissue was 43 ng/g, with 80% of this being in the form of MeHg.
Animal Studies
Effects of MeHg on the heart and circulatory system have been observed in several animal models (see Table 5-8). A report by Shaw et al. (1979) described cerebrovascular lesions in four nonhuman primates following long-term exposure to near-toxic to toxic doses of MeHg hydroxide (90 to 120 µg/kg per day). Lesions were similar to those observed in humans with hypertension; intimal thickening, smooth-muscle cell proliferation, and adventitial fibrosis were reported.
Mitsumori et al. (1983, 1984) fed Sprague-Dawley rats diets containing MeHg chloride (males, 0, 0.011, 0.05, or 0.28 mg/kg per day; females, 0.014, 0.064, or 0.34 mg/kg per day) for up to 130 weeks. Polyarteritis nodosa and calcification of the arterial wall were seen at the highest
TABLE 5-8 Summary of Cardiovascular Studies in Animals
|
Species |
NOAEL (mg/kg/d) |
LOAEL (mg/kg/d) |
Effects |
Reference |
|
Monkeys |
None |
0.09 |
Cerebrovasular changes, hypertension, intimal thickening |
Shaw et al. 1979 |
|
Rat |
0.05 (males) 0.06 (females) |
0.28 (males) 0.34 (females) |
Polyarteritis nodosa, calcification of arterial wall |
Mitsumori et al. 1983, 1984 |
|
Spontaneous hypertensive rat |
None |
2 (26 d) |
Increased blood pressure in females |
Tamashiro et al. 1986 |
|
Rat |
None |
0.4 |
Hypertension |
Wakita 1987 |
|
Rat |
None |
12 (2 d) |
18% decrease in heart rate |
Arito and Takahashi 1991 |
|
Abbreviations: NOAEL, no-observed-adverse-effect level; LOAEL, lowest-observed-adverse-effect level. |
||||
dose. Histological examination revealed evidence of hemosiderosis and extramedullary hematopoiesis of the spleen.
Tamashiro et al. (1986) reported an increase in blood pressure in spontaneous hypertensive rats (SHR) exposed to MeHg at 2 mg/kg per day for 26 consecutive days. That effect was sex specific, being observed only in females. Considerable variation was observed in blood pressure for both the MeHg-exposed and the control rats. Differences were observed at only two time points, week 3 and week 5 of the study.
In Wistar rats, hypertension was induced after a 30-day exposure to MeHg chloride at 0.4 or 1.2 mg/kg per day (Wakita 1987). The onset of hypertension occurred 42 days after the exposure period ended, and the effect persisted for more than 1 year. In rats, a decrease in heart rate (18%) was observed following 2 daily doses of MeHg at 12 mg/kg per day (Arito and Takahashi 1991).
HEMATOLOGICAL EFFECTS
Hematological changes have not been reported following human exposure to Hg. Studies conducted in animals suggest that Hg exposure might pose a risk of anemia and clotting disorders. Those animal studies are summarized in Table 5-9.
Munro et al. (1980) exposed rats to Hg at 0.25 mg/kg per day for up to 26 months. Exposed males had decreased hematocrit and hemoglobin values, as well as overt signs of neurotoxicity and increased mortality
TABLE 5-9 Summary of Hematological Studies in Animals
|
Species |
NOAEL (mg/kg/d) |
LOAEL (mg/kg/d) |
Effect |
Reference |
|
Rat |
None |
0.25 for 26 mon. |
Decreased hematocrit and hemoglobin values |
Munro et al. 1980 |
|
Rat |
None |
8.0 |
Decreased clotting time |
Kostka et al. 1989 |
|
Rat |
None |
4.2 |
Decreased hematocrit and hemoglobin values |
Solecki et al. 1991 |
compared with unexposed controls. Hematological changes were not observed in exposed female rats.
Abbreviations: NOAEL, no-observed-adverse-effect level; LOAEL, lowest-observed-adverse-effect level.
Kostka et al. (1989) examined the coagulability of blood in rats exposed to either a single dose of MeHg chloride at 17.9 mg/kg per day or 5 consecutive days of dosing at 8 mg/kg per day. Blood coagulation was measured 1, 3, and 7 days after administration of the single dose or 24 hr after the 5 consecutive days of dosing. A reduction in clotting time and an increase in the fibrinogen concentrations in plasma were observed in both MeHg dose groups. Reduced clotting time was observed in the single-dose group 1 day after exposure.
Decreased hemoglobin, hematocrit, and red-blood-cell counts were seen in rats exposed to phenylmercuric acetate in drinking water (4.2 mg/kg per day) for 2 years (Solecki et al. 1991). The anemia might have been secondary to blood loss associated with ulcerative lesions seen at that dose in the large intestine. Polycythemia developed in rats exposed in utero to a combinations of MeHg chloride, ethylurea, and sodium nitrate. The polycythemia occurred as early as 1 month of age in as many as 24% of the offspring. Many features of this condition were similar to the features of polycythemia vera in man (elevated hematocrit, white- and red-blood-cell counts, splenomegaly, and hyperplasia of bone marrow) (Koller et al. 1977). Because that study involved concurrent exposure to MeHg, ethylurea, and sodium nitrite, the observed effects cannot be attributed to MeHg.
DEVELOPING CENTRAL-NERVOUS-SYSTEM TOXICITY
Human Studies
The central-nervous-system (CNS) effects of MeHg in humans have been extensively studied following accidental poisoning incidents and low-dose exposures. In this section, the Minamata and Iraqi Hg poisoning episodes are reviewed, documenting the severe neurological dysfunctions and developmental abnormalities that occur in children exposed in utero to high doses of MeHg. That review is followed by a review of the effects of low-dose prenatal MeHg exposure on neurological status, age at achievement of developmental milestones, infant and preschool development, childhood development, sensory and neuro-
physiological functions, and other end points in children; and neurological, neurophysiological and sensory functions in adults.
High-Dose Poisonings
Poisoning Episode in Japan
The mass poisoning of residents living near Minamata Bay in Japan in the 1950s first raised awareness of the severe neurological sequelae associated with MeHg poisoning, particularly when it occurs prenatally. The primary route of exposure in that episode was the consumption of fish contaminated with MeHg that bioaccumulated as it ascended the aquatic food chain. According to Harada (1995), all children identified as suffering from the most severe form of congenital Minamata disease (CMD) expressed mental retardation, primitive reflexes, cerebellar ataxia, disturbances in physical growth, dysarthria, and limb deformities. Most of the affected children also expressed hyperkinesis (95%), hypersalivation (95%), seizures (82%), strabismus (77%), and pyramidal signs (75%). The incidence of cerebral palsy among children with CMD was also increased (9% of 188 births in three villages versus a national incidence of 0.2% to 2.3%). Some signs and symptoms decreased over time (e.g., paroxysmal events, hypersalivation, primitive reflexes, and ataxia), although others (e.g., reduced intelligence and dysarthria) did not (Harada 1995). Most of the patients with the severe form of CMD were unable to function successfully in society.
It is difficult to reconstruct the MeHg doses in the CMD patients. Measurements of Hg in hair and blood were not made until 1959, several years after the poisoning episode was identified. The Hg concentrations in maternal-hair samples taken 5 to 8 years after giving birth to infants with CMD ranged from 1.8 to 191 ppm (Harada 1995). Analyses of the Hg concentrations in 151 archived umbilical-cord tissue samples dating from 1950 to 1969 confirmed that exposures increased during this period (Harada et al. 1999). Concentrations were highest in patients with CMD, intermediate in patients with acquired MD, and lowest in asymptomatic individuals. On the basis of these data, Akagi et al. (1998) estimated that the mean maternal-hair Hg concentration in CMD patients was approximately 41 ppm (range 3.8 to 133 pm). The uncertainty
associated with that estimate, however, is likely to be substantial. Identification of cases was undoubtedly incomplete, particularly among individuals who suffered milder forms of CMD. For example, even excluding cases of known CMD, the prevalence of mental retardation among children born between 1955 and 1958 in the contaminated area was 29%, far higher than that expected as a background prevalence. That finding suggests that many children with less severe forms of CMD were undiagnosed. Thus, the data cannot provide precise estimates of the minimum dose of MeHg required to produce CMD.
Several observations associated with MD suggest that neurological deficits might emerge decades after exposure to MeHg has ended and that the severity of deficits might increase as a patient ages. It is difficult, however, to definitively rule out continued Hg exposure in adulthood as having a role in progressive neurological disorders. Harada (1995) distinguished three groups of patients with atypical, incomplete, or slight symptoms: (1) gradually progressive type, (2) delayed- onset type, and (3) escalator-progressive type. Evidence consistent with delay in the expressions of MeHg neurotoxicity was reported in a long-term follow-up study of 90% of diagnosed MD patients at least 40 years of age (1,144 patients). Kinjo et al. (1993) found not only that the prevalence of deficits in “activities of daily living” (i.e., eating, bathing, and dressing) was greater among cases than among age- and sex-matched controls but also that the difference between the prevalence rates of the two groups increased significantly with age. Increased deficits with age and delayed effects were also seen in animal studies (Spyker et al. 1972; Rice 1996, 1998; see section on Animal Studies).
Poisoning Episode in Iraq
A second episode of mass MeHg poisoning occurred in Iraq in the early 1970s when seed grain treated with a MeHg-containing fungicide was ground into flour and consumed. Those MeHg exposures were most likely more acute and involved higher exposures than those experienced by the residents of Minamata Bay. Early studies of the most severely affected children exposed to MeHg during fetal development were concordant with the Minamata findings. Those children manifested severe sensory impairments (blindness and deafness), general
paralysis, hyperactive reflexes, cerebral palsy, and impaired mental development (Amin-Zaki et al. 1974). Several follow-up studies of the exposed population were conducted. Marsh et al. (1987) identified 81 children who had been in utero at the time of the episode and collected information from two sources on children's neurodevelopmental outcomes: neurological examination of each child and a maternal interview regarding the age at which the child achieved standard developmental milestones, such as walking and talking. Maximum maternal-hair Hg concentrations during the time when the study child was in utero served as the index of fetal exposure and ranged from 1 to 674 ppm. Developmental retardation was defined as a child's failure to walk a few steps unaided by 18 months of age or to talk (two or three meaningful words) by 24 months of age. A point system was devised for scoring the neurological examination; a score greater than 3 indicated a definite abnormality. There was a dose-response relationship between the prevalence of those indicators of poor outcomes and maternal-hair Hg concentrations. The most frequent neurological findings were increased limb tone and deep tendon reflexes with persisting extensor plantar responses. Ataxia, hypotonia, and athetoid movements were also reported. Boys appeared to be more severely affected than girls. Seven of the 28 children with the highest exposures had seizures (versus none of the 53 children with the lowest exposures). For those seven children, maternal-hair Hg concentrations ranged from 78 to 674 ppm. Many children of mothers with hair concentrations exceeding 100 ppm had normal neurological scores and achieved milestones at the expected times. Moreover, many of the women who had very high hair Hg concentrations and whose infants did poorly experienced only mild and transient signs or symptoms of MeHg toxicity.
Additional analyses of that data set were conducted in an attempt to identify more precisely the shape of the dose-response relationship and, in particular, the threshold for adverse neurodevelopmental effects, if indeed such a threshold exists. Cox et al. (1989) obtained more accurate estimates of peak exposure during pregnancy by applying an X-ray fluorescent method to single strands of maternal hair. Using a variety of statistical models (logit, hockey-stick, and nonparametric kernel-smoothing methods), they estimated a population threshold of approximately 10 ppm for the outcomes investigated (see Figure 5-1, Figure 5-2, and Figure 5-3). However, the uncertainty associated with that estimate is heavily
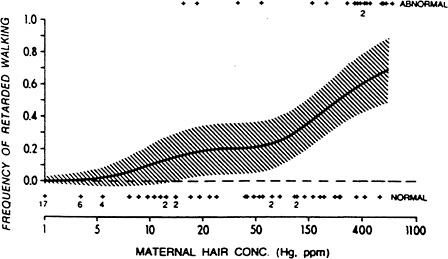
FIGURE 5-1 Nonparametric kernel-smoothing analysis of the relationship between maternal-hair concentration of Hg and retarded walking in the offspring. Maternal-hair concentrations were estimated using XRF single-strand analysis. The exposure value is the maximum level during gestation based on the growth rate of the hair and the birth date of the child. Results from multiple strands were averaged for the final exposure value. The shaded area denotes nonsimultaneous 95% confidence limits for individual points on the smoothed curve (for details, see text). Maternal-hair concentrations for normal and abnormal infants are plotted below and above the graph, respectively. Source: Cox et al. 1989. Reprinted with permission from Environmental Research; copyright 1989, Academic Press.
dependent on the assumed background prevalence of the poor outcomes. (No data were available on the true background prevalence of the poor outcomes among Iraqi children.) For example, for motor retardation, the upper bound of the 95% CI increases from 14 to 190 ppm when the estimate of background prevalence is changed from 0% to 4%. For neurological abnormality, the upper bound of the 95% CI for the threshold estimate is 287 ppm (assuming a 9% background prevalence). In re-analyses of those data, Crump et al. (1995) and Cox et al. (1995) showed that the estimate of population threshold is highly model de-
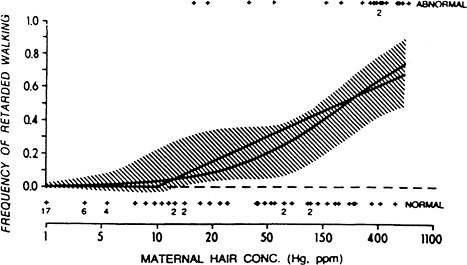
FIGURE 5-2 Plots of the logit and hockey-stick dose-response analysis of the relationship between retarded walking and maternal-hair concentrations during gestation. The two dose-response curves are shown by solid lines. The shaded area represents the 95% confidence limits from kernel smoothing. Source: Cox et al. 1989. Reprinted with permission from Environmental Research; copyright 1989, Academic Press.
pendent, sensitive to the definition of abnormality, and, in the case of delayed walking, heavily influenced by only four cases of delayed walking among children of women with hair Hg concentrations below 150 ppm. The statistical variability of the threshold estimates appears likely to be considerably greater than that provided by Cox et al. (1989). Crump et al. (1995) concluded that the Iraqi data do not provide convincing evidence of any adverse neurodevelopmental effects of MeHg below maternal-hair concentrations of 80 ppm.
In evaluating the Iraqi data, it is important to note that the interviews were conducted when the children were a mean age of 30 months. However, some children must have been considerably older, as the ages at which children in the sample were reported to have walked or talked were as high as 72 months. In addition, birth dates are generally not
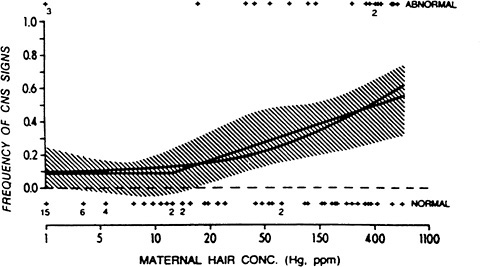
FIGURE 5-3 Plots of the logit and hockey-stick dose-response analysis of the relationship between CNS signs and maternal-hair concentrations during gestation. The two dose-response curves are shown by solid lines. The shaded area represents the 95% confidence limits from kernel smoothing. Source: Cox et al. 1989. Reprinted with permission from Environmental Research; copyright 1989, Academic ress.
important among Iraqi nomads. Therefore, maternal recollection of ages at which children achieved milestones had to be referenced to external events, such as the poisoning. The extent of the imprecision in those data is suggested by the strong digit preferences in the mothers responses. For instance, for 70 of the 78 children, the estimated age at walking was an even number of months. Furthermore, 75% of the estimates were multiples of 6 months. For age of talking, 70 of the 73 responses were an even number of months. (It should be noted, however, that the neurological scores were assigned to the children on the basis of a clinical examination and, therefore, were not subject to recall bias.) Finally, the extent of selection bias in this cohort cannot be charac-
terized, because the size of the base population from which it was drawn and the referral mechanism that brought mothers and children to medical attention are both unknown. For instance, women who knew that they had consumed large amounts of contaminated grain and had concerns about their children's welfare might have come forward, and women who consumed equally large amounts of contaminated grain but whose children were developing well might not have come forward. That issue is critical, because the calculation of a threshold, a reference dose, or a benchmark dose requires a denominator (i.e., the size of the exposed population) as well as the background prevalence of the adverse outcomes to estimate the added risk associated with the exposure of interest. It appears that the background prevalence of developmental abnormality was extremely high among the Iraqi children who participated in the follow-up studies. The prevalence of delayed walking among children whose mothers had hair Hg concentrations below 10 ppm (and can be viewed essentially as a control group for the purpose of estimating background prevalence) was 36% (11 of 31). In contrast, among the population of U.S. children on whom the Bayley Scales of Infant Development (first edition) were standardized, the prevalence of delayed walking by that criterion was approximately 5%. Similarly, the prevalence of delayed talking (two or three words by 24 months) among the Iraqi children was 22% (6 of 27), and 95% of 24-month-old U.S. children in the standardization sample of the MacArthur Communicative Development Inventory were producing approximately 50 words (Fenson et al. 1993).
Chronic Low-Dose-Exposure Epidemiological Studies
A number of epidemiological studies have been carried out on populations exposed chronically to low doses of MeHg. Table 5-10 summarizes some key methodological aspects of those studies. In this section, those studies are discussed in terms of the end points assessed. End points discussed are status on neurological examination, age at achievement of developmental milestones, infant and preschool development, childhood development, sensory, and neurophysiological functions, and other end points in children.
TABLE 5-10 Summary of Developmental Neurotoxicity Studies in Humans
|
Study Site |
Size of Cohort Identified and Enrolled |
Exposure Biomarker |
MeHg or Total Hg Concentration |
Age at Assessment |
Number of Children Assessed |
End Points |
Reference |
|
Amazon |
351 |
Child hair |
Mean, 11.0 ppm; 80% > 10 ppm |
7-12 years |
354 (Table 1) |
Fingertapping, WISC-III: digit span forward, Santa Ana dexterity test, Stanford-inet: copying, bead memory |
Grandjean et al.1999 |
|
Ecuador |
75 (36 children, 39 adults) |
Blood |
Mean, 17.5 mg/L (3.0 in 34 controls) |
Children: 3-15 years Adults: 16-57 years |
19-40 |
Pure tone conduction threshold BAEP |
Counter et al. 1998 |
|
Faroe Islands |
182 |
Maternal hair |
Geometric mean, 4.1 ppm; range, 2.5-7.4 ppm |
2 wk, adjusted for gestational age |
182 |
Neurological exam |
Steuerwald et al. 2000 |
|
Umbilical cord blood |
Geometric mean, 20.4 µg/L; range, 11.8-40.0 µg/L |
||||||
|
Umbilical cord serum |
Geometric mean, 2.5 µg/L; range, 1.7-3.7 µg/L |
||||||
|
1,023 |
Maternal hair |
Geometric mean, 4.3 ppm; interquartile range, 2.6-7.7 ppm |
Maternal interview “during the first year” |
583 |
Developmental milestones |
Grandjean et al. 1995 |
|
French Guiana |
Approx. 400 |
Maternal hair |
Median, 6.6 ppm range, 2.6-17.8 35%>10 ppm |
9 month-12 years |
248 (neuro exam) |
neurological exam fingertapping, Stanford-Binet: block design, copying, bead memory |
Cordier and Garel 1999 |
|
206 (psychological exam) |
MSCA: numerical memory, leg coordination |
||||||
|
Madeira |
149 |
Maternal hair |
Geometric Mean, 9.6 ppm Range, 1.1-54.4 52%> 10ppm |
6-7 years |
146-149 |
BAEP, VP NES: fingertapping, hand eye coordination, continuous performance test WISC-: digit span, block design Stanfford-Binet: bead memory |
Murata et al. 1999a |
|
Mancora, Peru |
369 |
Maternal hair |
Geometric mean, 7.1 ppm; geometric SD, 2.1; range, 0.9-28.5 |
? |
194 (131 with both exposure and outcome data) |
Neurological exam Developmental milestones |
Marsh et al. 1995a |
|
Northern Quebec |
247 |
Maternal hair |
Mean, 6 ppm; 6%, >20 ppm |
12-30 mon |
234 |
Neurological exam |
McKeown-Eyssen et al. 1983 |
|
New Zealand |
10,930 mothers screened, 935 “high” fish consumers identified, 73 8220;high” Hg mothers identified |
Maternal hair |
“High” Hg defined as >6 ppm; mean, 8.3 ppm in “high” Hg oup; range, 6-86 ppm; only 16 values >10 ppm |
4 yr |
74; 38 “high” Hg, 36 “low” Hg, including 30 matched pairs |
DDST, vision, functional neurological exam |
Kjellstrom et al. 1986 |
|
6 yr |
237; 57 complete sets of 1 “high” Hg child, 3 matched controls, and 4 incomplete sets |
WISC-R, TOLD, MSCA, CDS, BWRT, KMDAT, PPVT, EBRS |
Kjellstrom et al. 1989 |
|
Seychelles Islands (pilot) |
804 |
Maternal hair |
Median, 6.6ppm; range, 0.6-36.4 |
5-109 wk |
789 |
Neurological exam, DDST-R |
Myers et al. 1995a |
|
ppm, interquartile range: 6.1 |
66 mon |
217 |
MSCA, PLS, WJTA:LWI, WJTA:AP |
Myers et al. 1995c |
|||
|
Seychelles Islands (main) |
779 |
Maternal hair |
Median, 5.9ppm; interquartile range, 6.0 ppm; all values, <30 ppm |
6.5 mon |
712-737 |
Neurological exam, DDST-R, FTII, visual attention |
Myers.et al. 1995b |
|
19 mon |
738 |
Developmental milestones |
Myers et al. 1997; Axtell et al. 1998 |
||||
|
BSID |
Davidson et al. 1995b |
||||||
|
29 mon |
736 |
BSID |
Davidson et al.1995b |
||||
|
66 mon |
711 |
MSCA, PLS, B-G, WJTA:LWI, WJTA:AP, CBCL |
Davidson et al.1998 |
||||
|
Abbreviations: DDST, Denver Developmental Screening Test (DDST-R is revised version); MSCA, McCarthy Scales of Children's Abilities; PLS, Preschool Language Scale; WJTA, Woodcock Johnson Test of Achievement (AP, applied problems; LWI, letter-word identification); FTII, Fagan Test of Infant Intelligence; BSID, Bayley Scales of Infant Development; B-G, Bender-Gestalt Test; CBCL, Child Behavior Checklist; WISC-R, Wechsler Intelligence Scale for Children-Revised; TOLD, Test of Language Development; CDS, Clay Diagnostic Survey; BWRT, Burt Word Recognition Test; KMDAT, Key Math Diagnostic Arithmetic Test; PPVT, Peabody Picture Vocabulary Test; EBRS, Everts Behaviour Rating Scale; NES, Neurobehavioral Evaluation System; CVLT-C, California Verbal Learning Test-Children; BNT, Boston Naming Test; POMS, Profile of Mood States; VEP, Visual Evoked Potentials; BAEkP, Brainstem Auditory Evoked Responses. |
|||||||
Status on Neurological Examination
McKeown-Eyssen et al. (1983) studied 234 12- to 30-month-old Cree children (95% of eligible children) for whom prenatal MeHg exposure was estimated on the basis of maternal-hair samples. The subjects lived in four communities in northern Quebec. For 28% of the mothers, hair samples were collected during pregnancy; for the balance of the cohort, prenatal exposure was estimated on the basis of hair segments assumed to date from the time the study child was in utero. The measure of exposure used was the maximum concentration of Hg in the segment of hair corresponding most closely to the period from 1 month before conception to 1 month after delivery. The mean maternal-hair Hg concentration was approximately 6 ppm, with 6% of samples exceeding 20 ppm. One of four pediatric neurologists blinded to individual Hg-exposure status, measured height, weight, and head circumference, identified dysmorphologies, and conducted a neurological examination (assessing coordination, cranial nerves, muscle tone, and reflexes). The neurologist made a summary clinical judgment as to the presence of a neurological abnormality. No child was judged to have any abnormal physical findings. Overall, 3.5% (4) of the boys and 4.1% (5) of the girls were considered to have a neurological abnormality. The most frequent abnormality involved tendon reflexes, seen in 11.4% (13) of the boys and 12.2% (14) of the girls. The only neurological findings significantly associated with prenatal MeHg exposure, either before or after adjustment for confounding, were abnormalities of muscle tone or reflexes in boys. Two boys had increased tone in the legs only, five had isolated decreased reflexes, six had generalized decreased reflexes, and two had generalized increased reflexes ( p = 0.05). The risk of an abnormality of tone or reflexes increased 7 times with each 10-ppm increase in prenatal MeHg exposure (95% CI 1.0-51.0). With log transformation of prenatal MeHg exposure, however, the p value associated with the risk of an abnormality due to MeHg exposure increased to 0.14. When exposure was categorized, the prevalence of tone or reflex abnormality did not increase in a clear dose-response manner across categories (i.e., 15.8%, 5.6%, 26.3%, 0%, 7.1%, and 38.5%). In girls, the only association identified was in the unexpected direction between prenatal MeHg exposure and incoordination (60% decrease in probability of incoordination for each 10-ppm increment; odds ratio (OR), 0.3; 95% CI, 0.1-0.9; p = 0.02).
The authors noted five caveats about the one significant adverse association identified: (1) the abnormalities of muscle tone and reflexes in boys were isolated, mild, and of doubtful clinical importance; (2) children exposed to very high MeHg doses manifested as severe generalized neurological disease, including increases in tone and reflexes, rather than the mild, isolated muscle tone and reflex abnormalities (mostly decreased) seen in Cree children; (3) the absence of a coherent dose-response relationship; (4) the absence of consistency across sex; and (5) the possibility that the finding reflects chance, lack of normality in the distribution of the exposure index, or residual confounding.
Infants' status on neurological examination was also evaluated as an end point in a study of 194 children in Mancora, Peru. Although the study was conducted in the early 1980s, it was not published until 1995 (Marsh et al. 1995a). Fish consumption was the primary route of MeHg exposure, and maternal hair was used as the index of exposure (geometric mean, 7.05 ppm; range, 0.9 to 28.5 ppm). Geometric-mean peak hair MeHg concentration was similar (8.34 ppm; range, 1.2 to 30.0 ppm), suggesting that the women were in steady state due to stability in their fish-consumption patterns. Maternal-hair samples and data on child neurological status were available for 131 children. Several elements of the study design are not described, including the size of the eligible population from which the 131 children were sampled, the specific elements of the neurological assessment conducted, and the ages at which the children were examined. However, frequencies are reported for the following end points: tone decreased (two children), tone increased (none), limb weakness (one child), reflexes decreased (one child), reflexes increased (four children), Babinski's sign (an indication of a pyramidal-tract abnormality) (one child), primitive reflexes (none), and ataxia (none). No end point was significantly associated with either mean or peak maternal-hair Hg concentration.
A cross-sectional pilot study was carried out for the Seychelles Child Development Study (SCDS) (Myers et al. 1995a). For 2 years before the start of the study, all women attending an antenatal clinic were asked to provide one or more hair samples during and after pregnancy. A total of 804 infants were subsequently enrolled in the study, and tested during three visits over 2 months in 1987-1988. No data are provided on the size ,of the population from which that sample was drawn. Fifteen infants were excluded due to maternal illnesses during pregnancy (e.g.,
diabetes or eclampsia) or to newborn characteristics thought to place a child at developmental risk (e.g., low birth weight or maternal alcohol ingestion during pregnancy) (Marsh et al. 1995b). A total of 789 infants and children were evaluated between the ages of 5 and 109 weeks by one blinded pediatric neurologist. Mean maternal-hair Hg concentration in the cohort was 6.1 ppm (range, 0.6 to 36.4 ppm). The end points assessed were mental status, attention, social interactions, vocalizations, behavior, coordination, postures and movements, cranial nerves (II-XII), muscle strength and tone, primitive and deep tendon reflexes, plantar responses, and age-appropriate abilities such as rolling, sitting, pulling to stand, walking, and running. The statistical analyses focused on three end points selected due to their apparent sensitivity to prenatal MeHg exposure in the Iraq and Cree studies: overall neurological examination, increased muscle tone, and deep tendon reflexes in the extremities. The overall examination was considered to be abnormal if any findings judged to be pathological were present or if the examiner judged the child's speech or functional abilities to be below age level. Pathological findings included abnormalities of cranial nerves (pupils, extraocular muscles, facial or tongue movement, swallowing, or hearing), alteration in muscle tone or deep tendon reflexes (increase or decrease), incoordination, and involuntary movements. Findings that were not considered to be either normal or pathological were categorized as questionable. Because of the low frequency of abnormal examinations (2.8%), the questionable (11.3%) and abnormal categories were combined. No association was evident between maternal-hair Hg concentration and questionable and abnormal results. The frequency of those results ranged from 16.5% in the group with Hg at 0-3 ppm to 11.7% in the group with Hg at more than 12 ppm. The frequencies of abnormalities of limb tone or deep tendon reflexes were about 8%, and the frequency of both end points did not vary with maternal-hair Hg concentrations in a dose-dependent manner.
The main cohort of the SCDS consisted of 779 mother-infant pairs, representing approximately 50% of all live births during the recruitment period. The final sample size was 740. In addition to 18 infants being excluded for the criteria used in the pilot study, 15 were excluded because of insufficient maternal-hair samples, and 6 were excluded for being a twin. When the infants were 6.5 months old, one blinded pediatric neurologist administered essentially the same neurological exami-
nation that had been used in the pilot phase (Myers et al. 1995b). The overall examination was considered abnormal if changes in muscle tone, deep tendon reflexes, or other neurological features were pathological or if functional abilities were not considered appropriate for the age. An examination could also be coded as questionable. A total of 3.4% (25) of the children had overall neurological scores considered abnormal or questionable, a frequency too low to permit statistical analysis of the overall neurological examination. The frequency of abnormalities was 2% for both limb tone and abnormal deep tendon reflexes. Questionable limb tone was identified in approximately 20% of the children, and questionable deep tendon reflexes, in approximately 15%. Although such findings were not considered pathological, they were combined with abnormal findings for statistical analyses. The frequency of abnormal and questionable findings for limb tone or deep tendon reflexes was not significantly associated with maternal-hair Hg concentrations.
Steuerwald et al. (2000) recruited a cohort of 182 singleton, full-term infants born in the Faroe Islands and evaluated the associations between neurological function at 2 weeks of age and various dietary contaminants and nutrients. The cohort represents 64% of all births in the catchment area. The primary outcome variable was the neurological optimality score (NOS), which reflects an infant's functional abilities, reflexes, responsiveness, and stability of state. In addition, two subscores were generated (muscle tone and reflexes). A variety of thyroidfunction indices considered to be outcomes were also assessed. The exposure biomarkers measured were Hg concentration in maternal hair, cord whole blood, and cord serum. Measurements were also taken of 18 pesticides (or metabolites) and 28 polychlorinated biphenyl (PCB) congeners in maternal serum (lipid adjusted) and breast milk, selenium in cord whole blood, and fatty acids (arachidonic, eicosapentanoic, docosahexaenoic, and total omega) in cord serum. There was a significant inverse relationship between NOS scores and cord-whole-blood Hg concentrations. The mean concentration was 20.4 µg/L (range, 1.9-102 µg/L) (see Figure 5-4). Although the unadjusted correlation between cord-whole-blood Hg concentration and NOS score was modest (- 0.16), a 10-fold increase in cord-whole-blood Hg was associated with the equivalent of a 3-week reduction in gestational age based on NOS score. Adjustments for total PCBs and fatty acid concentrations did not appreciably affect the results. Selenium did not appear to function as an effect
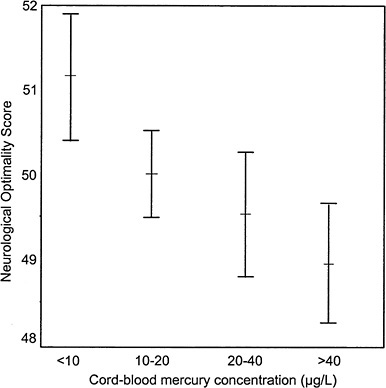
FIGURE 5-4 Neurological optimality score (mean ± standard error of the mean) in relationship to cord-blood Hg concentrations in approximate quartile groups. Source: Stewerwald et al. 2000. Reprinted with permission from the Journal of Pediatrics; copyright 2000, Mosby, a Harcourt Health Sciences Company.
modifier. Muscle-tone and reflexes subscores were not significantly associated with any exposure biomarker. Maternal hair-Hg concentrations (mean, 4.08 ppm; range, 0.36-16.3 ppm; 10.4%, more than 10 ppm) were not significantly associated with NOS scores.
A functional neurological examination, as part of a general physical examination, was administered at age 7 years to another cohort of children from the Faroe Islands. The cohort consisted of consecutive deliveries at three hospitals during a 21-month period between 1986 and
1987. Of 1,386 infants born, cord-blood and maternal-hair samples were obtained from 1,022 singleton births (75%) and 917 children were examined (66%) (Grandjean et al. 1992). The mean cord-blood Hg concentration was 22.9 µg/L; the mean maternal-hair Hg concentration was 4.3 ppm. In particular, the examination of the cohort at 7 years of age focused on motor coordination and perceptual-motor performance (Dahl et al. 1996). The coordination tests included diadochokinesia (fast pronation and supination), reciprocal coordination (alternately closing and opening the fists), and finger opposition (the pulpa of the thumb touching the pulpa of the other fingers of the same hand). The perceptual-motor tests included catching a ball with a diameter of 15 cm thrown from a distance of 4 m, finger agnosia, and double finger agnosia. Results were scored as automatic or questionable and poor. Hg concentration was not significantly associated with the number of tests on which a child's performance was considered automatic. On the tests of reciprocal motor coordination, simultaneous finger movement, and finger opposition, fewer than 60% of the children achieved a score of automatic. Finger opposition, however, was the only test in which children with questionable and poor performance (425 children) had a significantly higher mean Hg concentration than children with automatic performance (465 children) (23.9 versus 21.8 µg/L, p = 0.04) (Grandjean et al. 1997).
Cordier and Garel (1999) recently reported on the association between MeHg exposure and neurological status in 9-month-old to 6-year-old children living in gold-mining regions of French Guiana. The concentrations of Hg in samples of hair collected from children's mothers at the time of the study were used as a surrogate for exposure during pregnancy. The median concentration was 6.6 ppm (range, 2.6-17.8 ppm; 35%, greater than 10 ppm). Among children 2 years of age and older, the prevalence of increased reflexes was significantly higher with increased Hg concentrations in maternal hair, the association being stronger in boys than in girls. When 10 children who had been found to have increased reflexes were re-examined 9 months later by a different examiner, only three were considered to have increased reflexes. Therefore, the investigators advised caution in interpreting those data.
Overall, the evidence that children's neurological status is associated with low-dose prenatal Hg exposure consists of four findings: (1) an increased prevalence of tone or reflex abnormalities (most often de-
creased) in boys with increased maternal-hair Hg concentrations, although that effect is not dose dependent (McKeown-Eyssen et al. 1983); (2) an inverse association between newborns' NOS and umbilical-cord Hg concentration in the Faroe Islands (Steuerwald et al. 2000); (3) a modest but statistically significant increase (2.1 µg/L) in the mean cord-blood Hg samples of 7 year olds who performed suboptimally on a finger opposition test compared with Children whose performance was normal (Grandjean et al. 1997); and (4) an association, especially in boys, between increased reflexes and higher maternal-hair Hg concentrations in a cohort of 9-month-old to 6-year-old children in French Guiana (Cordier and Garel 1999). One limitation in the use of neurological status as an end point is its categorical nature; a child either expresses a particular abnormality or does not. In the SCDS main cohort, the prevalence of abnormal neurological findings was quite low (i.e., 3.4% for abnormal or questionable findings), limiting the statistical power of hypothesis testing. Although the high-dose exposure episodes that occurred in Minamata and Iraq produced classic signs of neurological dysfunction in children exposed in utero, the low doses of MeHg to which the cohorts in the epidemiological studies were exposed prenatally appeared to be associated with subtle neurological effects that are of uncertain clinical significance (e.g., tone or reflex abnormalities). Research on other environmental toxicants such as lead and PCBs has shown, however, that it is important to distinguish individual risk from population risk. A decrement in mean function that is too small to be clinically significant for the individual child might be quite important when it is considered from the standpoint of the impact on the population distribution of the affected function (Weiss 1998).
Age at Achievement of Developmental Milestones
The association between the achievement of developmental milestones and prenatal MeHg exposure was evaluated in the main cohort of the SCDS by Myers et al. (1997) and Axtell et al. (1998). The ages at which a child was able to walk without support and to say words other than “mama” or “dada” were determined by an interview with a child's primary caregiver (person with whom the child spent 5 or more nights per week) conducted at the 19-month evaluation. Those data
were available for 738 of the 779 children enrolled. Prenatal MeHg exposure was estimated as the total Hg in the single longest hair segment dating from the time the study child was in utero (mean, 5.8 ppm; range, 0.5 to 26.7 ppm; 22%, greater than or equal to 10 ppm). Several statistical approaches were carried out, including a standard multiple regression of a log transformation of the age at milestone achievement, hockey-stick models estimating the threshold maternal-hair Hg concentration associated with delay in milestone achievement, and logistic regression analyses of delayed walking, a binary variable in which an abnormal response was defined as greater than 14 months. The mean age at which a child was considered to talk was not significantly associated with maternal-hair Hg in any of the models tested. In regressions stratified by child sex, a positive association was found between age at walking and maternal-hair Hg in boys (p = 0.043) but not in girls. A term for the interaction between Hg and sex was not statistically significant in the analyses of the complete cohort, however. The magnitude of the delay in the age at which boys walked was viewed by the authors as clinically insignificant; a 10-ppm increase in maternal-hair Hg was associated with an approximate 2-week delay in walking (see Figure 5-5). The association in boys was not significant when four statistical outliers were excluded from the analysis. Hockey-stick models provided no evidence of a threshold, as the fitted curves were essentially flat. A child's risk of delayed walking was not associated with maternal-hair Hg concentration. Axtell et al. (1998) re-analyzed those milestone data, applying semiparametric generalized additive models, which use smoothing techniques to identify nonlinearities. Those models are less restrictive than the approaches used by Myers et al. (1997), whose approaches make strong assumptions about the true functional form of a relationship.
The major finding of the analyses of Axtell et al. (1998) was that the association between age at walking and maternal-hair Hg in boys was nonlinear, walking appearing at a later age as concentrations increased from 0 to 7 ppm but at a slightly earlier age as Hg concentration increased beyond 7 ppm. The size of the effect associated with the increase from 0 to 7 ppm was very small, corresponding to a delay of less than 1 day in the achievement of walking. Because a coherent dose-response relationship did not hold above 7 ppm, the authors expressed

FIGURE 5-5 Plot of partial residuals for log of age at walking versus maternal-hair Hg concentrations for the reduced model with Hg by gender interaction. The partial residual is the natural log of the subject's age at walking adjusted for all variables in the model except Hg. It is computed by adding the Hg effect (estimated coefficient on Hg times the Hg value for that subject) to the raw residual (observed value minus predicted value) obtained from the reduced model. The partial residuals have been rescaled by adding the mean value of log of age at walking to each partial residual. The axis for age at walking (in months) is on a log scale. Outliers are identified on the plot with a different symbol (solid squares). The slope of the solid lines is the regression coefficient for Hg in the originial regression analysis with statistical outliers. The dotted line is the slope with those outliers removed. Source: Myers et al. 1997. Reprinted with permission from NeuroToxicology; copyright 1997, Intox Press.
doubt that the association found below 7 ppm reflected a causal effect of Hg exposure on age at walking.
Data on developmental milestones were collected in the Peruvian study conducted by Marsh et al. (1995a). The ages of the children when mothers were queried about the milestones are not stated, although the study was conducted prospectively and data were apparently collected in an ongoing manner over the course of a woman's visits to a postnatal clinic. Regression analyses, including analyses stratified by child sex, did not reveal any significant associations between maternal-hair Hg concentrations and the ages at which children sat, stood, walked, or talked. The geometric mean maternal-hair Hg concentration was 7.05 (S.D. = 2.06). The rates of developmental retardation, especially in speech (13 of 131), were substantial, although the criteria used to define that outcome were not provided. Children's birth weight, height, and head circumference were also unrelated to maternal-hair Hg concentrations.
Ages at milestone achievement of motor development were investigated in a 21-month birth cohort (1022 infants, 1986-1987) of children in the Faroe Islands (Grandjean et al. 1995). Milestone data were obtained from maternal interviews and the observations of district health nurses who visited the homes on several occasions during the children's first year of life. Hg concentrations were determined in maternal-hair samples at delivery, infants' umbilical cord blood, and in children's hair samples obtained at about 12 months of age. Complete data were available for 583 children (57% of the complete cohort). Three motor-development milestones commonly achieved between 5 and 12 months of age were selected for analysis: “sits without support,” “creeps,” and “gets up into standing position with support.” The age at achievement was not significantly associated with either index of prenatal Hg exposure (cord-blood or maternal-hair concentrations) for any of the three milestones. For all three milestones, however, a significant inverse association was found between age at achievement and children's hair Hg concentration at 12 months. Children's hair Hg concentration was interpreted as an index of children 's postnatal exposure to MeHg. Nursing was associated with both higher hair Hg concentrations in children at 12 months of age and with more rapid achievement of milestones. Therefore, the authors concluded that the inverse associa-
tion reflected residual confounding by duration of breast feeding. That finding suggests that the beneficial effects of nursing on early motor development are sufficient to compensate for any slight adverse impact that low-dose prenatal MeHg exposure might have on the end points.
In conclusion, recent epidemiological studies provide scant evidence that prenatal MeHg exposures, at least those resulting in maternal-hair Hg concentrations below 30 ppm, are associated with the ages at which children achieve developmental milestones. Although the mean age at walking in the SCDS cohort was later among children whose mothers had high hair Hg concentrations, that association was limited to boys, and the risk of late walking did not appear to be dose related. The association was apparent only at concentrations below 7 ppm, and increases in maternal-hair Hg concentrations above 7 ppm were not associated with further delay in walking age of boys. In the Faroe Islands cohort, a negative association was found between children 's hair Hg concentration at 12 months and age at achievement of three motor-development milestones. That finding might be due to higher Hg exposure among breast-fed children and might actually reflect beneficial nutritional effects from breast milk. Those recent data are consistent with re-analyses of the Iraqi data (Cox et al. 1995; Crump et al. 1995), suggesting that the population thresholds for delayed achievement of milestones that were originally calculated might be too low. The thresholds appear to be highly dependent on the assumptions made about background prevalence of delay, the definition of late achievement used, and the influence exerted by a small number of data points.
Infant and Preschool Development
In several epidemiological studies, the association between low-dose prenatal MeHg exposure and early child development has been assessed using several widely used standardized tests.
In the Cree study reported by McKeown-Eyssen et al. (1983), the Denver Developmental Screening Test (DDST) was administered to the 12- to 30-month-old children in the cohort. Scores were reported as the percentage of items passed on each subscale (gross-motor, fine-motor, language, and personal and social subscales) and on the entire test.
Although quantitative estimates are not provided for the associations between test scores and maternal-hair Hg concentrations (mean, 6 ppm; 6% greater than 20 ppm), the authors reported that they did not find any significant associations in a direction compatible with an adverse effect of MeHg either before or after adjustment for confounding variables.
Kjellström et al. (1986) studied a cohort of New Zealand children for whom prenatal MeHg exposure was estimated on the basis of maternal-hair samples as well as dietary questionnaires collected during the period when the study child was in utero. Although exposure information was collected on nearly 11,000 women, the authors focused on 935 women who reported eating fish more than three times per week during pregnancy. Seventy-three women had hair Hg concentrations greater than 6 ppm. The 74 children of those women were designated as the “high-Hg group.” Efforts were made to match each child in the high-Hg group with a reference child on the basis of maternal ethnicity, hospital of birth, maternal age, and child age. In the follow-up evaluations completed when children were 4 years old, 38 exposed and 36 reference children were tested, including 30 complete matched pairs. On the DDST, the primary outcome used at this age, 52% of the children in the high-Hg group had an abnormal or questionable result compared with 17% of the children in the control group (p < 0.05). That result corresponds to an odds ratio of 5.3. Results were similar when pairs that were poorly matched on ethnicity were excluded. It was not possible to identify the specific developmental domains in which performance was most strongly associated with maternal-hair Hg concentrations.
In the SCDS pilot cross-sectional study, a revised version of the DDST (the DDST-R) was administered blindly by one examiner to 789 children between the ages of 1 and 25 months (Myers et al. 1995a). No association was found between maternal-hair Hg concentration during pregnancy (mean 6.6 ppm) and DDST-R results when normal and questionable examinations were combined in the conventional manner, although the prevalence of abnormal findings was so low (three children, less than 1%) that statistical analysis was not meaningful. When abnormal and questionable results were grouped (in 65 children, 8%), as was done in the New Zealand study (Kjellström et al. 1986), however, high maternal-hair Hg concentrations were significantly associated with poor outcomes (p = 0.04, one-tailed test). That result was largely attributable
to the higher frequency of abnormal and questionable results (approximately 13%) among children in the highest hair-Hg category (greater than 12 ppm), in contrast to the frequency of approximately 7% among children in each of the other four Hg groups (0-3, 3-6, 6-9, and 9-12 ppm).
In the main SCDS study, the DDST-R was administered by one blinded examiner to a cohort of 740 children at age 6.5 months (mean maternal-hair Hg concentration during pregnancy, 5.9 ppm; interquartile range, 6.0 ppm) (Myers et al. 1995b). The frequencies of examinations considered to be abnormal (three children, 0.4%) or questionable (11 children, 1.5%) were very low, precluding meaningful statistical analysis of the DDST-R data. The Fagan Test of Infant Intelligence (FTII), an assessment of visual-recognition memory or novelty preference, was also administered at 6.5 months to 723 children. The mean percent novelty preference in the entire cohort was 60%, similar to that observed in many other cohorts, and varied by less than 1% across categories of maternal-hair Hg concentration (less than 3 ppm to greater than 12 ppm). Visual attention (the time required to reach visual-fixation criterion on familiarization trials) also was unrelated to maternal-hair Hg concentrations.
The Bayley Scales of Infant Development (BSID) was administered by blinded examiners to children in the SCDS cohort at ages 19 and 29 months (738 at 19 months and 736 at 29 months) (Davidson et al. 1995b). In addition, at 29 months, six items of the Infant Behavior Record (IBR), a rating scale, were completed by the examiner, assessing activity level, attention span, responsiveness to examiner, response to caregiver, cooperation, and general emotional tone. The BSID yield two primary scores: the mental development index (MDI) and psychomotor development index (PDI). At both ages, MDI scores (97.5 and 100.4 at 19 and 29 months, respectively) were similar to the expected mean for U.S. children of 100 ± 16. At both ages, however, the SCDS children performed markedly better on PDI (with scores averaging 126.7 and 121.1 at 19 and 29 months, respectively) than the expected mean for U.S. children. In fact, at 19 months, approximately 200 children in the SCDS cohort achieved the highest possible PDI score of 150 (Davidson et al. 1995a), a finding that most likely reflects the ethnic composition of the cohort. Because of this skew, PDI scores at both ages were expressed as a binary
variable, splitting the distribution at the median score. The MDI scores at 19 or 29 months were not significantly associated with maternal-hair Hg concentration during pregnancy (see Figure 5-6). Similar results were obtained in a secondary analysis that included only children with the lowest (less than or equal to 3 ppm) or highest (greater than 12 ppm) maternal-hair Hg concentrations. Assessments of perceptual skills at 19 months (Kohen-Raz method), dichotomized due to skewing, were not associated with Hg exposure. Scores on that test at 29 months could not be evaluated because of a pronounced ceiling effect. Risk of a PDI score below the median was not significantly associated with maternal-hair Hg concentration in the full logistic regression model but was associated (p = 0.05) with this exposure index in a reduced model in which adjustment was made for a smaller number of covariates selected on an a priori basis. The secondary analysis of the PDI scores of children with the lowest and highest Hg concentrations was not conducted, because the full logistic regression model was not statistically significant.
In the analyses of the six IBR items, maternal-hair Hg concentration was significantly associated only with examiner ratings of activity level during the test session and only in males. The score decreased 1 point (on a 9-point scale) for each 10 ppm. Additional analysis of the data of the main SCDS study cohort failed to identify significant effect modification by factors such as caregiver intelligence, H.O.M.E. score, family income, and gender (Davidson et al. 1999).
Among the four studies that used the DDST (or DDST-R) as a measure of infant development, only in the New Zealand study and the SCDS pilot phase did children's scores appear to be associated with prenatal Hg concentrations, at least when the questionable and abnormal findings were combined. One factor that might partially account for the differences between the findings of those studies is the age at which the examinations were conducted (4 years in the New Zealand study, 1 to 25 months in the SCDS pilot phase and 6.5 months in the SCDS main phase). Another factor is the different rates of abnormal or questionable examinations (50% of the New Zealand group with prenatal maternal-hair concentrations greater than 6 ppm and 17% of controls; 8% of the Seychelles complete cohort in the SCDS pilot phase; and 1.9% of the cohort in the SCDS main phase). That difference is large enough to raise the possibility that the test items were either administered differently in
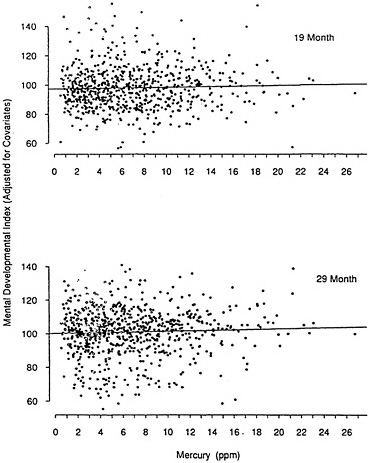
FIGURE 5-6 The 19-month and 29-month mental-developmental-index (MDI) partial residuals from the Bayley Scales of Infant Development. Each data point represents the overall cohort MDI mean plus the partial residual. The partial residual is defined as the subject's MDI score adjusted for all variables in the reduced model except Hg (computed by adding the Hg effect to the residual from the reduced model). The MDI has a U.S. mean of 100 (standard deviation, 16). Scores are plotted as a function of maternal-hair Hg in parts per million. The slope for the 19-month MDI, shown in the upper graph, was 0.125. The slope for the 29-month MDI, shown in the lower graph, was 0.149. Neither effect was significant. Source: Davidson et al. 1995b. Reprinted with permission from NeuroToxicology; copyright 1995, Intox Press.
the two studies or that different criteria were used in judging whether an individual passed or failed the tests. Kjellström et al. (1986) reported, however, that among 3- and 4-year-old children in South Auckland routinely assessed with the DDST, the rate of questionable, abnormal, or not testable results was 8-14%, roughly comparable to the rates observed among the low-Hg children in the study sample.
In general, the use of screening tests, such as the DDST, in neurobehavioral toxicology studies is not recommended because of their insensitivity to variations within the range of normal performance (Dietrich and Bellinger 1994). More detailed instruments, such as the BSID, currently considered to be the best in infant assessment, have proved to be sensitive to prenatal exposures to a variety of neurotoxicants, including lead (Bellinger et al. 1987; Dietrich et al. 1987; Wasserman et al. 1992) and PCB's (Rogan and Gladen 1991; Koopman-Esseboom et al. 1996). Among the Hg studies, the BSID was administered only in the SCDS, and no significant associations were found between children's scores and their prenatal exposures. It is notable that the PDI scores were very high in this cohort, requiring that the distribution be split at the median and analyzed as a categorical variable. The median value is not provided by Davidson et al. (1995b), but, based on Figure 3 in Davidson et al. (1995a), appeared to be approximately 130, or 2 standard deviations above the expected population mean.
Childhood Development
Children in the New Zealand cohort were followed up at 6 years of age. In that phase of the study, three controls were matched to each high-Hg child on the basis of ethnic group, sex, maternal age, maternal smoking, area of maternal residence, and the duration of maternal residence in New Zealand. One of the controls for each subject had a hair Hg concentration of 3 to 6 ppm, and the other two controls had hair Hg concentrations of 0 to 3 ppm. For one of the two low-Hg controls, maternal fish consumption was high (more than three times per week), and for the other, it was low. Fifty-seven fully matched groups of four children each and four incomplete sets (resulting in a cohort of 237 children) participated in a follow-up evaluation of neurodevelopmental status at 6 years of age (Kjellström et al. 1989). In the high-Hg group,
the mean maternal-hair Hg concentration was 8.3 ppm (range 6-86 ppm, with all but 16 between 6 and 10 ppm). Extensive information was collected on possible confounding factors, such as social class, medical history, and nutrition. A battery of 26 psychological and scholastic tests was administered, assessing the domains of general intelligence, language development, fine- and gross-motor coordination, academic attainment, and social adjustment. Multiple regression analyses of five primary end points were carried out: the Test of Language Development — spoken language quotient (TOLD_SL), the Wechsler Intelligence Scale for Children-Revised (WISC-R) performance IQ, the WISC-R full-scale IQ, the McCarthy Scales of Children's Abilities perceptual-performance scale (MC_PP), and the McCarthy Scales motor scale. Analyses were adjusted for potential confounders, including maternal ethnic group, maternal age, maternal smoking and alcohol use during pregnancy, length of maternal residence in New Zealand, social class, primary language, siblings, sex, birth weight, fetal maturity, Apgar score, and duration of breast feeding. In addition, robust regression methods were applied, involving the assignment of a weight (0 to 1) to an observation depending on the degree to which it was an outlier. In the robust regressions, maternal-hair Hg concentration was associated with poorer scores (p values ranging from 0.0034 to 0.074) on full-scale IQ, language development (spoken language quotient), visual-spatial skills (perceptual-performance scale) and gross-motor skills (motor scale). The unweighted regression analyses yielded findings that were similar in direction, although generally less statistically significant. The poorer mean scores of the children in the high-Hg group appeared to be largely attributable to the children whose mothers had hair Hg concentrations above 10 ppm (for whom the mean average hair Hg concentration during pregnancy was 13 to 15 ppm and the mean of the peak monthly hair segments was about 25 ppm). Maternal-hair Hg concentrations accounted for relatively small amounts of variance in the outcome measures and generally accounted for less than covariates, such as social class and ethnic group. In additional analyses of that data set, Crump et al. (1998) found that when maternal-hair Hg was expressed as a continuous rather than a binary variable, none of the 5 primary end points studied by Kjellstr öm et al (1989) were associated with Hg at p < 0.10. The results were heavily influenced, however, by the data of a child with a maternal-hair Hg concentration of 86 ppm (more than 4
times the next highest concentration), despite the fact that the child's test scores were not outliers by the usual technical criteria. When the data for this child were excluded, scores on the TOLD_SL and MC_PP were inversely associated with maternal-hair Hg concentration at p < 0.05. These associations were diminished somewhat in statistical significance, although not in the magnitude of the coefficient, when parental education and child's age at testing were included in the regressions. When these regressions were repeated on all 26 scholastic and psychological tests, 6 were associated with maternal hair-Hg (excluding the child with a level of 86 ppm) at p < 0.10: Clay Reading Test — concepts, Clay Reading Test — letter test, McCarthy Scales — general cognitive index, McCarthy Scales — perceptual-performance scale, Test of Language Development — grammar completion, and Test of Language Development — grammar understanding).
Several features of the New Zealand study are noteworthy, including the efforts made to collect data on potential confounding variables and the broad battery of standardized outcome measures administered by trained examiners. In contrast to the acute high-dose exposures experienced by the Iraqi population, the MeHg exposures of the New Zealand cohort were chronic, low dose, and most likely fairly constant over time, reflecting well-established food consumption patterns. In addition, the maternal-hair Hg concentrations were measured prospectively. As part of the SCDS pilot phase, children from the pilot cohort of 789 who turned 66 months old within a 1-year time window underwent developmental assessments (Myers et al. 1995c). Of the 247 eligible children, 217 (87.9%) were administered a test battery consisting of the McCarthy Scales of Children's Abilities, the Preschool Language Scale, and two subtests of the Woodcock-Johnson Tests of Achievement: letter-word identification and applied problems. All 73 children with maternal-hair Hg concentrations greater than or equal to 9 ppm or less than or equal to 4 ppm were assessed. The median maternal-hair Hg concentration in that subsample of the pilot cohort was 7.1 ppm (1.0 to 36.4). The frequency of missing values was substantial for some end points (e.g., 34% for the summary score of the general cognitive index (GCI) yielded by the McCarthy scales). Increased maternal-hair Hg concentrations were associated with significantly lower GCI scores (p = 0.024). Scores declined approximately 5 points between the lowest (3 ppm or less) and highest (greater than 12ppm) exposure categories. A similar association
was found on the perceptual-performance scale of the McCarthy scales (p = 0.013). Children's scores on the auditory comprehension scale of the Preschool Language Scale were also inversely associated with maternal-hair Hg concentrations (p = 0.0019). Scores declined approximately 2.5 points across the range of Hg concentrations. Additional analyses identified several outlier or influential data points, whose exclusion from the analyses reduced the estimates of the Hg effect substantially, sometimes to nonsignificance. In the pilot phase of the SCDS, information was not collected on several key variables that frequently confound the association between neurotoxicant exposures and child development. Those variables are socioeconomic status, caregiver intelligence, and quality of the home environment.
In the main SCDS, 711 children (91.2%) from the original cohort of 779 were evaluated at 66 months of age (5.5 years) ± 6 months using a battery of standardized neurodevelopmental tests (Davidson et al. 1998). The major domains assessed (and the tests used) were general cognitive ability (McCarthy Scales of Children's Abilities), expressive and receptive language (Preschool Language Scale), reading achievement (letter-word recognition subtest of the Woodcock-Johnson Tests of Achievement), arithmetic (applied problems subtest of the Woodcock-Johnson Tests of Achievement), visual-spatial ability (Bender Gestalt Test), and social and adaptive behavior (Child Behavior Checklist). Total Hg in a segment of maternal hair taken during pregnancy was the measurement of prenatal MeHg exposure (mean, 6.8 ppm; range, 0.5-26.7 ppm). Total Hg in a 1-cm segment of hair obtained from a child at 66 months served as the measurement of postnatal MeHg exposure (mean, 6.5 ppm; range, 0.9-25.8 ppm). The pattern of scores of the six primary end points did not suggest an adverse effect of either prenatal or postnatal Hg exposure. The associations that were found were consistent with enhanced performance among children with increased exposure to MeHg (see Figure 5-7 and Figure 5-8). For the total score on the Preschool Language Scale, increased prenatal and postnatal Hg concentrations were significantly associated with better scores (both p = 0.02). For the applied problems score, increased postnatal Hg concentrations were associated with better scores (p = 0.05). Among boys, increased postnatal Hg concentrations were associated with fewer errors on the Bender Gestalt Test (p = 0.009) (see Figure 5-8).
The R2 (square of the multiple correlation coefficient) value (0.10) of
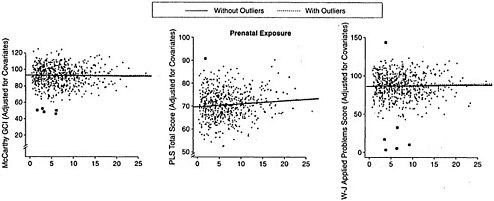
FIGURE 5-7 Partial residuals for prenatal exposure. The measures are the McCarthy Scales of Children's Abilities general cognitive index (GCI), the Preschool Language Scale (PLS)total score, and the Woodcock-Johnson (W-J) applied problems subtest. Each test score was added to the resulting partial residual. The slope of the line in the plot is the regression coefficient for the multiple regression model. Slopes are shown for the model with and without outliers. Black squares indicate outliers. Source: Davidson et al. 1998. Reprinted with permission from the Journal of the American Medical Association; copyright 1998, American Medical Association.
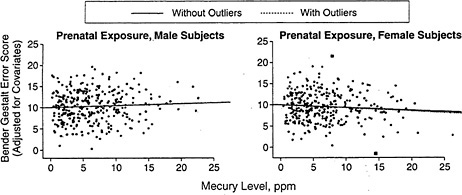
FIGURE 5-8 Partial residuals for prenatal exposure. The measures are Bender Gestalt error scores for male and female subjects. Each test score was adjusted for all reduced model predictors except the exposure value used in the plot. For graphical representations, the overall mean test score was added to the resulting partial residual. The slope of the line in the plot is the regression coefficient for the multiple regression model. Slopes are shown for the model with and without outliers. Black squares indicate outliers. Source: Davidson et al. 1998. Reprinted with permission from the Journal of the American Medical Association; copyright 1998, American Medical Association.
the reduced regression model for the GCI score in the main SCDS study was identical to that in the pilot study. That also appeared to be true for scores on the Preschool Language Scale (R2 of 0.12 for the auditory comprehension scale in the pilot study and 0.14 for total score in the main study). That finding is puzzling because the pilot-study models, as noted previously, did not include several key covariates, including socioeconomic status, caregiver intelligence, and the quality of the home environment, and because the regression coefficients for socioeconomic status and caregiver intelligence were statistically significant for total scores of the GCI and the Preschool Language Scale in the main study cohort. Those differences suggest that maternal-hair Hg concentration is very highly confounded with those key covariates in the Seychelles population, or they suggest that the associations between child neurodevelopment and the covariates differ substantially in the pilot and main study cohorts, or both.
In the Faroe Islands cohort, comprehensive evaluations were con-
ducted at approximately 7 years of age on 917 (90.3%) of the surviving members of a 1986-1987 birth cohort of 1,022 singleton births (Grandjean et al. 1997). The neuropsychological battery included three computer-administered tests from the Neurobehavioral Evaluation System (NES) (finger tapping, hand-eye coordination, and continuous performance test), the Tactual Performance Test, three subtests of the WISC-R (digit span, similarities, and block design), the Bender Gestalt Test, the California Verbal Learning Test — Children, the Boston Naming Test, and the Nonverbal Analogue Profile of Mood States. Parents were administered selected items from the Child Behavior Checklist. The primary measure of MeHg exposure was the concentration of Hg in umbilical cord blood (geometric mean, 22.9 µg/L; interquartile range, 13.4-41.3 µg/L; 894 measurements). Measurements were made of the concentration of Hg in maternal hair at parturition (geometric mean, 4.3 ppm; interquartile range, 2.6-7.7 ppm; N = 914), child hair at 12 months of age (geometric mean, 1.1 ppm; interquartile range, 0.7-1.9 ppm, N = 527), and child hair at 7 years (geometric mean, 3.0 ppm; interquartile range, 1.7-6.1 ppm, N = 903).
Not all children were able to complete all tests, and, in some cases, failure was associated with significantly increased Hg concentrations (e.g., finger opposition test and mood test). In multiple regression analyses, increased cord-blood Hg concentration was significantly associated with worse scores on finger tapping (preferred hand, p = 0.05), continuous performance test in the first year of data collection (false negatives, p = 0.02; mean reaction time, p = 0.001), WISC-R digit span (p = 0.05), Boston Naming Test (no cues, p = 0.0003; with cues, p = 0.0001), and the California Verbal Learning Test — Children (short-term reproduction, p = 0.02; long-term reproduction, p = 0.05). On the basis of the regression coefficients for Hg and age, the investigators estimated that a 10-fold increase in cord Hg concentration was associated with delays of 4 to 7 months in those neuropsychological domains (thus a doubling of Hg with delays of 1.5-2 months).
For two end points (WISC-R block design, Bender Gestalt Test errors), associations indicating adverse Hg effects (p < 0.05) were found when an alternative approach to adjustment for confounders (Peters-Belson method) was applied. Results were similar when the 15% of the cohort with maternal-hair Hg concentrations greater than 10 ppm were excluded from the analyses. A term for the interaction between Hg and
sex was not statistically significant, indicating that the Hg effects were similar among boys and girls. In general, children's test scores were more strongly associated with cord-blood Hg concentration than with maternal-hair Hg concentration or with Hg concentrations in samples of children's hair collected at 1 and 7 years of age. Five tests were selected, on the basis of high psychometric validity, to represent key domains of cognitive function: motor, attention, visual-spatial ability, language, and memory. For the tests selected to represent attention, language, and memory, the percentages of children with adjusted scores in the lowest quartile increased significantly as cord-blood Hg concentration increased (see Figure 5-9).
In an additional set of analyses (Grandjean et al. 1998), the investigators compared the neuropsychological scores of two groups of children: a case group of 112 children with maternal-hair concentrations of 10 to 20 ppm (median, 12.5 ppm) at parturition, and a control group of 272 children with maternal-hair Hg concentrations less than 3 ppm (median, 1.8 ppm) matched to cases on age, sex, year of examination, and care-giver intelligence. Median cord-blood Hg concentrations also differed substantially (59.0 µg/L in the case group versus 11.9 µg/L in the control group). On 6 of the 18 end points, the case group scored significantly lower than the control group (one-tailed p value of 0.05). Those end points were finger tapping (both hands), hand-eye coordination (average of all trials), WISC-R block design, Boston Naming Test (no cues, cues), and California Verbal Learning Test — Children (long-term reproduction). The results of those analyses differ in certain respects from those of the main analyses. First, the set of end points on which the cases and controls differed is similar but not identical to the set of end points that were significantly associated with cord Hg concentration found in the main analyses. Moreover, in contrast to the main analyses, a term for the interaction between Hg and sex was statistically significant for several scores, including the Bender Gestalt Test error score, short-term reproduction on the California Verbal Learning Test — Children, all three finger-tapping conditions, continuous-performance-test reaction time, and average hand-eye coordination score. For all scores, adverse Hg effects were noted for boys but not girls.
Grandjean and colleagues assembled an additional study cohort of 351 children 7 to 12 years old from four riverine communities in Amazonian Brazil (Rio Tapajos) with increased exposures to MeHg due to the
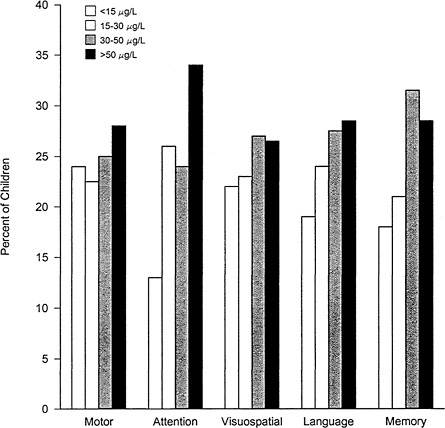
FIGURE 5-9 Prenatal Hg exposure concentrations (in quartile groups) of Faroe Island children with scores in the lowest quartile after adjustment for confounders. For each of five major cognitive functions, one neuropsychological test with a high psychometric validity was selected. Motor: neurobehavioral evaluation system 2 (NES2) finger tapping with preferred hand (p value for trend, 0.23). Attention: Reaction time on the NES2 continued performance test (p = 0.003). Visual-spatial: Bender visual motor gestalt test error score (p = 0.16). Language: Boston Naming Test score after cues (p = 0.02). Memory: California Verbal Learning Test — Children long-delay recall (p = 0.004). Source: Adapted from Grandjean et al. 1997.
consumption of fish contaminated by upstream gold-mining activities (Grandjean et al. 1999). Among children, the mean hair Hg concentration ranged from a geometric mean (range) of 11.9 (35.1) ppm for the lowest exposed of the three communities on the Rio Tapajos to 25.4 (82.9) ppm for the highest; 80% of the children in these villages exceeded 10 ppm. Most of the children reportedly ate fish for two meals per day. In the hair samples available for 63% of the children's mothers, the mean Hg concentration was 11.6 ppm. The battery of neurobehavioral tests administered to the children focused on motor function, attention, visual-spatial function, and short-term memory (finger tapping, Santa Ana dexterity test, WISC-III digit span forward, and Stanford-Binet copying (including recall), and bead memory subtests. In three villages, the tests were administered in Portuguese, although in the fourth (Village D), administration required the services of a Mundurucu interpreter. (The finger tapping, and Santa Ana dexterity tests could not be administered to children in that village.) Combining all four villages, children's hair Hg concentrations were significantly associated with their scores on finger tapping (both preferred and other hand; both p < 0.001), Santa Ana dexterity test (preferred hand, p = 0.005; other hand, p = 0.05), WISC-III digit span (p = 0.001), Stanford-Binet copying (p < 0.001) and recall (p < 0.001), and Stanford-Binet bead memory (p < 0.001). Adjustment for community generally reduced the magnitude of the associations, sometimes dramatically (e.g., from p < 0.001 to p = 0.99 for finger tapping preferred hand). Hair Hg concentrations and village of residence were so highly confounded, however, that adjustment for village might be inappropriate.
In the French Guiana cohort assembled by Cordier and Garel (1999) 206 children 5 to 12 years old were administered a battery of neuropsychological tests that included finger tapping, three subtests from the Stanford-Binet (block designs, copying designs, and bead memory), and two subtests from the McCarthy scales (numerical memory and leg coordination). Median maternal-hair concentration was 6.6 ppm (range, 2.6-17.8 ppm). With adjustment for potential confounders, increased Hg concentrations were associated with copying-design score especially in boys. The findings are complicated, however; when only the children living in the region that has higher exposures were considered and the analyses were stratified by sex, increased Hg concentrations were associated with poorer leg coordination in boys and poorer block-design scores in girls.
Sensory, Neurophysiological, and Other End Points in Children
In the Faroe Islands cohort, the 7-year evaluation included, in addition to the neuropsychological tests, assessments of visual acuity, near contrast sensitivity, otoscopy and tympanometry, and neurophysiological tests (pattern-reversal-visual-evoked potentials at 30' and 15', brainstem auditory-evoked potentials at 20 and 40 clicks per second (Hz), and postural sway) (Grandjean et al. 1997). Visual acuity, contrast sensitivity, auditory thresholds, and visual-evoked potentials were not significantly associated with prenatal MeHg exposures. For brainstem auditory-evoked potential, peaks I, III, and V were slightly delayed at increased cord-blood Hg concentrations at both 20 Hz and 40 Hz (p values, 0.01 to 0.10), although interpeak latencies were not associated with Hg at either frequency. In additional analyses reported separately (Murata et al. 1999b), in which data collected during the second year of this phase of the study were excluded due to concerns about the electromyograph used, higher maternal hair and cord-blood Hg concentrations were associated with lower peak III latencies, as well as with longer peak I-III latencies. Of the four conditions under which postural sway was assessed, only when subjects stood on the platform without foam under it with their eyes closed did the results approach significance (p = 0.09). Visual acuity and contrast sensitivity were not related to Hg exposure.
In a cross-sectional study of 149 6- to 7-year-old children living in a fishing village on Madiera, many of the same neurophysiological tests were administered (Murata et al. 1999a). Because patterns of fish consumption were considered to be stable, current maternal-hair Hg concentration was used as a measurement of a child's prenatal Hg exposure (mean, 9.6 ppm; range, 1.1-54.4 ppm). With respect to brainstem auditory evoked potential, maternal-hair Hg was significantly associated with I-III and I-V interpeak latencies at both 20 and 40 Hz, as well as with total latencies for peaks III and V at both frequencies. Those results are similar to the findings in the Faroe Islands cohort, at least among the children who were tested in the first year (see above). With respect to visual-evoked potentials on a pattern-reversal task, maternal-hair Hg concentration was significantly associated with one of the three latencies measured (N145 at 15' ), as well as with the N75-N145 and P100-N145 latencies (15' only). As noted above, VEP latencies were unrelated to Hg concentrations in the Faroe Islands cohort.
The relationship between blood Hg concentrations and auditory function in children and adults was investigated by Counter et al. (1998). The study sample consisted of 75 individuals (36 children and 39 adults) from a gold-mining region in Ecuador (study area) and 34 individuals (15 children and 19 adults) from a control area. Blood Hg concentrations were significantly higher in individuals from the gold-mining area than in individuals from the control region (17.5 µg/L versus 3.0 µg/L). Neuro-otological examinations were carried out on all individuals. Audiological evaluations, consisting of determinations of pure tone air-conduction thresholds in each ear at 0.25, 0.5, 1, 2, 3, 4, 6, and 8 kHz, were carried out on 40 individuals in the study area. Brainstem auditory-evoked-potential studies were carried out on 19 subjects in the study area. The absolute latencies of waves I, II, III, IV, and V and the interpeak latencies of I-III, III-V, and I-V were measured for left and right sides. Blood Hg concentration was significantly associated with hearing threshold at 3 kHz in the right ear only and for children only. A borderline association was found between blood Hg concentration and I-III interpeak transmission time on the left side. The authors concluded that although the end points assessed were generally unaffected at the blood Hg concentrations represented in the cohort of adults and children in the study area, the associations found were consistent with an effect of Hg at the level of the auditory nerve and the cochlear nuclear complex.
Animal Studies
Developmental Effects in Animals
The results of nearly 30 years of experimental studies using various animal models have helped characterize the neurotoxic effects of MeHg following in utero or early postnatal exposures (see Table 5-11). Several excellent reviews on the topic have been published over the years (WHO 1976, Chang 1977, Inskip and Piotrowski 1985, IPCS 1990, Burbacher et al. 1990, Gilbert and Grant-Webster 1995, Clarkson 1997) including a recent “Toxicological Profile for Hg” published by the Agency for Toxic Substances and Disease Registry (ATSDR 1999). In general, experimental studies have reported a continuum of neurodevelopmental effects similar to those reported in studies of humans exposed to MeHg (see
TABLE 5-11 Neurobehavioral Effects of Developmental MeHg Exposure in Animals
|
Species |
Exposure Time |
NOAEL (mg/kg/d) |
LOAEL (mg/kg/d) |
Effect |
Reference |
|
Monkey (M. fascicularis) |
Birth to 7 yr old |
No NOAEL |
0.05 |
Decreased visual-contrast sensitivity (spatial) thresholds at 3-4 yr old |
Rice and Gilbert 1982 |
|
Monkey (M. fascicularis) |
In utero |
No NOAEL |
0.05-0.07 |
Retarded Object Permanence Development |
Burbacher et al. 1986 |
|
Monkey (M. fascicularis) |
In utero |
No NOAEL |
0.05-0.07 |
Impaired visual-recognition memory in offspring (abstract) |
Gunderson et al. 1986 |
|
Monkey (M. fascicularis) |
In utero |
No NOAEL |
0.05-0.07 |
Impaired visual-recognition memory in offspring (social) |
Gunderson et al. 1988 |
|
Monkey (M. fascicularis) |
Birth to 7 yr old |
No NOAEL |
0.05 |
Increased clumsiness in exercise cage at 13 yr old |
Rice 1989 |
|
Monkey (M. fascicularis) |
In utero |
No NOAEL |
0.05 |
Reduced social play Increased nonsocial behaviors |
Burbacher et al. 1990 |
|
Monkey (M. fascicularis) |
In utero plus 4 yr postnatally |
No NOAEL |
0.01-0.05 |
Decreased visual-contrast sensitivity (spatial) thresholds at 5 yr old |
Rice and Gilbert 1990 |
|
Monkey (M. fascicularis) |
Birth to 7 yr old |
No NOAEL |
0.05 |
Increased pure-tone thresholds at 14 yr old |
Rice and Gilbert 1992 |
|
Monkey (Saimiriiureus) |
Gestation wk 11-14.5 to birth (22 wk) |
No NOAEL |
Not stated (dosed for stable blood concentration) |
Retarded schedule-control behavior during transitions |
Newland et al. 1994 |
|
Monkey (M. fascicularis) |
Birth to 7 yr old |
No NOAEL |
0.05 |
Increased vibration-sensitivity thresholds at 18 yr old |
Rice and Gilbert 1995 |
|
Monkey (M. fascicularis) |
In utero plus 4 yr postnatally |
No NOAEL |
0.01-0.05 |
Increased pure-tone thresholds at 19 yr old |
Rice 1998 |
|
Monkey (M. fascicularis) |
In utero |
No NOAEL |
0.05-0.09 |
Decreased visual-contrast sensitivity (spatial) |
Burbacher et al. 1999 |
|
Rat |
Gestation d 1 to postnatal d 42 (68 d) |
No NOAEL |
0.10 |
Abnormal swimming; delayed righting reflex; impaired learning in maze |
Olson and Bousch 1975 |
|
Rat |
Gestation d 1 to birth; birth to postnatal d 21; postnatal d 21 to d 30 |
No NOAEL |
2.5 |
Impaired learning in water T-maze for all 3 groups |
Zenick 1974 |
|
Rat |
Gestation d 10 (in utero only) |
6 |
8 |
Decreased activity during the postweaning period |
Su and Okita 1976 |
|
Gestation d 10-12 (in utero only) |
No NOAEL |
4 |
|||
|
Decreased activity during the postweaning period |
|||||
|
Rat |
Gestation d 1 to birth (in utero plus lactational) |
No NOAEL |
2.5 |
Abnormal visual-evoked potentials |
Zenick 1976 |
|
Rat |
Gestation d 7 (in utero plus lactational) |
No NOAEL |
5 |
Abnormal visual-evoked potentials |
Dyer et al. 1978 |
|
Rat (Wistar) |
Gestation d 6-9 (in utero plus lactational) |
No NOAEL |
0.05 |
Reduced behavioral performance on DRH operant test |
Musch et al. 1978 |
|
Rat (Wistar) |
Gestation d 6-9 (in utero only) |
0.005 |
0.01 |
Reduced behavioral performance on DRH operant test |
Bornhausen et al. 1980 |
|
Rat (Sprague-Dawley) |
Gestation d 4 (in utero plus lactational) |
No NOAEL |
10 |
Impaired avoidance learning |
Schalock et al. 1981 |
|
Rat |
Gestation d 8 or 15 (in utero plus lactational) |
No NOAEL |
5 |
Increased activity during the preweaning period; impaired learning in shuttle box |
Eccles and Annau 1982a,b |
|
Rat |
Gestation d 6-9 (in utero plus lactational) |
No NOAEL |
2 |
Increased auditory startle response; increased activity in Figure 8 maze |
Buelke-Sam et al. 1985 |
|
Rat (Sprague-Dawley) |
Gestation d 6-9 (in utero plus lactational) |
2 |
6 |
Delayed surface righting; delayed swimming ontogeny; decreased postweaning Figure 8 activity; increased time and errors in Biel maze |
Vorhees 1985 |
|
Rat (Sprague-Dawley) |
Gestation d 6-9 (in utero only) (cross-fostered) |
1.25 |
2.5 |
Delayed surface righting; delayed negative geotaxis; delayed swimming ontogeny; decreased activity in open field |
Geyer et al. 1985 |
|
Rat |
2 wk before mating through weaning |
0.08 |
Impaired tactile-kinesthetic function in offspring |
Elsner 1991 |
|
Rat (Sprague-Dawley) |
Gestation d 6-9 (in utero plus lactational) |
2 for MeHg No NOAEL (with Hg0) |
2 |
Potentiated effects of Hg0: increased activity; increased swimming speed; increased errors in radial maze |
Fredriksson et al. 1996 |
|
Rat |
4 wk before mating through postnatal d 16 |
6.4 |
No effects |
Normal behavioral performance on DRH operant test |
Rasmussen and Newland 1999 |
|
Mouse (129/SvS1) |
Gestation d 7 or 9 (in utero plus lactational) |
No NOAEL |
8 |
Abnormal swimming behavior |
Spyker et al. 1972 |
|
Mice |
Gestation d 8 (in utero only) |
No NOAEL |
3 |
Impaired avoidance learning |
Hughes and Annau 1976 |
|
Abbreviations: NOAEL, no-observed-adverse-effect level; LOAEL, lowest-observed-adverse-effect level; Hg0, elemental mercury; DRH |
|||||
Table 5-10). Those effects are largely dependent on the dose, timing, and duration of the MeHg exposure.
Fetal Minamata Disease
Experimental studies using nonhuman primates, cats, and rodent models exposed to high doses of MeHg have reported some or all of the cluster of neuropathological effects consistent with fetal Minimata disease (MD) that were first described from human autopsy cases following the catastrophic exposures in Minamata, Japan, and Iraq (Matsumoto et al 1965; Takeuchi 1968; Choi et al 1978). Those effects include microcephaly, degeneration and atrophy of cortical structures, loss of ceils in the cerebrum and cerebellum, a reduction of myelin, ventricular dilation, gliosis, disorganized cell layers, and ectopic cells. In addition, seizures, spasticity, blindness, and severe learning deficits have been reported. In nonhuman primates, maternal doses above 100 µg/kg per day were associated with MD in offspring autopsied during infancy (Mottet et al. 1987; Burbacher et al. 1990). Similar effects were observed at doses as low as 1 to 1.5 mg/kg per day in mice and rats (Khera and Tabacova 1973; O'Kusky 1983), 2 mg/kg per day in golden hamsters (Reuhl et al. 1981a,b), 12 mg/kg per day in guinea pigs (Inouye and Kajiwara 1988), and 0.25 mg/kg per day in cats (Khera 1973b). Differences in the lowest-observed-adverse-effect levels (LOAELs) for signs consistent with MD do not necessarily represent true species differences in susceptibility to MeHg, because the choices of doses and exposure periods used across the studies are not comparable.
Neurobehavioral Effects
The focus of many of the developmental studies using animal models has been to define the effects of MeHg at exposures that are not associated with gross signs of toxicity. Studies using nonhuman primate and rodent models have reported numerous subclinical effects at doses below those associated with overt maternal or offspring toxicity (see Table 5-11). In a long-term study examining the effects of maternal oral doses of MeHg hydroxide at 50, 70, or 90 µg/kg per day before and
during pregnancy in nonhuman primates (Macaca fascicularis), maternal toxicity (blindness and motor incoordination) was observed at the highest dose tested (90 µg/kg per day), and reproductive effects (nonconceptions, abortions, and stillbirths) were observed at 90 and 70 µg/kg per day (Burbacher et al. 1988). The maternal dose of MeHg hydroxide at 50 µg/kg per day was associated with developmental effects in offspring, but not with maternal toxicity or reproductive effects. Impairments in perceptual-cognitive functioning (Fagan Test and Object Permanence Test) and the development of species-specific social behavior were observed in offspring during infancy (Gunderson et al. 1986, 1988; Burbacher et al. 1986, 1990). A significant reduction in the weight gain of exposed males beginning at 2.5 years of age was also observed (Burbacher et al. 1993). That sex-specific effect appeared to be related to the adolescent growth spurt, because adult weight was not affected by MeHg. Studies conducted when the monkeys were adults indicated significant effects due to MeHg exposure on spatial vision (visual contrast-sensitivity functions). Although there were overall group differences in spatial vision, there were large individual differences in the response of the MeHg-exposed monkeys (Burbacher et al. 1999). Tests of adult learning and memory did not indicate significant effects due to MeHg exposure (Gilbert et al. 1993, 1996) and pure-tone auditory thresholds appeared normal when the monkeys were tested at approximately 12 to 15 years of age (Burbacher et al. 1999).
In another series of studies, Macaca fascicularis were orally exposed to MeHg at 50 µg/kg per day from birth to 7 years of age (Rice 1989) or at 0, 10, 25, or 50 µg/kg per day in utero plus 4 years postnatally (Rice and Gilbert 1990). No effects of MeHg were observed in the tests on infant or juvenile learning and memory for the in utero plus postnatally exposed animals (Rice 1992). However, impaired spatial vision was observed in monkeys from both dose groups when they were tested on a contrast-sensitivity task between 3 and 5 years of age (Rice and GIlbert 1982; Rice and Gilbert 1990). At 13 years of age, overt toxicity (clumsiness) was observed in some of the monkeys exposed postnatally to MeHg for 7 years (Rice 1989). Tests of those monkeys at 14 years of age indicated impaired high-frequency hearing in four of the five MeHg-exposed monkeys, and tests at age 18 indicated impaired somatosensory function (vibration sensitivity) in the same four monkeys (Rice and Gilbert 1992, 1995). Two of four monkeys exposed to MeHg in utero
plus 4 years postnatally also demonstrated impairments on the vibration-sensitivity test when tested at 15 years of age. Auditory testing of the monkeys exposed to MeHg in utero plus 4 years postnatally at 11 and 19 years of age indicated elevated pure-tone thresholds throughout the full range of frequencies tested (0.125 to 31.5 kHz) at 19 years of age (Rice 1998). Although both controls and MeHg-exposed monkeys showed higher thresholds at 19 years of age compared with 11 years, MeHg-exposed monkeys showed a greater deterioration in auditory function with increasing age. Across studies, MeHg effects were observed in individual monkeys at maternal doses of 10 µg/kg per day to 50 µg/kg per day or a dose of 50 µg/kg per day postnatally. However, the numbers of monkeys in the studies were small (one at 10 µg/kg per day), allowing only individual comparisons.
Newland et al. (1994) examined the effects of in utero exposure to MeHg in squirrel monkeys. Maternal exposure to MeHg varied to provide steady-state blood Hg concentrations between 0.7 and 0.9 ppm. At 5 to 6 years of age, offspring were trained to lever press under concurrent schedules of reinforcement. The results of the study indicated that MeHg-exposed monkeys were not able to change their response rates consistent with changes in reinforcement contingencies. Those effects were most prominent during transitions in reinforcement schedules.
Many of the studies using rodent models have also focused on examining the effects of MeHg exposure on neurobehavioral development. One of the largest studies to examine the effects of developmental exposure to MeHg in rats was the “Collaborative Behavioral Teratology Study ” (CBTS), which was performed to compare the results of a standard behavioral test battery across several laboratories (Buelke-Sam et al. 1985). Maternal rats were exposed to MeHg at 0, 2, or 6 mg/kg per day via gavage on gestation days 6-9. Offspring were exposed in utero and during lactation (no cross-fostering). Behavioral assessments of offspring indicated an increase in auditory startle-response habitation, mostly at the high dose. Maze activity increased with increasing MeHg exposure, and performance on a visual discrimination test was affected at the high dose. Two parallel studies, Vorhees (1985) and Geyer et al. (1985), reported similar findings, as well as delayed surface righting and swimming ontogeny. Retarded maze performance at the highest dose tested (Vorhees 1985) and retarded negative geotaxis and pivoting at a
dose of 2.5 mg/kg per day on gestation days 6-15 were also reported (Geyer et al. 1985). The effects observed by Geyer et al. (1985) were related to gestational exposure alone, because the MeHg offspring were cross-fostered to nonexposed dams at birth. Consistent with the results of the nonhuman primate studies, two studies have reported effects of early MeHg exposure on visual functions in rats (Zenick 1976; Dyer et al. 1978). Abnormal visual-evoked potentials were reported following in utero and lactational exposure to MeHg following a single maternal dose of 5 mg/kg per day on gestation day 7 (Dyer et al. 1978) or continuous maternal exposure at 2.5 mg/kg per day (Zenick 1976). Other studies of rats and mice have reported MeHg effects on motor performance and measures of activity and learning. MeHg effects on the swimming behavior of mice was reported following in utero and lactational MeHg exposure (maternal dose of 8 mg/kg on day 7 or 9 of gestation) (Spyker et al. 1972) or following exposure from gestation day 1 to postnatal day 42 (0.1 mg/kg per day) (Olson and Bousch 1975). Reports indicated increased activity in rats during the preweaning period following in utero and lactational MeHg exposure (5 or 8 mg/kg per day on gestation day 8 or 15) (Eccles and Annau 1982a,b), and decreased activity was reported in mice tested postweaning following in utero MeHg exposure alone (8 or 12 mg/kg per day on gestation day 10, or 4 mg/kg per day on gestation days 10-12 with cross-fostering at birth) (Su and Okita 1976). Learning deficits have been reported in both rats and mice following in utero or early postnatal MeHg exposure. Rats exposed prenatally to MeHg displayed impaired learning on a shuttlebox avoidance test (Eccles and Annau 1982a,b), and a single dose of 10 mg/kg per day on gestation day 4 with no cross-fostering of dams (in utero plus lactational exposure) was associated with decreased escape, avoidance, and appetitive learning (Schalock et al. 1981). Olson and Bousch (1975) reported impaired learning in rats on a maze task following exposure to Hg at 0.1 mg/kg per day via a fish diet from gestation day 1 to postnatal day 42. In mice, a maternal dose of 3 mg/kg on gestation day 8 (Hughes and Annau 1976) retarded both active and passive avoidance learning. The results suggested that the effects were due to exposure in utero, because the effects were observed in exposed offspring cross-fostered to control females at birth (no lactational exposure). Zenick (1974) compared the learning performance of rats following prenatal, lactational, or 9 days postweaning exposure to MeHg (2.5
mg/kg per day) in a water T maze. Deficits in learning were observed in the prenatal and postweaning exposure groups but not in the lactational exposure group. Thus far, the Differential Reinforcement of High Rates (DRL) test has proved to be the most sensitive of the behavioral tests used with rodents for detecting effects of in utero MeHg exposure (Müsch et al. 1978; Bornhausen et al. 1980). Rats exposed in utero to maternal doses of MeHg at 0.01 to 0:05 mg/kg per day and cross-fostered at birth displayed abnormal response patterns on the DRL task when tested at 4 months of age. Using a similar DRL paradigm, Rasmussen and Newland (1999), however, were not able to replicate that finding. A procedure designed to measure tactile-kinesthetic function in rodents has also been shown to be sensitive to MeHg exposure. Elsner (1991) reported a decrease with that procedure in the performance of rats following in utero and lactational MeHg exposure at a very low maternal dose (0.08 mg/kg per day, 2 weeks before mating and throughout gestation).
In 1996, Fredricksson et al. reported interactive behavioral effects following exposure of rats to MeHg and metallic Hg vapor. Exposure to Hg vapor at 1.8 mg/m3 for 1.5 hours per day on gestation days 14-19 was related to hyperactivity and decreased spatial learning. While exposure to MeHg at 2 mg/kg per day on gestation days 6-9 was not related to adverse behavioral effects, co-exposure to MeHg and Hg vapor potentiated the activity and spatial learning effects observed with Hg vapor exposure alone. The reported Hg vapor effects were consistent with previous reports (Danielsson et al. 1993, Fredriksson et al. 1992, 1993). This is the first report, however, of an interactive effect of in utero exposure toHg vapor and MeHg. The results indicate that total exposure to the different forms of Hg during pregnancy is critical in evaluating the effects on the fetus.
Finally, the results of a few of the studies using animal models have provided some preliminary data on the potential effects of early-developmental exposure to MeHg on the functional status of aging animals. An early report by Spyker (1975) summarized the effects of MeHg observed over the lifetime of mice exposed in utero and during lactation. Offspring were normal at birth but exhibited effects of exposure on exploratory activity and swimming ability at 1 month of age and neuromuscular and immune effects after 1 year of age. Those findings
provide the first evidence of delayed neurotoxicity in MeHg-exposed animals. The effects of in utero plus postnatal MeHg exposure described by Rice (1989) also support the notion of delayed neurotoxicity, which might be related to increased functional impairment with aging. Monkeys exposed to MeHg at 50 µg/kg per day from birth to 7 years of age were observed in an exercise cage throughout their life. Obvious motor incoordination was observed only after the monkeys reached 14 years of age (Rice 1989). Subsequent testing of those monkeys indicated higher thresholds for vibration sensitivity, indicating effects on somatosensory functioning (Rice and Gilbert 1995). More recently, monkeys exposed to MeHg at 10-50 µg/kg per day in utero plus 4 years postnatally showed a greater deterioration in auditory function with increasing age when tested at 11 and 19 years of age (Rice 1998). Whether those effects are related to cumulative damage from early MeHg exposure and aging or to a continuous process from long-term retention of inorganic Hg in the brain following MeHg exposure is not known. The results clearly indicate, however, that the health risks associated with early MeHg exposure could last a lifetime (Harada 1995; Kinjo et al 1993).
ADULT CENTRAL-NERVOUS-SYSTEM TOXICITY
Adult Human Neurological, Neurophysiological, and Sensory Function
Several neurological signs and symptoms are among the cardinal features of chronic high-dose exposures to MeHg in adults. As no pathognomonic test is available to confirm the diagnosis of Minamata disease, cases were identified on the basis of a characteristic combination of symptoms (Harada 1997; Uchino et al. 1995; Tsubaki and Takahashi 1986). These included peripheral neuropathy (e.g., sensory impairment of the extremities of the glove-stocking type and perioral dysesthesia), dysarthria, tremor, cerebellar ataxia, gait disturbance, ophthalmological impairment (e.g., visual-field constriction and disturbed ocular movements), audiological impairment (e.g., hearing loss),
disturbance of equilibrium (e.g., vertigo, dizziness and fainting), and subjective symptoms such as headache, muscle and joint pain, forgetfulness, and fatigue. In patients with classic Minamata disease, many of those signs and symptoms were still evident after 20 years. Later studies of patients with Minamata disease reported increased pain thresholds in the body (truncal hypesthesia) and distal extremities (Yoshida et al. 1992).
To evaluate the WHO (IPCS 1990) estimate that 5% of adults with a blood Hg concentration of 200 ppb would manifest paresthesia, Kosatsky and Foran (1996) reviewed 13 studies of neurological status in long-term fish consumers. Although they identified pervasive weaknesses in study design (e.g., crude measures of exposure and outcome, possible selection bias, and absence of blinding), the authors concluded that the studies suggested neurological effects in as few as 11% (95% confidence interval, 4-22) and as many as 31% (95% confidence interval, 19-45) of adults with a blood Hg concentration of 200 ppb or more. Thus, they argued that these data do not support the WHO (IPCS 1990) conclusion that a blood Hg concentration of 200 ppb (corresponding to a hair Hg concentration of 50 ppm) represents a LOAEL for adult paresthesia and identified a need for additional research to define the lower portion of the dose-response curve (20-200 ppb).
Important data on the impact of chronic low-dose MeHg exposures on adult neurological and sensory function are being generated in ongoing studies of fish-eating populations living in the Amazon Basin, where gold is extracted from soil or river sediments and Hg is released. Lebel et al. (1996) studied 29 young adults (ages, 15-35 years; 14 females and 15 males) randomly selected from participants in a previous survey. The geometric-mean hair Hg concentration was 14.0 ppm (range, 5.6 to 38.4 ppm). Subjects underwent a battery of quantitative behavioral, sensory, and motor tests, including tests of visual functions (near and far acuity, chromatic discrimination, near contrast sensitivity, and peripheral visual fields) and motor functions (maximum grip strength and manual dexterity). Individuals with increased hair Hg concentrations had reduced chromatic discrimination. Three individuals with hair Hg concentrations above 24 ppm demonstrated reduced contrast sensitivity, and individuals with concentrations above 20 ppm tended to demonstrate reductions in peripheral visual fields. An increase from 10 to 20 ppm was associated with about a 10 degree difference. Highly exposed
women tended to have lower scores than low-exposed women on both manual dexterity and grip strength. Such a tendency was not seen in men, indicating that association between hair Hg concentration and motor function was sex-specific.
In a subsequent study, Lebel et al. (1998) assembled another sample of 91 individuals (ages 15-81 years), representing approximately 38% of the adult population of the study village. Four measures of exposure were derived based on the Hg concentration in a hair sample (length not specified): mean total hair Hg averaged over all 1-cm segments of the sample (up to 24 segments), total Hg in the first centimeter, maximum total Hg in any segment, and MeHg in the first centimeter. Individuals for whom at least 1 cm of hair contained MeHg at more than 50 ppm were excluded. The mean hair MeHg concentration was approximately 13 ppm. The assessments included the same tests of motor (maximum grip strength and manual dexterity) and visual functions (acuity, chromatic discrimination, and near contrast sensitivity) that were used in the previous study. In addition, a clinical neurological examination was administered to a random sample of the cohort (59 subjects). That examination included the Branches Alternate Movement Task (BAMT), which requires imitation of a prescribed sequence of hand movements. Abnormal performance on the BAMT was significantly associated with all measures of Hg exposure, and abnormal visual fields were associated with mean hair Hg and peak Hg concentrations. Hyper-reflexia (patellar and bicepital) was not associated with any Hg measurement. Increased hair Hg concentrations, most notably peak Hg, were associated with poor scores on the intermediate and higher frequencies of near visual-contrast sensitivity (in the absence of near visual-acuity loss), with poor scores on the manual dexterity test, and with increased muscular fatigue. In women, but not in men, grip strength varied with peak Hg concentration. For many end points, the associations between hair Hg concentration and performance were stronger in younger subjects (less than 35 years) than in older ones. The authors stress that the dose-related decrements in visual and motor functions were associated with hair Hg concentrations below 50 ppm, a range in which clinical signs of Hg intoxication are not apparent. The Hg exposure of the cohort is presumed to have resulted from fish-consumption patterns that are stable and thus relevant to estimating the risk associated with chronic, low-dose MeHg exposure. In fact, the possibility cannot be
excluded that the neurobehavioral deficits of the adult subjects were due to increased prenatal, rather than ongoing, MeHg exposure.
Beuter and Edwards (1998) investigated the prevalence and severity of three types of subtle motor deficits in a cohort of 36 adult Cree (mean age 56 years), comparing them with patients with Parkinson 's disease (PD) (21 subjects), cerebellar deficit (6 subjects), essential tremor (3 subjects), or controls (30 subjects). The mean of the annual maximum hair Hg concentration over a period of 25 years varied from 2.2 to 31.1 ppm. Ten of 14 static tremor end points (with visual feedback) and 5 of 8 kinetic tremor end points (during voluntary finger movements) assessed were significantly related to group (i.e. Cree versus PD versus control). Nested analyses were carried out in which the six Cree with the highest hair Hg concentrations (mean of annual maximum hair concentrations greater than 24 ppm; range, 24.34-31.10 ppm) were matched to six Cree with low hair Hg concentrations (mean of annual maximum hair concentrations 6.02-11.89 ppm) and six controls to get a better idea of whether the group differences were likely to be due to Hg or some confounding factor associated with group membership. Despite the reduced number, significant group differences were still found on several end points. Overall, the performance characteristics that best discriminated groups were drift (static tremor), event index (static tremor), mean tracking error (kinetic tremor), and the center of mass harmonicity (static tremor).
The same groups of subjects were administered a test of rapid, precise promixo-distal movements (i.e. eye-hand coordination) (Beuter et al. 1999a). A eurythmkinesiometer recorded subjects' efforts to strike targets with a stylus, yielding measures of precision, imprecision, tremor, Fitts' constant (an index of the trade-off between speed and accuracy), and irregularity. The Cree subjects' performance was more than 1 standard deviation worse than the controls' performance on tremor, Fitts' constant, and irregularity. In the same type of nested analyses carried out in the study of tremor described above, the order of group scores, from best to worst, was control better than low Hg better than high Hg for all three end points, the group differences on Fitts' constant and irregularity being significant.
Rapid alternating movements (diadochokinesia) were assessed in those groups of subjects by asking them to rotate two foam spheres under three conditions: (1) both hands, natural cadence; (2) right and left
hands separately, fast cadence (i.e., as fast as possible); and (3) both hands, fast cadence (Beuter et al. 1999b). Seven dimensions of performance were measured: duration, range, maximum slope, similarity in shape, smoothness, sharpness, and coherence. Significant group difference were found on most end points, and the results of nested analyses provided additional evidence that group differences in Hg concentrations were probably contributory.
Neurotoxic Effects in Adult Animals
Experimental studies of the effects of MeHg exposure on adult animals have reported neurological effects similar to those reported for adult humans. Studies using monkeys, rodents, and cats have reported effects consistent with adult MD (Harada 1995). Some of those studies are summarized in Table 5-12. Neurotoxic signs reported reflect the regional specificity of the neuropathological effects observed in adult subjects. Signs of ataxia, constriction of the visual field, and sensory disturbances are commonly associated with pathological lesions in the calcarine cortices, dorsal root ganglia, and cerebellum (Chang 1980).
A study of macaque and squirrel monkeys has reported ataxia, tremor, and constriction of visual fields in animals with blood Hg concentrations between 1 and 2 ppm (Evans et al. 1977). The latency for the onset of symptoms in that study was 135 to 140 days.
Constriction of the visual field was reported in macaques following variable dosing schedules that produced blood MeHg concentrations from 1.5 to 3 ppm. The onset of visual-field disturbances preceded overt signs of toxicity (Merigan et al. 1983).
Ataxia, tremor, and apparent blindness was reported in adult female macaques exposed orally to doses of MeHg hydroxide at 70 µg/kg per day and above (Burbacher et al. 1988). The durations to onset of symptoms ranged from 177 days to 392 days.
In rodents, several studies have reported severe neurological effects, such as ataxia, paralysis, spasms, and hindlimb crossing in adult rats and mice, from exposure to MeHg (see Table 5-12). In general, the onset of symptoms is dependent on the dose and duration of exposure. In rats, overt signs of neurotoxicity were reported at doses ranging from 0.8 mg/kg per day for 6 weeks (Chang and Hartmann 1972) to 10 mg/kg
TABLE 5-12 Neurological Effects of MeHg Exposure in Adult Animals
|
Species |
Exposure Time |
NOAEL (mg/kg/d) |
LOAEL (mg/kg/d) |
Effect |
Reference |
|
Monkeyss (macaque and squirrel) |
135-1,000 d (variable dosing) |
NS |
NS |
Ataxia, tremor, constriction of visual field |
Evans et al. 1977 |
|
Monkeys (macaque) |
20-73 wk (variable dosing) |
NS |
NS |
Tremor, constriction of visual field |
Merigan et al. 1983 |
|
Monkeys (Macaca fascicularis) |
177-392 d |
0.05 |
0.09 |
Ataxia, tremor, blindness |
Burbacher et al. 1988 |
|
Rat |
29 d |
2.4 |
Ataxia, paralysis |
Hunter et al. 1940 |
|
|
Rat |
1-6 wk |
0.8 |
Ataxia, degeneration of cerebellum and dorsal root ganglia |
Chang and Hartmann 1972 |
|
|
Rat |
3-12 wk |
0.84 |
1.68 |
Ataxia, edema and necrosis of cerebellum |
Magos and Butler 1972 |
|
Rat (Wistar) |
2 d |
10 |
Impaired performance in tilting plane test |
Fehling et al. 1975 |
|
|
Rat (Wistar) |
9, 13, or 21 d |
2 |
4 |
Hindlimb crossing |
Inouye and Murakami 1975 |
|
Rat (Wistar) |
Gestation d 7-14 |
4 |
6 |
Spasms, gait disturbances |
Fuyuta et al. 1978 |
|
Rat (Sprague-Dawley) |
2 d |
1.32 |
4 |
Altered sleep cycles |
Arito and Takahashi |
|
Rat |
15 d (dosed every 3 d) |
10 |
Hindlimb crossing, flailing |
Leyshon and Morgan 1991 |
|
microgliocytosis and cerebellar degeneration |
|||||
|
Mouse |
24 wk |
1.9 |
Paralysis |
MacDonald and Harbison 1977 |
|
|
Mouse (C57B1/6) |
17 d 6 d |
4 8 |
Increased auditory brainstem response thresholds |
Wassick and Yonovitz 1985 |
|
|
Mouse (B6C3F1) 2 yr |
2 yr |
0.6 |
Paralysis, neuropathy |
Mitsumori et al. 1990 |
|
|
Rabbit (New Zealand) |
7 d |
30 |
Ataxia, decreased muscle tone, reduced splay reflex |
Jacobs et al. 1977 |
|
|
Cat |
0.05 |
Ataxia |
Khera et al. 1974 |
||
|
Cat |
60 wk |
0.046 |
Impaired hopping |
Charbonneau et al. 1976 |
|
|
Abbreviations: NOAEL, no-observed-adverse-effect level; LOAEL, lowest-observed-adverse-effect level; NS, not stated. |
|||||
per day given every 3 days for 15 days (Leyshon and Morgan 1991). Studies in mice reported that doses from 0.6 mg/kg per day for approximately 2 years (Mitsumori et al. 1990) to 1.9 mg/kg per day for 24 weeks (MacDonald and Harbison 1977) caused paralysis. A study by Jacobs et al. (1977) using New Zealand rabbits reported ataxia and decreased muscle tone following a dose of 30 mg/kg per day for 7 days. Two studies using cats reported ataxia and impaired hopping after long-term exposure at approximately 0.05 mg/kg per day (Khera et al. 1974; Charbonneau et al. 1976).
A few studies using rodents have reported less severe symptoms, such as altered sleep cycles, hindlimb weakness, or increased brainstem-auditory-response thresholds following exposure to MeHg. Altered sleep cycles in rats were reported by Arito and Takahashi (1991) following 2 days of exposure at 4 mg/kg per day. Hindlimb weakness in mice was reported by Berthoud et al. (1976) following exposure at 1 mg/kg per day for 60 days. Wassick and Yonovitz (1985) reported increased brainstem-auditory thresholds in mice following 17 days of exposure at 4 mg/kg per day or 6 days of exposure at 8 mg/kg per day.
In summary, reports from animal models of adult MD have provided supportive evidence for the neurological signs reported in humans. These studies have also provided detailed descriptions of the associated neuropathological effects from high-dose MeHg exposures (Chang 1979, 1990). Studies using adult animal models of chronic low-dose MeHg effects have been sparse, most likely because of the focus on neurodevelopmental effects following in utero or early postnatal MeHg exposure.
CONCLUSIONS
-
MeHg is highly toxic. The data reviewed in this chapter indicate that the adverse effects of MeHg exposure can be expressed in multiple organ systems throughout the lifespan.
-
Studies in humans on the carcinogenic effects of MeHg are inconclusive. Renal tumors have been seen in male mice but only at or above the MTD of MeHg.
-
The effect of MeHg on the human immune system is poorly understood. However, studies in vitro and in animals suggest that
-
exposure to MeHg could increase human susceptibility to infectious diseases and autoimmune disorders by damaging the immune system.
-
The reproductive effects of MeHg have not been fully evaluated in humans, but animal studies, including work in nonhuman primates, indicate that MeHg causes functional reproductive effects.
-
Damage to the renal tubules and nephron has been observed following human exposure to inorganic and organic forms of Hg. However, symptoms of renal damage have been seen only at Hg exposures that also caused neurological effects. In animals, similar effects have been observed as well as altered renal function and renal hypertrophy have been observed following early postnatal exposure to MeHg.
-
Although the data base is not as extensive for cardiovascular effects as it is for other end points (i.e., neurotoxic effects), the cardiovascular system appears to be a target for MeHg toxicity in both humans and animals. Evidence suggests that adverse health effects can occur at very low Hg exposures.
-
Exposure to elemental and organic forms of Hg alters blood-pressure regulation. That effect has been documented in children and adults who were exposed to toxic and subtoxic doses of Hg and have been induced experimentally in rats.
-
Prenatal exposure to MeHg has been shown to alter blood-pressure regulation and heart-rate variability in children. Those effects were observed at cord-blood Hg concentrations that have not been associated with other developmental effects (less than 10 µg/L).
-
Men who consumed at least 30 g of fish per day or had a hair Hg concentration of 2 ppm or more had a higher risk of suffering a fatal or nonfatal acute myocardial infarction. Mercury exposure was also correlated with an increased risk of dying from coronary heart disease or cardiovascular heart disease. A hair Hg concentration of 2 ppm has not been associated with other adverse health effects.
-
-
The human data base on the neurodevelopmental effects of MeHg is extensive, and includes studies of populations following high-dose Hg poisonings and chronic low-dose Hg exposure. Some study results appear to be conflicting. Table 5-10 provides informa
-
tion about the hair and blood Hg concentrations in the studies on which the following conclusions are based.
-
Several studies have detected significant MeHg-associated increases in the frequency of abnormal and questionable findings on standardized neurological examinations, although the functional importance of the apparent effects is uncertain.
-
Recent epidemiological studies provide little evidence that the ages at which children achieve major language and motor milestones are affected appreciably by low-dose prenatal MeHg exposure.
-
Two out of four studies using the Denver Developmental Screening Test reported an association of low-dose MeHg exposure on early childhood development.
-
Of the three major prospective long-term studies, the Faroes study reported associations between low-dose prenatal MeHg exposure and children's performance on standardized neurobehavioral tests, particularly in the domains of attention, fine-motor function, confrontational naming, visual-spatial abilities, and verbal memory, but the Seychelles study did not report such associations. The smaller New Zealand study also observed associations, as did a large pilot study conducted in the Seychelles.
-
Recent studies in adults suggest that hair Hg concentrations below 50 ppm are significantly associated with disturbances of the visual system (chromatic discrimination, contrast sensitivity, and peripheral fields) and with neuromotor deficits (tremor, dexterity, grip strength, complex-movement sequences, hand-eye coordination, and rapid alternating movement). Those findings suggest that the current reference dose for adults based on 50 ppm in hair might not be sufficiently protective.
-
Neurodevelopmental studies using animal models (nonhuman primates, rodents) exposed in utero and/or early postnatally to MeHg have reported a continuum of effects related to dose. Effects have been reported on sensory, sensorimotor, and cognitive development. Overall, sensory effects seem to be the most long-lasting.
-
Experimental studies of adult animal models exposed to MeHg have also reported a continuum of effects associated with dose. The
-
effects are similar to those observed in cases of human MeHg poisoning.
-
Neurodevelopmental effects are the most extensively studied sensitive end point for MeHg toxicity and are appropriate for use in establishing an RfD. New data are emerging, however, indicating that there might be important adverse effects on other end points (e.g., cardiovascular and immune systems) in the same exposure range. Those effects should be considered as the data become available.
RECOMMENDATIONS
-
Epidemiological research is needed to evaluate the prevalence of chromosomal aberrations and cancer, especially leukemia and renal tumors, among populations that have chronic exposure to MeHg through ingestion of contaminated fish.
-
The ability of MeHg to cause chromosomal damage and promote tumor growth should be considered in the establishment of exposure guidelines.
-
Research is needed to determine the effects of MeHg exposure on the immune system, including the effects on the developing immune system, resistance to microbial pathogens, and autoimmunity. Mechanisms by which the immune system is involved in the target-organ toxicity of Hg should also be examined.
-
Research is needed to assess the effects of MeHg on reproduction, including the effects on fertility indicators, such as sperm production, conception rates, and pregnancy outcomes.
-
Research is needed to evaluate the impact of dietary exposure to MeHg on the prevalence of hypertension and cardiovascular disease in the United States. The risk of fatal and nonfatal heart disease must be considered in the development of a reference dose for this contaminant.
-
Research is needed to determine the long-term implications of the neuropsychological and neurophysiological effects of low-level prenatal MeHg exposure detected in children, specifically whether
-
-
they are associated with an increased risk for later neurological diseases.
-
-
Research using animal models is needed to better define the immediate and long-term effects of early chronic low-level MeHg exposure. Studies should focus on several important issues:
-
Critical periods for MeHg effects (in utero or postnatal).
-
Low-level dose-response relationships (ppb range).
-
MeHg demethylation in the brain following early MeHg exposure.
-
Synergistic effects of early MeHg and Hg vapor exposure.
-
Neurodegenerative disorders related to early MeHg exposure.
-
-
Animal studies should be conducted to examine the neurodevelopmental effects of continuous versus peak MeHg exposures.
REFERENCES
Afonso, J.F., and R.R. de Alvarez. 1960. Effects of mercury on guman gestation. Am. J. Obstet. Gynec. 80(July):145-154.
Akagi, H., P. Grandjean, Y. Takizawa, and P. Weihe. 1998. Methylmercury dose estimation from umbilical cord concentrations in patients with Minamata disease. Environ. Res. 77(2):98-103.
Alcser, K.H., K.A. Brix, L.J. Fine, L.R. Kallenbach, and R.A. Wolfe. 1989. Occupational mercury exposure and male reproductive health. Am. J. Ind. Med. 15(5):517-29.
Amin-Zaki, L., S. Elhassani, M.A. Majeed, T.W. Clarkson, R.A. Doherty, and M. Greenwood. 1974. Intra-uterine methylmercury poisoning in Iraq. Pediatrics 54(5):587-95.
Anneroth, G., T. Ericson, I. Johansson, H. Mornstad, M. Ryberg, A. Skoglund, and B. Stegmayr. 1992. Comprehensive medical examination of a group of patients with alleged adverse effects from dental amalgams. Acta Odontol. Scand. 50(2):101-11.
Arito, H., and M. Takahashi. 1991. Effect of methylmercury on sleep patterns in the rat. Pp. 381-394 in Advances in Mercury Toxicology, T. Suzuki, N. Imura, and T.W. Clarkson, eds. New York: Plenum Press.
Aronow, R., C. Cubbage, R. Wiener, B. Johnson, J. Hesse, and J. Bedford. 1990. Mercury exposure from interior latex paint- Michigan. MMWR 39(8)125-136.
ATSDR (Agency for Toxic Substances and Disease Registry). 1999. Toxicologi-
cal Profile for Mercury. (Update). U.S. Department of Health and Human Services, Agency for Toxic Substances and Disease Registry, Atlanta, GA.
Axtell, C.D., G.J. Myers, P.W. Davidson, A.L. Choi, E. Cernichiari, J. Sloane-Reeves, C. Cox, C. Shamlaye, and T.W. Clarkson. 1998. Semiparametric modeling of age at achieving developmental milestones after prenatal exposure to methylmercury in the Seychelles child development study. Environ. Health Perspect. 106(9):559-564.
Bakir, F., S.F. Damluji, L. Amin-Zaki, M. Murtadha, A. Khalidi, N.Y. al-Rawi, S. Tikriti, H.I. Dhahir, T.W. Clarkson, J.C. Smith, and R.A. Doherty. 1973. Methylmercury poisoning in Iraq. Science 181(96):230-241.
Barr, R.D., P.H. Rees, P.E. Cordy, A. Kungu, B.A. Woodger, and H.M. Cameron. 1972. Nephrotic syndrome in adult Africans in Nairobi. Br. Med. J. 2(806):131-4.
Barregard, L., B. Hultberg, A. Schutz, and G. Sallsten. 1988. Enzymuria in workers exposed to inorganic mercury. Int. Arch. Occup. Environ. Health 61(1-2):65-9.
Barregard, L., B. Hogstedt, A. Schutz, A. Karlsson, G. Sallsten, and G. Thiringer. 1991. Effects of occupational exposure to mercury vapor on lymphocyte micronuclei . Scand. J. Work Environ. Health 17(4):263-8.
Bellinger, D.C., A. Leviton, C. Waternaux, H. Needleman, and M. Rabinowitz. 1987. Longitudinal analyses of prenatal and postnatal lead exposure and early cognitive development. N. Engl. J. Med. 316(17):1037-1043.
Berthoud, H.R., R.H. Garman, and B. Weiss. 1976. Food intake, body weight, and brain histopathology in mice following chronic methylmercury treatment. Toxicol. Appl. Pharmacol. 36(1):19-30.
Betti, C., T. Davini, and R. Barale. 1992. Genotoxic activity of methylmercury chloride and dimethyl mercury in human lymphocytes. Mutat. Res. 281(4):255-260.
Beuter, A., and R. Edwards. 1998. Tremor in Cree subjects exposed to methylmercury: a preliminary study . Neurotoxicol. Teratol. 20(6):581-9.
Beuter, A., A. de Geoffroy, and R. Edwards. 1999a. Quantitative analysis of rapid pointing movements in Cree subjects exposed to mercury and in subjects with neurological deficits. Environ. Res. 80(1):50-63.
Beuter, A., A. de Geoffroy, and R. Edwards. 1999b. Analysis of rapid alternating movements in Cree subjects exposed to methylmercury and in subjects with neurological deficits. Environ. Res. 80(1):64-79.
Blakley, B.R. 1984. Enhancement of urethane-induced adenoma formation in Swiss mice exposed to methylmercury. Can. J. Comp. Med. 48(3):299-302.
Bluhm, R.E., R.G. Bobbitt, L.W. Welch, A.J. Wood, J.F. Bonfiglio, C. Sarzen, A.J. Heath, and R.A. Branch. 1992. Elemental mercury vapour toxicity, treat-
ment, and prognosis after acute, intensive exposure in chloralkali plant workers. Part I: History, neuropsychological findings and chelator effects. Hum. Exp. Toxicol. 11(3):201-10.
Bornhausen, M., H.R. Müsch, and H. Greim. 1980. Operant behavior performance changes in rats after prenatal methylmercury exposure. Toxicol. Appl. Pharmacol. 56(3):305-10.
Buchet, J.P., H. Roels, A. Bernard, and R. Lauwerys. 1980. Assessment of renal function of workers exposed to inorganic lead, calcium or mercury vapor. J. Occup. Med. 22(11):741-50.
Buelke-Sam, J., C.A. Kimmel, J. Adams, C.J. Nelson, C.V. Vorhees, D.C. Wright, V. St Omer, B.A. Korol, R.E. Butcher, M.A. Geyer, J.F. Holson, C.L. Kutscher, and M.J. Wayner. 1985. Collaborative Behavioral Teratology Study: Results. Neurobehav. Toxicol. Teratol. 7(6):591-624.
Burbacher, T.M., K.S. Grant, and N.K. Mottet. 1986. Retarded object permanence development in methylmercury exposed Macaca fascicularis infants. Dev. Psychol. 22(6):771-776.
Burbacher, T.M., M.K. Mohamed, and N.K. Mottett. 1988. Methylmercury effects on reproduction and offspring size at birth. Reprod. Toxicol. 1(4):267-278.
Burbacher, T.M., P.M. Rodier, and B. Weiss. 1990. Methylmercury developmental neurotoxicity: a comparison of effects in humans and animals. Neurotoxicol. Teratol. 12(3):191-202.
Burbacher, T., P. Rodier, K. Grant-Webster, S. Gilbert, and N.K. Mottet. 1993. Pubertal growth retardation: a sex specific effect of in utero methylmercury exposure. Teratology 47(5):455.
Burbacher, T.M., K.S. Grant, S.G. Gilbert, and D.C. Rice. 1999. The effects of methylmercury exposure on visual and auditory functions in nonhuman primates. Toxicologist 48(1-S):362.
Cardenas, A., H. Roels, A.M. Bernard, R. Barbon, J.P. Buchet, R.R. Lauwerys, J. Rosello, G. Hotter, A. Mutti, I. Franchini, et al. 1993. Markers of early renal changes induced by industrial pollutants. I. Application to workers exposed to mercury vapour. Br. J. Ind. Med. 50(1):17-27.
Chang, L.W. 1977. Neurotoxic effects of mercury--a review. Environ. Res. 14(3):329-73.
Chang, L.W. 1979. Pathological effects of mercury poisoning. Pp. 519-580 in The Biogeochemistry of Mercury in the Environment, J.O. Nriagu, ed. New York: Elsevier.
Chang, L.W. 1980. Mercury. Pp. 508-526 in Experimental and Clinical Neurotoxicology, P.S. Spencer, and H.H. Schaumburg, eds. Baltimore MD: Williams & Wilkins.
Chang, L.W. 1990. The neurotoxicology and pathology of organomercury, organolead, and organotin. J. Toxicol. Sci. 15(Suppl. 4):125-51.
Chang, L.W., and H.A. Hartmann. 1972. Ultrastructural studies of the nervous system after mercury intoxication. I. Pathological changes in the nerve cell bodies. Acta Neuropathol. (Berl) 20(2):122-38.
Charbonneau, S.M., I.C. Munro, E.A. Nera, F.A. Armstrong, R.F. Willes, F. Bryce, and R.F. Nelson. 1976. Chronic toxicity of methylmercury in the adult cat. Toxicology 5(3):337-349.
Choi, B.H., L.W. Lapham, L. Amin-Zaki, and T. Saleem. 1978. Abnormal neuronal migration, deranged cerebral cortical organization, and diffuse white matter astrocytosis of human fetal brain: a major effect of methylmercury poisoning in utero. J. Neuropathol. Exp. Neurol. 37(6):719-33.
Cinca, I., I. Dumetrescu, P. Onaca, A. Serbanescu, and B. Nestorescu. 1979. Accidental ethyl mercury poisoning with nervous system, skeletal muscle, and myocardium injury. J. Neurol. Neurosurg. Psychiatry 43(2):143-149.
Clarkson, T.W. 1997. The toxicology of mercury. Crit. Rev. Clin. Lab. Sci. 34(4):369-403.
Cordier, S., and M. Garel. 1999. Neurotoxic Risks in Children Related to Exposure to Methylmercury in French Guiana. INSERM U170 and U149 -Study financed by the Health Monitoring Institute (RNSP). National Institute of Health and Medical Research. April.
Cordier, S., F. Deplan, L. Mandereau, and D. Hemon. 1991. Paternal exposure to mercury and spontaneous abortions. Br. J. Ind. Med. 48(6):375-81.
Costa, M., N.T. Christie, O. Cantoni, J.T. Zelikoff, X.W. Wang, and T.G. Rossman. 1991. DNA damage by mercury compounds: An overview. Pp. 255-273 in Advances in Mercury Toxicology, T. Suzuki, N. Imura, and T.W. Clarkson, eds. New York: Plenum Press.
Counter, S.A., L.H. Buchanan, G. Laurell, and F. Ortega. 1998. Blood mercury and auditory neuro-sensory responses in children and adults in the Nambija gold mining area of Ecuador. Neurotoxicology 19(2):185-196.
Cox, C., T.W. Clarkson, D.O. Marsh, L. Amin-Zaki, S. Tikriti, and G.G. Myers. 1989. Dose-response analysis of infants prenatally exposed to methyl mercury: An application of a single compartment model to single-strand hair analysis. Environ. Res. 49(2):318-332.
Cox, C., D. Marsh, G. Myers, and T. Clarkson. 1995. Analysis of data on delayed development from the 1971-72 outbreak of methylmercury poisoning in Iraq: Assessment of influential points . Neurotoxicology 16(4):727-730.
Crump, K.S., T. Kjellström, A.M. Shipp, A. Silvers, and A. Stewart. 1998. Influence of prenatal mercury exposure upon scholastic and psychological test performance: benchmark analysis of a New Zealand cohort. Risk Anal. 18(6):701-713.
Crump, K., J. Viren, A. Silvers, H. Clewell 3rd, J. Gearhart, and A. Shipp. 1995. Reanalysis of dose-response data from the Iraqi methylmercury poisoning episode. Risk Anal. 15(4):523-532.
Dahl, J.E., J. Sundby, A. Hensten-Pettersen, and N. Jacobsen. 1999. Dental workplace exposure and effect on fertility. Scand. J. Work Environ. Health 25(3):285-90.
Dahl, R., R.F. White, P. Weihe, N. Sørensen, R. Letz, H.K. Hudnell, D.A. Otto, and P. Grandjean. 1996. Feasibility and validity of three computer-assisted neurobehavioral tests in 7-year-old children. Neurotoxicol. Teratol. 18(4):413-419.
Danielsson, B.R., A. Fredriksson, L. Dahlgren, A.T. Gardlund, L. Olsson, L. Dencker, and T. Archer. 1993. Behavioural effects of prenatal metallic mercury inhalation exposure in rats. Neurotoxicol. Teratol. 15(6):391-6.
Dantas, D.C., and M.L. Queiroz. 1997. Immunoglobulin E and autoantibodies in mercury-exposed workers. Immunopharmacol. Immunotoxicol. 19(3): 383-92.
Danziger, S.J., and P.A. Possick. 1973. Metallic mercury exposure in scientific glassware manufacturing plants . J. Occup. Med. 15(1):15-20.
Davidson, P.W., G.J. Myers, C. Cox, C. Shamlaye, O. Choisy, J. Sloane-Reeves, E. Cernchiari, D.O. Marsh, M. Berlin, M. Tanner, and T.W. Clarkson. 1995a. Neurodevelopmental test selection, administration, and performance in the main Seychelles child development study. Neurotoxicology 16(4):665-676.
Davidson, P.W., G.J. Myers, C. Cox, C.F. Shamlaye, D.O. Marsh, M.A. Tanner, M. Berlin, J. Sloane-Reeves, E. Cernichiari, O. Choisy, A. Choi, and T.W. Clarkson. 1995b. Longitudinal neurodevelopmental study of Seychellois children following in utero exposure to methylmercury from maternal fish ingestion: outcomes at 19 and 29 months. Neurotoxicology 16(4):677-688.
Davidson, P.W., G.J. Myers, C. Cox, C. Axtell, C. Shamlaye, J. Sloane-Reeves, E. Cernichiari, L. Needham, A. Choi, Y. Wang, M. Berlin, and T.W. Clarkson. 1998. Effects of prenatal and postnatal methylmercury exposure from fish consumption on neurodevelopment:outcomes at 66 monts of age in the Seychelles child development study. JAMA 280(8):701-707.
Davidson, P.W., G.J. Myer, C. Shamlaye, C. Cox, P. Gao, C. Axtell, D. Morris, J. Sloane-Reeves, E. Cernichiari, A. Choi, D. Palumbo, and T.W. Clarkson. 1999. Association between prenatal exposure to methylmercury and developmental outcomes in Seychellois children: Effect modification by social and environmental factors. Neurotoxicology 20(5):833-41.
Dietrich, K.N., and D. Bellinger. 1994. The assessment of neurobehavioral development in studies of the effects of prenatal exposure to toxicants. Pp. 57-85 in Prenatal Exposure to Toxicants: Developmental Consequences, H.L. Needleman, and D. Bellinger, eds. Baltimore, MD: Johns Hopkins University Press.
Dietrich, K.N., K.M. Krafft, R.L. Bornschein, P.B. Hammond, O. Berger, P.A. Succop, and M. Bier. 1987. Low-level fetal lead exposure effect on neurobehavioral development in early infancy. Pediatrics 80(5):721-730.
Druet, E., J.C. Guery, K. Ayed, B. Guilbert, S. Avrameas, and P. Druet. 1994. Characteristics of polyreactive and monospecific IgG anti-laminin autoantibodies in the rat mercury model. Immunology 83(3):489-494.
Dyall-Smith, D.J., and J.P. Scurry. 1990. Mercury pigmentation and high mercury levels from the use of a cosmetic cream. Med. J. Aust. 153(7):409-410; 414-415.
Dyer, R.S., C.U. Eccles, and Z. Annau. 1978. Evoked potential alterations following prenatal methyl mercury exposure . Pharmacol. Biochem. Behav. 8(2):137-41.
Eccles, C.U., and Z. Annau. 1982a. Prenatal methylmercury exposure: I. Alterations in neonatal activity . Neurobehav. Toxicol. Teratol. 4(3):371-376.
Eccles, C.U., and Z. Annau. 1982b. Prenatal methylmercury exposure: II. Alterations in learning and psychotropic drug sensitivity in adult offspring. Neurobehav. Toxicol. Teratol. 4(3):377-382.
Elghany, N.A., W. Stopford, W.B. Bunn, and L.E. Fleming. 1997. Occupational exposure to inorganic mercury vapour and reproductive outcomes. Occup. Med. ( Lond) 47(6):333-6.
Eisner, J. 1991. Tactile-kinesthetic system of rats as an animal model for minimal brain dysfunction. Arch. Toxicol. 65(6):465-73.
Evans, H.L., R.H. Garman, and B. Weiss. 1977. Methylmercury: exposure duration and regional distribution as determinants of neurotoxicity in nonhuman primates. Toxicol. Appl. Pharmacol. 41(1):15-33.
Fehling, C., M. Abdulla, A. Brun, M. Dictor, A. Schutz, and S. Skerfving. 1975. Methylmercury poisoning in the rat: a combined neurological, chemical, and histopathological study. Toxicol. Appl. Pharmacol. 33(1):27-37.
Fenson, L., P.S. Dale, J.S. Reznick, D. Thal, E. Bates, J.P. Hartung, S. Pethick, and J.S. Reilly. 1993. MacArthur Communicative Development Inventory: User's Guide and Technical Manual. San Diego, CA : Singular Publishing Group.
Fiskesjo, G. 1979. Two organic mercury compounds tested for mutagenicity in mammalian cells by use of the cell line V 79-4. Hereditas 90:103-109.
Fowler, B.A. 1972. Ultrastructural evidence for nephropathy induced by long-term exposure tosmall amounts of methyl mercury. Science 175(23):780-781.
Franchi, E., G. Loprieno, M. Ballardin, L. Petrozzi, and L. Migliore. 1994. Cytogenetic monitoring of fishermen with environmental mercury exposure . Mutat. Res. 320(1-2):23-9.
Fredriksson, A., L. Dahlgren, B. Danielsson, P. Eriksson, L. Dencker, and T. Archer. 1992. Behavioural effects of neonatal metallic mercury exposure in rats . Toxicology 74(2-3):151-60.
Fredriksson, A., L. Dencker, T. Archer, and B.R. Danielsson. 1996. Prenatal coexposure to metallic mercury vapour and methylmercury produce interac-
tive behavioural changes in adult rats. Neurotoxicol. Teratol. 18(2):129-34.
Fredriksson, A., A.T. Gardlund, K. Bergman, A. Oskarsson, B. Ohlin, B. Danielsson, and T. Archer. 1993. Effects of maternal dietary supplementation with selenite on the postnatal development of rat offspring exposed to methyl mercury in utero. Pharmacol. Toxicol. 72(6):377-82.
Frustaci, A., N. Magnavita, C. Chimenti, M. Caldarula, E. Sabbioni, R. Pietra, C. Cellini, G.F. Possati, and A. Maseri. 1999. Marked elevation of mycardial trace elements in idiopathic dilated cardiomyopathy compared with secondary cardiac dysfunction. J. Am. Coll. Cardiol. 33(6):1578-83.
Fuyuta, M., T. Fujimoto, and S. Hirata. 1978. Embryotoxic effects of methylmercuric chloride administered to mice and rats during organogenesis. Teratology 18(3):353-366.
Fuyuta, M., T. Fujimoto, and E. Kiyofuji. 1979. Teratogenic effects of a single oral administration of methylmercuric chloride in mice. Acta Anat. ( Basel) 104(3):356-62.
Geyer, M.A., R.E. Butcher, and K. Fite. 1985. A study of startle and locomotor activity in rats exposed prenatally to methylmercury. Neurobehav. Toxicol. Teratol. 7(6):759-65.
Gilbert, S.G., and K.S. Grant-Webster. 1995. Neurobehavioral effects of developmental methylmercury exposure. Environ. Health Perspect. 103(Suppl. 6):135-42.
Gilbert, S.G., T.M. Burbacher, and D.C. Rice. 1993. Effects of in utero methylmercury exposure on a spatial delayed alternation task in monkeys. Toxicol. Appl. Pharmacol. 123(1):130-6.
Gilbert, S.G., D.C. Rice, and T.M. Burbacher. 1996. Fixed interval/fixed ratio performance in adult monkeys exposed in utero to methylmercury. Neurotoxicol. Teratol. 18(5):539-46.
Ghosh, A.K., S. Sen, A. Sharma, and G. Talukder. 1991. Effect of chlorophyllin on mercuric chloride-induced clastogenicity in mice. Food Chem. Toxicol. 29(11):777-779.
Grandjean, P., P. Weihe, and R.F. White. 1995. Milestone development in infants exposed to methylmercury from human milk. Neurotoxicology 16(1):27-34.
Grandjean, P., P. Weihe, P.J. Jørgensen, T. Clarkson, E. Cernichiari, and T. Viderø. 1992. Impact of maternal seafood diet on fetal exposure to mercury, selenium, and lead. Arch. Environ. Health 47(3):185-195.
Grandjean, P., P. Weihe, R.F. White, F. Debes, S. Araki, K. Yokoyama, K. Murata, N. Sørensen, R. Dahl, and P.J. Jørgensen. 1997. Cognitive deficit in 7-year-old children with prenatal exposure to methylmercury. Neurotoxicol. Teratol. 19(6):417-428.
Grandjean, P., P. Weihe, R.F. White, and F. Debes. 1998. Cognitive perfor-
mance of children prenatally exposed to “safe” levels of methylmercury. Environ. Res. 77(2):165-172.
Grandjean, P., R. White, A. Nielsen, D. Cleary, and E.C. de Oliveira Santos. 1999. Methylmercury neurotoxicity in Amazonian children downstream from gold mining. Environ. Health Perspect. 107(7):587-591.
Gunderson, V.M., K.S. Grant, T.M. Burbacher, J.F. Fagan, 3d, and N.K. Mottet. 1986. The effect of low-level prenatal methylmercury exposure on visual recognition memory in infant crab-eating macaques. Child Dev. 57(4):1076-83.
Gunderson, V.M., K.S. Grant-Webster, T.M. Burbacher, and N.K. Mottet. 1988. Visual recognition memory deficits in methylmercury-exposed Macaca fascicularis infants. Neurotoxicol. Teratol. 10(4):373-9.
Hallee, T.J. 1969. Diffuse lung disease caused by inhalation of mercury vapor. Am. Rev. Respir. Dis. 99(3):430-6.
Harada, M. 1995. Minamata Disease: Methylmercury poisoning in Japan caused by environmental pollution. Crit. Rev. Toxicol. 25(1):1-24.
Harada, M. 1997. Neurotoxicity of methylmercury: Minamata and the Amazon. Pp. 177-188 in Mineral and Metal Neurotoxicology, M. Yasui, M.J. Strong, K. Ota, and M.A. Verity, eds. Boca Raton, FL: CRC Press.
Harada, M., H. Akagi, T. Tsuda, T. Kizaki, and H. Ohno. 1999. Methylmercury level in umbilical cords from patients with congenital Minamata disease. Sci. Total Environ. 234(1-3):59-62.
Hirano, M., K. Mitsumori, K. Maita, and Y. Shirasu. 1986. Further carcinogenicity study on methylmercury chloride in ICR mice . Nippon Juigaku Zasshi (Jpn. J. Vet. Sci.) 48(1):127-135.
Höök, O., K.D. Lundgren, and A. Swensson. 1954. On alkyl mercury poisoning: With a description of two cases. Acta Med. Scand. 150(2):131-137.
Hu, H., G. Moller, and M. Abedi-Valugerdi. 1999. Mechanism of mercury-induced autoimmunity: Both T helper 1- and T helper 2-type responses are involved. Immunology 96(3):348-57.
Hua, J., L. Pelletier, M. Berlin, and P. Druet. 1993. Autoimmune glomerulonephritis induced by mercury vapour exposure in the Brown Norway rat. Toxicology 79(2):119-29.
Hughes, J.A., and Z. Annau. 1976. Postnatal behavioral effects in mice after prenatal exposure to methylmercury . Pharmacol. Biochem. Behav. 4(4):385-391.
Hultman, P., and H. Hansson-Georgiadis. 1999. Methyl mercury-induced autoimmunity in mice. Toxicol. Appl. Pharmacol. 154(3):203-11.
Hunter, D., R.R. Bomford, and D.S. Russell. 1940. Poisoning by methyl mercury compounds. Quart. J. Med. 9(July):193-213.
Ilbäck, N.G. 1991. Effects of methyl mercury exposure on spleen and blood
natural killer (NK) cell activity in the mouse. Toxicology 67(1):117-124.
Ilbäck N.G., J. Sundberg, and A. Oskarsson. 1991. Methyl mercury exposure via placenta and milk impairs natural killer (NK) cell function in newborn rats. Toxicol. Lett. 58(2):149-58.
Ilbäck, N.G., L. Wesslen, J. Fohlman, and G. Friman. 1996. Effects of methyl mercury on cytokines, inflammation and virus clearance in a common infection (coxsackie B3 myocarditis). Toxicol. Lett. 89(1):19-28.
Inouye, M., and Y. Kajiwara. 1988. Developmental disturbances of the fetal brain in guinea pigs caused by methylmercury. Arch. Toxicol. 62(1):15-21.
Inouye, M., and U. Murakami. 1975. Teratogenic effect of orally administered methylmercuric chloride in rats and mice. Congenital Anomalies 15(1):1-9.
Inskip, M.J., and J.K. Piotrowski. 1985. Review of the health effects of methylmercury. J. Appl. Toxicol. 5(3):113-33.
IPCS (International Programme on Chemical Safety). 1990. Environmental Health Criteria Document 101 - Methylmercury. Geneva: World Health Organization.
Jacobs, J.M., N. Carmichael, and J.B. Cavanagh. 1977. Ultrastructural changes in the nervous system of rabbits poisoned with methyl mercury. Toxicol. Appl. Pharmacol. 39(2):249-61.
Jalili, H.A., and A.H. Abbasi. 1961. Poisoning by ethyl mercury toluene sulphonanilide. Br. J. Ind. Med. 18:303-308.
Janicki, K., J. Dobrowolski, and K. Krasnicki. 1987. Correlation between contamination of the rural environment with mercury and occurrence of leukemia in men and cattle. Chemosphere 16(1):253-257.
Kanematsu, N., M. Hara, and T. Kada. 1980. Rec assay and mutagenicity studies on metal compounds. Mutat. Res. 77(2):109-116.
Kazantzis, G., K.F. Schiller, A.W. Asscher, and R.G. Drew. 1962. Albuminuria and the nephrotic syndrome following exposure to mercury and its compounds. Quart. J. Med. 31(Oct.):403-418.
Khera, K.S. 1973a. Reproductive capability of male rats and mice treated with methylmercury . Toxicol. Appl. Pharmacol. 24(2):167-77.
Khera, K.S. 1973b. Teratogenic effects of methylmercury in the cat: Note on the use of this species as a model for teratogenicity studies. Teratology 8(3): 293-303.
Khera, K.S., and S.A. Tabacova. 1973. Effects of methylmercuric chloride on the progeny of mice and rats treated before or during gestation. Food Cosmet. Toxicol. 11(2):245-254.
Khera, K.S., F. Iverson, L. Hierlihy, R. Tanner, and G. Trivett. 1974. Toxicity of methylmercury in neonatal cats. Teratology 10(1):69-76.
Kinjo, Y., S. Akiba, N. Yamaguchi, S. Mizuno, S. Watanabe, J. Wakamiya, M. Futatsuka, and H. Kato. 1996. Cancer mortality in Minamata disease pa-
tients exposed to methylmercury through fish diet. J. Epidemiol. 6(3):134-8.
Kinjo, Y., H. Higashi, A. Nakano, M. Sakamoto, and R. Sakai. 1993. Profile of subjective complaints and activities of daily living among current patients with Manamata disease after 3 decades. Environ. Res 63(2):241-251.
Kjellström, T., P. Kennedy, S. Wallis, and C. Mantell. 1986. Physical and Mental Development of Children with Prenatal Exposure to Mercury from Fish. Stage I: Preliminary tests at age 4. National Swedish Environmental Protection Board Report 3080. Solna, Sweden.
Kjellström, T., P. Kennedy, S. Wallis, A. Stewart, L. Friberg, B. Lind, T. Wutherspoon, and C. Mantell. 1989. Physical and Mental Development of Children with Prenatal Exposure to Mercury from Fish. National Swedish Environmental Protection Board Report No. 3642.
Koller, L.D. 1975. Methylmercury: effect on oncogenic and nononcogenic viruses in mice . Am. J. Vet. Res. 36(10):1501-4.
Koller, L.D., J.H. Exon, and B. Arbogast. 1977. Methylmercury: effect on serum enzymes and humoral antibody. J. Toxicol. Environ. Health 2(5):1115-1123.
Koopman-Esseboom, C., N. Weisglas-Kuperus, M.A. de Ridder, C.G. Van der Paauw, L.G. Tuinstra, and P.J. Sauer. 1996. Effects of polychlorinated biphenyl/dioxin exposure and feeding type on infants mental and psycho-motor development. Pediatrics 97(5):700-706.
Kosatsky, T., and P. Foran. 1996. Do historic studies of fish consumers support the widely accepted LOEL for methylmercury in adults. Neurotoxicology 17(1):177-86.
Kostka, B., M. Michalska, U. Krajewska, and R. Wierzbicki. 1989. Blood coagulation changes in rats poisoned with methylmercuric chloride (MeHg). Pol. J. Pharmacol. Pharm. 41(2):183-9.
Lauwerys, R., H. Roels, P. Genet, G. Toussaint, A. Bouckaert, and S. De Cooman. 1985. Fertility of male workers exposed to mercury vapor or to manganese dust: a questionnaire study. Am. J. Ind. Med. 7(2):171-6.
Lebel, J., D. Mergler, M. Lucotte, M. Amorim, J. Dolbec, D. Miranda, G. Arantes, I. Rheault, and P. Pichet. 1996. Evidence of early nervous system dysfunction in Amazonian populations exposed to low-levels of methylmercury. Neurotoxicology 17(1):157-167.
Lebel, J., D. Mergler, F. Branches, M. Lucotte, M. Amorim, F. Larribe, and J. Dolbec. 1998. Neurotoxic effects of low-level methylmercury contamination in the Amazonian Basin. Environ. Res. 79(1):20-32.
Lee, J.H., and D.H. Han. 1995. Maternal and fetal toxicity of methylmercuric chloride administered to pregnant Fischer 344 rats. J. Toxicol. Environ. Health 45(4):415-425.
Leyshon, K., and A.J. Morgan. 1991. An integrated study of the morphological and gross-elemental consequences of methyl mercury intoxication in rats,
with particular attention on the cerebellum. Scanning Microsc. 5(3):895-904.
MacDonald, J.S., and R.D. Harbison. 1977. Methyl mercury-induced encephalopathy in mice. Toxicol. Appl. Pharmacol. 39(2):195-205.
Magos, L., and W.H. Butler. 1972. Cumulative effects of methylmercury dicyandiamide given orally to rats. Food Cosmet. Toxicol. 10(4):513-7.
Marsh, D.O., T.W. Clarkson, C. Cox, G.J. Myers, L. Amin-Zaki, and S. Al-Tikriti. 1987. Fetal methylmercury poisoning: Relationship between concentration in single strands of maternal hair and child effects. Arch. Neurol. 44(10):1017-1022.
Marsh, D.O., M.D. Turner, J.C. Smith, P. Allen, and N. Richdale. 1995a. Fetal methylmercury study in a Peruvian fish-eating population. Neurotoxicology 16(4):717-726.
Marsh, D.O., T.W. Clarkson, G.J. Myers, P.W. Davidson, C. Cox, E. Cernichiari, M.A. Tanner, W. Ledhar, C. Shamlaye, O. Choisy, C. Hoareau, and M. Berlin. 1995b. The Seychelles study of fetal methylmercury exposure and child development: Introduction. Neurotoxicology 16(4):583-596.
Matsumoto, H., G. Koya, and T. Takeuchi. 1965. Fetal Minamata disease. A neuropathological study of two cases of intrauterine intoxication by a methyl mercury compound. J. Neuropathol. Exp. Neurol. 24(4):563-74.
Matsuo, N., T. Suzuki, and H. Akagi. 1989. Mercury concentration in organs of contemporary Japanese. Arch. Environ. Health 44(5):298-303.
McKeown-Eyssen, G.E., J. Ruedy, and A. Neims. 1983. Methyl mercury exposure in northern Quebec. II. Neurologic findings in children. Am. J. Epidemiol. 118(4):470-479.
Merigan, W.H., J.P. Maurissen, B. Weiss, T. Eskin, and L.W. Lapham. 1983. Neurotoxic actions of methylmercury on the primate visual system. Neurobehav. Toxicol. Teratol. 5(6):649-58.
Miller, C.T., Z. Zawidska, E. Nagy, and S.M. Charbonneau. 1979. Indicators of genetic toxicity in leukocytes and granulocytic precursors after chronic methylmercury ingestion by cats. Bull. Environ. Contam. Toxicol. 21(3):296-303.
Mitsumori, K., K. Maita, and Y. Shirasu. 1984. Chronic toxicity of methylmercury chloride in rats: Pathological study. Nippon Juigaku Zasshi ( Jpn. J. Vet. Sci.) 46(4):549-557.
Mitsumori, K., M. Hirano, H. Ueda, K. Maita, and Y. Shirasu. 1990. Chronic toxicity and carcinogenicity of methylmercury chloride in B6C3F1 mice. Fundam. Appl. Toxicol. 14(1):179-190.
Mitsumori, K., K. Maita, T. Saito, S. Tsuda, and Y. Shirasu. 1981. Carcinogenicity of methylmercury chloride in ICR mice: Preliminary note on renal carcinogenesis. Cancer Lett. 12(4):305-310.
Mitsumori, K., K. Takahashi, O. Matano, S. Goto, and Y. Shirasu. 1983.
Chronic toxicity of methylmercury chloride in rats: Clinical study and chemical analysis. Nippon Juigaku Zasshi (Jpn. J. Vet. Sci.) 45(6):747-757.
Mohamed, M., T. Burbacher, and N. Mottet. 1987. Effects of methylmercury on testicular functions in Macaca fascicularis monkeys. Pharmacol. Toxicol. 60(1):29-36.
Moszczynski, P., S. Slowinski, J. Rutkowski, S. Bem, and D. Jakus-Stoga. 1995. Lymphocytes, T and NK cells, in men occupationally exposed to mercury vapours. Int. J. Occup. Med. Environ. Health 8(1):49-56.
Mottet, N.K., C.M. Shaw, and T.M. Burbacher. 1987. The pathological lesions of methyl mercury intoxication in monkeys . Pp. 73-103 in The Toxicity of Methyl Mercury, C.U. Eccles, and Z. Annau, eds. Baltimore, MD: Johns Hopkins.
Munro, I.C., E.A. Nera, S.M. Charbonneau, B. Junkins, and Z. Zawidzka. 1980. Chronic toxicity of methylmercury in the rat. J. Environ. Pathol. Toxicol. 3(5-6):437-447.
Murata, K., P. Weihe, A. Renzoni, F. Debes, R. Vasconcelos, F. Zino, S. Araki, P.J. Jorgensen, R.F. White, and P. Grandjean. 1999a. Delayed evoked potentials in children exposed to methylmercury from seafood. Neurotoxicol. Teratol. 21(4):343-348.
Murata, K., P. Weihe, S. Araki, E. Budtz-Jorgensen, and P. Grandjean. 1999b. Evoked potentials in Faroese children prenatally exposed to methylmercury . Neurotoxicol. Teratol. 21(4):471-472.
Murphy, M.J., E.J. Culliford, and V. Parsons. 1979. A case of poisoning with mercuric chloride. Resuscitation 7(1):35-44.
Müsch, H.R., M. Bornhausen, H. Kriegel, and H. Greim. 1978. Methylmercury chloride induces learning deficits in prenatally treated rats. Arch. Toxicol. 40(2):103-108.
Myers, G.J., P.W. Davidson, C.F. Shamlaye, C.D. Axtell, E. Cernichiari, O. Choisy, A. Choi, C. Cox, and T.W. Clarkson. 1997. Effects of prenatal methylmercury exposure from a high fish diet on developmental milestones in the Seychelles Child Development Study . Neurotoxicology 18(3):819-830.
Myers, G.J., D.O. Marsh, C. Cox, P.W. Davidson, C.F. Shamlaye, M.A. Tanner, A. Choi, E. Cernichiari, O. Choisy, and T.W. Clarkson. 1995a. A pilot neurodevelopmental study of Seychellois children following in utero exposure to methylmercury from a maternal fish diet. Neurotoxicology 16(4):629-638.
Myers, G.J., D.O. Marsh, P.W. Davidson, C. Cox, C.F. Shamlaye, M. Tanner, A. Choi, E. Cernichiari, O. Choisy, and T.W. Clarkson. 1995b. Main neurodevelopmental study of Seychellois children following in utero exposure to methylmercury from a maternal fish diet: Outcome at six months. Neurotoxicology 16(4):653-664.
Myers, G.J., P.W. Davidson, C. Cox, C.F. Shamlaye, M.A. Tanner, O. Choisy, J. Sloane-Reeves, D.O. Marsh, E. Cernichiari, A. Choi, M. Berlin, and T.W. Clarkson. 1995c. Neurodevelopmental outcomes of Seychellois children sixty-six months after in utero exposure to methylmercury from a maternal fish diet: Pilot study. Neurotoxicology 16(4):639-652.
Nakatsuru, S., J. Oohashi, H. Nozaki, S. Nakada, and N. Imura. 1985. Effect of mercurials on lymphocyte functions in vitro. Toxicology 36(4):297-306.
Newberne, P.M., O. Glaser, L. Friedman, and B.R. Stillings. 1972. Chronic exposure of rats to methyl mercury in fish protein. Nature 237(5349):40-41.
Newland, M.C., S. Yezhou, B. Logdberg, and M. Berlin. 1994. Prolonged behavioral effects of in utero exposure to lead or methyl mercury: Reduced sensitivity to changes in reinforcement contingencies during behavioral transitions and in steady state. Toxicol. Appl. Pharmacol. 126(1):6-15.
NRC (National Research Council). 1991. Frontiers in Assessing Human Exposures to Environmental Toxicants : Report of the Symposium. Washington, DC: National Academy Press.
NRC (National Research Council). 1997. Environmental Epidemiology, Vol. 2.: Use of the Gray Literature and Other Data in Environmental Epidemiology. Washington, DC: National Academy Press.
O'Kusky, J. 1983. Methylmercury poisoning of the developing nervous system: Morphological changes in neuronal mitochondria. Acta Neuropathol. ( Berl) 61(2):116-22.
Olson, K., and G.M. Bousch. 1975. Decreased learning capacity in rats exposed prenatally and postnatally to low doses of mercury. Bull. Environ. Contam. Toxicol. 13(1):73-9.
Ortega, H.G., M. Lopez, A. Takaki, Q.H. Huang, A. Arimura, and J.E. Salvaggio. 1997. Neuroimmunological effects of exposure to methylmercury forms in the Sprague-Dawley rats. Activation of the hypothalamic-pituitary-adrenal axis and lymphocyte responsiveness. Toxicol. Ind. Health 13(1):57-66.
Popescu, H.I., L. Negru, and I. Lancranjan. 1979. Chromosome aberrations induced by occupational exposure to mercury . Arch. Environ. Health 34(6):461-3.
Queiroz, M.L., and D.C. Dantas. 1997. B lymphocytes in mercury-exposed workers. Pharmacol. Toxicol. 81(3):130-3.
Queiroz, M.L., and D.C. Dantas. 1997a. T lymphocytes in mercury-exposed workers. Immunopharmacol. Immunotoxicol. 19(4):499-510.
Queiroz, M.L., C. Bincoletto, M.R. Quadros, and E.M. De Capitani. 1999. Presence of micronuclei in lymphocytes of mercury exposed workers . Immunopharmacol. Immunotoxicol. 21(1):141-50.
Rasmussen, E.B., and M.C. Newland. 1999. Acquisition of a Multiple DRH
Extinction Schedule of Reinforcement in Rats Exposed during Development to Methylmercury. No. 697. Pp. 149. SOT 1999 Annual Meeting.
Reuhl, K.R., L.W. Chang, and J.W. Townsend. 1981a. Pathological effects of in utero methylmercury exposure on the cerebellum of the golden hamster. 1. Early effects upon the neonatal cerebellar cortex. Environ. Res. 26(2):281-306.
Reuhl, K.R., L.W. Chang, and J.W. Townsend. 1981b. Pathological effects of in utero methylmercury exposure on the cerebellum of the golden hamster. II. Residual effects on the adult cerebellum . Environ. Res. 26(2):307-27.
Rice, D.C. 1989. Delayed neurotoxicity in monkeys exposed developmentally to methylmercury . Neurotoxicology 10(4):645-650.
Rice, D.C. 1992. Effects of pre- plus postnatal exposure to methylmercury in the monkey on fixed interval and discrimination reversal performance. Neurotoxicology 13(2):443-52.
Rice, D.C. 1996. Evidence for delayed neurotoxicity produced by methylmercury. Neurotoxicology 17(3-4):583-596.
Rice, D.C. 1998. Age-related increase in auditory imapirment in monkeys exposed in utero plus postnatally to methylmercury. Toxicol. Sci. 44(2):191-196.
Rice, D.C., and S.G. Gilbert. 1982. Early chronic low-level methylmercury poisoning in monkeys impairs spatial vision. Science 216(4547):759-761.
Rice, D.C., and S.G. Gilbert. 1990. Effects of developmental exposure to methyl mercury on spatial and temporal visual function in monkeys. Toxicol. Appl. Pharmacol. 102(1):151-63.
Rice, D.C., and S.G. Gilbert. 1992. Exposure to methyl mercury from birth to adulthood impairs high-frequency hearing in monkeys. Toxicol. Appl. Pharmacol. 115(1):6-10.
Rice, D.C., and S.G. Gilbert. 1995. Effects of developmental methylmercury exposure or lifetime lead exposure on vibration sensitivity function in monkeys. Toxicol. Appl. Pharmacol. 134(1):161-9.
Robison, S.H., O. Cantoni, and M. Costa. 1984. Analysis of metal-induced DNA lesions and DNA-repair replication in mammalian cells. Mutat. Res. 131(3-4): 173-81.
Rogan, W.J., and B.C. Gladen. 1991. PCBs, DDE, and child development at 18 and 24 months. Ann. Epidemiol. 1(5):407-413.
Rowland, A.S., D.D. Baird, C.R. Weinberg, D.L. Shore, C.M. Shy, and A.J. Wilcox. 1994. The effect of occupational exposure to mercury vapour on the fertility of female dental assistants. Occup. Environ. Med. 51(1):28-34.
Salonen, J.T., K. Seppänen, K. Nyyssönen, H. Korpela, J. Kauhanen, M. Kantola, J. Tuomilehto, H. Esterbauer, F. Tatzber, and R. Salonen. 1995. Intake of mercury from fish, lipid peroxidation, and the risk of myocardial infarction
and coronary, cardiovascular, and any death in Eastern Finnish men . Circulation 91(3):645-655.
Samuels, E.R., H.M. Heick, P.N. McLaine, and J.P. Farant. 1982. A case of accidental inorganic mercury poisoning. J. Anal. Toxicol. 6(3):120-2.
Schalock, R.L., W.J. Brown, R.A. Kark, and N.K. Menon. 1981. Perinatal methylmercury intoxication: behavioral effects in rats. Dev. Psychobiol. 14(3):213-9.
Schroeder, H., and M. Mitchener. 1975. Life-time effects of mercury, methyl mercury, and nine other trace metals in mice. J. Nutr. 105(4):452-458.
Sekowski, J.W., L.H. Malkas, Y. Wei, and R.J. Hickey. 1997. Mercuric ion inhibits the activity and fidelity of the human cell DNA synthesome. Toxicol. Appl. Pharmacol. 145(2):268-76.
Shaw, C.M., N.K. Mottet, and D.V. Finocchio. 1979. Cerebrovascular lesions in experimental methyl mercurial encephalopathy . Neurotoxicology 1(1):57-74.
Shenker B.J., P. Berthold, C. Rooney, L. Vitale, K. DeBolt, and I.M. Shapiro. 1993. Immunotoxic effects of mercuric compounds on human lymphocytes and monocytes. III. Alterations in B-cell function and viability. Immunopharmacol. Immunotoxicol. 15(1):87-112.
Shenker, B.J., T.L. Guo, and I.M. Shapiro. 1999. Induction of apoptosis in human T-cells by methyl mercury: Temporal relationship between mitochondrial dysfunction and loss of reductive reserve. Toxicol. Appl. Pharmacol. 157(1):23-35.
Siblerud, R.L.. 1990. The relationship between mercury from dental amalgam and the cardiovascular system. Sci. Total Environ. 99(1-2):23-35.
Skerfving, S., K. Hansson, and J. Lindsten. 1970. Chromosome breakage in humans exposed to methyl mercury through fish consumption. Arch. Environ. Health 21(2):133-139.
Skerfving, S., K. Hansson, C. Mangs, J. Lindsten, and N. Ryman. 1974. Methylmercury-induced chromosome damage in man. Environ. Res. 7(1):83-98.
Slotkin, T.A., S. Pachman, J. Bartolome, and R.J. Kavlock. 1985. Biochemical and functional alterations in renal and cardiac development resulting from neonatal methylmercury treatment. Toxicology 36(2-3):231-41.
Solecki, R., L. Hothorn, M. Holzweissig, and V. Heinrich. 1991. Computerised analysis of pathological findings in longterm trials with phenylmercuric acetate in rats. Arch. Toxicol. (Suppl.):14:100-3.
Soni, J.P., R.U. Singhania, A. Bansal, and G. Rathi. 1992. Acute mercury vapor poisoning. Indian Pediatr. 29(3):365-8.
Sørensen, N., K. Murata, E. Budtz-Jørgensen, P. Weihe, and P. Grandjean. 1999.
Prenatal methylmercury exposure as a cardiovascular risk factor at seven years of age. Epidemiology 10(4):370-375.
Spyker, J.M. 1975. Assessing the impact of low level chemicals on development: Behavioral and latent effects. Fed. Proc. 34(9):1835-44.
Spyker, J., S. Sparber, and A.M. Goldberg. 1972. Subtle consequences of methylmercury exposure: Behavioral deviations in offspring of treated mothers. Science 177(49):621-623.
Steuerwald, U., P. Weihe, P. Jorgensen, K. Bjerve, J. Brock, B. Heinzow, E. Budtz-Jørgensen, and P. Grandjean. 2000. Maternal seafood diet, methylmercury exposure, and neonatal neurological function. J. Pediatr. 136(5):599-605.
Su, M.Q., and G.T. Okita. 1976. Behavioral effects on the progeny of mice treated with methylmercury . Toxicol. Appl. Pharmacol. 38(1):195-205.
Tamashiro, H., H. Akagi, M. Arakaki, M. Futatsuka, and L.H. Roht. 1984. Causes of death in Minamata disease: Analysis of death certificates . Int. Arch. Occup. Environ. Health 54(2):135-146.
Tamashiro, H., M. Arakaki, M. Futatsuka, and E.S. Lee. 1986. Methylmercury exposure and mortality in southern Japan: A close look at causes of death. J. Epidemiol. Community Health 40(2):181-185.
Takeuchi, T. 1968. Pathology of Minamate disease. Pp. 141-228 in Minamata Disease. Study Group of Minanata Disease, ed. Kumamoto, Japan: Kumamoto University.
Thompson, S.A., K.L. Roellich, A. Grossmann, S.G. Gilbert, and T.J. Kavanagh. 1998. Alterations in immune parameters associated with low level methylmercury exposure in mice. Immunopharmacol Immunotoxicol 20(2):299-314.
Thuvander, A., J. Sundberg, and A. Oskarsson. 1996. Immunomodulating effects after perinatal exposure to methylmercury in mice. Toxicology 114(2):163-75.
Tsubaki, T., and H. Takahashi, eds. 1986. Clinical aspects of Minamata disease. Neurological aspects of methylmercury poisoning in Minamata. Pp. 41-57 in Recent Advances in Minamata Disease Studies. Tokyo: Kodansha.
Tubbs, R.R., G.N. Gephardt, J.T. McMahon, M.C. Pohl, D.G. Vidt, S.A. Barenberg, and R. Valenzuela. 1982. Membranous glomerulonephritis associated with industrial mercury exposure. Study of pathogenetic mechanisms. Am. J. Clin. Pathol. 77(4):409-13.
Uchino, M., T. Okajima, K. Eto, T. Kumamoto, I. Mishima, and M. Ando. 1995. Neurologic features of chronic Minamata disease (organic mercury poisoning) certified at autopsy. Intern. Med. 34(8):744-7.
Verschaeve, L., M. Kirsch-Volders, C. Susanne, C. Groetenbriel, R.
Haustermans, A. Lecomte, and D. Roossels. 1976. Genetic damage induced by occupationally low mercury exposure. Environ. Res. 12(3):306-16.
Verschuuren, H.G., R. Kroes, E.M. Den Tonkelaar, J.M. Berkvens, P.W. Helleman, A.G. Rauws, P.L. Schuller, and G.J. Van Esch. 1976. Toxicity of methylmercury chloride in rats. III. Long-term toxicity study. Toxicology 6(1):107-123.
Vorhees, C.V. 1985. Behavioral effects of prenatal methylmercury in rats: A parallel trial to the Collaborative Behavioral Teratology Study. Neurobehav. Toxicol. Teratol. 7(6):717-25.
Vroom, F.Q., and M. Greer. 1972. Mercury vapour intoxication. Brain 95(2): 305-18.
Wakita, Y. 1987. Hypertension induced by methyl mercury in rats. Toxicol. Appl. Pharmacol. 89(1):144-7.
Warkany, J., and D.M. Hubbard. 1953. Acrodynia and mercury. J. Pediat. 42(3):365-386.
Wasserman, G., J.H. Graziano, P. Factor-Litvak, D. Popovac, N. Morina, A. Musabegovic, N. Vrenezi, S. Capuni-Paracka, V. Lekic, E. Preteni-Redjepi, S. Hadjialjevic, V. Slavkovich, J. Kline, P. Shrout, and Z. Stein. 1992. Independent effects of lead exposure and iron deficiency anemia on developmental outcome at age 2 years. J. Pediatr. 121(5 Pt. 1):695-703.
Wassick, K.H., and A. Yonovitz. 1985. Methyl mercury ototoxicity in mice determined by auditory brainstem responses. Acta Otolaryngol. 99(1-2): 35-45.
Weiss, B. 1998. A risk assessment perspective on the neurobehavioral toxicity of endocrine disruptors. Toxicol. Ind. Health 14(1-2):341-59.
WHO (World Health Organization). 1976. Mercury. Environmental Health Criteria 1. Geneva, Switzerland: World Health Organization.
Wild, L.G., H.G. Ortega, M. Lopez, and J.E. Salvaggio. 1997. Immune system alteration in the rat after indirect exposure to methylmercury chloride or methylmercury sulfide. Environ. Res. 74(1):34-42.
Williams, M.V., T. Winters, and K.S. Waddell. 1987. In vivo effects of mercury (II) on deoxyuridine triphosphate nucleotidohydrolase, DNA polymerase (alpha, beta), and uracil-DNA glycosylase activities in cultured human cells: relationship to DNA damage, DNA repair, and cytotoxicity. Mol. Pharmacol. 31(2):200-7.
Wössmann, W., M. Kohl, G. Grüning, and P. Bucsky. 1999. Mercury intoxication presenting with hypertension and tachycardia . Arch. Dis. Child. 80(6):556-7.
Wulf, H.C., N. Kromann, N. Kousgaard, J.C. Hansen, E. Niebuhr, and K. Alboge. 1986. Sister chromatid exchange (SCE) in Greenlandic Eskimos.
Dose-response relationship between SCE and seal diet, smoking, and blood cadmium and mercury concentrations. Sci. Total Environ. 48(1-2):81-94.
Yasutake, A., Y. Hirayama, and M. Inouye. 1991. Sex Difference of nephrotoxicity by methylmercury in mice. Pp. 389-396 in Nephrotoxicity: Mechanisms, Early Diagnosis, and Therapeutic Management . Fourth International Symposium of Nephrotoxicity, Guilford, England, UK, 1989. P.H. Bach, and K.J. Ullrich, eds. New York: Marcel Dekker.
Yoshida, Y., H. Kamitsuchibashi, R. Hamada, Y. Kuwano, I. Mishima, and A. Igata. 1992. Truncal hypesthesia in patients with Minamata disease. Intern. Med. 31(2):204-7.
Zenick, H. 1974. Behavioral and biochemical consequences in methylmercury chloride toxicity. Pharmacol. Biochem. Behav. 2(6):709-13.
Zenick, H. 1976. Evoked potential alterations in methylmercury chloride toxicity. Pharmacol. Biochem. Behav. 5(3):253-5.







































































































