
PAPER CONTRIBUTION E
Preadolescent and Adolescent Influences on Health
Cheryl L.Perry, Ph.D.
Adolescence, the stage of development between childhood and adulthood, and approximately the second decade of the life cycle, was first presented as a subject for scientific inquiry only a century ago by G.Stanley Hall (1904) and was characterized as the developmental stage of “storm and stress.” Manifestations of storm and stress included adolescents ' tendencies to contradict their parents, experience mood changes, and engage in antisocial behaviors (Arnett, 1999). After nearly 100 years of research, this picture of adolescence seems both limited in scope and too broad a generalization (even if the tendencies are still familiar and relevant). In particular, as we enter the twenty-first century, adolescence is viewed as part of life span development, with continuities from childhood, unique developmental challenges and tasks, and implications for adulthood. Adolescence is also examined within context, so that adolescence is seen as a dynamic developmental process that is influenced by proximal and distal social environments. The manifestation of this developmental process can be seen in adolescents ' behaviors, behaviors that cause considerable concern in American society. Thus, this paper attempts to provide a snapshot of the dynamics of adolescence and adolescent behavior, what factors influence the adoption or maintenance of behavior, examples of how changes in behavior
|
Dr. Perry is professor, Division of Epidemiology, School of Public Health, University of Minnesota. This paper was prepared for the symposium, “Capitalizing on Social Science and Behavioral Research to Improve the Public's Health,” the Institute of Medicine, and the Commission on Behavioral and Social Sciences and Education of the National Research Council, Atlanta, Georgia, February 2–3, 2000. |
have been achieved, and the implications of this research for healthful adolescent development in the twenty-first century.
DEVELOPMENTAL INFLUENCES DURING ADOLESCENCE
The Dynamics of Adolescence
Adolescence is a time of metamorphosis. Some changes are biologically —and others socioculturally—determined. The latter are often referred to as the “developmental tasks” of adolescence and are discussed in the next section. From a biological viewpoint, during adolescence, children become adults. They experience puberty, acquire reproductive capabilities, and secondary sexual characteristics, and grow to reach full adult height (Susman, 1997). Hormones are primarily responsible for the biological changes in adolescence (Hopwood et al., 1990; Buchanan et al., 1992). The primary hormones begin to differ by gender at about age 11 (Susman, 1997), with the most dramatic biological changes occurring during early adolescence, between the ages of 12 and 16 (Tanner, 1978). The timing of biological changes differs by gender and racial or ethnic group (Money, 1980; Susman, 1997). On average, females mature 1–2 years ahead of males, and reach their full adult height by age 14 (Marshall and Tanner, 1970); African American females mature even earlier than white females (Kaplowitz and Oberfield, 1999). Interestingly, the age of pubertal onset, as measured by menarche in females, has become younger throughout the past century, most likely due to improved nutritional intake (Wyshak and Frisch, 1982; Hopwood et al., 1990; Herman-Giddens et al., 1997; Kaplowitz and Oberfield, 1999).
Hormonal changes have been “blamed” for their influence on adolescent mood and behavior. Recent provocative research suggests that hormones do influence behavior; the direct effects are small but stable and may be mediated by the social environment (Buchanan et al., 1992; Brooks-Gunn et al., 1994; Susman, 1997). For example, Olweus et al. (1988) found that boys with relatively higher testosterone levels were more likely to become aggressive if they were provoked. Thus, some boys might never exhibit aggressive behavior in a social environment without provocation. Similarly, Udry (1988) found that testosterone levels were a strong predictor of sexual involvement among young adolescent girls. This relationship was attenuated or eliminated by their involvement in sports or having a father in the home. Again, the hormone-behavior relationship existed, but did not manifest in particular environments.
Substantial research has been done on the timing of puberty relative to peers (Silbereisen et al., 1989). Early maturers are differentiated from on-time and late maturers in terms of the development of secondary sexual characteristics, height velocity, and menarche (Silbereisen and Kracke, 1993). Most studies in the United States have found that early maturation among boys is positive for them, with early maturers reporting more confidence, less dependence, and greater popularity than their peers (Nottelmann et al., 1990; Petersen and Taylor, 1980).
For girls, the picture is more mixed, with studies showing more negative affect, lower self-esteem, and greater contact with deviant peers among early-maturing females (Brooks-Gunn, 1988; Brooks-Gunn and Warren, 1989; Silbereisen and Kracke, 1993). However, these associations with early maturation may be mediated by social, cultural, and socioeconomic factors (Clausen, 1975; Silbereisen and Kracke, 1993). For example, in homes where the father was absent, females matured at significantly younger ages (Surbey, 1990). Also, closeness of mothers to their daughters was associated with slower maturational development among girls (Steinberg, 1989; Silbereisen and Kracke, 1993). Thus, even for biological changes that are examined relative to age-mates or peers, the rate of maturation may be mediated by the social context of the adolescent.
Changes in cognitive processes also occur during preadolescence and adolescence. These changes may be the result of continued brain growth during adolescence and more efficient neural processing (Crockett and Petersen, 1993; Brownlee, 1999). Pre- and young adolescents are concrete thinkers (Blum and Stark, 1985). To experience something, concrete thinkers need to see, feel, touch, smell, or hear it, rather than being able to rely on abstract descriptions. By middle or late adolescence, formal operational or abstract thinking is possible (Blum and Stark, 1985; Crockett and Petersen, 1993). Rather than strictly relying on experience, abstract thinkers can generate hypotheses, possible solutions, rules, and ideals using symbols and abstractions. Adolescents can learn to arrange pieces of information into multiple combinations, understand words that are not reflecting real life, think about thinking, and conceptualize ideals. However, many adolescents may not attain formal operational thinking levels (Flavell, 1985) or may revert to concrete thinking in unfamiliar or emotionally charged situations (Hamburg, 1986).
The level and sophistication of thinking has important implications for adolescents' behavior. As concrete thinkers, young adolescents cannot truly comprehend abstract concepts such as “health” or project the outcomes of their current behavior into the future (Blum and Stark, 1985). Even as adolescents learn to think abstractly, this occurs through trial, error, and experimentation. Messages about health behaviors, therefore, that rely on long-term consequences or fail to provide relevant and concrete examples will have little meaning to many adolescents. Likewise, adolescents may misperceive that others are preoccupied with them, confusing their own thoughts with the thoughts of others (Arnett, 1992). This can lead to a sense of invulnerability and participation in reckless behavior (Elkind, 1967; Arnett, 1992). The lack of rational and abstract thinking abilities leaves adolescents particularly vulnerable to messages from the social environment that portray some behaviors, such as smoking, drinking, and sexual behavior, as potentially functional and rewarding (Perry, 1999a), even though the longer-term consequences may be dire for them.
In terms of biology, then, adolescents are maturing earlier than in previous times; so physically, they become adults at a younger age, yet do not have the cognitive capabilities to cope with a complex social environment as adults. Ad-
ditionally, the changes within and between adolescents are not synchronous — there are enormous differences in the rate and timing of these changes. This sets the stage for a kind of “prolonged” adolescence, during which young people are expected to become prepared to become adults in our society, mentally and socially, yet with physical bodies that are already mature. This tension may contribute to some of the problems associated with adolescents, such as precocious or unprotected sexual behavior, which have a biological as well as a social etiology (Hine, 1999).
The “Tasks” of Adolescence
Puberty and the associated physical and cognitive changes are perhaps the only parts of adolescence that are culture-free; that is, adolescents worldwide experience these metamorphoses. Yet, as the examples above indicate, even biological changes interact with social environmental factors to influence adolescent behavior. Still, from within specific cultures and subcultures come the answers to the question, What are adolescents supposed to achieve during this developmental stage? These achievements are considered the psychosocial tasks of adolescence (Havighurst, 1972; Hill, 1980; Hill and Holmbeck, 1986; Masten et al., 1995).
For adolescents in the United States, the specific tasks have been described in psychological and social terms, and include accomplishments related to autonomy, sexuality, attachment, intimacy, achievement, and identity (Havighurst, 1972; Hill and Holmbeck, 1986). Adolescents strive to accomplish these tasks (1) to become independent and able to make their own decisions, (2) to understand their changing social-sexual roles and sexual identity, (3) to change their relationships with their parents, (4) to transform acquaintances into deeper friendships, (5) to focus their ambitions on their futures, and (6) to transform their images of themselves to accommodate their physical and psychosocial changes. These tasks have been characterized as the driving forces in adolescent behavior (Havighurst, 1972). Adolescents are more likely to think of themselves as being adults when these psychosocial tasks, rather than particular events, such as high school graduation, are achieved (Scheer et al., 1996). However, these tasks may also be changing in scope and interpretation as greater cultural and ethnic diversity is found throughout the United States.
Recent research has examined the continuity and coherence of developmental tasks in childhood and adulthood, using sophisticated methodologies. Masten et al. (1995) defined developmental tasks as “broad dimensions of effective behavior evaluated in comparison to normative expectations for people of a given age” (p. 1636). They observed three areas of competence in late childhood and adolescence (academic achievement, rule-abiding conduct, and getting along with peers) and two additional areas that emerge in adolescence (holding a job for pay and romantic relationships). Using structural equation modeling techniques, they examined the coherence of these areas of competence and demonstrated the continuity of the three childhood areas into late adoles-
cence. Notably, rule-abiding or rule-breaking conduct in late childhood strongly predicted such conduct in adolescence, thus “demonstrating the stability of anti-social behavior by late childhood” (Masten et al., 1995, p. 1654). Adolescent conduct problems in adolescence were also associated with lower academic achievement and being able to hold a job. This suggests that focusing attention on early conduct problems and competencies in childhood should be beneficial for academic and job achievements, as well as reducing conduct problems, in adolescence (Moffitt, 1993; Masten et al., 1995). Additionally, this study strongly underlines the need to examine early precursors to some adolescent behaviors as an avenue to early prevention and intervention.
The promotion of positive youth development is complementary to the goal of healthfully achieving the developmental tasks of childhood or adolescence (Catalano et al., 1999). As Bronfenbrenner and Morris (1998, p. 996) note:
Especially in its early phases, but also throughout the life course, human development takes place through progressively more complex reciprocal interactions between an active, evolving, biopsychological human organism and the person, objects, and symbols in its immediate external environment. To be effective, the interaction must occur on a fairly regular basis over extended periods of time.
The authors then describe the developmental process for adolescents as a series of interactions within particular social contexts—families, schools, neighborhoods, and communities—that progressively shape young people and their behavior (lessor, 1993). These interactions, and resulting behavior, are also determined by the time in history and the culture of the young person (Elder, 1974; Hine, 1999; Vega and Gil, 1998). Thus, the way in which youth develop, and whether they have the resources and environmental supports to achieve developmental tasks, serve as the background against which healthful or unhealthful behavior in the United States should be examined.
Threats to Health Among Preadolescents and Adolescents
Adolescence is the developmental period that has been characterized as the physically healthiest in the life cycle: adolescents have outgrown most of the childhood infectious diseases and are not yet old enough to suffer from the chronic diseases that plague adults (Ozer, Brindis et al., 1998). Yet, even a brief review of adolescent health issues suggests otherwise. Adolescents engage in a range of behaviors that impact their current and future risk of injury or premature death; many of these behaviors have their onset during this developmental stage (Blum, 1998; Perry, 1999b).
The United States continues to lead the developed world in adolescent mortality rates, even though there has been a significant decline in these rates in the past 10 years (Blum, 1998). Unintentional injuries, homicide, and suicide are the primary causes of adolescent mortality, accounting for four out of five deaths (Ozer et al., 1998). Among these deaths, more than half are due to motor vehicle collisions (CDC, 1993), and a third of those are related to alcohol use.
Fortunately, the fatal collision rate has been declining since 1980, primarily due to environmental and policy changes such as improved highway construction, safer cars, and a uniform 21-year-old drinking age (Blum, 1998). Of recent concern is the startling increase in the young adolescent suicide rate, which has risen 35% since 1990 among those 10 to 14 years old (Blum, 1998).
The mortality rates among adolescents show notable differences by ethnic or racial group and gender. Although there has been a 14% decline overall in mortality rates over the past decade, there has been a 17% decline among white males, and an 11% increase among African American males (Blum, 1998). Also among African American males, death from homicide is nine times higher than among white males, reaching epidemic proportions (Ozer et al., 1998). Suicide rates, however, are higher among white adolescents. In general, males are more likely than females to die from any type of injury (although females are more likely to attempt suicide, males are more likely to commit suicide). Among those 15–19 years old, males are about two times more likely to die of any unintentional injury and five times more likely to die of homicide or suicide than females (Ozer et al., 1998).
The major causes of adolescent morbidity are also behavioral, with differences in subgroups of adolescents who engage in particular risk-related behaviors, as shown in Table 1. The behaviors of most concern are tobacco, alcohol, and drug use; precocious and unprotected sexual behavior; unhealthful eating practices; sedentariness; violence; and deviant, risky behaviors. Although these are being reviewed separately, there is significant covariation among these health behaviors, making some adolescents at increased risk for a range of short-term and long-term health problems (Jessor and Jessor, 1977; U.S. DHHS, 1994; Lytle et al., 1995).
Drug Use
The gateway drugs—tobacco, alcohol, and marijuana—require particular attention during adolescence because they are initiated during this period; cause injury, illness, and death during adolescence and in adulthood; and are precursors to “heavier” drugs such as cocaine, hallucinogens, and heroin (U.S. DHHS, 1994). In addition, the majority of adolescents in the United States engages in each of these behaviors before they graduate from high school—74% have tried a cigarette, 84% have had an alcoholic drink, and 52% have used marijuana (CDC, 1998). Clearly, societal and personal decisions concerning tobacco, alcohol, and marijuana use are an integral part of examining adolescence in the United States, as the entire population can be considered “at risk.”
There are important differences in tobacco, alcohol, and marijuana use by ethnic or racial group and gender. These differences are particularly important to note as the United States continues to become increasingly multicultural (Vega and Gil, 1998). Overall, African American adolescents smoke, drink, and use illegal drugs at significantly lower rates than white and Hispanic adolescents
TABLE 1 Adolescent Health Risk Behaviors: Prevalence and Risk Status by Racial or Ethnic Group and Gender
|
Prevalence (%) |
Greatest Risk by Race or Ethnicitya |
By Genderb |
||||||
|
Behavior |
9th–12th Grades |
Whites |
Blacks |
Hispanics |
Asians |
American Indians |
Female |
Male |
|
Smoking (past month) |
36.4% |
X |
X |
X |
X |
|||
|
Alcohol use (past month) |
50.8% |
X |
X |
X |
X |
|||
|
Marijuana use (past month) |
26.2% |
X |
X |
X |
X |
|||
|
Sexual intercourse (ever) |
48.4% |
X |
X |
X |
X |
|||
|
Pregnant or made pregnant (ever) |
6.5% |
X |
X |
X |
||||
|
High fat intake (past day) |
37.7% |
X |
X |
|||||
|
Insufficient fruits and vegetables (past day) |
70.7% |
X |
||||||
|
Dieting (past month) |
39.7% |
X |
X |
X |
||||
|
Insufficient vigorous activity (3 times in past week) |
36.2% |
X |
X |
X |
||||
|
Fighting (past year) |
36.6% |
X |
X |
X |
X |
|||
|
Carried weapon (past month) |
18.3% |
X |
X |
|||||
|
Carried gun (past month) |
5.9% |
X |
X |
X |
||||
|
Riding with a drinking driver (past month) |
36.6% |
X |
||||||
|
Drove after drinking (past month) |
16.9% |
X |
* |
X |
X |
|||
|
aDoes not take into account subcategories of racial or ethnic groups or acculturation. Data are from the 1997 Youth Risk Behavior Surveillance System for white, black, and Hispanic high school students (CDC, 1998). Data for American Indians and Asians come from the Monitoring the Future Study and other non-nationally representative studies (U.S. DHHS, 1998) for drug use, sexual behavior, and fighting only. bMales were significantly more likely than females to report smokeless tobacco use and episodic heavy drinking, and to initiate sexual intercourse at a younger age. |
||||||||
CDC, 1998). White students are more likely to smoke cigarettes than Hispanic students (U.S. DHHS, 1998). National data from American Indian and Asian students have only recently become available from the Monitoring the Future study (Johnston et al., 1998; U.S. DHHS, 1998), and rates of tobacco, alcohol, and marijuana use among American Indians are consistently as high or higher than among white students, while Asian students' use was similar to African Americans and lower than other racial or ethnic groups (Beauvais, 1992; Gruber et al., 1996; Neumark-Sztainer et al., 1996; Epstein et al., 1998; U.S. DHHS, 1998; Chen et al., 1999).
Several authors make note, and this is relevant across all behaviors, that the classification of ethnic or racial groups masks significant differences within groups, such as differences between American Indian tribal groups and whether they live on or off reservation lands, and subcategories of Asians (Chinese, Japanese, Korean, etc.) and Hispanics (Gruber et al., 1996; Epstein et al., 1998; Bell et al., 1999). The classifications also do not account for levels of acculturation among recent immigrant groups and differences in drug use based on level of acculturation (Vega et al., 1993; Chen et al., 1999).
Gender differences in drug use among adolescents are also noted. Males are more likely than females to use smokeless tobacco, engage in episodic heavy drinking, and use marijuana (CDC, 1998), but females now are equally as likely as males to use other substances. Finally, rates of tobacco and marijuana use increased substantially in the 1990s, although that increase may now have leveled off; the increases occurred across all ethnic or racial and gender groups (Johnston et al., 1998).
Sexual Behavior
Sexual behavior also has its debut in adolescence, with two out of three adolescents reporting having had sexual intercourse prior to high school graduation (CDC, 1998). This sexual activity incurs the risk of pregnancy and infectious diseases, which have significant social, economic, and physical health ramifications (Ozer et al., 1998). Overall, males are more likely to initiate sexual activity earlier than females (Ozer et al., 1998; Upchurch et al., 1998). Black adolescents are more likely than Hispanics and whites to have initiated sexual intercourse, to have had more sexual partners, and to have had begun sexual activity at a younger age (Ozer et al., 1998). Asian adolescents appear to begin sexual activity later (Upchurch et al., 1998; Bell et al., 1999) and American Indian adolescents earlier, than do whites (Gruber et al., 1996; Neumark-Sztainer et al., 1996), but these were not nationally representative samples.
In contrast with drug use behavior, sexual behaviors have declined in prevalence since the early 1990s. This decline occurred after a steady two-decade increase in the percentage of adolescents engaging in sexual activity. The decline is associated with changes in related sexual behaviors. About 75% of teens report using contraceptives at first intercourse (up from 62% in 1988) and 54% report using condoms (Ozer et al., 1998). Condom use is more prevalent
among younger adolescents, while the use of birth control pills increases with age (Kann et al., 1996). Whites are more likely than blacks or Hispanics to use contraception at first intercourse (Ozer et al., 1998).
Similarly, rates of pregnancy also appear to be declining after dramatic increases since the 1970s. Still, 12% of all females ages 15–19 become pregnant each year—19% of black females, 13% of Hispanic females, and 8% of white females. Notably, of the 1 million adolescents who become pregnant each year, most (85%) report that their pregnancy was unintended (Ozer et al., 1998). More than half of these pregnancies result in births and more than a third result in abortion (Ozer et al., 1998). The birth and abortion rates among black and Hispanic adolescent females is about double that of white females. About 70% of these births occur out of wedlock. And, unfortunately, for the children of teenage mothers, there are also consequences—lower birth weight, lower cognitive and socioemotional functioning, and greater likelihood of death during the first year of life. These outcomes are linked to lower socioeconomic status, which is both a predictive factor for teenage pregnancy and an outcome of the limited opportunities and instability that are associated with being a teenage mother (Irwin and Shafer, 1992).
Sexual behavior may also result in sexually transmitted diseases, with adolescents at greater risk for these infectious diseases than any other age group (Irwin and Shafer, 1992). Chlamydia is most prevalent, affecting about 2% of female adolescents ages 15–19 (CDC, 1997). Gonorrhea and syphilis decreased in the 1990s; both of these infectious diseases are most prevalent among black adolescents (Ozer et al., 1998). Finally, although AIDS cases among adolescents are rare because of the 10-year incubation period, many adolescents become infected with HIV that will become manifest when they are in their 20s. Young adults, ages 20–29, comprise nearly one-fifth of the AIDS cases in the United States. Thus, teenage sexual behavior, while now appearing to decline, has increased dramatically in the past 25 years. The outcomes—teenage pregnancy, abortion, out-of-wedlock births, sexually transmitted diseases, and HIV—have significant implications for the future for these young people as well as for the next generation of young people in the United States.
Eating Behaviors and Physical Activity
In comparison with drug use, violence, and sexual behavior, eating and exercise may seem like relatively benign behavioral areas for adolescents. Yet eating behaviors significantly affect growth during adolescence (Story, 1992), are the second leading cause of cancer (World Cancer Research Fund, 1997), and track from adolescence to adulthood (Perry et al., 1997). Sedentary behavior contributes to obesity and chronic diseases, with activity patterns forming and tracking in childhood and adolescence (Kelder et al., 1994; U.S. DHHS, 1996; Troiano and Flegal, 1998).
The primary diet-related concerns among adolescents involve overconsumption of fat, overweight and obesity, unsafe weight-loss methods, eating
disorders, and insufficient intake of fruits, vegetables, and calcium. Most adolescents do not eat a diet that meets the U.S. Department of Agriculture's (1995) Guidelines for Americans (Perry et al., 1997). National data show that children and adolescents, more than any other age group, are more likely to exceed the recommendations for fat and saturated fat, with more than 90% of adolescent males consuming more than 30% of their calories from fat (Kennedy and Goldberg, 1995). Black adolescents are more likely than Hispanic and white adolescents to eat more servings of high-fat food per day (CDC, 1998).
On the other hand, adolescents are not eating sufficient fruits and vegetables—only 29% eat the recommended five servings per day. Males are more likely to eat five or more servings per day than females (32% vs. 26%). In addition, the low intake of calcium is of special concern to female adolescents. Females ages 12–19 consume only 68% of the recommended amount of calcium, making it unlikely that many adolescent females will reach their full biological potential for bone mass development and making it more likely they will experience osteoporosis later in life (Kennedy and Goldberg, 1995).
Obesity is now considered the most prevalent nutrition-related health problem of children and adolescents in the United States. (Dietz, 1998). The current generation of children and adolescents will grow up to be the most obese adults in American history (Hill and Trowbridge, 1998). Although many of the outcomes of being obese or overweight during adolescence are social, such as discrimination and more negative self-images, there is now evidence that being obese contributes to earlier physical maturation, increased blood lipid levels, and diabetes among adolescents (Dietz, 1998). The Third National Health and Nutrition Examination Survey (NHANES III) data indicate that about 11% of children and adolescents ages 6–17 are overweight, compared with a 5% expected prevalence (Troiano et al., 1995; Troiano and Flegal, 1998). In other words, the prevalence of overweight children and adolescents has doubled in the past 20 years. About one-quarter of children and adolescents are in the upper 85th percentile for weight, compared with the expected prevalence of 15%, placing them at risk for continued overweight and obesity into adulthood. Black and Hispanic females were more likely to be overweight than white females (Troiano and Flegal, 1998). However, females were not more likely to be overweight than males, except among African Americans (Troiano and Flegal, 1998). In the 1997 Youth Risk Behavior Survey, 27% of high school students reported they were overweight (CDC, 1998). Females were more likely to report being overweight than males; and Hispanic students were more likely than black students to report being overweight (CDC, 1998). Notably, perceptions of being overweight did not necessarily correspond with objective measures, particularly between the genders.
Correspondingly, about 40% of high school students report trying to lose weight in the past month—60% of females and 23% of males. Healthy weight loss behaviors (such as moderate exercise, decrease in snacks, decrease in fat intake) are more prevalent than unhealthy practices (such as fasting, diet pills, laxatives, vomiting; French et al., 1995). Still, nearly 5% of students reported taking laxatives or vomiting, and 5% had taken diet pills, to control weight in
the month prior to the survey (CDC, 1998); 30% of students dieted and 52% exercised to control their weight. Females were significantly more likely to use all forms of dieting methods than males. Hispanic and white students were more likely than black students to diet or exercise to lose weight; Hispanic students were more likely than white students to use laxatives or vomiting to control weight (CDC, 1998). In one study, American Indian females were more likely to engage in unhealthy weight loss practices than whites, while Asians were less likely (Neumark-Sztainer et al., 1996) Despite some evidence that African American females are heavier than Hispanic and white females, they are more likely to be satisfied with their weight and body image, and have a lower prevalence of eating disorders (Resnicow et al., 1997). The prevalence of eating disorders ranges from 1 to 5% among adolescent females and is associated with serious outcomes (Perry et al., 1997).
Physical activity significantly declines during adolescence for both males and females, despite the benefits of regular exercise for weight control, mental health, and the prevention of osteoporosis, cardiovascular diseases, and cancer (Kelder et al., 1995; U.S. DHHS, 1996; CDC, 1998; Kohl and Hobbs, 1998). Overall, 64% of high school students participate in vigorous physical activities on three or more days each week, with male students (72%) more likely to exercise than female students (54%), and white students (67%) more likely than Hispanic (60%) or black (54%) students to participate in vigorous physical activity (CDC, 1998). Still, 14% of young people reported no recent physical activity.
Violence and Other Risky Behaviors
Violent behavior by adolescents both on school property and in the community has been a topic of national discussion and debate for the past few years, prompted by several tragic school shootings. In fact, adolescents in the United States have relatively easy access to weapons and guns (Komro, 1999); overall, 18% of high school students reported having carried a weapon during the month prior to the survey and 6% reported having carried a gun (CDC, 1998). Males (28%) were more likely than females (7%) to have carried a weapon and a gun; black (9%) and Hispanic (10%) students were more likely than white (4%) students to have carried a gun (CDC, 1998). Nearly half of male students and one-fourth of female students had been in a physical fight during the year prior to the survey. Black, Hispanic, and Asian students were more likely than white students to have been in a physical fight on school property (Hill and Drolet, 1999). Reported physical fighting decreases as students get older (CDC, 1998). Still, among older males ages 18–21, about one-third reported carrying a gun in the month prior to the survey (Ozer et al., 1998).
Adolescents engage in other behaviors that put them at risk for unintentional injury, including driving after drinking, driving at high speeds, riding with a driver who has been drinking, and not using seat belts, motorcycle helmets, or bicycle helmets. Since motor vehicle collisions are the primary cause of death for adolescents, these behaviors are of considerable concern during
this period. For example, 37% of high school students reported having ridden in the past month with a driver who had been drinking; the percentage increased as students got older (CDC, 1998). Nearly 17% of students reported that they had driven a vehicle after drinking in the prior month; this was more likely for male students (21%), white (19%) and Hispanic (18%) students, and older students (CDC, 1998). Among students who rode motorcycles and bicycles, 36 and 88%, respectively, had never or rarely worn a helmet. And nearly 20% of students rarely or never use their seat belts when riding in a vehicle driven by someone else. All of these behaviors increase the risk of injury or death by motor vehicle collision.
This collection of health-related adolescent behaviors is not exhaustive. Other behaviors such as skin tanning, body piercing, prolonged listening to loud music, shoplifting, joining gangs, watching television, and playing video games, are engaged in by adolescents and may influence their short-term or long-term health. Still other behaviors, such as attending school and church, participating in extracurricular activities, helping at home, and doing volunteer work, are not usually considered “health related” yet may have a substantial influence on these behaviors. Other areas of adolescent health, such as the quality of health care for adolescents and adolescent mental health issues, are now beginning to be explored. National data on a range of other adolescent behaviors by gender and racial or ethnic subgroups, particularly with sufficient samples of Asian and American Indian adolescents, would be useful and important in order to provide a more complete picture of what adolescents are “doing.”
In fact, the types of behaviors “of concern” vary across time, place, and culture. Some of the behaviors are most problematic during adolescence and would be “normal” for adults, such as moderate alcohol use and sexual behavior. Other behaviors are problematic at any age, yet have their onset or have a higher prevalence during adolescence, such as tobacco and marijuana use, violence, and eating disorders. Still other behaviors, such as eating and activity patterns, truly reflect the society at large and are problematic because of their long-term health consequences. Still, the behaviors have meaning to young people and represent adolescents' response to what the society-at-large “teaches” them to become to fit into adult society. Thus, the focus in etiology is on the social environment, rather than the adolescents themselves, because it is within the social context that behavior change can take place and interventions appear to be most efficacious.
The Etiology of Health Behaviors in Adolescence
The reasons American adolescents engage in health-compromising behaviors have been the focus of several academic and popular books, as well as hundreds of journal articles, over the past several years (DiClemente et al., 1996; Schulenberg et al., 1997; Jessor, 1998; Brownlee, 1999; Hine, 1999; Vida, 1999). Factors that influence adolescent behavior have been examined within and between multiple domains, including genetic and biological factors, social and environmental factors, and personal factors (Flay and Petraitis, 1994; Pe-
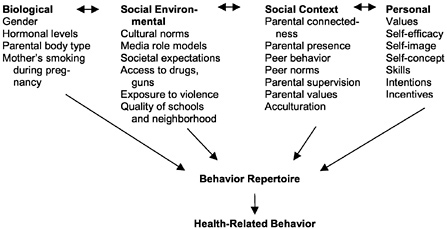
FIGURE 1. The etiology of adolescent health behavior: Examples of predictive factors. SOURCE: Adapted from Petraitis et al. (1995), Flay and Petraitis (1994), and Perry (1999b).
traitis et al., 1995; Jessor, 1998; Perry, 1999b), as shown in Figure 1. Recently, several researchers have begun to use the terms “risk” and “protective” factors within these domains to define those etiological factors that increase or decrease, respectively, the occurrence of health-compromising behavior (or, conversely, health-enhancing behavior; Catalano et al., 1999). Still, what is most important for subsequent intervention development is the identification of factors that are predictive of adolescent health-related behaviors, because those factors, whether they increase risk or are protective, explain why adolescents engage in particular behavior(s) and become the foundation for intervention design (Perry, 1999b). In particular, it is important to identify factors that are strongly predictive of subsequent behavior; that is, they account for a large proportion of the variance in health-related behavior (Baranowski et al., 1999). The factors also need to be amenable to intervention: they should be able to be promoted, changed, reduced, or eliminated through social, educational, political, and/or public health efforts.
A common thread in the recent etiological research, which parallels the trend in intervention development, is increased attention to the social environment and social context of adolescents. This has not been the exclusive focus of recent etiological research; some very interesting genetic and individual-level work has also been done (Kandel, 1998). Still, since adolescents are in a state of social transition, their social contexts acquire new and important meanings and influence. Adolescents are searching the social environment for clues on how to accomplish their developmental tasks, and peers, family members, other adults, and media all become “mentors” in the quest for development. How the environment “fits” the needs of adolescents becomes critical to successful development (Eccles et al., 1993). Thus, important concerns in analyzing adolescent health behavior are the type, frequency, and source of messages and opportunities that young people are exposed to, particularly as these relate to decisions
about becoming an adult in this society. Aspects of the social environment that have received new or renewed research attention in the past decade, and have important implications for intervention design, include the role of social capital, poverty, media and advertising, family relations, work, school, and peers in the health behaviors of young people.
Social Capital
One of the most important new perspectives on adolescent behavior is the notion of social capital (Coleman, 1988). Similar to financial capital (wealth) and human capital (skills and knowledge), which are quantifications of personal acquisitions (or access) associated with more successful development, social capital is “accrued” by the types of available relationships in a young person's community, neighborhood, school, or family (Coleman, 1988; Furstenberg and Hughes, 1995; Runyan et al., 1998). Important components of social capital are social structures that effectively promote positive social norms and appropriate role models, provide useful information, are trustworthy in meeting obligations, and have definite expectations (Coleman, 1988). Runyan and colleagues (1998) demonstrated that social capital, in particular church affiliation, the perception of personal social support, and neighborhood support, was strongly associated with children's well-being. Furstenberg and Hughes (1995) found, in a longitudinal study of higher-risk adolescents, that most measures of social capital during adolescence were predictive of success in young adulthood. Significant predictors included having support from one's mother, living with one's biological father, having parents ' help with homework, having a strong helping network in the community, frequently visiting with close friends, and the quality of the school (Furstenberg and Hughes, 1995). Social capital was also found to be a significant macrolevel predictor of firearm homicide rates at the state level (Kennedy et al., 1998), even when controlling for other factors. Thus, the social context and social environment, as measured by particular attributes within the family, neighborhood, school, and community, can facilitate healthy development of adolescents by providing greater opportunities, more stability, consistent norms, access to human capital, and social support.
As an example of the influence of social capital at the community level, we assessed social environmental factors related to young adolescents' alcohol use as part of a 20-community prevention trial, Project Northland (Perry et al., 1996). It was interesting to us that there was such a large amount of variability in alcohol use among eighth grade students among the 20 communities, since they appeared very homogeneous—small rural and mostly white communities in northeastern Minnesota. The prevalence of past-month alcohol use among eighth grade students, however, ranged from 16 to 43% in these communities. By creating scales with indicators of norms, role models, opportunities, and social support that were aggregated at the community level, we found that community-level norms and role models accounted for nearly 50% of the variance in eighth grade alcohol use rates (Roski et al., 1997). This guided our efforts during the
second phase of Project Northland: to create appropriate community norms concerning high schools students' alcohol use (Perry, Williams et al., 2000).
Poverty
Social capital may be able to mediate some of the effects that poverty and the lack of financial resources have on young people's health (Kennedy et al., 1998). But the effects of poverty are still far-reaching in our society. In 1998, children made up 39% of the poor but only 26% of the total population. The poverty rate for children (18.9% in 1998) is higher than for any other age group, although lower than its recent peak of 22.7% in 1993. In 1998, 13.5 million children were poor. Black and Hispanic households were twice as likely to live in poverty than were white households (U.S. Census Bureau, 1999), although socioeconomic status does not explain all racial or ethnic group differences in health status (Lillie-Blanton and Laveist, 1996).
Poverty exerts its influence as an environmental and social factor in many aspects of young people's health behavior. Poor, urban youth are exposed to high rates of community violence that influence subsequent aggressive and violent behaviors and depression (Farrell and Bruce, 1997; Gorman-Smith and Tolan, 1998). Young people who are poor are less likely to finish school and are more likely to experience conduct problems and conflicts with peers (Lerner and Galambos, 1998). Young people living in poverty are more likely to experience hunger, fewer food options, and less fresh produce (Crockett and Sims, 1995), undermining their nutritional health. Thus, adolescents who live in poverty often live in poor communities, where exposure to drugs and violence is high and where access to healthful resources also may be limited. Thus, the elimination of poverty for children and adolescents must be an important goal for those involved in improving the health of young people. Secondarily, efforts should be directed toward alleviating those influences within poor communities that exacerbate health problems for young people, such as by providing more-than-adequate educational opportunities, restricting access to weapons, and offering supervised afterschool and weekend activities, free and reduced-fat meals at schools, and mentoring programs.
Media and Advertising
Among young people of all socioeconomic strata, the increase in exposure to electronic communications has been a notable characteristic of the past decade, and its effects on adolescent behavior are beginning to be documented. Media that have been studied include television, radio, movies, and music videos. Less is known about the effects of video games and Internet exposure. One problem in assessing the impact of media has been that it is both distal and all pervasive —very few young people are not exposed, so there are often inade-
quate samples of “controls.” Thus, studies have examined levels or types of media use and may underestimate the total effect of media on behavior.
The most widely evaluated relationship is between various forms of media and subsequent or concurrent aggressive or violent behavior, although media has been shown to be associated with a range of health-risk behaviors (Wood et al., 1991; Klein et al., 1993; Strasburger, 1997; Willis and Strasburger, 1998). On average, adolescents watch about 3–6 hours of television and listen to the radio about 6 hours each day (Klein et al., 1993; Strasburger, 1997). Strasburger (1997) notes that during an average year, an adolescent is exposed to “10,000 acts of violence, 15,000 sexual innuendoes, jokes, and behaviors, and 20,000 commercials, including 1,000–2,000 beer and wine advertisements ” on television (p. 404). For example, 22.4% of music television videos (MTVs) and 20.4% of rap videos portrayed violence (DuRant et al., 1997). And the result of these portrayals is clear: the greater the exposure to media violence, the more likely is subsequent aggressive behavior among adolescents (Committee on Communications, 1995; Strasburger, 1997; Strasburger, 1998; Willis and Strasburger, 1998).
There is increasing evidence of the effects of advertising on young people's behavior (U.S. DHHS, 1994; Committee on Communications, 1995; Perry, 1999a). In the last decade, substantial research has focused on the relationship between cigarette advertising or promotional activities and smoking by young people, which became very important in the tobacco litigations in states around the country (Perry, 1999a): 86% of adolescents smoke the most advertised brands of cigarettes —Marlboro, Camel, and Newport—while they are smoked by only 32% of adults (CDC, 1994). Adolescents, much more than adults, respond to new advertising campaigns, such as the introduction of women's brands in the late 1960s (Pierce et al., 1994) and Joe Camel in the early 1990s (CDC, 1994). The themes of advertising correspond with the tasks of adolescence, displaying images of independence, peer approval, and sexuality (U.S. DHHS, 1994). It is not a coincidence that the cigarette brands smoked by adolescents are significantly more likely to be in magazines with relatively high youth readership (King et al., 1998). Youth have high exposure to cigarette advertising and the greater the exposure, the more likely that the adolescent is a smoker (Schooler et al., 1996). One study found that adolescents were three times more sensitive to cigarette advertising than adults and, that a 10% increase in advertising dollars resulted in a 3% increase in market share among adults and a 9.5% increase among adolescents (Pollay et al., 1996). Finally, Pierce and colleagues (1998) found that when nonsmoking, not-susceptible adolescents had a favorite cigarette advertisement or said they would be willing to use a promotional item, they were two to three times more likely to progress to smoking 3 years later, accounting for 34% of the reason that adolescents began to smoke. Perhaps the relationship between the tobacco industry and adolescents is best summarized by an R.J.Reynolds researcher who wrote: “Realistically, if our company is to survive and prosper, over the long term, we must get our share of the youth market” (Teague, 1973).
The influence of media and advertising on adolescent behavior warrants further research, especially as the forms of electronic media change rapidly and as young people continue to be the targets of advertising. The recent removal of cigarette billboards is one example of an intervention to reduce exposure to health-compromising media messages. Similarly strong action might be warranted with violent portrayals on television (Strasburger, 1997). Children and adolescents might also benefit by learning media literacy skills to identify, analyze, investigate, and refute what is being portrayed in media and advertising (Kubey and Baker, 1999).
Family Relationships
The families of the twenty-first century bear little resemblance to those 100 years ago. It is now normative for adolescents to have experienced the separation or divorce of their parents, to have both parents working outside the home, to prepare meals for themselves, and to have several hours of unsupervised time after school (Fuchs and Reklis, 1992; Crockett and Sims, 1995). These changes, among others, provide considerable new challenges for healthy development among adolescents.
The National Longitudinal Study on Adolescent Health (Resnick et al., 1997) provides important quantification of the ways families influence adolescent behavior. Adolescents were found to be less at risk for emotional distress, violence, and drug use if they perceived themselves as connected to their parents: that is, they experienced feelings of warmth, love, and caring from their parents. This was more important than the actual presence of parents during key times of the day, although that was a significant factor as well. Parents having high expectations for their adolescents concerning school attainment was also associated with healthier and less risky behavior. On the other hand, adolescents in homes with easy access to tobacco, alcohol, drugs, and guns were more likely to be involved in violence and drug use themselves (Resnick et al., 1997).
The notion of “family capital” was developed by assessing parents' human, social, and education capital (Marjoribanks, 1998). Family capital included parents' own educational attainment, parent-child activities and homework time together, parents' aspirations for their children in terms of education and work, and parents' values on independence and learning. Family capital was found to have a moderate to large association with adolescents' academic performance and aspirations for the future (Marjoribanks, 1998).
Several researchers have examined the changes in family relationships in the context of adolescent development and developmental tasks. Associated with the task of striving for autonomy, parent-adolescent conflict has received considerable attention, although most empirical examinations show little evidence of increased conflict after early adolescence, even though there may be more emotional intensity in the conflict from early to middle adolescence (Laursen et al., 1998). When conflict exists, it is primarily concerning mundane issues such as cleaning one's room or curfew, which may be attempts by adolescents to de-
fine themselves or make their own decisions (Eccles et al., 1993). Adolescents express a desire for more participation in the decisions made in the family, and when allowed to participate more fully, there were positive results in school motivation and self-esteem (Eccles et al., 1993). Likewise, adolescents who received support from their parents to be more autonomous were less likely to initiate sexual intercourse; those who were more emotionally attached to their parents were less likely to engage in fighting and drug use (Turner et al., 1993). Finally, adolescents who perceived that their parents knew their friends, where they went at night, how they spent their money, what they did with their free time, and where they were most afternoons, were less likely to begin to use drugs (Steinberg et al., 1994).
Fostering competence and positive connections between adolescents and their parents seems critical to promoting healthy development (Resnick et al., 1997; Masten and Coatsworth, 1998). These connections may include involvement in activities together, having clear expectations about school performance, allowing greater decision making for the adolescent within the family, and communicating about how, where, and with whom the adolescent is spending time. As available time becomes an issue, these connections may need to be provided by the larger community of caring adults.
Schools, Work, and Peers
Adolescents usually progress from the relatively protected and connected environment of the elementary school to the more impersonal middle or junior high school and then to the larger high school in their communities. During this time, they also begin to work for income, and most have some formal paid work experience by the end of high school (Mortimer and Johnson, 1998). In both of these environments, same-age peers are found, and relationships are formed that carry increasing influence on adolescents' behavior. Thus, understanding how to create school and work environments that foster positive behavior among adolescents is an important area of research (Dryfoos, 1994; 1998).
Eccles and colleagues (1993) argue that the transition to middle or junior high school and the new school environment do not “fit” the developmental needs of young adolescents. They point out that in contrast to the young adolescent's need for greater participation in decision making, junior high classrooms have increased emphasis on teacher control and discipline, and fewer opportunities for decision making than did elementary school classrooms. The junior high classrooms also were less personal and had more negative teacher-student relationships; they tended to teach whole-class tasks rather than small groups; the teachers felt less effective and taught at a lower cognitive level yet they judged students' competence at a higher standard, compared with elementary schools. Thus, the junior high environment is likely, by its structure, to adversely impact the motivation and connectedness that young adolescents have for school (Eccles et al., 1993). Simmons and Blyth (1987) found a greater drop in grades
among those who made the transition to a junior high school than among those who remained in a K–8 school.
Connectedness to school is critical since it is the major formal socializing institution in the United States. In the National Longitudinal Study on Adolescent Health, connectedness to school was a primary protective factor for adolescents for a variety of risk-related behaviors (Resnick et al., 1997). School can serve as a major protective factor because adolescents who are involved with school spend much of their time and attention on schoolwork and extracurricular activities, plus associate with peers who are also involved with school, and thus have fewer opportunities to engage in other health-compromising behaviors (Steinberg and Avenevoli, 1998). Disengagement from school may also lead to more intensive involvement in the workplace (Steinberg and Avenevoli, 1998), with its own implications for health behaviors. The development of a positive, caring school setting has been shown to be associated with a more positive school climate, better student behavior, and higher overall academic achievement (Haynes and Comer, 1990).
Although most adolescents work part-time during high school, Steinberg et al. (1993) found that those who worked more than 20 hours a week were more likely to become disengaged from school, engaged in delinquency and drug use and more disengaged from parents and to have decreased self-reliance. Most of these effects remained even after they stopped working. However, Mortimer and Johnson (1998) point out that work experiences during high school are a preparation for later work involvement and can be seen as a transition between school and work, with the formation of important attitudes and orientation about work. Employed adolescents learn new skills in their jobs, their income increases in the years following high school, and the experiences expand the adolescents' repertoire to manage the demands of home, school, work, and others (Mortimer and Johnson, 1998). For adolescents working less than 20 hours a week, grades and school dropout rates were improved by their involvement with a job. In their thoughtful review of long-term outcomes of working by adolescents, Mortimer and Johnson (1998) conclude that working is associated with drinking during high school (for both males and females) and smoking during high school and later (for females), but with very few other negative outcomes and with positive outcomes related to later employment.
In the context of school, work, and community, peer relationships are formed and assume an important if not central role in adolescents ' social world. Peer relationships that are positive are associated with achievement, job competence, and higher sense of self-worth (Masten et al., 1995). Peer rejection is associated with aggressive behaviors and maladjustment (Masten and Coatsworth, 1998). In adolescence, peers can exert influences that can be positive rather than negative, such as encouraging academic achievement or participation in extra-curricular activities (Komro et al., 1994). Peers may also encourage deviant or risky behaviors; adolescents who begin to associate with drug-using peers, for example, increase their drug use to match their peers (Steinberg et al., 1994).
Thus, the inclusion of the peer group as a part of health behavior interventions may be crucial for their success (Perry et al., 1989; Komro et al., 1996).
This brief review of some recent work in the etiology of adolescent health behaviors has focused on the social environment and social context of adolescents because of the great amount of research that is taking place in this area and because changes in the social environment are generally possible through intervention and may be critical for behavior changes of adolescents (Perry, 1999b). On one hand, the review indicates the need to “capitalize” —to improve the social, family, financial, and access-to-human capital for adolescents. However, although etiological research is the basis of intervention, intervention research demonstrates what is possible and how change can be achieved. Thus, larger changes need to be balanced by the reality of what can be accomplished in each domain of an adolescent's life and concerning which behaviors. The past two decades have provided considerable insight into these questions.
MAJOR INTERVENTION POINTS: CHANGING THE SOCIAL ENVIRONMENT
Intervention research has made considerable progress in the last quarter century. In 1975, for example, there were no school-based smoking prevention programs that had demonstrated reductions in smoking onset among adolescents (U.S. DHHS, 1994; Perry, 1999b). By 1994, meta-analyses had been written involving hundreds of studies and identifying which components of smoking prevention programs were associated with greater effectiveness in reducing onset and prevalence rates (U.S. DHHS, 1994). The expansion in prevention and intervention research involved the consistent use of theory to guide program development, process evaluation and measures of mediating variables to determine which components were most critical, and increasingly sophisticated research designs and methodologies to examine the effects of these programs. Prevention and intervention research is now considered a scientific inquiry that is independent from etiology, health education, community psychology, or social psychology, yet builds on the findings from these disciplines (and others). While epidemiological, biological, and etiological research on adolescence has a rich history and serves as a foundation for intervention programs, intervention research is concerned with trying to define, measure, and analyze changes in behavior, with its own unique set of methodological challenges (Eddy et al., 1998).
This section reviews examples of prevention-intervention research on how changes in the social environment or social context of adolescents were made. These recent intervention experiences provide models for how more general adolescent health behavior change might be approached, even when the intervention addresses only a particular behavior. Some intervention approaches may be relevant for improving a range of adolescent behaviors, and these include strategies such as changing community educational policies, improving the school environment, providing after school activities, or increasing the general social or
life skills of adolescents (Botvin et al., 1995; Dryfoos, 1998). Other interventions need to be behavior specific, such as reducing access to tobacco or alcohol, providing opportunities for physical activity, or increasing the choices of foods that are served at school. What is notable about recent adolescent health behavior intervention research is that the interventions tend to be multicomponent, with changes in several social contexts; multiyear, theory driven; and evaluated using sophisticated research designs and analysis methodologies. Thus, intervention research is where the answer to, How? can truly be addressed.
Increasing Social Capital—The Seattle Social Development Project
The question of when to begin to intervene to reduce health-compromising behaviors in adolescence has not been thoroughly investigated, even though developmental research suggests continuity from childhood for several domains of concern (Masten et al., 1995). Hawkins and colleagues (1999) reported the effects at age 18 of a multicomponent, multiyear intervention with 18 urban public elementary schools, which took place when the targeted cohort was in the first through sixth grades. The intervention consisted of (1) annual in-service training with teachers on proactive classroom management, interactive teaching, and cooperative learning; (2) social competence training for students when they were in first and sixth grades; and (3) parent training classes when students were in first through third and fifth through sixth grades to provide skills to promote academic achievement of their children and reduce their risk of drug use. These interventions were intended to increase the social bonds that children had to school and their families.
At age 18, students exposed to the entire intervention reported less involvement in violence, sexual intercourse, and heavy drinking, and greater commitment to school and better academic achievement (Hawkins et al., 1999). Students exposed to the intervention only in fifth and sixth grades did not demonstrate these long-term outcomes, suggesting that an intervention embedded in the entire elementary school experience can have significant and lasting effects on adolescent behavior. However, the intervention had the greatest effects on school-related and sexual behaviors. There were no effects on criminal behavior, smoking, alcohol use, marijuana use, or other drug use (except heavy drinking). This suggests that the social development approach might serve as a preliminary and even necessary step in promoting health among adolescents by creating an appropriate, positive, and consistent orientation toward schooling and achievement prior to and during adolescence (Catalano et al., 1999). But additional interventions appear to be needed to delay or prevent the onset of tobacco, alcohol, and other drug use.
Marketing Health—Prosocial Media, Counterads, and the Truth Campaign
The significant influence of media and marketing on adolescent consumer behavior suggests that these approaches might be used to improve health behavior as well. Flynn and colleagues (1992) demonstrated long-term reductions in smoking onset with adolescents when television and radio messages supplemented a school-based program. It is interesting that although the school and media programs shared similar themes, they were developed independently, so they were perceived by the students to be messages from multiple sources and reinforced the notion that smoking was not normative (U.S. DHHS, 1994).
Dorfman and Wallack (1993) point out that advertising strategies for health promotion include a range of strategies from person- to policy-oriented media, with public service announcements generally aimed at individual behavior change and counterads aimed at larger environmental or policy changes. The latter often suggest political action and are more likely to generate controversy. Ads that specifically targeted the tobacco industry executives, and questioned the marketing of a deadly product, were designed in California to change the perception that smoking is normative and acceptable, and to turn the public 's attention to the tobacco industry, rather than smokers, as the cause of problems related to tobacco (Dorfman and Wallack, 1993). Targeting industry manipulation was also suggested by youth as being one of the most effective strategies for making smoking less normative (Goldman and Glantz, 1998).
This approach was taken one step further in Florida in an effort to reduce teen smoking. Using funds from its settlement with the tobacco industry, the “Truth” campaign was developed by Florida's teens during the Governor's Teen Tobacco Summit in March 1998. This was part of the larger Florida Tobacco Pilot Program, which had as one of its main goals to empower youth to lead community involvement against tobacco (Holtz, 1999). The advertising campaign focused on the tobacco industry, with teens demanding more honesty from the industry, including tobacco distributors, retailers, advertising agencies, and media associated with the industry. The Truth campaign included print and broadcast ads, a teen grassroots movement against tobacco use, school curricula, enforcement of retail sales restrictions, and the creation of a web site (www.wholetruth.com; Florida Department of Health, 1999). The ads used quotes or situations with tobacco executives and others to create rebellion among youth against the tobacco industry. For example, one ad portrayed an Academy Awards-like event “in downtown Hades” where an award was to be given for the most deaths in a single year (News America Digital Publishing, 1999). Suicide, illicit drugs, tobacco, and murder were contestants, and known mass killers such as Adolf Hitler were in the audience. Tobacco wins the award, and it is accepted by a clean-cut tobacco executive, who exclaims, “I want to thank all you smokers out there. This one is for you.”
The Truth campaign resulted in significant declines in smoking among middle, junior high, and high school students from February 1998 to February
1999—a larger decrease than has been documented with any of the other large statewide campaigns and in sharp contrast to the level or increasing rates of smoking among adolescents nationwide (Clary, 1999; News America Digital Publishing, 1999). The combination of hard-hitting media—which some have argued is of questionable taste—extensive youth involvement, higher cigarette prices, and enforcement of youth access laws may all have contributed to the success of the campaign. Unfortunately, funding for the campaign was significantly reduced during its second year by the Florida legislature (Clary, 1999). Still, the campaign results suggest that media and advertising that is designed to attract the attention of youth, and uses some of the same methods as commercial advertising may have a significant impact on adolescent behavior.
Changing Community Norms—The Tobacco Policy Options Program
Obtaining community involvement and changing community norms are critical to providing a social environment that supports the healthy development of adolescents (Hansen and Graham, 1991; Glanz et al., 1995; Perry et al., 2000). The short-term effects of school-based programs, for example, may be the result of behavior change that is inconsistent with the larger community norms, so that healthy behavior is not supported and reinforced after the program is completed. Longer-term effects for smoking prevention have generally involved changes in the larger community (Flynn et al., 1992; Perry et al., 1992; U.S. DHHS, 1994). However, a more systematic approach to community organizing around adolescent health has emerged in the past few years.
In the Tobacco Policy Options Program, 14 communities were randomly assigned to receive the intervention or to serve as a control (Forster et al., 1998). The goal of the intervention program was to reduce teenage access to tobacco, from stores and vending machines, by using a direct action community organizing model (Blaine et al., 1997). Community organizers were hired in each of the seven intervention communities and trained in organizing methods. These included doing extensive interviews (“one-on-ones”) with community citizens representing a variety of sectors such as business, education, religion, government, service, and so forth. Each organizer conducted one-on-ones until there were no more nominations from those interviewed; this resulted in hundreds of interviews. Then, an “action team” was organized of people, with a personal commitment to do something about teenage smoking, who represented a variety of community sectors; the teams also had youth representatives. These action teams created action plans that involved policy changes at the community level concerning how to deal with commercial access to tobacco. The resulting actions included purchase attempts by adolescents to demonstrate ease in access, local media, presentations at meetings, and ordinance changes in all of the intervention communities over a period of 2–3 years. The intervention resulted in significant reductions in youth smoking over the period of the project and suggests the power of community normative change, since actual access to tobacco
was not changed by the intervention (Forster et al., 1998). Direct action community organizing has been adapted for use in other interventions involving alcohol use and nutrition policies, as well as social access to tobacco (Perry et al., 2000; Wagenaar et al., 2000).
Connecting with Parents—The Adolescent Transitions Program
While parenting practices have repeatedly been identified as key etiological factors in adolescent health behavior development, effective interventions have only recently been forthcoming that are applicable to most or all parents. Parents are difficult to reach, since their involvement is voluntary and participation rates in organized activities tend to be low (Perry, 1999b). Still, when the topic is one that many parents are concerned about, such as drug use, or if their adolescent is involved in the presentation, or if young people bring activities home to complete with their parents, higher participation rates and more positive outcomes have been achieved (Williams and Perry, 1998).
The Adolescent Transitions Program (ATP) was a multicomponent program for parents of high-risk young adolescents (Andrews et al., 1995; Dishion and Andrews, 1995). ATP included a parent program that targeted family management practices and communication skills, and a teen program that targeted self-management and prosocial behavior. The parent program involved 12 weekly 90-minute sessions that were conducted by trained therapists and assisted by parents who had taken part in the program. Three additional sessions took place individually with each family. The parent program had a structured curriculum that focuses on skills related to monitoring their adolescent, positive reinforcement, limit setting, and problem solving, based on Patterson 's (1982) research. The teen program provided skill development in self-monitoring and tracking, prosocial goal setting, developing positive peer environments, problem solving, and communications with peers and parents. The results of the parent program showed considerable promise—parent-child conflict was reduced as well as problem behaviors in school (Andrews et al., 1995). However, the teen program had long-term untoward effects of increasing tobacco use and problem behaviors, probably due to the closer associations among high-risk adolescents that the groups provided (Dishion and Andrews, 1995; Eddy et al., 1998).
Promoting Positive Peer Involvement—Project Northland
Project Northland was a randomized community trial to reduce the onset and prevalence of alcohol use among young adolescents in 24 school districts and surrounding communities (Perry et al., 1993). The three-year intervention program consisted of classroom-based curricula in sixth through eighth grades, parental education and involvement activities, peer leadership opportunities, and community-wide task force activities. Each year had a specific theme that corresponded to the developmental stage of the students, and brought together the
four components of the intervention. In the first year, the focus was on parental involvement and parent-child communication (the Slick Tracy Program); the second-year focus was on peer influence and alternative activities (Amazing Alternatives!); the third-year focus was on community influence and involvement (PowerLines). At the end of eighth grade, students in the intervention communities had significantly reduced their alcohol use. Baseline nondrinkers, about two-thirds of the sample, additionally reported significant reductions in cigarette smoking and marijuana use (Perry et al., 1996).
Recent mediation analyses show that the important mediators of Project Northland's effect on alcohol use were changes in peer norms, peer influences to use alcohol, functional meanings of alcohol use, and risk-related attitudes and behaviors. Project Northland appears to have been most effective in changing the peer groups to be more prosocial and less supportive of alcohol use (Komro et al., in press).
Peer leadership permeated the Project Northland intervention, with increasing opportunities for involvement from young people over the course of the three years. In the sixth grade, the Slick Tracy Program was facilitated by the students both in the classrooms and at home. The students created and presented their projects at Slick Tracy Night, so the evening revolved around their ideas (Williams et al., 1995). In the seventh grade, elected students in each classroom were trained to conduct the eight-session classroom program. Having peers teach the Amazing Alternatives! curriculum had previously been shown to be critical to its success (Perry et al., 1989). Student volunteers also participated in teams that designed, developed, and implemented extracurricular social activities for their peers (Komro et al., 1994). The involvement of students in planning activities was shown to significantly reduce their alcohol use (Komro et al., 1996). In the eighth grade, students again acted as group leaders in the classroom and continued planning social activities. They also participated in producing a play in each of the communities and performed the play for other students, their parents, and community members (Perry et al., 1996). The active involvement of sixth through eighth grade students, then, was central to the design and implementation of Project Northland; the results demonstrate that such involvement can affect peer norms and behaviors, as well as associated problem behaviors, which is consistent with a recent meta-analysis of prevention programs (Black et al., 1998). Thus, in changing the social context for adolescents, we need to consider their roles and leadership in their own educational and social endeavors.
More comprehensive reviews of recent interventions around each of the adolescent health behaviors have been undertaken by the Centers for Disease Control and Prevention and others (Drug Strategies, 1996, 1998; Catalano et al., 1999; Perry, 1999b; U.S. DHHS, 1999; Komro and Stigler, in press). In addition, the science of intervention development has evolved considerably, so that there are now available resources to guide program design that is based on research, theory, and creativity (Cullen et al., 1998; Perry, 1999b). These five examples of interventions are a sampling of the types of recent research that seems
particularly promising—interventions that significantly change the social context of adolescents to be supportive of their development and reduce their opportunities for health risk behaviors.
New Opportunities for Research and Intervention
Despite the successes noted above, there still exists a dire need for more large-scale intervention research to demonstrate that healthful behavior among adolescents can be achieved. There is much more that we know about the etiology of adolescent behavior than what we have been able to translate into effective intervention strategies. Thus, one opportunity that exists is to fund well-designed, large-scale, longitudinal intervention research that includes careful delineation and assessment of process, mediating, and outcome variables. This can lead to intervention research that serves three purposes: (1) the research can demonstrate whether or not a particular strategy or set of strategies is effective in changing targeted behaviors; (2) it can demonstrate how the changes were achieved, through mediation analyses; and (3) it can chart the course of development of the behaviors with and without intervention, so that etiological research becomes embedded in intervention. Intervention research, across the range of behaviors and social contexts of adolescents, should be given high priority to more quickly and efficiently move ahead the knowledge of how to achieve changes in the health and social behaviors of adolescents.
This review has revealed a significant mismatch in our society between the social contexts in which adolescents often find themselves and what they need to develop healthfully. Overall, adolescents need greater opportunities to learn social, emotional, and educational skills; more support and collaboration with adults; fewer hours spent unsupervised, alone, or in a place where they must be sedentary; less access to harmful substances, weapons, and images; and more access to positive, active, and healthful role models. This may require a national-level commitment to, and policies for, healthy youth development, so that schools have the resources to stay open and provide opportunities in the evenings and weekends; so that communities can provide safe transportation for adolescents if they do stay after school; so that all parents have the opportunity to learn how best to deal with their adolescents; so that youth have the mentors and opportunities to take increasing leadership roles in their communities; so that access for adolescents to drugs and weapons is eliminated; so that the national media are required to consider the violence of the messages they send; and so that schools or other groups who want to implement successful targeted programs have the financial resources to do so. Despite all the research on the “capital” of youth, it seems that not enough actual capital has been spent on increasing the social, educational, human, and family capital of adolescents in the United States.
Given the backdrop of greater attention to youth development, beginning early in children's lives and extending through adolescence, with strong federal and state support, there are specific areas of intervention research that are im-
portant to continue to guide this process. First, there needs to be more research on interventions with varied cultural and ethnic groups, and by gender, specifically concerning behaviors where they are at greater risk. This has already been forthcoming from various funding agencies, but needs to be underscored, given the high rates of some risk behaviors in these groups. Second, there needs to be research on timing of interventions. For example, long-term outcomes were observed for an eating pattern intervention that was implemented with third through fifth graders, but such outcomes have not been observed with drug use interventions (Nader et al., 1999). There may be targeted programs that will be most efficacious at particular times in a young person's life. Third, the types of competencies, skills, or opportunities for adolescents that might influence their behavior need to be more fully explored and expanded and included in intervention research, and might include self-management, communication, academic planning, character building, community organizing, and even spiritual skills. For example, in Project Northland, students ' self-evaluation of their own wisdom (including harmony and warmth, intelligence, and spirituality scales) was significantly predictive of their alcohol, tobacco, and marijuana use and their violence at 12th grade (Jason et al., in press). These new areas may be alternative avenues or skills for adolescents, with multiple potential outcomes. Fourth, we must have greater knowledge of the needed competencies for schools, neighborhoods, families, clinics, and communities that work with and serve adolescents, and importantly, how these competencies can be taught, promoted, or disseminated. This is particularly critical for communities with varied ethnic or racial groups or with recent immigrants. Fifth, dissemination research should be supported, since outcomes found in controlled trials often cannot be replicated when more broadly implemented (DiClemente and Wingood, 1998; Perry, 1999b). Finally, policy research, where changing public policy is the goal, should be encouraged, to learn about the process and outcomes of policy changes that affect adolescents. It is clear that we need much more than competent adolescents—we need to create and provide a social environment for them that is competent and compassionate as well.
The American experiment has had some side effects in the latter part of the twentieth century. While countries such as India, China, Japan, and Singapore have relatively few problems with their adolescents, the United States continues to have significant and, in some cases, growing problems among its youth. While turning the clock back a century, or adopting social policies from Asia, are not feasible solutions to these concerns, it might be useful to examine social contexts in which the overwhelming majority of youth are healthful, productive, and content. How many hours do they spend in school? Do they spend significant time unsupervised? Are they involved in food preparation? Are there safe places to walk or bicycle to be with friends? Is academic achievement rewarded throughout the community? And so forth. This might lead to broader societal changes, alternative solutions, or creative options that may have salutary effects on adolescents and their health behaviors in the twenty-first century.
REFERENCES
Andrews, D.W., Soberman, L.H., and Dishion, T.J. ( 1995). The Adolescent Transitions Program for high-risk teens and their parents: Toward a school-based intervention. Education and Treatment of Children, 18, 478–498.
Arnett, J. ( 1992). Reckless behavior in adolescence: A developmental perspective. Developmental Review, 12, 339–373.
Arnett, J.J. ( 1999). Adolescent storm and stress, reconsidered. American Psychologist, 54(5), 317–326.
Baranowski, T., Cullen, K.W., and Baranowski, J. ( 1999). Psychosocial correlates of dietary intake: Advancing dietary intervention. . Annual Review of Nutrition, 19, 17–40.
Beauvais, F. ( 1992). Trends in Indian adolescent drug and alcohol use. Journal of the National Center for American Indian and Alaskan Native Mental Health Resources, 5, 1–12.
Bell, D.L., Ragin, D.F., and Cohall, A. ( 1999). Cross-cultural issues in prevention, health promotion, and risk reduction in adolescence. Adolescent Medicine: State of the Art Reviews, 10(1), 57–69.
Black, D.R., Tobler, N.S., and Sciacca, J.P. ( 1998). Peer helping/involvement: An efficacious way to meet the challenge of reducing alcohol, tobacco, and other drug use among youth? Journal of School Health, 68(3), 87–93.
Blaine, T.M., Forster, J.L., Hennrikus, D., O'Neil, S., Wolfson, M., and Pham, H. ( 1997). Creating tobacco policy control at the local level: Implementation of a direct action organizing approach. Health Education and Behavior, 24, 640–651.
Blum, R. ( 1998). Adolescent health: Priorities for the next millennium. Maternal and Child Health Journal, 22, 368–375.
Blum, R.W., and Stark T. ( 1985). Cognitive development in adolescence. Seminars in Adolescent Medicine, 1(1), 25–32.
Borvin, G.J., Baker, E., Dusenbury, L., Borvin, E.M., and Diaz, T. ( 1995). Long-term follow-up results of a randomized drug abuse prevention trial in a white middle-class population. Journal of the American Medical Association, 273, 1106–1112.
Bronfenbrenner, U., and Morris, P.A.( 1998). The ecology of developmental processes. In W.Damon and R.M.Lerner (Eds.), Handbook on Child Psychology: Vol.1. Theoretical Models of Human Development (5th ed., pp. 993–1028). New York: John Wiley and Sons,.
Brooks-Gunn, J. ( 1988). Commentary: Developmental issues in the transition to early adolescence . In M.R.Gunnar and W.A.Collins (Eds.), Minnesota Symposia on Child Psychology: Vol. 21. Development During the Transition to Adolescence (pp. 189–208). Hillsdale, NJ: Lawrence Erlbaum Associates.
Brooks-Gunn, J., and Warren, M.P. ( 1989). Biological and social contributions to negative affect in young adolescent girls. Child Development, 60, 40–55.
Brooks-Gunn, J., Graber, J.A., and Paikoff, R.L. ( 1994). Studying links between hormones and negative affect: Models and measures . Journal of Research on Adolescence, 4(4), 469–486.
Brownlee, S. ( 1999). Inside the teenage brain. U.S. News and World Report, 45–54.
Buchanan, C.M., Eccles, J.S., and Becker, J.B. ( 1992). Are adolescents the victims of raging hormones: Evidence for activational effects of hormones on moods and behavior at adolescence. Psychological Bulletin, 111(1), 62–107.
Catalano, R.F., Berglund, ML., Ryan, J.A.M., Lonczak, H.S., and Hawkins, J.D. ( 1999). Positive Youth Development in the United States: Research Findings on Evaluations of Positive Youth Development Programs. Washington, DC: U.S. DHHS, NICHHD.
Centers for Disease Control and Prevention (CDC). ( 1993). Mortality trends, causes of death, and related risk behaviors among U.S. adolescents. Adolescent Health: State of the Nation Monograph Series #1 (CDC Pub No 099–4112). Atlanta: CDC.
Centers for Disease Control and Prevention (CDC). ( 1994). Changes in cigarette brand preferences of adolescent smokers—United States, 1989–1993. Morbidity and Mortality Weekly Report, 43(32), 577–581.
Centers for Disease Control and Prevention (CDC). ( 1997). Sexually Transmitted Disease Surveillance 1996. Atlanta: CDC.
Centers for Disease Control and Prevention (CDC). ( 1998). Youth risk behavior surveillance—United States, 1997. Morbidity and Mortality Weekly Report, 47, SS-3.
Chen, X., Unger, J.B., Cruz, T.B., and Johnson, C.A. ( 1999). Smoking patterns of Asian-American youth in California and their relationship with acculturation. Journal of Adolescent Health, 24, 321–328.
Clary, M. ( 1999). Lawmakers try to get apparently successful anti-smoking campaign. Los Angeles Times, A14.
Clausen, J.A. ( 1975). The social meaning of differential physical and sexual maturation . In S.E.Dragastin and G.H.Elder (Eds.), Adolescence in the Lifecycle (pp. 25–47). New York: Halsted.
Coleman, J.S. ( 1988). Social capital in the creation of human capital. American Journal of Sociology, 94, S95–S120.
Committee on Communications. ( 1995). Children, adolescents, and advertising. Pediatrics, 95(2), 295–297.
Crockett, L.J., and Petersen, A.C. ( 1993). Adolescent development: Health risks and opportunities for health promotion. In S.G.Millstein, A.C.Petersen, and E.O. Nightingale (Eds.), Promoting the Health of Adolescents (pp. 13–37). New York: Oxford University Press.
Crockett, S.J., and Sims, L.S. ( 1995). Environmental influences on children's eating. Journal of Nutrition Education, 27(5), 235–249.
Cullen, K.W., Bartholomew, L.K., Parcel, G.S., and Kok, G. ( 1998). Intervention mapping: Use of theory and data in the development of a fruit and vegetable nutrition program for Girl Scouts. Journal of Nutrition Education, 30, 188–195.
Dietz, W.H. ( 1998). Health consequences of obesity in youth: Childhood predictors of adult disease. Pediatrics, 101, 518–525.
DiClemente, R.J., Hansen,W.B., and Ponton, L.E. ( 1996). Handbook of Adolescent Health Risk Behavior. New York: Plenum Press.
DiClemente, R.J., and Wingood, G.M. ( 1998). Monetary incentives: A useful strategy for enhancing enrollment and promoting participation in HIV/STD risk reduction interventions. Sexually Transmitted Infections, 74, 239–242.
Dishion, T.J., and Andrews, D.W. ( 1995). Preventing escalation in problem behaviors with high-risk young adolescents: Immediate and 1-year outcomes. Journal of Consulting and Clinical Psychology, 63, 538–548.
Dorfman, L., and Wallack, L. ( 1993). Advertising health: The case for counter-ads. Public Health Reports, 108(6), 716–726.
Drug Strategies ( 1996). Making the grade: A guide to school drug prevention programs. Washington, DC, Drug Strategies.
Drug Strategies ( 1998). Safe schools, safe students: A guide to violence prevention strategies . Washington, DC: Drug Strategies.
Dryfoos, J.G. ( 1994). Full-Service Schools. San Francisco: Jossey-Bass.
Dryfoos, J.G. ( 1998). Safe Passage: Making It Through Adolescence in a Risky Society. New York: Oxford University Press.
DuRant, R.H., Rich. M., Emans, S.J., Rome, E.S., Allred, E., and Woods, E.R. ( 1997). Violence and weapon carrying in music videos. Archives of Pediatrics and Adolescent Medicine, 151, 443–448.
Eccles, J.S., Midgley, C., Wigfield, A.Buchanan, C.M., Reuman, D., Flanagan, C., and Iver, D.M. ( 1993). Development during adolescence: The impact of stage-environment fit on young adolescents' experiences in schools and in families. American Psychologist, 48(2), 90–101.
Eddy, J.M. Dishion, T.J., and Stoolmiller, M. ( 1998). The analysis of intervention change in children and families: Methodological and conceptual issues embedded in intervention studies. Journal of Abnormal Child Psychology, 26(1), 53–69.
Elder, G.H. ( 1974). Children of the Great Depression. Chicago: University of Chicago Press.
Elkind, D. ( 1967). Egocentrism in adolescence. Child Development, 38, 1025–1034.
Epstein, J.A., Botvin, G.J., Baker, E., and Diaz, T. ( 1998). Patterns of alcohol use amongethnically diverse black and Hispanic urban youth. Journal of Gender, Culture, and Health, 3(1), 29–39.
Epstein, J.A., Botvin, G.J., and Diaz, T. ( 1998). Ethnic and gender differences in alcohol use among a longitudinal sample of inner-city adolescents. Journal of Gender, Culture, and Health, 3(4), 193–207.
Farrell, A.D., and Bruce, S.E. ( 1997). Impact of exposure to community violence on violent behavior and emotional distress among urban adolescents. Journal of Clinical Child Psychology, 26(1), 2–14.
Flavell, J.H. ( 1985). Cognitive Development (2nd ed). Englewood Cliffs, NJ: Prentice-Hall.
Flay, B.R., and Petraitis, J. ( 1994). The theory of triadic influence: A new theory of health behavior with implications for preventive interventions. Advances in Medical Sociology, 4, 19–44.
Florida Department of Health. ( 1999). Tobacco Prevention and Control: Resources for a Comprehensive Plan for Florida. Florida Leadership Council for Tobacco Control. Tallahassee, FL: Florida Department of Health.
Flynn, B.S., Worden, J.K., Seeker-Walker, R.H., Badger, F.J., Geller, B.M., and Costanza, M.C. ( 1992). Prevention of cigarette smoking through mass media intervention and school programs. American Journal of Public Health, 82(6), 827–834.
Forster, J.L., Wolfson, M., Murray, D.M., Blaine, T.M., Wagenaar, A.C., and Hennrikus, D.J. ( 1998). The effects of community policies to reduce youth access to tobacco . American Journal of Public Health, 1193–1196.
French, S.A., Perry, C.L., Leon, G.R., and Fulkerson, J.A. ( 1995). Dieting behaviors and weight change history in adolescent females . Health Psychology, 14(6), 548–555.
Fuchs, V., and Reklis, D. ( 1992). The status of American children. Science, 255, 41–46.
Furstenberg, F.F., and Hughes, M.E. ( 1995). Social capital and successful development among at-risk youth. Journal of Marriage and Family, 57, 580–592.
Glanz, K., Lankenau, B., Foerster, S., Temple, S., Mullis, R., and Schmid, T. ( 1995). Environmental and policy approaches to cardiovascular disease prevention through nutrition: Opportunities for state and local action. Health Education Quarterly, 22(4), 512–527.
Goldman, L.K., and Glantz, S.A. ( 1998). Evaluation of antismoking advertising campaigns. Journal of the American Medical Association, 279 (10), 772–777.
German-Smith, D., and Tolan, P. ( 1998). The role of exposure to community violence and developmental problems among inner-city youth. Development and Psychopathology, 10, 101–116.
Gruber, E., DiClemente, R.J., and Anderson, M.M. ( 1996). Risk-taking behavior among Native American adolescents in Minnesota public schools: Comparisons with black and white adolescents. Ethnicity and Health, 1(3), 261–267.
Hall, G.S. ( 1904). Adolescence: Its Psychology and Its Relation to Physiology, Anthro pology, Sociology, Sex, Crime, Religion, and Education (Vols. I and II). Englewood Cliffs, NJ: Prentice-Hall.
Hamburg, B. ( 1986). Subsets of adolescent mothers: Developmental, biomedical, and psychosocial issues. In J.B.Lancaster and B.A.Hamburg (Eds.). School-Age Pregnancy and Parenthood: Biosocial Dimensions (pp. 115–145). New York: Aldine de Gruyter.
Hansen, W.B., and Graham, J.W. ( 1991). Preventing alcohol, marijuana, and cigarette use among adolescents: Peer pressure resistance training versus establishing conservative norms. Preventive Medicine, 20, 414–430.
Havighurst, R.J. ( 1972). Developmental Tasks and Education (3rd ed.). New York: David McKay.
Hawkins, J.D., Catalano, R.F., Kosterman, R., Abbott, R., and Hill, K.G. ( 1999). Preventing adolescent health-risk behaviors by strengthening protection during childhood. Archives of Pediatrics and Adolescent Medicine, 153, 226–234.
Haynes, N.M., and Comer, J.P. ( 1990). The effects of a school development program on self-concept. Yale Journal of Biology and Medicine, 63, 275–283.
Herman-Giddens, M.E., Slora, E.J., and Wasserman, R.C. ( 1997). Secondary sexual characteristics and menses in young girls seen in office practice: A study from the pediatric research in office settings network. Pediatrics, 99, 505–512.
Hill, J.O., and Trowbridge, F.L. ( 1998). Childhood obesity: Future directions and research priorities. Pediatrics, 101, 570–574.
Hill, J.P. ( 1980). Understanding Early Adolescence: A Framework. Center for Early Adolescence. Durham, NC: Wordworks.
Hill, J.P., and Holmbeck, G.N. ( 1986). Attachment and autonomy during adolescence. Annals of Child Development, 3, 145–189.
Hill, S.C., and Drolet, J.C. ( 1999). School-related violence among high school students in the United States, 1993–1995. Journal of School Health, 69(7), 264–272.
Hine, T. ( 1999). The Rise and Fall of the American Teenager. New York: Avon Books.
Holtz, A. ( 1999). Turning the rebellion: How Florida is trying to incite teens against tobacco. Holtz Report [on line]. Available: nasw.org/users/holtza/FL_paper.htm; accessed 11/12/99.
Hopwood, NJ.Kelch, R.P., Hale, P.M., Mendes, T.M., Foster, C.M., and Beitins, I.Z. ( 1990). The onset of human puberty: Biological and environmental factors. In J. Bancroft, J.M.Reinisch (Eds.), Adolescence and Puberty (pp. 29–49). New York: Oxford University Press.
Irwin, C.E., and Shafer, M.A. ( 1992). Adolescent sexuality: Negative outcomes of a normative behavior. In D.E.Rogers and E.Ginzbert (Eds.), Adolescents at Risk: Medical and Social Perspectives (pp. 35–79). Boulder, CO: Westview Press.
Jason, L.A., Reichler, A., King, C., Madsen, D., Camacho, J., and Marchese, W. (in press). The measurement of wisdom: A preliminary effort. Journal of Community Psychology.
Jessor, R. ( 1993). Successful adolescent development among youth in high-risk settings . American Psychologist, 48(2), 117–126.
Jessor, R. ( 1998). New Perspectives on Adolescent Risk Behavior. Cambridge, UK: Cambridge University Press.
Jessor, R., and Jessor, S.L. ( 1977). Problem Behavior and Psychosocial Development: A Longitudinal Study of Youth. New York: Academic Press.
Johnston, L.D., O'Malley, P.M., and Bachman, J.G. ( 1998). Drug Use by American Young People [on line]. Available: www.isr.umich.edu/src/mtf; accessed 11/10/99.
Kandel, D.B. ( 1998). Persistent themes and new perspectives on adolescent substance use: A lifespan perspective. In R.Jessor (Ed.), New Perspectives on Adolescent Risk Behavior (pp. 43–89). Cambridge, UK, Cambridge University Pres.
Kann, L., Warren, C.W., Harris, W.A., Collins, J.L., Douglas, K., Collins, B., Williams,B., and Kolbe, L.J. ( 1996). Youth Risk Surveillance, 1995. Division of Adolescent and School Health. Atlanta: CDC.
Kaplowitz, P.B., and Oberfield, S.E. ( 1999). Reexamination of the age limit for defining when puberty is precocious in girls in the United States: Implications for evaluation and treatment . Pediatrics, 104(4), 936–941.
Kelder, S.H., Perry, C.L., Klepp, K-I., and Lytle, L.A. ( 1994). Longitudinal tracking of adolescent smoking, physical activity, and food choice behaviors. American Journal of Public Health, 84, 1121–1126.
Kelder, S.H., Perry, C.L., Peters, R.J., Lytle, L.A., and Klepp, K-I. ( 1995). Gender differences in the Class of 1989 Study: The school component of the Minnesota Heart Health Program. Journal of Health Education, 26(2), S36–S44.
Kennedy, B.P., Kawachi, I., Prothrow-Stith, D., Lochner, K., and Gupta, V. ( 1998). Social capital, income inequality, and firearm violent crime. Social Science and Medicine, 47(1), 7–17.
Kennedy, E., and Goldberg, J. ( 1995). What are American children eating? Implications for public policy . Nutrition Reviews, 53, 111–126.
King, C., Siegel, M., Celebucki, C., and Connolly, G.N. ( 1998). Adolescent exposure to cigarette advertising in magazines. Journal of the American Medical Association, 279(7), 516–520.
Klein, J.D., Brown, J.D., Childers, K.W., Oliveri, J., Porter, C., and Dykers, C. ( 1993). Adolescents' risky behavior and mass media use. Pediatrics, 92(1), 24–31.
Kohl, H.W., and Hobbs, K.E. ( 1998). Development of physical activity behaviors among children and adolescents . Pediatrics, 101, 549–554.
Komro, K.A. ( 1999). Adolescents' access to firearms: Epidemiology and prevention. Journal of Health Education, 30(5), 290–296.
Komro, K.A. and Stigler, M.H. (In press). A Community Road Map to Healthy Youth Development: Vehicles for Success. University of Minnesota, Konopka Institute for Best Practices in Adolescent Health.
Komro, K.A., Perry, C.L., Murray, D.M., Veblen-Mortenson, S., Williams, C.L., and Anstine, P.S. ( 1996). Peer planned social activities for the prevention of alcohol use among young adolescents. Journal of School Health, 66(9), 328–336.
Komro, K.A., Perry, C.L., Veblen-Mortenson, S., and Williams, C.L. ( 1994). Peer participation in Project Northland: A community-wide alcohol use prevention project. Journal of School Health, 64(8), 318–322.
Komro, K.A., Perry, C.L., Williams, C.L., Stigler, M.H., Farbakhsh, K., and Veblen-Mortenson, S. (In press). How did Project Northland reduce alcohol use among young adolescents? Analysis of mediating variables. Health Education Research.
Kubey, R., and Baker, F. ( 1999). Has media literacy found a curricular foothold? Education Week [on line]. Available: www.edweek.org/ew/ewstory.cfm?slug=09ubey2.h19; accessed 11/11/99.
Laursen, B., Coy, K.C., and Collins, W.A. ( 1998). Reconsidering changes in parent-child conflict across adolescence: A meta-analysis. Child Development, 69(3), 817–832.
Lerner, R.M., and Galambos, N.L. ( 1998). Adolescent development: Challenges and opportunities for research, programs, and policies. Annual Review of Psychology, 49, 413–446.
Lillie-Blanton, M., and Laveist, T. ( 1996). Race/ethnicity, the social environment, and health. Social Science and Medicine, 43(1), 83–91.
Lytle, L.A., Kelder, S.H., Perry, C.L., and Klepp K-I. ( 1995). Covariance of adolescent health behaviors: The Class of 1989 Study . Health Education Research, 10, 133– 146.
Marjoribanks, K. ( 1998). Family capital, children's individual attributes, and adolescents' aspirations: A follow-up analysis. Journal of Psychology, 132(3), 328–336.
Marshall, W.A., and Tanner, J. ( 1970). Variations in the pattern of pubertal changes in boys. Archives of Diseases in Childhood, 45, 13–23.
Masten, A.S., and Coatsworth, J.D. ( 1995). Competence, resilience, and psychopathology. In D.Cicchetti and D.Cohen (Eds.), Developmental Psychopathology: Vol 2. Risk, Disorder, and Adaptation (pp. 715–752). New York: John Wiley and Sons.
Masten, A.S., and Coatsworth, J.D. ( 1998). The development of competence in favorable and unfavorable environments: Lessons from research on successful children. American Psychologist, 53(2), 205–220,.
Masten, A.S., Coatsworth, J.D., Neemann, J., Gest, S.D., Tellegen, A., and Garmezy, N. ( 1995). The structure and coherence of competence from childhood through adolescence. Child Development, 66, 1635–1659.
Moffitt, T.E. ( 1993). Adolescence-limited and life-course-persistent antisocial behavior: A developmental taxonomy. Psychological Review, 100(4), 674–701.
Money, J. ( 1980). Love and Love Sickness: The Science of Sex, Gender Difference, and Pair-Bonding. Baltimore: Johns Hopkins University Press.
Mortimer, J.T., and Johnson, M.K. ( 1998). New perspectives on adolescent work and the transition to adulthood . In R.Jessor (Ed.), New Perspectives on Adolescent Risk Behavior (pp. 425–496). Cambridge, UK: Cambridge University Press.
Nader, P.R., Stone, E.J., Lytle, L.A., Perry, C.L., Osganian, S.K., Kelder, S., Webber, L.S., Elder, J.P., Montgomery, D., Feldman, H.A., Wu, M., Johnson, C., Parcel, G.S., and Luepker, R.V. ( 1999). Three-year maintenance of improved diet and physical activity: The CATCH cohort. Archives of Pediatrics and Adolescent Medicine, 153, 695–704.
Neumark-Sztainer, D., Story, M., French, S., Cassuto, N., Jacobs, D.R., and Resnick, M.D. ( 1996). Patterns of health-compromising behaviors among Minnesota adolescents: Sociodemographic variations. American Journal of Public Health, 86(11), 1599–1606.
News America Digital Publishing. ( 1999). CDC: Anti-smoking campaign in Florida shows solid results. Fox Market Wire [on line]. Available: www.foxwire.com; accessed 11/4/99.
Nottelmann, E.D., Inoff-Germain, G., Susman, E.J., and Chrousos, G.P. ( 1990). Hormones and behavior at puberty. In J.Bancroft and J.M.Reinisch (Eds.), Adolescence and Puberty (pp. 88–123). New York: Oxford University Press.
Olweus, D., Mattsson, A., Schalling, D., and Low, H. ( 1998). Circulating testosterone levels and aggression in adolescent males: A causal analysis. Psychosomatic Medicine, 50, 261–272.
Ozer, E.M., Brindis, C.D., Millstein, S.G., Knopf, D.K., and Irwin, C.E. ( 1998). America's Adolescents: Are They Healthy? San Francisco: National Adolescent Health Information Center, University of California, San Francisco.
Patterson, G.R. ( 1982). Coercive Family Process. Eugene, OR: Castalia.
Perry, C.L. ( 1999a). The tobacco industry and underage youth smoking: Tobacco industry documents from the Minnesota litigation. Archives of Pediatrics and Adolescent Medicine, 153, 935–941.
Perry, C.L. ( 1999b). Creating Health Behavior Change: How to Develop Communitywide Programs for Youth. Thousand Oaks, CA: Sage.
Perry, C.L., Grant, M., Ernberg, G., Florenzano, R.U., Langdon, M.D., Blaze-Temple, D., Cross, D., Jacobs, D.R., Myeni, A.D., Waahlberg, R.B., Berg, S., Andersson, D., Fisher, K.J., Saunders, B., and Schmid, T. ( 1989). WHO collaborative study on alcohol education and young people: Outcomes of a four-country pilot study. International Journal of Addictions, 24(12), 1145–1171.
Perry, C.L., Kelder, S.H., Murray, D.M., and Klepp K-I. ( 1992). Community-widesmoking prevention: Long-term outcomes of the Minnesota Heart Health Program and the Class of 1989 Study. American Journal of Public Health, 82(9), 1210–1216.
Perry, C.L., Story, M., and Lytle, L.A. ( 1997). Promoting healthy dietary behaviors. In R.P.Weissberg, T.P.Gullotta, G.R.Adams, R.L.Hampton, and B.A.Ryan (Eds). Healthy Children 2010: Enhancing Children's Wellness, Volume 8: Issues in Children's and Families' Lives. Thousand Oaks, CA: Sage.
Perry, C.L., Williams, C.L., Forster, J.L., Wolfson, M., Wagenaar, A.C., Finnegan, J.R., McGovern, P.G., Veblen-Mortenson, S., Komro, K.A., and Anstine, P.S. ( 1993). Background, conceptualization, and design of a communitywide research program on adolescent alcohol use: Project Northland. Health Education Research: Theory and Practice, 8(1), 125–136.
Perry, C.L., Williams, C.L., Komro, K.A., Veblen-Mortenson, S., Forster, J., Bernstein-Lachter, R., Pratt, L.K., Dudovitz, B., Munson, K.A., Farbakhsh, K., Finnegan, J., and McGovern, P. ( 2000). Project Northland high school interventions: Community action to reduce adolescent alcohol use. Health Education and Behavior. 27(1), 29–49.
Perry, C.L., Williams, C.L., Veblen-Mortenson, S., Toomey, T., Komro, K.A., Anstine, P.S., McGovern, P.G., Finnegan, J.R., Forster, J.L., Wagenaar, A.C., and Wolfson, M. ( 1996). Project Northland: Outcomes of a community-wide alcohol use prevention program during early adolescence. American Journal of Public Health, 86(7), 956–965.
Petersen, A.C., and Taylor, B. ( 1980). The biological approach to adolescence: Biological change and psychological adaptation. In J.Adelson (Ed.), Handbook of Adolescent Psychology (pp. 117–155). New York: John Wiley and Sons.
Petraitis, J., Flay, B.R., and Miller, T.Q. ( 1995). Reviewing theories of adolescent substance use: Organizing pieces of the puzzle. Psychological Bulletin, 117(1), 67–86.
Pierce, J.P., Lee, L., and Gilpin, F.A. ( 1994). Smoking initiation by adolescent girls; An association with targeted advertising. Journal of the American Medical Association, 271(8), 608–611.
Pierce, J.P., Choi, W.S., Gilpin, E.A., Farkas, A.J., and Berry, C.C. ( 1998). Tobacco industry promotion of cigarettes and adolescent smoking. Journal of the American Medical Association, 279 (7), 511–515.
Pollay, R.L., Siddarth, S., Siegel, M., Haddix, A., Merritt, R.K., Giovino, G.A., and Eriksen, M.P. ( 1996). The last straw? Cigarette advertising and realized market shares among youths and adults. Journal of Marketing, 60, 1–16.
Resnick, M.D., Bearman, P.S., Blum, R.W., Bauman, K.E., Harris, K.M., Jones, J., Tabor, J., Beuhring, T., Sieving, R.E., Shew, M., Ireland, M., Bearinger, L.H., and Udry, J.R. ( 1997). Protecting adolescents from harm: Findings from the National Longitudinal Study on Adolescent Health. Journal of the American Medical Association, 278(10), 823–832.
Resnicow, K., Braithwaite, R.L, and Kuo, J.A. ( 1997). Interpersonal interventions for minority adolescents. In D.K.Wilson, J.R.Rodrigue, and W.C.Taylor (Eds.), Health-Promoting and Health-Compromising Behaviors Among Minority Adolescents (pp. 201–228). Washington, DC: American Psychological Association.
Roski, J., Perry, C.L., McGovern, P.G., Williams, C.L., Farbakhsh, K., and Veblen-Mortenson, S. ( 1997). School and community influences on adolescent alcohol and drug use . Health Education Research: Theory and Practice, 12(2), 255–266.
Runyan, D.K., Hunter, W.M., Socolar, R.R.S., Amaya-Jackson, L., English, D., Landsverk, J., Dubowitz, H., Browne, D.H., Bangdiwala, S.L., and Mathew, R.M. ( 1998). Children who prosper in unfavorable environments: The relationship to social capital. Pediatrics, 101(1), 12–18.
Scheer, S.D., Unger, D.G., and Brown, M.B. ( 1996). Adolescents becoming adults: Attributes for adulthood. Adolescence, 31(121), 127–131.
Schooler, C., Feighery, E., and Flora, J.A. ( 1996). Seventh graders' self-reported exposure to cigarette marketing and its relationship to their smoking behavior. American Journal of Public Health, 86(9), 1216–1221.
Schulenberg, J.Maggs, J., and Hurrelmann, K. ( 1997). Health Risks and Developmental Transitions During Adolescence. Cambridge, UK: Cambridge University Press.
Silbereisen, R.K. and Kracke, B. ( 1993). Variation in maturational timing and adjustment in adolescence. In S.Jackson and H.Rodriguez-Tome (Eds.), Adolescence and Its Social Worlds (pp. 67–94). East Sussex, UK: Erlbaum.
Silbereisen, R.K., Petersen, A.C., Albrecht, H.T., and Kracke, B. ( 1989). Maturational timing and the development of problem behavior: Longitudinal studies in adolescence. Journal of Early Adolescence, 9, 247–268.
Simmons, R.G., and Blyth, D.A. ( 1987). Moving into Adolescence: The Impact of Pubertal Change and School Context. Hawthorne, NY: Aldine de Gruyter.
Steinberg, L.D. ( 1989). Pubertal maturation and parent-adolescent distance: An evolutionary perspective. In G.R.Adams, R.Montemayor and T.P.Gulotta (Eds.), Biology of Adolescent Behavior and Development (pp. 71–97). Newbury Park, CA: Sage.
Steinberg, L., and Avenevoli, S. ( 1998). Disengagement from school and problem behavior in adolescence: A developmental-contextual analysis of the influences of family and part-time work. In R.Jessor (Ed.), New Perspectives on Adolescent Risk Behavior (pp. 392–424). Cambridge, UK: Cambridge University Press.
Steinberg, L., Fegley, S., and Dornbusch, S.M. ( 1993). Negative impact of part-time work on adolescent adjustment: Evidence from a longitudinal study. Developmental Psychology, 29(2), 171–180.
Steinberg, L., Fletcher, A., and Darling, N. ( 1994). Parental monitoring and peer influences on adolescent substance use . Pediatrics, 93(6), 1060–1064.
Story, M. ( 1992). Nutritional requirements during adolescence. In E.R.McAnarney, R.E. Kreipe, D.P.Orr, and G.D.Comerci (Eds.), Textbook of Adolescent Medicine (pp. 75–84). Philadelphia: W.B.Saunders.
Strasburger, V.C. ( 1997). “Sex, drugs, rock ‘n' roll” and the media—Are the media responsible for adolescent behavior? Adolescent Medicine: State of the Art Reviews, 8(3), 403–414.
Strasburger, V.C. ( 1998). Is it only rock ‘n' roll? The chicken-and-the-egg dilemma. Journal of Adolescent Health, 23(1), 1–2.
Surbey, M.K. ( 1990). Family composition, stress, and the timing of human menarche. In T.E.Ziegler and F.B.Bercovitch (Eds.), Socioendocrinology of Primate Reproduction (pp. 11–32). New York: John Wiley and Sons.
Susman, E.J. ( 1997). Modeling developmental complexity in adolescence: Hormones and behavior in context. Journal of Research on Adolescence, 7(3), 283–306.
Tanner, J.M. ( 1978). Fetus into Man: Physical Growth from Conception to Maturity. Cambridge, MA: Harvard University Press.
Teague, C.E. ( 1973). Some Thoughts About New Brands of Cigarettes for the Youth Market, RJ Reynolds' research planning memorandum. RJR Bates # 50298 7357. Minnesota documents depository.
Troiano, R.P., and Flegal, K.M. ( 1998). Overweight children and adolescents: Description, epidemiology, and demographics. Pediatrics, 101(3), 497–504.
Troiano, R.P., Flegal, K.M., Kuczmarski, R.J., Campbell, S.M., and Johnson, C.L. ( 1995). Overweight prevalence and trends for children and adolescents. Archives of Pediatrics and Adolescent Medicine, 149, 1085–1091.
Turner, R.A., Irwin, C.E., Tschann, J.M., and Millstein, S.G. ( 1993). Autonomy, relatedness, and the initiation of health risk behaviors in early adolescence. Health Psychology, 12(3), 200–208.
Udry, J.R. ( 1988). Biological dispositions and social control in adolescent sexual behavior . American Sociological Review, 53, 709–722.
Upchurch, D.M., Levy-Storm, L., Sucoff, C.A., and Aneshensel, C.S. ( 1998). Gender and ethnic differences in the timing of first sexual intercourse . Family Planning Perspectives, 30(3), 121–127.
U.S. Census Bureau. Press briefing on 1998 income and poverty estimates. ( 1999) [on line]. Available: www.census.gov/hhes/income/income98/prs99acs.html; accessed 11/11/99.
U.S. Department of Agriculture ( 1995). Dietary Guidelines for Americans. Washington, DC: U.S. Department of Health and Human Services.
U.S. Department of Health and Human Services ( 1994). Preventing Tobacco Use Among Young People: A Report of the Surgeon General. Atlanta: CDC.
U.S. Department of Health and Human Services ( 1996). Physical Activity and Health: A Report of the Surgeon General. Atlanta: CDC.
U.S. Department of Health and Human Services ( 1998). Tobacco Use Among U.S. Racial/Ethnic Minority Groups: A Report of the Surgeon General. Atlanta: CDC.
U.S. Department of Health and Human Services ( 1999). Understanding Substance AbusePrevention: Toward the 21st Century: A Primer on Effective Programs . DHHS Pub No 99–3301. Washington, DC: CSAP.
Vega, W.A. and Gil, A.G. ( 1998). Drug Use and Ethnicity in Early Adolescence. New York, Plenum Press.
Vega, W.A, Gil, A.G., and Zimmerman, R.S. ( 1993). Patterns of drug use among Cuban Americans, African Americans, and white non-Hispanic boys. American Journal of Public Health, 83, 257–259.
Vida, V. ( 1999). Girls on the Verge. New York: St. Martin's Press.
Wagenaar, A.C. Murray, D.M., Gehan, G.P., Wolfson, M., Forster, J.L., Toomey, T.L., Perry, C.L., and Jones-Webb, R. ( 2000). Communities mobilizing for change on alcohol: Outcomes from a randomized community trial. Journal of Studies on Alcohol, 61, 85–94.
Williams, C.L., and Perry, C.L. ( 1998). Design and implementation of parent programs for a community-wide adolescent alcohol use prevention program. Journal of Prevention and Intervention in the Community, 17, 65–80.
Williams, C.L., Perry, C.L., Dudovitz, B., Veblen-Mortenson, S., Anstine, P.S., Komro, K.A., and Toomey, T. ( 1995). A home-based prevention program for sixth grade alcohol use: Results from Project Northland. Journal of Primary Prevention, 16(2), 125–147.
Willis, E., and Strasburger VC. ( 1998). Media violence. Pediatric Clinics of North America, 45(2), 319–331.
Wood, W., Wong, F.Y., and Chachere J.G. ( 1991). Effects of mass media on viewers' aggression in unconstrained social interaction. Psychological Bulletin, 109(3), 371–383.
World Cancer Research Fund. ( 1997). Food, Nutrition and the Prevention of Cancer: A Global Perspective. Washington, DC: American Institute for Cancer Research.
Wyshak, G., and Frisch, R.E. ( 1982). Evidence for a secular trend in age of menarche. New England Journal of Medicine, 306, 1033–1035.





































