
SLIDE 3
SLIDE 3 NOTES: The longitudinal data base currently spans an 11-year history of claims for a sample of Medicare beneficiaries.
The sample is updated in every month, with the addition of a sample of only newly eligible beneficiaries and the deletion of those who die.
The particular subsample on which this analysis is based is for people who were continuously enrolled in fee-for-service (i.e., traditional) Medicare. About 10–15 percent of Medicare beneficiaries enrolled in Medicare managed care plans in any year, and we have no claims data for that group.
Claims data in this dataset are grouped by month. Therefore, we can only know whether an individual had at least one service of a particular type (e.g., sigmoidoscopy) but cannot determine the exact date(s) on which such a service occurred.
SLIDE 4
SLIDE NOTES 4: To address the first question: What happens to patients in the years following a polypectomy with respect to receipt of a colonoscopy? The sample consisted of individuals present in 1994 and later years. Each individual was followed until death, disenrollment from fee-for-service Medicare; or the end of the study period (1999).
Of that group, any individual who had undergone a polypectomy, either by sigmoidoscopy or full colonoscopy was identified.
I then identified the month of the first colonoscopy that occurred at least 6 months following the polypectomy. Colonoscopies performed within 6 months of the index polypectomy could have been follow-up procedures related to the polypectomy. We were interested in long-term surveillance procedures.
Finally, we tested the effect on the analysis of eliminating any individual with any kind of cancer diagnosis. Because we were dealing with claims data, we had to rely on a record of an ICD-9 cancer diagnosis in any claim over the beneficiary’s claim history. We defined as “potential cancer beneficiaries” any individuals who had a cancer diagnosis in at least two different months in the period.
SLIDE 5
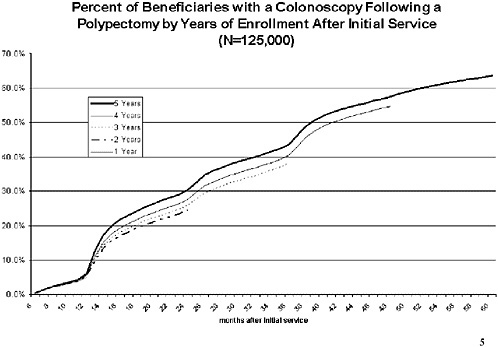
SLIDE 5 NOTES: This chart describes the percent of beneficiaries who received their first post-polypectomy colonoscopy in or before the month shown on the x-axis. Because the sample included individuals with different follow-up periods, we provide separate estimates for individuals at least 1 (but not 2) years of follow-up; at least 2 years of followup; and so on, until the maximum of 5 years of followup.
There are modest differences in the cumulative frequency curves for each of the groups. Those with shorter follow-up periods tended to have slightly lower rates of colonoscopy than those with longer periods.
In examining data among various demographic subgroups, I noticed some interesting trends among some smaller subgroups. However, the number of individuals sampled in those groups was too small to draw any significant conclusions. The probability of follow up among patients by race, sex, age and income may be worth closer examination with larger databases.
SLIDE 6
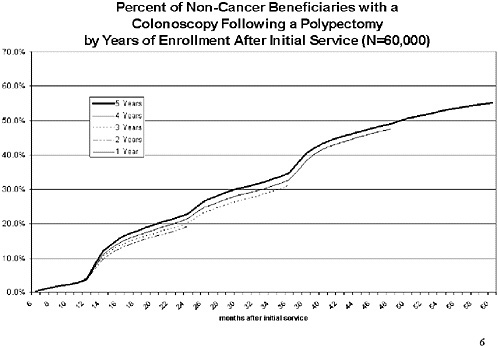
SLIDE 6 NOTES: This chart shows the same results as the previous group, except that this is the sample that excludes possible cancer beneficiaries. The pattern is similar as for the larger group, but this group is somewhat less likely to have a subsequent colonoscopy. For those with 5 years of data available, 55 percent had had at least one colonoscopy in the period between 6 months and 5 years following the index polypectomy.
SLIDE 7
SLIDE 7 NOTES: The results shown up to this point have several important limitations. Because the database is exclusively Medicare claims for payment, it is impossible to differentiate among types of polyps removed, or sizes. We also cannot differentiate between polypectomies that arose out of a screening examination and those that occurred for diagnostic reasons. Nor can we differentiate between subsequent colonoscopies done for surveillance purposes and those done for diagnostic purposes.
SLIDE 8
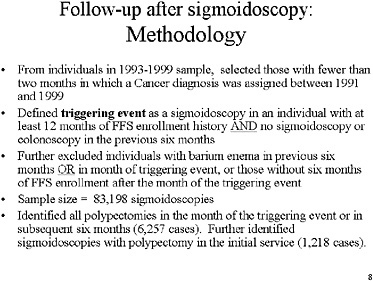
SLIDE 8 NOTES: Now for the second question: What happens to people who receive a sigmoidoscopy in the months immediately following the procedure? In particular, how are positive sigmoidoscopy examinations followed up?
In this case we examined individuals in the sample in the period 1993–1999 and we eliminated all individuals who met the “possible cancer beneficiary” criterion.
We defined a triggering event as any sigmoidoscopy that met the following criteria:
-
performed on a patient with at least 12 months of history in the sample,
-
no history of a sigmoidoscopy or colonoscopy in the previous 6 months;
-
no barium enema in the same or previous six months;
-
at least six months’ worth of data available after the index date.
Those criteria resulted in 83,000 index (triggering) events. We zeroed in on 6,257 of those with polypectomies in the month of the triggering event. And we further scrutinized about 1,200 beneficiaries whose index sigmoidoscopy included the removal of a polyp.
SLIDE 9
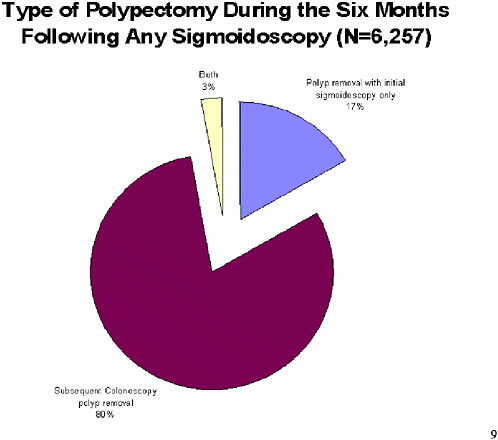
SLIDE 9 NOTES: In the universe of 6,257 sigmoidoscopy examinations associated with a polypectomy at any point in the succeeding six-months, fully 80 percent had the polypectomy in a subsequent colonoscopy, not in the initial sigmoidoscopy.
Seventeen percent of the polypectomies occurred as part of the triggering sigmoidoscopy examination.
SLIDE 10
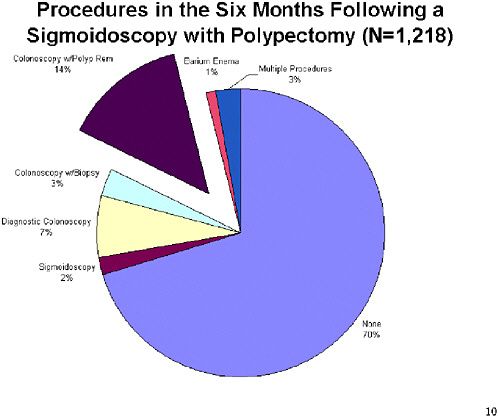
SLIDE 10 NOTES: This chart examines in greater detail what happened to the 17 percent of polypectomies that occurred as part of the sigmoidoscopy, in the months following sigmoidoscopy. Here, 25 percent of the cases went on to have at least one other colorectal diagnostic procedure in the six months following the triggering event.
SLIDE 12
SLIDE 12 NOTES: We conclude that somewhere between 55 and 64 percent of Medicare beneficiaries who undergo a polypectomy have at least one subsequent colonoscopy in the 5 year surveillance window.
Diagnostic and therapeutic follow-up following a sigmoidoscopy is frequent, and a large majority of those how underwent polypectomy within six months of the sigmoidoscopy had their polyps removed in subsequent procedures.












