
C
RISK AND PROTECTIVE FACTORS
Some people who are exposed to a traumatic event will develop posttraumatic stress disorder (PTSD) while others will not. Its occurrence depends on a complex interplay between risk factors that increase the likelihood of onset and protective factors that diminish it. Other variables influence the development of PTSD, including factors that preceded the exposure to trauma, factors associated with the trauma exposure itself, and factors associated with the recovery environment.
This appendix presents an abbreviated discussion of a few of the numerous risk factors and protective factors that might influence the development of PTSD among military personnel. The topic will be considered by the committee in greater detail in a report on deployment-related stress due to be published in 2007.
RISK FACTORS
For a military population, one of the most important risk factors for the onset of PTSD is exposure to combat. Features of combat, such as its intensity, whether an injury was sustained, or whether torture or captivity occurred, are related to the severity of exposures that by definition qualify within the Diagnostic and Statistical Manual (DSM-IV) criteria as traumatic. Other risk factors that might be involved with the development of PTSD are, for example, military sexual assault, homecoming environment, sex, and ethnicity (see Table C.1).
TABLE C.1 Risk Factors for PTSD in Military Populations
|
Risk Factor |
References |
|
Combat Exposure |
|
|
Combat and its severity |
Black et al. 2004; Goldberg et al. 1990; Hoge et al. 2004; Kang et al. 2003; Kulka et al. 1990; O’Toole et al. 1998; Roy-Byrne et al. 2004; Wolfe et al. 1999 |
|
Being wounded or injured |
Koren et al. 2005; North et al. 1999; Schreiber and Galai-Gat 1993; |
|
Witnessing death |
Breslau et al. 1999; Ford 1999 |
|
Witnessing grotesque death |
Green et al. 1990 |
|
Serving on graves-registration duty |
Sutker et al. 1994 |
|
Being tortured or being taken captive |
de Jong et al. 2001; Mollica et al. 1998; Speed et al. 1989; Sutker et al. 1993 |
|
Unpredictable and uncontrollable stressful exposure |
Foa et al. 1992; Southwick et al. 1993 |
|
Military Environment |
|
|
Sexual trauma, including assault |
Fontana et al. 1997b; Kang et al. 2005 |
|
Combat preparedness |
Asmundson et al. 2002 |
|
Deployment to war zone without combat |
Ikin et al. 2004 |
|
Homecoming Environment |
|
|
Lack of social support |
Fontana and Rosenheck 1994; Fontana et al. 1997a; Green et al. 1990; Johnson et al. 1997; Koenen et al. 2003; Stretch 1985; Stretch et al. 1985 |
|
Personal Factors |
|
|
Cumulative life stress before or after the traumatic event |
Breslau et al. 1999; Brewin et al. 2000; King et al. 1998; Maes et al. 2001; North et al. 1999 |
|
More resource loss, lower income or education, older age |
Norris et al. 2002 |
|
Being female |
Kang et al. 2003; Wolfe et al. 1999 |
Table C.1 calls attention to a variety of risk factors for PTSD identified in studies of military populations. Most of the studies cited were conducted in Vietnam or Gulf War veteran populations. A few of the risk factors noted above are discussed below because they are important or frequent predictors of PTSD in veterans.
Combat Exposure
Combat exposure and its severity are well-established risk factors documented in carefully designed studies of Vietnam and Gulf War veterans (e.g., Goldberg et al. 1990; Kang et al. 2003; Kulka et al. 1990; O’Toole et al. 1996). Combat exposure, in this context, includes many specific types of related exposures, such as prisoner-of-war status and witnessing gruesome injuries, torture, and death. Generally speaking, the greater the degree of combat exposure, the greater the likelihood of developing PTSD and the longer the duration of symptoms (Hoge et al. 2004; Kang et al. 2003; Koenen et al. 2003; Wolfe et al. 1999; Wolfe et al. 1999). A nationally representative study of 30,000 veterans of the Gulf War era found that the likelihood of PTSD increased as the number of combat-related stressors increased (Kang et al. 2003). Likewise, combat troops returning from Iraq report increased rates of PTSD compared to troops before deployment and compared to rates after deployment to Afghanistan (Hoge et al. 2004; Koenen et al. 2003; Roy-Byrne et al. 2004).
For many soldiers and other military personnel, deployment to a war zone is the most traumatic event in their lives. Relative to other common types of trauma, men who name combat trauma as the most traumatic event of their lives are at the highest risk for PTSD, according to a nationally representative study. They were 7 times more likely to have PTSD than those who named other events as their “worst lifetime traumatic event” (Prigerson et al. 2001). Nearly 42% of men who regarded combat as their worst lifetime experience met criteria for PTSD at some point in their lives. That rate was higher than that for any of the other common types of trauma reported by men in the study, including being sexually molested or raped and being physically abused or neglected as a child (Table C.2). Combat-related PTSD also was more likely to be associated with serious occupational and marital problems. In
TABLE C.2 Rates of PTSD, Occupational Problems, and Marital Problems in Traumatized Men in National Comorbidity Survey
|
|
Lifetime PTSD |
Occupational and Marital Problems Associated with Combat Trauma (%) |
||||
|
Traumatic Incident Identified as Worst Lifetime Event |
N |
% |
Currently Unemployed |
Recently Fired |
Ever Divorced |
Spousal Abuse |
|
Combat |
96 |
41.8 |
20.2 |
13.6 |
39.0 |
15.2 |
|
Life-threatening accident |
292 |
5.5 |
7.9 |
9.7 |
18.8 |
7.6 |
|
Natural disaster I |
178 |
3.9 |
13.4 |
4.9 |
9.5 |
4.0 |
|
Witnessing someone being badly beaten or killed |
492 |
6.1 |
7.7 |
4.4 |
11.3 |
5.4 |
|
Raped or sexually molested |
32 |
32.5 |
4.8 |
3.0 |
12.0 |
3.7 |
|
Physical attack, threatened with weapon, or held captive |
273 |
1.6 |
4.4 |
4.3 |
12.0 |
10.4 |
|
Physically abused or seriously neglected as child |
58 |
24.2 |
2.6 |
4.0 |
28.3 |
1.5 |
|
Other qualifying trauma |
152 |
5.1 |
8.3 |
6.3 |
12.2 |
8.0 |
|
Shock on learning of trauma to a person close to you |
130 |
4.4 |
3.0 |
22 |
7.8 |
3.9 |
|
SOURCE: Adapted with permission from Prigerson et al. 2001. |
||||||
Military Sexual Assault
Several factors in the military environment may be risk factors for development for PTSD but sexual assault is an important one. Suris et al. (2004) noted that woman veterans were 9 times more likely to develop PTSD if they had a history of military sexual assault. Another study (Kang et al. 2005) examined self-reported in-theater experiences of sexual harassment or assault and combat exposure and found statistically significant increases in PTSD associated with sexual assault in female and male veterans of the Gulf War.
Homecoming Environment
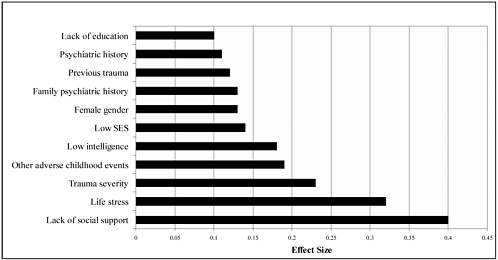
Lack of social support, particularly after the traumatic event, is a significant risk factor for PTSD. As soldiers return home, lack of social support from family, friends, and community is associated with PTSD, according to studies of Vietnam veterans (Fontana and Rosenheck 1994; Fontana et al. 1997a; Green et al. 1990; Johnson et al. 1997; Koenen et al. 2003; Stretch 1985; Stretch et al. 1985). The Vietnam War was unpopular and many veterans returning from combat were greeted with disrespect, hostility, or condemnation. Although many Iraq and Afghanistan veterans might be returning to more welcoming attitudes, the role of strong social, family, and community support is still important. In a meta-analysis of more than 50 studies on risk factors for PTSD in military and civilian populations, researchers found that lack of social support was a leading risk factor for development of PTSD compared with such other risk factors as lack of education, life stress, trauma severity, and other previous trauma (Figure C.1) (Brewin et al. 2000). A later meta-analysis by a team of investigators who used somewhat different methods also found that lack of social support was a strong risk factor for development of PTSD (Ozer et al. 2003).
Sex
In the US general population, women are about twice as likely as men to have PTSD at some point in their lives. Their lifetime prevalence is 10–12% versus 5% for men (Kessler et al. 1995; Resnick et al. 1993). It is not clear why women have higher rates of PTSD than men. That sex difference, however, is not peculiar to PTSD; women generally have higher rates of depression and anxiety disorders (Kessler et al. 1995).
Women veterans serving in the Gulf War were more likely than men to screen positive for likelihood of PTSD (Kang et al. 2003; Wolfe et al. 1999). Studies have not determined whether that is due to different exposures or specifically to inherent sex differences in the development of PTSD.
Ethnicity
After Vietnam, there was no difference in prevalence of PTSD between black, American Indian, and white veterans. Rates among blacks were higher until the investigators performed analyses to remove the effects of their having had greater combat exposure (Beals et al. 2002; Kulka et al. 1990). Still, questions linger about the ethnic minority differences, because several less representative studies reported higher rates of PTSD among black Vietnam veterans (e.g., Allen 1986; Penk et al. 1989). Latino Vietnam veterans, especially Puerto Rican veterans, had higher PTSD prevalence and more severe symptons even after adjustment for combat exposure (Ortega and Rosenheck 2000). Members of ethnic minorities appear to have a more chronic course of PTSD as well (King et al. 1998; Koenen et al. 2003). Distinct ethnic groups might differ in how they manifest symptoms, how they describe the symptoms, how they cope, what support systems they use, and whether they seek or stay in care (Department of Health and Human Services 2001).
PROTECTIVE FACTORS
Just as risk factors likely increase a person’s chances of developing PTSD, protective factors might reduce the risk. Researchers have found that protective factors include coping with the traumatic event in positive and active ways rather than by avoiding it (Benotsch et al. 2000; Norris et al. 2002; North et al. 2001), better training and preparation to respond to a traumatic event (Alvarez and Hunt 2005; Basoglu et al. 1997), higher education and income, a sense of mastery or self-esteem, and male sex (Brewin et al. 2000; Kulka et al. 1990; Orcutt et al. 2004); (Coker et al. 2005; Norris et al. 2002).
Beginning in the 1980s, research has shown that after a traumatic event, social support is associated with reduced likelihood of PTSD (e.g., Cohen and Wills 1985; Kaniasty and Norris 1997; Koenen et al. 2003; Ozer et al. 2003). The research involved largely civilians exposed to community or domestic violence. Social support is often defined as help with physical activities, emotional support, and having someone to talk with about traumatic experiences or to turn to for advice. Such social support might be provided by a network of health care and mental health care professionals as well as by family and community members (Flannery 1990).
Studies of veterans have shown that social support, particularly after homecoming, is also associated with reduced likelihood and severity of PTSD (Fontana and Rosenheck 1994; Fontana et al. 1997b; King et al. 1998). It was found that the protective effects of homecoming were greatest among those veterans who had the greatest war-zone exposures (Fontana et al. 1997a). Interestingly, Fontana et al. (1997a) also showed that having been part of a cohesive military unit did not have the protective effect of postwar social support.
One study (King et al. 1998), conducted in a sample of 1,632 Vietnam veterans from the National Vietnam Veterans Readjustment Study, found that hardiness as a personality trait was protective. Hardiness was a construct defined as having a sense of control over life, feeling that life is meaningful, and being open to change.
CONCLUSION
This appendix provided a very brief discussion of some of the risk and protective factors that might influence who will develop PTSD. Not all people who are exposed to traumatic events develop a psychiatric disorder, such as depression or PTSD. Its development can depend on the intensity of the traumatic event or stressor and on a host of pretrauma and posttrauma factors.
REFERENCES
Allen IM. 1986. Posttraumatic stress disorder among black Vietnam veterans. Hospital and Community Psychiatry 37(1):55–61.
Alvarez J, Hunt M. 2005. Risk and resilience in canine search and rescue handlers after 9/11. Journal of Traumatic Stress 18(5):497–505.
Asmundson GJ, Stein MB, McCreary DR. 2002. Posttraumatic stress disorder symptoms influence health status of deployed peacekeepers and nondeployed military personnel. Journal of Nervous and Mental Disease 190(12):807–815.
Basoglu M, Mineka S, Paker M, Aker T, Livanou M, Gok S. 1997. Psychological preparedness for trauma as a protective factor in survivors of torture. Psychological Medicine 27(6):1421–1433.
Beals J, Manson SM, Shore JH, Friedman M, Ashcraft M, Fairbank JA, Schlenger WE. 2002. The prevalence of posttraumatic stress disorder among American Indian Vietnam veterans: Disparities and context. Journal of Traumatic Stress 15(2):89–97.
Benotsch EG, Brailey K, Vasterling JJ, Uddo M, Constans JI, Sutker PB. 2000. War zone stress, personal and environmental resources, and PTSD symptoms in Gulf War veterans: A longitudinal perspective. Journal of Abnormal Psychology 109(2):205–213.
Black DW, Carney CP, Peloso PM, Woolson RF, Schwartz DA, Voelker MD, Barrett DH, Doebbeling BN. 2004. Gulf War veterans with anxiety: Prevalence, comorbidity, and risk factors. Epidemiology 15(2):135–142.
Breslau N, Chilcoat HD, Kessler RC, Davis GC. 1999. Previous exposure to trauma and PTSD effects of subsequent trauma: Results from the Detroit Area Survey of Trauma. American Journal of Psychiatry 156(6):902–907.
Brewin CR, Andrews B, Valentine JD. 2000. Meta-analysis of risk factors for posttraumatic stress disorder in trauma-exposed adults. Journal of Consulting and Clinical Psychology 68(5):748–766.
Cohen S, Wills TA. 1985. Stress, social support, and the buffering hypothesis. Psychological Bulletin 98(2):310–357.
Coker AL, Weston R, Creson DL, Justice B, Blakeney P. 2005. PTSD symptoms among men and women survivors of intimate partner violence: The role of risk and protective factors. Violence and Victims 20(6):625–643.
de Jong JT, Komproe IH, Van Ommeren M, El Masri M, Araya M, Khaled N, van De Put W, Somasundaram D. 2001. Lifetime events and posttraumatic stress disorder in 4 postconflict settings. Journal of the American Medical Association 286(5):555–562.
Department of Health and Human Services. 2001. Mental Health: Culture, Race, and Ethnicity. A Report of the Surgeon General. Rockville, MD: U.S. Department of Health and Human Services, Substance Abuse and Mental Health Services Administration, Center for Mental Health Services, National Institutes of Health, National Institute of Mental Health.
Flannery RB. 1990. Social support and psychological trauma: A methodological review. Journal of Traumatic Stress 3(4):593–611.
Foa EB, Zinbarg R, Rothbaum BO. 1992. Uncontrollability and unpredictability in post-traumatic stress disorder: an animal model. Psychological Bulletin 112(2):218–238.
Fontana A, Rosenheck R. 1994. Posttraumatic stress disorder among Vietnam Theater Veterans. A causal model of etiology in a community sample. Journal of Nervous and Mental Disease 182(12):677–684.
Fontana A, Rosenheck R, Horvath T. 1997a. Social support and psychopathology in the war zone. Journal of Nervous and Mental Disease 185(11):675–681.
Fontana A, Schwartz LS, Rosenheck R. 1997b. Posttraumatic stress disorder among female Vietnam veterans: A causal model of etiology. American Journal of Public Health 87(2):169–175.
Ford JD. 1999. Disorders of extreme stress following war-zone military trauma: Associated features of posttraumatic stress disorder or comorbid but distinct syndromes? Journal of Consulting & Clinical Psychology 67(1):3–12.
Goldberg J, True WR, Eisen SA, Henderson WG. 1990. A twin study of the effects of the Vietnam War on posttraumatic stress disorder. Journal of the American Medical Association 263(9):1227–1232.
Green BL, Grace MC, Lindy JD, Gleser GC, et al. 1990. Risk factors for PTSD and other diagnoses in a general sample of Vietnam veterans. American Journal of Psychiatry 147(6):729–733.
Hoge CW, Castro CA, Messer SC, McGurk D, Cotting DI, Koffman RL. 2004. Combat duty in Iraq and Afghanistan, mental health problems, and barriers to care. New England Journal of Medicine 351(1):13–22.
Ikin JF, Sim MR, Creamer MC, Forbes AB, McKenzie DP, Kelsall HL, Glass DC, McFarlane AC, Abramson MJ, Ittak P, Dwyer T, Blizzard L, Delaney KR, Horsley KWA, Harrex WK, Schwarz H. 2004. War-related psychological stressors and risk of psychological disorders in Australian veterans of the 1991 Gulf War. British Journal of Psychiatry. 185(Aug.):116–126.
Johnson DR, Lubin H, Rosenheck R, Fontana A, Southwick S, Charney D. 1997. The impact of homecoming reception on the development of posttraumatic stress disorder: The West Haven Homecoming Stress Scale (WHHSS). Journal of Traumatic Stress 10(2):259–277.
Kang H, Dalager N, Mahan C, Ishii E. 2005. The role of sexual assault on the risk of PTSD among Gulf War veterans. Annals of Epidemiology 15(3):191–195.
Kang HK, Natelson BH, Mahan CM, Lee KY, Murphy FM. 2003. Posttraumatic stress disorder and chronic fatigue syndrome-like illness among Gulf War veterans: A population-based survey of 30,000 veterans. American Journal of Epidemiology 157(2):141–148.
Kaniasty K, Norris FH. 1997. Social support dynamics in adjustment to disasters. In: Duck S, Editor. Handbook of Personal Relationships. 2nd ed. New York: Wiley. Pp. 595–619.
Kessler RC, Sonnega A, Bromet E, Hughes M, Nelson CB. 1995. Posttraumatic stress disorder in the National Comorbidity Survey. Archives of General Psychiatry 52(12):1048–1060.
King LA, King DW, Fairbank JA, Keane TM, Adams GA. 1998. Resilience-recovery factors in post-traumatic stress disorder among female and male Vietnam veterans: Hardiness, postwar social support, and additional stressful life events. Journal of Personality & Social Psychology 74(2):420–434.
Koenen KC, Stellman JM, Stellman SD, Sommer JF, Jr. 2003. Risk factors for course of posttraumatic stress disorder among Vietnam veterans: A 14-year follow-up of American Legionnaires. Journal of Consulting and Clinical Psychology 71(6):980–986.
Koren D, Norman D, Cohen A, Berman J, Klein EM. 2005. Increased PTSD risk with combat-related injury: A matched comparison study of injured and uninjured soldiers experiencing the same combat events. American Journal of Psychiatry 162(2):276–282.
Kulka RA, Schlenger WE, Fairbank JA, Hough RL, Jordan BK, Marmar CR, Weiss DS. 1990. Trauma and the Vietnam War Generation: Report of Findings From the National Vietnam Veterans Readjustment Study. New York: Brunner/Mazel.
Maes M, Mylle J, Delmeire L, Janca A. 2001. Pre- and post-disaster negative life events in relation to the incidence and severity of posttraumatic stress disorder. Psychiatry Research 105(1–2):1–12.
Mollica RF, McInnes K, Pham T, Smith Fawzi MC, Murphy E, Lin L. 1998. The dose-effect relationships between torture and psychiatric symptoms in Vietnamese ex-political detainees and a comparison group. Journal of Nervous and Mental Disease 186(9):543–553.
Norris FH, Friedman MJ, Watson PJ, Byrne CM, Diaz E, Kaniasty K. 2002. 60,000 disaster victims speak: Part I. An empirical review of the empirical literature, 1981–2001. Psychiatry 65(3):207–239.
North CS, Nixon SJ, Shariat S, Mallonee S, McMillen JC, Spitznagel EL, Smith EM. 1999. Psychiatric disorders among survivors of the Oklahoma City bombing. Journal of the American Medical Association 282(8):755–762.
North CS, Spitznagel EL, Smith EM. 2001. A prospective study of coping after exposure to a mass murder episode. Annals of Clinical Psychiatry 13(2):81–87.
Orcutt HK, Erickson DJ, Wolfe J. 2004. The course of PTSD symptoms among Gulf War veterans: A growth mixture modeling approach. Journal of Traumatic Stress 17(3):195–202.
Ortega AN, Rosenheck R. 2000. Posttraumatic stress disorder among Hispanic Vietnam veterans. American Journal of Psychiatry 157(4):615–619.
O’Toole BI, Marshall RP, Grayson DA, Schureck RJ, Dobson M, Ffrench M, Pulvertaft B, Meldrum L, Bolton J, Vennard J. 1996. The Australian Vietnam Veterans Health Study: III. psychological health of Australian Vietnam veterans and its relationship to combat. International Journal of Epidemiology 25(2):331–340.
O’Toole BI, Marshall RP, Schureck RJ, Dobson M. 1998. Posttraumatic stress disorder and comorbidity in Australian Vietnam veterans: Risk factors, chronicity and combat. Australian and New Zealand Journal of Psychiatry 32(1):32–42.
Ozer EJ, Best SR, Lipsey TL, Weiss DS. 2003. Predictors of posttraumatic stress disorder and symptoms in adults: A meta-analysis. Psychological Bulletin 129(1):52–73.
Penk WE, Robinowitz R, Black J, Dolan M, Bell W, Dorsett D, Ames M, Noriega L. 1989. Ethnicity: Post-traumatic stress disorder (PTSD) differences among black, white, and Hispanic veterans who differ in degrees of exposure to combat in Vietnam. Journal of Clinical Psychology 45(5):729–735.
Prigerson HG, Maciejewski PK, Rosenheck RA. 2001. Combat trauma: Trauma with highest risk of delayed onset and unresolved posttraumatic stress disorder symptoms, unemployment, and abuse among men. Journal of Nervous & Mental Disease 189(2):99–108.
Prigerson HG, Maciejewski PK, Rosenheck RA. 2002. Population attributable fractions of psychiatric disorders and behavioral outcomes associated with combat exposure among US men. American Journal of Public Health 92(1):59–63.
Resnick HS, Kilpatrick DG, Dansky BS, Saunders BE, Best CL. 1993. Prevalence of civilian trauma and posttraumatic stress disorder in a representative national sample of women. Journal of Consulting and Clinical Psychology 61(6):984–991.
Roy-Byrne P, Arguelles L, Vitek ME, Goldberg J, Keane TM, True WR, Pitman RK. 2004. Persistence and change of PTSD symptomatology—a longitudinal co-twin control analysis of the Vietnam Era Twin Registry. Social Psychiatry and Psychiatric Epidemiology 39(9):681–685.
Schreiber S, Galai-Gat T. 1993. Uncontrolled pain following physical injury as the core-trauma in post-traumatic stress disorder. Pain 54(1):107–110.
Southwick SM, Krystal JH, Morgan CA, Johnson D, Nagy LM, Nicolaou A, Heninger GR, Charney DS. 1993. Abnormal noradrenergic function in posttraumatic stress disorder. Archives of General Psychiatry 50(4):266–274.
Speed N, Engdahl B, Schwartz J, Eberly R. 1989. Posttraumatic stress disorder as a consequence of the POW experience. Journal of Nervous and Mental Disease 177(3):147–153.
Stretch RH. 1985. Posttraumatic stress disorder among U.S. Army Reserve Vietnam and Vietnam-era veterans. Journal of Consulting and Clinical Psychology 53(6):935–936.
Stretch RH, Vail JD, Maloney JP. 1985. Posttraumatic stress disorder among Army Nurse Corps Vietnam veterans. Journal of Consulting & Clinical Psychology 53(5):704–708.
Suris A, Lind L, Kashner TM, Borman PD, Petty F. 2004. Sexual assault in women veterans: An examination of PTSD risk, health care utilization, and cost of care. Psychosomatic Medicine 66(5):749–756.
Sutker PB, Allain AN Jr, Winstead DK. 1993. Psychopathology and psychiatric diagnoses of World War II Pacific theater prisoner of war survivors and combat veterans. American Journal of Psychiatry 150(2):240–245.
Sutker PB, Uddo M, Brailey K, Allain AN, Errera P. 1994. Psychological symptoms and psychiatric diagnoses in Operation Desert Storm troops serving graves registration duty. Journal of Traumatic Stress 7(2):159–71.
Wolfe J, Erickson DJ, Sharkansky EJ, King DW, King LA. 1999. Course and predictors of posttraumatic stress disorder among Gulf War veterans: A prospective analysis. Journal of Consulting and Clinical Psychology 67(4):520–528.
















