
1
Introduction
You are a 38-year-old woman with abnormal vaginal bleeding because of early-stage cervical cancer. In 4 years, will you be living the rest of your life with little interruption after a lifesaving, low-risk hysterectomy, or dying far from home with advanced and painful cancer, an outcast from friends and family? If you have adequate resources, either because you live in a high-income country or have personal wealth, it is unlikely that you would have found yourself in this situation at all—with early-stage cervical cancer. In the United States, for example, periodic screening with a Pap smear would have detected precancerous changes years before, and the abnormal tissue would have been removed in a minimally invasive procedure. But if you are poor and come from a rural village in a low-income country such as Tanzania, the next 4 years will be agonizing physically and psychologically, and crippling financially as you try again and again to get help. You are unlikely to have anything to ease the pain of your final days.
How could this scenario turn out differently, in Tanzania or other resource-limited countries, in the short-to-medium term? Rewinding the story, the 38-year-old woman could have reached the cancer center in the city months sooner, had she not been discouraged by traditional healers, family, and friends. She could have been cared for and lived a full life. Even at a somewhat advanced stage, cervical cancer is curable by radiotherapy, which is practicable and available in many low- and middle-income countries (LMCs) at an affordable cost. If her story could be fast forwarded a decade, she could be screened at age 30 or 35 using one of the single-visit “screen-and-treat” approaches now beginning to gain an evidence base. The slow-progressing lesion on her cervix could have been removed and normal
life resumed after possibly a month of some discomfort. In the worst case, if the cervical cancer progressed anyway and eventually led to death, her final days could have been relatively free of pain and her other basic physical, psychological, and emotional needs met by village palliative care workers and family—services already available in some parts of Africa. If the 38-year-old has a daughter entering adolescence, that daughter soon might be able to get a vaccine that will protect her against cervical cancer by preventing its cause, infection with human papillomavirus (HPV). Even in LMCs, these alternate endings are possible, with increased global awareness of the magnitude of the cancer problem, the opportunities that exist already, and those just around the corner.
The long view back over the 20th century in the United States and other wealthy countries, where the picture of cancer incidence and mortality is reasonably clear, gives perspective and reason for optimism that the cancer burden can be lessened in LMCs today.
REASONS FOR OPTIMISM
Over the course of the 20th century, the cancer burden changed dramatically—positively and negatively—in the United States and other wealthy countries. Changing lifestyles, environmental influences, and improved health care all have contributed. In 1900, cancer was eighth in the list of causes of death.1 By 1950, it was second only to heart disease. Cancer death rates continued to rise through the early 1990s, when overall rates were nearly three times the 1900 rate (National Cancer Institute, 1997). The single greatest cause of the cancer increase was the rise in lung cancer from tobacco use. While lung cancer (and other smoking-related cancers) increased, rates for other cancers were falling. Death rates for stomach cancer—the most frequent cause of cancer deaths early in the 20th century—fell by nearly 90 percent over that period, with the greatest declines occurring in the 1950s. The reasons are thought to be improved living conditions, which reduced chronic infection with the cancer-inducing bacterium Helicobacter pylori, and better diet, including more fresh and less preserved food. Treatment of stomach cancer is still relatively ineffective, so medical care contributed little. The story is different for cervical cancer, which claimed more women’s lives than any other cancer in the United States in the early 1900s. Declines in death rates began early, again probably due to better living conditions. Death rates decreased quickly and were driven to their current low levels by early detection and curative medical care.
After the earlier continuous increases, by the early 1990s, lung cancer
death rates among U.S. men had declined, following several decades of concerted action against smoking. (The epidemic in women began later and may now be plateauing.) Overall cancer death rates also declined by a few percentage points, reflecting the combined effects of improved environmental conditions, healthier lifestyle choices, and better medical care (Wingo et al., 2003).
The changes that have been seen in wealthy countries during the past century and into this century, and the knowledge gained about the causes of cancer and preventive and other interventions, are evidence that control measures can be effective. These changes and knowledge provide goals for practicable cancer control measures for LMCs that can begin to be established widely over the next few decades, once the opportunities are recognized and pursued. With the growing recognition that chronic, noncommunicable diseases are increasing in importance in LMCs, the time is right to move forward.
The remainder of this chapter introduces the need for greater focus on cancer (and other chronic diseases), defines low- and middle-income countries, and describes the intent and framework of the report.
CANCER AND OTHER CHRONIC DISEASES
The lives of far too many people in the world are being blighted and cut short by chronic diseases such as heart disease, stroke, cancer, chronic respiratory diseases and diabetes. This is no longer only happening in high income countries. Four out of five chronic disease deaths today are in low and middle income countries.
J.W. Lee, Director General, World Health Organization October 2005
Chronic diseases have recently been called “the neglected epidemic” (Strong et al., 2005). Even the United Nations Millennium Development Goals—the vehicle for improving the health and welfare of the world’s poorest starting at the beginning of the 21st century—mention only the major infectious diseases by name. But that has begun to change. The World Health Organization (WHO) has begun a campaign to raise the profile of chronic diseases in LMCs, recognizing that these countries suffer the double burden of the major infectious disease killers and mounting chronic illnesses. WHO dispels the idea that we can wait to conquer infectious diseases before turning to chronic diseases. The two must be addressed simultaneously.
Greater efforts at cancer control in LMCs have long been promoted by those in the cancer community. The WHO cancer program has played its role by providing guidance for governments; the broader cancer interest community, including the International Union Against Cancer and its mem-
TABLE 1-1 World Bank Classification of Countries by Income Level, 2004
|
Classification |
Income Boundaries Gross National Income per Capita |
|
Low income |
$825 or less |
|
Lower middle-income |
$826–$3,255 |
|
Upper middle-income |
$3,256–$10,065 |
|
High income |
$10,066 or more |
|
SOURCE: World Bank (2005). |
|
bers, has reached out to the public and professionals. However, international health efforts historically have been dominated by the immediate problems of infectious diseases that kill infants and children. It is largely the progress made against those diseases that has led to the aging of the global population and the greater impact of chronic diseases.
LOW- AND MIDDLE-INCOME COUNTRIES DEFINED
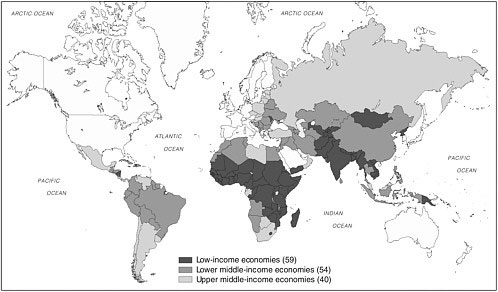
This report uses the World Bank classification of countries by income level (Table 1-1, Figure 1-1, and Box 1-1). This grouping of LMCs takes in most of the world’s population—all but the wealthy countries—and represents a broad spectrum of development. The low-income countries are relatively similar in health profiles and services. This is not so true of the middle-income countries, however. These countries have different levels of infrastructure, different histories, and a much wider range of per-capita health spending. For low-income and some middle-income countries, the challenge is to add services from a very low base. For at least some of the middle-income countries—the emerging economies of Eastern and Central Europe, in particular—the challenge is to upgrade an existing infrastructure that may not provide the most appropriate services and that could become more efficient. In all cases, planners must consider the costs of services and who will pay. Each country must evaluate its own needs and opportunities, regardless of the income rubric in which it falls, and plan accordingly. This report highlights major global opportunities in cancer control that are relevant to most countries regardless of their current situation. It does not prescribe the actions that should be taken by those countries.
INTENT OF THIS REPORT
This report is intended to highlight major opportunities for LMCs toward better cancer control—cancer planning, cancer prevention and early
detection (screening), cancer management (diagnosis and treatment, including palliative care) and psychosocial support for patients and families—even where resources are limited. Whatever the status quo, next steps are feasible everywhere. The report is written to bring this message to policy makers in LMCs as well as the many global partners involved in international health, as cancer becomes an ever-widening global health concern. One conclusion of the report—echoing what others have stated—is that cancer is a global disease, and global cooperation and collaboration will allow all countries to move forward. Knowledge sharing among the high-income countries enjoys
|
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
a long history among private-sector advocates and cancer control health professionals in and out of government. The sponsors of this report—the U.S. National Cancer Institute (part of the National Institutes of Health) and the American Cancer Society—are among the global leaders in research, training, and advocacy.
The report is not a how-to manual that prescribes specific interventions, a role left best to WHO, the health care professions, and others. Instead, it shines a light on areas of great opportunity that countries should at least be aware of, that could lessen the current and growing burden of cancer.
Reflected in the report framework outlined below, the opportunities include aspects of prevention; services to patients who have cancer, at whatever stage; and building cancer capacity. No report on the global cancer problem could ignore the growth in tobacco use in LMCs, guaranteeing an epidemic of cancer, cardiovascular disease, and respiratory disease, if known effective actions are not taken now to curtail tobacco use. Global awareness of the hazards of tobacco has never been higher. Many people in LMCs still have not heard that message, but are beginning to hear messages about the glamor of taking up smoking.
The opportunities that exist for tackling some of the leading causes of death from cancer are less well known. Most liver cancers—among the most numerous and deadly—can be prevented by simple childhood immunization. Future generations can be protected against cancer of the cervix, also caused by a virus, with a new vaccine.
Current generations can be saved with simple, yet highly effective, screening techniques. Treatment for children and young adults with highly curable cancers has been an attractive way to build cancer management infrastructure, guaranteeing success for some significant proportion and demonstrating that cancer does not have to be a death sentence, a message that will be new to many citizens of LMCs. But when death from cancer is inevitable, for adults and children, feasible and inexpensive palliative care to ease symptoms vastly improves the comfort of patients and those around them.
Beyond the specific interventions, a way forward has been demonstrated to tailor cancer control to differing resource levels, maintaining a focus on evidence of effectiveness and appropriateness to the setting. This “resource-level appropriate” approach ties in with recommendations about cancer centers and centers of excellence as focal points for cancer control where none now exists.
All of the opportunities identified are feasible at least in some LMCs. We recognize, however, that undertaking new initiatives and moving existing ones forward requires a long view and a sustained commitment. There are no quick fixes in cancer control, but the payoffs will come for appropriate, effective efforts put in place today in LMCs, with the support of the global health community.
FRAMEWORK OF THE REPORT
The remainder of the report consists of the following chapters:
2. Cancer Causes and Risk Factors and the Elements of Cancer Control Major and minor causes of and risk factors for cancer in LMCs as a basis for setting the control agenda. The broad elements of cancer control: cancer
planning, cancer prevention and early detection (screening), cancer management—diagnosis and treatment, including palliative care—and psychosocial support for patients and families.
3. The Cancer Burden in Low- and Middle-Income Countries and How It Is Measured The best available data on incidence and mortality from cancer in LMCs, trends in the leading types of cancer, the availability of relevant data, and opportunities for improving understanding of the cancer burden.
4. Defining Resource-Level-Appropriate Cancer Control “Resource-level appropriateness” introduced, using the example of the Breast Health Global Initiative. An approach to applying this idea to other cancers is presented.
5. Preventing Cancers (and Other Diseases) by Reducing Tobacco Use The impact of tobacco use, and the evidence for reducing tobacco use through a series of public policy and personal interventions.
6. Compelling Opportunities in Global Cancer Control Opportunities in three areas: (1) furthering the global agenda to eliminate most deaths from liver cancer through universal vaccination against the hepatitis B virus; (2) eliminating most cervical cancers through a combination of new screening techniques and vaccination against HPV, the cause of virtually all cervical cancers; and (3) developing the capacity to treat curable cancers in children and young adults.
7. Palliative Care The status of palliative care in LMCs, and feasible and cost-effective measures that can be taken to extend pain control and other measures much more broadly, even in very low-resource environments.
8. Cancer Centers in Low- and Middle-Income Countries The role of cancer centers—from modest to sophisticated, as appropriate to available resources—as a path to move forward in cancer control. “Centers of excellence” are proposed as hubs for national cancer control planning and programs, as well as cancer management.
9. Advocacy for Cancer Control Needs and opportunities for stepping up advocacy efforts in LMCs. Advocacy from the public and health professionals has played a critical role in advancing cancer control in the United States and other high-income countries, a lesson that should be transferred to LMCs.
10. Expanding the Role of the Global Community in Global Cancer Control The “global community”—governments, academia, the private sector—and
their roles in helping LMCs set and carry out their health care agendas, which thus far have lacked a focus on cancer.
Appendix A. Cancer Control in Malaysia and Tanzania Profiles of cancer control in Malaysia (an upper middle-income country) and Tanzania (a low-income country) from papers by cancer professionals in those countries, commissioned by IOM.
Appendix B. Acronyms and Abbreviations.
REFERENCES
National Cancer Institute. 1997. A New Agenda for Cancer Control Research: Report of the Cancer Control Review Group. Bethesda, MD: National Cancer Institute.
Strong K, Mathers C, Leeder S, Beaglehole R. 2005. Preventing chronic diseases: How many lives can we save? Lancet 366(9496):1578–1582.
Wingo PA, Cardinez CJ, Landis SH, Greenlee RT, Ries LA, Anderson RN, Thun MJ. 2003. Long-term trends in cancer mortality in the United States, 1930–1998 [erratum appears in Cancer 103(12):2658]. Cancer 97(12 Suppl):3133–3275.
World Bank. 2005. World Development Indicators 2005. Washington, DC: World Bank.










