
2
The Current and Future State of Acute Care
Hospitals are complex and often chaotic places, said Dr. Marilyn Chow, vice president of National Patient Care Services at Kaiser Permanente in Oakland, CA. This complexity is due in part to the nature of patients’ conditions. But it also arises from technologies that are not seamlessly connected to each other, including electronic health records (EHRs), biomedical devices, and robotic devices.
Nurses are the primary professional caregivers in hospitals. The efficient use of their time and energy is critical to the functioning of hospitals and acute care. Yet nurses’ time is not used efficiently today. According to a study led by Chow and Ann Hendrich, vice president of Clinical Excellence Operations for Ascension Health in St. Louis, of 767 nurses at 36 medical surgery units, the tasks of medication administration, care coordination, and documentation consumed the majority of all nursing practice time—part of an estimated $50 billion spent on documentation in health care annually. As shown in Figure 2-1, less than one fifth of nursing practice time went to direct patient care activities, such as providing procedures and treatments at the bedside. Just 7.2 percent of nursing time was spent on patient assessment and vital signs. “That equates to about 31 minutes out of each 10-hour shift,” Chow observed (Hendrich et al., 2008).
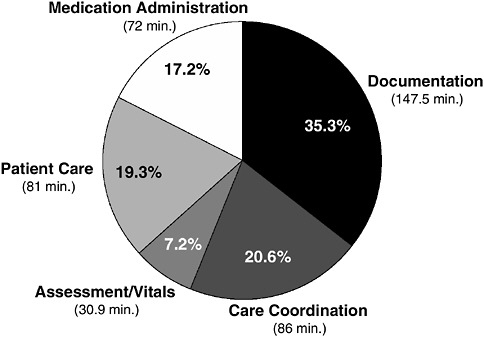
FIGURE 2-1 How do nurses spend their time?
SOURCE: Hendrich et al. (2008). Reprinted from The Permanente Journal, (www.kp.org/permanentejournal) 12(3), Hendrich, A., M. Chow, B. A. Skierczynski, and Z. Lu, A time and motion study: How do medical-surgical nurses spend their time?, 37-46, copyright 2008, reprinted with permission from The Permanente Press.
The working conditions of nurses are extremely stressful. They often deliver care within inefficient and disconnected systems; they manage a complex list of physician orders that require continuous reprioritizing; they perform the critical functions of surveillance and continuous monitoring of patients; and they do this work while “hunting and gathering” for equipment, supplies, and personnel, and experiencing frequent interruptions and distractions. They become what Chow called “masters of work-arounds” for systems that do not function well.
Over the next decade, Chow asserted, new practice models are needed “that focus on the real contributions of nurses, and we need to change the way we organize and deliver that care.” For example, the Gordon and Betty Moore Foundation has funded a project called Destination Bedside in two Kaiser facilities in Northern California. It is seeking to create more effective work environments that seamlessly support nurses and other clinicians in the delivery of patient care. In addition, a
variety of recent articles, reports, and books have brought new thinking and new ideas to the practice of nursing from both within and outside of health care.
Chow said she has spent a lot of time listening to people about their hospital experiences and asking them what was missing, what could be done differently, and what made a difference in their experiences. She has found that information and knowledge are growing “at warp speed.” The acute care environment is being reshaped by technologies, new business models, and human needs. New acute care models will either emerge haphazardly by default or coherently by design. Furthermore, aspects of some coherent new models are already evident in the health care system. “The future is already here. It’s just not everywhere.”
CORE CONCEPTS FOR IMAGINING THE FUTURE OF NURSING
Chow focused on five core concepts, described below, for imagining the future of nursing in acute care.
Core Concept 1:
Leverage the Power of the Electronic Health Record
The EHR could be the connective tissue of the health care system. An EHR not bound to one site or caregiver could enable improved care coordination and transitions, provide complete information connectivity, and transform the manner in which care is delivered and received, Chow said.
Kaiser Permanente has learned many lessons from the electronic system it has developed and implemented. Last year the system had 6 million electronic visits—“imagine the personal time savings for the patient, having an e-visit, versus coming into a clinic or an emergency department,” Chow said. The EHR has enabled the invention of new patient-centered roles for nurses. For example, a pilot program in a Southern California Kaiser Permanente emergency department called the “Virtual Charge Nurse” tracks patients from the time they arrive at a hospital until a decision is made to discharge or admit them. The EHR shows what has or has not happened to a patient, allowing tests and procedures to be moved online and providing patients with a “virtual advocate.” In another program, EHRs have been used to standardize the documentation
and management of pressure ulcers. In Kaiser’s experience, the implementation of EHRs has reduced documentation loads and increased nurses’ time in patient rooms. “The EHR is a tool that will raise the bar for care delivery across all settings, including acute care,” said Chow. “It must be seamlessly integrated with other technologies and devices so that nurses are not the human interface for technology that does not work together.”
Core Concept 2:
Achieve a Balance Among Technologies, Disruptive Business Models, and Human Needs
Incredible technological developments are on the horizon. For example, Chow highlighted miniaturization and wireless technologies that are being used to create body sensor networks that will monitor everything from heartbeats to brainwaves to temperature to blood glucose levels from anywhere in the hospital or even remotely from home.
The convergence of molecular biology, computer, and medical science with electrical, mechanical, genetic, and biomedical engineering could have profound effects on practice models. In a revolutionized future, technologies could assist nurses with much of their work and help consumers in diagnosing and treating themselves with self-help tools and personalized designer drugs. An example is the website developed by Microsoft and Emory University (www.h1n1responsecenter.com) that allows users to determine if they likely have the flu, whether or not to be seen by a health care provider, and what their overall risk is as a flu patient. “Imagine smart systems to guide patients and clinicians through available health information,” Chow said. Such technologies produce what she called a “wow factor.”
So-called disruptive innovations and business models,1 such as retail health care clinics, nurse navigators, health coaches, and patient advocates, could be another prominent feature of a future health care system. These disruptive business models could have a major impact on nursing practice. Furthermore, these innovations can be combined with or en-
abled by technology. In the future, technology will come to people rather than people going to the technology. “Remember when you had to send your printing requests to a central duplication center?” Chow asked. “Now you can print at your own desk.” In 2002, for example, General Electric sold a conventional ultrasound machine for $100,000 and up to sophisticated hospital imaging centers. In 2007, GE sold a portable ultrasound machine for emerging markets in developing countries at a price of $15,000, giving remote areas access to high technology.
Disruptive innovations aimed directly at human needs have been far less plentiful. “What would we [need to] do to actually be human centered? What are the core human needs? Is it that I hate to travel to the doctor’s office or the emergency department, but that I still want someone to look me in the eye, to listen to me, to touch my hand, and to advocate for me? How might we design for human needs and more efficiency, while using innovative business-to-business and technology tools?” The goal is to find a balance among technology, disruptive innovations, and human needs.
Core Concepts 3 and 4:
Implement Rapid Translation Teams and Interdisciplinary Teams of Designers
Nurses cannot design a patient-centered system by themselves. Technologies are arriving faster than they can be integrated into the health care system, and people are not able to make sense of much of the information already available. Chow suggested that one possible solution to this deluge of new technology and information is the creation of rapid translation teams. They would assist in the implementation of patient-centered systems that were developed by interdisciplinary teams of designers.
These rapid translation teams could scan, understand, and integrate the technological environment and make connections among technology, research, science, and acute care. Teams could include nurses and other experts such as engineers, geneticists, academic researchers, architects, ethnographers, designers, technologists, change specialists, and frontline clinicians. Rapid translation teams could in turn interact with interdisciplinary teams of designers, including behavioral scientists, marketers, engineers, clinicians, and patients. The result would be a system for designing the future of acute care, with human needs consciously incorpo-
rated into the design process. “Change in acute care will happen,” Chow said. “It is a question of how we design it.”
Core Concept 5:
Create an Infrastructure for Rapid Network Exchange of Successful System Design Innovations
A system to design successful innovations will need to be agile. Technological changes occur too quickly to plan, prototype, and test innovations over the course of several years. “We need to create a simple, easy venue for the quick exchange of what’s working and not working,” Chow explained.
Successful system design innovations also demand leadership and coordination. For example, a national institute for human-centered, empathy-based care with regional nodes could help spread the work of the rapid translation teams and interdisciplinary design teams. Such an institute might focus on economic measures of the value of nursing. It could emphasize an approach to nursing comparable to how one would care for a parent or sibling. “We nurses want to help patients and family members the way we do as the nurses for our families,” said Chow. Health innovation design forums could also help disseminate the work of rapid translation and interdisciplinary teams. Nurses could help prototype and pilot new processes, systems, and multidisciplinary practice models.
Several institutions have demonstrated the value of these approaches. For example, the University of Pittsburgh Medical Center has piloted equipment in 22 rooms designed to improve patient safety, increase customer satisfaction, and help nurses and other health care professionals to deliver the right care at the right time, every time. Ascension Health is planning to have three innovation units, and Kaiser Permanente has established a 37,000-square-foot facility to explore the intersection of technology, space, and workflow.
INSTITUTIONAL AND POLICY CHANGES
Nurses have much to learn from other specialties. An example is the role of the nurse navigator in oncology care that could be adapted for use in elder care. Nurses could work to re-purpose solutions found elsewhere. Nurses could also work to generate metrics for face-to-face interactions or system-level measures.
Payment systems need to be changed to recognize the time nurses spend with patients and their families, instead of forcing nurses to squeeze such interactions into their spare time. Chow asked what would need to change from a technology and a systems perspective to make this happen. For example, what if nurses partnered with hospitalists to admit patients? The physician could handle the medical diagnosis and orders while the nurse handles everything else. The nurse could be a single point of contact for the patient and family during a hospital stay as well as during discharge and transition to the home. The nurse could even visit the patient at home, potentially for several months, as happens with Mary Naylor’s Transitional Care Model.2 “We need nurses to think like entrepreneurs and be willing to be designers and experimenters.”
Chow also suggested that consideration be given to assigning patients a primary nurse. Patients may have a primary physician and a primary medical assistant. But they do not have a primary nurse.
Federal waivers for state experiments with new practice models could enable expansion of the scope of practice for nurses. In California, for example, a statute enabling health workforce pilot projects has expanded the scope of practice of clinicians beyond current law to test the safety and quality of new, innovative practices. Bringing such waivers to the federal level would allow experimentation that challenges state scope-of-practice laws.
CONCLUSIONS
In Great Britain, Prime Minister Gordon Brown issued the following mandate to the Commission on the Future of Nursing and Midwifery: Reposition nurses and nursing in the eyes of the consumer. That mandate fits with the mission of the Robert Wood Johnson Foundation Initiative on the Future of Nursing, at the Institute of Medicine, Chow said. The chair of the commission, Ann Keen, advised Donna Shalala, the leader of the Initiative on the Future of Nursing, to “have courage, come to the forefront, and stand up for the care you know nurses can do.” Chow issued similar advice to the committee: “Timing is everything. Be bold and seize the day.”








