
8
Opportunities for Change
Summarizing the workshop discussions, Rouse organized the workshop into three themes: the problem, research approaches, and people.
THE PROBLEM
During the workshop, the problem facing quality improvement was often characterized as a multifaceted problem. Components of the problem were said to exist on many levels, ranging from process improvements and process innovations to reductions in costs and errors. Connecting these components are the ways in which information is gathered and conclusions are reached. Commonly, information sharing occurs though stories, online information, evidence, and statistics. These components and connections collectively define the areas where problems occur with health care quality improvement research. For example, at the individual intervention level, problems with process improvements centered on their ability to generate only modest effects (around 5 percent) and variability (the high variability of organizations, variability of time, and variability of locations). At the organizational level, challenges in quality improvement research include management of processes, management of the transition between research findings and practice, management of innovation, and management of organizational change.
On a systems level, the issues of cost and value and the incentives for improvement and change were also of concern.
RESEARCH APPROACHES
The workshop identified a number of research approaches used to address the problem. Rouse recognized the current cultural conflict in the field related to conducting quality improvement evaluations as medical research when much of the work is actually organizational research. These types of research are conducted differently and often have different goals, thereby creating a dilemma for researchers. Other research approaches that were discussed include interdisciplinary collaboration and the approaches required to properly address ethical questions surrounding quality improvement research. These approaches employed a variety of interventions at different levels, such as provider reminders and methods to manage risk. It was often mentioned that to study change, secular trends needed to be separated from trends actually caused by an intervention. To disseminate approaches and findings, the role of journals was discussed as critical.
PEOPLE
Bringing the approaches, the tools, and the problems together are the people, who range from providers and purchasers to patients and researchers. The central question, Rouse said, is how to deal with professionals and their disciplines in terms of dealing with change. Effecting change requires people, but engaging people is itself a difficult task. Change requires encouragement of coordination, identification of attractors, understanding of patterns of behavior, and recognition of routines, rituals, and beliefs of all people involved. In other words, everyone is a participant in the process of addressing the problem, Rouse said.
PUTTING IT TOGETHER
The health care quality improvement ecosystem can thus be organized around the three themes—problem, approach, and people (Figure 8-1). The problem and approaches are connected by information gleaned from the problem and the interventions at all levels. In addressing the problem, people face the paradox of being agents of change as well as being the focus of change. People are connected to the approach because implementation of identified approaches
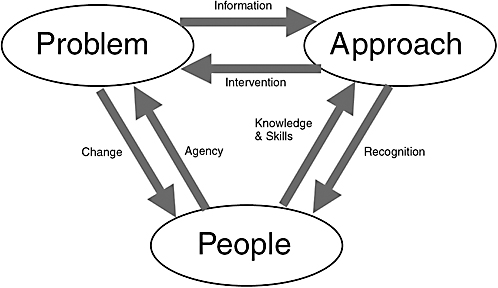
FIGURE 8-1 The quality improvement ecosystem.
is driven by their knowledge and skills. In the opposite direction, people need to receive recognition of their work at an individual level, organization level, or subdiscipline level.
A new model should be developed to study the delivery of health services in the 21st century. As opposed to experimental designs and analyses of variance to determine best models, process models could be developed to simulate different scenarios, Rouse said. Simulations are often used in industry; for example, IBM used a model to decrease the time to market for some of its products by 50 percent. Although simulations are difficult to validate, their potential implications are huge, and validation is not always necessary, particularly if the goal is insights rather than predictions. Large-scale changes are very difficult to achieve based purely on empirical data, Rouse said. It was noted, however, that it is difficult for simulations to adequately capture human interactions and the effects of those interactions.
The nature of the current health care system constrains improvements, Rouse concluded. Simply improving all current efforts will not produce desired changes. Using an example from government, it was believed that if researchers worked harder, better outcomes would result. Simulations showed this not to be true—in fact, the way in which the government operates actually constrained the yield from the system. Substantial change requires dramatic shifts in culture and innovation; however, innovation is difficult because it is both afforded and hindered by people.
CHANGING THE SYSTEM
In addressing the question of what would really drive fundamental change in the overall system, Rouse suggested a lesson from the university system, where students are “free electrons” and catalyze enthusiasm for new areas of study, attracting faculty to focus on those areas. In the health care system, the catalyst is unclear, but very well could be patients as consumers of care.
Building off Rouse’s points, Wallace discussed consumers as the way to identify change and as the source of leadership for change. For example, the ability for patients to access large parts of their medical charts and to securely e-mail their physicians directly was not an innovation stimulated by providers, but by patients. The success of this was largely due to the innovation being aligned with patient interests. As an example, Kaiser used directed consumer advertising to notify consumers of the availability of a new patient–physician secure messaging service. Another example of how consumers have stimulated change is the Internet itself. Beginning about a decade ago, patients began bringing in piles of research from the Internet about their conditions, changing the physician role from being an oracle to someone who helped patients understand what the information means to them. The opportunities for transparency and access to information to change the system are great. Whether patients will learn how to use this information for their own benefit remains to be seen.
Part of leveraging patients to change the system requires understanding patient preferences and the tradeoffs patients make. For example, the rise of retail-based clinics could be interpreted as patients’ willingness to give up the idea of continuity of care with a single physician because they would rather have care be more tailored to their schedules (e.g., open late and in more convenient locations).
Patients can be used as implementers to facilitate spread for those ideas truly in patients’ interests. This capacity needs to be leveraged where appropriate, Wallace said, such as disease management. On the other side of the continuum, provider systems must also become more self-aware and act on opportunities outside of consumers’ view. Different solutions will be necessary for various parts of the health care system, but the ability to both engage and leverage the consumer has been underused. The design of the health care system, research designs, and program designs all must recognize the need to put the patient at the center of health care and allow patients to become participants in and drivers of change.




