
Stretching Across International Borders
In spring 2009, a new type of influenza appeared in Mexico and quickly spread to the United States and around the world. Its cause: a mutated strain of swine flu virus—labeled H1N1 influenza A by scientists. Thousands of people fell seriously ill, and though most recovered, some did not.
The outbreak underscores the message that health threats recognize no political or geographic borders. Indeed, given today’s increasingly interconnected world, new or reemerging diseases are no more than an airplane ride—or even a car ride—away. Moreover, global events, ranging from climate disruption to poverty and violence, threaten public health as well.
In this era of globalization, the United States has a key role to play in maintaining health and mitigating risk. The Institute of Medicine (IOM) examines different aspects of this responsibility. The IOM looks at how the nation can best protect its own residents from global health threats and also at how the nation can help other countries with limited resources to tackle health problems within their own borders.
Meeting the global need for U.S. commitment
In 2008, the IOM—with the support of four federal agencies and five private foundations—formed an independent committee to examine the nation’s current and future role in global health. The committee issued a report in two installments, the first specifically targeting recommendations to government and the second offering recommendations for the public and private sectors as well. The report as a whole revisits the IOM’s 1997 study America’s Vital Interest in Global Health, which argued that a firm commit-
ment by the United States to promote health around the world serves not only the international population, but also the American people.
The U.S. Commitment to Global Health: Recommendations for the New Administration (2008), the first installment of the new report, calls for highlighting health as a pillar of U.S. foreign policy and backing this up with significant funding increases for global health efforts over the next 4 years. It lays out a broad path for how the President and administration can demonstrate their commitment to global health:
-
Expanding and rebalancing the federal government’s aid portfolio, particularly by increasing funding for chronic, noncommunicable diseases, which account for more than half of all deaths in low- and middle-income countries.
-
Creating a White House Interagency Committee on Global Health, composed of heads of major federal departments and agencies involved in global health, and designating a senior administration official as its leader.
-
Improving evaluation in order to determine which interventions are working and which are not.
-
Developing and implementing an expanded research agenda—supporting, in particular, new research targeting health problems specific to poor populations—that could yield new tools, such as a vaccine for malaria, for use in global health programs.
-
Ensuring that health improvements will be sustainable by working with pivotal international groups, such as the World Health Organization; partnering with other national governments; and strengthening local health systems and workforces.
The U.S. Commitment to Global Health: Recommendations for the Public and Private Sectors (2009), the second installment, provides a more detailed action plan that requires the participation of every sector of the U.S. global health enterprise. It calls on U.S.-based commercial entities, foundations, universities, and other nonprofit organizations to join with the government in taking action in five key areas:
-
Scaling up proven interventions for improving health outcomes and reducing poverty, a known contributor to health problems, in low-and middle-income countries. Numerous interventions are available, but many nations lack the infrastructure or resources to take sufficient action on their own.
-
Generating and sharing knowledge that serves the global community. Typically, the United States and other wealthy countries focus their health research on conditions that affect their own people. This situation too often means that the tools to prevent and treat many diseases in resource-limited countries are either inadequate or not fully used because there is insufficient understanding of how best to apply them in such settings.
-
Investing in capacity building with global partners. Many countries face critical health workforce deficits that directly affect efforts at combating disease and death. U.S. institutions should establish long-term partnerships with universities, research centers, and health care systems in resource-limited countries to help them build a cadre of capable local leaders and researchers who can identify effective solutions to health problems that are sustainable in their own countries.
-
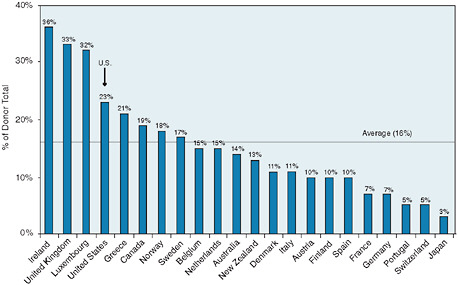
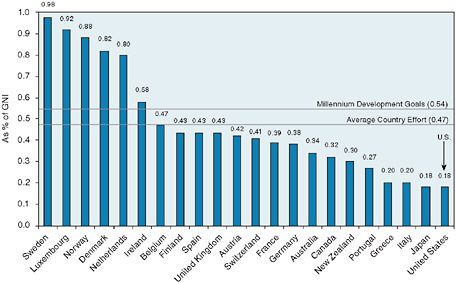
Increasing financial commitments to global health. Although the U.S. government has made record commitments to global health, its overall commitment to overseas development assistance falls below the efforts of other developed countries. The government also should consider novel approaches, such as results-based financing, to delivering aid that is effective.
-
Setting an example by engaging in respectful partnerships. To ensure that countries retain ownership and accountability for the health of their people, the United States should support resource-limited countries in developing results-focused, country-led agreements that rally all development partners around one health plan, one monitoring and evaluation framework, and one review process.
International aid focusing on global health is a longstanding tradition in the United States, and the White House increased its commitments under President George W. Bush. On July 30, 2008, President Bush signed into law a reauthorization of the President’s Emergency Plan for AIDS Relief (PEPFAR), originally launched in 2003, providing $15 billion in relief. The new law expanded funding more than threefold, to $48 billion, to treat not
only AIDS, but also tuberculosis and malaria. The reauthorization eliminated a previous requirement that one-third of all prevention funding must go to abstinence and fidelity programs, as well as other earmarks to allow local implementers to allocate funds based on the needs of at-risk populations. These modifications, along with an increased focus placed on women and girls, were recommended in the 2007 IOM report PEPFAR Implementation: Progress and Promise, a congressionally mandated evaluation of the program.
Yet the reach of global health goes far beyond worldwide disease prevention and international relations. It is an interdisciplinary field that also incorporates economics, epidemiology, and public health, among others. One area that tends to be overlooked is violence, which may include interpersonal and self-directed violence, violence in society, violence in the family, and violence against women and children, among others. Such violence, comprising both suicidal behavior and interpersonal violence, is among the leading causes of death and disability worldwide. In 2000 alone, the latest year for data, violence claimed an estimated 1.6 million lives globally—more than 1.5 times the number of deaths from malaria. The devastating impact of violence also extends far beyond immediate death, resulting in injuries that are often lifelong, hospitalizations, political instability, and stagnation of economic growth for families, communities, and nations. Although it strikes everywhere, violence overwhelmingly and disproportionately affects low- and middle-income countries, which often lack the resources to invest in prevention and to respond to the consequences of violence.

The IOM, together with the nonprofit group Global Violence Prevention Advocacy, convened a workshop to examine how a public health approach might be applied in lessening the pressing dangers. Among their goals, workshop participants—drawn from an array of fields related to health, criminal justice, public policy, and economic development—set out to discuss specific opportunities for the U.S. government and other public and private groups with resources to more effectively support programs aimed at preventing the many forms of violence that occur. Violence Prevention in Low- and Middle-Income Countries: Finding a Place on the Global Agenda: Workshop
Summary (2008) highlights the need for the timely development of an integrated, science-based agenda to support research, clinical practice, program development, policy analysis, and advocacy for violence prevention.
In 2000 alone, the latest year for data, violence claimed an estimated 1.6 million lives globally—more than 1.5 times the number of deaths from malaria.
One central message is that the current state of science in violence prevention reveals progress, promise, and a number of remaining challenges. Most of what is known about effective violence prevention comes from studies in developed countries, but improved collaboration could help developing countries apply these lessons to their own circumstances. Promising, effective interventions are currently being implemented in and by developing countries, but they have not been rigorously evaluated for scaling up to regional and national levels. Both government and private efforts are needed to span this knowledge gap.
Top 10 Causes of Death, Ages 5-44 Years, Both Sexes, 2002
Confronting infectious diseases
In recent decades, most of the emerging infectious disease events in humans have been caused by zoonotic pathogens—those infectious agents that are transmitted from animals to humans. Noteworthy changes in the patterns of human and animal contact in recent years make conditions ripe for global outbreaks of zoonotic diseases, the 2009 swine flu outbreak among them. Some of these diseases, including AIDS, severe acute respiratory syndrome (SARS), and West Nile virus infection, have already caused global health and economic crises. With an estimated billion people crossing international borders every year, the shipment of animals and animal products over great distances to reach their final destinations, and rampant population growth in countries where poverty rates are high and people by necessity live in close proximity to animals, new outbreaks could emerge with devastating health, economic, environmental, agricultural, and sociopolitical results.
The IOM and the National Research Council jointly convened a workshop to examine how well the United States and the world are prepared to deal with the threats of zoonotic diseases over the long term. Achieving Sustainable Global Capacity for Surveillance and Response to Emerging Diseases of Zoonotic Origin: Workshop Summary (2008) outlines what is known about the transmission of zoonotic disease and explores the current global capacity for zoonotic disease surveillance. In particular, the report discusses methods of disease surveillance as a way of detecting outbreaks of diseases in animals, spotting outbreaks of zoonotic disease in humans, and using these data to inform public health responses to outbreaks or perhaps prevent them in the future. It also describes components of a research plan to explore many of the questions that remain about how best to protect humans worldwide from the transfer and spread of diseases from animals.
Changing climatic conditions also have contributed to a shift in the global spread of disease. Climatic change has long been known to influence the appearance and spread of epidemic diseases, but evidence is mounting that Earth’s climate is changing at a faster rate than previously appreciated and that this change likely will be accompanied by more frequent occurrences of extreme weather events, such as droughts and hurricanes. This awareness is leading researchers to view the relationships between climate and disease with a new urgency and from a global perspective.
The IOM explored various aspects of this climate–health link at a workshop convened by its Forum on Microbial Threats. Global Climate
Change and Extreme Weather Events: Understanding the Contributions to Infectious Disease Emergence: Workshop Summary (2008) notes that the projected impacts of climate change and extreme weather events are predominately negative. Impacts are expected to be most severe in low-income countries where the capacity to adapt is weakest, though developed countries also are vulnerable, as was demonstrated in 2003 when tens of thousands of Europeans died as a result of record-setting summer heat waves.
The report discusses some of the scientific questions that must be answered in order to discern—and, ultimately, to predict—the effects of a changing climate on specific infectious diseases, as well as to identify technical means to tackle these issues. For example, it will be critical to develop a greater understanding of the interaction of climate with other major factors, such as the globalization of travel and trade, population growth, urbanization, land-use patterns, and habitat destruction, that play a role in disease emergence and resurgence. Governments also will need to establish long-term monitoring programs to simultaneously track climate and infectious disease dynamics, and to optimize measurement instruments (many of which were designed for other purposes) for use in such programs. In addition, researchers must continue to develop and refine predictive models of climate and infectious disease as the basis for early warning and public health response systems, and governments should encourage more stakeholders to become involved in the operation of such systems.
Assessing treatment of disease
Malaria is a leading cause of death among children in the developing world. Of the more than 1 million people who die of malaria each year, more than 80 percent are young children in sub-Saharan Africa. One promising approach for reducing malaria’s toll is called intermittent preventive treatment, in which all infants, regardless of whether or not they are infected, are given a full therapeutic course of an antimalarial drug—typically sulfadoxine-pyrimethamine—at defined intervals, usually in conjunction with regularly scheduled visits to health clinics. But questions have remained about the method’s effectiveness.
Observed Changes in North American Extreme Events, Assessment of Human Influence for the Observed Changes, and Likelihood That the Changes Will Continue Through the Twenty-first Centurya
|
Phenomenon and Direction of Change |
Where and When These Changes Occurred in Past 50 Years |
Linkage of Human Activity to Observed Changes |
Likelihood of Continued Future Changes in This Century |
|
Warmer and fewer cold days and nights |
Over most land areas, the last 10 years had lower numbers of severe cold snaps than any other 10-year period |
Likely warmer extreme cold days and nights and fewer frostsb |
Very likelyd |
|
Hotter and more frequent hot days and nights |
Over most of North America |
Likely for warmer nightsb |
Very likelyd |
|
More frequent heat waves and warm spells |
Over most land areas, most pronounced over northwestern two-thirds of North America |
Likely for certain aspects, e.g., night-time temperatures; and linkage to record high annual temperatureb |
Very likelyd |
|
More frequent and intense heavy downpours and higher proportion of total rainfall in heavy precipitation events |
Over many areas |
Linked indirectly through increased water vapor, a critical factor for heavy precipitation eventsc |
Very likelyd |
|
Increases in area affected by drought |
No overall average change for North America, but regional changes are evident |
Likely, Southwest USA.c Evidence that 1930s and 1950s droughts were linked to natural patterns of sea surface temperature variability |
Likely in Southwest USA, parts of Mexico, and Carribeand |
|
Phenomenon and Direction of Change |
Where and When These Changes Occurred in Past 50 Years |
Linkage of Human Activity to Observed Changes |
Likelihood of Continued Future Changes in This Century |
|
More intense hurricanes |
Substantial increase in Atlantic since 1970; likely increase in Atlantic since 1950s; increasing tendency in W. Pacific and decreasing tendency in E. Pacific (Mexico West Coast) since 1980e |
Linked indirectly through increasing sea surface temperature, a critical factor for intense hurricanes;e a confident assessment requires further studyc |
Likelyd |
|
aBased on frequently used family of Intergovernmental Panel on Climate Change emission scenarios. bBased on formal attribution studies and expert judgment. cBased on expert judgment. dBased on model projections and expert judgment. eAs measured by the Power Dissipation Index (which combines storm intensity, duration, and frequency). SOURCE: Global Climate Change and Extreme Weather Events: Understanding the Contributions to Infectious Disease Emergence, p. 7. |
|||
At the request of the Bill & Melinda Gates Foundation, which is investing heavily in malaria treatment and prevention worldwide, the IOM convened an expert committee to examine the body of evidence about the technique’s effectiveness. The committee relied heavily on work conducted by the Intermittent Preventive Treatment in Infants Consortium, comprising 17 leading organizations involved in malaria research in Africa, Europe, and the United States. Assessment of the Role of Intermittent Preventive Treatment for Malaria in Infants: Letter Report (2008) concludes that the method yields significant benefits. Some reported data, for example, showed that treated infants experienced approximately 20 to 30 percent fewer clinical malaria episodes than did untreated infants.
Based on such findings, the report concludes that intermittent preventive treatment is worthy of further investment as part of a public health
strategy to decrease morbidity from malaria infections among infants who are at high risk because they reside in malaria-endemic areas. The report also recommends, however, that if public health authorities elect to expand use of the method in sub-Saharan Africa, they should include monitoring efforts during the early stages to further assess their safety, effectiveness, cost effectiveness, acceptability, and sustainability at the community level.
Because malaria kills so many people and is an enormous public health problem, health experts around the world are searching for new ways to fight the disease. While the recent IOM report discusses intermittent preventive treatment, that is only one option among many. In 2004, the IOM released Saving Lives, Buying Time: The Economics of Antimalarial Drugs, which recommended ways to make the new combination malaria treatments—called artemisinin-combination therapies, or ACTs—widely accessible despite their high cost. The report’s central recommendation came to pass in April 2009 with the announcement of a program called Affordable Medicines Facility for Malaria. Funded by international public health organizations and European governments, the program will be piloted in Cambodia and 10 African countries initially, and then evaluated after 2 years to determine its success and viability.
Although it may not claim as many lives each year as malaria, influenza poses an even broader geographic sweep of health challenges. During the early stages of an influenza pandemic, physicians and other public health workers may rely on two antiviral drugs, oseltamivir (sold as Tamiflu®) and zanamivir (sold as Relenza®), to treat illness and slow its spread during the several months it takes to develop a vaccine. But as the emergence of a new strain of flu virus in spring 2009 demonstrated, it is difficult to estimate in advance how severe the next pandemic will be and what mix of treatment and prophylaxis will be optimal.
At the request of the U.S. Department of Health and Human Services (HHS), the IOM examined the nation’s strategies for coping with major new influenza outbreaks. Antivirals for Pandemic Influenza: Guidance on Developing a Distribution and Dispensing Program (2008) concludes that governments at all levels—federal, state, and local—currently lack a coordinated plan to get drugs fairly and efficiently to people who need them. The report calls for government officials to begin a national and public process of creating an ethical framework for allocating antivirals, and for the federal government to appoint a science-based advisory body that can guide decision making during a pandemic.
Prioritized Strategies for Antiviral Drug Use from November 2007 HHS Draft Proposed Guidance
|
Population to Receive Prophylaxis |
Estimated Number of Antiviral Courses Needed |
|
|
Initial pandemic outbreaks overseas and in the United States |
|
6 million |
|
Exposed travelers entering the United States early in a pandemic |
||
|
Persons with pandemic influenza illness (outbreak and post-exposure) |
79 million |
|
|
Health care and emergency services workers |
103 million |
|
|
Outbreak control in closed settings (e.g., nursing homes) |
5 million |
|
|
Immunocompromised and not candidates for vaccine |
2 million |
|
|
Unique and specialized infrastructure workers |
2 million |
|
|
Household contacts of cases The summary of the proposed guidance, dated November 20, 2008, revises the preliminary position on household prophylaxis: “No national recommendation is made at this time for PEP [post-exposure prophylaxis] of household contacts of an influenza case or for workers in sectors other than healthcare and emergency services.” |
88 million |
|
|
Total estimated number of courses for treatment and prophylaxis |
285 million |
|
|
Total excluding household post-exposure prophylaxis |
197 million |
|
|
SOURCE: Antivirals for Pandemic Influenza: Guidance on Developing a Distribution and Dispensing Program, p. 29. |
||
In developing a strategic framework, officials should establish, among other things, a process for prioritizing which groups of people should first receive antiviral medications currently stored in federal and state stockpiles. In most instances, first priority should go to health care workers and emergency personnel who are likely to face repeated viral exposures, followed by other health care providers and emergency responders, and then people in households in which a member has been infected. The prioritization process should be built to have enough flexibility to adjust for the
particular circumstances of an actual outbreak, including how quickly the virus spreads, which population groups it affects most severely, and how readily it responds to drugs.
In most instances, first priority should go to health care workers and emergency personnel who are likely to face repeated viral exposures, followed by other health care providers and emergency responders, and then people in households in which a member has been infected.
In addition to engaging the public in prioritization planning, government officials also should connect with the corporations and other private entities that are building stockpiles of antiviral drugs for their employees. Efforts to establish agreements and understanding between the public and private sectors could lead to collaboration in an actual outbreak and reduce confusion and inefficiencies during a pandemic.
While malaria and influenza remain everyday threats to human health, in the late 20th century the global health community eradicated one of the most devastating diseases ever to plague humanity: smallpox. Today, all known stocks of the disease’s causative agent, variola virus, are stored in two repositories sanctioned by the World Health Organization—in the United States at the federal Centers for Disease Control and Prevention, and in Russia at the State Centre for Research on Virology and Biotechnology. But debate has continued about whether to retain or destroy these stocks of live virus.
In 1999, the Institute of Medicine explored this question, and its report, Assessment of Future Scientific Needs for Live Variola Virus, concluded that preserving live strains of the virus could help researchers in developing medical countermeasures for smallpox. That same year, the World Health Assembly, the decision-making body of the World Health Organization, declared that given the important research remaining, a decision about retaining stocks of the live virus should be deferred until 2010.

To help prepare for this decision, the HHS and the Centers for Disease Control and Prevention requested the IOM review the body of research that has accumulated over the past decade and determine what unmet needs still exist that require the use of live variola virus. Live Variola Virus:
Overview of Essential Versus Useful Scientific Needs for Live Variola Virus
|
Need |
Requires Use of Live Virus |
Does Not Require Live Virus |
|
Essential |
|
|
|
Useful |
|
|
|
SOURCE: Live Variola Virus: Considerations for Continuing Research, p. 4. |
||
Considerations for Continuing Research (2009) finds that developing medical countermeasures against this deadly pathogen remains an essential need because of the potential for an accidental or deliberate release, and that having access to stocks of live variola virus will critically aid researchers in reaching their goals. The report singles out four areas for particular attention: development of improved therapeutics; development of new or improved vaccines; genomic analysis to improve the fundamental understanding of the virus and identify new strategies for therapies; and “discovery research” that can yield fundamental insights about human biology as well as lessons on how to improve smallpox prevention and treatment.














