
To respond to its charge (see Chapter 1), the committee needed a multipronged approach. This chapter describes the committee’s methods.
The committee conducted a systematic review to evaluate the scientific literature on therapies to eliminate or alleviate the symptoms associated with chronic multisymptom illness (CMI). Details on the methods of the review are included below, and the results of the review are discussed in Chapter 4.
Many people who have CMI also have other unexplained conditions with shared symptoms (such as chronic fatigue syndrome [CFS], fibromyalgia, and irritable bowel syndrome) and may have comorbid conditions (such as depression and anxiety). As summarized in Chapter 5, the committee reviewed treatments for the related and comorbid conditions in an attempt to identify treatments potentially beneficial for people who have CMI. For that review, the committee relied on current evidence-based clinical practice guidelines from government and scientific organizations and existing systematic reviews, rather than conduct a de novo evaluation of the primary literature.
Managing patients who have CMI involves more than administering a therapy. It requires a broader view of treatment. To explore other aspects of care, the committee drew on multiple sources (such as the scientific literature, government reports, care programs used by organizations, and testimony from veterans and their families) so that it could offer recommendations to the Department of Veterans Affairs (VA) aimed at improving its model of care for veterans who have CMI, educating VA clinicians to improve their knowledge on caring for these patients, and improving communication between clinicians and the patients (see Chapter 6 and 7).
SYSTEMATIC REVIEW OF TREATMENTS FOR
CHRONIC MULTISYMPTOM ILLNESS
The committee conducted a systematic review of treatments for CMI, following guidance in Finding What Works in Health Care: Standards for Systematic Reviews (IOM, 2011) and the Cochrane Handbook for Systematic Reviews of Interventions (Higgins and Green, 2011).
In January 2012, a number of reference databases—PubMed, Embase, The Cochrane Library (Cochrane Central Register of Controlled Trials, Health Technology Assessment, Cochrane Database of Systematic Reviews, Database of Abstracts of Reviews of Effectiveness [DARE]), American College of Physicians (ACP) Journal Club, PsycINFO, and Web of Science—were searched by using terms relevant to treatment for CMI.1 An additional database, Cumulative Index to Nursing and Allied Health Literature (CINAHL), was searched in April 2012. The search was limited to literature published in 2000–2012 to identify evidence that had become available since a previous Institute of Medicine report, Gulf War Veterans: Treating Symptoms and Syndromes (IOM, 2001) was released. Searches were limited to adult populations. Additional potentially eligible studies were identified by hand searching of reference lists of relevant review articles.
Gray-literature sources were searched in April 2012 by using the approach outlined in Grey Matters: A Practical Search Tool for Evidence-Based Medicine (CADTH, 2011). Sources searched included the Food and Drug Administration, VA, Health Canada, the Australian Government Department of Health and Aging, the European Commission on Public Health, the System for Information on Grey Literature in Europe, Veterans Affairs Canada, and the Agency for Healthcare Research and Quality (AHRQ). Databases of clinical trials (Congressionally Directed Medical Research Programs, DeployMed ResearchLINK, BioMed Central current controlled trials, International Federation of Pharmaceutical Manufacturersand Associations clinical-trials portal, Thomson CenterWatch Clinical Trials Listing Service, UK Clinical Research Network Study Portfolio, US National Institutes of Health’s ClinicalTrials.gov, and World Health Organization International Clinical Trials Registry Platform Search Portal) and clinical practice guidelines (for example, the VA–Department of Defense [VA–DOD] Clinical Practice Guidelines website and the National Guideline Clearing House) were also included in the search. Search terms included CMI, Gulf War syndrome, Gulf War illness, unexplained illness, undiagnosed illnesses, undiagnosed symptoms, medically unexplained symptoms, somatoform disorder, fatigue, pain, concentration, memory, headaches, and
_____________
1The strategy used to search PubMed can be found in the public-access file for this study. For information on accessing the public-access file, visit http://www8.nationalacademies.org/cp/projectview.aspx?key=49452.
gastrointestinal symptoms. In addition to consideration for the systematic review, the search identified relevant resources for use in other parts of the report.
Selection of Evidence
Two reviewers independently screened the search results at the title and abstract level to exclude studies that
• Contained no original data (for example, commentaries and narrative reviews; systematic reviews and meta-analyses were not excluded).
• Described only a case or case series.
• Did not assess medically unexplained symptoms.
• Described only one symptom in the general population (studies of one symptom in military or veteran populations were not excluded).
• Did not describe the results of a treatment or intervention.
• Described only defined syndromes (such as CFS, fibromyalgia, and functional gastrointestinal disorders).
• Did not include humans.
• Did not include an adult population.
• Were published before 2000.
No limits based on study design were used. References that the two reviewers agreed should be excluded were removed from further consideration. References that the two reviewers disagreed about remained for full-text screening. Non-English-language citations were translated, where necessary, to determine eligibility.
After the title and abstract screen, two reviewers independently screened the references remaining by using the full-text articles. In addition to the eligibility criteria applied during the title and abstract screen, they excluded citations at this level that were only meeting abstracts, that were systematic reviews that had been updated, or that described only study protocols but had no results. Disagreements between the reviewers on whether an article should be excluded were resolved by consulting a third reviewer.2
Summary of the Literature Search and Study Selection Process
Searches identified 6,541 unique references. After exclusion at the abstract and full-text levels according to the criteria described above,
_____________
2References excluded at the full-text level and the reasons for their exclusion can be found in the public-access file for this study; see http://www8.nationalacademies.org/cp/projectview.aspx?key=49452.
47 studies remained for committee evaluation. Figure 3-1 summarizes the search process.
Data Abstraction and Assessment
Data were abstracted from the eligible studies into tables describing study design, population, intervention, outcomes, and risk of bias. Risk of bias was assessed by using study-design–specific tools: the Cochrane Risk of Bias Tool was used to evaluate controlled trials (Higgins and Green, 2011), and Assessment of Multiple Systematic Reviews (AMSTAR) was used to evaluate systematic reviews (Shea et al., 2007). Studies were grouped by type of intervention, and each group of studies was later evaluated by two committee members.
Chapter 4 summarizes the evidence on each type of intervention. The body of evidence was evaluated for each intervention according to the strength-of-evidence guidance developed by AHRQ (Owens et al., 2010). The AHRQ grading scheme is presented in Table 3-1. To make the determination, the committee examined risk of bias, consistency, directness, and precision of the body of evidence for each intervention.
TREATMENTS FOR COMORBID CONDITIONS
WITH SHARED SYMPTOMS
To augment the systematic review of treatments for CMI, the committee also reviewed treatments for other conditions that are closely related to it (see Chapter 5). The committee first identified conditions that are commonly comorbid with CMI or exhibit symptoms that are similar to those seen in people who have CMI. The committee believes that symptoms shared by CMI and the other conditions may respond similarly to approaches to symptom management.
Twelve commonly comorbid conditions or conditions with shared symptoms were identified: fibromyalgia, chronic pain, CFS, somatic symptom disorders, sleep disorders, functional gastrointestinal disorders, depression, anxiety, posttraumatic stress disorder, traumatic brain injury, substance use and addictive disorders, and self-harm. For those conditions, the committee relied on existing systematic reviews and evidence-based clinical practice guidelines to identify the most effective treatment and management techniques. Systematic reviews were collected in March 2012 by searches of several bibliographic databases (PubMed, EMBASE, PsycINFO, Evidence-based Medicine Reviews files in Ovid: Cochrane Database of Systematic Reviews, ACP Journal Club, and DARE). Evidence-based clinical practice guidelines were identified by searches of the National Guideline Clearinghouse, which contains systematically developed evidence-based
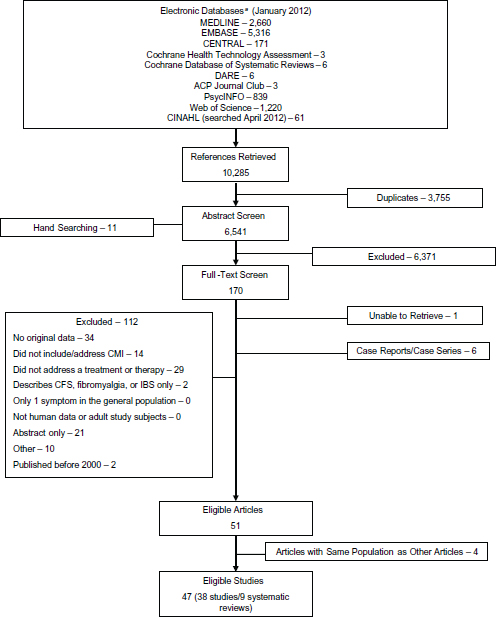
FIGURE 3-1 Summary of search and review process.
aMEDLINE accessed via PubMed.
NOTE: ACP = American College of Physicians; CENTRAL = Cochrane Central Register of Controlled Trials; CFS = chronic fatigue syndrome; CINAHL = Cumulative Index to Nursing and –Allied Health Literature; DARE = Database of Abstracts of Reviews of Effectiveness; EMBASE = Excerpta Medica database; IBS = irritable bowel syndrome. 3-1
TABLE 3-1 AHRQ’s Strength-of-Evidence Grades and Definitions
| Grade | Definition |
| High | High confidence that the evidence reflects the true effect. Further research is very unlikely to change the confidence in the estimate of effect. |
| Moderate | Moderate confidence that the evidence reflects the true effect. Further research may change the confidence in the estimate of effect and may change the estimate. |
| Low | Low confidence that the evidence reflects the true effect. Further research is likely to change the confidence in the estimate of effect and is likely to change the estimate. |
| Insufficient | Evidence either is unavailable or does not permit a conclusion. |
SOURCE: Reprinted from Owens et al., 2010. Copyright 2010, with permission from Elsevier.
guidelines. Chapter 5 summarizes the existing evidence on conditions that are comorbid and have shared symptoms with CMI.
ADDITIONAL SOURCES OF INFORMATION
As stated above, the committee reviewed several sources of information in addition to the scientific and medical literature to accomplish its task. Three meetings open to the public were held to hear from invited speakers. Presentation topics included general information on CMI, current practices and capabilities in the Veterans Health Administration, current understanding of the underlying mechanism of CMI, treatments for CMI, and how health information technology is being used in managing chronic conditions. Members of the public were given the opportunity to share information and experiences with the committee at the public meetings. Written materials submitted by the public also were considered by the committee.
To understand better the experiences of veterans who have CMI, the committee commissioned an analysis of social media. The analysis, conducted by ConsumerSphere, collected social media discussion data of veterans and their families to describe experiences with CMI in the VA health care system. The program used Web-scraping technology that collects all text, including conversations and discussion, on social media, for example, blogs and microblogs (such as Twitter), message boards, forums, and social networks (such as Facebook). In some cases, Google searches also were conducted. All the information in question is in the public domain. Data were collected for a 12-month period. More than 275,000 conversations, messages, and threads were analyzed. The collected data were analyzed with text analytics programs that used natural-language processing, which allowed an assessment of trends and patterns, connections,
and networks; and relevance and associative relationships among the key words. The results, used to inform the committee about veterans’ perception of the patient–clinician relationship (Chapter 6) and their satisfaction with VHA care (Chapter 7), are a combination of quantitative and qualitative information.
CURRENT RESEARCH ON CHRONIC MULTISYMPTOM ILLNESS
As part of its information gathering, the committee searched clinical-trial databases (Congressionally Directed Medical Research Programs, DeployMed ResearchLINK, BioMed Central current controlled trials, International Federation of Pharmaceutical Manufacturers and Associations clinical-trials portal, Thomson CenterWatch Clinical Trials Listing Service, UK Clinical Research Network Study Portfolio, US National Institutes of Health’s ClinicalTrials.gov, and World Health Organization International Clinical Trials Registry Platform Search Portal) and identified a number of current research projects on CMI treatments. The research is funded largely by VA and DOD. Research projects on CMI treatment deal with, for example, the use of drugs (such as naltrexone, dextromethorphan, and mifepristone), supplements (such as coenzyme Q10 and Sentra), complementary medicine and alternative medicine therapies (such as acupuncture), exercise, mind–body programs, environmental medicine (that is, being in an environment with clear air, eating organic food, and drinking filtered water), and telemedicine. Other research projects are studying the mechanisms of CMI. Because the current research has not yet been completed or results were not available in the published literature, the committee was not able to evaluate it for inclusion in the present report.
CADTH (Canadian Agency for Drugs and Technologies in Health). 2011. Grey Matters: A Practical Search Tool for Evidence-Based Medicine.
Higgins, J. P. T., and S. Green, eds. 2011. Cochrane Handbook for Systematic Reviews of Interventions. Version 5.1.0: The Cochrane Collaboration.
IOM (Institute of Medicine). 2001. Gulf War Veterans: Treating Symptoms and Syndromes, The Compass Series. Washington, DC: National Academy Press.
IOM. 2011. Finding What Works in Health Care: Standards for Systematic Reviews. Washington, DC: The National Academies Press.
Owens, D. K., K. N. Lohr, D. Atkins, J. R. Treadwell, J. T. Reston, E. B. Bass, S. Chang, and M. Helfand. 2010. AHRQ series paper 5: Grading the strength of a body of evidence when comparing medical interventions: Agency for Healthcare Research and Quality and the Effective Health-Care Program. Journal of Clinical Epidemiology 63(5):513-523.
Shea, B. J., J. M. Grimshaw, G. A. Wells, M. Boers, N. Andersson, C. Hamel, A. C. Porter, P. Tugwell, D. Moher, and L. M. Bouter. 2007. Development of AMSTAR: A measurement tool to assess the methodological quality of systematic reviews. BMC Medical Research Methodology 7(10): doi:10.1186/1471-2288-7-10.








