
1
The Artificial Heart Program: Current Status and History
BY THE LATE 1990s, patients with heart failure may be able to receive a fully implantable device to assist their weakened hearts. A small battery pack will be the only visible evidence of the technology, in contrast to the large console needed to power earlier models of these devices. Five to ten years after assist devices are perfected, a fully implantable total artificial heart (TAH)—a device that replaces the natural heart instead of only assisting it—may be technologically possible.
As soon as 1992, the first patient will receive a fully implantable, long-term ventricular assist device (VAD). The implant will begin a clinical trial of a VAD developed by the Novacor Division of Baxter Healthcare Corporation and is the result of a major effort by the artificial heart program of the National Heart, Lung, and Blood Institute (NHLBI). In the trial, 20 patients will receive the device over a 2-year period, 10 at St. Louis University and 10 at the University of Pittsburgh; each patient will be followed for up to 2 years, and extensive data analysis will be performed. Formal reports of the trial's outcome thus will be available in the latter half of the 1990s.
The longest use of a temporary Novacor VAD (similar but externally powered) in either animals or human beings has been about one year, but the cumulative experience since the first human use in 1984 suggests that the forthcoming trial of the fully implanted model will yield positive results in some patients. Because the two technologies have similar components and face similar problems, the Novacor trial results will have considerable relevance not only for VAD development but also for the future of TAHs. Nevertheless, TAHs are very different devices; replacing a natural heart presents many more challenges than does supporting left ventricular function.
At present, four TAH developers are just beyond the mid-point of NHLBI contracts for continuing R&D. If NHLBI funding continues, the next phase of extensive device readiness testing might require up to five years; this would be followed by another five or more years of clinical trials. TAHs are not likely to be a candidate for wide use until at least 2005.
This report of an Institute of Medicine (IOM) study is primarily intended to help NHLBI determine the extent of its support of the next step of TAH development after the current contracts end in September 1993. The report also considers the need to continue developing additional VAD models and examines issues related to both types of devices, such as appropriateness of technology use and access by patients to this technology. Finally, the report suggests several methods that can assist NHLBI in allocating resources among R&D programs and examines related R&D policy issues. (Temporary-use devices are not considered, except as their experience provides a basis for projecting the performance of long-term devices.)
END-STAGE HEART DISEASE
Consideration of the future role of TAHs and VADs—referred to collectively as mechanical circulatory support systems (MCSSs)—is helped by a basic understanding of the heart's functioning. As Figure 1.1 illustrates, the heart is a double pump. Oxygenated blood from the lungs flows into the left atrium and from there into the left ventricle. The left ventricle pumps the blood via the aorta into arteries throughout the body. After oxygen has been removed in organs and capillaries, the blood flows through veins back to the heart's right atrium and then to the right ventricle. This chamber sends the venous blood to the lungs to be oxygenated, completing a pumping cycle that normally occurs 70 to 90 times per minute.
Because considerably more pumping force is needed to move arterial blood throughout the body than to move venous blood through the lungs, the left ventricle's muscle strength is greater than the right ventricle 's and it is also more likely to fail than is the right ventricle. Heart failure is identified as left-sided, right-sided, or both (biventricular); end-stage heart disease occurs when one ventricle (or both) is unable to perform the necessary pumping function. As the name indicates, the typical case of end-stage heart disease becomes steadily more severe, until death occurs.
End-stage heart disease may result from a variety of cardiovascular causes; “heart failure”—sometimes called congestive heart failure—is, technically speaking, not itself a disease but a condition that is caused by many different disease processes. The most common causes of end-stage heart disease and heart failure are hypertension and coronary atherosclerosis (also called coronary artery disease or coronary heart disease, a constriction of the arteries that convey blood to the heart muscle itself). Viral
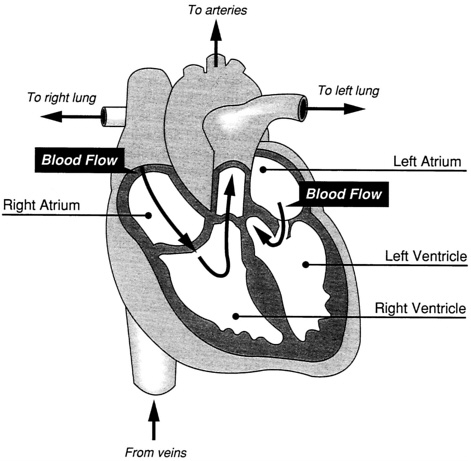
FIGURE 1.1 A simplified drawing of the heart.
infections of the heart and idiopathic cardiomyopathy are other major causes of heart failure. As discussed further in Chapter 4, these diseases of the heart result in most of the 700,000 cardiac deaths that occur in the United States each year. A substantial number of these deaths might be postponed by MCSS use; perhaps half of them, however, occur suddenly and without warning as a result of acute myocardial infarction or a sudden fatal rhythm disturbance of the heart.
The interest in long-term MCSSs is a response to the current limitations on cardiovascular science's ability to prevent or cure end-stage heart disease. The alteration of risk factors for atherosclerosis (e.g., treatment of high blood cholesterol levels and of hypertension, dietary alterations, cessation of smoking) may ultimately reduce the number of patients with end-stage heart disease resulting from coronary artery disease. Patients who already have coronary artery disease may have the natural history of their disease altered, at least temporarily, by coronary artery bypass surgery,
percutaneous transluminal angioplasty, or other similar techniques that are currently the focus of clinical practice and research. Patients with cardiomyopathy or already established heart failure may achieve symptomatic improvement and some prolongation of life with medical therapy, but currently such therapy is palliative at best. Research to further elucidate the cellular mechanisms of heart failure (Francis and Cohn, 1990) may ultimately lead to effective therapy to halt or reverse the progression of disease, but this is not yet possible.
For many heart failure patients, therefore, the treatment of choice is heart transplantation, which is currently achieving five-year survival rates of about 70 percent (Kriett and Kaye, 1990). However, the supply of potential donor hearts is severely restricted. In 1990, 2,085 heart transplants were performed in the United States, up 23 percent from the volume in 1989 (UNOS, 1991). Although the number of donor hearts may continue to increase slightly, there are also a number of factors working against growth in the availability of donor organs generally (IOM, 1991). For the large number of heart failure patients who are unable to receive a transplant, either because of limited donor availability or because they do not meet transplant criteria, the only current alternative is drug treatment. Annual mortality rates of patients receiving conventional medical treatment range from 15 to 50 percent, depending on the severity and rate of progression of the underlying disease.
VADs and TAHs must, therefore, be evaluated as an alternative treatment for end-stage disease within a framework that acknowledges the limitations of heart transplantation and other conventional medical and surgical forms of treatment. Research may eventually lead to successful drug therapy that prevents heart failure, but hundreds of thousands of heart disease patients face serious risk of death until that becomes possible. Any technology such as MCSSs that offers these patients the promise of prolonged functional life thus warrants careful consideration.
HOW LONG-TERM IMPLANT ABLE DEVICES COULD HELP
Mechanical circulatory support devices are being developed either to assist or to replace a failing heart on a long-term basis, with the expectation that the patient will resume a relatively normal, productive life. Such devices were under development before the artificial heart program's inception in the 1960s (Norman, 1984).
Ventricular Assist Devices
A ventricular assist device may be implanted in the upper abdomen, chest, or elsewhere (see Figure 1.2). Long-term VADs will normally be
used to assist the left ventricle, connected by large tubes (cannulas) to it and to the aorta. Each pumping stroke of the VAD is coordinated with the left ventricle's contraction, so as to optimize the functioning of both the device and the natural heart.
Inside the VAD's rigid casing, an electrically powered mechanism squeezes a plastic blood sac between two plates; the direction of blood flow is controlled by a pair of valves, the same types used when a natural heart valve must be replaced (e.g., valves from pigs' hearts or ones made of metal and plastic). Electric power is transmitted through the skin in a transformer-like arrangement; in Novacor's design, one of a pair of coils is permanently implanted below the skin and the other is strapped around the waist. An internal rechargeable battery provides power for 20 to 30 minutes, for emergency use or during bathing; external rechargeable batteries
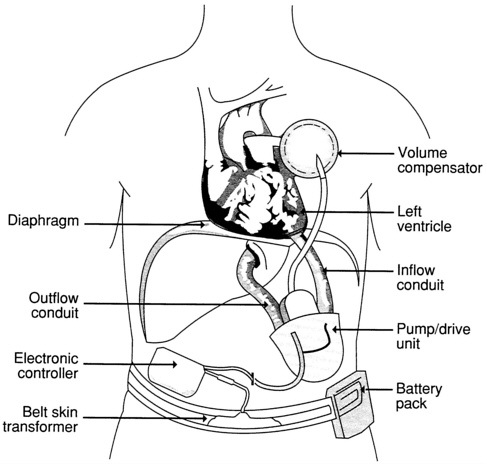
FIGURE 1.2 The Novacor fully implantable ventricular assist device.
are carried on a belt. The external batteries provide power for six to eight hours, so the patient must change to fully charged ones several times per day. A volume compensator or compliance chamber is implanted to accommodate the air displaced by each filling stroke of the pump.
Total Artificial Hearts
A total artificial heart is, in basic design and operation, similar to a VAD, with one power source driving two pumping chambers that perform the ventricles' functions (see Figure 1.3). In the models currently under development, top portions of the natural heart's atria are left in place when the heart's larger components are removed, to facilitate suturing the TAH into position. In models in which the TAH's pumping speed is synchro
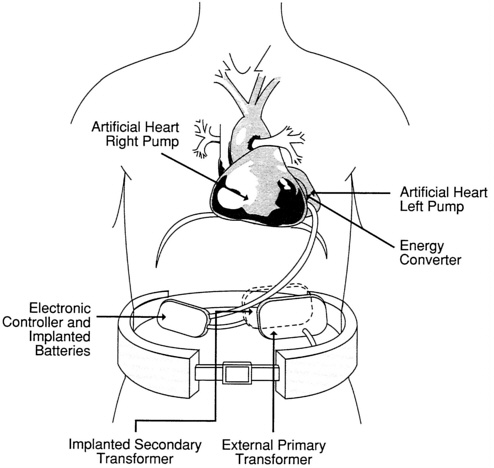
FIGURE 1.3 A fully implantable total artificial heart.
nized to physiological need, those portions of the atria provide the natural electric stimuli so the TAH's speed can increase during exercise and slow during rest.
Depending on when in the patient's disease course a long-term MCSS could be implanted, a TAH may or may not be necessary; as discussed in Chapter 4, further investigation is needed to establish these clinical considerations in detail. Some researchers believe that most patients' needs could be satisfied by a VAD assisting the left ventricle, particularly if it is implanted before serious right heart failure and damage to other organ systems has occurred. Others believe that, regardless of when the implant procedure occurs, a TAH will be needed by a substantial number of end-stage heart disease patients. (In contrast to temporary-use external VADs, a pair of which can be used for biventricular support, developers currently plan to implant only one long-term VAD.)
Temporary Circulatory Support
The current stage of development of long-term fully implantable devices has been made possible by more than 12 years of investigational use of both VADs and TAHs as a temporary support for three classes of patients: those who are awaiting a donor organ for transplant; those who cannot be removed from a heart-lung machine after open-heart surgery but have an anticipated opportunity for recovery in the short term; and those whose hearts need time and rest to recover function after a myocardial infarction. Hundreds of patients have regained satisfactory cardiac function as a result of temporary MCSS use.
Many forms of temporary VADs have been used. Most have been powered pneumatically by an external pump; in several models the VAD itself is external to the body, with blood cannulas running through the chest wall. A single temporary VAD may assist either of the ventricles, or two VADs or a TAH may be used; the availability of a particular type of device sometimes determines this. Even the Jarvik-7 TAH, used for four U.S. and one Swedish long-term implantations in the mid-1980s, has been employed more than a hundred times worldwide as a temporary device.
THE ARTIFICIAL HEART PROGRAM
The NHLBI mission is to “provide leadership for a national research program in diseases of the heart, blood vessels, lungs, and blood and in the uses of blood and the management of blood resources to improve the health of the nation” (NHLBI, 1990). This responsibility is fulfilled by means of 23 program areas in 3 areas of responsibility, 11 of them pertaining to the cardiovascular system (see Table 1.1).
TABLE 1.1 National Heart, Lung, and Blood Institute Program Areas
As with other components of the National Institutes of Health (NIH), the principal mechanism for achieving NHLBI's overall mission is the funding of extramural research through investigator-initiated, nontargeted (“R01”) grants. Most of the institutes that make up NIH do not fund later developmental stages of medical technologies, focusing instead on fundamental or basic research.
The NHLBI artificial heart program is, however, a notable exception to this generalization. Historically, the funding mechanism for R &D with MCSSs has been targeted contracts, issued following requests for proposals.
From the first appropriation of funds in 1964, one of the program 's major goals has been to produce, through focused development, devices for long-term clinical use (see Appendix B for a chronology of the program's activities and others related to it).
Over the years, the artificial heart program has been one of the more closely studied of all NIH activities. Table 1.2 lists the reports previously issued, all by groups under NHLBI's direct auspices.
The artificial heart program now supports six R&D projects through the contract mechanism, with the goals of assessing the Novacor fully implantable VAD and developing other electrically powered, implantable VADs and total artificial hearts. Figure 1.4 shows the projected timetables of these projects as well as of two R01 grants for thermal power development.
Figure 1.5 shows the artificial heart program's historical expenditures, including estimates for the 1990-1991 fiscal year. In addition to the 2 thermal power grants, 29 other grants (including 8 in the category of Small Business Innovation Research awards to small industrial firms) were active as of August 1990 (NHLBI, 1990). This research addresses such areas as cardiac assistance using skeletal-muscle power, specialized MCSSs for pediatric use, and studies of the immune system's response to blood pump implantation.
TABLE 1.2 Previous Evaluations of the NHLBI Mechanical Circulatory Support Program
|
1969 |
Cardiac Replacement: Medical, Ethical, Psychological, and Economic Implications; Ad Hoc Task Force on Cardiac Replacement |
|
1973 |
The Totally Implantable Artificial Heart: Legal, Social, Ethical, Medical, Economic, Psychological Implications; Artificial Heart Assessment Panel |
|
1977 |
Mechanically Assisted Circulation: The Status of the NHLBI Program and Recommendations for the Future; Report of the Cardiology Advisory Committee |
|
1980 |
Mechanically Assisted Circulation: Report of the NHLBI Advisory Council Working Group on Circulatory Assistance and the Artificial Heart |
|
1981 |
Report of the Artificial Heart Working Group |
|
1985 |
Artificial Heart and Assist Devices: Directions, Needs, Costs, Societal and Ethical Issues; Report of the Working Group on Mechanical Circulatory Support of the NHLBI |
|
SOURCE: NHLBI (1990). |
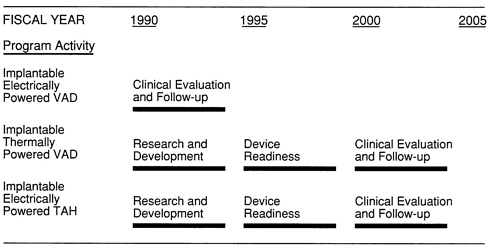
FIGURE 1.4 Estimated timetable for the NHLBI artificial heart program. SOURCE: NHLBI (1990).
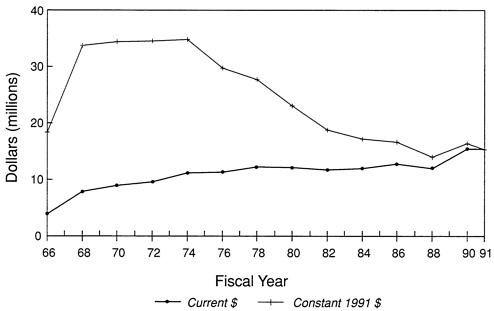
FIGURE 1.5 Total annual expenditures of the NHLBI artificial heart program. SOURCE: NHLBI (1990) (constant dollar adjustments based on U.S. Department of Commerce Biomedical Research and Development Price Index; $4.543 million expended in 1976 transitional quarter not shown).
THE INSTITUTE OF MEDICINE STUDY
This report of a study by the IOM had its origins in a 1988 decision by the director of NHLBI to cancel the four current contracts for TAH development; that decision was later rescinded. Appendix A describes the history and methods of this study in more detail; it also provides details about the preceding planning study that culminated in the 1989 IOM report The Artificial Heart Program of NHLBI: Plan for Evaluation (Washington, D.C.: National Academy Press, 1989).
In the 1989 report, the IOM planning committee formulated nine questions to be addressed in this study, as listed in Table 1.3. These questions form the basis for the many topics discussed in the chapters of this report as indicated in Table 1.3. The report's scope is, moreover, broader than the nine questions, including consideration of several issues of R&D policy and decision making.
TABLE 1.3 Nine Questions Identified by the Institute of Medicine Planning Study for the Main Evaluation and Chapters Where Mainly Considered in This Report
The committee report will also examine methods to enhance communication and cooperation among agencies and others involved in MCSS research in the United States and abroad. (Chapter 9) |
|
SOURCE: Institute of Medicine. 1989. The Artificial Heart Program of NHLBI: Plan for Evaluation. Washington, D.C.: National Academy Press. |
REFERENCES
Francis, J. M., and J. N. Cohn. 1990. Heart failure: Mechanisms of cardiac and vascular dysfunction and the rationale for pharmacologic intervention. Federation of American Societies of Experimental Biology Journal 4:3068-3075.
IOM (Institute of Medicine). 1991. Kidney Failure and the Federal Government. R. A. Rettig and N. G. Levinsky, eds. Washington, D.C.: National Academy Press.
Kriett, J. M., and M. P. Kaye. 1990. The Registry of the International Society for Heart Transplantation: Seventh official report—1990. Journal of Heart Transplantation 9:323-330.
NHLBI (National Heart, Lung, and Blood Institute). 1990. Information provided by NHLBI to IOM.
Norman, J. C. 1984. The Hastings file: A search for solutions. Eighth Annual Hastings Lecture, Annual NHLBI Contractors' Meeting, Rockville, Md. (unpublished).
UNOS (United Network for Organ Sharing). 1991. UNOS Update 7(May):2.











