
Since 1993, a great deal of attention has been focused on policy, practice, and program initiatives aimed at improving both the delivery of child welfare services and the outcomes for children who come in contact with the public child welfare system—the system that implements, funds, or arranges for many of the programs and services provided when child abuse and neglect is suspected or has actually occurred. As described by Sanders (2012) at a workshop held for this study and elucidated by the discussion of research needs in Chapter 6, there is a need for further study of systemic factors that impact the response to child abuse and neglect. In keeping with the committee’s statement of task, this chapter considers system-level issues and legislative, practice, and policy reforms as context for the discussion of interventions and evidence-based practices and of their implementation and dissemination in the following chapter. An understanding of these issues can illuminate what happens to children after their risk for child abuse and neglect has been determined, including dispositions and outcomes for children and families, as well as how the system that serves them functions. The chapter begins with an overview of the child welfare system. Following this overview, examined in turn are major policy shifts in child welfare since the 1993 National Research Council (NRC) report was issued, research on key policy and practice reforms, and issues that remain to be addressed. The final section presents conclusions.
OVERVIEW OF THE CHILD WELFARE SYSTEM
Public child welfare agencies provide four main sets of services—child protection investigation, family-centered services and supports, foster care, and adoption. Child welfare agencies need to have some availability 24 hours a day, 7 days a week, to respond to child abuse and neglect reports. They are also expected to meet the needs of diverse populations that come to their attention, despite the families’ different histories, needs, resources, cultures, and expectations (McCroskey and Meezan, 1998).
For situations involving child abuse and neglect, children come into contact with the designated state or local (county-based) child welfare agency when a call is made to report child abuse and neglect, and the child protective services agency decides whether to accept the report and investigate it, and then decides on a course of action related to the outcome of that investigation.
Children found to be abused or neglected may remain in their own home, but those assessed as not being safe in their own home are placed in out-of-home care. Initially, such care is almost always considered to be temporary, providing an opportunity for change in the behavior, social supports, and living environment of the parents and/or the children’s behavior or health status such that is safe to reunify the children with their families. According to data from the 2007-2008 round of Child and Family Service Reviews, which cover 32 states, reasons for a child welfare agency’s opening a case were neglect (37 percent), parental substance abuse (15 percent), physical abuse (13 percent), child’s behavior (7 percent), other (5 percent), domestic violence (4 percent), sexual abuse (4 percent), juvenile justice system (4 percent), abandonment (3 percent), medical neglect (3 percent), health of parent (3 percent), health of child (2 percent), emotional maltreatment (1 percent), and substance abuse of the child (0.4 percent) (ACF, 2012b) (see Figure 5-1). Figure 5-2 depicts a child’s journey through the child welfare system, while Box 5-1 describes the child welfare system for American Indian children.
Scope of Child Welfare Placement
Each year, more than 3 million referrals for child abuse and neglect are received (3.4 million in 2011) that involve around 6 million individual children (6.2 million in 2011) (ACF, 2012c). In 1998, 560,000 children were in foster care (ACF, 2000). By September 30, 2011, the number of children in foster care had declined to 400,540 (ACF, 2012a). Approximately 3 of 5 referrals to child protective services agencies are screened in for investigation or assessment, and from 1 in 4 to 1 in 5 (25.2 percent in 2007, 20.0 percent in 2011) of these investigations lead to a finding that
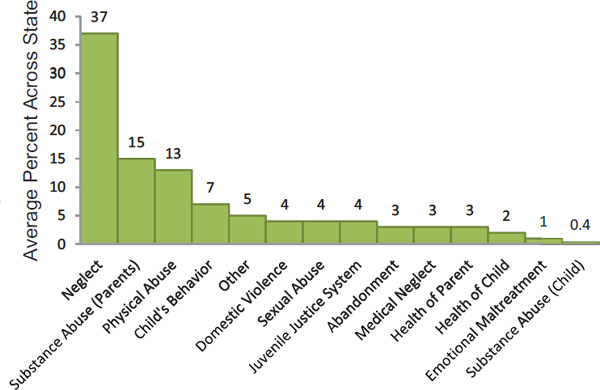
FIGURE 5-1 Case-level data: Primary reason for case opening in 32 states.
SOURCE: ACF, 2012b.
at least one child was a victim of child abuse or neglect, resulting in an estimated number of 794,000 unique child victims in 2007 and 681,000 in 2011 (ACF, 2007, 2012c). Neglect is by far the major type of maltreatment, with more than four-fifths (78.5 percent) of victims being neglected in 2011, while 17.6 percent were physically abused and 9.1 percent were sexually abused (ACF, 2012c).
Although the public perception may be that most substantiated child abuse and neglect reports result in placement of the child in out-of-home care (and perhaps siblings as well, who may or may not have been abused), this is not in fact the case. The number of child victims (and child nonvictims) placed in foster care represents a relatively small percentage of substantiated reports and can best be estimated from the National Survey of Child and Adolescent Well-Being (NSCAW). In the first NSCAW cohort, 82.3 percent of the children remained in their home after investigation (Horwitz et al., 2011) (compared with 79.3 percent based on federal data in 2007 [ACF, 2007]).
Whether any given abused or neglected child is placed in foster care varies substantially. Children under 1 year old are most likely to be placed (ACF, 2012a). Among black children in this age group, the risk of placement is particularly high. Once children are in foster care, placement trajectories
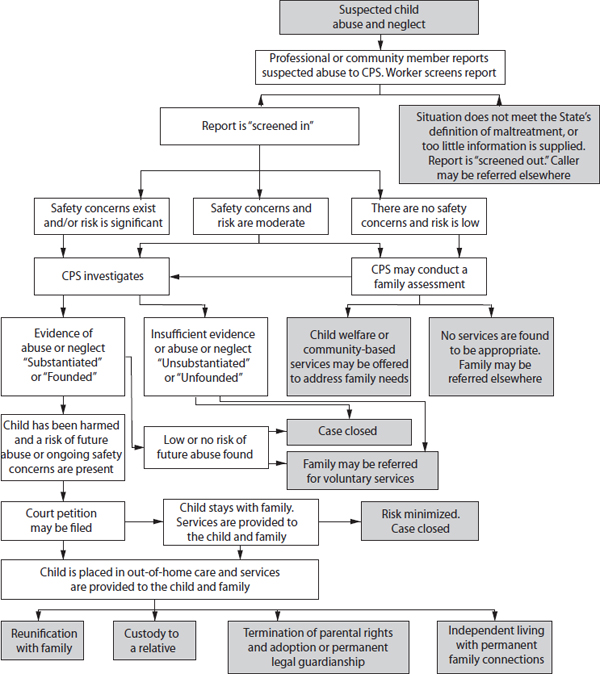
FIGURE 5-2 A child’s journey through the child welfare system.
SOURCE: CWIG, 2013b, p. 9.
vary considerably. Although group and other forms of congregate care have been linked to negative developmental sequelae (Barth, 2005; Berger et al., 2009), 22 percent of all children and 48 percent of all teenagers are placed in some type of group facility upon admission to out-of-home care.
Caregiver changes, which also are associated with negative developmental sequelae (Aarons et al., 2010; Barth et al., 2007; Newton et al., 2000), affect more than half of all children who are placed, with roughly 30 percent of foster children experiencing three or more placements (Landsverk
BOX 5-1
The Child Welfare System for American Indian Children
A child abuse and neglect report relating to an American Indian child may be investigated by the child’s tribe, the Bureau of Indian Affairs, or a state or county agency (Cross, 2012; see also CWIG, 2012b). Child abuse and neglect reports may also be investigated by multiple actors, with tribes being involved in 65 percent of investigations (23 percent as sole investigators), states in 42 percent, counties in 21 percent, the Bureau of Indian Affairs in 19 percent, and a consortium of tribes in 9 percent (Earle, 2000).
The aim of the Indian Child Welfare Act (ICWA),* which was passed in 1978, is to preserve tribal authority over decisions to place American Indian children in out-of-home care. According to the ICWA, tribes with active courts maintain exclusive jurisdiction for American Indian children residing on the reservation, and states and tribes share jurisdiction for children who do not live on reservations but are members of federally recognized tribes or are eligible for tribal membership with a biological parent who is a tribal member. State courts conducting involuntary child welfare proceedings concerning children subject to the ICWA must notify the appropriate tribe, which has the right to intervene in the case. The ICWA requires that American Indian children placed in foster care be placed close to home, with preference for placement with a member of the child’s extended family; a foster home licensed, approved, or specified by the tribe; an American Indian foster home licensed or approved by a nontribal authority; or an institution approved by the tribe. American Indian children placed for adoption should be placed with a member of the child’s extended family, a member of the child’s tribe, or another American Indian family.
________________
*P.L. 95-068.
and Wulczyn, 2013). About 60 percent of all placed children are reunified with their family; 20 percent are adopted; and the remainder leave for other reasons, including aging out (6 percent). Frequently unaccounted for, however, is the significant variation among and within states with respect to how long children remain in foster care. The median length of stay ranges from 5 to 24 months at the state level and from 2 to 35 months at the county level. Finally, about 1 in 5 children will return to care within 2 years of exit; for some populations, the reentry rate is as high as 35 percent (Wulczyn et al., 2007, 2011).
Aging out of foster care is strongly related to age at entry, as shown in Figure 5-3. Infants are the least likely to age out. Based on the Multistate Foster Care Data Archive (FCDA), fewer than 25 of 2,500 infants (less than 1 percent) remained in placement for their entire childhood. At the other end of the age continuum, about 50 percent of 17-year-olds aged out
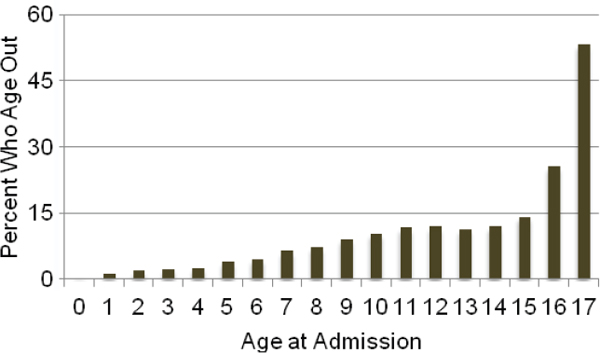
FIGURE 5-3 Probability of aging out of foster care by age at admission.
SOURCE: Data from Wulczyn, 2012.
directly from foster care. Between these two extremes, less than 15 percent of any single age group aged out, except for 16-year-olds.
As noted, the youngest children, particularly those under the age of 1 year, have the greatest risk of placement. For that age group, placement rates were never below 10 per 1,000 and reached 12 per 1,000 in 2006. Among children aged 6 and above, the incidence of placement hovered close to 2 per 1,000, also with a peak in 2006.
The stark age-graded disparity in placement rates is seen clearly in Figure 5-4. The height of these bars depicts the magnitude of the difference in placement rates for infants relative to three other age groups. Compared with 1- to 5-year-olds, infants are about 3.5 times more likely to be placed. The disparity between infant placement rates and the rates for 6- to 12-year-olds averaged 6 placements per 1,000 between 2003 and 2010.
Type of Placement
Because of how much time foster children spend in living arrangements other than those provided by their parents, the settings in which they are placed make a difference. In general, states offer three main types of placement. Family-based care, which is preferred, consists of regular foster family care and relative (kinship) care. Children placed in family foster care may live with other foster children, but the number of unrelated foster children allowed in the home is regulated. More important, the foster parents are in
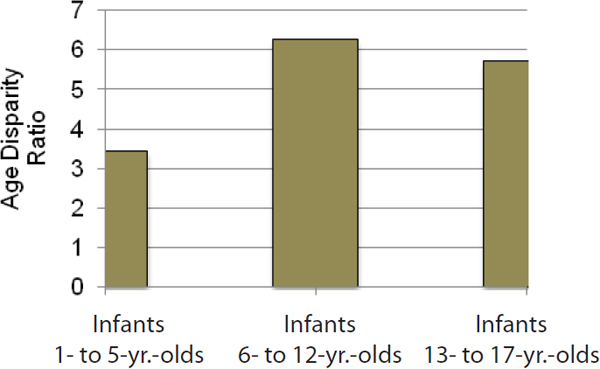
FIGURE 5-4 Age disparity ratios for infants relative to children of other ages.
SOURCE: Data from Wulczyn, 2012.
most cases psychological strangers to the child. Relative foster care involves foster parents who are related to the child either biologically or through fictive kin relationships. Over the past 15 years, kinship care has become the preferred practice option, and its use has increased as a result. The last general placement type is group care. States support a wide variety of group or congregate care settings, from smaller group homes with, for example, six unrelated youth residents to larger campus-based residential treatment facilities. States vary considerably in the range of group care settings, with some states using classification systems that differentiate 10 or more group-based settings depending on the level of care needed.
The data in Figure 5-5 show, by age at admission, how children spent the majority of their time with regard to placement setting in 2003 and 2010. “Predominant placement setting” refers to the setting where children spent more than half their time in foster care. The mixed care type refers to situations in which no one placement type accounted for more than half the time spent in care. The overwhelming majority of children under the age of 13 spent most of their time in placement in a family setting. Nearly 96 percent of infants admitted between 2003 and 2010 spent the majority of their time in a family setting. For older children, group care was the most common care type, with about 38 percent of adolescents spending the majority of their time in foster care in some type of group care setting.
Data also suggest that the use of family-based care is on the rise. As shown in Figure 5-6, the data suggest that the use of both regular and
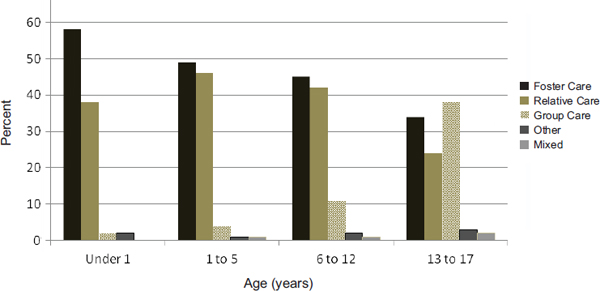
FIGURE 5-5 Predominant placement type.
SOURCE: Data from Wulczyn, 2012.
kinship foster care increased between 2003 and 2010, whereas the use of group care declined.
The deleterious impact on children of multiple placements in foster care has been a salient topic in child welfare policy and programmatic debates for decades. Legislative initiatives to promote permanency for foster children (e.g., the Adoption Assistance and Child Welfare Act, the Adoption and Safe Families Act) have led to increased emphasis on greater placement stability. The U.S. Department of Health and Human Services (HHS) now monitors the number of movements recorded for children in foster care as part of the national outcomes standards (ACF, 2002).
Although stable placements are preferred, children do move between
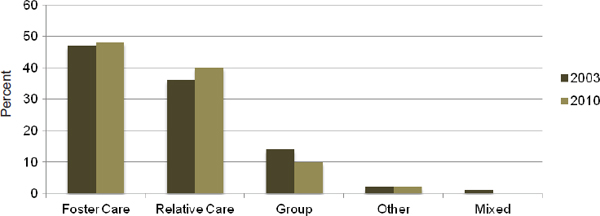
FIGURE 5-6 Change in predominant placement settings, 2003-2010.
SOURCE: Data from Wulczyn, 2012.
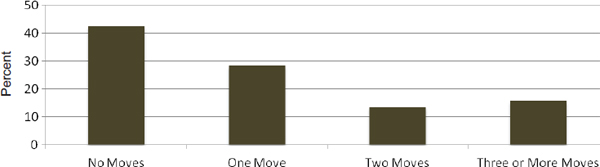
FIGURE 5-7 Average number of moves per child, 2003-2010.
SOURCE: Data from Wulczyn, 2012.
placement settings (see Figure 5-7). Grouped by how many moves they experienced, the largest group of children (43 percent) experienced but one placement (i.e., no moves). About 28 percent of children experienced two placements, while 30 percent experienced three or more placements.
The clinical literature documents the negative effects of placement instability on children. Multiple placements are alleged to affect children’s attachment to primary caregivers, an important early developmental milestone (e.g., Fahlberg, 1991; Lieberman, 1987; Provence, 1989; Stovall and Dozier, 1998). Empirical evidence from other strands of research suggests that multiple placements lead to psychopathology and other problematic outcomes in children, such as externalizing behavior problems (Kurtz et al., 1993; Newton et al., 2000; Widom, 1991).
Despite what is known about the likely impact of placement moves, relatively little research exists on placement stability. An early review of that literature (Proch and Taber, 1985) indicates that the majority of foster children do not experience more than two placements while in foster care. The limited subsequent research focuses on placement disruption rates and factors associated with movement. Generally, researchers report that between one-third and two-thirds of traditional foster care placements are disrupted within the first 1-2 years (e.g., Berrick et al., 1998; Palmer, 1996; Staff and Fein, 1995). Research on treatment foster care has documented a wider range for rates of disruption, from 17 to 70 percent (Redding et al., 2000; Smith et al., 2001; Staff and Fein, 1995). Although kinship foster homes tend to be more stable than traditional foster homes (Courtney and Needell, 1997), some evidence suggests that kinship placements also may be disrupted frequently, reflecting the vulnerability of the child and the family (Terling-Watt, 2001). Findings from Cochrane Collaboration systematic review of kinship care for children who have experienced child abuse and neglect (Winokur et al., 2009) suggest that children in kinship foster care experience better behavioral development, mental health functioning, and placement stability
than children in nonkinship foster care. Although no difference in reunification rates was found, children in nonkinship foster care were more likely to be adopted, while children in kinship foster care were more likely to be in guardianship. Children in nonkinship foster care also were more likely to utilize mental health services.
Several studies identify factors associated with placement disruption. Early research by Pardeck and colleagues (Pardeck, 1984, 1985; Pardeck et al., 1985) suggests that such child characteristics as older age and behavioral or emotional problems are associated with increased rates of disruption. These findings are corroborated by more recent research (e.g., Palmer, 1996; Smith et al., 2001; Staff and Fein, 1995; Walsh and Walsh, 1990). Findings concerning the relationship of placement disruption to child race and gender are mixed (Palmer, 1996; Smith et al., 2001).
Another study on placement stability examined the link between turnover among child welfare caseworkers and the achievement of permanence for children in Milwaukee County. The authors found that children who experienced caseworker turnover had more placements (Flower et al., 2005).
Many studies investigate the attributes of children and their circumstances in an effort to explain variation in the number of movements. Relatively little work focuses on the movement patterns themselves, and few studies (James et al., 2004; Usher et al., 1999) examine combinations of moves to understand whether the patterns have meaning for child welfare policy and practice.
The timing of moves is also important (see Figure 5-8). Movement early in the placement experience may magnify a child’s sense of instability; movement late in the placement experience may signal changes in the child’s status, the caregiver’s capacity, or both. Because movement and length of stay are so closely intertwined, however, care must be taken in isolating when movement is most common.
Although placement stability is desirable, placement changes are sometimes necessary. For example, children placed in a group care setting may transfer to a family setting if the reasons for placement in group care are no longer material to further progress. Similarly, when caseworkers find a willing and able relative, transfer out of foster care to relative care may be in the long-term best interest of the child. Thus, the number of moves is not the only metric by which to judge whether stability has been achieved. Movement between levels of care or up and down the care continuum provides another view of what happens while children are placed away from home.
The data do suggest that changes in the level of care are common. About 60 percent of children who started off in family foster care and were then transferred to a group care setting went on to experience a third placement, which half of the time involved a return to family care.
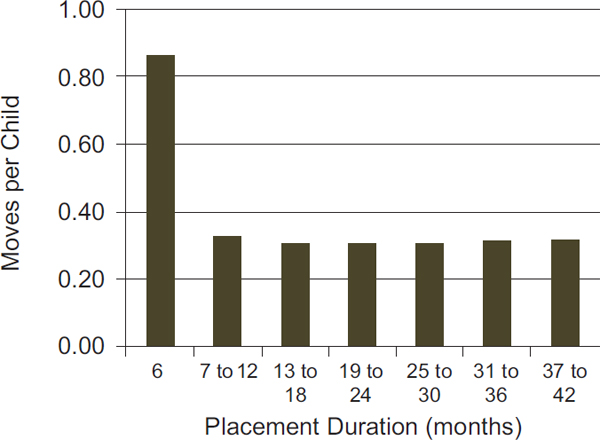
FIGURE 5-8 Period-specific movement rates, 2003-2010.
SOURCE: Data from Wulczyn, 2012.
Exit from Foster Care
For the past 30 years, child welfare policy and practice have focused on reducing the time spent in foster care. The goal of reduced time in care aligns with the notion that foster care is a temporary alternative to care provided by parents. Figure 5-9 shows the cumulative probability of exit for reunification, by age at first admission to foster care. The cumulative probability indicates the likelihood of exit with the passage of time. Referring to Figure 5-9, for example, about 40 percent of infants placed will have been discharged back to their parents within 5 years. Among 13- to 17-year-olds, the figure is closer to 50 percent; for children between the ages of 1 and 12 at the time of admission, the cumulative probability of reunification falls to between 55 and 60 percent.1
The data in Figure 5-9 also suggest that after 2 years, the cumulative probability does not change dramatically, regardless of the age at admission.
________________
1The cumulative probabilities are based only on those cohorts for which at least 3 years of data are available: 2003, 2004, and 2005. The cumulative probability of reunification within 6 months is based on the experience of the 2003 through 2009 admission cohorts. Thus, for the first interval (i.e., 6 months), seven estimates are averaged together, while for the last interval, only three estimates are available.
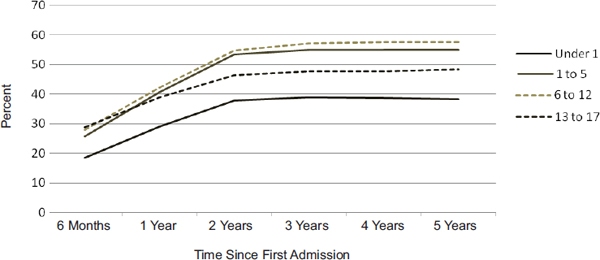
FIGURE 5-9 Cumulative probability of reunification by age at first admission to foster care.
SOURCE: Data from Wulczyn, 2012.
In large measure, this pattern is attributable to the fact as the likelihood of reunification drops off, the likelihood of some other exit to permanency increases. The drop-off in reunification after 2 years is compensated for by an increase in exits to relatives and adoptions.
Reentry to Foster Care
Reentry to foster care refers to children who return to placement after having been discharged from foster care. Although reentry to foster care may be preceded by repeated child abuse and neglect, few studies actually follow that sequence of events. From a policy and practice perspective, there are three types of permanency: reunification, guardianship, and adoption. Of those types, reentry to foster care following reunification or guardianship is easy to track with administrative data. Tracking reentry to foster care following adoption is more difficult. When children are adopted, in keeping with the idea that a new family has been formed, states typically establish a new identity for the child, including new client and case identifiers. In the process of creating a new identity, connections between the old and the new are often severed.
Even among children who exit to permanency for reasons unrelated to adoption, following reentry is difficult with respect to the amount of time needed to observe the full extent of the process. For example, some children admitted to foster care will be reunited with their families after 2 years in placement. Among those children, some will return to care, but not for 2 or more years after reunification. When the time segments are added together, it can take more than 5 years to establish the likelihood of reentry.
Although statistical methods are available to address these concerns, those methods do not alleviate completely the time needed to understand the full extent of reentry.
Child Abuse and Neglect in Out-of-Home Care
While the impact of placement on access to ameliorative services is clearly beneficial, as has been robustly shown in the case of access to mental health services, it is also important to consider the potential negative consequences of placement in foster care. This section examines this issue briefly with regard to what is known about child abuse and neglect in foster care. This subject is difficult to address because of the nature of abuse and neglect that occurs while a child is under the official care of the state, the court, and the child welfare system as a result of abuse and neglect suffered in the child’s biological home—a kind of double jeopardy. It is also a difficult subject to examine empirically because there are three quite disparate sources of information to consider: (1) “official” data generated by child welfare systems and reported by states to the federal government through the Child and Family Service Reviews (CFSRs) and the National Child Abuse and Neglect Data System (NCANDS); (2) findings from investigative and advocacy organizations, such as newspapers and advocacy groups; and (3) data and findings generated by researchers.
When children are placed in out-of-home care, the state assumes responsibility for their care, including their safety. The Adoption and Safe Families Act2 states that child safety is the primary consideration in determining services, placement, and permanency. The federal CFSRs require that child welfare agencies reduce the incidence of abuse and neglect of children in out-of-home care. In 2010, states reported that abuse and neglect rates for children in foster care ranged from 0.00 to 2.33 percent, with a median of 0.35 percent (ACF, 2010).
There are reasons to believe that this source generates underestimates of the true rate of abuse and neglect experienced by children while in foster care. First, the definition used by the CFSRs—“Of all children who were in foster care during the year, what percentage were the subject of substantiated or indicated maltreatment by a foster parent or facility staff member?” (ACF, 2011)—is very limited. It does not include abuse or neglect by other adults or youth in the home, or abuse and neglect that was experienced by the child while in care but that might have been prevented by actions of the adult caregivers in the home. Second, investigative sources such as newspaper articles offer clear evidence that some child welfare systems, or other agencies designated to respond to such reports, do not thoroughly
________________
2P.L. 105-89.
investigate allegations of abuse or neglect of children in foster care or keep good records of these investigations (Cleveland, 2013; Kaufman and Jones, 2003). Investigative reporting has quite different rules of evidence from those used in formal research studies, and may also be biased toward negative examples (e.g., the most egregious service systems) and fail to consider the full range of child welfare systems. Yet these examples raise serious question about the possible underestimation of child abuse and neglect in foster care, although they do not provide research evidence on the size of this underestimation.
Unfortunately, research on abuse and neglect in out-of-home care is sparse (Benedict et al., 1994; Poertner et al., 1999; Zuravin et al., 1993). Nonetheless, it demonstrates some differences in the type of abuse reported and the substantiation rate for reports as compared with abuse and neglect reports in general. Some studies indicate that reports received while a child is in foster care may pertain to abuse or neglect that occurred prior to entering foster care (Tittle et al., 2001, 2008). Poertner and colleagues (1999) report on the results of a study of a large state public child welfare agency using existing management information systems that found a rate of abuse and neglect in foster care ranging from a low of 1.7 percent to a high of 2.3 percent over a 5-year period. However, this study suffers from the same problems seen in the CFSR reports and does little to resolve the large differences in rates between research-based work and newspaper investigations. The conclusion to be drawn is that this research literature is thin, and a well-designed national study that can address the problem is needed.
Finally, the committee notes that efforts to prevent abuse and neglect in foster care include (1) training and services for foster families and facility staff members; (2) increased interaction among the caseworker, the caregiver, and the youth; and (3) more stringent background check requirements for those who provide foster care. The Child Welfare League of America has established best practice guidelines for how child welfare agencies should prevent abuse and neglect and respond to abuse and neglect reports for youth in foster care (Child Welfare League of America, 2003).
State-to-State Variation
Although federal child welfare policy creates a national context for the operation of foster care programs, it is important to remember that states have considerable leeway as to the form and structure of their local child welfare systems. Most states operate what are called state-supervised, state-administered systems; however, 11 states devolve authority for administering the child welfare system to counties. Almost all states use private foster care providers to some extent; in some localities, all foster care is in the hands of private, nongovernmental agencies. As important, states differ
with respect to the types of child abuse and neglect brought to the public agency’s attention. Thus considerable variation exists among and within states in the use of foster care as a response to child abuse and neglect.
As a result of these many sources of variation in state and local child welfare systems, state-to-state comparisons of children’s experiences in child welfare systems may obscure important and consequential differences in child and case characteristics. Only rarely are data collected to a level of detail sufficient to permit examination of the fate of equivalent cases across states and policies, beyond simple comparisons of cases matched by race and age. With this type of data, analysis using emerging quasiexperimental methods may be able to examine more complex interactions between state and local policies and children’s experiences in child welfare systems.
States vary as well in the duration of out-of-home care. Figure 5-10 shows the duration for three states to illustrate the magnitude of the differences. First, it is important to highlight the similarities. In each of these three states, infants remain in care longer than children of other ages; older children (13- to 17-year-olds) remain for the least amount of time. That said, the state differences are stark. In state A, the median duration of care for infants is in excess of 30 months; in state B, the figure for the same group of children is under 10 months; and in state C, the figure is just over 20 months. State variation also is considerable for other indicators—use of group care, placement stability, and reentry.
It should be noted that variability within states is as significant as that among states. To a large extent, states are a reflection of their largest county or counties, and what is true in medium-sized counties can be quite different from what is true in larger counties. Because of the variability among states, one must be careful in drawing inferences about state-level outcomes
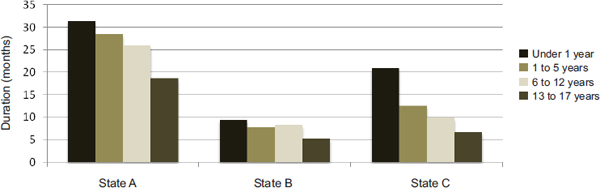
FIGURE 5-10 Variation among states in median duration (in months) of first admission to out-of-home care, by age.
SOURCE: Data from Wulczyn, 2012.
from a national picture; likewise, local (e.g., county) outcomes may be quite different from state-level outcomes.
Finally, a note about the possible impact of state differences with respect to their administrative structure (i.e., county- versus state-administered systems) is in order. No published research examines whether state administrative structure is in some way related to the performance of child welfare systems. In an unpublished exploratory study looking at length of stay in foster care, Wulczyn and colleagues (2011) used administrative structure as a model covariate and found no significant relationship between duration of care and administrative structure, given other variables in the model. More to the point, states differ in so many ways—spending on foster care, poverty rates, policy, use of private agencies—that it is difficult to predict whether administrative structure makes a unique contribution to the system’s underlying performance. This is an important area for study given the cost of operating county-administered systems.
Finding: Contrary to popular belief, most investigated reports of child abuse and neglect do not result in out-of-home placement; only about 20 percent of investigated cases result in the removal of a child from his or her home.
Finding: Risk of placement and length of stay in out-of-home care can vary considerably based on such factors as the child’s age and the family’s race, socioeconomic status, and state of residence.
Finding: Significant variation has been found among and within states in the length of time children remain in foster care. However, this variable frequently is omitted in studies on out-of-home placement. Little research has assessed the factors accounting for this variation to support the development of placement, placement prevention, and reunification practices so as to avoid or shorten placements.
Finding: Children placed in kinship foster care have been shown to experience better behavioral development, mental health functioning, and placement stability than children placed in other forms of care, and can achieve permanency through guardianship (as supported by the Guardianship Assistance Program in the Fostering Connections to Success Act of 2008). As a result, evidence suggests that placement with kin has in the last 15 years become an increasingly preferred option for child welfare systems.
Finding: Evidence suggests that placement instability can lead to a variety of negative consequences for children in the child welfare system.
However, relatively little research has been conducted on this issue, especially with regard to the impact of multiple placements, including research on the separate effects of movement patterns, the timing of moves, and movement between levels of care. Further, definitions of placement instability vary across states, and little research has been done to elucidate the meaning of these varying definitions.
Finding: Current research is inadequate to permit an accurate assessment of rates of reentry into foster care, particularly with regard to tracking reentry after adoption and following children longitudinally for a length of time sufficient to observe the full extent of reentry.
Finding: The experiences of children involved in the child welfare system vary considerably among and within states. These variations are due largely to differences in the form and structure of states’ local child welfare systems, as well as differences in how child abuse and neglect are defined, reported, and responded to by public agencies. Research is insufficient to determine whether differences in state administrative structures (county- versus state-administered systems, extent of privatization) relate to the performance of child welfare systems.
MAJOR POLICY SHIFTS IN CHILD WELFARE SINCE 1993
Public child welfare services occur in the context of the prescribed federal child welfare outcomes of safety, permanency, and well-being that were codified in the Adoption and Safe Families Act. The three principal outcomes—safety (being safe from further child abuse and neglect), permanency (stability when in child welfare care and achieving permanency through reunification, adoption, or guardianship), and well-being (often characterized as child well-being, focused primarily on physical health; behavioral, emotional, and social functioning; and education)—frame the mission for child welfare services in response to child abuse and neglect. Historically, child welfare agencies have focused on the first two outcomes as their primary mandate and the areas in which they have clear expertise. They have been ambivalent about fully embracing the third element because the expertise for providing both preventive and ameliorative services targeting child well-being usually resides in other child-serving systems, such as child physical and mental health, developmental, and educational services. Nonetheless, child welfare policy, practice, and research recently have demonstrated a more robust focus on child well-being, as indicated by both the title of the landmark national child welfare study National Survey on Child and Adolescent Well-Being and multiple initiatives from the Administration
on Children, Youth and Families (ACYF) under the leadership of Commissioner Bryan Samuels since 2009.
Child welfare services also are intended to embrace a “systems of care” perspective that federal child welfare oversight has recommended for adoption by state and local agencies (Children’s Bureau, 2012). Systems of care, drawn from wraparound services in the children’s mental health field, is a service delivery approach intended to build partnerships for creating an integrated process that can meet families’ multiple needs. It is based on principles of interagency collaboration; individualized, strengths-based care practices; cultural competence; community-based services; accountability; and full participation and partnerships with families and youth at all levels of the system. To be effective, systems of care need to build an infrastructure that will result in positive outcomes for children, youth, and families (CWIG, 2008).
Since 1993, child welfare systems have undergone a number of changes in policy, service delivery, and system design so as to better meet safety, permanency, and well-being goals. Some of these changes are due to the implementation of new federal3 and state legislation (see Chapter 8) and to replications of innovative program models (see Chapter 6) that have been widely disseminated after garnering some positive program evaluations.
Improvements and service changes also have occurred as a result of efforts to address service gaps identified in class action lawsuits, frequently filed by national entities such as Children’s Rights or the Youth Law Center, or in response to deficiencies identified in the federal CFSRs that assess states’ delivery of child welfare services. These changes have signaled the desire to implement programs and services that better target the needs of children in their own homes, that address service and decision-making disparities that result in the overrepresentation of children of color in the child welfare system, and that address strategies for engaging families more effectively and actively in the development of their own plan of services. The focus of child welfare services may also change after a horrific and highly visible death due to child abuse and neglect—sometimes causing the decision-making pendulum to swing toward placing children in out-of-home care, while at another point in time the same assessment might have resulted in a child’s staying with his or her family.
Numerous policy and programmatic initiatives have been designed to keep children from entering the child welfare service system (e.g., differential or alternative response—see the discussion on p. 198); to keep children from being placed in out-of-home care (family-based interventions such as family preservation services and family group conference decision making); to place children with kin (e.g., subsidized guardianship and increased at-
________________
3For example, see P.L. 103-66, P.L. 105-89, and P.L. 110-351.
tention to finding relatives that might become placement options); and to move children on to more permanent placement more quickly through family reunification, subsidized guardianship with kin, or adoption. Expedited time frames for permanency were made more explicit through the imposition of placement time limits designed to achieve permanency once a child has entered out-of-home care, along with incentives to states to increase adoptions, under the Adoption and Safe Families Act of 1997.4 During the 20-year period since the 1993 NRC report was issued, increased attention has been focused on the development of decision-making tools for assessing immediate risk, safety, and family and child functioning to support the formulation of a plan of care (see the discussion of risk, safety, and needs assessment later in this chapter).
To understand the outcomes of abused and neglected children in the child welfare system, it is important to understand the legislative and system-level reforms that drive child welfare services. The key reforms are described in the following subsections.
Legislative Reforms
Legislative reforms driving child welfare services include provisions for family preservation and family support programs, the Adoption and Safe Families Act, the Fostering Connections to Success and Increasing Adoptions Act, the Child and Family Services Improvement and Innovation Act, and Title IV-E waivers.
Family Preservation and Family Support
The release of the 1993 NRC report occurred close to the passage of the Family Preservation and Family Support provisions of P.L. 103-66, amending the Social Security Act to create Title IV-B Part 2. The hope was that states would use these new funds to focus on prevention through community-based family support programs designed to strengthen and stabilize families through parent training, drop-in centers and early screening, and family preservation programs targeting families at risk or in crisis, thus helping to keep children out of out-of-home care and to support more timely reunification.
Not only was this funding very limited, however, but as with many child welfare services, states varied widely in how they carried out these efforts, how the funds were allocated across the state, whether specific program models (e.g., Homebuilders) were implemented, and which particular populations were targeted (e.g., urban/rural, older/younger, preplacement
________________
4P.L. 105-89.
interventions/reunification). The 1993 legislation required the Secretary of HHS to evaluate the effectiveness of Family Preservation and Family Support Programs, which would also help better identify the evidence base for these efforts. But variations in implementation made evaluation difficult, and the federal evaluations were equivocal, especially with respect to outcomes of foster care placement (ASPE, 2008a).
Although attention to programs specifically called Family Preservation and Family Support has waned, a commitment to working together with families in their own homes and assisting with parenting and other interventions has continued, using different terms and program names (see below and Chapter 6).
Adoption and Safe Families Act
Enacted in 1997, the Adoption and Safe Families Act5 reauthorized the Family Preservation and Family Support Programs, retitled Safe and Stable Families; codified the expectations of child welfare outcomes related to safety, permanency, and well-being; and required that safety be assessed at every decision point in case planning and judicial review. The legislation also emphasized the role of substance abuse in child abuse and neglect, stressed children’s health and safety and clarified “reasonable efforts” emphasizing children’s health and safety, and required states to specify situations in which services to prevent foster care placement and reunification are not required. The Adoption and Safe Families Act also set specific timelines for making decisions about permanent placement, requiring that states initiate termination of parental rights after a child has been in foster care for 15 of the previous 22 months. When parental rights are terminated, the parents no longer have a legal relationship with their child, allowing the child to be placed for adoption (CWIG, 2013a). States also became eligible for bonuses for increasing the number of children adopted. HHS was required to establish new outcome measures with which to monitor and improve states’ performance, which resulted in creation of the CFSRs. Finally, the act reauthorized the option of using child welfare funding more flexibility through Title IV-E waivers (discussed below), first created in 1994.
Fostering Connections to Success and Increasing Adoptions Act
Enacted in 2008, the Fostering Connections to Success and Increasing Adoptions Act6 amended Title IV-E and Title IV-B of the Social Security Act
________________
5P.L. 105-89.
6P.L. 110-351.
to connect and support relative caregivers, improve outcomes for children in foster care, provide for tribal foster care and adoption access, improve incentives for adoption, and extend Medicaid eligibility to children in kinship guardian assistance settings. The act also required agencies to find relatives and make greater efforts to keep siblings together, and sought to ensure better coordination among education, health, dental, mental health, and child welfare services. In addition, Title IV-E assistance was extended to older youth who are in care by age 16, and the development of a youth-directed transition plan for such cases was encouraged. The act also emphasized connection to families for children in foster care or at risk of placement by providing states with grants to find families, support kinship placements through subsidized guardianship, and support family group conferencing and kinship navigators so that youth could remain more connected to family and perhaps find family with whom to stay.
Child and Family Services Improvement and Innovation Act of 20117
This legislation reauthorized the Safe and Stable Families Program and further amended Title IV-B by focusing on the well-being of children, addressing the emotional trauma of children who experience the child welfare system, providing special attention to the needs of young children (under 5), and requiring states to monitor the use of psychotropic medications for children in foster care. This legislation also reauthorized the availability of Title IV-E waivers (see below) through 2014.
Title IV-E Waivers
Title IV-E waivers, first authorized in 1994 under P.L. 103-432 and reauthorized under the Adoption and Safe Families Act, expired in 2006, but were reauthorized again in 2011 under the Child and Family Services Improvement and Innovation Act (described above). They allow states to waive certain Title IV-B and Title IV-E requirements that govern foster care, adoption, kinship guardianship assistance, and other programs to create demonstration programs that are cost neutral. States can redistribute the use of funding to keep children from entering out-of-home care and to offer and access more comprehensive services. Between fiscal year (FY) 1994 and FY 2006, 23 states implemented one or more waivers to target service strategies including subsidized guardianship and kinship permanence, flexible funding to local child welfare agencies, managed care systems, services for caregivers with substance abuse disorders, intensive services including expedited reunification, and adoption and postpermanency services (Patel
________________
7P.L. 112-34.
et al., 2012). These initiatives required extensive evaluations, several of which used random assignment in experimental designs (Testa, 2010), and the findings from these programs helped set the stage for the reauthorization of both the authority and provisions related to kinship guardianship assistance that were included in the Fostering Connections Act.
The new 2011 waiver authority, which enables the secretary of HHS to authorize up to 10 demonstration projects each year during FY 2012-2014, has more explicit goals than the previous waiver programs, including increasing permanency for youth; reducing time in foster care; promoting positive outcomes for children, youth, and families in their homes; and preventing child abuse and neglect and the reentry of infants, children, and youth into foster care. The legislation also contains a stipulation that the federal waiver application review cannot consider whether the waiver will use an experimental design for the application, an interesting turn since many view the use of random assignment in the earlier waivers as a positive process (Testa, 2012). The new waiver authority specifies that funds can be used to establish programs designed to provide permanency and prevent children from entering foster care. These programs include intensive family finding, kinship navigator, and family counseling programs; comprehensive family-based substance abuse treatment; programs designed to identify and address domestic violence; and youth mentoring programs. The new waiver authority also establishes as priorities the production of positive well-being outcomes, with attention to addressing trauma; enhancement of the social and emotional well-being of children and youth; contributions to the evidence base for improving the lives of children and families; and leveraging of the involvement of other resources and partners. In FY 2012, the Children’s Bureau funded nine new waivers. (Summaries of these new programs can be found at http://www.acf.hhs.gov/programs/cb/programs/child-welfare-waivers#summaries [accessed March 6, 2014].) It will be important to continue to follow these efforts, especially with regard to the intent to reduce child abuse and neglect and implement evidence-based programs.
SYSTEM-LEVEL REFORMS INTENDED TO
IMPROVE PRACTICE AND OUTCOMES
Beyond specific federal legislation that has paved the way for practice reforms, states and localities have adopted a number of system-level reforms most likely intended to improve child and family outcomes.
Safety, Risk, and Needs Assessment
Assessment in child welfare involves at least three distinct processes: safety assessment, in which the social worker determines whether a child
is currently safe in his or her home or out-of-home placement; risk assessment, in which the social worker assesses the likelihood that the child will experience a recurrence of abuse and neglect in the future; and needs assessment of child and family functioning, which is used to develop case plans. Assessment may occur at multiple points during the child’s engagement with the child welfare system, including determination of the response to an initial report of abuse or neglect, placement decisions, and case closure (D’andrade et al., 2008).
All three types of assessment are critical decision aids designed to complement case workers’ clinical judgment in determining the best course of action for each child and case. Two approaches to assessment have been pursued within the field of child abuse and neglect: actuarial, which has been used to determine risk, and consensus-based, which has been used to determine safety, risk, and needs. Actuarial risk instruments use statistical methods to calculate the probability that a child will experience a recurrence of abuse or neglect in the future, based on risk factors identified with recurrence of abuse and neglect in the empirical literature. Consensus-based instruments are created based on theories of child abuse and neglect etiology, empirical research, and expert opinion on relevant case characteristics.
Actuarial risk assessment instruments clearly have the greatest potential to estimate the recurrence of child abuse and neglect reliably and accurately, and child welfare agencies in the majority of U.S. states use such tools (Coohey et al., 2013; Schwalbe, 2008). This type of risk assessment, however, does not indicate which clinical factors are most important to address and certainly does not indicate which services are most likely to be effective. The Structured Decision Making (SDM)© approach is an example of an effort to integrate actuarial risk assessment and consensus-based assessment of child and family needs into child welfare practice (Kim et al., 2008). In the SDM model, a case worker uses a consensus-based safety assessment at points throughout the case to determine whether a child can safely remain in his or her home, as well as an actuarial risk assessment to determine the level of risk (high, medium, or low) that a child will experience a recurrence of abuse or neglect in the long term. These assessments of risk and safety are complemented by a consensus-based family strengths and needs assessment, which is used to identify relevant services. This approach was developed and is trademarked by the National Center for Crime and Delinquency (CWIG, 2013c; NCCD, 2013).
In their research using SDM©, Shlonsky and Wagner (2005) identify the process of evidence-based practice as the key to linking the predictive power of actuarial risk assessment with the choice of effective services based on structured needs assessment. Building on their work, Schwalbe (2008) suggests further theoretical refinement of the link between actuarial risk assessment and the identification of needs for the purposes of case planning,
arguing that the distinction is not between risk factors and needs but between static and dynamic risks. Empirical testing of these theoretical models will be critical to understanding the best practices to support caseworkers’ decision making about safety, risk, and interventions. As states, localities, and tribes implement such efforts, it will also be important to ensure that they are integrated with other practice efforts and that staff have the necessary competencies to make these clinical judgments, suggesting the continuing need for evaluation and implementation research.
Differential Response
An innovation over the past 20 years, one that is encouraged by the 2010 reauthorization of the Child Abuse Prevention and Treatment Act, is differential or alternative response, also referred to as dual-track, multitrack, or multiple-response systems (QIC-DR, 2011). The several differing names are just one indication that this innovation has been implemented quite differently across states. The term “differential response” is used here to denote the various processes by which child welfare agencies have implemented a differential way of responding to child abuse and neglect cases based on the severity of the alleged abuse or neglect and the child’s needs (Casey Family Programs, 2012). An overview of differential response is available from the Quality Improvement Center on Differential Response,8 funded by the Children’s Bureau.
Differential response offers multiple pathways for addressing the needs of children and families referred to child welfare services. In its simplest form, child abuse and neglect referrals are screened and, based on level of risk and other criteria, referred to either an assessment pathway or a traditional investigation pathway. Low- or moderate-risk families are often assigned to the assessment pathway, whereby workers assess the strengths and needs of families and offer services to address those needs, engaging families in the planning of services (QIC-DR, 2011). No formal determination is made regarding the alleged abuse or neglect, and families may decide to accept or refuse services (QIC-DR, 2011). Families are assigned to the traditional investigation pathway when they are at moderate to high risk; the child abuse and neglect type is sexual abuse, serious physical abuse, or other abuse and neglect types designated by the state (e.g., serious neglect in some states); and when other state-specific criteria are met (e.g., age of the child, precipitating factors) (Merkel-Holguin et al., 2006).
Differential response systems allow workers to reassign families from the assessment pathway to investigation if higher risk is discovered, and
________________
8See http://www.ucdenver.edu/academics/colleges/medicalschool/departments/pediatrics/subs/can/DR/Pages/DiffResp.aspx (accessed January 27, 2014).
in some states workers may reassign families from the investigation to the assessment pathway (Merkel-Holguin et al., 2006; QIC-DR, 2012). This approach is intended to provide an engaging service array for low- or moderate-risk families, supporting the well-being of children and families while still protecting child safety and avoiding future involvement with child protection systems (QIC-DR, 2011).
Tremendous growth has occurred in the implementation of differential response systems over the two decades since the first two states piloted the approach in 1993 (QIC-DR, 2011). Currently, differential response systems have been implemented in 21 states, the District of Columbia, and four tribes (QIC-DR, 2012). Another state (Maryland) enacted legislation requiring a study of differential response, and currently has a bill in the state legislature proposing the establishment of a differential response system beginning in 2013 (NCSL, 2012). In addition, some states and localities have implemented this approach without legislation to guide them (QIC-DR, 2012). Three-quarters of the above 21 states and the District of Columbia have implemented differential response statewide, and the remaining states have implemented it regionally in pilot sites (QIC-DR, 2012). More states (n = 12) are planning or considering the implementation of differential response (QIC-DR, 2012), including one state (Florida) that previously discontinued the approach (QIC-DR, 2011). A few states (Arizona, Arkansas, West Virginia) have discontinued the use of differential response (QIC-DR, 2012).
Privatization
Also known as “outsourcing,” “public-private partnership,” or “community-based care,” child welfare privatization involves an arrangement in which private agencies assume responsibility for public child welfare functions. Privatization is a cross-cutting issue because of the variety of child welfare services that can be outsourced, including case management, family preservation and support, contracting, referral, foster care, and adoptions. In Florida, all child protection functions have been outsourced except for child protection investigation (Armstrong et al., 2008), although in most instances, states that have pursued privatization of their case management functions have not privatized child protection functions. The private-sector provision of child welfare services has a long history, even predating the rise of public child welfare agencies, entailing an array of family services and child welfare and residential agencies, many of which were under sectarian auspices. With the growth of the public child welfare system, many states contracted with private agencies for specific services, and public funding has become an increasing source of revenue for private agencies over the past 30 years (Collins-Camargo et al., 2011). In recent
years, however, states have begun to pursue contracting out not just child welfare services but also their case management functions.
To understand the evolving roles of private agencies in the provision of public services, HHS’s Office of the Assistant Secretary for Planning and Evaluation undertook a series of studies to understand privatization efforts, their rationale, and their implications (ASPE, 2009). The major focus was on the privatization of the case management functions—how it affects placement, placement stability, decision making, court efforts, staffing, and all of the processes needed to meet the needs of abused and neglected children in the child welfare system (ASPE, 2008b).
Models of Family and Parent Engagement
Since the 1993 NRC report was published, child welfare systems have expanded their efforts to engage families, especially parents (including fathers), more fully as part of the service planning and intervention process. Findings of the CFSRs indicated that agencies had difficulty involving parents and children in case planning, and 46 states addressed this issue in their Program Improvement Plans. The findings of the CFSRs suggested that agencies had difficulty with family engagement because of (CWIG, 2012a)
• Staff lacking the skills needed for family engagement in case planning (42 states);
• Staff attitudes and behaviors (25 states);
• Organizational issues (e.g., high workloads) (21 states);
• Parent attitudes, behaviors, or conditions that impede active involvement in case planning (17 states);
• Difficulties created by court-related requirements (14 states); and
• System issues and documentation requirements precluding the production of a written case plan in a family-friendly format (17 states) (CWIG, 2012a, pp. 7-8).
Safe and stable families legislation and community-based child abuse prevention efforts have been among the forces that have promoted a number of family engagement models (see Center for the Study of Social Policy, Kempe Centre Family Group Decision-making, Friends National Resource Center, for information on different models). Family group decision making is one key model, found in 29 states (CWIG, 2012a, p. 8). This model has been broadly disseminated and vigorously promoted since the late 1990s by the American Humane Association’s Child Division (now housed at the Kempe Center). Parent engagement models such as Parents Anonymous (discussed below in the section on models of parent and family engagement) also have long-standing connections with child protection programs
in addressing child abuse and neglect through promotion of a self-help and parent leadership model.
RESEARCH ON KEY POLICY AND PRACTICE REFORMS
The years since the 1993 NRC report was issued have seen improved access to and use of empirical data that are now having a greater influence on decision making. As will be described, focus on the use of administrative and case data to inform child welfare practices has increased. As states and localities use these data, agencies begin to examine differences in decision making among workers and to develop services that are more responsive to the age of the child and the characteristics of the parents (e.g., mothers experiencing depression or parents who abuse substances or have disabilities). Reforms also are being driven by the findings of the federally funded NSCAW, which provide a fuller picture than was previously available of the characteristics of children, families, and workers involved in the child welfare system.
The NSCAW, mandated under the Personal Responsibility and Work Opportunity Reconciliation Act of 1996, Sec. 429A,9 has been under way since 1997, with two cohorts of children being enrolled. Data are drawn from first-hand reports from children, parents, and other caregivers, as well as reports from caseworkers and teachers and data from administrative records. The NSCAW is a nationally representative, longitudinal survey of children and families who have been the subject of investigation by child protective services. The study examines child and family well-being outcomes in detail and seeks to relate those outcomes to experience with the child welfare system and to family characteristics, the community environment, and other factors (OPRE, 2013). It is the first longitudinal study in the child welfare field to collect information directly from children and families. The Cohort 1 phase of the NSCAW collected information 5 to 7 years following investigation by child protective services. Because of budget restraints, the Cohort 2 phase is collecting data only over the course of 3 years, and additional funds for further study are not available.
Another data source that provides useful information at the national level is the FCDA.10 Containing the records of more than 2 million chil-
________________
9P.L. 104-193.
10As a resource for social scientific research, the archive was designed deliberately to capture children’s experiences in foster care using a life-course, social ecological lens, making it possible to overlay those experiences onto age-graded trajectories that provide a basis for understanding whether placement happens and when in the life course it is most likely to happen. From the socioecological perspective, it is known that where children live exerts a strong influence on what happens to them over the life course. All of the state data in the FCDA are available at the county level, which includes a link to relevant time-series census
dren, the FCDA is the oldest reliable source of data on foster care, dating back as far as 1976. For the 25 states that contribute data to the archive today, the FCDA maintains a harmonized record of placement through each revision to the state’s data. The discussion below uses information on the experiences of abused and neglected children in the child welfare system drawn from FCDA data for 2003 to 2010, when coverage within the archive reached as high as 70 percent of all foster children in the United States, depending on the question posed. The FCDA is the closest thing to a record of exactly what happened to 2 million children placed away from home in the United States.
A more accurate picture of the experiences of abused and neglected children in the child welfare system has allowed researchers to better evaluate the effectiveness of programs and services. As will be discussed in Chapter 6, child welfare agencies, along with other service providers, now have a robust array of proven model programs on which to draw in designing service practices. However, more research is needed to devise strategies for replicating these models across the varied settings and localities in which children and families receive care.
Title IV-E Waivers
As discussed previously, Title IV-E waivers have been used to target service strategies, including subsidized guardianship and kinship permanence; flexible funding to local child welfare agencies; managed care systems; services for caregivers with substance abuse disorders; intensive services, including expedited reunification; and adoption and post-permanency services (Patel et al., 2012). Many of these initiatives required extensive evaluation, in several cases using random assignment in experimental designs.
In Illinois, the first 10 years of a subsidized guardianship demonstration that used random assignment and an experimental evaluation design saw the state’s foster care population shrink from 51,000 children in 1997 to 16,000 in 2007. The subsidized guardianship waiver allowed the state to use millions of dollars in IV-E reimbursements for child welfare services and system improvements that it otherwise would not have been able to accomplish (Testa, 2010). The strong evidence resulting from the demonstration’s experimental evaluation design encouraged five additional states to apply for waivers to replicate the Illinois strategy, and as previously noted, the findings from these programs resulted in reauthorization in the Fostering Connections Act to use Title IV-E dollars to fund guardianship subsidies.
data. In some states, the geographic data are available at the block group level, a vantage point from which one may assess close up where placement as a response to child abuse and neglect fits into the community narrative.
Several states that used Title IV-E waivers only to allow more flexible use of funds, without a specific program focus, had less clear outcomes. Absent an experimental evaluation design, determining whether changes are due to the waiver or to broader social, economic, and demographic influences is more difficult (HHS 2005 synthesis of findings from IV-E flexible funding child welfare waiver demonstrations).
Differential Response
The literature examining differential response has uncovered some key considerations for the design and implementation of differential response systems. Examples are shown in Boxes 5-2 and 5-3. Box 5-2 presents core components of differential response, developed by Merkel-Holguin and colleagues (2006), while Box 5-3 presents core values to be included in the noninvestigation pathway of differential response, derived by Kaplan and Merkel-Holguin (2008).
The growth in the use of differential response systems has been accompanied by evaluations in some states, as well as the establishment of the federally funded National Quality Improvement Center for Differential
BOX 5-2
Core Elements of Differential Response
• The use of two or more discrete responses of intervention;
• The creation of multiple responses for reports of maltreatment that are screened in and accepted for response;
• The determination of the response assignment by the presence of imminent danger, level of risk, and existing legal requirements;
• The capacity to re-assign families to a different pathway in response to findings from initial investigation or assessment (e.g., a family in the alternative response pathway could be re-assigned to the investigation pathway if the level of risk of the child is found to be higher than originally thought);
• The establishment of multiple responses is codified in statute, policy, and/or protocols;
• Families in the assessment pathway may refuse services without consequence as long as child safety is not compromised;
• No formal determination of child abuse and neglect is made for families in an assessment pathway, and services are offered to such families without any such determination; and
• No listing of a person in an assessment pathway as a child abuse and neglect perpetrator in the state’s central registry of child abuse and neglect.
SOURCE: Merkel-Holguin et al., 2006, pp. 10-11.
BOX 5-3
Core Values for a Differential Response
Non-investigative Pathway
• Family engagement versus an adversarial approach;
• Services versus surveillance;
• Labeling as “in need of services/support” versus “perpetrator”;
• Being encouraging with families versus threatening;
• Identification of needs versus punishment; and
• A continuum of response versus “one size fits all.”
SOURCE: Kaplan and Merkel-Holguin, 2008, p. 7.
Response in Child Protective Services (QIC-DR). Evaluations of differential response systems have been undertaken with varying levels of rigor (QIC-DR, 2011). To the committee’s knowledge, just three randomized controlled trials (RCTs) of the approach have been conducted, including studies in Ohio (Loman and Siegel, 2012), Minnesota (Siegel and Loman, 2006), and one county in New York (Ruppel et al., 2011). In each RCT, families that met the criteria for the assessment pathway were randomly assigned to receive either the assessment pathway or traditional investigation services, allowing comparison of outcomes for similar groups of families. Random assignment yielded equivalent groups in one study (Loman and Siegel, 2012) and groups that were similar on all measured characteristics except history of child protective services/previous case, which the researchers statistically controlled for, in the other two studies (Ruppel et al., 2011; Siegel and Loman, 2006). Administrative data were used for most measures, minimizing problems with attrition but also limiting the quality of measurement of outcomes related to developmental well-being.
In addition to the RCTs, seven quasiexperimental studies have evaluated differential response systems using comparison groups of matched sites or families, supplemented in two states by pre-post data comparisons (QIC-DR, 2011). Another 10 states have only monitored administrative data as they implemented their differential response systems (QIC-DR, 2011).
Results from the most rigorous evaluations—three RCTs of differential response—indicate better outcomes for families on an assessment pathway compared with investigated families. Overall, these studies suggest that differential response maintains or increases safety of children, increases
access to services, and increases family satisfaction with services. Findings include the following:
• Child safety was maintained. Evaluators found that children in families following the assessment pathway were as safe as or safer than investigated families as measured by administrative data. The assessment pathway families were the basis for similar (Ruppel et al., 2011) or significantly lower numbers of subsequent screened-in child abuse and neglect reports (Loman and Siegel, 2012; Siegel and Loman, 2006) compared with traditionally investigated families. Because this finding is based on administrative data rather than direct measures of safety, however, it must be interpreted carefully, because the differential response process could plausibly result in less involvement of any agency with the children, who could then be less likely to be rereported even though they were being reabused.
• Fewer removals from home occurred. Children in families receiving assessments were also less likely to be removed from home (Loman and Siegel, 2012; Siegel and Loman, 2006) than those in families subject to the investigation pathway.
• Access to services increased. Among families responding to follow-up surveys, those receiving assessments reported increased access to services compared with investigated families (Loman and Siegel, 2012; Ruppel et al., 2011; Siegel and Loman, 2006).
• Families were more satisfied. Families receiving assessments reported higher levels of satisfaction than investigated families (Ruppel et al., 2011; Siegel and Loman, 2006).
Quasiexperimental studies and natural experiments have yielded similar results, including similar or increased levels of safety (Loman and Siegel, 2004; QIC-DR, 2011), increased access to services (QIC-DR, 2011), and increased cooperation and satisfaction (Loman and Siegel, 2004; QIC-DR, 2011) for families in the assessment pathway compared with those in the investigation pathway. However, several studies have found no positive impact on removals from home (e.g., Loman and Siegel, 2004), and one of the three RCTs did not report a finding on removals (Ruppel et al., 2011).
In addition to positive outcomes for families, evidence suggests that differential response systems cost less in the long term. In a cost-benefit analysis, differential response was identified as an evidence-based policy associated with improved outcomes that has a positive benefit-to-cost ratio ($8.88), thus being highly likely to have a net positive value and save taxpayers money (Lee et al., 2012). This analysis was based on the three RCTs discussed above, as the analysts opted to use only studies of high
rigor. Results of the examination of costs in individual studies are, however, mixed. In one study (Siegel and Loman, 2006), the researchers reported that the initial average costs for the assessment group were higher, but over the longer term, the average cost per assessment family ($3,688) was lower than the cost per investigated family ($4,967). In another study (Loman et al., 2010), also included in the cost-benefit analysis (Lee et al., 2012), the researchers found that on average, overall costs were somewhat higher for assessment families ($1,325) than for investigated families ($1,233).
Results from existing RCTs are promising, and consistent with findings from less rigorous evaluations. However, the number of rigorous evaluations of differential response systems is low. More rigorous evaluations are needed to understand what factors guide successful implementation and ensure desired outcomes and to learn the extent to which the differential response approach works within different contexts. Knowledge also is needed of how different definitions of abuse and neglect, varied criteria for the assessment pathway, unique approaches to service provision, and adequate funding for services contribute to outcomes. Perhaps most critically, there is a need for studies that do not rely solely on administrative data. Fortunately, three additional RCTs and a cross-site evaluation are under way to add to the evidence base (QIC-DR, 2011). As more rigorous studies emerge, additional cost-benefit analyses will be needed as well, including examination of costs associated with different differential response models. At the same time, states should initiate or continue with state-specific evaluations to understand the ongoing impact of their differential response systems.
Privatization
Privatization efforts have undergone limited evaluation, and most applicable studies have methodological shortcomings that limit the generalizability of their results. Evaluation studies included mainly quasiexperimental designs or qualitative analyses of implementation processes. The committee was unable to identify any RCTs of the privatization of child welfare services. A quasiexperimental study (Yampolskaya et al., 2004) analyzed longitudinal administrative data in Florida to compare outcomes for 4 counties using community-based care with those for 33 counties using traditional public care. Results of this study suggested that the performance of counties using community-based care was similar to that of counties not using this approach; however, this study had several methodological limitations, and thus its results should be interpreted with caution.
Three qualitative studies have focused on barriers to implementation. Yang and van Landingham (2012) conducted a qualitative case study of contract monitoring in Florida. Barillas (2011) conducted a historical review of three states (Florida, Kansas, Texas) in an effort to examine the
implementation of outsourced case management. And Flaherty and colleagues (2008) examined implementation processes by conducting focus groups with participants from 12 states. Two common themes emerged from these implementation studies: the key role of politics in privatization and the critical importance of strategic planning before crafting legislation that forces outsourcing. Because government outsourcing often occurs as a reaction to a tragic event, political pressures can lead to ignoring strategic planning and creating overly aggressive implementation schedules and procedures. Yang and van Landingham (2012) suggest that states contemplating whether to outsource services should consider several key questions, including Is privatization economically desirable? Is it administratively feasible? Is it socially and democratically controllable? Is it politically viable? Is it legally appropriate? Identification of measurable performance indicators should also be a key part of the strategic planning process (Flaherty et al., 2008; Yampolskaya et al., 2004). Finally, time and learning play important roles in the successful implementation of privatization; unfortunately, political environments often do not allow the time necessary for systems to mature and management capacities to fully develop (Yang and van Landingham, 2012).
Empirical evidence on the benefits of privatization is limited. Because the focus of recent studies is largely on implementation, further research is required to better understand the effectiveness of specific privatization efforts. The heterogeneity of the field complicates evaluation, as the scope of privatization efforts ranges from very limited performance-based contracts to large, statewide initiatives. Single case studies such as those reviewed above have limited generalizability and would benefit from replication. Future research also should include cost-benefit analyses of privatization. Privatization of the differential response assessment pathway is one area ripe for evaluation. One quasiexperimental study evaluating a differential response program that entails privatizing the assessment pathway through family resource centers (Siegel et al., 2010) yielded promising results, but a more rigorous design and comparison with a publicly provided assessment pathway are needed. Future studies with experimental designs and more robust measurement of effects could examine differences in outcomes and costs between a privatized assessment pathway and public provision of this pathway.
A critical concern identified in several privatization efforts relates to staffing issues. When Kansas privatized foster care, family preservation, and adoption in the mid-1990s, for example, the public agency caseworkers did not choose to move to the private agency, and there have been similar experiences in other states and localities (ASPE, 2008b; Flower et al., 2005). Furthermore, for staff in the private agencies, the need to recompete contracts results in job uncertainty. The Center for Public Policy Priorities
(2005) found that private and public agencies faced similar concerns related to the ability to access adequate services, caseload, and staff turnover (McCown, 2005). That same report notes that improved case outcomes through privatization will not be achieved without adequate social, health, and mental health resources in communities, as well as sufficient numbers of qualified staff and foster and adoptive homes—the same factors that would improve outcomes in the public delivery of services.
Models of Family and Parent Engagement
Family group decision making (FGDM), one of the key models of family engagement, has been examined through many small qualitative and quantitative studies across the globe (Pennell and Burford, 2000), and these authors are now undertaking a systematic review. The model is currently being tested in an RCT as part of a 2011-2014 Family Connections grant from the Children’s Bureau. No Place Like Home is a collaboration among the Kempe Center, Casey Family Programs, and three child welfare jurisdictions. The California Evidence-Based Clearinghouse for Child Welfare rates FGDM as Promising Research Evidence (3 on the Scientific Rating Scale), and notes that it has several distinctive features:
FGDM promotes the involvement of family groups in decision making about children who need protection or care. Child welfare agencies initiate it in making critical decisions regarding the child. Features of the specific FGDM model include a trained coordinator/facilitator who is independent of the case, bringing together the family and agency staff to create and carry-out a safety plan. The intent is for the family group to undergo a process that leads to a case decision that the statutory authorities agree to support if it adequately addresses the agency concerns. The child welfare agency will also organize other service providers to assist in implementing the plan.11
Other models of family engagement include child protection mediation, family group conferencing, family team meetings, the permanency teaming process, and the family unity meeting model (American Humane, n.d.). Additional rigorous research on these models is needed, as is examination of a range of parent and child outcomes with respect to safety, permanency, and well-being. Cost analysis, looking at both long- and short-term costs, also is important.
Parents Anonymous (founded in 1969), a parent engagement model, addresses child abuse and neglect through promotion of a self-help and
________________
11See http://www.cebc4cw.org/program/family-group-decision-making/detailed (accessed January 27, 2014).
parent leadership model. Despite its more than 40-year history, Parents Anonymous is identified as a Promising Practice by the California Evidence-Based Clearinghouse for Child Welfare because of the lack of rigorous studies. A 2010 study funded by the Department of Justice and published in Child Welfare found that, measured using standardized scales, all parents showed improvements in some child abuse and neglect outcomes, risk factors, and protective factors. Parents starting out with particularly serious needs showed statistically significant improvement on every scale. Results indicated that participation in Parents Anonymous contributes to reductions in child abuse and neglect (Polinsky et al., 2010).
Family Support Programs, developed through the Family Preservation and Family Support provisions of P.L. 103-66 discussed earlier, underwent extensive evaluation during the first few years of implementation (Layzer et al., 2001). That evaluation, a meta-analysis of the programs, found that
• Family Support services generally were small-scale efforts with modest budgets and produced small but significant effects across a range of outcomes for parents and children.
• A range of Family Support Program models addressed a host of problems, from child abuse and neglect to school failure and delinquency. Those models with the largest effects had been tested in single sites.
• Among the hundreds of Family Support Programs nationwide, effects were unevenly distributed across program models. The core services were primarily parent education, and programs using professional staff and delivering parent education and support through group meetings had the strongest effects on parenting behavior and on outcomes for children.
o Programs targeting a specific type of family rather than all low-income families in a neighborhood were found to be more effective. This finding is in contrast to philosophies that emphasize nontargeted services.
o Family Support Programs focused on teen mothers with very young children and on families with children with special needs or behavioral problems had the strongest positive effects on both children and families.
o Parent groups led by professional staff were important for parents of children with special needs, and organized parent-child activities were important for teenage parents.
Such findings, along with the implementation and replication of an array of Family Support Programs targeting early parenting over the past 15 years, have not only built the evidence base for Family Support efforts but
also set the stage in 2010 for inclusion of the Maternal and Infant and Early Childhood Home Visitation Program in the Affordable Care Act and other efforts to implement early parent-child interventions. Current evidence regarding the efficacy of these efforts in reducing subsequent child abuse and neglect, and particularly in targeting child welfare populations, is mixed.12 (See Chapter 6 for additional detail.)
In Los Angeles County, a partnership among the public child welfare agency and diverse community agencies has yielded promising outcomes by developing stronger relationships to engage public child welfare agencies; allied public agencies; and community-based networks that offer family-centered services, economic assistance, and capacity building. Findings indicate that the Prevention Initiative Demonstration Project could make a significant contribution to the prevention of child abuse and neglect as well as its recurrence, and that both clinical and community support services are required (McCroskey et al., 2012).
Several recent developments signal a renewed focus on the prescribed federal child welfare outcome of child well-being. These developments include the Initiative to Improve Access to Needs-Driven, Evidence-Based/Evidence-Informed Mental and Behavioral Health Services in Child Welfare (HHS-2012-ACF-ACYF-CA-0279) and Regional Partnership Grants to Increase the Well-Being of, and to Improve the Permanency Outcomes for, Children Affected by Substance Abuse (HHS-2012-ACF-ACYF-CU-0321), buttressed by policy documents such as the Information Memorandum issued by the Administration for Children and Families (ACF)/ACYF on April 17, 2012, on “Promoting Social and Emotional Well-Being for Children and Youth Receiving Child Welfare Services” (Log No: ACYF-CB-IM-12-04). This increase in attention to child well-being can also be linked to a recent significant decrease in the number of children entering foster care, with 2011 seeing the lowest number of foster care placements in the 15 years since the Adoption and Safe Families Act was enacted. This decline has allowed child welfare agencies to consider how to use potential savings in funding for out-of-home care to increase resources for prevention services and services to address child well-being. These shifts are exemplified and supported by the recent ACF/ACYF initiative to award up to 30 state-level Title IV-E waivers over the next 3 years (9 were recently awarded).
________________
12Many Family Support interventions have shifted enrollment guidelines to focus on first-time or new parents or families who have not had prior contact with the public child welfare system. The evidence on the efficacy of those home-based interventions not engaging child welfare-involved families is discussed in the section on prevention strategies in Chapter 6.
Recent findings from analyses of the NSCAW data commissioned by the Annie E. Casey Foundation (Landsverk et al., 2009) support this increased focus on child well-being, not only for children placed in foster care but also for children in families investigated for child abuse who have not been placed:
• Children involved with child welfare systems (including both those placed and those not placed in foster care) showed marked elevations on measures of risk for behavioral and developmental problems compared with population norms. For example, such children are about four times as likely as the normative population to score within the clinical range of the Child Behavior Checklist, and about twice as likely to score in the clinical range on measures of intelligence, language, adaptive behavior, and school achievement (Landsverk et al., 2009).
• Children placed in foster care following a protective services investigation and those not placed showed marked similarities on measures of risk for behavioral and developmental problems. At the time of the NSCAW Wave 1 interviews, children placed were somewhat more likely than those remaining at home to score in the clinical range on measures of behavior and adaptive behavior; significant differences between the two groups were not seen on the other measures of child risks and needs. In addition, other studies have shown that children placed in foster care have elevated levels of internalizing problems, increased behavior problems, poorer school performance and educational attainment, higher levels of cortisol in their blood stream, and poorer mental and physical health (Berger et al., 2009; Dozier et al., 2006; Fisher et al., 2000; Gunnar and Fisher, 2006; Gunnar et al., 2007; Lawrence et al., 2006; see also Chapter 4).
The researchers divided the children who remained at home after a protective services investigation into four groups based on (1) whether the allegation was substantiated (or, in jurisdictions where substantiation is not recorded, whether the allegation was classified as “high risk”) and (2) whether the child(ren) and family involved received services from the child welfare system after investigation. Children in these four in-home groups showed remarkable similarities on measures of behavioral and developmental functioning; in fact, there were no statistically significant differences among the four subgroups on any of these measures.
Children served by the child welfare system, whether in out-of-home care or not, also have similar health characteristics. According to Schneiderman’s analysis of NSCAW data and other research, children’s chances of being diagnosed with a health problem are greater the longer
they remain in foster care and the more visits are made by the agency, and young children (under age 6) in foster care are more likely to be diagnosed with a health problem or a developmental delay than their older counterparts or the general population (Berkoff et al., 2006; Leslie et al., 2005; Stahmer et al., 2005; Sullivan and van Zyl, 2008). Chronic medical conditions, occurring at a high rate among children in out-of-home care (27.9 percent), are more likely among children under age 2 than among older children, and the rate does not vary across placement type (Ringeisen et al., 2008). Among children who have been in foster care for 1 year, 30 percent have chronic conditions—20 percent having one such condition, 3.8 percent having two, and 3.1 having three or more (Jee et al., 2006).
Finding: Public child welfare services occur in the context of the prescribed federal child welfare outcomes of safety, permanency, and well-being that were codified in the Adoption and Safe Families Act. Historically, child welfare agencies have focused on safety and permanency as their primary mandate and the areas in which they have clear expertise. However, child welfare policy, practice, and research recently have demonstrated a more robust focus on child well-being.
Finding: The implementation of differential response systems has greatly expanded in the past two decades across a number of states and localities. Program characteristics of differential response vary, as have approaches to its evaluation, which have varied in design and rigor. Such evaluations have generally shown positive results when families involved in differential response have been compared with those to which traditional child welfare approaches have been applied, particularly with regard to such metrics as child safety, access to services, and family satisfaction. However, there has been a lack of rigorous evaluations needed to understand what factors guide successful implementation of differential response and ensure desired outcomes, as well as the extent to which the approach works within different contexts. Also, many current evaluations are limited by relying solely on administrative data.
Finding: Rigorous evaluations of the privatization of child welfare functions have been limited and have focused mainly on implementation issues. Thus there is limited evidence to support an understanding of the effectiveness and cost-effectiveness of specific privatization efforts and of mechanisms for the effective replication of successful case studies.
Finding: In the past two decades, child welfare systems have expanded their efforts to engage families and parents in their planning and in-
tervention processes. Many promising models, such as family group decision making, have been promulgated, but analysis of these models has been limited to focused, small-scale studies, with little examination of a range of parent and child outcomes regarding safety, permanency, and well-being, as well as short- and long-term cost-effectiveness.
ISSUES THAT REMAIN TO BE ADDRESSED
A number of important issues concerning the child welfare system remain to be addressed by research. These issues include disproportionality and disparity by race/ethnicity, region, and socioeconomic status; interaction between the child welfare system and related systems and services; and a number of systemic issues.
Disproportionality and Disparity
Contact with the child welfare system by children of color in the United States has been a focal point of attention for quite some time (Hill, 2006; Rosner and Markowitz, 1997). With respect to black children in particular, Billingsley and Giavonnoni (1972) wrote about the tragic effects of racism on black children and used the child welfare system as their primary example. Similarly, the modern-day treatment of American Indian children within the child welfare system is burdened by a history of racist practices by the U.S. government, in which American Indian children were removed from their families and communities in a concerted effort to promote their assimilation into mainstream American society by breaking their ties to their tribes (Jones et al., 2000).
Although it depends on the specific indicator of interest (i.e., incidence rate or length of stay) and on the region of the country one examines, children of color generally have greater involvement with the foster care system than white children. According to an analysis of 2010 data from the Adoption and Foster Care Analysis and Reporting System (AFCARS)13 and U.S. census data, American Indian children were disproportionately represented within foster care by an index of 2.1 and black children by an index of 2.0 nationwide, with significant variation among states (Summers et al., 2012). Explanations for these disparities tend to focus on differing needs, racial bias, and policy effects (Fluke et al., 2011; Hines et al., 2004; Osterling et al., 2008), a framework that mimics how the Institute of
________________
13AFCARS is a federally mandated reporting system for all state and tribal Title IV-B/IV-E agencies responsible for the placement, care, or supervision of children in foster care and adoption (45 CFR 1355.40). Case-level data on all children in foster care and adopted with Title IV-E agency involvement are reported to the Children’s Bureau of HHS twice a year.
Medicine differentiates the sources of health disparities (IOM, 2003). On nearly all measures of risk for involvement with foster care—poverty, family structure, unemployment, and adult education levels—children of color face significantly higher risks.
Child abuse and neglect is the main entry point into the child welfare system, and a significant body of research points to higher rates of reported child abuse and neglect among children of color, especially black children, while evidence suggests that these children experience abuse and neglect at higher rates as well (Drake and Johnson-Reid, 2010; Drake et al., 2009; Sedlak et al., 2010). Research also suggests that, along the various decision points that determine whether a child will be placed (i.e., investigation, disposition, and service choice), black children have a greater likelihood of moving forward in the system than either Hispanic or white children (Needell et al., 2003; Rivaux et al., 2008), perhaps because they are less likely to be offered in-home services (GAO, 2007; Marts et al., 2008). There is a marked lack of research on the mechanisms of disparate treatment of American Indian and Asian children in the child welfare system (Hill, 2006).
The overrepresentation of children of color within the foster care population is a function of differences in entry and exit rates. Measured as disparity in entry rates, the gap between placement rates for white and black or Latino children measures how much more likely placement is for the latter children. Disparity ratios for black and white, black and Latino, and Latino and white children are presented in Figure 5-11.
The data in Figure 5-12 provide deeper background on the reasons why disparity rates have changed. Displayed are the changes in disparity ratios between 2000 and 2009 for each pair of comparisons, controlling for the level of urbanicity. “Urban” refers to each state’s largest county based on a count of foster children; “secondary urban” refers to counties that, according to the census designation, have urban populations smaller than that of the one largest county; and “rural” includes all other counties not included in the other two categories. These data show that changes in disparity are highly idiosyncratic with respect to geography. In large urban counties, black/white and black/Hispanic disparity ratios fell dramatically, whereas the Hispanic/white disparity increased. In secondary urban and rural counties, disparity ratios increased except for the Hispanic/white disparity in rural counties. All told, the changes in large urban counties, where most black children live, were large enough to offset the increases observed in the other parts of states.
There has been a surprising lack of research with which to better understand disproportionality, the term (along with disparity) most often used to characterize the difference in black and white child welfare experiences. As discussed in Chapter 2 of this report, disproportionality has a variety
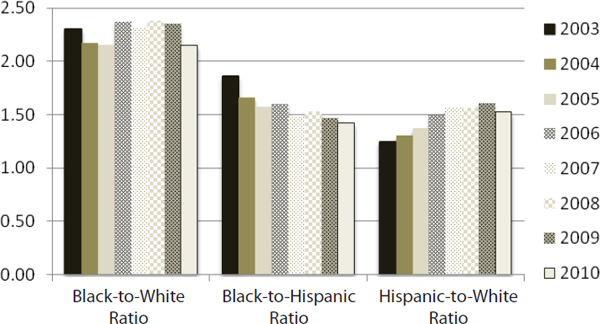
FIGURE 5-11 Change in entry rate disparity ratios, 2003-2010.
SOURCE: Data from Wulczyn, 2012.
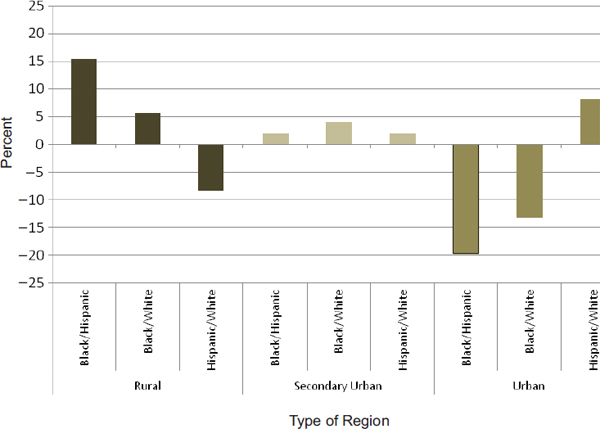
FIGURE 5-12 Change in entry rate disparity ratios by type of region and race/ethnicity, 2000-2009.
SOURCE: Data from Wulczyn, 2012.
of causes. One of the gaps in the disproportionality literature relates to the fact that relatively few studies have looked directly at ecological variation. For example, differences in the likelihood of entry into foster care often are described in relation to poverty, but only a handful of studies actually examine foster care placement across a range of spatial units (e.g., counties, neighborhoods, or census tracts) and social contexts (Freisthler et al., 2007; Lery, 2009; Wulczyn, 1986). As a consequence, even though placement rates are higher on average in poor areas, little is known about how placement rates vary with respect to poverty rates and other social conditions. Because the issue has not been studied, the field is essentially blind to the reasons why some high-poverty areas place many more children per thousand than other areas with equally high poverty rates (Garbarino and Crouter, 1978). A recent study by Wulczyn and colleagues (2013) highlights the need to look more closely at these issues.
Missing from disproportionality analyses and other research, then, is the important work needed to understand why observed levels of disproportionality differ from place to place. In this regard, a Government Accountability Office (GAO) (2007) report serves as a ready example. The GAO found state disproportionality ratios that ranged from 0.44 in Hawaii (i.e., underrepresentation of blacks) to 6.06 in Utah, yet the GAO did not test whether the observed variation in disproportionality accorded with state poverty rates and the presence of bias, even though poverty and bias were used to explain why black children were overrepresented in the child welfare system.
Put more succinctly, research to date has concentrated on analyses that feature race and ethnicity as independent variables in models that treat involvement in the child welfare system (e.g., placement, reporting, or substantiation) as the dependent variable. These models often include other child and family characteristics, such as poverty level or family structure, but the purpose of including those characteristics is limited to understanding whether the effect of a child’s race or ethnicity remains intact when other covariates are included in the model. What the research does not do is assess black/white differences in models that treat those differences as the dependent variable. Disproportionality is nearly 14 times greater in Utah than in Hawaii. Is this because poverty levels are so much greater in Utah than in Hawaii? Or is it because racial bias is so much more pronounced in Utah than anywhere else? The answer to both questions requires a shift from an approach that treats race effects as independent variables to one that examines the level of disparity across units of aggregation (e.g., organizations, administrative units, neighborhoods, or counties). Without such analysis, it is much more difficult to say how service units (e.g., states, counties, offices, agencies, or workers) that exhibit greater levels of bias are linked to greater disparity.
Interaction Between the Child Welfare System
and Related Systems and Services
The past two decades have seen a growing emphasis on coordination and collaboration across the legal and social service systems that serve abused and neglected children and vulnerable families. A related development has been increased federal emphasis on the implementation of evidence-based practices (Haskins and Baron, 2011). A by-product of these efforts is an increasing emphasis on evaluation, which is often multidisciplinary. This section details the important relationships between the child welfare system and providers of mental health and substance abuse services as well as court systems, and explores opportunities to support cross-system collaboration and interdisciplinary research.
Child Welfare and Mental Health Services
A rich literature on the use of mental health care by children involved with the child welfare system has developed over the past 20 years (Horwitz et al., 2010; Landsverk et al., 2002). The research has evolved from regional studies to more recent findings from the NSCAW, with a national probability sample that includes a sample of all children in families investigated by child protective services, a 36-month cohort design, and standardized measures of the need for and use of mental health services (Haskins et al., 2007; Webb et al., 2010). The NSCAW is the first national study to allow examination of whether entry into any child welfare service increases use of subsequent mental health care and whether there is continuity in mental health care after involvement with child welfare ends. Child welfare researchers also have developed methods for understanding the complex longitudinal service pathways of children as their biological and nonbiological caregivers facilitate access to mental health care.
The child welfare system as a gateway to mental health services Because all children in foster care are categorically eligible for Medicaid, an examination of statistics on the use of mental health services among child and adolescent Medicaid populations highlights the increased needs for mental health services of children involved in the child welfare system. While children in foster care represent only 3.7 percent of nondisabled children enrolled in Medicaid, they account for 12.3 percent of expenditures for this group. Use of mental health services is 8 to 15 times greater for children enrolled in foster care than for other low-income, high-risk children enrolled in Medicaid. Children in foster care also are much more likely to use psychotropic medications and are prescribed such medications at a 2 to 3 times higher rate than other children who qualify for Medicaid (dosReis
et al., 2001; Green, 2005; Harman et al., 2000). NSCAW data have now confirmed that the child welfare system functions as a gateway into the child mental health care system, and this increased access to mental health care is associated with high levels of continuity of mental health care even when children leave foster care.
Leslie and colleagues (2005) used NSCAW 18-month cohort data on youth aged 2-14 at study enrollment and examined use of mental health care at three time points: entry into investigation by child protective services, opening of a service case by the child welfare system, and entry into out-of-home care. A significant increase in the use of mental health services occurred immediately after the initial contact with child welfare, varying by level of child welfare involvement and leveling off by 3 months after the initial contact. The models indicated that children involved in child welfare at all three time points were more likely to receive mental health services after that involvement was initiated by an investigation, with rates of use directly related to level of involvement. Thus those in in-home care who received no further child welfare services after investigation were one-third as likely to use mental health services as those who were placed out of home, and those in in-home care receiving child welfare services after investigation were half as likely to use mental health services as those placed in out-of-home care. Based on these findings, the authors conclude that child welfare functions as a gateway into the mental health care system, with the size of the gateway increasing as the child enters more deeply into the child welfare system. Figure 5-13 shows this finding graphically.
As noted, NSCAW data have also been used to determine whether this increased use of mental health care by children involved in child welfare continues after involvement stops. Landsverk and colleagues (2010) examined the use of mental health services by youth after exiting from out-of-home care. The authors believed that because the movement into out-of-home care was found to be by far the largest gateway into the mental health system, examining continuity or discontinuity of mental health services after exit from out-of-home care would provide the strongest test of the offset hypothesis. Their findings were consistent across multiple tests using different longitudinal cohorts and varying statistical techniques for analyzing longitudinal mental health services. No tests showed that children reunified with their parents after out-of-home care subsequently used specialty mental health care less than children who remained in out-of-home care. In fact, one comparison demonstrated statistically significant greater use of such care for reunified children compared with children remaining in out-of-home care. In addition, the results suggested relatively high continuity of use of specialty mental health services in both groups of children. These findings are displayed graphically in Figure 5-14.
These findings strongly suggest that children’s involvement with the
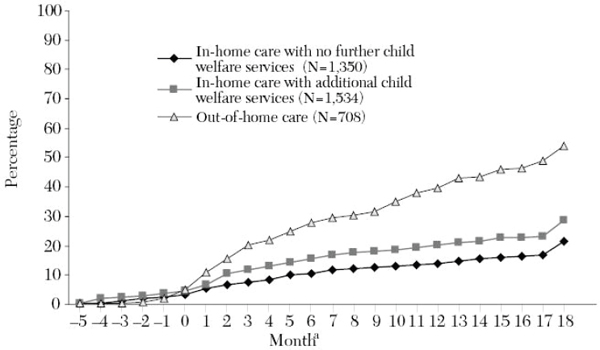
FIGURE 5-13 Cumulative percentage of mental health service use by level of child welfare involvement for a cohort of children investigated for possible child abuse or neglect (N = 3,592, weighted percents).
aPercentages are weighted. Time frame is from 5 months before the initial contact with child welfare to 18 months after the contact; time zero is contact date with child welfare.
SOURCE: Leslie et al., 2005 (reprinted with the permission of Scientific American).
child welfare system is positively associated with this high-risk population’s increased access to mental health care and that involvement with the child welfare system also is associated with high levels of continuity of mental health care. The association of increased access to and high continuity of mental health care with child welfare involvement also has been reported by Horwitz and colleagues (2010), who used different approaches to the NSCAW longitudinal study, making the evidence even stronger. To use the metaphor of a service system functioning as a gateway into another service system, the gateway into mental health care provided by the child welfare system clearly does not swing both ways. This finding lends support to the idea that the child welfare system can be positively conceptualized as a gateway system from a public health perspective (Garrison, 2004). If one thinks of the child protection system as a kind of surveillance system for risky parenting behaviors and the related heightened risk for the onset of emotional and behavioral problems in children, one can also think of the child welfare system as a gateway into other service systems that can address the higher rates of problems in children involved with the child
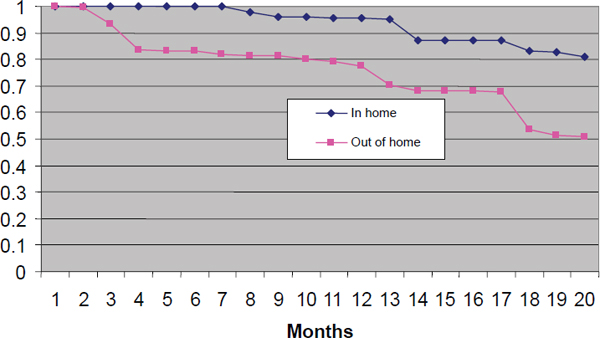
FIGURE 5-14 Survival curves for use of mental health services (N = 453).
SOURCE: Landsverk et al., 2010 (reprinted with the permission of Oxford University Press).
welfare system, especially given that continuity of mental health care is not contingent upon remaining in out-of-home care.
Quality of the mental health services received by children in the child welfare system While it has been shown that the child welfare system provides increased access to mental health care, it is important as well to assess whether children are receiving sufficient and appropriate forms of care to fully understand whether their needs are being met. That is, one must consider not only access and continuity but also the quality of the services being received. Access to ineffective or inappropriate mental health care provides no greater benefit to children than no access at all. Indeed, Bickman’s research on the impact of the systems of care model (Bickman, 1996; Bickman and Heflinger, 1995; Bickman et al., 1997) suggests that better access to care may not be associated with better outcomes for youth receiving care from public mental health systems.
Mental health care also may be inappropriate. For example, despite the clear evidence pointing to high rates of externalizing behavior problems in children involved with the child welfare system (see Chapter 4), much of the mental health care offered in public service systems is provided directly to children, whereas research evidence supports the use of parent training models designed to change parents’ response to the problematic behaviors exhibited by their children. Recently, Chamberlain and Fisher from the
Oregon Social Learning Center demonstrated promising outcomes from the use of multidimensional treatment foster care (Chamberlain, 2003; Chamberlain and Reid, 1991; Fisher and Kim, 2007; Fisher et al., 2005), while Chamberlain and colleagues have shown promising outcomes with relative and nonrelative foster parents with a modified version of this approach (Chamberlain et al., 2008a,b). This research is taking evidence-based mental health interventions directly into child welfare settings and shows great promise for enhancing child well-being by strengthening the response of substitute and biological parents to the behavioral problems of children and adolescents.
The National Child Traumatic Stress Network The National Child Traumatic Stress Network (NCTSN) was authorized in 2000 by the U.S. Congress as part of the Children’s Health Act. The original 17 centers have grown to more than 150 funded and affiliated centers located in diverse communities as well as within academic institutions in more than 40 states. The NCTSN is funded by the Substance Abuse and Mental Health Services Administration (SAMHSA) with HHS. Cumulatively funded since 2001 at more than $377 million and with an FY 2013 budget of $46 million, the NCTSN represents a well-established, multidisciplinary, trauma treatment services-based network with significant potential as a national child abuse and neglect/family trauma research infrastructure. Local NCTSN centers frequently have extensive partnerships with service organizations in their neighborhoods and are well positioned for community-based research.
The NCTSN consists of three types of funded centers and a wider range of affiliated centers, many of which were previously funded centers. The National Center for Child Traumatic Stress, collocated at Duke University and the University of Southern California, Los Angeles, has national partnerships with major professional and service organizations (the American Psychological Association, the National Council of Family Court Judges, Zero-to-Three, the Red Cross, and the Child Welfare League of America) and can coordinate multicenter studies.14 Its role is to develop and integrate the network structure, provide technical assistance to NCTSN centers, oversee resource development and product dissemination, and coordinate national educational and training efforts. Treatment and Services Adaptation Centers (Category II Centers) usually are academically affiliated and provide national expertise on specific types of traumatic events (e.g., child abuse and neglect, disaster, school crises) and/or work with specific populations (e.g., minorities, Native Americans, or immigrant groups) and/or systems (military, juvenile justice, child welfare). These centers develop and adapt existing evidence-based treatments for specific traumas, populations,
________________
14See http://www.nctsn.org/about-us/strategic-partnerships (accessed January 27, 2014).
and systems. The Community Treatment and Services Centers (Category III) implement and evaluate the treatment and services developed by the Category II Centers in their local communities. They also collaborate with other NCTSN centers on clinical issues, new approaches to service, and postgrant sustainability initiatives.
The NCTSN has a long track record of high-quality program evaluation and a core data system with detailed trauma histories on more than 14,000 children and adolescents. Forty percent of this sample have experienced four or more types of traumatic events and are at high risk for costly long-term outcomes. The majority of children, however, show improvement with treatment. Although the SAMHSA NCTSN grants do not include research funds, all NCTSN centers contribute data on their clients, services, and outcomes to a core dataset. Utilizing other funding, some NCTSN Category II Centers are conducting formal clinical trials and other trauma-related research.
Child Welfare and the Courts
Since the Adoption Assistance and Child Welfare Act of 1980 was enacted, the juvenile/family courts hearing abuse and neglect cases (often referred to as dependency courts) have played an increasingly active role in the child welfare system process. Once a child has been removed from home, if the child welfare agency is to have that child’s placement eligible for Title IV-E funding, certain “findings” must be made by the court and clearly recorded. These include findings that the child’s continuing to live in his/her home is contrary to the child’s welfare and that “reasonable efforts” have been made both to avoid placement and to speed reunification. Moreover, the 1980 law established a requirement for periodic judicial involvement as cases progress. Coupled with the Child Abuse Prevention and Treatment Act (CAPTA) requirement dating back to 1974 that every child in these cases must have an appointed lawyer, guardian ad litem, or court-appointed special advocate, these requirements have meant that in the past 40 years, the child welfare process has become far more guided by legal and judicial requirements than was previously the case.
Since the advent of the HHS-supported federal Court Improvement Program (CIP), interactions and coordination at the statewide level between the child welfare agency and the state’s high court administration have greatly increased. The state CIP, authorized under section 438 of the Social Security Act and established by the Omnibus Budget Reconciliation Act of 1993, provides annual grants to all 50 states, the District of Columbia, and Puerto Rico to improve dependency court proceedings in child welfare cases. Funds are awarded to the highest court in the state to assess foster care and adoption laws and judicial processes and to develop and implement plans for system improvement. Coordination activities between child
welfare agencies and the courts include joint agency-court training, linked agency-court data systems, one judge/one family models, time-specific docketing, and formalized relationships with the child welfare agency.15 Although each jurisdiction is required to conduct assessments, some have engaged in more intensive efforts that support the development of research infrastructure across the courts and the child welfare system. A national evaluation of the State CIP found that more than one-third of the states augmented their statewide management information systems; eight states targeted research and evaluations of court activities and reforms with CIP funds, addressing kinship placement, minority overrepresentation, large-scale reviews, or statistical analyses (National Evaluation of the Court Improvement Program, 2007). Technical assistance to support system reform efforts and research/evaluation between courts and child welfare agencies is provided by the National Council of Juvenile and Family Court Judges and the National Center on State Courts (Fiermonte and Sidote Salyers, 2005).
Over the years, many state CIP programs collaborated with tribes as required by the legislation and provided support for cross-trainings, ICWA conferences, and implementation of best practices. However, tribes were not eligible to apply directly for CIP funding. The Child and Family Services Improvement and Innovation Act of 2011,16 discussed earlier, created a new tribal CIP. Through this discretionary grant program, eligible tribes and tribal consortia17 will receive funds to enhance and improve tribal courts’ ability to handle child welfare cases. The law allocates $1 million annually for FY 2012-2016 for competitive grants.18 Activities include conducting assessments of tribal court child welfare proceedings; creating or revising child welfare or family code; enhancing court orders; addressing the handling of ICWA cases; providing training for judges, attorneys, and legal personnel in child welfare cases; and building infrastructure for the collection of court data or improving case management systems.19 Seven grants were awarded for FY 2012.20 As with the state CIP, the tribal CIP calls for third-party evaluations of project activities.
________________
15See http://www.acf.hhs.gov/programs/cb/resource/court-improvement-program (accessed January 27, 2014).
16P.L. 112-34.
17Eligible applicants are the highest courts of Indian tribes or tribal consortia that (1) are operating an approved Title IV-E Foster Care and Adoption Assistance Program, (2) have been awarded a tribal implementation grant (indicating that they are seeking to implement a Title IV-E plan), or (3) have a court responsible for proceedings related to foster care or adoption.
18ACF Tribal Consultation Response: Tribal Consultation for the Tribal Court Improvement Program.
19See http://www.acf.hhs.gov/grants/open/foa/view/HHS-2012-ACF-ACYF-CS-0323 (accessed January 27, 2014).
20See https://www.acf.hhs.gov/programs/cb/resource/discretionary-grant-awards-2012 (accessed January 27, 2014).
The state-level involvement demonstrated by the state CIPs has been replicated at the local level, particularly with courts designated “model courts” by the National Council of Juvenile and Family Court Judges (NCJFCJ). HHS also has for many years supported a National Child Welfare Resource Center on Legal and Judicial Issues through the American Bar Association’s Center on Children and the Law. During the past few years, the courts, through the work of the Resource Center and both NCJFCJ and the National Center for State Courts, have addressed such issues as how the courts can more effectively address such topics as child safety, racial disproportionality, and measurement of child well-being.
Despite these legal and judicial advances, one cannot state unequivocally that specific court reforms in child welfare cases are evidence-based practices. Greater support for program evaluation is needed to focus on how various court actions and reforms are related to child and family outcomes. For example, does providing higher-quality legal representation for parents accused of child abuse and neglect lead to better outcomes for both the child and family? How does the quality of legal representation for children, or for the child welfare agency, affect case outcomes? Do special types of court hearings (e.g., addressing mental health/trauma) help improve access to needed services?
Integration of Child Abuse and Substance Abuse Programs and Services
Another area of interagency collaboration and integration of programs and services with a rigorous evaluation component concerns the co-occurrence of child abuse and neglect and substance abuse and the associated risk or reality of out-of-home placement. The Child and Family Services Improvement Act of 2006 reauthorized the Promoting Safe and Stable Families program and provided funding over a 5-year period to implement a targeted program of grants to Regional Partnerships aimed at improving permanency outcomes for children affected by methamphetamine or other substance abuse. This legislation was enacted to address parental substance abuse as a key factor underlying the abuse or neglect experienced by many children in the child welfare system. In FY 2007, 53 Regional Partnership Grants were awarded to strengthen cross-system collaboration and service integration through a number of strategies, including family treatment drug courts, increased staffing to address shortages in both child welfare services and substance abuse treatment systems, reconciliation of conflicting time frames across legal and treatment systems to achieve outcomes, and use of evidence-based practices and delivery of trauma-informed services. The Child and Family Services Improvement and Innovation Act continues this collaborative emphasis and includes a targeted grants program (section 437(f) of the Social Security Act) for Regional Partnership Grants
to Improve the Well-Being of Children Affected by Substance Abuse.21 In FY 2012, the Children’s Bureau awarded 17 grants to grantees with demonstrated collaborative infrastructure in place across child welfare, substance abuse treatment and mental health agencies, and the courts.22 Along with tracking performance indicators that form the basis of the annual Report to Congress, grantees are required to implement evidence-based (or evidence-informed) and trauma-informed services/activities and to conduct rigorous impact evaluations of child and family outcomes.
Child Welfare: Systemic Issues
Casey Family Programs’ (2012) analysis of evidence-informed interventions to address common forms of child abuse and neglect identified many promising practices that need further testing and limited interventions that could be directly implemented by public child welfare agencies. In many instances, the need for specialized expertise or more intensive services for many of the evidence-based practices requires contracting out the services. PolicyLab of The Children’s Hospital of Philadelphia found that to implement the delivery of the two-tiered intervention of parent-child interaction therapy and child-adult relationship enhancement, it was necessary to build organizational/agency capacity, including collocation of behavioral health services with the foster care agency, training of local mental health providers, and identification of public Medicaid and child welfare dollars to support service delivery (Social Work Policy Institute, 2012a). As noted in Chapter 7, as well as in numerous other publications, child welfare agencies face many issues related to high caseloads, poorly trained staff, limited supervision, and a culture that does not necessarily support autonomy, quality practice, and critical thinking (GAO, 2003; Zlotnik et al., 2005).
Child welfare agencies face challenges regarding instability of leadership and funding streams, as well as workforce issues related to staff retention, competency, and supervision. Notable efforts to improve service delivery in child welfare agencies have included child welfare performance assessment and continuous quality improvement initiatives, as well as training and technical assistance strategies; however, more systematic evaluation and implementation of such efforts are needed.
________________
21The original grant program focused principally on the prevalence of methamphetamine use and its relation to child abuse and neglect.
22Note that this is another area in which the Children’s Bureau requires rigorous local evaluation and participation of grantees in a national evaluation. Reports to Congress on the current regional grants can be found on the Child Welfare Information Gateway at http://www.childwelfare.gov (accessed January 27, 2014).
Leadership
Among the many issues that can impact child abuse and neglect outcomes is the lack of stability of child welfare reforms. Leadership of child welfare agencies changes, perhaps as often as every 18 months, and new leaders bring new visions, new key staff, and new plans. Changes often occur when political leaders change, as the child welfare director responsible for child protection and other child welfare services may be a political appointee or hold a senior position under a political appointee. Because of this changing environment, the leadership qualities of middle managers in child welfare programs are also a concern. Indeed, one of the essential elements of the federally funded National Child Welfare Workforce Institute is the Leadership Academy for Middle Managers (www.ncwwi.org). Research has indicated that involving all levels of staff in leadership and planning efforts can help change the climate and culture of child welfare agencies.
Funding
Both federal and state funding of child protective services is subject to the current fiscal crisis and constraints on public support for human services. When funding is tight, money to support caseworker staff who conduct mandated investigations may be saved or even increased; however, some of the support programs that help improve child and family outcomes are cut or curtailed. This situation is especially problematic for prevention services and evidence-based practices that must follow a specific protocol and are predicated on being carried out by highly skilled staff. As noted in Chapter 8, the Child Abuse Prevention and Treatment Act’s appropriation has never come close to matching its authorization level, and child welfare agencies provide services by cobbling together local and state funds, along with funds from CAPTA, Titles IV-B and IV-E, and Title XX (Social Services Block Grant) of the Social Security Act, along with Temporary Assistance for Needy Families (TANF) and Medicaid funding. While the entitlement funds are not subject to appropriations, the Title IV-B and IV-E and Medicaid dollars are more oriented to children receiving foster care and adoption services—hence the appeal to many states, as previously discussed, to pursue Title IV-E waivers.
Front-Line Workforce and Supervision
Since the 1993 NRC report was published, an increasing body of research has focused on recruitment and retention of child welfare workers—those who serve as the key point of contact between children and families
and the child welfare system. It is increasingly understood that competent and committed workers with support from supervisors and with attention to the organizational culture and climate are critical to quality service delivery (GAO, 2003; Glisson and Hemmelgarn, 1997; Mor Barak et al., 2009; Social Work Policy Institute, 2011) and to the implementation of evidence-based programs (see Chapter 6).
Attention to workforce issues is essential in decision making related to child protection. For example, substantiation is closely tied to definitions of child abuse and neglect, the training and caseloads of the child protective services workforce, and the type and volume of reports received. As stated earlier in Chapter 2, the utilization of substantiation is questionable in practice. All states and territories have specific requirements for the initial response by agencies receiving reports of child abuse and neglect. In most states, a screening process is used to determine whether a report will be accepted, a process that includes a review of the report against the state’s definitions of child abuse and neglect. All states require that child protective services initiate an investigation in a timely manner, usually within 72 hours, and even sooner when there is reasonable cause to believe that the child is in imminent danger (CWIG, 2009). The outcomes of these assessments are dependent on the knowledge, skills, and caseload of the investigative workers, along with the supervision and support they receive from those above them. Reflecting workforce concerns, the 2010 reauthorization of the Child Abuse Prevention and Treatment Act23 includes a provision (Sec. 106(d)) that requires states “to include data on numbers of [child protective services] personnel, average caseloads, education and training requirements, demographic information, and workload requirements” in the plans they present to the federal agency.
In examining the connection among staff turnover, rates of reabuse, and child welfare system functioning, a California study found that counties with low rates of reabuse also had the lowest turnover rates and best-paid staff, as well as compliance with recognized practice standards (http://www.cpshr.us/workforceplanning/documents/06.02_Relation_Staff.pdf [accessed March 6, 2014]). A systematic review identified several personal and organizational factors that impact retention of child welfare staff (with recruitment considered an independent variable of retention). In addition, using a targeted strategy to educate social workers for child welfare careers is an effective strategy for bringing workers into the system, as well as linking them to the knowledge and skills required to do the work (Ellett et al., 2003; Zlotnik, 2009; Zlotnik et al., 2005). Research on retention indicates the following salient factors (see Figure 5-15):
________________
23P.L. 111-320.
• Personal factors
o commitment to child welfare,
o personal experience (age and being bilingual),
o previous experience,
o wanting to work with children and families, and
o goodness of fit.
• Organizational factors
o quality supervision,
o attributes of supervisors (e.g., skills in mentoring, high level of practice knowledge),
o manageable workload,
o peer support,
o feeling valued,
o opportunities for advancement,
o safety and resource availability, and
o salary and benefits.
Negative factors that decrease staff retention include the attributes of burnout, including emotional exhaustion, depersonalization, and lack of personal accomplishment; a negative organizational environment that can lead to or reinforce personal burnout factors; imbalance in work and family life; and lack of commitment that might be viewed as having no “goodness of fit.” Although a systemic review by the American Public Human Service Association (2005) found that states reported training as the most frequent strategy used to address retention, the review uncovered no studies examining the link between in-service training and retention. The most studied retention strategy was Title IV-E-supported education for master’s in social work (MSW) and/or bachelor’s in social work (BSW) students. Retained workers who have benefited from the specialized child welfare education and placement efforts cite self-efficacy, commitment to the agency, feeling valued, and special job title/position for those with social work degrees as important factors in their retention. Research indicates that those who participate in these programs tend to remain on the job longer. Other research has found that these IV-E graduates also facilitate better service outcomes for the children they work with and have a better understanding of the children and families served in the system (Zlotnik et al., 2005).
Although the systematic review of the American Public Human Service Association (2005) found that providing support for social workers to obtain BSW and MSW degrees to pursue child welfare careers is an effective strategy, the major funding source for its implementation is Title IV-E entitlement. Thus the focus is more on the administration of foster care than specifically on educating social workers to be child protective service
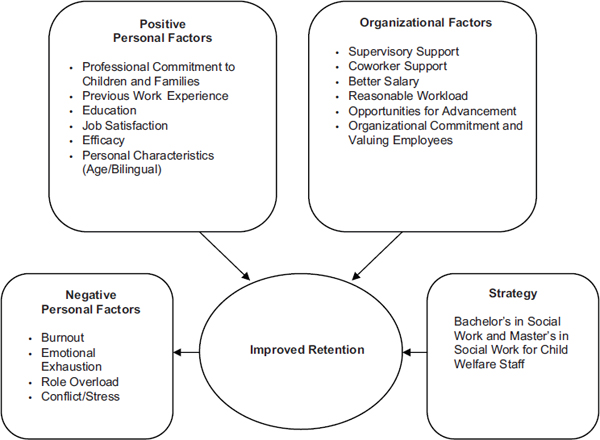
FIGURE 5-15 Strategies and conditions that influence the retention of staff in public child welfare.
SOURCE: Adapted with permission from Zlotnik et al., 2005.
investigators or on developing the clinical skills needed for protective service intervention (Social Work Policy Institute, 2012b).
Several states and counties have implemented some of the organizational change strategies that have been found to be evidence based and effective for addressing retention of child welfare staff. For example, Glisson and colleagues (2006) implemented the availability, responsiveness, and continuity (ARC) organizational intervention strategy in a combined child welfare and juvenile justice system in a southeastern state. They found that 39 percent of employees in case management teams that received the ARC intervention quit their jobs during the 1-year period following the intervention, compared with 65 percent of caseworkers in the control group during the same time period. The study also found that the ARC intervention improved the organizational climate, with caseworkers who participated in the entire intervention reporting lower levels of depersonalization, emotional exhaustion, role conflict, and role overload than their peers in the control group. Analysis of NSCAW data has linked engaged organizational climates in child welfare systems to greater psychosocial improvements for
children served by those systems compared with children served by caseworkers in less engaged organizational climates (Glisson, 2010; Glisson and Green, 2011). This is an area in which more research is needed, especially to understand the mechanisms of the links between practice outcomes and workforce issues. Furthermore, it should be recognized that, looking across all of the processes involved, child protection work is a multidisciplinary field, and evidence-based strategies are necessary to ensure competent, qualified staff in medicine, social work, nursing, early childhood, law, and other subject areas.
Need for Continuous Quality Improvement
Public child welfare agencies often must face negative media attention, which in turn puts pressure on politicians to take some form of action (Chenot, 2011). Exposés of child protection efforts following a high-profile death of a child can result in the firing of both agency heads and front-line workers. Child welfare agencies appear to be unable as yet to take the same approach used by hospitals—fully examining internally what went wrong and creating a learning organization to learn from those mistakes. Instead, highly visible changes are made that have repercussions for staff at all levels. Rzepnicki and colleagues (2010) suggest that child welfare agencies need to learn more about the practices of high-reliability organization and incorporate them into the delivery of child welfare services. Agencies seeking accreditation must carry out a program improvement process, but little information is available about the extent to which these efforts are well developed and implemented (Zayas et al., 2013). One of the changes since the 1993 NRC report has been the targeted effort in a number of states, working with the Council on Accreditation (http://www.coanet.org/programs/public-agency-accreditation [accessed March 6, 2014]), to use accreditation as a way to address workforce standards, caseload, supervision, and quality improvement and monitoring of services. The Children’s Bureau also has increased attention to continuous quality improvement by asking one of the resource centers to conduct an environmental scan of states to identify the processes they are using (http://www.acf.hhs.gov/programs/cb/news/continuous-quality-improvement [accessed March 6, 2014]), as well as by issuing an information memorandum in August 2012 (ACYF-CB-IM-12-07) to outline some expectations for continuous quality improvement efforts.
According to Zlotnik (2010, p. 328): “The barriers to establishing research, evaluation, and quality improvement departments in public child welfare agencies have prompted public administrators to seek out this expertise and to encourage its development by establishing and supporting partnerships with universities. These research partnerships also emerge
from a more general desire to forge tighter linkages between universities and child welfare departments in the training of students and staff for public service careers.” Lawrence and colleagues (2012) also note that it is difficult to design evaluations in child welfare agencies because of workforce turnover and organizational issues that impact workers’ intent to leave.
Performance Assessment of Child Welfare Agencies
Another key change since 1993 is that in 2000, the Children’s Bureau created the CFSR effort, which assesses how states are performing with respect to safety, permanency, and well-being outcomes; looks at how children and families are being served; and provides a process for improving performance. In the first round of the reviews (2001 to 2004), no state was found to be in substantial compliance, and the greatest gap in services was in serving children in their own homes. All states were required to implement Program Improvement Plans. The second round of reviews took place between 2007 and 2010.
The CFSRs measure seven outcomes and seven systemic factors. The outcomes measured include whether children under the care of the state are protected from abuse and neglect, whether children have permanency and stability in their living conditions, whether the continuity of family relationships and connections is preserved for children, whether families have enhanced capacity to provide for their children’s needs, and whether children receive adequate services to meet their physical and mental health needs. The systemic factors measured by the reviews include the effectiveness of the state’s systems for child welfare information, case review, and quality assurance; training of child welfare staff, parents, and other stakeholders; the array of services that support children and families; the agency’s responsiveness to the community; and foster and adoptive parent licensing, recruitment, and retention.
Results of the first 2 years of the second round of CFSRs, covering 32 states, indicated that foster care was more likely than in-home services to achieve outcomes and that services to mothers were stronger than services to fathers in relationship to the systemic factors that were assessed. With regard to safety, 22 percent of the cases had unaddressed safety concerns, including child abuse and neglect reports that were inappropriately screened out, child abuse and neglect allegations that were never formally reported or investigated, delays in accepting an allegation for investigation, and allegations that were not substantiated despite evidence that would support substantiation. With regard to permanency, findings indicated that concurrent planning—the pursuit of primary and secondary permanency options simultaneously from the child’s entry into the child welfare system (CWIG, 2012c)—was not implemented consistently or effectively. The reviews also
found that petitions for termination of parental rights were not necessarily filed in a timely fashion (as defined by the Adoption and Safe Families Act). With regard to well-being, some challenges were identified: educational services were not well coordinated; dental services were not necessarily available in the community; and mental and behavioral health services in the community were insufficient to meet the need or were assessed but not addressed, or delays were incurred because of waiting lists (ACF, 2012b). More information on the results of the CFSRs is available at http://www.acf.hhs.gov/programs/cb/resource/cfsr-compiled-results-2001-2010 (accessed March 6, 2014).
Training and Technical Assistance Strategies: Filling a Gap
Since the 1993 NRC report was issued, the Children’s Bureau has broadened its training and technical assistance strategy to work with states, counties, and tribes to improve child welfare practice and has convened states and tribes (including representatives from multiple agencies—child welfare, mental health, judicial, health, education) around critical issues (e.g., child fatality review, psychotropic medication, child welfare evaluation, workforce issues, prevention network). A complex network of close to 50 entities—including national resource centers, quality improvement centers, implementation centers, clearinghouses and information resources, institutes, and providers of services to grantees—is now engaged in the training and technical assistance endeavor (http://www.acf.hhs.gov/programs/cb/assistance [accessed March 6, 2014]). Many states also seek consultation from a broad range of fee-for-service experts, and Casey Family Programs, working with the top leadership in many states, has developed a strategic consulting effort to improve outcomes. In the face of all of this effort to achieve change, individual programs have been evaluated, but there has been no known analysis of how all of these efforts work synergistically to improve the lives and outcomes of children who experience child abuse and neglect.
Finding: Research to date has not provided a clear understanding of differences in the experiences of children in the child welfare system based on race, socioeconomic status, and culture.
Finding: Children involved with the child welfare system often come into contact with a number of other systems, such as the courts or various service providers. Cohesive interaction between the child welfare system and these other, related systems is critical for the well-being of at-risk children. The interaction of these various systems also provides an opportunity for conducting interdisciplinary child abuse and
neglect research that entails exploring systemic improvement through collaboration, aggregating data from multiple sources where abused and neglected children are seen, and understanding the relationship among cross-disciplinary outcomes.
Finding: The child welfare system functions as a gateway into the child mental health care system, and this increased access to mental health care is associated with high levels of continuity of mental health care even when children leave foster care. However, this improved access to care is not necessarily associated with improved child well-being outcomes, as the quality or type of care received may not adequately address a child’s needs. There has been a lack of rigorous research on the effectiveness, quality, and scope of care received by children in the child welfare system.
Finding: Evidence has shown that rates of use of mental health referral services among children in the child welfare system are influenced by both clinical factors and nonclinical factors, such as the type of child abuse or neglect experienced, racial/ethnic background, age, and type of placement. However, most research in the area has taken an epidemiologic approach that entails simply reporting rates of need for service and rates of service utilization. Limited analysis has addressed the relationship between need and use, the role of the many different influences on service utilization, and the efficacy of actual interventions and their outcomes.
Finding: The Court Improvement Program, integration of the provision of child abuse and substance use services, and the National Traumatic Stress Network represent notable efforts to improve collaborative service provision for abused and neglected children and to create multidisciplinary research infrastructures.
Finding: The delivery of effective, evidence-based services by child welfare agencies requires an administrative, leadership, and workforce capacity that is often lacking. Barriers to sufficient organizational capacity include issues related to reduced funding; high caseloads; poorly trained staff, especially staff who are not trained to address the social and emotional needs of the children who come in contact with the child protective services system; and limited staff supervision.
Finding: While certain organizational change strategies have been found to be evidence based and effective for improving workforce retention
in child welfare, more research in this area is needed, especially to link practice outcomes and workforce issues.
Finding: The evidence base is insufficient on effective strategies for bringing in the interdisciplinary knowledge necessary to carry out all the diverse functions of a child welfare agency, including experience in medicine, social work, nursing, early childhood, law, and other subject areas.
Finding: Child welfare agencies need to employ more effective quality improvement strategies. While agencies currently engage in a program improvement process, little evidence is available on the extent to which these processes are well developed, implemented, and sustained. These processes need to be thoroughly examined to determine the most successful strategies for quality improvement.
The societal response to child abuse and neglect is a complex one. Even before the passage of CAPTA (see Chapter 8), the public child welfare system was supported by the federal government and by states to respond to child abuse and neglect, with roles that ranged from responding to reports; to working with children and families; to strategizing on assessment, intervention, placement, and case disposition. This chapter has provided an overview of the children who come into contact with this complex child welfare system and framed the system’s policies and practices as ever changing to best focus on children’s safety, permanency, and well-being. Despite some progress, much remains to be done, and research is needed to connect what is found to work with the structures and processes that need to be addressed to implement evidence-based policy and practice in complex systems.
Improved access to empirical data from sources such as the NSCAW and the FCDA has led to a greater understanding of the experiences of children who come in contact with the child welfare system, which can help guide decision making and service delivery. However, further research is needed to fully understand important issues such as the impact of multiple foster care placements, especially the separate effects of movement patterns, the timing of moves, and movement between levels of care; differences in the experiences of children in the child welfare system based on race, socioeconomic status, and culture; and the impact of varying state administrative structures on the performance of the child welfare system.
Improved access to data also has enabled a more comprehensive examination of the impact of various child welfare system initiatives designed to improve performance with regard to the core goals of safety, permanency,
and well-being. While a growing body of evaluations has shown the benefits of strategies such as differential response, family and parent engagement, and the use of practice models, there is a need for more rigorous evaluations and an even greater need to evaluate strategies used to implement successful models across varying settings. As the focus of child welfare system initiatives continues to evolve based on changes to laws and administrative policies and responses to tragic events, the developing evidence base needs to be used to promote the implementation of programs and service delivery strategies that have proven effectiveness.
While research on the effectiveness of programs and the science of implementation offers insight into successful strategies for child welfare agencies to replicate, the potential benefits of such research cannot be realized without the institutional capacity to implement programs and service delivery strategies. Achieving this capacity requires reconsideration of the competency and commitment of front-line staff, a link between training and education and service delivery, a greater focus on leadership and organization, and greater alignment of the policies and practice imperatives that are presented to child welfare managers. In light of the many aspects of the causes and consequences of child abuse and neglect (see Chapters 3 and 4, respectively), it is necessary to integrate the multidisciplinary experience needed for child welfare service delivery and to coordinate with the various other systems and service providers that encounter abused and neglected children.
To meet the above research needs in the varying contexts of individual agencies and in the face of the difficulties associated with conducting research in large, complex systems, a research enterprise needs to be built within child welfare agencies. Doing so would allow for examination of the experiences of children in the child welfare system in relation to the implementation of programs in specific settings, as well as the promotion of strategies to improve institutional performance.
Aarons, G. A., S. James, A. R. Monn, R. Raghavan, R. S. Wells, and L. K. Leslie. 2010. Behavior problems and placement change in a national child welfare sample: A prospective study. Journal of the American Academy of Child and Adolescent Psychiatry 49(1):70-80.
ACF (Administration for Children and Families). 2000. Child welfare outcomes 1998: Annual report. Washington, DC: U.S. Department of Health and Human Services, Children’s Bureau.
ACF. 2002. Child welfare outcomes 1999: Annual report. Safety, permanency, well-being. Washington, DC: Administration for Children and Families.
ACF. 2007. Child maltreatment, 2007 report. Washington, DC: U.S. Department of Health and Human Services, ACF.
ACF. 2010. Child welfare outcomes 2007-2010: Report to Congress. Washington, DC: U.S. Department of Health and Human Services, Children’s Bureau.
ACF. 2011. Child welfare outcomes 2003-2006: Report to Congress. Washington, DC: U.S. Department of Health and Human Services, Children’s Bureau.
ACF. 2012a. The AFCARS report: Preliminary FY 2011 estimates as of July 2012. No. 19. Washington, DC: U.S. Department of Health and Human Services, Children’s Bureau.
ACF. 2012b. Results of the 2007 and 2008 child and family services reviews. http://www.acf.hhs.gov/programs/cb/resource/07-08-cfsr-results (accessed April 22, 2013).
ACF. 2012c. Child maltreatment, 2011 report. Washington, DC: U.S. Deparment of Health and Human Services, Children’s Bureau. http://www.acf.hhs.gov/sites/default/files/cb/cm11.pdf (accessed August 6, 2013).
American Humane. n.d. Quick reference guide: Various approaches and models to engage the family group in child welfare decision making. http://www.americanhumane.org/assets/pdfs/children/fgdm/quick-reference.pdf (accessed August 26, 2013).
American Public Human Services Association. 2005. Report from the 2004 Child Welfare Workforce Survey: State agency findings. Washington, DC: American Public Health Human Services Association.
Armstrong, M. I., A. C. Vargo, N. Jordan, T. King-Miller, C. Sowell, and S. Yampolskaya. 2008. Report to the legislature—evaluation of the department of children and families community-based care initiative fiscal year 2006-2007. Tallahassee: Florida Department of Children and Families.
ASPE (Assistant Secretary for Planning and Evaluation). 2008a. Evaluation of family preservation and reunification programs: Overview. http://aspe.hhs.gov/hsp/evalfampres94/ (accessed May 3, 2013).
ASPE. 2008b. Evolving roles of public and private agencies in privatized child welfare systems. Washington, DC: U.S. Department of Health and Human Services.
ASPE. 2009. Child welfare privatization initiatives. Assessing their implications for the child welfare field and the federal child welfare programs. http://aspe.hhs.gov/hsp/07/CWPI/ (accessed July 10, 2013).
Barillas, K. H. 2011. State capacity: The missing piece in child welfare privatization. Child Welfare 90(3):111-127.
Barth, R. P. 2005. Residential care: From here to eternity. International Journal of Social Welfare 14(3):158-162.
Barth, R. P., E. C. Lloyd, R. L. Green, S. James, L. K. Leslie, and J. Landsverk. 2007. Predictors of placement moves among children with and without emotional and behavioral disorders. Journal of Emotional and Behavioral Disorders 15(1):46-55.
Benedict, M. I., S. Zuravin, D. Brandt, and H. Abbey. 1994. Types and frequency of child maltreatment by family foster-care providers in an urban-population. Child Abuse & Neglect 18(7):577-585.
Berger, L. M., S. K. Bruch, E. I. Johnson, S. James, and D. Rubin. 2009. Estimating the “impact” of out-of-home placement on child well-being: Approaching the problem of selection bias. Child Development 80(6):1856-1876.
Berkoff, M. C., L. K. Leslie, and A. C. Stahmer. 2006. Accuracy of caregiver identification of developmental delays among young children involved with child welfare. Journal of Developmental & Behavioral Pediatrics 27(4):310-318.
Berrick, J. D., B. Needell, R. P. Barth, and M. Jonson-Reid. 1998. The tender years: Toward developmentally sensitive child welfare services for very young children. New York: Oxford University Press.
Bickman, L. 1996. Implications of a children’s mental health managed care demonstration evaluation. Journal of Mental Health Administration 23(1):107-117.
Bickman, L., and C. A. Heflinger. 1995. Seeking success by reducing implementation and evaluation failures. In Children’s mental health services: Research, policy, and evaluation, Vol. 1, edited by L. Bickman and D. J. Rog. Newbury Park, CA: Sage Publications. Pp. 171-205.
Bickman, L., W. T. Summerfelt, J. Firth, and S. Douglas. 1997. The stark county evaluation project: Baseline results of a randomized experiment. In Evaluating mental health services: How do programs for children “work” in the real world?, edited by D. Northrup and C. Nixon. Newbury Park, CA: Sage Publications. Pp. 231-258.
Billingsley, A., and J. M. Giovannoni. 1972. Children of the storm: Black children and American child welfare. New York: Harcourt, Brace and Jovanovich.
Casey Family Programs. 2012. Comparison of experiences in differential response (DR) implementation: 10 child welfare jurisdictions implementing DR. Seattle, WA: Casey Family Programs.
Chamberlain, P. 2003. The Oregon multidimensional treatment foster care model: Features, outcomes, and progress in dissemination. Cognitive and Behavioral Practice 10(4): 303-312.
Chamberlain, P., and J. B. Reid. 1991. Using a specialized foster care community treatment model for children and adolescents leaving the state mental hospital. Journal of Community Psychology 19(3):266-276.
Chamberlain, P., J. Price, L. D. Leve, H. Laurent, J. A. Landsverk, and J. B. Reid. 2008a. Prevention of behavior problems for children in foster care: Outcomes and mediation effects. Prevention Science 9(1):17-27.
Chamberlain, P., J. Price, J. Reid, and J. Landsverk. 2008b. Cascading implementation of a foster and kinship parent intervention. Child Welfare 87(5):27-48.
Chenot, D. 2011. The vicious cycle. Recurrent interactions among the media, politicians, the public, and child welfare services organizations. Journal of Public Child Welfare 5(2-3): 167-184.
Child Welfare League of America 2003. CWLA best practice guidelines: Child abuse and neglect in foster care. Washington, DC: Child Welfare League of America.
Children’s Bureau. 2012. Promising approaches. http://www.acf.hhs.gov/programs/cb/resource/promising-approaches (accessed November 27, 2012).
Cleveland, C. 2013. Who will protect state’s children? Chattanooga Times Free Press (Tennessee), May 2, 2013, E1.
Collins-Camargo, C., B. McBeath, and K. Ensign. 2011. Privatization and performance-based contracting in child welfare: Recent trends and implications for social service administrators. Administration in Social Work 35(5):494-516.
Coohey, C., K. Johnson, L. M. Renner, and S. D. Easton. 2013. Actuarial risk assessment in child protective services: Construction methodology and performance criteria. Children and Youth Services Review 35(1):151-161.
Courtney, M. E., and B. Needell. 1997. Outcomes of kinship care: Lessons from California. Child Welfare Research Review 2:130-150.
Cross, T. 2012. An overview of child maltreatment data in American Indian/Alaska Native communities. Presentation to the Committee on Child Maltreatment Research, Policy, and Practice for the Next Decade, December 10, Washington, DC. http://iom.edu/~/media/Files/Activity%20Files/Children/Child%20Maltreatment/cross.pdf (accessed August 7, 2013).
CWIG (Child Welfare Information Gateway). 2008. Systems of care. Washington, DC: U.S. Department of Health and Human Services, Children’s Bureau.
CWIG. 2009. Making and screening reports of child abuse and neglect: Summary of state laws. Washington, DC: U.S. Department of Health and Human Services, Children’s Bureau.
CWIG. 2012a. Engaging families in case planning. Washington, DC: U.S. Department of Health and Human Services, Children’s Bureau.
CWIG. 2012b. Tribal-state relations. Washington, DC: U.S. Department of Health and Human Services, Children’s Bureau.
CWIG. 2012c. Concurrent planning: What the evidence shows. Washington, DC: U.S. Department of Health and Human Services, Children’s Bureau. https://www.childwelfare.gov/pubs/issue_briefs/concurrent_evidence/concurrent_evidence.pdf (accessed August 16, 2013).
CWIG. 2013a. Grounds for involuntary termination of parental rights. Washington, DC: U.S. Department of Health and Human Services, Children’s Bureau.
CWIG. 2013b. How the child welfare system works. Washington, DC: U.S. Department of Health and Human Services, Children’s Bureau.
CWIG. 2013c. Structured decision making. https://www.childwelfare.gov/systemwide/assessment/approaches/decision.cfm (accessed June 14, 2013).
D’andrade, A., M. J. Austin, and A. Benton. 2008. Risk and safety assessment in child welfare: Instrument comparisons. Journal of Evidence-Based Social Work 5(1-2):31-56.
dosReis, S., J. M. Zito, D. J. Safer, and K. L. Soeken. 2001. Mental health services for youths in foster care and disabled youths. American Journal of Public Health 91(7):1094-1099.
Dozier, M., M. Manni, M. K. Gordon, E. Peloso, M. R. Gunnar, K. C. Stovall-McClough, D. Eldreth, and S. Levine. 2006. Foster children’s diurnal production of cortisol: An exploratory study. Child Maltreatment 11(2):189-197.
Drake, B., and M. Johnson-Reid. 2010. NIS interpretations: Race and the national incidence studies of child abuse and neglect. Children and Youth Services Review 33(1):309-316.
Drake, B., S. L. Lee, and M. Jonson-Reid. 2009. Race and child maltreatment reporting: Are blacks overrepresented? Children and Youth Services Review 31(3):309-316.
Earle, K. 2000. Child abuse and neglect: An examination of American Indian data. Seattle, WA: Casey Family Programs.
Ellett, A. J., C. D. Ellett, and J. K. Rugutt. 2003. A study of personal and organizational factors contributing to employee retention and turnover in child welfare in Georgia: Final report. Athens, GA: University of Georgia School of Social Work.
Fahlberg, V. I. 1991. A child’s journey through placement. Indianapolis, IN: Perspectives Press.
Fiermonte, C., and N. Sidote Salyers. 2005. Improving outcomes together: Court and child welfare collaboration. Urbana-Champaign: Children and Family Research Center, School of Social Work, University of Illinois at Urbana-Champaign.
Fisher, P. A., and H. K. Kim. 2007. Intervention effects on foster preschoolers’ attachment-related behaviors from a randomized trial. Prevention Science 8(2):161-170.
Fisher, P. A., M. R. Gunnar, P. Chamberlain, and J. B. Reid. 2000. Preventive intervention for maltreated preschool children: Impact on children’s behavior, neuroendocrine activity, and foster parent functioning. Journal of the American Academy of Child & Adolescent Psychiatry 39(11):1356-1364.
Fisher, P. A., B. Burraston, and K. Pears. 2005. The early intervention foster care program: Permanent placement outcomes from a randomized trial. Child Maltreatment 10(1):61-71.
Flaherty, C., C. Collins-Camargo, and E. Lee. 2008. Privatization of child welfare services: Lessons learned from experienced states regarding site readiness assessment and planning. Children and Youth Services Review 30(7):809-820.
Flower, C., J. McDonal, and M. Sumski. 2005. Review of turnover in Milwaukee county private agency child welfare ongoing case management staff. Milwaukee, WI: Bureau of Milwaukee Child Welfare.
Fluke, J., B. J. Harden, M. Jenkins, and A. Ruehrdanz. 2011. A research synthesis on child welfare disproportionality and disparities. In Disparities and disproportionality in child welfare: Analysis of the research. Denver, CO: American Humane Association and the Annie E. Casey Foundation. Pp. 1-93.
Freisthler, B., P. J. Gruenewald, L. G. Remer, B. Lery, and B. Needell. 2007. Exploring the spatial dynamics of alcohol outlets and Child Protective Services referrals, substantiations, and foster care entries. Child Maltreatment 12(2):114-124.
GAO (Government Accountability Office). 2003. Child welfare: HHS could play a greater role in helping child welfare agencies recruit and retain staff. Washington, DC: GAO.
GAO. 2007. African American children in foster care: Additional HHS assistance needed to help states reduce the proportion in care. Washington, DC: GAO.
Garbarino, J., and A. Crouter. 1978. Defining the community context for parent-child relations: The correlates of child maltreatment. Child Development 49(3):604-616.
Garrison, M. 2004. Reforming child protection: A public health perspective. Virginia Journal of Social Policy and the Law 12:590.
Glisson, C. 2010. Organizational climate and service outcomes in child welfare settings. In Child welfare and child well-being: New perspectives from the national survey of child and adolescent well-being, edited by M. B. Webb, K. Dowd, B. J. Harden, J. Landsverk, and M. Testa. New York: Oxford University Press. Pp. 380-408.
Glisson, C., and P. Green. 2011. Organizational climate, services, and outcomes in child welfare systems. Child Abuse & Neglect 35(8):582-591.
Glisson, C., and A. Hemmelgarn. 1997. The effects of organizational climate and inter-organizational coordination on the quality and outcomes of children’s service systems. Child Abuse & Neglect 22(5):401-421.
Glisson, C., D. Dukes, and P. Green. 2006. The effects of the ARC organizational intervention on caseworker turnover, climate, and culture in children’s service systems. Child Abuse & Neglect 30(8):855-880.
Green, H. 2005. Mental health of children and young people in Great Britain, 2004. Palgrave Macmillan Basingstoke.
Gunnar, M. R., and P. A. Fisher. 2006. Bringing basic research on early experience and stress neurobiology to bear on preventive interventions for neglected and maltreated children. Development and Psychopathology 18(3):651-677.
Gunnar, M. R., M. H. Van Dulmen, T. Achenbach, E. Ames, E. Ames, M. Berry, R. Barth, G. Bohlin, L. Janols, and M. Bohman. 2007. Behavior problems in postinstitutionalized internationally adopted children. Development and Psychopathology 19(1):129.
Harman, J. S., G. E. Childs, and K. J. Kelleher. 2000. Mental health care utilization and expenditures by children in foster care. Archives of Pediatrics & Adolescent Medicine 154(11):1114.
Haskins, R., and J. Baron. 2011. Building the connection between policy and evidence: The Obama evidence-based initiatives. London: NESTA.
Haskins, R., F. Wulczyn, and M. B. Webb, eds. 2007. Child protection: Using research to improve policy and practice. Washington, DC: Brookings Institution Press.
Hill, R. B. 2006. Synthesis of research on disproportionality in child welfare: An update. Washington, DC: Casey-Center for the Study of Social Policy (CSSP) Alliance for Racial Equity in the Child Welfare System. http://www.cssp.org/reform/child-welfare/other-resources/synthesis-of-research-on-disproportionality-robert-hill.pdf (accessed June 11, 2013).
Hines, A. M. , K. Lemon, P. Wyatt, and J. Merdinger. 2004. Factors related to the disproportionate involvement of children of color in the child welfare system: A review and emerging themes. Children and Youth Services Review 26(6):507-527.
Horwitz, S. M., M. S. Hurlburt, and Z. Zhang. 2010. Patterns and predictors of mental health services use by children in contact with the child welfare system. In Child welfare and child wellbeing: New perspectives from the National Survey of Child and Adolescent Well-Being, edited by M. B. Webb, K. Dowd, B. J. Harden, J. A. Landsverk, and M. F. Testa. New York: Oxford University Press. Pp. 279-329.
Horwitz, S. M., M. S. Hurlburt, S. D. Cohen, J. Zhang, and J. Landsverk. 2011. Predictors of placement for children who initially remained in their homes after an investigation for child abuse and neglect. Child Abuse & Neglect 35(3):188-198.
IOM (Institute of Medicine). 2003. Unequal treatment: Confronting racial and ethnic disparities in health care. Washington, DC: The National Academies Press.
James, S., J. Landsverk, and D. J. Slymen. 2004. Placement movement in out-of-home care: Patterns and predictors. Children and Youth Services Review 26(2):185-206.
Jee, S. H., R. P. Barth, M. A. Szilagyi, P. G. Szilagyi, M. Aida, and M. M. Davis. 2006. Factors associated with chronic conditions among children in foster care. Journal of Health Care for the Poor and Underserved 17(2):328-341.
Jones, B. J., J. A. Gillette, D. Painte, and S. Paulson. 2000. Indian Child Welfare Act: A pilot study of compliance in North Dakota. Washington, DC: Casey Family Programs. http://www.nicwa.org/resources/research/?p=Research_Docs_170 (accessed June 24, 2013).
Kaplan, C., and L. Merkel-Holguin. 2008. Another look at the National Study on Differential Response in Child Welfare. Protecting Children 23(1-2):5-21.
Kaufman, L., and R. L. Jones. 2003. Trenton finds abuse high in foster care. The New York Times, April 16.
Kim, A. K., D. Brooks, H. Kim, and J. Nissly. 2008. Structured Decision Making® and child welfare service delivery project. Berkeley: University of California at Berkeley, California Social Work Education Center (http://www.csulb.edu/projects/ccwrl/Brooks.pdf (accessed August 27, 2013).
Kurtz, P. D., J. M. Gaudin, P. T. Howing, and J. S. Wodarski. 1993. The consequences of physical abuse and neglect on the school age child: Mediating factors. Children and Youth Services Review 15(2):85-104.
Landsverk, J., and F. Wulczyn. 2013 (unpublished). Child placement as a response to child abuse and neglect. Paper commissioned by the Committee on Child Maltreatment Research, Policy, and Practice for the Next Decade, IOM, Washington, DC.
Landsverk, J. A., A. F. Garland, and L. K. Leslie. 2002. Mental health services for children reported to Child Protective Services. In ASPAC handbook on child maltreatment, edited by J. E. B. Myers, H. C. T., L. Berliner, C. Jenny, J. Briere, and T. Reid. Thousand Oaks, CA: Sage Publications. Pp. 487-507.
Landsverk, J., M. Hurlburt, S. Horwitz, J. Rolls Reutz, and J. Zhang. 2009. Children and familes involved in child welfare and remaining in home after investigation for child abuse and neglect: Findings from the National Survey of Child Adolescent Well-Being (NSCAW). Baltimore, MD: Annie E. Casey Foundation.
Landsverk, J., M. Hurlburt, L. Leslie, J. Rolls-Reutz, and J. Zhang. 2010. Exits from out-of-home care and continuity of mental health services use. In Child welfare and child well-being: New perspectives from the National Survey of Child and Adolescent Well-Being edited by M. B. Webb, K. Dowd, B. J. Harden, J. Landsverk, and M. F. Testa. New York: Oxford University Press. Pp. 330-350.
Lawrence, C. K., J. Strolin-Goltzman, J. Caringi, N. Claiborne, M. McCarthy, E. Butts, and K. O’Connell. 2012. Evaluation in child welfare organizations. Administration in Social Work 37(1):3-13.
Lawrence, C. R., E. A. Carlson, and B. Egeland. 2006. The impact of foster care on development. Development and Psychopathology 18(1):57-76.
Layzer, J. I., B. D. Goodson, L. Bernstein, and C. Price. 2001. National evaluation of family support programs. Final report, Vol. A. Cambridge, MA: Abt Associates.
Lee, S., S. Aos, E. Drake, A. Pennucci, M. Miller, and L. Anderson. 2012. Return on investment: Evidence-based options to improve statewide outcomes technical appendix. Washington State Institute for Public Policy http://www.wsipp.wa.gov/Reports/322 (accessed August 25, 2013).
Lery, B. 2009. Neighborhood structure and foster care entry risk: The role of spatial scale in defining neighborhoods. Children and Youth Services Review 31(3):331-337.
Leslie, L. K., M. S. Hurlburt, S. James, J. Landsverk, D. J. Slymen, and J. Zhang. 2005. Relationshiop between entry into child welfare and mental health service use. Psychiatric Services 56(8):981-987.
Lieberman, A. 1987. Separation in infancy and toddlerhood: Contributions of attachment theory and psychoanalysis. The Psychology of Separation and Loss: Perspectives on Development, Life Transitions, and Clinical Practice 109-135.
Loman, L. A., and G. L. Siegel. 2004. Differential response in Missouri after five years: Final report. St. Louis, MO: Institute of Applied Research.
Loman, L. A., and G. L. Siegel. 2012. Ohio alternative response evaluation extension: Interim report. St. Louis, MO: Institute of Applied Research.
Loman, L. A., C. S. Filonow, and G. Siegel. 2010. Ohio alternative response evaluation: Final report with technical appendix. St. Louis, MO: Institute of Applied Research.
Marts, E. J., E. K. O. Lee, R. Mcroy, and J. McCroskey. 2008. Point of engagement: Reducing disproportionality and improving child and family outcomes. Child Welfare 87(2):335-358.
McCown, F. S. 2005. Privatization of Child Protective Services. Austin, TX: Center for Public Policy Priorities. http://library.cppp.org/files/4/privatization_pb.pdf (accessed August 27, 2013).
McCroskey, J., and W. Meezan. 1998. Family-centered services: Approaches and effectiveness. The Future of Children 8(1):54-71.
McCroskey, J., P. Pecora, T. Franke, C. Christie, and J. Lorthridge. 2012. Can public child welfare help to prevent child maltreatment? Promising findings from Los Angeles. Journal of Family Strengths 12(1):1-23. http://digitalcommons.library.tmc.edu/jfs/vol12/iss1/5 (accessed August 6, 2013).
Merkel-Holguin, L., C. Kaplan, and A. Kwak. 2006. National study on differential response in child welfare. Washington, DC: Child Welfare League of America.
Mor Barak, M. E., D. J. Travis, H. Pyun, and B. Xie. 2009. The impact of supervision on worker outcomes: A meta analysis. Social Service Review 83(1):3-32.
National Evaluation of the Court Improvement Program. 2007. The national evaluation of the Court Improvement Program (CIP): Synthesis of 2005 Court Improvement Program reform and activities-final report. Washington, DC: U.S. Department of Health and Human Services. https://docs.google.com/viewer?a=v&q=cache:2e88RgueWEQJ:www.pal-tech.com/cip/files/FirstSynthesis.pdf+national+CIP+evaluation+final+report&hl=en&gl=us&pid=bl&srcid=ADGEEShtnHYZqHLyzoRzJZFouKT0ZaE9BRPT_IrFnBfc5l2fLhshHU9-kxuy5N73plkZeVTIu9WFrPaJHZ4Wq7DZX04V-m13is08bEyHm9tbdFpoZDxb7vhL_c-yAlKxdSUZG_r_PVGA&sig=AHIEtbQKNjVeY9esdv_MeGJZ-1f1AzIVTg (accessed June 13, 2013).
NCCD (National Council on Crime and Delinquency). 2013. Structured Decision Making (SDM) system. http://www.nccdglobal.org/assessment/structured-decision-making-sdm-system (accessed May 3, 2013).
NCSL (National Conference of State Legislatures). 2012. Mandatory reporting of child abuse and neglect: 2012 introduced state legislation (review from). http://www.ncsl.org/issues-research/human-services/2012-child-abuse-mandatory-reporting-bills.aspx (accessed December 3, 2013).
Needell, B., M. A. Brookhart, and S. Lee. 2003. Black children and foster care placement in California. Children and Youth Services Review 25(5-6):393-408.
Newton, R. R., A. J. Litrownik, and J. A. Landsverk. 2000. Children and youth in foster care: Disentangling the relationship between problem behaviors and number of placements. Child Abuse & Neglect 24(10):1363-1374.
NRC (National Research Council). 1993. Understanding child abuse and neglect. Washington, DC: National Academy Press.
OPRE (Office of Planning, Research, and Evaluation). 2013. National Survey of Child and Adolescent Well-Being (NSCAW), 1997-2013: Project overview. http://www.acf.hhs.gov/programs/opre/research/project/national-survey-of-child-and-adolescent-well-being-nscaw-1 (accessed February 15, 2013).
Osterling, K. L., A. D’Andrade, and M. J. Austin. 2008. Understanding and addressing racial/ethnic disproportionality in the front end of the child welfare system. Journal of Evidence-Based Social Work 5(1-2):9-30.
Palmer, S. E. (1996). Placement stability and inclusive practice in foster care: An empirical study. Children and Youth Services Review 18(7):589-601.
Pardeck, J. T. 1984. Multiple placement of children in foster family care: An empirical analysis. Social Work 29(6):506-509.
Pardeck, J. T. 1985. A profile of the child likely to experience unstable foster care. Adolescence 20(79):689-696.
Pardeck, J. T., J. W. Murphy, and L. Fitzwater. 1985. Profile of the foster child likely to experience unstable care: A re-examination. Early Child Development and Care 22(2-3): 137-146.
Patel, D., P. Matyanga, T. Nyamundaya, D. Chimedza, K. Webb, and B. Engelsmann. 2012. Facilitating HIV testing, care and treatment for orphans and vulnerable children aged five years and younger through community-based early childhood development playcentres in rural Zimbabwe. Journal of the International AIDS Society 15(Suppl 2):17404.
Pennell, J., and G. Burford. 2000. Family group decision making: Protecting children and women. Child Welfare 79(2):131-158.
Poertner, J., M. Bussey, and J. Fluke. 1999. How safe are out-of-home placements? Children and Youth Services Review 21(7):549-563.
Polinsky, M. L., L. Pion-Berlin, S. Williams, T. Long, and A. M. Wolf. 2010. Preventing child abuse and neglect: A national evaluation of parents anonymous groups. Child Welfare 89(6):43-62.
Proch, K., and M. A. Taber. 1985. Placement disruption: A review of research. Children and Youth Services Review 7(4):309-320.
Provence, S. 1989. Infants in institutions revisited. Zero to Three 9(4):1-4.
QIC-DR (National Quality Improvement Center on Differential Response in Child Protective Services). 2011. Differential response in Child Protective Services: A literature review. Version 2. CRDA Number: 93:670. Washington, DC: U.S. Department of Health and Human Services, Children’s Bureau.
QIC-DR. 2012. Differential response approach in Child Protective Services: An analysis of state legislative provisions. Denver, CO: QIC-DR.
Redding, R. E., C. Fried, and P. A. Britner. 2000. Predictors of placement outcomes in treatment foster care: Implications for foster parent selection and service delivery. Journal of Child and Family Studies 9(4):425-447.
Ringeisen, H., C. Casanueva, M. Urato, and T. Cross. 2008. Special health care needs among children in the child welfare system. Pediatrics 122(1):e232-e241.
Rivaux, S. L., J. James, K. Wittenstrom, D. Baumann, J. Sheets, J. Henry, and V. Jeffries. 2008. The intersection of race, poverty, and risk: Understanding the decision to provide services to clients and to remove children. Child Welfare 87(2):151-168.
Rosner, D., and G. Markowitz. 1997. Race, foster care, and the politics of abandonment in New York City. American Journal of Public Health 87(11):1844-1849.
Ruppel, J., Y. Huang, and G. Haulenbeek. 2011. Differential response in child protective services in New York state. New York: New York State Office of Children and Family Services.
Rzepnicki, T. L., P. R. Johnson, D. Kane, D. Moncher, L. Coconato, and B. Shulman. 2010. Transforming child protection agencies into high reliability organizations: A conceptual framework. Protecting Children 25(1):48-62.
Sanders, D. 2012. Presentation at the Child Maltreatment, Research, Policy, and Practice for the Next Decade Workshop, January 31, 2012, Washington, DC.
Schwalbe, C. S. 2008. Strengthening the integration of actuarial risk assessment with clinical judgment in an evidence based practice framework. Children and Youth Services Review 30(12):1458-1464.
Sedlak, A. J., K. McPeherson, and B. Dias. 2010. Supplementary analyses of race differences in child child abuse and neglect rates in the NIS-4. Rockville, MD: Westat, Inc.
Shlonsky, A., and D. Wagner. 2005. The next step: Integrating actuarial risk assessment and clinical judgment into an evidence-based practice framework in CPS case management. Child and Youth Services Review 27(4):409-427.
Siegel, G. L., and L. A. Loman. 2006. Extended follow up study of Minnesota’s Family Assessment Response: Final report. St. Louis, MO: Institute of Applied Research.
Siegel, G. L., C. S. Filonow, and L. A. Loman. 2010. Differential response in Nevada. St. Louis, MO: Institute of Applied Research.
Smith, D. K., E. Stormshak, P. Chamberlain, and R. B. Whaley. 2001. Placement disruption in treatment foster care. Journal of Emotional and Behavioral Disorders 9(3):200-205.
Social Work Policy Institute. 2011. Supervision: The safety net for front-line child welfare practice. http://www.socialworkpolicy.org/wp-content/uploads/2011/03/SWPI-ChildWelfare-Supervision-Final-Report.pdf (accessed December 3, 2013).
Social Work Policy Institute. 2012a. Children at risk: Optimizing health in an era of reform. Washington, DC: National Association of Social Workers. http://www.socialworkpolicy.org/wp-content/uploads/2012/06/childrenatrisk-report1.pdf (accessed August 15, 2013).
Social Work Policy Institute. 2012b. Educating social workers for child welfare practice: The status of using Title IV-E funding to support BSW & MSW education. Washington, DC: National Association of Social Workers. http://www.socialworkpolicy.org/wp-content/uploads/2013/01/SWPI-IVE-Policy-Brief.pdf (accessed August 15, 2013).
Staff, I., and E. Fein. 1995. Stability and change: Initial findings in a study of treatment foster care placements. Children and Youth Services Review 17(3):379-389.
Stahmer, A. C., L. K. Leslie, M. Hurlburt, R. P. Barth, M. B. Webb, J. Landsverk, and J. Zhang. 2005. Developmental and behavioral needs and service use for young children in child welfare. Pediatrics 116(4):891-900.
Stovall, K., and M. Dozier. 1998. Infants in foster care: An attachment theory perspective. Adoption Quarterly 2(1):55-88.
Sullivan, D. J., and M. A. van Zyl. 2008. The well-being of children in foster care: Exploring physical and mental health needs. Children and Youth Services Review 30(7):774-786.
Summers, A., S. Wood, and J. Russell. 2012. Disproportionality rates for children of color in foster care. http://www.ncjfcj.org/sites/default/files/Disproportionality%20Rates%20for%20Children%20of%20Color%202010.pdf (accessed June 24, 2013).
Terling-Watt, T. 2001. Permanency in kinship care: An exploration of disruption rates and factors associated with placement disruption. Children and Youth Services Review 23(2): 111-126.
Testa, M. F. 2010. Flexibility, innovation, and experimentation: The rise and fall of child welfare waiver demonstrations. In Fostering accountablilty: Using evidence to guide and improve child welfare policy, edited by M. F. Testa and J. Poertner. New York: Oxford University Press. Pp. 269-290.
Testa, M. F. 2012. Fostering innovation through Title IV-E waiver demonstrations. Policy and Practice 70(3):28-30, 48.
Tittle, G., J. Poertner, and P. Garnier. 2001. Child maltreatment in foster care: A study of retrospective reporting. Urbana, IL: Children and Family Research Center.
Tittle, G., J. Poertner, and P. Garnier. 2008. Child maltreatment in out of home care: What do we know now? Urbana: Children and Family Research Center, School of Social Work, University of Illinois at Urbana-Champaign.
Usher, C. L., K. A. Randolph, and H. C. Gogan. 1999. Placement patterns in foster care. Social Service Review 73(1):22-36.
Walsh, J. A., and R. A. Walsh. 1990. Studies of the maintenance of subsidized foster placements in the Casey Family Program. Child Welfare 69(2):99-114.
Webb, M. B., K. Dowd, B. Jones Harden, J. Landsverk, and M. Testa. 2010. Child welfare and child well-being: New perspectives from the National Survey of Child and Adolescent Well-Being. New York: Oxford University Press.
Widom, C. S. 1991. Avoidance of criminality in abused and neglected children. Psychiatry: Journal for the Study of Interpersonal Processes 54(2):162-174.
Winokur, M., A. Holten, and D. Valentine. July 2009. Kinship care for the safety, permanency, and well-being of children removed from the home for maltreatment. Cochrane Database of Systematic Reviews (1):CD006546.
Wulczyn, F. 1986. Child welfare caseloads: A sociological interpretation. Unpublished doctoral dissertation, University of Chicago.
Wulczyn, F. 2012. Multistate foster care data archive. Chicago: Center for State Child Welfare Data, Chapin Hall, University of Chicago.
Wulczyn, F., L. Chen, and K. B. Hislop. 2007. Foster care dynamics, 2000-2005: A report from the multistate foster care data archive. Chicago: Chapin Hall Center for Children, University of Chicago.
Wulczyn, F., L. Chen, L. Collins, and M. Ernst. 2011. The foster care baby boom revisited: What do the numbers tell us? Zero to Three 31(3):4-10.
Wulczyn, F., R. Gibbons, L. Snowden, and B. Lery. 2013. Poverty, social disadvantage and the black/white placement gap. Child and Youth Services Review 35(1):65-74.
Yampolskaya, S., R. I. Paulson, M. Armstrong, N. Jordan, and A. C. Vargo. 2004. Child welfare privatization: Quantitative indicators and policy issues. Evaluation Review 28(2): 87-103.
Yang, K. F., and G. van Landingham. 2012. How hollow can we go? A case study of the Florida’s efforts to outsource oversight of privatized child welfare services. American Review of Public Administration 42(5):543-561.
Zayas, L. E., J. C. McMillen, M. Y. Lee, and S. J. Books. 2013. Challenges to quality assurance and improvement efforts in behavioral health organizations: A qualitative assessment. Administration and Policy in Mental Health and Mental Health Services Research 40(3):190-198.
Zlotnik, J. L. 2009. Social work and child welfare: A national debate. University of Michigan Fauri Lecture, October 27, Ann Arbor, MI.
Zlotnik, J. L. 2010. Fostering and sustaining university/agency partnerships. In Fostering accountability: Using evidence to guide and improve child welfare policy, edited by M. F. Testa and J. Poertner. New York: Oxford University Press. Pp. 328-356.
Zlotnik, J. L., D. DePanfilis, C. Daining, and M. M. Lane. 2005. Factors influencing recruitment and retention of child welfare workers: A systematic review of research. Washington, DC: Institute for the Advancement of Social Work Research. http://www.socialworkpolicy.org/wp-content/uploads/2007/06/4-CW-SRRFinalFullReport.pdf (accessed August 6, 2013).
Zuravin, S. J., M. Benedict, and M. Somerfield. 1993. Child maltreatment in family foster-care. American Journal of Orthopsychiatry 63(4):589-596.





































































