
Health Management and Promotion
Another major use of technology is for health management and promotion. Joseph Agostini, senior medical director at Aetna Medicare, cited two examples of health monitoring among this group to draw broader lessons about opportunities and continuing barriers. Carolee Winstein, director of the Optimizing Participation through Technology Rehabilitation Engineering Research Center at the University of Southern California, analyzed four factors that together are forestalling the onset of disability. And Timothy Bickmore, associate professor in the Department of Computer and Information Science at Northeastern University, described a particular technology he has helped develop to improve interactions with patients. Such applications will continue to proliferate as the population ages and technology advances.
Joseph V. Agostini, M.D.
Aetna Medicare
Ideally, geriatric care management is a holistic, integrated experience characterized by dedicated teams, prevention of disease, chronic disease management, risk management, and responses to major health events. It matches tools, resources, benefits, and care management programs to improve health outcomes. It sees the whole person physically, intellectually, emotionally, and financially. Agostini used two examples of health monitoring in older populations to derive a broader set of lessons learned.
Aetna Hypertension Program
Agostini stated that high blood pressure affects about two-thirds of people who reach Medicare age, and 50 percent of people are inadequately or suboptimally treated for the condition. The Aetna Hypertension Program offers an automated blood pressure monitor at no cost to people who volunteer for the program. Once a month, in response to an interactive voice response call, participants record their blood pressure and enter their results along with answers to a series of questions over the phone. They also receive supplementary educational mailings about hypertension, conditions associated with hypertension such as hyperlipidemia, and other topics. If participants have an out-of-range blood pressure, they get immediate feedback from a nurse case manager. The goal is to encourage self-management over time. As people gather data and enter information into the phone, they learn about their blood pressure and about things they can do to manage their condition.
A review of the program found that about 18 percent of people who started in the program moved from out-of-control blood pressure to in-control blood pressure by the end of the study (Wade et al., 2010). Low density lipoprotein (LDL) screening rates increased approximately 90 percent, and 87 percent of survey respondents said they knew more about controlling their blood pressure as a result of the program. Economic modeling showed that if just 8 percent of eligible candidates participated in the program, better management of blood pressure could result in 23 fewer strokes, 22 fewer coronary artery disease events, and 16 fewer deaths per 100,000 people annually. In reality, more than 20 percent of eligible candidates chose to participate in the program, which will hopefully lead to even better outcomes in the long term.
Agostini identified a number of opportunities generated by the program. This low-technology intervention relies on phone communications rather than the Internet, which many older people still do not use. By entering and sending information to a central location, people learn more about their blood pressure than they would if the data were monitored and relayed to a central location automatically. Also, having nurses available for management backup allows for more efficient use of higher-cost resources.
Agostini also described several barriers revealed by the program. Adherence rates can wane, which often happens when people are asked to interact with a technology over time. Some participants prefer to interact with a human rather than entering their data into an automated system. Also, nurse case managers are trained in motivational interviewing, can respond in a thoughtful way, and understand what motivates people to make health behavior changes. This personalization cannot be done as well with an interactive voice response system.
Congestive Heart Failure Telemonitoring
The second example Agostini described involves biometric monitoring for congestive heart failure. Congestive heart failure is the number one cause for readmissions to the hospital, yet many of these readmissions are avoidable with high-quality care management. In this program, people at high risk of congestive heart failure had a device installed in their homes that allowed for blood pressure monitoring, weight management, and other biometrics as needed. Researchers then studied the difference in outcomes between a group of patients who had case managers versus a group who had both case managers and the monitoring technology.
The researchers found no significant impact for this intervention on hospitalizations, emergency department visits, or death (Wade et al., 2011). Part of the reason for the negative results may be the effectiveness of the case managers, said Agostini. Also, converting data from telehealth monitoring into actionable information turned out to be difficult, even though the alerts prompted more frequent telephone contact (which also had the effect of increasing case managers’ workload). A similar study at the Mayo Clinic for older people with multiple chronic conditions also had negative results on hospitalizations and emergency department visits (Takahashi et al., 2012).
Participation is lower when people are invited to participate in a program than when the program is implemented through physicians’ offices as part of the patients’ health care, Agostini noted. Also, the installation and maintenance of the devices took more effort than anticipated. Finally, deciding which patients to recruit to the program was difficult, because it is not clear which patients would benefit most from such a program.
Concluding Remarks
Technology and connectivity will continue to improve and will become cheaper, which could improve outcomes in the future. Also, closer collaboration is likely to yield better results. In particular, teams in patient-centered medical homes and accountable care organizations could work together to keep people healthy and out of the hospital. Technology provides tremendous opportunities, Agostini concluded, but it is a tool and not an end in itself. The goal is to increase the quality of health care at reasonable costs by increasing patient engagement and improving clinical outcomes.
Carolee J. Winstein, Ph.D., PT, FAPTA University of Southern California
New technologies are changing rapidly and have great promise. But technological change also creates challenges in translating advances into practices that address real problems. According to Winstein, solutions will come through effective collaborations at the nexus of new technologies, aging, and disability among those working in a wide range of fields, including
- rehabilitation engineering,
- psychological science,
- implementation science,
- gerontology,
- clinical science,
- social science,
- cinematic arts,
- health economics and policy,
- the health care industry, and
- consumers.
Winstein compared the nexus subfield of rehabilitation to a tetrahedron in which four major forces are coming together to forestall the onset of disability (see Figure 6-1).
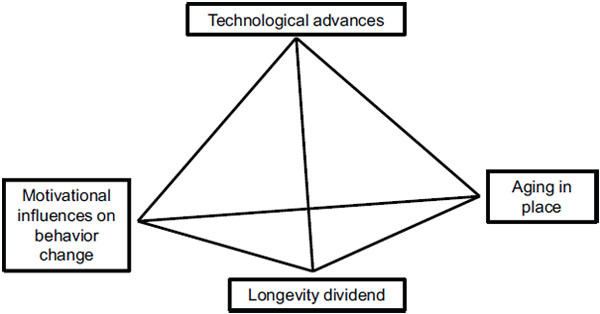
FIGURE 6-1 Four factors combining to transform the subfield of rehabilitation.
SOURCE: Reprinted with permission from Carolee J. Winstein (2012).
Technological Advances
At one corner of the pyramid are technological advances such as mobile health monitoring devices, commercial devices such as the Kinect sensor, emergency notification devices, virtual reality and game-based rehabilitation devices, and applications of smartphones, tablets, and computers. As an example, Winstein mentioned an elastic tape that is placed on a person’s back and monitors posture over the course of the day. Similarly, the use of robotics for assessment and rehabilitation has expanded rapidly. A PubMed search for “robotic rehabilitation stroke” that she did returned 394 hits, with 196 since 2010.
Motivational Influences on Behavior Change
At another corner of the pyramid are motivational influences on behavior change, which Winstein analyzed in terms of three fundamental psychological needs: autonomy, competence, and social relatedness. Autonomy involves the need to determine or feel in control of one’s actions. For example, simply giving people a choice can increase autonomy. Competence relates to the need to perceive oneself as capable. For example, giving people feedback that they have been successful doing something makes them feel good. This is particularly an issue for people engaging in rehabilitation, who often do not feel competent because of a loss of function. Finally, social relatedness involves the need to feel included, accepted, or connected to others. For example, the use of social media can increase satisfaction in one’s involvement in the social world.
Virtual-reality simulation technology is ideally suited to incorporate these basic psychological needs, Winstein observed. Best practice in rehabilitation is focused on a specific skill or task, has adjustable levels of difficulty, is quantifiable in order to assess progress, is administered repetitively and hierarchically to allow the right amount of challenge, provides the user with feedback about success, has some relevance to real-world function, and motivates and engages the user. Virtual reality–based exercise programs can achieve all these ends.
Aging in Place
At the third corner of the pyramid is aging—and rehabilitation—in place. Rehabilitation is not something that happens just in the hospital or clinic. It can also happen at home and in the community. Closing the gap between the current evidence base and common practice could keep seniors and people with disabilities in their homes and communities longer. For example, one of the greatest fears of seniors in surveys is that they will fall and
lose their autonomy. Winstein described a technology-based program called Preventing Falls in Aged People Living Locally, or PreFALL. This interactive app and Web-based system for health professionals and patients will enable them to use current evidence to identify and decrease risk factors for falling, identify and implement behaviors to prevent falling, and maintain healthy behaviors after one or more initial falls. It uses psychological theory, the best evidence from implementation science, and leading technology to create an interactive system that clinicians and patients can use through the convenience of their smartphone, tablet, or computer. This is an excellent example of how to close the gap between theory and practice in care for older adults and individuals with disabilities, said Winstein.
The Longevity Dividend
At the fourth corner of the pyramid is what Winstein termed the longevity dividend, which refers to the health, social, and economic benefits that result from slower aging. As an example of how to realize this dividend, Winstein described work being done at her center that uses the Kinect camera with seniors as they reach for virtual objects. By monitoring the cognitive load on participants, researchers have for the first time determined that the heightened attention during the virtual reality–based activity is associated with higher engagement in the task. The higher engagement leads to sustained participation and a more active lifestyle. The project has provided a wealth of data that improve our understanding of how these new technologies benefit those aging into and with disabilities. The increase in average lifespan was the great success of the 20th century, Winstein observed. The great challenge of the 21st century is disability.
Timothy Bickmore, Ph.D.
Northeastern University
Bickmore described a particular technology that he and his students have been developing for the past 8 years to implement health behavior change interventions. They have studied one-on-one, face-to-face counseling conversations between health providers and patients to understand the verbal and nonverbal cues that go on in such conversations. They have examined not only the verbal content of the conversations but the nonverbal channels such as the use of hand gestures for conveying information, gaze cues for taking turns, body postures, head nods for understanding, and facial displays of emotion. Face-to-face communication, in conjunction with written communication, is the best means of conveying information
to patients. Still, most health professionals have extremely limited time to spend with patients.
By emulating human relationship-building behavior to create and maintain a trusting therapeutic alliance, virtual characters can maintain engagement for longitudinal inventions. Bickmore and his team simulated the patient–provider interactions they observed with as much fidelity as possible in automated health care providers. Patients need to like and trust a virtual character so they will keep talking to it over time and follow its recommendations. Thus, the characters rely heavily on nonverbal cues such as facial displays of empathy, simulating closer proximity, orientation toward the patient, more facial animation, more direct gaze or smiling, and other cues that would be difficult or impossible to create in a text-based system. Bickmore and his colleagues have even conducted studies where the character has a human backstory, and patients react positively and log in more frequently to home-based interventions when the character has this human dimension (Bickmore et al., 2010).
Virtual Discharge Nurse
Bickmore demonstrated such interactions with an automated virtual discharge nurse developed with clinicians at Boston Medical Center (Bickmore et al., 2009). A computer that contains information about a patient is wheeled next to the patient before discharge. The patient then has a half-hour conversation with the virtual nurse about self-care procedures at home. The nurse talks using synthetic speech, and the conversation is dynamically assembled from the patient’s medical record. The simulated nurse has hand gestures, gaze cues, and body posture shifts that are synchronized with speech. The patient interacts with the nurse by choosing options on a touchscreen. Patients can be trained to use the system in seconds, after which they can use it on their own.
The system has been used with about 200 patients in a safety-net hospital where patients typically have low levels of computer and health literacy. When asked whether they would rather have their discharge instructions from the automated nurse or a real nurse, 70 percent choose the automated character, saying that it provides them with a more relaxed environment to get the information they need and have questions answered. Indeed, the highest levels of acceptance are in patients who have low computer health literacy.
Health Behavior Change Interventions
With a variety of collaborators, Bickmore’s team has used the system for various health behavior change interventions, from medication adher-
ence for antipsychotic drugs to breast-feeding promotion. At the workshop, he focused on a particular line of research involving exercise promotion in older adults. In one of their studies, 21 geriatric ambulatory patients from Boston Medical Center, half of whom had no experience with computers, received a touchscreen computer to use at home for 2 months (Bickmore et al., 2005). They also received pedometers to wear and had a 10-minute conversation with an automated exercise coach every day. Overall the patients responded positively to the automated coach, and especially to the social dimensions of the interactions. They had a high level of desire to continue using the system at the end of 2 months and were disappointed when the trial ended. The interactions doubled the amount of walking they did relative to a control group who were just given pedometers and log sheets. As one patient said of the coach, “She’s nice. She’s really good. Really good. She asks you the right questions. She tells you if you’re not doing up to par, you know, and all that. And if you’re doing good, she’ll tell you. If you’re not she’ll tell you. And it’s honest. And it works. It really does. I like it. I like talking to her.”
They also looked at exercise promotion in patients with Parkinson’s disease (Ellis et al., 2013). Twenty patients given a touchscreen system to take home for a month had high levels of interacting with the coach, closely followed the recommendations for walking, and exhibited clinically meaningfully outcomes.
Finally, Bickmore mentioned a project involving a linguistically and culturally tailored version of the system for use with an older adult Latino population in San Jose, California (King et al., 2013). Participants came to a community center twice per week for 4 months and had a conversation with a virtual coach. Again, the intervention group exhibited significantly increased levels of exercise as compared to a control group.
Concluding Remarks
Virtual agents can provide always-on social support for older adults, Bickmore concluded. They can provide wellness counseling, promote exercise, and encourage social engagement. A potential barrier is maintaining engagement over the long term. After 1,000 conversations, will patients want to continue interacting with their virtual coaches? Hardware and network connectivity are also continuing issues for patients. But simulation of human behavior can lead to increased accessibility, engagement, adherence, and retention, and it is especially effective for disadvantaged populations.








