
2
The Potential of the ACA to Reduce Health Disparities
Important Points Made by the Speakers
- All the major goals of the ACA—expanded coverage, reduced costs, and improved health care quality and population health—will have the effect of reducing health disparities. (James)
- Many provisions in the ACA directly affect insurers, who will be expanding the numbers of people and conditions covered. (Rawlins)
- Current experiences in Connecticut and Massachusetts demonstrate that the number of uninsured people could be dramatically reduced, but doing so requires comprehensive and personalized outreach and careful planning. (Counihan)
Provisions of the ACA related to health equity are woven throughout the act. Three speakers at the workshop discussed various aspects of these provisions and their potential to reduce differences in health outcomes among racial, ethnic, and primary language groups. This chapter integrates the presentations and the responses to questions in order to provide an overview of the ACA and a more detailed examination of some of the ways in which it addresses health disparities.
The ACA has five basic goals, said Cara V. James, director of the Office of Minority Health at the Centers for Medicare & Medicaid Services (CMS):
- Expand coverage,
- Reduce health care costs,
- Improve health care quality,
- Improve population health, and
- Reduce health care fraud and abuse.
To expand coverage, the act creates marketplaces, known as exchanges, in which people can purchase health insurance and determine their eligibility for financial assistance. Three types of marketplaces will exist: federally facilitated marketplaces, state-based marketplaces, and state-partnership marketplaces. The responsibilities of the states will vary by type of marketplace. The exchanges will have a single process to determine whether someone is eligible for tax credits to reduce the cost of premiums, in the form of cost sharing, Medicaid, or the Children’s Health Insurance Program.
Health plans qualified to be included in the exchanges will be required to cover a range of essential health benefits, including ambulatory patient services, prescription drugs, emergency services, rehabilitative and facilitative services, hospitalization, laboratory services, maternity and newborn care, preventive and wellness services and chronic disease management, mental health and substance use disorder services (including behavioral health treatment), and pediatric services (including oral and vision care). Plans will vary by level depending on how much of the total health care cost the plan will pay versus how much the member will pay. Platinum will be the highest level of coverage, followed by gold, silver, and bronze, but each level will cover the services listed above.1
Marketplaces are to be established by October 1, 2013, with the coverage and services becoming available on January 1, 2014. The applications for coverage are somewhat complicated; James observed, to verify incomes, eligibility, and so on. As a result, assistance will be provided to help with applications, including navigators, in-person assistants, certified application counselors, agents, and brokers. This assistance will help, James said, but “we’re going to need the churches, we’re going to need the schools, and
__________________
1 In his presentation later in the workshop, Kevin Counihan, chief executive officer for Connecticut’s Health Insurance Exchange, described the origins of the metallic levels. When he was involved with health care reform in Massachusetts, he was describing to his wife several possible systems to refer to kinds of coverage in the state. She said that they were all too complicated and that the best system would be to use the colors of metals given in the Olympics, to which platinum was later added.
[we need] a lot of thinking about how to build a very strong ground game to help get the word out, get people covered, and get them the assistance they need to apply for coverage and select a qualified plan.”
To improve health care quality, the ACA mandates several initiatives:
- A national quality strategy,
- Increased reliance on value-based purchasing,
- Expansion of meaningful use of electronic health records (EHRs),
- Better care coordination,
- Development of quality measures for Medicaid and Medicare, and
- Measures of quality in the marketplace.
Innovation also will be a way to improve quality, James emphasized. Existing demonstration projects are already boosting innovation. Such projects include Strong Start, which is a program to reduce early deliveries, particularly among Medicaid populations; nurse-managed care organizations; programs supported by Health Care Innovation Awards and the Community-Based Care Transitions Program; accountable care organizations (ACOs); and the Advanced Primary Care Practice demonstrations at federally qualified health centers (FQHCs). In addition, CMS and other organizations are seeking to develop and test models to reduce health care costs, improve health care quality, and evaluate how well models work across different populations.
A number of initiatives will also be used to improve population health, including
- Quality-of-care improvements,
- Employee wellness benefits,
- Preventive services for Medicare beneficiaries,
- Preventive services for women,
- A dental sealant program for children, and
- Community transformation grants.
Strengthening the health care workforce is another major focus of the ACA. The act includes grants to institutions to train physicians in family medicine, general internal medicine, and general pediatrics, as well as to train physician’s assistants; increased funding for training in mental and behavioral health; and removal of previous caps on the U.S. Public Health Service Commissioned Corps and the National Health Service Corps. It also has a loan repayment program that encourages providers from diverse backgrounds, including rural backgrounds, to pursue careers in health services, because, said James, “we know that those are providers who are more apt to treat the same population from which they’ve come.”
The ACA includes an increased reliance on nurses because of anticipated difficulties in training the requisite number of doctors. A $50 million grant program for clinics run by advanced practice registered nurses (APRNs), who have post-graduate education in health care, will provide primary care and wellness care to underserved populations. Other provisions include improved access to nurse-midwife services, establishment of Community Health Teams, an independence-at-home demonstration program, a nursing student and faculty loan program, and retention grants and a demonstration project for the education of APRNs. “We’re going to have to maximize health services across all levels,” said James.
The ACA includes many provisions specific to the reduction of health disparities, said James. In 2014, almost 50 million people were uninsured, with communities of color overrepresented among that group (see Figure 2-1). Furthermore, disparities in the quality of care among racial and ethnic groups have not changed much over time (AHRQ, 2012).
New data collection standards require monitoring by race, ethnicity, primary language, sex, and disability, and the secretary of the U.S. Department of Health and Human Services (HHS) has the authority to add other categories, such as socioeconomic status and sexual orientation. Monitoring will also look beyond large racial and ethnic groups to more specific groups.
Circumstances vary by state. The southeastern and southwestern states have the highest proportions of people of color (see Figure 2-2). They also have the highest proportions of uninsured individuals (see Figure 2-3). About half of African Americans, American Indians, and Hispanics are eligible to be covered through the expansion of Medicaid, which some states are undertaking and others are not.
Coverage also does not necessarily imply access, James said. For example, people who have been uninsured for long periods need to have the tools to access health care; they cannot just be told to go find a physician. For example, many people need to be educated about health insurance, such as what a copay is, what coinsurance is, and how a navigator program works. And even people who have had insurance coverage can have trouble finding a provider who will accept new patients.
The HHS Action Plan to Reduce Racial and Ethnic Health Disparities (HHS, 2011) has five goals:
- Transform health care.
- Strengthen the workforce and infrastructure of HHS.
- Advance the health, safety, and well-being of the American people.
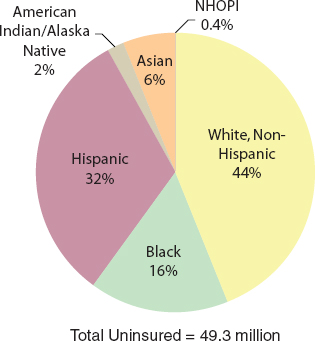
FIGURE 2-1 Minority groups and uninsured people in the United States.
NOTE: NHOPI = Native Hawaiians and other Pacific Islanders.
SOURCE: James workshop presentation, April 22, 2013.
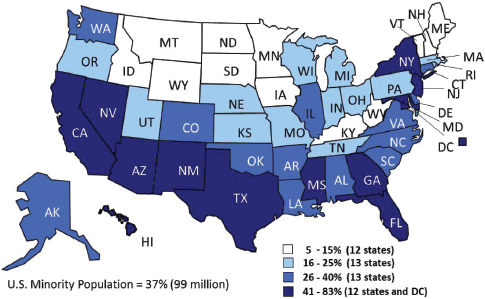
FIGURE 2-2 Southern states and proportions of non-elderly persons of color.
SOURCE: Kaiser Family Foundation.
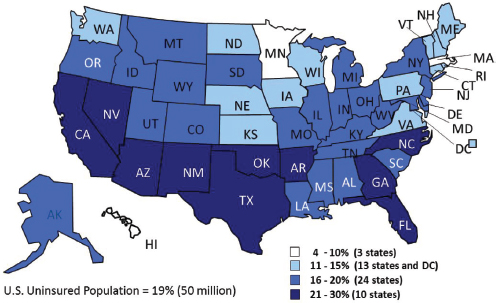
FIGURE 2-3 Southern states and proportions of non-elderly uninsured persons.
SOURCE: Kaiser Family Foundation.
- Advance scientific knowledge and innovation.
- Increase the efficiency, transparency, and accountability of HHS programs.
Each goal has a strategy and a lead agency to ensure that the goal is achieved. In addition, the ACA created offices of minority health in many agencies within HHS that did not have such offices previously, including CMS, the U.S. Food and Drug Administration, the Centers for Disease Control and Prevention, and the Substance Abuse and Mental Health Services Administration.
James cited several programs addressing disparities that have received Health Care Innovation Awards:
- The Delta Dental Plan of South Dakota has focused on oral health improvements for women and children in American Indian and Alaska Native populations.
- The Joslin Diabetes Center is expanding its On the Road program.
- Duke University’s program, From Clinic to Community, aims to reduce death and disability from type 2 diabetes in the southeastern United States.
- The Ravenswood Family Health Center in San Mateo, California, is creating a disparities collaborative and training care managers to address chronic diseases.
“Across the board,” said James, “demonstration programs offer an opportunity for us to review how these models are working and where we can improve them through tracking and improving data.”
James also noted that part of the ACA consists of legislation known as the Indian Health Care Improvement Act, which was reauthorized for the first time since 2001. That act includes a comprehensive set of provisions focused on improving access to care for American Indians. The Indian Health Care Improvement Act:
- Provides authorization for hospice, assisted living, long-term, and home- and community-based care.
- Makes it easier for facilities run by tribes to recover costs from third parties.
- Establishes a Community Health Representative program for urban Indian organizations to train and employ American Indians to provide health care services.
- Directs the Indian Health Service to establish comprehensive behavioral health, prevention, and treatment programs for American Indians.
At the federal level, the secretary of HHS engages in consultation with representatives from American Indian tribes on a regular basis, James said. The Office of Tribal Affairs at CMS also works with tribes on an ongoing basis.
Even as regulations are being developed to implement the ACA, some of its benefits are already in place, including
- A ban on lifetime limits,
- No denial of coverage for children with preexisting conditions,
- Coverage for children on their parents’ coverage until they turn 26 years of age,
- No denial of coverage for adults with preexisting conditions starting in 2014,
- Prevention and wellness benefits for seniors at no cost,
- Help for seniors who reach the “donut hole” in prescription coverage, and
- Preventive services for women.
As a more detailed example of the new services in place, James listed the preventive services that now are covered for women:
- Well-woman visits;
- Domestic violence screening;
- Gestational diabetes screening;
- Breastfeeding support, supplies, and counseling;
- Sexually transmitted infections counseling;
- HIV screening and counseling;
- Contraception and contraceptive counseling; and
- Human papillomavirus testing.
James encouraged everyone to get engaged and stay informed. Proposed regulations are being posted in the Federal Register for comments. The website healthcare.gov has information for consumers to learn about the ACA and its implementation. “We rely on you to help us to make sure that we are doing the best that we can for the populations that we are trying to serve.”
“[We need] a very strong ground game to help get the word out, get people covered, and get them the assistance they need to apply for coverage and select a qualified plan.”
—Cara James
Communities of color have much to gain from the ACA, James concluded. But these communities need to be connected with the health care system, which will require that all parts of that system take steps to engage more fully with these communities. As James said, quoting Lao-tzu, “A journey of a thousand miles begins with a single step.”
Health Equity and the ACA: An Insurer’s Perspective
Many provisions in the ACA related to health disparities affect insurers, said Wayne Rawlins, national medical director for racial and ethnic equality initiatives at Aetna. Under the ACA, insurers will provide plans and health insurance exchange marketplaces, and all insured patients must
receive culturally and linguistically appropriate information on appeals procedures and explanations of coverage. Experts predict that by 2016 more than 19 million new consumers will purchase commercial insurance in the individual market. In addition, Medicaid expansion will bring probably 6 million new enrollees into the Medicaid market, and many of these will be handled under Medicaid plans managed by insurers.
The characteristics of the 19 million people who will be in the exchange marketplace will be somewhat different from the characteristics of people in the commercial marketplace, Rawlins noted. They will be more racially and ethnically diverse. They will be poorer and have less education. One in four will speak a language other than English at home. More than 65 percent will have been uninsured. They will have ways of accessing and using health care services different from those that are routinely seen in the commercial marketplace.
Insurers must provide first dollar coverage (no deductible) for major health benefits surrounding prevention and wellness. Many will be either contracting with or collaborating with ACOs and other entities focused on improving population health. They will also be taking part in the data collection activities around race, ethnicity, language, and other patient characteristics.
ACOs were created in the ACA as entities for eligible Medicare enrollees. They are provider-run organizations in which the participating providers are collectively responsible for the care of a particular population. Their goal is to deliver seamless high-quality care for enrollees while at the same time improving quality and reducing costs. ACOs can share in any savings associated with improvements in the quality and efficiency of the care that they deliver. For minority populations, one benefit of these organizations is the increased attention to keeping patients healthy. “Like the rising tide that raises all boats, we hope this will shrink the current disparities we see in health care delivery,” said Rawlins.
The increased racial and ethnic diversity of the health care workforce and the strengthening of cultural competency training for all health care providers will affect insurers through their network development and physician outreach activities, Rawlins said. Also, the results of comparative effectiveness research on health outcomes for minority populations conducted by the Patient-Centered Outcomes Research Institute (PCORI), which is described in more detail in Chapter 6, will need to be embedded into the business models of health plans.
Aetna is participating in the collection of data on health care disparities. For example, Aetna has an analytical tool called the racial and ethnic equality dashboard that compiles racial and ethnic information from its members. About 6.5 million currently active Aetna members have voluntarily provided their race and ethnicity, and this information has been
combined with medical claims, pharmacy, and laboratory information to get a precise view of disparities within Aetna’s membership. Aetna also has quality measures that cover about 70 different areas, such as asthma care, behavioral health, cancer screening, cardiovascular care, and maternal and child health. For example, it measures hemoglobin A1C, which is a test of diabetes control. These data have shown that African Americans and Latinos in Aetna’s population have poorer control of diabetes than their white counterparts. Poorer control of diabetes can result in more episodes of blindness, kidney failure, heart attacks, and premature deaths.
The National Health Plan Collaborative, which was established in 2004 and includes nearly a dozen major health plans, brings together major health insurance companies to identify ways to improve the quality of health care for racially and ethnically diverse patient populations. The goals of the collaborative are to collect racial, ethnic, and primary language data to inform efforts to reduce disparities in health care within their respective memberships; improve health care access and quality by enhancing language services for patients whose primary language is not English; support investments in efforts to reduce disparities by making a business case for addressing disparities; and improve knowledge management and the dissemination of disparities-related information.
“It is very important for America to have the healthiest population in the world. We’re paying the most for health care of any country in the world, and we’re actually not getting our value for it.”
—Wayne Rawlins
Rawlins pointed to multiple arguments for addressing health care disparities, including social justice, clinical quality, and financial sustainability. Health care disparities are affecting American businesses and employers through increased medical costs, worse health outcomes, and lost productivity. “It is very important for America to have the healthiest population in the world. We’re paying the most for health care of any country in the world, and we’re actually not getting our value for it. As a consumer and as a citizen, I personally would be okay with paying as much as we do as long as we get the absolute best value for it,” he concluded.
Kevin Counihan, the chief executive officer for Connecticut’s Health Insurance Exchange, described the operational challenges in setting up and running an exchange, which can be “quite complicated,” he said. The
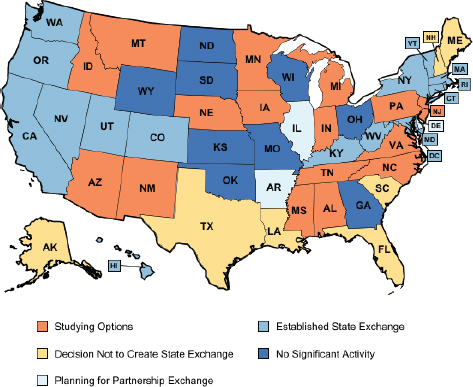
FIGURE 2-4 State-based exchanges.
SOURCE: Kaiser Family Foundation.
options for exchanges are a state-based exchange (as in Connecticut), a federal partnership program, and a federal “default” exchange. Roughly 13 state-based exchanges are in the process of being established (see Figure 2-4).2 Officials in some other states, however, have expressed their desire to do as little as possible to comply with the ACA.
According to Counihan, about 9.6 percent of the population of Connecticut—about 344,000 people—is uninsured. In the first year of the ACA’s implementation, the state hopes to reduce that number by one-third. It hopes to enroll about 100,000 people in the exchange, with 85,000 in the individual market and about 15,000 in the small-group market, and another 30,000 covered from Medicaid expansion. A longer-term goal is to reduce the 9.6 percent rate to 2 to 3 percent, as in Massachusetts. “I think that is practical to do, although there are situations in the law that are very different than in Massachusetts.” One issue is that the penalty for
__________________
2 The current number of states with exchanges is 19, as of July 2014.
not being insured in Connecticut is just $95, which is at more of a nuisance level and is unlikely to drive behavior. In Massachusetts, the penalty will be at the $1,000 level in 3 or 4 years, which is a level more likely to reduce the number of uninsured.
One concern of insurance companies has been that changes in the law would saddle the companies with high-risk patients, but Counihan cast doubt on this idea. Many people are uninsured because they consider themselves to be healthy and at low risk. Data about the health status of the uninsured are scarce, and much remains to be learned about the effects of the ACA. For example, small companies tend to know their employees better than large companies, which can make it more difficult for them to make decisions that result in a loss of coverage. “I always caution audiences not to think that the sky is going to fall when [the ACA] comes about, because that certainly was not the experience that we had in the one state pool on which this is clearly patterned.”
In Connecticut, the exchange enrollment process will be defined by six major steps (see Figure 2-5). As of October 1, 2013, an individual, small business, broker, navigator, or in-person assistor will go to a website, AccessHealthCT.com, where he or she will be able to enter demographic and financial information. This information will be validated through a data hub by a series of federal and state agencies to determine eligibility. Plan options will be displayed and individuals will be directed into one of
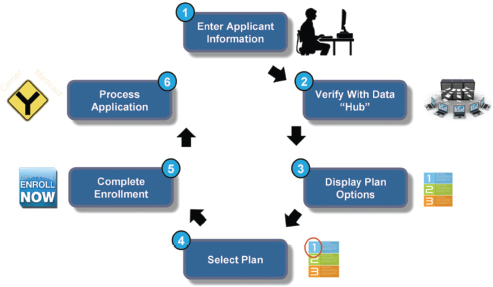
FIGURE 2-5 The exchange enrollment process in Connecticut.
SOURCE: Counihan workshop presentation, April 22, 2013.
three areas: Medicaid, subsidized insurance, or unsubsidized insurance. The individual will be able to compare different plans, such as which benefits and which providers are included, and then choose the appropriate plan, with decision support tools available to help the individual make a choice. Once a decision is made, the individual will be enrolled in a plan and issued an identification card.
“Is this going to go smoothly all the time? Absolutely not,” said Counihan. “Are there going to be times when the federal data hub is down? Yes. Are we going to build contingencies in place for when that happens? Yes we are. Is our system ever going to go down? You bet it is. But that’s just the way things in life happen.” Though the process appears to be complex, in Massachusetts enrollment took an average of just 22 minutes. “This is the type of enrollment experience that we aspire to.”
Customer service, including an empathetic and effective call center, will be critical to the process, Counihan said. The uninsured tend to view buying insurance as confusing, complicated, and expensive. “When people get on the phone, we want them to feel comfortable and safe to ask any question, no matter how stupid they think it is, and not feel in any way they are being intimidated. For example, our call center is expecting that the average call is going to be between 20 and 30 minutes. . . . We’re staffing up to that point, because we want people not to feel afraid and intimidated by calling.”
Outreach will be important. It needs to be broad-based, so that it reaches everyone in a state. It also needs to be population-based, so that it reaches groups that have the lowest levels of insurance coverage. And it needs to work closely with navigator and in-person assistor programs, to enroll people and keep them enrolled. The one-on-one relationships at the community level made possible through in-person assistors will build trust and personal relationships. “Everyone talks about health care being local. It’s completely true. That’s also true about enrollment,” said Counihan. Insurance is not a sexy product like an iPhone or a car. Lack of insurance is associated with poor health, and people tend to shy away from those thoughts. In Massachusetts, an organization of churches and synagogues called the Greater Boston Interfaith Organization went door to door to encourage enrollment. The Massachusetts program also partnered with the Boston Red Sox to do outreach. “There is a lot to be learned from consumer product marketing techniques in terms of enrollment and advocating for health insurance.”
Counihan pointed out that the state-based exchanges have strong and detailed privacy and security features, which will be especially important in addressing concerns about federal agencies revealing personal information. “I am completely confident that we are going to be fully conforming with the security requirements of CMS in this, and I think that those requirements are going to be very sufficient and adequate.” However, he
acknowledged that the exchanges have not devoted sufficient attention to the concerns of people who fear government reviewing their personal data. “We need to think about it, and we haven’t.”
Technology will be a factor. In Connecticut, the zip codes of 85 percent of the uninsured are known, whereas those data did not exist in Massachusetts. Also, the collection and analysis of data will “provide a level of transparency around cost and [quality] which has been unprecedented in our state.” For example, with these data, it should be possible to identify high-performing networks of providers and provide greater health care efficiency and value to particular populations.
Health care is a shared responsibility, Counihan said, especially since everyone has the potential of ending up uninsured if things go wrong. “We’re all in this together, whether you’re insured or uninsured, as a business or not. To make this work, everybody has to feel that they have a stake in this game.” The system will not be perfect on the first day or even after several years. “This is going to take 3 to 4 years to settle down.” People’s expectations should be high but realistic. The program is “going to evolve and get better every year.”
“To make this work, everyone has to feel that they have a stake in this game.”
—Kevin Counihan
The first question for the panelists was about what activities are taking place around informing and engaging new health insurance consumers. James noted that HHS has created a navigator program and the in-person assister programs to help educate people. Counihan added that the goal in Connecticut is to not only get people enrolled, but also to keep people engaged in their health over the long term.
Jeff Henderson of Black Hills Center for American Indian Health asked about HHS’s plans to ensure coverage for American Indians and Alaska Natives under the ACA. Kevin Counihan responded that Connecticut has been “actively engaged” with the tribal leadership and they are working together on a policy. This policy will outline how best to engage the tribes, both in terms of access to coverage and in the communication of unique benefits for tribal members.” James added that the secretary of HHS engages in consultation with tribes on a regular basis. She noted that HHS is focusing on the urban American Indian population, as this group has particular needs that are not met on a reservation.
Terri Wright of the American Public Health Association asked how the exchanges will be made available to individuals with low health literacy. She also said that there is an issue with trust, given that the data collected at the exchanges are shared with other federal agencies. Counihan responded that there is “a very strong and detailed privacy and security feature” to which exchanges must conform. With regard to reaching people with low health literacy levels, staff at the call centers and in-person assisters are trained to deal with these issues.
The final question focused on the requirements in the ACA for the collection of data on race, ethnicity, and primary language. The attendee asked about the scope of these requirements: do all commercial insurers have to do this? James responded that the requirements apply to activities supported and financed by HHS.
This page intentionally left blank.
















