
Important Points Made by the Speaker
- Children and their parents with gaps in insurance coverage have higher odds of experiencing unmet met medical needs and difficulty accessing health care. (DeVoe)
- Insurance needs to be affordable for families to have continuous coverage. (DeVoe)
- Information technology offers a way for insurers, educational services (including schools), medical homes, and social services and public health to share information designed to keep people covered by insurance. (DeVoe)
- Networks of patient-centered medical homes, community health centers, school-based health centers, rural health centers, and other organizations could constitute patient-centered “medical villages” that could share resources, develop and replicate best practices, and spread successful innovations. (DeVoe)
Keynote speaker Jennifer DeVoe, associate professor of family medicine at Oregon Health & Science University, identified several of the specific problems addressed by the ACA and possible ways of solving those problems. As both a family physician and a health services researcher, DeVoe focused in particular on the potential of innovation and evaluation to point the way toward advances in practice.
CONTINUOUS VERSUS NONCONTINUOUS COVERAGE
Whether children are covered continuously by insurance over the course of 1 year is a major determinant of their health outcomes, DeVoe noted. Children with gaps in insurance coverage have higher odds of experiencing unmet medical needs and difficulty accessing health care. Even children with less than a 6-month gap in coverage had five times the odds of unmet medical needs (DeVoe et al., 2008). DeVoe noted that despite the availability of additional insurance programs for children in the past decade, children still experience preventable gaps in coverage, and those children whose parents lack continuous coverage are less likely to have continuous coverage themselves (Yamauchi et al., 2013).
Adults, too, have unmet medical needs when they are not continuously covered by insurance. Among more than 4,000 adults with diabetes who received health care services at federally qualified health centers (FQHCs) from 2005 to 2007, only 64 percent of those partially insured but 82 percent of those continuously insured had received cholesterol screening (Gold et al., 2012). In fact, according to these results, more but incomplete coverage is no better than less coverage.
DeVoe played a recording, collected during her research, of a parent who faced stark choices in paying for insurance (DeVoe et al., 2012):
When we had jobs . . . we were able to do it, but there were times we’d have to pick, “Let’s see, the first of the month, do we pay the insurance or do we pay the water, sewer, and electricity?” . . . If you have to choose between water and electricity and insurance that you’re not using on a daily basis, you have to pick your utilities. . . . We doubled up the next month, and then after two times in a row we had to pay $550. . . . We just said, “We’re cutting our throats, we can’t afford to do this.” So we just stopped the insurance, and it was hard because we wanted to keep the insurance for the kids. . . . That really hurt. I didn’t want to have to do that.
In the first decade of the 21st century, insurance coverage for children increased somewhat, which offers lessons for the ACA, DeVoe said. She and her colleagues used the Medical Expenditure Panel Survey to evaluate trends in children’s health insurance coverage from 1998 to 2009. During that time, the percentage of low-income children who had continuous insurance coverage over the course of 1 year, as opposed to discontinuous coverage or no coverage, rose from less than 70 percent to approximately 80 percent (see Figure 3-1). In contrast, insurance coverage for middle-income children fluctuated but held at slightly more than 80 percent; toward the end of that period the middle-income group had a rise in coverage gaps, and insurance coverage for upper-income children remained stable at about 90 percent. Also, older children were more likely to have gaps, whereas younger children
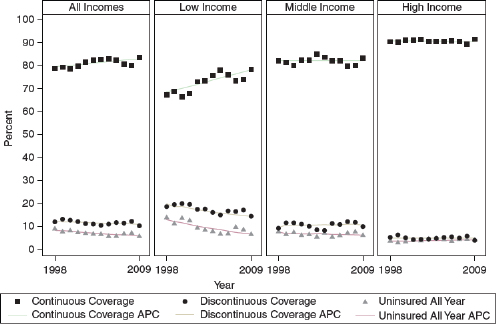
FIGURE 3-1 Child health insurance continuity by family income, 1998–2009.
NOTE: APC = annual percent change.
SOURCE: DeVoe workshop presentation, April 22, 2013.
were less likely, and racial and ethnic disparities were somewhat reduced. Disparities persist, she said, but “some progress” has been made in closing the gap in insurance coverage.
However, as more children have gained coverage, their parents have lost coverage (see Figure 3-2). This is especially the case among low-income parents, which puts their children at risk of insurance gaps. If both parents have coverage gaps or are uninsured, a child is 10 times more likely to experience a coverage gap, said DeVoe. “The parents really matter in terms of keeping the kids covered, . . . and that number is still very high.”
“The parents really matter in terms of keeping the kids covered.”
—Jennifer DeVoe
In many ways, insurance is “all or nothing,” said DeVoe, adding that “you have it continuously or you don’t. . . . We really need to work on getting people continuously covered.”
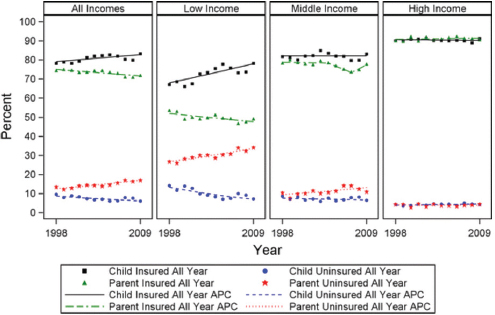
FIGURE 3-2 Child and parent full-year health insurance status, 1998–2009, by family. Source data medical expenditure panel survey-household component, 1998–2009 APC annual percentage change.
NOTE: APC = annual percent change.
SOURCE: DeVoe, 2013. With kind permission from Springer Science and Business Media.
THE AFFORDABILITY OF INSURANCE
Coverage also needs to be affordable, said DeVoe, playing another audio clip from a parent:
At this point the health coverage my husband has offered to him through his job is so astronomically expensive, it’s almost like, “Holy crap, why did you sign up for that?” . . . They [the kids] will [soon] be on his insurance, but I honestly don’t know how we’ll pay for it. If it’s too much more than $600 a month, I don’t know how we’ll pay for it.
Employee premiums and out-of-pocket costs are currently rising much faster than family incomes. If current rates were extrapolated into the future, the average household would be paying half its income in health care costs by the year 2030 and all of the family’s income by 2040.
These rates of increase will have to change quickly for insurance coverage to be affordable, said DeVoe. Today, middle-income families are already cutting back on elective expenses to cover health care costs, but low-income families are cutting back on essentials. Families often face a choice of
whether to pay for health insurance or to pay for the medical needs that are not covered by insurance, such as glasses, orthodontics, counseling, and uncovered medications. Either benefits packages need to be adequate to cover what families need, or, if packages are more limited, they need to be affordable enough for families to buy the things they do not cover.
DeVoe also discussed the importance of health care beyond health insurance. The ACA focuses on insurance, but insurance needs to be accepted by providers and cover the services that are needed. Even with insurance, costs can be high because of deductibles, copays, and uncovered expenses. When costs are high and people with medical problems face difficulties paying for care, they have an added emotional burden.
The United States already spends much more money on health care than other high-income countries, yet its population has worse health status than the populations in those countries. Furthermore, as health care costs continue to rise, other valuable investments, such as spending on education, are inevitably squeezed.
The idea that an expansion of insurance will eliminate the need for community health centers and other safety net providers of health care is a “myth,” said DeVoe. The safety net in health care will need to be strengthened, not eliminated. Studies in Massachusetts have shown that as insurance coverage expanded, the demand for safety net services increased, and the same thing has occurred in Oregon (Ku et al., 2011a,b). For example, DeVoe’s group studied insured people with diabetes and found that they used safety net services more often than those who are partially insured or uninsured (Bailey et al., 2015; Gold et al., 2012).
Uninsured people may not be eligible for insurance even under the ACA, and for them, FQHCs will continue to be vital. Also, as partially insured and uninsured patients gain coverage, they are more likely to use the safety net for services that they have delayed or have not been able to afford. “As more and more people get health insurance, the safety net is going to be used much more frequently, and we’re going to need to be ready with the workforce to meet that demand.” For this reason, said DeVoe, the ACA’s provisions for expanding FQHCs and the National Health Service Corps need to be supported.
“As more and more people get health insurance, the safety net is going to be used much more frequently.”
—Jennifer DeVoe
DeVoe discussed several different models that could both extend coverage and ensure that coverage remains in effect.
One model involves new linkages among four different groups: insurers, educational services (including schools), health homes,1 and social services–public health. New information technologies provide ways of sharing information about the patient among these four components as well as with the patient. For example, DeVoe and her colleagues have been studying the use of electronic health records (EHRs) to monitor children’s health insurance status through community health centers. They analyzed more than 185,000 children who had a visit to a community health center and found that about one-fifth of the children were uninsured, including many of whom were likely eligible for the Children’s Health Insurance Program and more than half the uninsured children continued to be uninsured at subsequent visits (Hatch et al., 2013). Using information technologies, the group has been building tools to connect children with the health insurance products for which they are eligible and keep them enrolled. Data from the EHR are available for outreach and “in-reach” efforts to inform health care providers and social services workers about insurance applications and enrollments (see Figure 3-3). Text messages and emails can then be sent to social workers and others to notify them about new and existing insurance products and to monitor coverage over time. The group will be testing the effectiveness of these tools in pilot clinics over the next several years.
Another model relates to what is known as the “ecology of health care” (see Figure 3-4). In any given month, among an average sample of 1,000 people in the United States, 800 report some sort of symptoms, more than 300 consider seeking medical care, more than 200 visit a physician’s office (half of that in a primary care physician’s office), 65 visit complementary or alternative health care providers, 13 visit emergency departments, 8 are hospitalized, and 1 is hospitalized in an academic medical center (Green et al., 2001). However, academic health centers are where the health care system trains new providers and does the majority of research, DeVoe pointed out.
To expand the number of sites where training and research take place, health care services need to be better organized, coordinated, and delivered. Primary care is the foundation of health care, DeVoe stated, and the Primary Care Extension Program, which has been authorized but not funded, could speed the transformation of primary care centers into a hub for
__________________
1 As defined under the ACA, a health home provides comprehensive care management, care coordination and health promotion, comprehensive transitional care, patient and family support, referral to support service, and use of information technology to link services (if applicable).
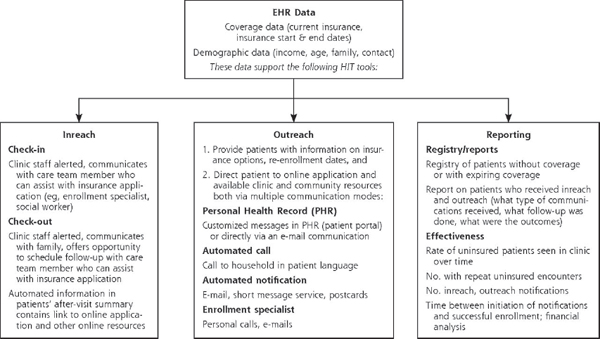
FIGURE 3-3 Electronic health record data.
NOTE: EHR = electronic health record; SMS = short message service, commonly known as text messages.
SOURCE: Angier, 2014. Adapted or reprinted with permission from Health Information Technology: An Untapped Resource to Help Keep Patients Insured, November/December, 2014, Vol. 12, No. 6, Annals of Family Medicine Copyright © 2014 American Academy of Family Physicians. All Rights Reserved.
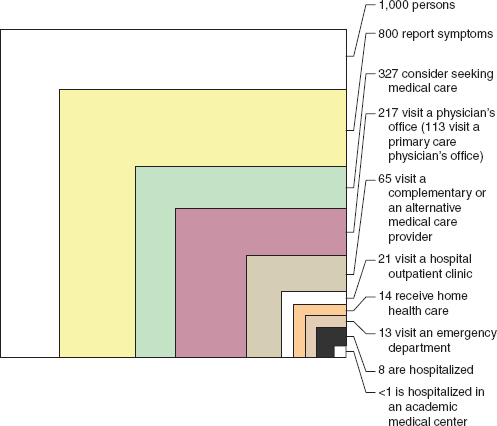
FIGURE 3-4 Symptoms versus hospitalizations.
SOURCE: Green et al., 2001.
training and research. Networks of patient-centered medical homes could allow the sharing of resources and the development and replication of best practices, with primary care “champions” spreading innovations. More training sites in the community would allow medical residents to provide care while learning in settings where care is needed.
As an example, DeVoe cited the OCHIN group, with which she has been involved. An independent nonprofit founded in 2002 and headquartered in Portland, Oregon, OCHIN is one of the nation’s largest health information networks and is recognized for its innovative use of information technology to improve the integration and delivery of health care services across a wide variety of practices. OCHIN has demonstrated how health homes, community health centers, school-based health centers, rural health centers, and other organizations could be organized into a patient-
centered medical village that would use information technologies and data sharing to integrate public health and primary care (see Figure 3-5).
At the same time, DeVoe pointed to the need for more research to continue surveillance and to develop and test solutions. Continued research on disparities is needed to monitor changes, to determine which problems are being fixed, and to identify new problems. Funding agencies need to make strategic investments in innovative solutions and evaluate the effectiveness of innovations. Demonstration projects for the transformation of primary care need to be continued and expanded through the use of community laboratories that support the development of the primary care infrastructure. As an example of infrastructure development, DeVoe highlighted that OCHIN is part of a larger network funded by the Health Resources
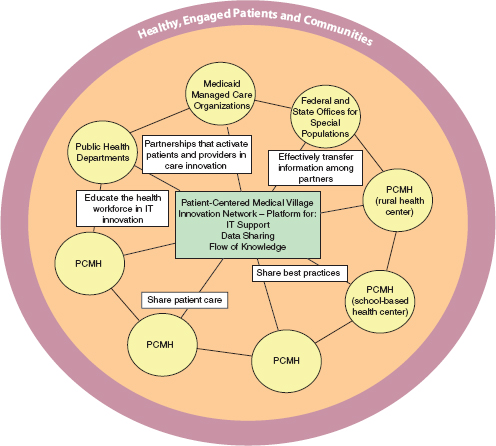
FIGURE 3-5 Information technologies and building patient-centered medical bases.
NOTE: IT = information technology; PCMH = patient-centered medical home.
SOURCE: DeVoe and Sears, 2013.
and Services Administration that focuses on research that is applied in a community setting. Such networks could help move training, research, and innovation out of academic health centers and into communities.
DeVoe concluded with an audio recording of another parent interviewed in her study:
Maybe they’ve never been poor, or had to live in their car, or had to stand in line for food, maybe they’ve never been there. . . . Maybe they need to walk in those people’s shoes and hear from those people. . . . There are people that really just want to provide the best home they can for their kids and the best environment, and part of that is being able to treat their kids when they’re sick and not worry about where the money is going to come from.
The ACA poses some risks, DeVoe acknowledged, such as the possibility that employers will reduce employees’ hours to avoid providing them with health insurance. Also, some of the programs authorized by the ACA have not been funded in a sustainable way, such as the Primary Care Extension Program and teaching health centers.
Nevertheless, the ACA offers an unprecedented opportunity, DeVoe said. Health equity is about ensuring that people in the United States have their basic needs met, and one of those basic needs is access to health insurance and health care. “There are going to be struggles, . . . but we need to make sure that we’re doing all the good we can with the means that we have.”2
“There are going to be struggles, . . . but we need to make sure that we’re doing all the good we can with the means that we have.”
—Jennifer DeVoe
__________________
2 This session did not include a question-and-answer period.










