
Working Across Sectors to Improve Health
In the third panel session, speakers discussed strategies and tools for effective intersectoral collaboration and decision making. Aaron Wernham, Director of the Health Impact Project, a collaboration of the Robert Wood Johnson Foundation and The Pew Charitable Trusts, provided further support for health impact assessments (HIAs) as a practical tool to facilitate health-informed public policy. Loel Solomon, Vice President for Community Health at Kaiser Permanente, described his organization’s conduct of community health needs assessments, and discussed examples of cross-sector collaboration at the community level to address the needs identified. Linda Rudolph, Co-Director of the Center for Climate Change and Health at the Public Health Institute, and Connie Mitchell, Chief of the Policy Unit in the Office of Health Equity at the California Department of Public Health, together described lessons learned from California’s Health in All Policies Task Force. Following the presentations, an open discussion was moderated by Phyllis Meadows, Senior Fellow at The Kresge Foundation.
Aaron Wernham elaborated on one of the key tools for cross-sector public health collaboration, the HIA. For detailed information about HIAs, he referred participants to the National Research Council (NRC) report on HIAs (NRC, 2011).
There are a variety of challenges to working across sectors, includ-
ing the lack of common language; lack of understanding of each other’s processes, and the constraints (political, funding, and legislative) on the way each does business, as well as differing priorities. Policy makers in other sectors such as transportation and housing, for example, may not understand health data, and public health professionals may not understand the constraints and limitations of the planning process. In addition, there is not a lot of funding for new activity, and there are few formalized requirements for doing this work, Wernham said.
As an example of an HIA, Wernham described the process of integrating health into an environmental impact statement (EIS) in Alaska. The Bureau of Land Management was conducting an EIS to examine a proposal to open a vast tract of land near several Alaska Native Communities to oil and gas leasing. Historically, many people in these communities have been supportive of oil and gas development, and much of their $300 million annual local government budget is derived from oil and gas revenues. On the one hand, these revenues are very important to health as they support the health department and the local water and sewer system, for example. On the other hand, Wernham explained, this land is a culturally important area, and also where residents hunt and fish for food, and much of the community was opposed to this particular proposal. Rather than simply attending community meetings, the local government became a “cooperating agency” (allowed under the regulations that drive the EIS process), and the local health department drafted the HIA that was incorporated into the EIS.
The HIA addressed a wide range of health determinants, including air and water quality; noise; food security and dietary change; the influx of non-resident workers; the risk of alcohol and drug trafficking to previously very remote, isolated communities; and benefits such as increased revenues, employment, and income. As a result of the intense engagement among the local government, tribal governments, and the federal agency, an effective relationship was established, and the agency modified the leasing plan and protected key harvest areas. A number of mitigation measures that the community had been asking for (after more than one decade) were finally put into place by the agency to protect the safety of fish and game, and to monitor air and water quality. The final plan was widely accepted by communities, industry, and by state and federal agencies, and there was no litigation. Also as a result of the successful collaboration, the agency is actively soliciting help on additional HIAs and EISs, and the Alaska Department of Health and Social Services now does HIAs on every large project in the state. This is funded mainly through the permit structure of the Department of Natural Resources, Wernham explained. In Alaska, natural resource development is the largest part of
the state budget, and is thus one of the major drivers of all of the determinants of health in communities.
HIAs are being used across a broad range of social, environmental, and economic policies, Wernham said. After Hurricane Katrina, energy prices spiked considerably, especially in the Northeast which was facing a very severe winter at the same time. The state legislature in Massachusetts was considering whether or not to increase funding to the Low-Income Housing Energy Assistance Program. This was not viewed as a health policy, Wernham noted. The HIA highlighted the health effects of lack of heat, such as the use of space heaters and ovens, which can lead to carbon monoxide poisoning, burns, and the spread of infectious diseases when many people crowd into one room. In addition, people faced such difficult decisions as whether to buy food and medicines, or pay for heat. Ultimately, the report recommended an increase in funding for the energy assistance program and noted that it would have implications for Medicaid expenditures as well, because many of the beneficiaries are also publicly insured.
Another example described by Wernham is the Healthy, Hunger-Free Kids Act, which required the U.S. Department of Agriculture (USDA) to regulate the sale of snack foods and beverages sold in schools. The HIA that was conducted found that there would be less student access to, purchase of, and consumption of unhealthy foods and beverages, and improved nutrition because of increased participation in school meal programs. USDA was wrestling with a key concern from school districts around the country regarding the impact of such changes on revenues. The HIA included an analysis of revenues after districts enacted policies that restricted the sale of snack foods and beverages, and found quantitatively that revenues would actually increase because more students would purchase the school meal program. This was important because the HIA helped answer not only the salient health questions, but also offered data that addressed a central policy challenge (schools’ concern about revenue loss) in the rulemaking process.
The use of HIAs has expanded significantly since they were first used in 2000. A 2007 study found a total of 27 HIAs completed across several states, Wernham said, while ongoing data collection by the Health Impact Project and partners showed at least 241 HIAs completed or in progress across 35 states, Washington, DC, Puerto Rico, and at the federal level as of 2013 (an increase of more than 800 percent).
HIAs are being used to achieve concrete policy changes that benefit health, as well as effecting systems changes. An HIA is not just a tool to inform a single decision, he said, but a tool to build effective, more streamlined collaborations. With regard to funding, Wernham noted that conducting an HIA on every decision is not feasible or necessary. Fortu-
nately, in many cases, health-based standards have been routinely incorporated into city planning decisions and a separate HIA is not needed. Many of the HIAs can be completed in 1 or 2 months, rather than 1 or 2 years.
In conclusion, Wernham said that the goal is improving the conditions that allow more people to be healthier. Policy reform and tactics are one approach, but Wernham also posed a question regarding whether, ultimately, a larger-scale social movement may be needed to address some of the root causes of illness and health iniquity. He noted that many of the important changes that led to improved conditions for people in poverty stemmed from the civil rights, worker protection, and women’s suffrage social movements, for example.
CROSS-SECTOR COLLABORATION AT THE COMMUNITY LEVEL
Kaiser Permanente is an integrated health care delivery system that includes 37 hospitals and covers 9 million members. As part of the hospital function, Loel Solomon explained, Kaiser conducts community health needs assessments, and it is clear that the health burdens that communities are facing cannot be addressed with the limited tools that hospitals and doctors in the medical system have. Multisector collaboration is essential. In addressing healthy eating and active living in relation to obesity and diabetes, for example, there are issues of the safety of physical activity environments (e.g., parks, sidewalks). Violence is another overarching issue in communities, and people are dealing with toxic stress, the impacts of stress on parenting, and a social service system that does not serve their needs. For families who are under tremendous financial pressure and are struggling to make ends meet, health moves downward on the priority list.
Solomon shared several key insights from conducting community health needs assessments. In addressing community health needs with community partners, he said, it is necessary to focus on convergent strategies, even if the goals of the collaborating organizations are divergent. The goal is to harness the expertise, the passion, and the interest that different groups bring to the issues (not to get everybody to sign on to the same platform or the same mission). A key organizing principle is the concept of co-benefits. Sometimes practitioners need to “leave the health language and principles at the door,” he said, and meet the community partners on their ground, learn their language, and their priorities. This is an unusual kind of partnership structure in many ways, and he likened it to being a gracious dinner party host and ensuring that everybody feels comfortable at the table. It is also important to be flexible and take opportunities where we find them, he said.
Solomon illustrated these insights with several examples. The Valley Hi HEAL (Healthy Eating Active Living) Zone in Sacramento, California, is 1 of 40 community health initiatives that Kaiser Permanente and its funding partners have launched across the country. The focus is on improving food and physical activity environments to drive behavior change of a small geographic population. Partners in the development and implementation of the plan included the school district, city agencies, local elected officials, the business improvement district, the police department, residents, faith leaders, social service providers, and open space groups. One of the early priorities they identified was community safety and walkability around Valley Hi Park. The process of taking back the park galvanized this community around safety and quality of life issues. Solomon noted that more than half of the communities in the HEAL initiatives identified violence as a major issue. For a health care organization, the focus is on health outcomes, but there must be a balance between focusing on strategies to address health behavior change, and meeting the community where they are.
Another example is the Every Body Walk! campaign, a collaborative of partners working to build a movement for walking and walkability. The partners have very different goals, Solomon said. For example, the developers consider this to be business development strategy for economic vitality (e.g., pedestrians are part of a vibrant downtown), while the national Parent-Teacher Association (PTA) wants to see students walking and biking to school, and views this as quality time between parents and their children. It is important to maintain a broad perspective around engaging constituencies, Solomon said, and that means not leading with health all of the time.
The final example shared by Solomon is the Convergence Partnership, which is focused on improving food and physical activity environments in the community by promoting equity, making policy and systems changes to create the conditions for health, and fostering connections among people to work together more effectively for co-benefits. There have been several key successes, for example, the federal Healthy Food Financing Initiative (HFFI). HFFI scaled up an initiative in Pennsylvania that began as a jobs/social justice initiative to bring supermarkets to underserved areas, which has drawn national attention. Solomon highlighted several key factors for success of the Convergence Partnership. The first factor was disciplined focus on the value proposition. In the case of the Convergence Partnership, this was whether proposed investments drive the equity agenda and support the connection between health and one or more non-health goals (i.e., whether they are co-benefit strategies). There was also a concerted effort to enlist and engage new partners with a focus on funders that target areas aside from health. The partnership
structure and operating agreements are also important to foster trust, and an understanding each other’s different interests and benefits. Finally, a capable program director is essential.
HEALTH IN ALL POLICIES: CALIFORNIA’S EXPERIENCE
Linda Rudolph and Connie Mitchell discussed their experiences with the California Health in All Policies Task Force as an example of collaboration and decision making across sectors. The presentation was based on a discussion paper prepared for the workshop (Rudolph et al., 2013a).
California Health in All Policies Task Force: Structure and Function
The California Health in All Policies Task Force was created through an executive order under Governor Schwarzenegger in 2010, explained Mitchell. A senate concurrent resolution in 2012 recognized the value of Health in All Policies (HiAP), and the task force was included in statute in the health and safety codes of California under the new Office of Health Equity. The 19-member task force includes state agencies, offices, and departments under the auspices of the Strategic Growth Council. The task force regularly reports to the Strategic Growth Council and to the public, and seeks public input on documents and implementation plans. Mitchell noted that in addition to quarterly task force meetings and work-groups in between, task force staff visit each agency to engage in longer discussions with them about priorities, barriers, and how the task force can help them achieve their goals. The task force also interacts with local governments, regional efforts, and nongovernmental organizations to see how discussions and policy changes at the state level are playing out at the local level.
The task force is funded through several mechanisms. The Strategic Growth Council gets an allocation of funding from the Air Resources Board for their support of the task force. The Department of Health provides two staff positions (full-time equivalents, FTEs), office space, equipment, and supplies for the staff that support the task force. The Public Health Institute, through their funding from The California Endowment, Kaiser Community Benefits, and Community Transformation Grants provides another five FTEs.
Health as a Bridge
HiAP supports intersectoral collaboration by bringing together partners from many sectors to recognize the links between health and other issue and policy areas, break down silos, and build new partnerships to
promote health and equity, and increase government efficiency. Health serves as a bridge for the process, Mitchell said, not the driver. A key part of the task force staff’s work is nurturing collaboration and negotiation among competing interests.
The task force began its work by gathering input from the people it hoped to serve, through a series of workshops around the state. More than 1,200 initial recommendations were collected, which were reduced to 34 priority recommendations and 8 implementation plans that were approved by the Strategic Growth Council.
Activities and Achievements
Mitchell highlighted several major activities and achievements of the task force, including the creation of an interagency Farm to Fork Office and a Food Procurement Interagency Workgroup, and the incorporation of health considerations into the updated California General Plan Guidelines. The task force is working to align school facility and city planning processes to rejuvenate schools and their communities, and there are guidance documents near completion regarding crime prevention through environmental design; housing siting near major thoroughfares; and nutrition guidelines for state agencies.
Challenges
A key challenge for the task force, Mitchell said, has been balancing the implementation of current plans and meeting plan goals, with the development of the new ideas and projects that are constantly being suggested. The staff is also asked to provide technical assistance in response to growing interest from other agencies and local communities. Another challenge is fostering ongoing communication across multiple sectors, which she said requires a special skillset and a lot of time. Securing sufficient staff and resources is essential to meeting all of these challenges. She also noted the importance of demonstrating value through evaluation and accountability. Evaluation can be particularly challenging because of the time lag from policy design, through decision making, implementation, and monitoring of results. These are complex adaptive systems; they are nonlinear, dynamic, co-evolutionary, and uncertain, she said. HiAP is not a model that can be tested, but an approach to decision making.
The Health in All Policies Approach
Rudolph defined HiAP as a collaborative approach to improving the health of all people by incorporating health considerations into decision
making across sectors and policy areas. Decision makers are informed about the health, equity, and sustainability consequences of the policy options that are under consideration during the policy development process, with the intent that policy outcomes will reflect those consequences (Rudolph et al., 2013b).
The conceptual underpinnings of the HiAP work in California is that the physical, social, economic, and services environments in which people live, work, study, and play are the key determinants of their health choices and their health outcomes, Rudolph said. The stark differences in these environments contribute to persistent social and health inequities in disadvantaged communities that have unhealthy environments, few resources, and few opportunities for health and thus, significantly unhealthy outcomes. In these environments, the living conditions that are determinants of health outcomes are largely shaped by institutions, businesses, agencies, and sectors outside of health, such as finance, education, housing, employment, parks, and others.
The forces that shape living conditions also shape systems (e.g., transportation, energy, agriculture). These systems have global impacts on the environment (e.g., air and water pollution, ecosystems collapse, soil loss, climate change), creating significant public health threats (see Figure 5-1). Rudolph stressed that, in addition to its many direct health impacts, climate change threatens the systems on which human life depends. Health and social equity within the United States, global equity, and intergenerational equity cannot be achieved without very serious attention to ecosystems and climate change, she said.
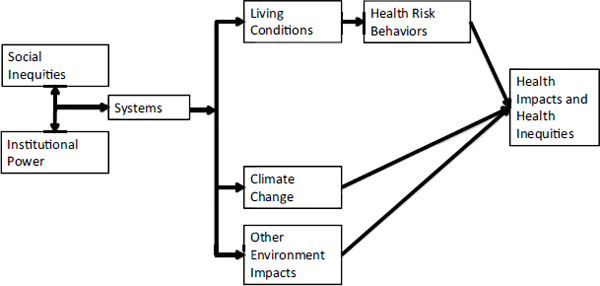
FIGURE 5-1 Health, equity, and sustainability.
SOURCE: Rudolph presentation (September 19, 2013).
The California HiAP Task Force identified five key elements for the implementation of HiAP approaches: health, equity, and sustainability; intersectoral collaboration; co-benefits; engaging community and stakeholders; and creating structural or procedural change. Rudolph noted that HiAP really means health, equity, and sustainability in all policies. One of the first challenges for the task force’s 19 member agencies was to develop a shared understanding of health, and thus form a shared vision and goals for what a healthy community is (see Box 5-1).
Other key elements are collaboration and co-benefits. Rudolph reiterated the concept mentioned by others that when public health practitioners collaborate, they have to balance the fact that while health is their central goal, it is often not the central goal of others. Identifying and prioritizing strategies with health and sustainability co-benefits is one important way to promote collaboration. As an example, she described a study by the California Department of Public Health demonstrating the potentially significant health benefits gained by shifting from driving cars to active transportation such as walking or biking, as well as significant reduction in greenhouse gases (Maizlish et al., 2013).
Keeping the Momentum
HiAP, in many forms and under different names, is spreading across the United States and internationally, Rudolph said. However, the concept of HiAP and of cross-sectoral collaboration in health is not new, and many public health achievements have been the result of significant intersectoral collaboration (e.g., the Alma Ata Declaration of 1978, the Ottawa Charter for Health Promotion of 1986, and the Rio Political Declaration of 2011). As the nation faces dramatically rising social and economic inequality, and the urgent challenge of climate change, what will it take to maintain the HiAP momentum? Rudolph suggested that what is needed is
- structural and procedural change that embeds and institutionalizes the consideration of health equity and sustainability into the cultural organization and processes of government;
- support and opportunity for substantive community and stakeholder engagement that empowers participation of the most vulnerable;
- societal and government prioritization of health, equity, and sustainability;
- strong and visionary leadership and the political will to challenge the status quo; and
- robust democracy and social movements such as those our forbearers were involved in.
BOX 5-1
Healthy Communities Framework:
What Is a Healthy Community?
Meets basic needs of all
- Safe, sustainable, accessible, and affordable transportation options
- Affordable, accessible, and nutritious foods and safe drinkable water
- Affordable, high-quality, socially integrated, and location-efficient housing
- Affordable, accessible, and high-quality health care
- Complete and livable communities, including quality schools, parks and recreational facilities, child care, libraries, financial services, and other daily needs
- Access to affordable and safe opportunities for physical activity
- Able to adapt to changing environments, resilient, and prepared for emergencies
- Opportunities for engagement with arts, music, and culture
Quality and sustainability of environment
- Clean air, soil, and water, and environments free of excessive noise
- Tobacco- and smoke-free
- Green and open spaces, including healthy tree canopy and agricultural lands
- Minimized toxics, greenhouse gas emissions, and waste
- Affordable and sustainable energy use
- Aesthetically pleasing
Adequate levels of economic, social development
- Living wage, safe and healthy job opportunities for all, and a thriving economy
- Support for healthy development of children and adolescents
- Opportunities for high-quality and accessible education
Health and social equity
- Social relationships that are supportive and respectful
- Robust social and civic engagement
- Socially cohesive and supportive relationships, families, homes, and neighborhoods
- Safe communities free of crime and violence
SOURCE: Rudolph presentation (September 19, 2013) citing California HiAP Task Force (2010).
In the discussion that followed the presentations, the panelists, roundtable members, and other participants discussed how decision makers from different sectors can find co-benefits in cross-sector collaboration, what could be the first steps in building a movement or at least a “field of fields,” the characteristics of conveners and leaders in this work, the contribution of social networks of different kinds in supporting the work of improving community health; and finally, what constitutes evidence for decision making.
Co-Benefits
Panelists discussed further what benefits would incentivize groups, organizations, or agencies to engage as partners, while acknowledging that that the answer depends on the needs and goals of the specific groups. From a community perspective, Solomon said that desired benefits are often about quality of life, such as the kinds of neighborhoods people want to live in, the ability to spend more time with family, or finding meaningful work that is close to home. Rudolph said that the health frame can add value to and support the goals that other sectors are trying to achieve. For example, the urban forestry program in California has benefitted from articulating the health perspective on the value of shade in the face of increased extreme heat associated with climate change, or the value of greenery in terms of the aesthetics and quality, and in the crime prevention aspects of urban forestry. Wernham reiterated that in Alaska, the Bureau of Land Management avoided costly and time-consuming litigation over land leasing through effective community and stakeholder engagement, and an HIA to address community concerns before the plan was implemented. Mitchell said that educational attainment is a social determinant of health, and school planners are becoming interested in revitalizing schools, and fostering parental participation and higher educational achievement. Transportation officials became interested in school revitalization when they found that 40 percent of the commuting in some areas of Los Angeles was attributed to transporting children to school, and saw reduction in greenhouse gas emission as a benefit. The community saw safety and walkable streets as a benefit of school revitalization. It is not only about how they benefit, she said, but the synergy effect that moves the project forward to the next level.
Building a Movement
The topic of whether there is, or needs to be, a social movement was again discussed in this session. Mitchell lamented that it is often a fight
to prove the legitimacy of this work, and to gain appropriate funding and staffing for it. There are many people who understand that health care reform is important, but it will fail if more effective prevention strategies are not identified, and if Americans do not make the sociocultural changes needed in their neighborhoods, she said. Wernham concurred that health inequity is a manifestation of economic inequity, racial inequity, and environmental injustice. He added that health care is not health. Public health workers and their partners need to communicate more effectively that medical care is for making people less sick, while health is what happens to people the rest of the hours of the year. Rudolph agreed that there is not a movement for social equity and justice, and added that there is not a movement to address climate change. These are tightly linked because climate change will make all of the other work around health and equity harder, and will take up more of the budget (e.g., to cover the costs of climate change related disasters such as the impacts of extreme weather). Solomon noted that different from building a movement is “building the field,” as well as building a “field of fields,” a group of professionals that can work across these many different areas. Rudolph said that there is limited engagement or involvement at a deep level of the people who live in the most vulnerable and disadvantaged communities. It is crucial to find ways to hear their voices and their solutions, and to empower and facilitate more active citizen participation in these discussions, she said.
Roundtable member Debbie Chang said that before there can be a social movement, there needs to be spread and scale. There is so much innovation going on (tools, solutions, technical assistance) that there should be intentional efforts to expand spread and scale of that knowledge. Solomon noted the challenges of addressing spread and scale of these approaches across different states, with different market dynamics, and different leadership personalities. It is not the same as scaling a disease prevention program. Co-benefits conversations are tailored to each specific group, and there are a lot of face-to-face conversations, and complex relationships and dynamics. Wernham noted that while there is much more interest in health and the built environment now than 15 years ago, there is still work to be done to draw attention to other fundamental inequities, and he noted specifically the lack of a climate change movement, or a movement around economic inequality. From a practical standpoint, it is important to make it easy and automatic for other sectors to integrate health into the way they do business, for example, through innovations in the form of tools that can help planners.
Rudolph said that the spread of the concept of HiAP is happening. However, there is not a network of people that are doing HiAP in the way there is an HIA network that can provide technical assistance. Mitchell added that efforts toward spread and scale must be done in a way that
aggregates resources and people around shared issues, rather than depleting resources.
Codd suggested that there is a generational aspect to many of these issues that could be interpreted as a movement. For example, the millennial generation is buying cars later, and while some of that may be due to the economy, many are hoping to live in the center of a community and be able to live car-free.
Conveners and Leaders
Panelists discussed the attributes of a good convener organization, and how they can sustain engagement and trust among different participants. Solomon said that a good convener has the ability to understand the complexity of this work, to live in the middle space and not drive a specific agenda, but drive a co-benefits agenda. The convener makes sure that information is translated and shared with other decision makers. Facilitation skills are essential. The ability to tell the difference between what is a distraction in the conversation and what is the true problem to be addressed, is a specialized skill. Solomon cited the role that Policy Link has played with the Convergence Partnership as an example of a successful convening organization. The Policy Link team understands enough of the depth in all of the different policy areas to have complete credibility with the various agencies they are working with, he said. Rudolph stressed the importance of taking the time to get to know each member agency individually, and demonstrate interest in understanding their concerns, fears, and priorities. Listening with humility and respect, and looking for the touch points in individual conversations that offer opportunities for bringing people together. Mitchell referred participants to a forthcoming guide on HiAP that answers some of the questions about the nature of the team and the specific skills needed to be an effective convener (Rudolph et al., 2013b).
Panelists were asked also about what constitutes successful leadership on these issues. Codd said that based on his experience, government leaders need to understand the importance of the field and how it interrelates to other sectors, and need to enable and encourage their staff to support HiAP efforts. Rudolph added her experience in working with government leaders who enabled health to be at the table with other sectors, and who were willing to listen, and who helped advance the work.
Social Networks
Roundtable member Sanne Magnan pointed out that many presentations throughout the day referred to the importance of social networks
and connections, for example, the role of HIAs in creating social cohesion in the community, or the role of supportive and respectful social relationships in fostering a sustainable community. She asked about the potential role of faith communities in planning. Solomon said that social cohesion has been shown to impact health in the sense that neighbors who know each other will check on each in times of need. Critical elements are whether settings or environments work in favor of people meeting each other on the street and getting to know each other, and how issues such as violence, street disconnectivity, or sprawl, keep people separated. He added that in the initiatives that Kaiser Permanente has been involved with, engaging the faith community has added a different voice to help express the hopes and aspirations of the community. Rudolph concurred and noted that the framework for a healthy community includes relationships among family members that are safe, respectful, and nurturing. There is clear evidence about the effect of adverse childhood experiences, including violence, on children’s social, cognitive, and health development. Faith communities are an important part of building social support.
What Constitutes Evidence for Decision Making?
A participant pointed out that some areas of policy and practice require randomized, controlled trials as evidence. To move policy forward and secure the necessary investments, is there a need for a common definition of evidence? Solomon agreed that there is a disconnect in the scientific community as to what constitutes evidence, and that for some disciplines, randomized trials are seen as the only level of evidence that is appropriate. That is actually the wrong standard of evidence for many of the phenomena to be studied, he said, in particular for understanding the impact of community context, which is frequently randomized away by randomized controlled rials. More broadly, there are complex interactions between these factors, and the right kind of study design depends on the phenomena studied and the questions asked. Wernham noted that many factors involved in decisions, such as politics, personal preferences, or culture, are not evidence. He also raised the concept of adaptive management, that is, taking actions and defining metrics, and then making adjustments to those actions based on feedback over time. Impact assessment is not about making definite predictions.














