
2
Selection of Domains for Consideration
Social and behavioral factors are widely recognized to be important determinants of health and disease. Health care providers and systems can more effectively influence the health of their patient population if they have information on these determinants. Unfortunately, such information is currently insufficiently captured in most electronic health records (EHRs) (Tai et al., 2012). According to the Institute of Medicine (IOM) Committee on Data Standards for Patient Safety the key capabilities of EHR system are for patient safety, health information and data, management of results, order entry and management, decision support, patient support, electronic communication and connectivity, administrative processes and reporting, and population health management (IOM, 2003). Although the inclusion of social and behavioral determinants of health data in the EHR will provide clinicians with useful information that will allow them to better care for and support their patients, such information is also vital for improving the public’s health.
A National Institutes of Health (NIH) 2011 report titled Identifying Core Behavioral and Psychosocial Data Elements for the Electronic Health Record provided the committee with a helpful description of the goals of including social and behavioral health domains in EHRs and standardizing them to maximize harmonization across systems and populations. The NIH report suggested that harmonized screening and collection of data on behavioral and psychosocial health issues will facilitate
1. Brief interventions in primary care and improved, patient-centered clinical decision making;
2. Shared decision making, goal setting, and action planning with increased engagement of patients, families, and care teams;
3. Improved patient education on risks associated with health behaviors and benefits of behavior change;
4. Patient population management for clinics, accountable care organizations (ACOs), and similar groups;
5. Meaningful use of EHR data, quality of care, and follow-up in primary care medical homes; and
6. Research that integrates data elements common to health behavior with biometric data, health care utilization, and clinical outcomes in EHRs (NIH, 2011).
This IOM committee agreed to add a seventh goal to NIH’s list, which would be a population health and public health goal.
FRAMEWORKS FOR DOMAIN SELECTION
In deciding which social and behavioral domains to consider for inclusion in EHRs, the committee identified and applied several frameworks that capture the range of health determinants, and using the criteria described below narrowed the list to a candidate set best suited for inclusion in all EHRs throughout the life course.
Several conceptual frameworks provide lists of key health determinants and indicate ways in which they are linked to disease onset and progression. These frameworks generally distinguish individual-level characteristics (such as biological factors, emotional and cognitive traits, and health-related behaviors) from features of the physical and social environmental contexts in which they emerge and operate. Although the frameworks vary with regard to the labeling of determinants of health and in organizing the determinants of health (Dahlgren and Whitehead, 1992; Evans and Stoddart, 1990; IOM, 2000a), they generally depict biological and physiological factors to be “downstream” determinants of health that may be modified through complex pathways shaped by “upstream” determinants, such as governmental or institutional policies and community-based conditions and interventions.
The committee reviewed a number of existing conceptual frameworks and selected three that appeared to be best suited for the committee’s use in that they captured a range of determinants occurring at different levels along the continuum from upstream to downstream that affect morbidity, mortality, functional status, and quality of life. The multilevel model of Kaplan et al. (2000) bridges various levels of explanation and intervention, bringing together theory and empirical work that link observations of causal influence and mechanisms at a high level overview (see Figure 2-1).
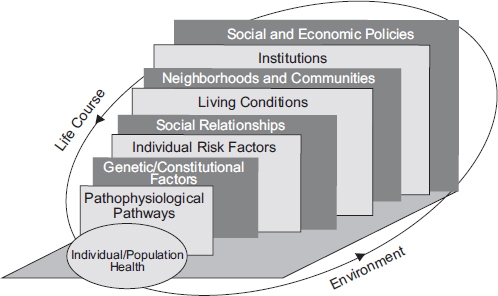
FIGURE 2-1 Multilevel approach to epidemiology, 2000. The approach of Kaplan et al. (2000) attempts to bridge various levels of explanation and intervention, bringing together theory and empirical work that link observations of causal influence and mechanism at multiple levels.
SOURCE: IOM, 2000a.
The public health models of the social determinants of health of Ansari et al. (2003) provide more specificity about the specific determinants that operate at each of these levels (see Figures 2-2 and 2-3). Finally, Figure 2-4, the MacArthur Research Network on Socioeconomic Status and Health’s model moves beyond identifying determinants at various levels to positing some of the interrelationships among them (Adler and Stewart, 2010).
The committee used the model of Kaplan et al. (2000) in conjunction with the models of Ansari et al. (2003) to establish an overall framework and cross-checked the categories in the combined model with categories suggested by the MacArthur Research Network. Each framework addresses social and behavioral determinants of health from a distinct yet overlapping perspective. Although the public health model put forth by Ansari et al. (2003) is primarily anchored by the framework of Kaplan et al. (2000), it helps to explain why it is important to collect information about social determinants of health by illustrating that social determinants affect health in multiple ways: directly, through disease-inducing behaviors, and through the interactions that occur within the health system that people use. The
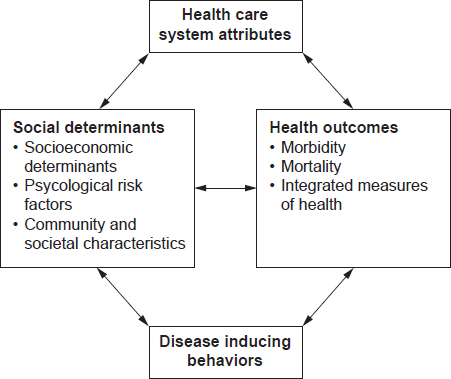
FIGURE 2-2 Categorizations of social determinants of health. The approach to Ansari et al. (2003) illustrates how social determinants of health are usually put into four categories (social determinants, health care system attributes, health outcomes, and disease inducing behaviors) and the relationship among them.
SOURCE: Reprinted with kind permission from Springer Science + Business Media: Soz Präventivmed, 2003, Ansari et al., Figure 1.
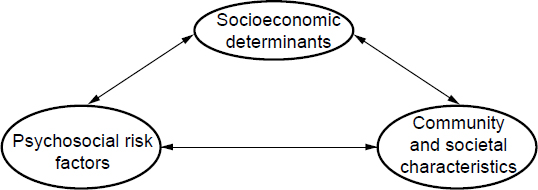
FIGURE 2-3 The public health model of social determinants of health. Approach of Ansari et al. (2003) used to diagram the interrelationship of the components of social determinants (socioeconomics, community and societal characteristics, and psychosocial risk factors) by use of a public health model of the social determinants of health.
SOURCE: Reprinted with kind permission from Springer Science + Business Media: Soz Präventivmed, 2003, Ansari et al., Figure 2.
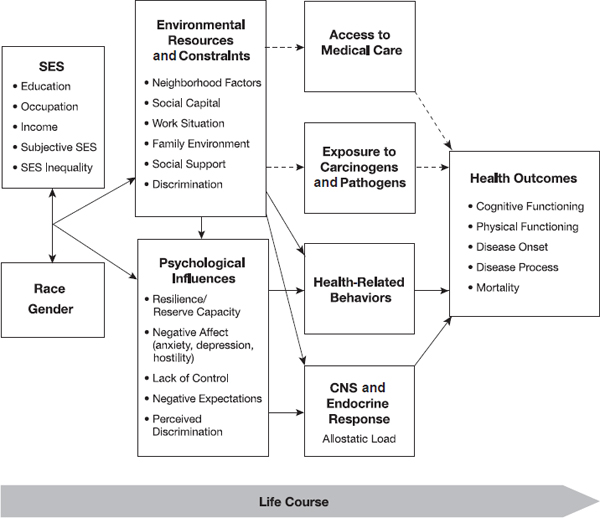
FIGURE 2-4 Pathways linking socioeconomic status and health. The solid lines indicate the pathways studied by the MacArthur Research Network on Socioeconomic Status and Health, and the dashed lines indicate pathways of importance that the network did not study.
NOTE: CNS = central nervous system; SES = socioeconomic status.
SOURCE: Adler and Stewart, 2010, Figure 3.
outcomes that the model aims to explain are integrative measures of health that take into account disability. Although the MacArthur Research Network model focuses on those determinants associated with socioeconomic status, it comes up with a similar set of pathways to health involving access to care, health behaviors, exposure to toxins and pathogens, and responses to stressors.
The committee noted the strong linkage of health behaviors with a wide range of health outcomes. Numerous IOM reports have discussed the impact of behaviors at various times during the course of one’s life span and stage of development, and strategies for modifying behaviors to
improve the health of specific populations (IOM, 2000a,b, 2005a,b, 2010). However, the committee was also keenly aware that the development and maintenance of health-damaging as well as health-promoting behaviors are affected by social and contextual factors. For example, changes in smoking behavior have occurred not only as a result of research findings on the harms of tobacco, but also as a result of policy changes affecting the cost of cigarettes, encouragement by health care providers to quit smoking, media campaigns, the existence of smoke-free environments, and changing social norms.
SOCIAL AND BEHAVIORAL HEALTH DOMAINS
This section outlines the full set of domains that the committee reviewed as an initial step in identifying the set of candidate domains to be considered for inclusion in EHRs. Although most domains suggested for possible inclusion operated as a distal or a fundamental (in the terminology of Link and Phelan [1995]) cause of health, a few (e.g., depression) are both a health outcome that is affected by more upstream factors and a contributor to the etiology and course of other diseases (e.g., cardiovascular disease).
The majority of domains that the committee reviewed involve patient-reported variables. In addition, the committee identified some domains related to neighborhoods and communities that patients themselves would not be likely to know but that are potentially geocodable. If the EHR contains information on the geographic location where an individual lives or works (e.g., a zip code or census block), this information can be linked to other databases to determine environmental conditions, such as air pollution or the availability of sidewalks, public transportation, and healthy food options.
At this first stage, the committee simply listed a wide array of potential domains for later evaluation. Table 2-1 lists all the potential domains that the committee evaluated. The committee agreed on the importance of the standardization of data collection and the need for this standardization to be accepted across geographical levels—federal, state, and community. Standardization needs to occur across agencies, including public health departments, medical settings, and health care organizations. In the long run, with the standardization of information and data linkages, fewer burdens will be placed on the health care community because some data will only need to be collected once (e.g., the patient’s place of birth, the level of education of the patients’ parents, the parents’ medical history, and the patient’s history).
CRITERIA TO BE USED FOR DOMAIN SELECTION
Having adopted frameworks for identifying the social and behavioral determinants of health and reviewed the goals for inclusion of such domains in EHRs, the committee then established the key criteria that it would use in its Phase 1 and Phase 2 reports. Its deliberations were informed by the 2013 IOM report Toward Quality Measures for Population Health and the Leading Health Indicators (IOM, 2013).
The committee decided to use the following criteria to give domains high priority for inclusion in EHRs:
1. Strength of the evidence of the association of the domain with health.1
2. Usefulness of the domain as measured for
a. The individual patient for decision making between the clinician and patient for management and treatment;2
b. The population to describe and monitor population health and make health care–related policy decisions that affect the population cared for by the particular health system or as a whole; and
c. Research to conduct clinical and population health research to learn about the causes of health, the predictors of outcomes of care, and the impact of interventions at multiple levels.
3. Availability and standard representation of a reliable and valid measure(s) of the domain.
4. Feasibility, that is, whether a burden is placed on the patient and the clinician and the administrative time and cost of interfaces and storage.
5. Sensitivity, that is, if patient discomfort regarding revealing personal information is high and there are increased legal or privacy risks.
6. Accessibility of data from another source (as shown in Table 2-2, information from external sources may be accessible to meet the needs of patient care, population health, and research; if so, the domains would have less priority for inclusion in the EHR).
_________________
1 The committee supports the concept of the World Health Organization’s definition of health being a state of complete physical, mental, and social well-being and not merely the absence of disease or infirmity. This definition was not originally included in the committee’s Phase 1 report.
2 After publication of the Phase 1 report, edits were made to criteria 2.a., to clarify that decision making is between a clinician and a patient, and to criteria 5, to clarify that sensitivity includes legal risk.
TABLE 2-1 All Domains Committee Considered
| I. Individual Factors | II. Individual–Level Social Relationships and Living Conditions | III. Neighborhoods/Communities | |
|
Sociodemographics History Financial Resource Strain Parental Level of Education Type of Insurance |
Behavioral Activity Substance Abuse Sexual Practices Exposure to Firearms Risk-Taking Behavior Distractive driving Helmet use Seat belt use |
Social Engagement Marital Status/Family Structure Religious Involvement Civic, Sports, and Community Involvement Social Isolation Social Connections Instrumental Support Emotional Support Exposure to Violence Housing Stability Quality and Safety Work Conditions |
Compositional Characteristics Socioeconomic and Racial/Ethnic Characteristics Contextual Characteristics Air Pollution Allergens Other Hazardous Exposures Land Use, Urban Design, Walkability Spaces Efficacy |
|
Psychological Negative Mood and Affect Psychological Assets Cognitive Function in Later Life |
History of Incarceration Military Service Stress Social Norms/Culture—health decision making |
||
NOTE: The domains that are highlighted in gray shading note the committee’s candidate set of domains best suited for inclusion in all electronic health records. The final list included in Chapter 3 indicates the committee’s final phrasing of the domain title, which in some cases, folded two or more domains (listed in the table) into one domain. The original publication in Phase 1 had several editorial errors regarding the shading of the candidate set of domains and the labeling of domains/subdomains. The report has been updated to correct the errors.
TABLE 2-2 Health Information Surveys and Technologies
|
|
||
| Data Source | Purpose | Example |
|
|
||
| Electronic health record (EHR) |
• Captures data during course of care • Provides data useful for decision making in the health system • Provides a legal record of care |
• Domains and measures selected by committee |
| Personal journal/personal health record |
• Captures information during life/work activities • Allows the individual to record information • Allows the appropriate information to be summarized in an EHR |
• Personal activity tracking log (i.e., Fitbit) |
| Domain-specific measurement instruments |
• Assesses state or progression • Allows the appropriate information to be summarized in an EHR |
• Health-related quality of life |
| Community datasets |
• Analysis of population samples • Analysis of patterns and trends |
• Community resources |
| National surveys |
• Analysis of population samples • Analysis of patterns and trends |
• Health interview survey |
|
|
||
Table 2-2 provides a brief summary of the purposes of the EHR along with the purpose of data from other data sources to inform thinking about what is needed in the EHR and if linkages to other surveys or electronic storage of health information have potential use.
After the committee’s first meeting, an expert consensus process was used so that the committee could promptly complete its first task: to identify a set of candidate domains for consideration for inclusion in all EHRs. Each committee member drafted write-ups on domains relevant to her or his areas of expertise.
Each committee member voted for her or his top ten priorities for consideration on the basis of the evidence provided by fellow committee members and the committee’s review of the strength of association of the domain with health and the usefulness of the domain for the treatment of
individual patient, population health, and research—the first two criteria listed above. The committee strove to err on the side of inclusion while also trying to limit the number of candidate domains. To further the committee’s work in its subsequent report, criteria 3–6 will be applied. The Phase 2 report will likely produce a smaller set of recommended domains once all of the criteria have been applied.
The results of this first pass at a systematic scan of the evidence were summarized for a full committee discussion at its second meeting. The domains that received the most votes were discussed first. However, the committee did not feel that they could prioritize domains based on this vote without further application of the full criteria. Further, following the vote, some domains were aggregated and others were demoted because they had less compelling evidence of utility in the EHR. After a discussion of the full list of domains, unanimous agreement was reached on a candidate set of 17 domains.
Feasibility was not one of the criteria applied in this Phase 1 report, because existing measures had not been compiled for this Phase 1 report. The committee did discuss feasibility in the context of variables included under geocoding because some of those variables are not consistently defined and measured in current datasets and would require costly and time-intensive efforts to develop linkages to individual EHRs. The committee debated whether it was better to consider each variable as a domain or to treat the domain of “geocoding” as a single category, of which specific measures (e.g., the composition of a neighborhood or community by socioeconomic status or race/ethnicity and the level of air pollution and density of housing in a neighborhood or community) could be linked on the basis of a patient’s home address. The first two examples, described later in the text, have the strongest evidence base, but other measures have potential uses as evidence gathers over time.
In sum, the committee, motivated by the value of including social and behavioral data in EHRs and informed by the various goals for doing so, developed a set of domains based on conceptual frameworks on the determinants of health. The results of that process are described in Chapter 3.
Adler, N. E., and J. Stewart. 2010. Health disparities across the lifespan: Meaning, methods, and mechanisms. Annals of the New York Academy of Sciences 1186(1):5–23.
Ansari, Z., N. J. Carson, M. J. Ackland, L. Vaughan, and A. Serraglio. 2003. A public health model of the social determinants of health. Soz Praventivmed 48(4):242–251.
Dahlgren, G., and M. Whitehead. 1992. Policies and strategies to promote equity in health. Copenhagen, Denmark: World Health Organization.
Evans, R. G., and G. L. Stoddart. 1990. Producing health, consuming health care. Social Science Medicine 31(12):1347–1363.
IOM (Institute of Medicine). 2000a. Promoting health: Intervention strategies from social and behavioral research. Washington, DC: National Academy Press.
IOM. 2000b. The role of nutrition in maintaining health in the nation’s elderly. Washington, DC: National Academy Press.
IOM. 2003. Patient safety: Achieving a new standard for care. Washington, DC: The National Academies Press.
IOM. 2005a. Estimating the contribution of lifestyle-related factors to preventable death. Washington, DC: The National Academies Press.
IOM. 2005b. Preventing childhood obesity: Health in the balance. Washington, DC: The National Academies Press.
IOM. 2010. Women’s health research: Progress, pitfalls, and promise. Washington, DC: The National Academies Press.
IOM. 2013. Toward quality measures for population health and the leading health indicators. Washington, DC: The National Academies Press.
Kaplan, G. A., S. A. Everson, and J. K. Lynch. 2000. The contribution of social and behavioral research to an understanding of the distribution of disease: A multilevel approach. Paper commissioned by the Committee on Capitalizing on Social Science and Behavioral Research to Improve the Public’s Health. In Promoting Health Strategies from Social and Behavioral Research (see Appendix A). Washington, DC: National Academy Press.
Link, B. G., and J. Phelan. 1995. Social conditions as fundamental causes of disease. Journal of Health and Social Behavior Special Issue 80–94.
NIH (National Institutes of Health). 2011. Identifying core behavioral and psychosocial data elements for the electronic health record. Bethesda, MD: Office of Behavioral and Social Sciences Research, NIH.
Tai, B., L. T. Wu, and H. W. Clark. 2012. Electronic health records: Essential tools in integrating substance abuse treatment with primary care. Substance Abuse and Rehabilitation 3:1–8.












