

Guidance for VHA Staff Honoring America’s Veterans and Caring for Camp Lejeune Families Act of 2012, Section 102, Covered Clinical Conditions
September 2013
PURPOSE AND KEY POINTS
Purpose:
To provide guidance for clinicians who are supporting qualified Camp Lejeune Veteran or family member who are covered by Section 102 of Public Law 112-154, Honoring America’s Veterans and Caring for Camp Lejeune Families Act of 2012. This guidance will assist healthcare providers in determining whether the Veteran or family member has a medical condition or illness that is covered by the law and will also assist in determining whether the episode of care is related to the covered condition.
According to its published rules, VA will provide care in its healthcare system facilities for eligible Veterans. Camp Lejeune Veterans who qualify will be Priority Level 6, will receive the VHA uniform benefits package, and will have their copayments waived for care related to the 15 covered conditions. VA will reimburse as the last payer eligible Camp Lejeune family members for private sector healthcare related to the 15 conditions covered by the law. Family members are not eligible for care within VA healthcare facilities.
Key Points:
- Section 102 of Public Law 112-154 addresses healthcare for eligible Veterans and family members with 15 covered conditions. It does not change existing disability compensation determinations for Veterans exposed to contaminated water at Camp Lejeune.
- The law does not give VA authority to cover conditions other than the 15 designated conditions and illnesses and “hospital care and medical services may not be furnished…for an illness or condition of a Camp Lejeune Veterans or family member that is found, in accordance with guidelines issued by the Under Secretary for Health, to have resulted from a cause other than the residence” at Camp Lejeune.”
- In cases where there is reasonable doubt as to the diagnosis or primary cause for the diagnosis, clinicians should resolve in favor of the Camp Lejeune Veteran or family member.
- VA is required by law to be the last payer for treatments provided for the 15 covered conditions for family members. Clinical review using these guidelines may be needed to determine if a clinic visit or treatments were related to one of the 15 covered conditions.
- Clinical input is required for three decision points:
1. Does the applicant have one of the medical illnesses or conditions specified in the law?
2. Is there another cause for the medical illness or condition?
3. Which treatments are associated with the medical illness or condition?
- There are some medical conditions in the law that do not have well established diagnostic criteria or have many potential causes. In these cases clinical judgment guided by the applicant’s medical history and available scientific findings will be needed to determine if a Camp Lejeune Veteran or family member has a condition covered by the law.
BACKGROUND
Public Law 112-154 (subsequently referred to as “the law”) requires VA to furnish hospital care and medical services to Camp Lejeune Veterans and family members with the following conditions even if there is insufficient medical evidence to conclude that such illnesses or conditions are attributable to residence at Camp Lejeune.
Table 1: Fifteen Covered Clinical Conditions
- Bladder cancer
- Breast cancer
- Esophageal cancer
- Female infertility
- Hepatic steatosis
- Kidney cancer
- Leukemia
- Lung cancer
- Miscarriage
- Multiple myeloma
- Myelodysplastic syndromes
- Non-Hodgkin’s lymphoma
- Neurobehavioral effects
- Renal toxicity
- Scleroderma
In order to be eligible for care, the law requires that Camp Lejeune Veterans and family members must have served on activity duty at, or resided at, Camp Lejeune for not less than 30 days during the period January 1, 1957, through December 31, 1987. Camp Lejeune Veterans and family members who meet the 30 day requirement will be eligible for the Camp Lejeune program. Veterans can enroll in the VA (Category 6 priority
group) and receive comprehensive health care. As category 6 enrollees, Veterans will be responsible for co-pays for all care other than the 15 conditions in the law. Qualifying family members may be reimbursed for healthcare costs related to the 15 illnesses or conditions listed in the law.
The law does not give authority to cover conditions other than the 15 designated conditions and illnesses and “hospital care and medical services may not be furnished…for an illness or condition of a Camp Lejeune Veterans or family member that is found, in accordance with guidelines issued by the Under Secretary for Health, to have resulted from a cause other than the residence” at Camp Lejeune. Clinically indicated screening without co-pays is part of the comprehensive health benefit for enrolled Veterans. VA will reimburse eligible family members for screening that is clinically indicated or recommended by the U.S Preventive Services Task Force that leads to a diagnosis of a covered condition.
According to the law, VA is the payer of last resort for the 15 covered conditions in family member care after all other third party payers. VA will reimburse hospital care or medical services that were provided to family members on, or after, March 26, 2013, which is the date that funds were first appropriated and available to implement medical care provided to family members.
Clinical input required to administer the Camp Lejeune Program.
Clinical input may be needed in administering the Camp Lejeune Program for those conditions that are difficult to define or have multiple potential causes. In those cases where clinical input is necessary, clinicians will use a three-step process to determine whether a medical illness, injury or condition is eligible for coverage under the Camp Lejeune Program. First, the clinician must determine whether or not the applicant has one or more of the 15 covered conditions. Second, for those conditions with multiple potential causes the clinician must decide whether the condition is probably due to a cause other than exposure to contaminated water at Camp Lejeune. This guidance and clinical algorithms will assist clinicians in making this determination. Third, the clinician may sometimes be called upon to decide whether or not an episode of care or treatment is related to one of the 15 covered conditions. This third determination must be made independently for each clinic visit or treatment delivered.
Decision point # 1 - Does the Camp Lejeune Program participant have one or more of the covered conditions?
To establish if a patient has a condition covered by the law, diagnostic criteria and time of onset will need to be evaluated. Some of the 15 conditions have clear evidence-based clinicopathologic diagnostic criteria while others are less clearly defined or supported by existing medical scientific knowledge. Some of the 15 conditions are well defined but have an onset concurrent with exposure and are unlikely to occur years after exposure to contaminated water. Table 2 divides the 15 conditions according to these general categories:
Table 2: Diagnostic Criteria and Time of Onset
| Covered conditions with well-established diagnostic criteria | |
|
|
| Covered conditions whose onset occurs at the time of solvent exposure | |
| Covered conditions with poorly defined diagnostic criteria | |
| * Listed twice | |
Clinicians will consider the medical history and diagnostic criteria in determining if Camp Lejeune Veteran or family member has a covered condition.
Covered conditions with well-established diagnostic criteria:
Diagnoses such as cancers, myelodysplastic syndrome, and scleroderma are made according to established clinicopathologic diagnostic criteria. Veterans or family members with these diagnoses will be covered by the Camp Lejeune program.
Covered conditions whose onset occurs at the time of solvent exposure:
Hepatic steatosis, female infertility, miscarriage, and neurobehavioral effects have been described in the scientific literature to occur as a result of acute exposure to solvents. The conditions occur during acute exposure or shortly thereafter. Hepatic steatosis and neurobehavioral effects generally resolve after cessation of exposure. It is unlikely that these conditions would have an onset many months or years after exposure to contaminated water at Camp Lejeune. Clinicians will need to review the clinical history or provider report form of the Veteran or family member, respectively, for these conditions and determine the onset of the condition. If a clinician comes to the conclusion that the timing of onset of the covered condition is not consistent with exposure to contaminated water at Camp Lejeune, then VA cannot waive co-payments for Veterans or reimburse care for family members. For example, current scientific studies provide some evidence that solvent exposure during, but not before, pregnancy is associated with miscarriage and that there are no persistent effects of solvent exposure on miscarriage or fetal loss after the acute exposure.
Clinical conditions with poorly defined diagnostic criteria:
Neurobehavioral effects and renal toxicity are not discrete diagnostic entities with commonly recognized criteria or clinicopatholigcal findings. Therefore, for the covered
conditions that are not well defined, clinical judgment guided by the applicant’s medical history and diagnostic findings will be needed to determine if a Camp Lejeune Veteran or family member has a covered condition and that the manifestations began during or shortly after the time of exposure at Camp Lejeune. In cases where there is reasonable doubt as to the diagnosis or primary cause for the diagnosis, clinicians should resolve in favor of the Camp Lejeune Veteran or family member. Specific clinical guidance for these conditions is provided below.
Decision point #2 – Is there evidence that the condition occurred as a result of a cause other than residence at Camp Lejeune?
Another provision of the law directs that “hospital care and medical services may not be furnished…for an illness or condition of a family member that is found, in accordance with guidelines issued by the Under Secretary for Health, to have resulted from a cause other than the residence” of the Camp Lejeune Program family member.
Examples of this include:
- Current infertility or miscarriage in a woman who resided at Camp Lejeune as a child.
- Chronic renal disease with onset 25 years after residence at Camp Lejeune in a patient with obstructive uropathy.
- Neuropathy with onset 30 years after residence at Camp Lejeune in a patient with diabetes.
- Hepatic steatosis in an obese patient who requests bariatric surgery.
If a clinician comes to the conclusion that the cause for the covered condition is related to other etiology (cause(s)) not consistent with exposure to contaminated water at Camp Lejeune, then VA cannot waive co-payments for Veterans or reimburse care for family members.
Decision point # 3 - Is the episode of care or treatment related to the covered condition?
Clinicians providing care to Veterans will be asked to verify at each clinical visit if treatments provided to Veterans are related to one of the fifteen Camp Lejeune conditions. This will ensure that Veterans are not charged copays for Camp Lejeune related conditions.
Bills for family member care will be received by the Financial Services Center. In most cases, the Financial Services Center claims processing system should be able to determine if a billed episode of care is related to one of the 15 covered conditions. However in some cases, it will be very difficult to determine if a bill is related to the covered condition. In those cases clinical input will be required.
The following principles will be used by clinicians for decision point # 3.
- Comprehensive coverage during active cancer treatment: According to the medical literature, surgery, chemotherapy and/or radiation therapy for cancer can result in secondary systemic effects on virtually all other organ systems in the body. In recognition of these systemic whole body effects of treatment of the covered cancers, VA will provide family member reimbursement of most medical treatments (as the last payer) during the active treatment phase of these cancers. Similarly, VA will not require Veteran copays for these cancers. VA will not pay for treatments specifically excluded in 38 CFR 17.38 (for example, abortions). The treating oncologist can certify the duration of active treatment or this type of coverage will be provided in six month increments following the initial cancer diagnosis. Once the active treatment of the cancer is completed, VA will provide healthcare reimbursement for treatments only of the covered condition.
- In those situations where the bill for family member care is not itemized by diagnosis, such as a general medical visit to a primary care provider, VA will reimburse for care as a last payer for bills in which the ICD9/10 code of the primary diagnosis is a covered condition.
- Reimbursement of family member bills medical conditions determined to be secondary to a covered condition: VA has determined that it has the legal authority to provide last payer coverage for health care of conditions that are directly caused by one of the 15 covered conditions or their treatment. In order for Camp Lejeune program participants to be reimbursed for health care of a secondary condition, they will need to have their health care providers certify that the secondary condition is caused or exacerbated by the covered condition or its treatment. VA will review the medical evidence provided and make a determination on eligibility for coverage.
GUIDANCE ON COVERED CONDITIONS
As listed in Table 1, Public Law 112-154 requires VA to furnish hospital care and medical services to Camp Lejeune Veterans and family members with 15 covered medical conditions. Clinicians should consider this guidance in conjunction with standard diagnostic criteria to determine whether a Veteran or family member seeks care for one of these conditions. The following section discusses diagnosis of the 15 conditions and related determinations.
Cancer and neoplastic diagnoses:
The law covers eight neoplasms and myelodysplastic syndrome.
|
|
|
Current scientific research demonstrates that these conditions can be associated with a toxic exposure, can have a long latency period, and can be diagnosed years after the exposure occurred. These conditions have specific clinical and pathological criteria which makes establishing these diagnoses straightforward.
Scleroderma:
Scleroderma has well established diagnostic criteria. The American College of Rheumatology has defined criteria, which are 97% sensitive and 98% specific for systemic sclerosis (SSc) as follows:
Major criterion:
- Proximal diffuse (truncal) sclerosis (skin tightness, thickening, non-pitting induration)
Minor criteria:
- Sclerodactyly (only fingers and/or toes)
- Digital pitting scars or loss of substance of the digital finger pads (pulp loss)
- Bilateral basilar pulmonary fibrosis
The patient should fulfill the major criterion or two of the three minor criteria. Raynaud’s phenomenon is observed in 90-98 % of Systemic Scleroderma patients.
Scleroderma can occur at any time following a toxic exposure. Camp Lejeune Veterans and family members who present with scleroderma will be covered by the law.
Miscarriage:
Miscarriage is a layperson’s term for a spontaneous abortion. A spontaneous abortion is the naturally occurring expulsion of an embryo or fetus before viability. In clinical practice, spontaneous expulsion of a fetus that weighs less than 500 grams or is at or before 20 weeks gestation (or 18 weeks after fertilization) is considered a spontaneous abortion or miscarriage. Spontaneous expulsion of a fetus that is beyond 20 weeks gestation or weighs more than 500 grams is considered a preterm birth. (Sources: American Society for Reproductive Medicine, Stedman’s medical dictionary, Medline Plus, HHS Office of Women’s Health)
Spontaneous abortion is the most common complication of early pregnancy. About 15% to 20% of known pregnancies end in spontaneous abortion. With the use of serial human chorionic gonadotropin (hCG) measurements to detect early subclinical pregnancy losses, the percentage increases to 30%. About 80% of spontaneous
pregnancy losses occur in the first trimester; the incidence decreases with each gestational week.
Most spontaneous abortions are caused by chromosome abnormalities that occur spontaneously and are not related to the mother’s or father’s genetic make-up. Other factors that may increase the risk for spontaneous abortion include: drug and alcohol abuse, smoking, exposure to environmental toxins, hormone level abnormalities, infection, obesity, physical abnormalities of the uterus or cervix, and some chronic systemic diseases (like diabetes and other autoimmune diseases).
Current scientific studies provide some evidence that solvent exposure during, but not before, pregnancy is associated with miscarriage. Therefore miscarriages that occurring during the period 1957-87 while the Veteran or family member lived on Camp Lejeune shall be covered if they require ongoing medical treatment. Current scientific evidence suggests that there are no persistent effects of solvent exposure on miscarriage or fetal loss (National Research Council (NRC) Contaminated Water Supplies at Camp Lejeune: Assessing Potential Health Effects. p. 182). Clinicians should carefully assess whether continued health care is needed for chronic, persistent medical problems associated with a miscarriage that occurred during solvent exposure at Camp Lejeune.
Female Infertility:
The current scientific literature suggests an association between concurrent exposure to solvents and reduced fecundity (a woman’s ability to become pregnant). Infertility and any associated chronic persistent medical problems that occurred during the period 1957 to 1987 while the Veteran or family member lived on Camp Lejeune are covered. There is currently no scientific evidence to support an association with chronic female infertility after cessation of exposure to solvents (NRC p. 181). Similarly the NRC report found no evidence that exposure to organic solvents while in-utero increases the risk for adverse fertility effects as a reproductively mature adult.
Neurobehavioral effects:
According to the current scientific literature, neurobehavioral symptoms associated with solvent exposure have included acute decrements in concentrating ability and visuospatial skills, fine motor abnormalities, at, or shortly after, solvent exposure. Neurobehavioral symptoms secondary to the contaminant levels in the water at Camp Lejeune would likely have been manifest at the time of exposure or shortly thereafter.
In assessing whether current neurobehavioral effects that require medical treatment are associated with exposure to water contaminants at Camp Lejeune, clinicians should evaluate the onset and duration of symptoms to determine if the Veteran or family member has symptoms that are as likely as not, related to exposure to volatile organic compounds in the past. The current evidence suggests that neurobehavioral effects occurring after a long asymptomatic period are not likely to be secondary to the contaminated water at Camp Lejeune. The scientific literature to date indicates that with
the type of exposure at Camp Lejeune (contaminated water used by adults for activities such as drinking and bathing), and its remoteness in time (the exposure occurred more decades ago); it is unlikely that neurobehavioral effects would have persisted and would require treatment at this time.
Organic solvent exposure has been associated with various forms of central nervous system toxicity. There is a widespread agreement that chronic effects are seen primarily after long-term, high-level occupational exposure, with objective testing showing decrements in concentrating ability, visuospatial skills, and fine motor abnormalities, after 10 years or more of occupational exposure (Flodin 1984). Such long-term exposures are also associated with the development of personality changes (Chen 2001). Earlier, mild disease may be seen after as little as three years of exposure. Some exposed individuals develop peripheral neuropathy with acute onset at the time of exposure that can persist. Mild disease, with acute symptoms, generally resolves after cessation of exposure and has not been associated with progressive disease (van Valen 2009). Low-level exposures are not associated with adverse long-term cognitive outcomes (Dick 2010). Research to date has not shown any evidence of progression or worsening after cessation of exposure. There are also no known cases of onset of symptoms after cessation of exposure.
Current classification systems to define neurobehavioral effects are summarized below:
Type 1: Acute symptoms only, including impairment of memory, poor concentration, fatigue, and decreased motivation. In general these resolve rapidly after cessation of exposure. Headaches are not commonly included in a listing of symptoms, because nonspecific headaches are known to occur frequently in the general population.
Type 2A: A sustained change in mood and / or personality, with reduced motivation, poor impulse control, irritability and often anxiety is seen after longer term exposures. This form is generally not associated with performance decrements
Type 2B: Impairment in intellectual function that is associated with cognitive deficits, including problems with attention, concentration, visuospatial skills, and verbal memory. In addition, fine motor performance can be impaired.
Type 3: Severe chronic toxic encephalopathy is characterized by global deterioration in cognitive functions and memory.
Type 1 and 2 disorders are the most likely to be reported among solvent-exposed workers. Type 3 disorders to date have been seen only in individuals who have abused solvent-containing products (i.e., by deliberately inhaling organic solvent vapors for their euphoric properties (NIOSH 1987).
The scientific literature demonstrates that there is inadequate information to associate exposure to solvent contaminated water with Alzheimer’s disease, amyotrophic lateral sclerosis, attention deficit/hyperactivity disorder, multiple sclerosis, reductions in color discrimination, hearing and olfactory functions. While these conditions may have
symptoms that overlap with those of neurobehavioral effects, the law does not include coverage for other diagnosable neurologic diseases.
Renal toxicity:
In evaluating whether a Camp Lejeune Veteran or family member has renal toxicity due to solvent exposure, the clinician should perform a thorough assessment of the patient’s history and onset of chronic kidney disease and other comorbid medical conditions. Once a diagnosis is made, the clinician should consider whether it is probable that the patient’s kidney disease resulted from a known etiology other than solvent toxicity. Chronic kidney disease has many known etiologies. The most common causes of chronic kidney disease include long term diabetes and hypertension. Conditions that might be excluded as a covered condition due to renal toxicity from a Camp Lejeune exposure would include a patient with forms of chronic kidney disease with another known etiology such as those with underlying diabetic nephropathy, obstructive uropathy, hypertensive nephrosclerosis, sickle cell kidney disease, HIV-associated nephropathy, drug-induced kidney disease, etc. Reviewing clinicians should determine if a patient’s clinical course of chronic kidney disease is associated with a known cause, e.g. a 20 year history of diabetes. A clinician might reasonably conclude that the renal disease is as likely as not associated with the patient’s diabetes and they would not be covered by the law. If a patient’s clinical course of kidney disease appears atypical, in that their progression of kidney disease is faster than expected, then exacerbation by TCE, PCE or other organic solvents in the contaminated water should be considered.
Hepatic steatosis:
Hepatic steatosis is not a disease rather it is a common pathological finding in medical conditions that affect the liver. In western countries, it affects up to one third of the population and up to 75% in some subgroups such as obese patients. Hepatic steatosis or simple fatty liver can be caused by a variety of conditions including alcohol abuse, overweight or obesity, Type 2 Diabetes, metabolic syndrome, medication use and hepatitis.
Generally hepatic steatosis or fatty liver resolves by treating the underlying condition. In evaluating whether a Camp Lejeune Veteran or family member has hepatic steatosis related to Camp Lejeune, the clinician should consider whether it is more likely than not that the patient has fatty liver disease from a known etiology. The most common causes of hepatic steatosis include obesity and alcohol abuse. If a patient’s clinical course is consistent with a known cause of hepatic steatosis, their treatment for hepatic steatosis should not be covered by the law.
Camp Lejeune Veterans and family members with hepatic steatosis of unclear or unknown etiology should be covered by the Camp Lejeune law. Moreover, if a patient’s clinical course of hepatic steatosis is atypical or progresses faster than expected, then exacerbation by TCE, PCE or other organic solvents in the contaminated water should be considered.
Points of contact for this guidance:
The VA Camp Lejeune Task Force is co-led by the VHA Office of Public Health and the VHA Chief Business Office (CBO), with representation from the VA Office of General Counsel, VA Office of Congressional and Legislative Affairs, VA Office of Public and Intergovernmental Affairs, VHA Office of Primary Care in the Office of Patient Care Services, VHA Communications, and other offices. The main VA Web site for Camp Lejeune historic water contamination and potential health concerns is http://www.publichealth.va.gov/exposures/camp-Lejeune; individuals can subscribe to email updates. The Marines’ registry appears on their Camp Lejeune Historic Drinking Water site: https://clnr.hqi.usmc.mil/clwater/index.html. The ATSDR site is http://www.atsdr.cdc.gov/sites/lejeune/ The Task Force co-chairs are Terry Walters, MD, MPH, Office of Public Health, 202-461-1020; Katie Shebesh, Chief Business Office, 202-461-1600.
Selected Reading:
General
Agency for Toxic Substances and Disease Registry, U.S. Department of Health and Human Services, Atlanta GA. Available: http://www.atsdr.cdc.gov/sites/lejeune/ [accessed September 4, 2013].
Committee on Contaminated Water at Camp Lejeune; National Research Council. Contaminated Water Supplies at Camp Lejeune: Assessing Potential Health Effects. 2009. Washington, DC: The National Academies Press. Available: http://www.nap.edu/catalog.php?record_id=12618
Committee on Human Health Risks of Trichloroethylene; National Research Council. Assessing the Human Health Risks of Trichloroethylene: Key Scientific Issues. Washington, DC: The National Academies Press, 2006. Available: http://www.nap.edu/catalog/11707.html
Committee on Gulf War and Health. Institute of Medicine. 2003. Gulf War and Health: Volume 2. Insecticides and Solvents:: Literature Review of Pesticides and Solvents. Washington, DC: The National Academies Press, 2003. Available: http://www.nap.edu/catalog/10628.html.
Honoring America’s Veterans and Caring for Camp Lejeune Families Act of 2012. Available:http://www.gpo.gov/fdsys/pkg/BILLS-112hr1627enr/pdf/BILLS-112hr1627enr.pdf. [accessed September 4, 2013]
Hepatic Steatosis:
Mishra P, Younossi ZM. 2007. Current treatment strategies for non-alcoholic fatty liver disease (NAFLD). Curr Drug Discov Technol. 4(2):133-40.
Raman M, Allard J. 2006. Nonalcoholic fatty liver disease: A clinical approach and review. Can J Gastroenterol. 20(5): 345–349.
Younossi ZM. 2008. Review article: current management of non-alcoholic fatty liver disease and non-alcoholic steatohepatitis. Aliment Pharmacol Ther. 28(1):2-12.
Neurobehavioral effects:
Attarchi MS, Labbafinejad Y, Mohammadi S. 2010. Occupational exposure to different levels of mixed organic solvents and colour vision impairment. Neurotoxicol Teratol. 32(5):558-62.
Baker and Seppalainen 1986. International Solvent Workshop, Raleigh, N.C. October 1985.; Anonymous. 1986. Human aspects of solvent neurobehavioral effects (Raleigh Workshop). Neurotoxicology 7:43-56.
Chen R, Dick F, Semple S, Seaton A, Walker LG. 2001. Exposure to organic solvents and personality. Occup Environ Med. 58(1):14-8.
Costa TL, Barboni MT, Moura AL, Bonci DM, Gualtieri M, de Lima Silveira LC, Ventura DF. 2012. Long-term occupational exposure to organic solvents affects color vision, contrast sensitivity and visual fields. PLoS One. 7(8):e42961
Dick FD, Bourne VJ, Semple SE, Fox HC, Miller BG, Deary IJ, Whalley LJ. 2010. Solvent exposure and cognitive ability at age 67: a follow-up study of the 1947 Scottish Mental Survey. Occup Environ Med. 67(6):401-7.
Flodin U, Edling C, Axelson O. 1984. Clinical studies of psychoorganic syndromes among workers with exposure to solvents. Am J Ind Med. 5:287-95.
Janulewicz PA, White RF, Winter JM, et al. 2008. Risk of learning and behavioral disorders following prenatal and early postnatal exposure to tetrachloroethylene (PCE)-contaminated drinking water. Neurotoxicol. Teratol. 30(3):175-185.
Kilburn KH, Warshaw RH. 1993. Effects on neurobehavioral performance of chronic exposure to chemically contaminated well water. Toxicol Ind Health. 9(3):391-404.
Meyer-Baron M, Blaszkewicz M, Henke H, Knapp G, Muttray A, Schäper M, van Thriel C. 2008. The impact of solvent mixtures on neurobehavioral performance: conclusions from epidemiological data. Neurotoxicology29:349-60.
NIOSH. Organic Solvent Neurotoxicity. Current Intelligence Bulletin 48. DHHS (NIOSH) Publication Number 87-104 (http://www.cdc.gov/niosh/docs/87-104/)
Reif JS, Burch JB, Nuckols JR, Metzger L, Ellington D, Anger WK. 2003. Neurobehavioral effects of exposure to trichloroethylene through a municipal water supply. Environ Res. 93(3):248-58.
van Valen E, Wekking E, van der Laan G, Sprangers M, van Dijk F. 2009. The course of chronic solvent induced encephalopathy: a systematic review. Neurotoxicology. 30:1172-86.
Zamyslowska-Szmytke E, Politanski P, Sliwinska-Kowalska M. 2011. Balance system assessment in workers exposed to organic solvent mixture. J Occup Environ Med. 53(4):441-7.
Renal Toxicity
Brosnahan G, Fraer M. 2010. Chronic kidney disease: whom to screen and how to treat, part 1: definition, epidemiology, and laboratory testing. South Med J. 103(2):140-6.
Calvert GM, Ruder AM, Petersen MR. 2011. Mortality and end-stage renal disease incidence among dry cleaning workers. Occup Environ Med.68(10):709-16.
Jacob S, Héry M, Protois JC, Rossert J, Stengel B. 2007. Effect of organic solvent exposure on chronic kidney disease progression: the GN-PROGRESS cohort study. J Am Soc Nephrol. Jan;18(1):274-81.
NIDDK. National Institutes of Health. U.S. Department of Health and Human Services. Kidney Disease Statistics for the US. Available: http://kidney.niddk.nih.gov/kudiseases/pubs/kustats/KU_Diseases_Stats_508.pdf. [Downloaded 1 March 2013]
Scleroderma:
LeRoy EC, Medsger TA, Jr. 2001. Criteria for the classification of early systemic sclerosis. J Rheumatol. 28(7):1573-6.
Mora GF. 2009. Systemic sclerosis: environmental factors. J Rheumatol. 36(11):2383-96.
Kettaneh A, Al Moufti O, Tiev KP, Chayet C, Toledano C, Fabre B, et al. 2007. Occupational exposure to solvents and gender-related risk of systemic sclerosis: a metaanalysis of case-control studies. J Rheumatol. 34(1):97-103.
Guidance for VHA Staff Honoring America’s Veterans and Caring for Camp Lejeune Families Act of 2012, Covered Clinical Conditions
CLINICAL ALGORITHM
The clinical algorithm incorporates the information presented in the guidance in a format that maximally facilitates clinical decision-making. The algorithm can be used as a structured approach in assessing the clinical eligibility of an applicant to the Camp Lejeune program.
The Core Algorithm is a pictorial description of the key steps in evaluating if the applicant has one or more of the conditions covered by the law. The Core Algorithm refers to four sub-algorithms used to identify if there is evidence that the condition occurred as a result of a cause other than exposure to contaminated water during residence at Camp Lejeune.
Standardized symbols are used to display each step in the algorithm. Arrows connect the numbered boxes indicating the order in which the steps should be followed. Rounded rectangles represent a clinical state or condition. Hexagons represent a decision point, formulated as a question that can be answered “Yes” or “No”. A horizontal arrow points to the next step if the answer is YES. A vertical arrow should be followed for a negative answer. Rectangles represent an action in the assessment process. Ovals represent a link forward to another section (i.e. sub-algorithm) or a link back to the Core Algorithm. A letter within a box (e.g., C- 1) refers to text annotation following the flowchart.
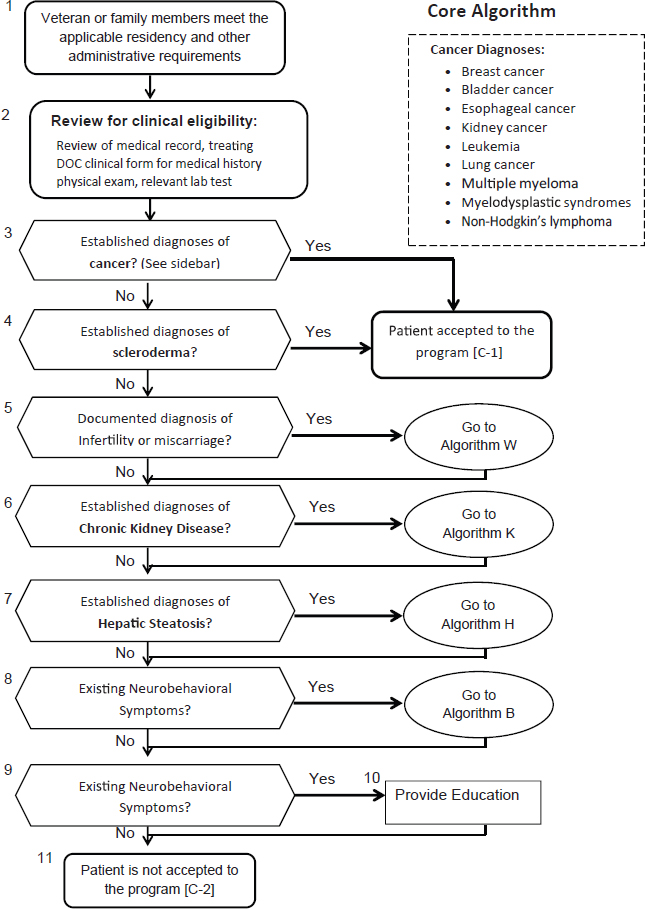
Annotations --- Core Algorithm
C1 --- Applicant has a confirmed diagnosis of cancer or scleroderma. Applicant is clinically eligible for the Camp Lejeune program.
C2 --- Applicant is administratively eligible for the Camp Lejeune program (has resided in camp Lejeune for at least 30 days between Jan 1, 1957 and Dec 31, 1987, but does not yet have any of the 15 medical conditions specified in the law.
Annotations --- Kidney Toxicity
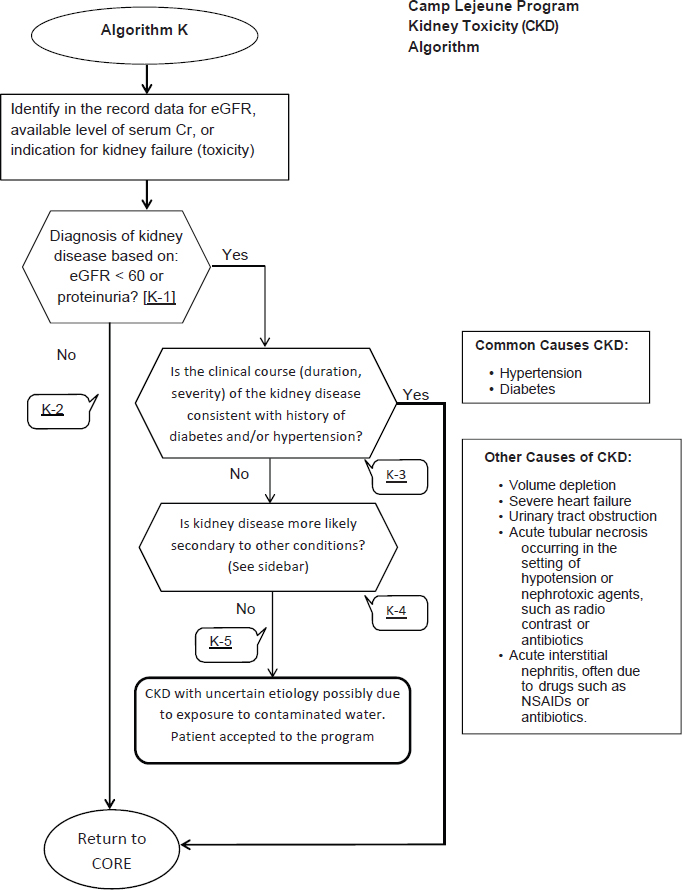
K1 -- Diagnosis of kidney disease: Applicant has a history of renal toxicity or kidney disease concurrent with Camp Lejeune residence or shortly after the time of possible exposure to contaminated water at Camp Lejeune.
The two most common causes of chronic kidney disease (CKD) are diabetes and hypertension. In most instances, it will be possible to identify the most likely cause of CKD using history, physical examination, laboratory testing and imaging tests. A kidney biopsy should be considered for patients with nephrotic range proteinuria (urine to creatinine ratio >3.5), particularly in the absence of diabetes, to determine the histopathology of the kidney disease.
K2 -- Applicant is still administratively eligible for the Camp Lejeune Program but does not have evidence of renal toxicity as a covered condition.
K3 -- Applicant has no history of renal toxicity or kidney disease concurrent with Camp Lejeune residence or around the time of possible exposure to contaminated water at Camp Lejeune. Applicant has evidence of kidney disease due to long standing diabetes or refractory hypertension, which are common causes of kidney failure and are not related to exposure to the contaminants in the water at Camp Lejeune. Current kidney disease is due to another cause other than exposure to contaminated water at Camp Lejeune. Applicant is does not have a covered condition eligible for coverage by the Camp Lejeune Program at this time.
In most patients with diabetes, CKD should be attributable to diabetes if:
- Macroalbuminuria is present; or
- Microalbuminuria is present
- in the presence of diabetic retinopathy,
- in type 1 diabetes of at least 10 years’ duration
Other cause(s) of CKD should be considered in the presence of any of the following circumstances:
- Absence of diabetic retinopathy;
- Low or rapidly decreasing GFR;
- Rapidly increasing proteinuria or nephrotic syndrome;
- Presence of active urinary sediment;
- Signs or symptoms of other systemic disease; or
- >30% reduction in GFR within 2-3 months after initiation of an ACE inhibitor or ARB.
K4-- Applicant has no history of renal toxicity or kidney disease concurrent with Camp Lejeune residence or around the time of possible exposure to contaminated water at Camp Lejeune. Applicant has evidence of kidney disease consistent with a secondary condition that is not related to exposure to the contaminants in the water at Camp Lejeune. Current kidney disease is due to another cause other than exposure to contaminated water at Camp Lejeune. Applicant does not have a covered condition eligible for coverage by the Camp Lejeune Program at this time.
K5-- Applicant has Chronic Kidney Disease of uncertain etiology, possibly related to exposure to contaminated water at Camp Lejeune. Applicant has kidney disease of uncertain etiology possibly related to exposure to contaminated water at Camp Lejeune. Applicant has a covered condition, renal toxicity, and is accepted into the Camp Lejeune Program.
Annotations --- Hepatic Steatosis
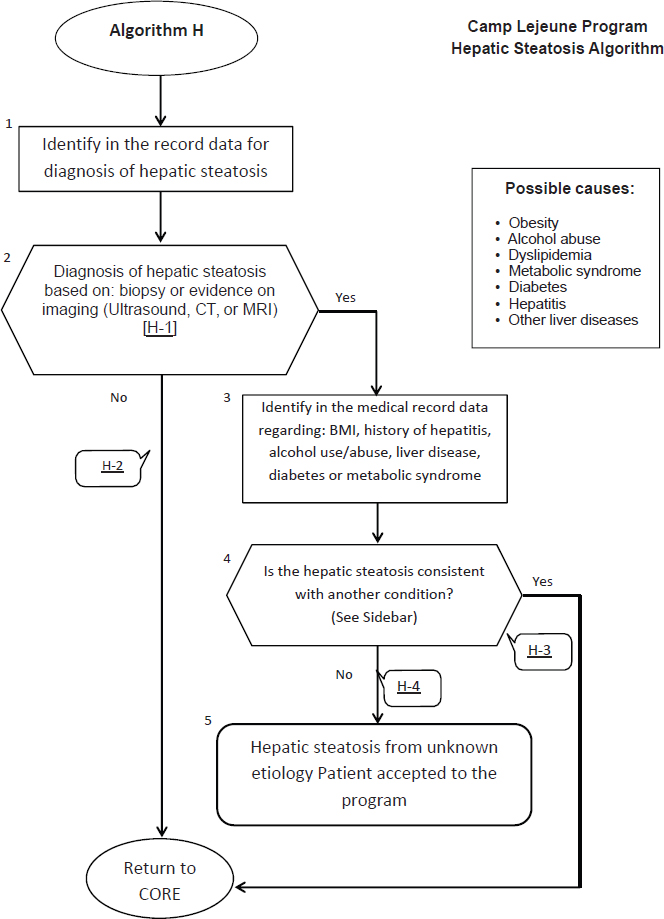
H1 – Hepatic Steatosis (fatty liver) is an accumulation of lipids (triglycerides and other lipids) in the liver hepatocytes. Patients are often asymptomatic. It is often diagnosed as an incidental finding on routine medical exams with blood tests revealing abnormal liver function tests. The most common known causes of steatosis are obesity and alcohol abuse. Other possible causes include dyslipidemia, metabolic syndrome, diabetes, hepatitis or other liver disease. Liver biopsy is the only definitive test to confirm diagnosis, exclude other causes, assess extent and predict prognosis. In most instances, it will be possible to identify the existence of hepatic steatosis and define the extent of the condition using diagnostic imaging techniques (Ultrasound, CT or MRI).
H2 -- Applicant does not have clinical evidence (positive biopsy, CT, MRI, or ultrasound test) of hepatic steatosis at this time.
H3 -- Applicant has clinical evidence of hepatic steatosis due to a cause other than exposure at Camp Lejeune. Fatty liver disease can be divided into two main categories: alcohol-related fatty liver disease and non-alcoholic fatty liver disease (NAFLD). A threshold of <20 gm alcohol per day in women and <30 gm in men suggests a diagnosis of NAFLD. NAFLD is associated with obesity, abnormal glucose tolerance and dyslipidemia, and has been described as the hepatic manifestation of the metabolic syndrome. Fatty liver develops in 46-90% of heavy alcohol users, and in up to 94% of obese individuals.
Current hepatic steatosis is due to another cause other than exposure to contaminated water at Camp Lejeune. Applicant is does not have a covered condition eligible for coverage by the Camp Lejeune Program at this time.
H4 -- Applicant has Hepatic Steatosis of unknown etiology. Applicant is accepted into the Camp Lejeune program.
Annotations --- Neurobehavioral Symptoms
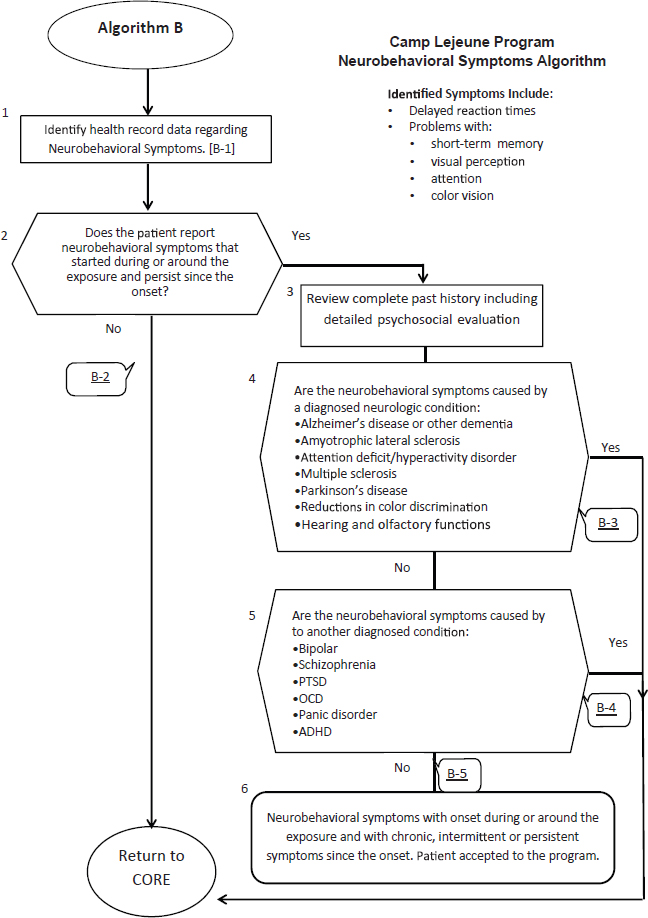
B1 – Identified neurobehavioral symptoms include delayed reaction times, short-term memory impairment, visual perception problems, decreased attention and problems with color vision.
B2 --Applicant did not have symptoms at the time of exposure or documented symptoms first occurred a prolonged time after residence at Camp Lejeune ceased. Research to date has not shown any evidence of onset or progression of symptoms after cessation of exposure.
Applicant does not have neurobehavioral symptoms as a covered condition and is not eligible for the Camp Lejeune Program at this time.
B3 --- Applicant has a neurological diagnosis with neurobehavioral symptoms that are commonly caused by this diagnosis. IOM reviews of solvent exposures in 2003 and 2008 have found inadequate or insufficient evidence of an association between these neurological diagnoses and exposure to the chemicals in the water at Camp Lejeune
B4--- Applicant has a psychiatric diagnosis that causes neurobehavioral symptoms. IOM reviews of solvent exposures in 2003 and 2008 have found inadequate or insufficient evidence of an association between these psychiatric diagnoses and exposure to the chemicals in the water at Camp Lejeune.
B5 --- Applicant has evidence of neurobehavioral symptoms whose onset during or around their exposure at Camp Lejeune. A chronic, intermittent, or persistent symptom since their exposure suggests neurobehavioral effects secondary to exposure at Camp Lejeune. Applicant accepted into the Camp Lejeune program.
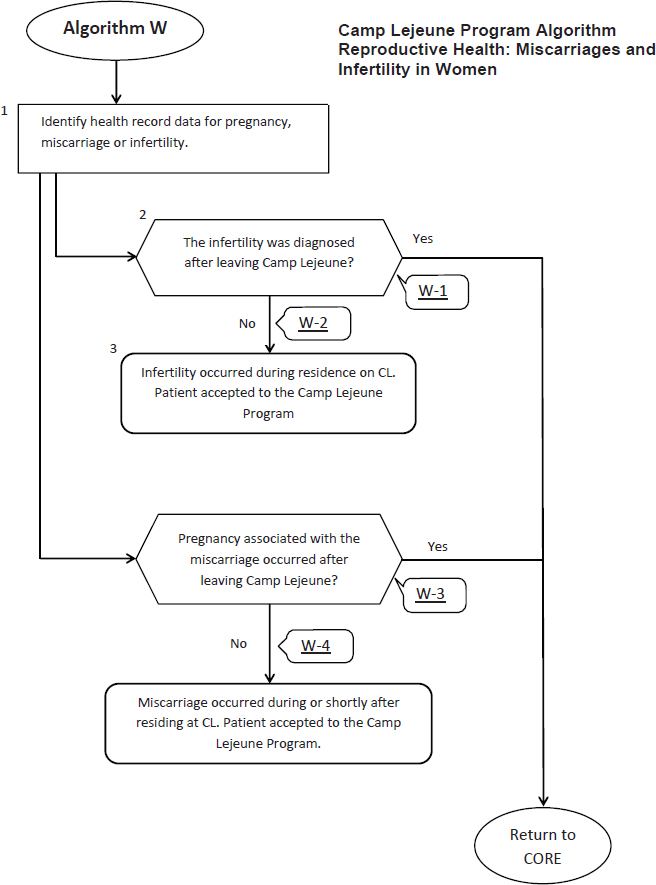
Annotations--- Female Health:
W1 - Infertility was diagnosed after leaving Camp Lejeune. There is currently no scientific evidence to support an association with chronic female infertility after cessation of exposure to solvents. Similarly the NRC report found no evidence that exposure to organic solvents while in-utero increases the risk for adverse fertility effects as a reproductively mature adult. Applicant does not have female infertility that is covered by the Camp Lejeune program.
W2 -Applicant has medical complications requiring continued medical treatment from female infertility while exposed to contaminated water at Camp Lejeune. Medical condition is related to infertility during residence at Camp Lejeune. Applicant accepted into the Camp Lejeune program.
W3 - Miscarriage occurred after leaving Camp Lejeune. Current scientific evidence suggests that there are no persistent effects of solvent exposure on miscarriage or fetal loss. Applicant does not have a miscarriage that is covered by the Camp Lejeune program. Applicant is not accepted into the Camp Lejeune Program at this time.
W4 --Applicant has medical complications requiring continued medical treatment from a miscarriage while exposed to contaminated water at Camp Lejeune. Clinicians should carefully assess whether continued health care is needed for chronic, persistent medical problems associated with a miscarriage that occurred during solvent exposure at Camp Lejeune; if care needs persist applicant is accepted into the Camp Lejeune Program.


























