
9
Place-Based Recovery Strategies for Healthy Communities
Consider that Detroit, an area of 139 square miles and over 900,000 citizens, has just
five grocery stores. An apple a day may help keep the doctor away but that assumes
you can find an apple in your neighborhood.
—James Marks, Robert Wood Johnson Foundation (Marks, 2009)
As discussed in Chapter 2, the concept of “place matters” has grown in recent years, with many health departments and community groups around the country realizing the connection between health status and social determinants such as transportation, housing, and education. As noted by the Robert Wood Johnson Foundation in Time to Act, “place-based differences in health are strongly linked with differences in people’s incomes, educational attainment, and racial or ethnic group” (RWJF, 2014, p. 32). The World Health Organization defines social determinants of health more broadly as “the conditions in which people are born, grow, live, work and age, including the health system. These circumstances are shaped by the distribution of money, power and resources at global, national and local levels, which are themselves influenced by policy choices. Social determinants of health are mostly responsible for health inequities—the unfair and avoidable differences in health status seen within and between countries” (WHO, 2014).
As an example of action to combat some of these place-based health inequities, the Boston Public Health Commission operationalized the concept in 2010 when it launched an interactive “What’s Your Health Code” website to show the variations in health throughout the city depending on the neighborhood and to bring awareness to health equity needs (Boston Public Health Commission, 2010). Other cities have employed various place-based strategies,1 some of which are discussed throughout this chapter, to improve the physical and social environments in communities in hopes of improving the health status of their residents (see Box 9-1 for differences between place-based and people-based interventions). “Place-based policies leverage investments by focusing resources in targeted places and drawing on the compounding effect of well-coordinated action. Effective place-based policies can influence how rural and metropolitan
________________
1 It is important to note that although place-based strategies are geographically targeted, they are not limited to alterations of the physical environment. Place-based strategies often also address the social and economic environments of a community.
BOX 9-1
Place- Versus People-Based Interventions
Although there are a number of ways to define place- versus people-based interventions, the terms are used here as follows:
Place-based—encompasses “real estate- and infrastructure-based activities, including affordable housing preservation and development, commercial development, green space set-asides and improvements, and community facilities including charter schools, health centers, day and elder care centers, and community centers devoted to other community activities and gatherings; transit, communications, and energy improvements.”
People-based—encompasses “child care and job training and placement to enable adults to work and improve their incomes, savings and homeownership programs to help people build assets (but not tied to housing development or rehabilitation), early childhood interventions and charter school services intended to narrow educational achievement gaps, small business development and lending for economic development, community policing and safety, community organizing, and social case work to address special needs like addiction or disabilities or reentry after incarceration.”
People-based interventions are discussed in more detail in Chapter 8.
SOURCE: Belsky and Fauth, 2012, p. 76.
areas develop, and how well they function as places to live, work, operate a business, preserve heritage, and more. Such policies can also streamline otherwise redundant and disconnected programs” (The White House, 2009).
While coordinated, place-based initiatives are strong in theory and academic support, they can be difficult to achieve in practice because of the need for robust collaboration across community agencies, as well as sometimes-significant reallocation of funding. Disaster recovery also requires multi-agency coordination and long-term planning, but it can sometimes be accompanied by more funding and fewer restrictions. Combining these areas of practice and intertwining their goals and policies can have an increased collective impact on a community’s progress toward becoming healthy, resilient, and sustainable. This chapter outlines the evidence behind these theories while highlighting real-life examples that illustrate the effect these types of initiatives can have in practice—both in normal times and during recovery from a disaster.
During this study and throughout its deliberations, the committee identified key place-based recovery strategies that appear as recurring themes throughout this chapter and cut across multiple sectors involved in planning, transportation, sustainability, health, and community development. Application of these strategies, which apply to multiple pre- and post-disaster activities, will facilitate the protection and promotion of health as a community works to meet physical, social, and infrastructure needs after a disaster:
- Reduce health disparities and improve access to essential goods, services, and opportunities.
- Preserve and promote social connectedness.
- Use a systems approach to community redevelopment that acknowledges the connection among social, cultural, economic, and physical environments.
- Seek holistic solutions to socioeconomic disparities and their perverse effects on population health through place-based interventions.
- Rebuild for resilience and sustainability.
- Capitalize on existing planning networks to strengthen recovery planning, including attention to public health, medical, and social services, especially for vulnerable populations.
The chapter concludes with a checklist of key activities that need to be performed during each of the phases of recovery.
A SYSTEMS VIEW OF A HEALTHY COMMUNITY
As discussed in Chapter 2, viewing a community from a systems perspective can help in considering options for rebuilding and holistic recovery. Healthy behaviors do not occur in isolation within a community, so it is important to consider connections among a society’s social, cultural, economic, and physical elements. Simply building a park and a walking trail for residents may not be successful if the trail is not well lit or the park is in an area plagued by crime. In addition to examining how these different systems intersect, it is important to consider how residents in a community are able to access those systems. Rebuilding after a disaster is an opportunity to give these elements a fresh look.
There is growing consensus on the elements that help build a healthy and sustainable community (see Box 2-2 in Chapter 2). This chapter examines some of those elements in the context of the physical and social environments of a community. Specifically, these elements can include clean air, parks and green spaces, a sustainable transportation grid promoting active living, access to nutritious food and clean water, safe communities free of violence, and accessible and integrated community services that can contribute to increased social cohesion. How communities are structured and how public transportation, health care, and social services are built within a city often can dictate the level of access residents have to these and other community services and features. When these elements are not present in a community or their integration is not well designed, making access strained or difficult, adverse health effects can result. The following section expands on this evidence.
The environment in which a person lives influences health in countless ways. The natural and built environments of a community can promote the health of its residents by providing opportunities for physical activity, clean air and water, safe roadways, and access to healthy food and essential services; as noted above, the absence of these elements can hinder health. The physical environment is heavily influenced by a community’s social environment. Neighborhoods with high concentrations of racial minorities or low-income families tend to lack elements that promote health, such as opportunities for activity, and contain elements that hinder health, such as pollution from highways or factories.
Physical Activity and the Environment
Regular physical activity can help reduce or maintain body weight; reduce the risk of cardiovascular disease, diabetes, and some cancers; improve mental health; and increase life expectancy (CDC, 2011). Unfortunately, fewer than half of U.S. adults meet the recommended guideline of 150 minutes of moderate activity per week (CDC, 2014a). Chronic diseases associated with a lack of physical activity plague millions of Americans: more than one-third of adults and 17 percent of children are obese (Ogden et al., 2014), 29.1 million have diabetes (CDC, 2014c), and one in four deaths each year are due to heart disease (Murphy et al., 2013). Inactivity’s burden on the health care system is sizable, with one study estimating the aggregate national cost of overweight and obesity at $113.9 billion (Tsai et al., 2011).
Communities that include parks, sidewalks, and public transit give residents opportunities to be active and can make activity safer and more appealing (Williams, 2007). For example, physical activity levels are higher for people who live near recreational facilities—parks, playgrounds, sports facilities (Sallis et al., 2012)—or whose neighborhood sidewalks are well maintained (Kwarteng et al., 2013). Walking and
biking for transportation are increased when neighborhoods are more densely populated, use a grid pattern, and have commercial areas within walking distance (Transportation Research Board, 2005). People who use public transportation are more active than those who do not, and 29 percent of those who use transit meet the recommended activity level of 150 minutes per week by simply walking to and from transit (Sallis et al., 2012).
When the Austin, Texas, airport was relocated in 1999, the community of Mueller, Texas, was left with 700 acres of what could have been unused space (Mueller, 2014). Instead, Mueller is being redeveloped as a mixed-use urban village as a joint project with the city of Austin. Following a Texas A&M study sponsored by the American Institute of Architects, researchers found that nearly three of four residents reported more physical activity after joining the new community. They found that such elements as sidewalks, parks, open space, and bike routes, along with diverse uses and destinations, supported more physical and social activity (ULI, 2013).
Air and Water Pollution
John Snow famously demonstrated the link between environment and health when he mapped the public wells in his London neighborhood along with the location of cholera deaths. Noticing a cluster around one particular well, he lobbied local authorities to remove the handle from the pump, and the outbreak subsided. Today, environmental threats to communities include particulate air pollution associated with motor vehicle traffic and industrial facilities, and poor water quality related to stormwater management.
Air becomes polluted with particles when mechanical or chemical processes—such as construction, agriculture, or burning of fossil fuels in cars or factories—create tiny particles of chemicals, metals, and other pollutants that are inhaled. This pollution is linked to short- and long-term health issues including respiratory and cardiovascular diseases, cancer, inflammation of lung tissue, exacerbation of asthma, infant mortality, and decreased life expectancy (State of the Air, 2013). The air quality of a community is influenced by its characteristics; for example, industrial plants or large agriculture operations in a community will produce particulate pollutants, while motor vehicles contribute to more than 50 percent of the air pollution in urban areas (CDC, 2009). Altering the built environment of a community to eliminate or diminish these elements may reduce pollution. For example, to accommodate the visitors to the 1996 Olympic Games, Atlanta developed an extensive public transportation system, encouraged telecommuting, and closed the downtown to private automobiles. As a result, peak weekday morning traffic was reduced by 22.5 percent, and there were measurable decreases in air levels of ozone, carbon monoxide, and nitrogen dioxide. During this time period, the number of children seeking acute care or hospitalization for asthma events was significantly reduced (Friedman et al., 2001). This example starkly demonstrates the close relationship among environment, pollution, and health and suggests that changes in the community environment can have an immediate impact on residents’ health. Using “green,” or environmentally friendly, infrastructure also can lower air temperatures, which is valuable in tightly packed urban areas that suffer from the “urban heat island” effect (ASLA, 2010). Another study found that large numbers of trees and green spaces throughout a city can reduce the local air temperature by 1-5 degrees Celsius (McPherson, 1994).
The water quality in a community is affected in part by stormwater management. Stormwater runoff can pollute drinking and recreational water with harmful pathogens such as Cryptosporidium, Giardia, and E. coli, as well as pollutants such as heavy metals, insecticides, and excess nitrogen. While community drinking water is usually treated, several common microorganisms are resistant to treatment and remain in the water (Gaffield et al., 2003). These waterborne pathogens can cause illness and death. In Milwaukee, for example, an outbreak of Cryptosporidium spread via the public water supply and sickened 403,000 people (Mac Kenzie et al., 1994) and contributed to the deaths of 54 people (Hoxie et al., 1997). Contamination by stormwater runoff is more likely when a community has large impervious surface areas, such as roads and parking lots (Gaffield et al., 2003). Runoff can be controlled, and water contamination reduced,
by adding such features as green parking lots, grassed swales, permeable pavement, and vegetation. These types of “green infrastructure” allow stormwater to be absorbed by the ground rather than into the city water system or a nearby waterway. A program in Michigan, for example, diverted roof downspouts into yards rather than into the sewer system. This simple change reduced the flow of stormwater into sewers by up to 62 percent, thus reducing both the cost of water treatment and potential contamination (Kaufman and Wurtz, 1997). Green absorbent infrastructure, while aesthetically pleasing, also can be the most cost-effective way to manage stormwater, in addition to appreciating in value over time and providing multiple uses (Francis, 2010). Elements such as rain gardens or green roofs can mitigate flooding and pollution of the aquifer. One inch of rainwater hitting 1 acre of asphalt produces 27,000 gallons of stormwater over the course of 1 hour (Elmendorf, 2008).
Injuries Associated with Unsafe Streets
Millions of people are injured or killed each year on the nation’s roads. In 2013, 26,491 drivers or passengers and 5,552 pedestrians or cyclists died in traffic crashes (NHTSA, 2014). While many of these injuries and deaths are attributable to individual error, some are due to unsafe road conditions, including roadway design, maintenance, and such features as lighting and crosswalks. A study by the National Highway Traffic Safety Administration (NHTSA) found that 16.3 percent of motor vehicle crashes involved at least one roadway-related factor—roadway condition, view obstruction, geometry of the road, narrow shoulder or road, or missing traffic signs (NHTSA, 2008). Another NHTSA study found that 24 percent of nonfatal pedestrian injuries were due to tripping on cracked or uneven sidewalks, and 13 percent of nonfatal cyclist injuries occurred because the roadway was not in good repair (NHTSA, 2012). Pedestrian safety can be improved not only by maintaining sidewalks but also by using crosswalks with traffic signals, raised medians, and traffic-calming measures such as curb extensions and lane reductions (FHWA, 2005). In short, the condition and design of a community’s roads can contribute greatly to the safety and well-being of its residents.
Hazard Risk
The natural and built features of a community can dramatically affect its ability to withstand and recover from disasters. Natural protective land features such as sand dunes, wetlands, and barrier islands can blunt the impact of a storm or hurricane and protect inland areas from flooding and damage. The design of the built environment—including homes, buildings, and infrastructure—is a critical factor in the health and safety of residents during and after a disaster. It has been said that “earthquakes don’t kill people—buildings do” (FEMA, 2014a). Residences and buildings that are well built and well maintained can help keep residents safe from seismic activity, fire, flooding, and strong winds. In addition, if facilities such as water treatment and power plants are not sufficiently disaster-resilient, the loss of these critical services can make disaster response and recovery even more difficult. For example, millions of residents in New York City lost power during Hurricane Sandy as a result of storm-related damage and flooding. Many residents—including those in the city’s public housing—were without power for more than 2 weeks, during which time they lacked electricity for such essentials as heat and medical devices (Rexrode and Dobnik, 2012).
Health Disparities
Health disparities are “preventable differences in the burden of disease, injury, violence, or opportunities to achieve optimal health that are experienced by socially disadvantaged populations” (CDC, 2013a). Socially disadvantaged populations—such as those of lower socioeconomic status or racial minorities—bear a disproportionate burden of disease and death. African Americans, for example, have higher rates of premature death, infant mortality, obesity, and homicide than their white counterparts, and poor people are
more likely to suffer from asthma, diabetes, and poor self-rated health (CDC, 2013c). These disparities are due in part to differences in the communities in which people live (LaVeist et al., 2011). Neighborhoods populated primarily by racial minorities and/or low-income families are less likely to have a retail outlet offering healthy food (Grimm et al., 2013), more likely to be in close proximity to a highway (and thus pollution) (Boehmer et al., 2013), less likely to have access to recreational facilities (Gordon-Larsen et al., 2006), and more likely to have high rates of street violence (Prevention Institute, 2011). These neighborhoods also have less access to health and other essential services, and their housing, infrastructure, and roads may be poorly built or maintained.
By almost every measure, neighborhoods with concentrations of low-income people and racial minorities tend to be less conducive to health than other neighborhoods, and this difference is exhibited in the disparities in their health outcomes. Babies born in the suburbs of Maryland and Virginia have a life expectancy 6 to 7 years longer than those born a few miles away in Washington, DC (RWJF, 2014). Children who live in low-income urban neighborhoods are more likely to suffer from asthma than their counterparts in bordering neighborhoods (Olmedo et al., 2011). These health disparities might be diminished by efforts to change the environment of the neighborhood through policies designed to improve housing, transit, infrastructure, sources of pollution, and access to healthy food and health care (Lee and Rubin, 2007).
A Systems Approach for Health Improvement
While the natural and built environments have direct effects on population health and the social determinants of health, it is important to consider the socioeconomic systems that operate within those environments. There are obvious relationships between the shape, pattern, and composition of physical environmental features and socioeconomic systems. When it is necessary to rebuild or repair a community’s physical infrastructure, including residences and businesses, it makes sense to do so in concert with strategies addressing the services and systems that operate there. In New Orleans after Hurricane Katrina, for example, major repairs were needed for many features of the health care infrastructure. In light of more serious underlying problems represented by low metrics of population health, however, the community and its health care leadership fashioned a whole new approach, a reconfiguration of the entire system, instead of simply rebuilding those buildings that had been damaged by the storm and subsequent flooding. Thus, physical environments and human systems within those environments determine success in striving for a healthy community.
Well-being is a general metric of how well the community functions, how smoothly its systems perform. Social and health disparities typically arise when system performance wanes or, rarely, in the event of a disaster. Significantly, many federal and other government programs address issues of socioeconomic system failure. Those same programs, to varying degrees, are forced into “overdrive” when a disaster strikes—old problems are exacerbated and new problems arise. One example concerns crime, especially violent crime that has a severe negative effect on health. A contributor to crime is poor community design. A partial remedy for crime is to design streets, sidewalks, businesses, and housing to incorporate impediments to criminal behavior and to increase social observance of public places through increased social activity and stronger social capital. Also needed, however, is attention to crime prevention systems such as crime analysis, effective policing, and new inducements for those who may be inclined to pursue crime. Obvious linkages are education, employment, poverty, behavioral health, and a variety of social service initiatives pertaining to substance abuse, teen pregnancy, gambling addiction, and early childhood development. In this context, it is not sufficient simply to restore the community to its prior state after a disaster. Achieving a safe environment promises major co-benefits for health, especially for vulnerable populations.
These relationships are crucially important after a disaster, and they affect the pace of recovery because these fundamental risks in society’s systems are ever present, but they are stressed and exacerbated by a disaster. The committee heard testimony, for example, on the toxic effect of temporary housing on children as a result of relocation, change of schools, and other disruptions (Redlener, 2014). Restoring the natural and built environments after a disaster is an important step, but attention must also be paid to
system weaknesses. Importantly, this is a challenge already well recognized because communities of all sizes must wrestle with the high cost of servicing neighborhoods dominated by disparities in the socioeconomic system. Addressing blight, poverty, low educational attainment, commercial decline, joblessness, and the full range of negative influences from deteriorated housing is the mission of community development (supported in part by the U.S. Department of Housing and Urban Development’s [HUD’s] Community Development Block Grant). Communities with experience in system remedies are well suited to bridging the gap between concerns for the natural and the built environment and the social and economic functions within those environments.
Box 9-2 highlights a real-world example of a community using this type of systems planning in its disaster recovery. Springfield, Massachusetts, came together as a community following a tornado in 2011 that destroyed areas of the city and used a “nexus” framework for an integrated approach to recovery project planning. Since creating the plan and executing the plan are fundamentally different and also can be separated by a period of months or even years, it will be important to monitor how Springfield’s plan becomes operational to see whether the community’s needs are truly met when competing financial priorities arise. Coordinated implementation of the plan elements is necessary so that each element is not implemented as an individual project, which could lead to inefficiencies and gaps in execution.
Contemporary Approaches to Healthier and More Resilient and Sustainable Communities
Revisiting the “duality of use” concept, many agencies and organizations outside the health sector also are thinking about sustainable, long-term planning for communities. As it happens, many of the smart growth strategies recommended by the U.S. Environmental Protection Agency (EPA) for achieving sustainability also can have positive impacts on community health as well as mitigate the impacts of a disaster.
As discussed earlier, environmental quality has both direct and indirect effects on population health. Major improvements in water quality in the nation’s streams and lakes have been made since the 1970s. Planning for better infrastructure for wastewater treatment has lowered concentrations of toxic material. In some extreme cases—such as Love Canal in New York and Times Beach in Missouri—homes have been relocated away from hazards because of explicit health risks. Community plans also have become more health conscious. Transportation planning has integrated measures of environmental effects on the population, including emissions, noise, safety, and elements that facilitate pedestrian and bicycle travel for both recreational and commuting trips. Themes such as smart growth represent an attempt to balance social and economic objectives. EPA’s report on creating equitable, healthy, and sustainable communities describes smart growth as “a range of strategies for planning and building cities, suburbs, and small towns in ways that protect the environment and public health, support economic development, and strengthen communities” (EPA, 2013, p. 4). The Partnership for Sustainable Communities, an initiative of the U.S. Department of Transportation (DOT), HUD, and EPA, is the centerpiece of the nation’s new approach (DOT et al., 2014), empowered by three factors: (1) coordinated financing, (2) planning mandates, and (3) technical assistance. While this notion of development and interaction with the environment goes back decades, new ways of incorporating sustainable strategies and elements into homes, public centers, parks, and other sections of a community have increased in recent years.
Accompanying this shift is guidance and renewed energy from EPA and such groups as the Partnership for Sustainable Communities and the American Society of Landscape Architects. In 2009, through a partnership with local government councils, EPA developed smart growth guidelines for sustainable design and development for communities striving to achieve future growth that results in stronger neighborhoods, protected open space and watersheds, and healthier and more affordable homes (EPA, 2009). These strategies, coupled with “green” initiatives—environmentally friendly approaches that can range from building practices to product labeling to chemical engineering—can lead to a more resilient, sustainable community. These practices, although created with sustainability in mind, can have an impact on the health of a population. For example, people in communities with abundant green space tend to be healthier (Maas et al., 2006). Cities incorporating green infrastructure into their planning often find
BOX 9-2
Building the Community Nexus
Significant social and financial costs are associated with siloed approaches to community planning and the resultant inefficiency. For communities looking to design a more collaborative and systematic approach, particularly in the process of rebuilding following a disaster, the “nexus” concept may serve as a guideline for meeting the comprehensive needs of community members. These needs, which include a community’s most crucial quality-of-life resources, fall into six domains:
- the physical domain, which includes a community’s built and natural resources;
- the cultural domain, which includes those aspects of a community related to individual and collective values;
- the social domain, which governs well-being and includes a community’s health and human services;
- the economic domain, which works to maintain a healthy balance among a community’s financial, human, and environmental capital;
- the organizational domain, which encompasses programs and services such as community clubs, civic societies, and city and county school boards and councils; and
- the educational domain, which covers the span from early childhood education to college, as well as workforce training programs.
It is the nexus of interactions among these domains that will best serve to promote a community’s overall wellbeing and health.
The nexus planning framework is a highly integrated model in which a nexus of planning exists for the people, programs, and places involved in the provision of public services and programs. A fully developed nexus site will serve as the place where a variety of community services and amenities—such as grocery stores, farmer’s markets, parks, libraries, child care centers, and schools—are situated, coordinated, and administered to best address and serve the needs of the community. Importantly, the approach transcends physical design,
that the environmental benefits justify the up-front costs and are worthwhile for day-to-day needs, such as by reducing energy use, filtering air and water pollutants, and preserving wildlife habitats. Preserving habitats to ensure healthy ecosystem functioning can have a positive impact on the dense urban and suburban environments in which more than 80 percent of the U.S. population lives (USDA, 2014). For those concerned about hazard mitigation and resiliency, such strategies as green roofs, rain gardens, and porous concrete can help manage stormwater runoff, alleviate flooding, and prevent aquifer pollution after a hurricane or other disaster.
Again, however, many of these ideas are attractive in theory and in the planning stages, but they are sometimes challenging to execute. To overcome such barriers, federal agencies are using programmatic incentives to drive sustainable change in communities that aligns with national strategic priorities. Leadership in Energy & Environmental Design (LEED) for Neighborhood Development (LEED-ND), for example, is “a rating system that incorporates principles of smart growth, New Urbanism, and green building into a voluntary framework for sustainable neighborhood planning and design” (HUD, 2012). To incentivize the use of this framework, “HUD recently incorporated LEED-ND into all of its grant funding through the General Section and required LEED-ND certification for Choice Neighborhoods Planning Grant recipients” (HUD, 2012). Other federal support and community grants with this type of focus on green development and smart growth strategies can help communities manage hazards in a cost-effective way while realizing other benefits for social and physical well-being.
and also integrates program design and policy tools. For example, joint use agreements can expand access to amenities by enabling the community to use school facilities such as gyms, auditoriums, and libraries during evenings and weekends. The result is not only a more sustainable community but also a more equitable one—vehicle ownership is no longer a prerequisite for accessing community amenities and services. The opportunity for increased physical activity benefits all community members.
In Springfield, Massachusetts, redevelopment under a nexus framework is under way in response to a devastating tornado that tore through the city on June 1, 2011. In the aftermath of this disaster, citizens came together to develop a community-driven plan called Rebuild Springfield, with both residents and stakeholders working collaboratively inside the nexus framework. Among the recommendations prioritized as part of this plan is putting schools and libraries at the center of a nexus approach to provide a wide range of community services and programs. One proposed approach for catalyzing this process is the development of partnerships between public library branches and educational institutions.
Springfield has been designated as a “Gateway City,” a title given to formerly thriving industrial cities now showing promise as regional economic and cultural centers. Many recommendations of the Rebuild Springfield plan take into account and celebrate Springfield’s cultural diversity. The redevelopment proposal emphasizes the need to better connect the community, both physically and culturally. This will be accomplished with improved transportation systems, as well as efforts to increase access to cultural amenities through coordinated outreach.
Rebuild Springfield represents a unique example of a planning project developed entirely around the nexus framework and domains. While implementation of Springfield’s plan is still in progress, there are numerous examples of completed nexus sites whose positive impact on their communities can already be observed. In Houston, Texas, the Baker-Ripley Neighborhood Center was completed in 2010 and serves as a true neighborhood nexus site. The center includes an elementary school, a public library, a farmer’s market, parks, business facilities, and a community health center. Since its completion, the center has become a vibrant community hub, providing a vast number of services for a previously underserved community.
SOURCES: Bingler, 2011, 2014; Springfield Redevelopment Authority, 2012.
DISASTER IMPACTS ON COMMUNITY SYSTEMS: IMPLICATIONS FOR HEALTH AND RECOVERY
Following a disaster, the short-term impacts on community systems and overall health generally are well known, often receiving significant media coverage. Initial concerns include impeded access to goods and services—including food and supplies and ambulance services—because of impassable roads or nonfunctioning transit. Another concern is impaired functioning of critical infrastructure that provides clean water to the community and power to important buildings such as hospitals. Environmental degradation that can exacerbate existing conditions (e.g., asthma) or cause new ones may be less apparent in the immediate aftermath of a disaster. After Hurricane Sandy, for example, “Floodwaters, massive storm runoff, wind damage, and loss of electricity combined to cause wastewater treatment plants up and down the mid-Atlantic coast to fail. These failures sent billions of gallons of raw and partially treated sewage into the region’s waterways, impacting public health, aquatic habitats, and resources” (Hurricane Sandy Rebuilding Task Force, 2013, p. 27).
By the time long-term disaster impacts start to manifest in a community, the media cameras usually are long gone, and many downstream consequences go unnoticed until the situation reaches a threshold. Occasionally, commercial buildings or housing projects are too damaged to be repaired easily, so they are abandoned or shifted further down the priority list. The result can be an increase in blight and associated crime, causing the community to break up and individuals to scatter across a state or region. Positive health effects of the social capital that existed in the neighborhood may be at risk. Because disasters often cause disproportionate hardship for vulnerable populations and low-income neighborhoods, recovery planning
requires careful demographic analysis. Post-disaster reconstruction and relocations are steep hurdles for individuals and families. Upgraded construction codes, mitigation requirements, and changes in actuarial insurance rates are major challenges for elderly and fixed-income individuals, for example. Neighborhood changes and the loss of hospitals, physicians, grocery stores, and pharmacies can exacerbate the hardships faced by residents even if temporary housing is provided. Rarely do recovery plans address all of these needs, nor can restoration of full community services be accomplished immediately, leaving the population in dire straits at a time when all forms of stress and uncertainty are at their highest levels. This is an important unmet need. If a family is displaced from its affordable housing but wants to stay in the community, there may be limited options for doing so. All of these scenarios lead to further deterioration of the social determinants of health.
It is possible to overcome these challenges, although as Robert Olshansky from the University of Illinois testified to the committee, intensive planning is required to rebuild a city successfully after a disaster (Olshansky, 2014). Building a city under normal circumstances is highly complex, with many different actors involved. Added complexity arises during disaster recovery as a result of the compression of time in which the same set of tasks must be accomplished. Despite the added challenges, this planning process should be guided by a shared goal of helping people create settlements that are healthy and safe places to live that provide viable livelihoods, and that enable convenient access to all of the things they need. Sudden loss creates opportunities for reorganizing the elements of a community—not just facilities, but also services. As discussed earlier, disaster-related challenges provide an opportunity to approach community redevelopment in ways that improve health and social well-being. It is important to note, however, that the extent of need and opportunities for community redevelopment will depend on the pattern and extent of the damage caused by a disaster. Every disaster may not present the opportunity to revamp the community or undertake long-term planning. For example, tornados usually leave the foundations or basements of buildings intact, so the most economical solution often is to build on the preexisting base, keeping the same footprint.
ORGANIZATIONAL STRUCTURES AND RESOURCES FOR HEALTHY COMMUNITY PLANNING AND REDEVELOPMENT
In steady-state times, a number of federal agencies provide funding and technical assistance to support the development of the built and natural environments. A comprehensive review of these resources is beyond the scope of this report, but the relevant agencies and funding sources related to community development and rebuilding are briefly reviewed here. As mentioned earlier, the major federal agencies whose policies and funding shape the built and natural environments in the United States came together in 2009 to form the Partnership for Sustainable Communities. Through the efforts of DOT, HUD, and the EPA, “more than 1,000 communities in all 50 states, Washington, D.C., and Puerto Rico have received more than $4 billion in grants and technical assistance to help them grow and improve their quality of life” (DOT et al., 2014, p. 2).
Individually, the agencies within the partnership also are major funding sources for sustainable community building. DOT offers the Transportation Investment Generating Economic Recovery (TIGER) Discretionary Grant program that enables applicants to invest in road, rail, transit, or port projects. Applicants must describe the benefits of their proposed project for “five long-term outcomes: safety, economic competitiveness, state of good repair, livability and environmental sustainability” (DOT, 2015).
In response to community demands from around the country, EPA’s Office of Sustainable Communities launched the Building Blocks for Sustainable Communities Program. This program offers targeted technical assistance to selected communities using tools that already have demonstrated widespread results.
________________
2 A broader synopsis of legislation and federal policy related to disaster recovery and health security can be found in Appendix A.
To illustrate some of the topic areas within the program, the topics highlighted for the 2015 program are listed below, showing overlap among sustainable objectives for cities, hazard mitigation needs, and healthy community elements:
- bikeshare planning,
- supporting equitable development,
- infill development for distressed cities,
- sustainable strategies for small cities and rural areas, and
- flood resilience for riverine and coastal communities (EPA, 2014).
HUD offers the Community Development Block Grant (CDBG) program, alluded to earlier, which provides funds for addressing a wide range of community needs. Specifically, grantees must use at least 70 percent of the funding for projects directed at low- or moderate-income populations and encourage citizen participation (HUD, 2015). The program provides annual funding to state and local entities, but it also is flexible enough to provide assistance following a presidentially declared disaster, subject to the availability of a congressional supplemental appropriation.
HHS also has a role in healthy community development. The Centers for Disease Control and Prevention’s (CDC’s) Built Environment and Health Initiative (also known as the Healthy Community Design Initiative) works to improve community design decisions by linking them with public health surveillance, utilizing such tools as the health impact assessment (HIA), building partnerships with key decision makers in the community, and conducting research and translating its results into best practices. The initiative funded and supported 34 HIAs in 2011 and continued to fund 6 local, county, and state entities’ HIAs from 2011 to 2014. Data from the HIAs have been used to develop health-focused frameworks in communities in Nebraska, North Carolina, and Oregon (CDC, 2013b). Additionally, the Patient Protection and Affordable Care Act (ACA) authorized the Community Transformation Grant Program through the CDC, aimed at helping communities design changes to their built and social environments to address chronic diseases3 (CDC, 2014b).
After a disaster, a number of different federal funding mechanisms come into play. When a disaster exceeds the capacity of the state or locality to respond, a presidential disaster declaration can bring in federal aid under the Robert T. Stafford Disaster Relief and Emergency Assistance Act4 (CRS, 2014; see also Chapter 4). The National Disaster Recovery Framework (NDRF, described in detail in Chapter 3), serves as a conceptual guide for recovery planning at all levels of government and is intended to improve coordination of federal recovery resources (FEMA, 2014b). Similar to the Emergency Support Functions (ESFs) of the National Response Framework (NRF), the NDRF introduces six Recovery Support Functions (RSFs), each designated to a different lead federal agency:
- Community Planning and Capacity Building—Federal Emergency Management Agency,
- Economic—U.S. Department of Commerce,
- Health and Social Services—U.S. Department of Health and Human Services,
- Housing—U.S. Department of Housing and Urban Development,
- Infrastructure Systems (including transportation) —U.S. Army Corps of Engineers, and
- Natural and Cultural Resources—U.S. Department of the Interior (FEMA, 2014b).
Under the NDRF, a FEMA official functions as the federal disaster recovery coordinator and for presidentially declared disasters, FEMA also provides public assistance and hazard mitigation funding for repair and restoration of public (and some nonprofit) infrastructure where needed. Although HUD leads
________________
3 Funding for the Community Transformation Grant Program was eliminated by Congress in the Fiscal Year 2014 Omnibus package.
4 42 U.S.C. § 5121 et seq.
the Housing RSF, it is also an important funder for major disasters if Congress makes a supplemental appropriation through HUD’s CDBG program for Disaster Recovery (CDBG-DR) as a vehicle to aid rebuilding efforts and to provide the start-up funds necessary to initiate the recovery process. Since such funding may support a wide range of recovery activities, it enables HUD to better assist communities that otherwise might not recover because of limited resources and to prevent them from experiencing the long-term health impacts discussed previously (HUD, 2014). However, as discussed in Chapter 3, HUD’s community development function has not adequately been integrated into the NDRF.
The framework aspires to better utilization of existing resources; however, it does not yet clearly capture the contemporary healthy community and sustainable development practices that are being led by CDC and the Partnership for Sustainable Communities. As discussed in Chapter 3, the NDRF needs to be upgraded to reflect these prior achievements and their relevance to disaster circumstances. Combined, these additional themes of integration and transformation could foster a major advance in the nation’s capacity for disaster recovery.
As discussed in Chapter 3, states and regional entities have key roles in recovery, and in many cases, they are the grantees for federal grant programs in the case of a presidentially declared disaster. State emergency management agencies, for example, are the grantees for FEMA Public Assistance and Hazard Mitigation Grant Programs, and they must work closely with community planning entities to manage mitigation activities. For optimal vertical integration, state agencies need to align with the NDRF structure and, in doing so, should ensure that their state-level entities with everyday responsibilities for urban or regional planning and development are incorporated into the RSF structure and understand their roles. For long-range transportation planning, for example, there are transportation planning and policy assets and personnel at both state and regional levels that need to be incorporated into long-term recovery planning following a disaster to see projects through to fruition. The state should not rely on the emergency operations personnel that may have represented that sector during the immediate response to fulfill an ESF.
In contrast to the strong state-local relationships designed into financial, technical, and operational systems funded by DOT, HUD, and EPA for steady-state community planning, disaster recovery is a process that often reveals a mismatch between state and municipal governments. Because of the infrequency of disaster occurrences and the absence of strong policy foundations, states, cities, and counties do not have regular opportunities to share information or practice how to address recovery issues that arise during disasters. Strategies of redevelopment, economic incentives, and neighborhood revitalization are inherently in the municipal domain and may not be well understood by state agency personnel. After Hurricanes Katrina, Rita and Ike, both Louisiana and Texas experienced tumultuous reorganizations of their disaster recovery programs midstream, with legislative and media investigations of disharmony (Kirkland, 2012). States need to organize and align their RSF structure with both the national and the local level to ensure that events from past disasters are not repeated.
Since some planning—particularly for transportation and economic development—takes place primarily at the regional (substate) level, it is important for those organizations to be included in the development of recovery plans, especially as their functions may align with the NDRF structure. Metropolitan planning organizations (MPOs) play a large role in organizing and executing transportation planning throughout a defined urban area of one or more counties and sometimes a multistate region. Since they already exist, with defined leadership, processes, and networks, they often can play an important role in making recovery decisions for transportation- and development-related issues. In Washington’s Puget Sound region, for example, the 2014 Transportation Recovery Annex recommends including MPOs in a transportation stakeholder forum for the development of regional transportation recovery policies (Washington Emergency Management Division, 2014). Because the Economic Development Administration serves as the coordinating agency for the Economic RSF (EDA, 2015), organizing the regional economic development districts to align with the NDRF structure also can facilitate the recovery process for a community. By
becoming involved in recovery at the regional level, the economic development districts can provide important on-the-ground knowledge and awareness to the federal RSF lead and ensure that national recovery decisions are being made with the most accurate economic information available.
Comprehensive plans created at the local level drive land use policy and community investments in infrastructure, but different locally derived structures for developing and implementing policies for health exist across the country. In Pinellas County, Florida, for example, the health department is actively engaged with other departments in addressing the needs of blighted and deteriorated neighborhoods, followed by redevelopment with new, safe construction enabled by HUD grants and interagency collaboration. King County in Washington is taking a similar approach through its Communities of Opportunity program (see Box 2-8 in Chapter 2). Yet there are virtually no known research cases that address how this kind of demonstrated capacity of health and social service agencies at the local level to achieve high levels of collaboration around development policies translates to better post-disaster recovery. It is reasonable to assume that this approach can offer distinct advantages and that better plans will result when health, medical, and social services are viewed holistically among themselves and with other community policies of a recovery plan.
Like state and regional entities, local government agencies need to align with the NDRF structure and appoint or identify representatives to coordinate with their state, regional, and federal counterparts. Such arrangements should be put in place before a disaster. While recommendations and guidelines may come from the state or national level, ultimately it is often up to the local government to decide how to reinvest in its community. As discussed throughout this chapter, there are many ways to leverage strategies and the energy and interest of community leaders to bring about positive change at the local level.
Nonprofits, Philanthropies, and the Private Sector
Nonprofit organizations and businesses have a vested interest in rebuilding in the communities in which they work and with which they feel a connection, and therefore, they also should be included in discussions at the local government level to facilitate and execute recovery planning. Philanthropies can be important funders for redevelopment to address the needs of underserved populations, especially those groups, such as the Rockefeller Foundation and the Robert Wood Johnson Foundation, that support resilience building and improvement of the social determinants of health in their day-to-day work. Following a disaster, having their added funding along with expertise in focusing health interventions on vulnerable populations also can aid in long-term recovery. After a disaster, nonprofit organizations such as Architecture for Humanity provide pro bono design services through their membership. These groups need to be engaged proactively in recovery planning to ensure that recovery activities are seamless across the spectrum of a community.
Nonprofit institutions and the private sector also can play a role in financing recovery and supporting public health outcomes. The Reinvestment Fund is a Community Development Financial Institution (CDFI) that serves people who might otherwise be disconnected from the credit system (TRF, 2015). CDFIs use federal resources, such as incentives, tax credits, and bond guarantees, to serve low-income people and communities that lack access to affordable financial services and products (U.S. Department of the Treasury, 2014). This sector also is experiencing a change in focus, with increased awareness of the nexus between healthy and productive communities. In recognition of this nexus, one nonprofit CDFI, the Low Income Investment Fund, has been taking a more holistic approach that involves not only building affordable housing in a neighborhood but also building and supporting high-performing schools, health clinics, and recreational facilities with access to public transit (IOM, 2014b). While some might be skeptical that larger banking institutions would invest in these kinds of community development projects, the Commu-
nity Reinvestment Act,5 passed in 1977, mandates that banks reinvest in low-income communities from which they take deposits. They are graded on their performance in this regard and so are incentivized to strive for higher rankings. Tax credit incentives through the New Markets Tax Credit also are spurring investors to revitalize impoverished areas. Established as part of the Community Renewal Tax Relief Act of 2000,6 it has helped jump-start community development and is used to capitalize lending institutions that finance small businesses and help address the social determinants of health in low-income neighborhoods (Erickson and Andrews, 2011).
Collaboration and Coordination
During steady-state periods, mechanisms for collaboration and coordination are necessary because of the interconnected nature of the various facets of community planning (e.g., land use and transportation). These mechanisms are essentially systematic arrangements for professional teams and advisory groups to carry out analysis and program development that includes plans, projects, and budgets. Some groups, such as MPOs, are more familiar and comfortable with working together than others because they operate together routinely. For others, it is important to assess the ability to work together on short notice in the event of a disaster demanding multisector recovery planning. Such an assessment needs to consider the ability to collaborate across sectors and whether the partners are familiar with each other’s language and terminology. With the emergence of many new opportunities for partnerships with the health sector, the question arises of what collaboration among various sectors would look like. In a 2013 study conducted for the Robert Wood Johnson Foundation’s Commission to Build a Healthier America, the researchers wanted to measure the degree to which cross-sector collaboration occurs between health and other sectors, whether such collaborations have positive effects, and what the indicators of positive collaboration are (Mattessich and Rausch, 2013). They report that respondents frequently cited major benefits of collaboration such as pooling resources and dividing risk. They also note that skilled leadership was identified as one of the top three factors for a successful collaboration, yet at the national level, no single formal network exists to unify this newly emerging field of cross-sector collaboration aimed at improving health (Mattessich and Rausch, 2013). Finally, they emphasize the importance of “building the evidence base for cross-sector initiatives that effectively improve health by creating environments that protect and actively promote health” (Mattessich and Rausch, 2013, p. 10). Determining how to acquire and share the evidence needed to make the case for joint investments can make partnerships between the health sector and entities involved in the design of the physical environment even more attractive and widespread. If such integrated initiatives can be shown to save medical costs downstream, health management and affordable care organizations may have an even greater incentive to collaborate (Erickson and Andrews, 2011). New networks can create an opportunity for breaking down siloes to achieve shared goals across sectors. Opportunities for such collaborations are discussed in the sections below.
Planning and Design
Although community planning as a field was created in large part in response to public health needs (e.g., addressing sanitation issues), the fields of public health and planning have since diverged. There is growing recognition, however, that these two sectors cannot continue to operate in isolation (Ricklin et al., 2012). Health concerns increasingly are falling within the scope of planning departments, and the public health field has discovered the power of comprehensive plans, social capital and cohesion, and other planning tools for altering the physical and social environments that impact health. As discussed earlier in this chapter, decisions being made about community design, land use, and transportation are
________________
5 Community Reinvestment Act of 1977, Public Law 95-128, 91 Stat. 1147, Title VIII of the Housing and Community Development Act of 1977, 12 U.S.C. § 2901 et seq.
6 Community Renewal Tax Relief Act of 2000, incorporated into Public Law 106-554.
having effects on air and water quality, physical activity, exposure to contaminated industrial sites, and other important determinants of health.
Recognizing this linkage, New York City established a working group in 2010 comprising design organizations; academics; and city agencies involved in health, city planning, transportation, and construction. The group was tasked with developing Active Design Guidelines—“evidence-based and best-practice strategies for increasing physical activity in the design and construction of neighborhoods, streets, and buildings” (Lee, 2012, p. 5). Likewise, the American Institute of Architects has established a New Design and Health Agenda, and in 2014 it held a summit focusing on how public health officials and designers can intersect (AIA, 2014). Planners are beginning to understand the impact they can have on public health, and some public health departments are even hiring planning professionals to advise communities on healthy designs. Likewise, planners would benefit from data and metrics that are available to public health departments to understand where interventions would best be implemented. A recent example of such partnerships is King County Board of Health’s adoption of “Planning for Healthy Communities” guidelines in 2011. These guidelines are intended to inform land use and transportation planners about strategies that could have an effect on all residents of King County, Washington, based on actual causes of death and illness (King County, 2011).
Community Development Entities
Recent years also have seen increased collaboration between the community development sector and the public health sector as greater understanding of their shared goals reveals opportunities to coordinate or combine their individual funding streams. As with the planning and green infrastructure sector, community development entities are realizing that the benefits of their efforts extend to health. At an Institute of Medicine (IOM) workshop on financing population health, Raphael Bostic, the Judith and John Bedrosian Chair in Governance and the Public Enterprise at the Sol Price School of Public Policy, University of Southern California, said he believes a reset is occurring in the way people think about community development and population health (IOM, 2014b). He attributed this reset in part to demonstration projects in the housing and urban development sectors revealing the largest effect on health benefits:
For example, the Moving to Opportunity program, in which low-income families were given vouchers that enabled them to move out of areas with concentrated poverty, produced marked improvements in stress-related outcomes, depression, obesity, and diabetes. “That was a wake-up call,” Bostic said. “When the demonstration started, health was not even on the radar screen.” (IOM, 2014b, p. 27)
Erickson and Andrews (2011) also argue that through the ACA, federally qualified health centers should coordinate more closely with community development entities. If medical clinics were able to connect more easily and seamlessly with a network with existing links to funders, social services, and other community organizations, divisions between sectors could be further broken down.
The increased awareness of shared goals between the community development and health sectors is encouraging but represents only a first step. The Robert Wood Johnson Foundation’s Commission to Build a Healthier America recommends that the United States fundamentally change its approach to revitalizing neighborhoods by fully integrating health into community development (RWJF, 2014). By extending the concept of “health” into the neighborhoods where people live, play, and work, both sectors can think more broadly about potential interventions and desired outcomes to build healthier communities.
Transportation
Transportation has long been associated with public health with respect to prevention of injuries related to vehicle crashes and safety laws such as those mandating the use of seatbelts. However, DOT and the Federal Highway Administration (FHWA) also have been involved in policies related to health,
and increasingly are regarding healthy outcomes as an important part of their objective in creating livable, sustainable communities. In 2012, they created a Health in Transportation Working Group to examine their policies and regulations on health issues, as well as ways to incorporate health into transportation planning and educate both internal and external stakeholders (FHWA, 2015).
Awareness of this connection occurred at the state level in Massachusetts. In 2009, a strong transportation reform law designed to consolidate disparate services in the state led to the development of the Healthy Transportation Compact, an interagency group chaired by the secretary of transportation and secretary of health and human services at the state level. Its goal is to collaborate on the potential health effects of transportation decisions. Examples of the group’s initiatives include:
- Mass in Motion Program (a statewide program that promotes opportunities for active living);
- Municipal Wellness Grants (distributed at the local level so communities can increase opportunities and customize initiatives to their needs); and
- Safe Routes to School (which promotes healthy alternatives for children to travel to school) (IOM, 2014a).
Creating a Healthy Community Vision for Recovery
Prior to a disaster, when there is time to think through priorities, leaders can take various actions to create and promote a healthy vision for recovery should a disaster strike. Holding community planning and visioning workshops—also called charrettes—is a good way to obtain input from residents with which to prioritize needed actions, and it also can secure buy-in for projects or developments. Such visioning exercises may have been conducted in the past, either as a coordinated effort or by separate groups. As discussed in Chapter 3, building on these efforts and being as inclusive as possible can ensure less push-back by those who contributed previously and may shorten the timeline for action if work has already been done or processes designed.
In these efforts, it is important to engage the health sector. The health sector is a source of data and information that may be difficult to find elsewhere (e.g., from community health assessments); it has connections with various community networks; and it brings a different perspective on strategies for building stronger communities. The vision and goals created from these workshops should be incorporated into the overall comprehensive plan for a town or city, as discussed in Chapter 3.
Organizing for Disaster Recovery Planning
Each sector has its own roles and responsibilities in recovery planning that need to be laid out, but a forum also is needed to identify and create synergy among the various projects and programs being planned. There may often be overlap or shared goals across projects within a community, and being aware of those projects and their goals before a disaster will facilitate streamlining recovery in a coordinated manner should such an event occur. It is difficult to plan what every sector’s actions will be during pre-event recovery planning, since most communities are at risk of several different types of disasters with varying impacts. Nonetheless, it is important to plan the operations and identify roles and contingencies. As part of its project to update its 1998 report, Planning for Post-Disaster Recovery, the American Planning Association created an annotated Model Pre-event Recovery Ordinance designed to guide communities in preparing prior to a disaster so they can better manage the recovery process. This guidance includes advising communities to create a recovery management organization prior to a disaster (APA, 2014a).
As discussed earlier, the representatives for the RSFs in community recovery will need to be different from those leading the ESFs. In some cases there may be some overlap but, generally, different expertise is needed to address long-term needs versus those associated with the emergency response. As discussed
in Chapter 3, jurisdictions need to leverage existing community structures that promote an integrated approach. There is no value to building a new network of people and processes that will be used only in the aftermath of a disaster. Structures and networks already in place are familiar with their target audiences, stakeholders, and potential vendors and partners for rebuilding. After a tornado demolished much of Joplin, Missouri, in 2011, City Manager Mark Rohr attributed some of the success of the town’s recovery, including the development of the Citizens Advisory Recovery Team (CART), to activities initiated in 2001 to revitalize the downtown area. Rohr suggested that the community’s history of engagement in downtown revitalization served as a precursor to the CART’s mission to consider and outline a long-term disaster recovery strategy (Abramson and Culp, 2013). By building on a holistic vision, especially one already known and shared among stakeholders, sectors in a community can determine how they can best work together to realize that vision for their neighborhood, town, or city during recovery.
Conducting Vulnerability and Capacity Assessments
In addition to creating a vision for recovery and organizing sectors and stakeholders for recovery management, it is important for communities to conduct assessments of their vulnerable infrastructure, populations, and locations; take inventory of their assets; and understand their capacity limitations that would be stressed during the recovery process. For example, rebuilding and redevelopment will likely necessitate a massive amount of permitting so communities should assess in advance their capacity to meet this surge in need rapidly and smoothly. Capacity assessments of physical assets alone will be insufficient; the workforce needed to provide the increased services required after a disaster must also be assessed, and alternatives explored if it is inadequate. Having memorandums of understanding in place and processes for waiving regulations and collaborating across sectors prior to an event can facilitate recovery. Pinellas County, Florida, in its recent post-disaster redevelopment plan (PDRP), described its capacity assessment as follows:
The purpose of the Pinellas County Institutional Capacity Analysis is to examine the capacity of the county to facilitate redevelopment in the context of the goals and objectives of this plan. “Capacity” in the context of this plan is not focused on physical assets (i.e., number of fire trucks, ambulances, etc.). Instead, capacity is assessed to determine if the framework exists to implement the goals and actions in the PDRP, such as programs, agencies, organizations (and their associated staffs) and other tools. The assessment is intended to determine the robust programs and resources that strongly support post-disaster redevelopment, programs that exist but could be improved to better support post-disaster redevelopment goals, and the weakness or gaps where programs or plans could be implemented to improve the County’s capacity to recover in the long term. (Pinellas County, 2012, p. 4-55)
In addition to capacity, a strong understanding of a community’s vulnerabilities is needed to inform recovery planning. Although these kinds of analysis often focus on critical infrastructure, social vulnerability is increasingly being evaluated in the risk management process (see Chapter 2 for discussion on social vulnerability). The Pinellas County PDRP, for example, includes a socioeconomic profile (Pinellas County, 2012) as a component of its vulnerability assessment. Digital technologies are enabling emergency managers and health officials alike to identify areas with high social vulnerability. While geographic information systems (GIS) often are used in emergencies to map flood plains or key assets that can be deployed, they also can be used to map public health and social services data to show community and government officials where vulnerable neighborhoods may be following a disaster. In New Orleans, the health department, using data from the Centers for Medicare & Medicaid Services (CMS), created a map of residents who were oxygen dependent and would need immediate assistance in the case of lost power. The CMS data were found to be 93 percent accurate, giving the health department a clear picture to start with in the event of an emergency (DeSalvo et al., 2014). Similarly, King County, Washington, used GIS software to map socioeconomic factors in the county that are associated with health risks (see Figure 9-1). Such data are invaluable to the effective targeting of resources to areas of need after a disaster.
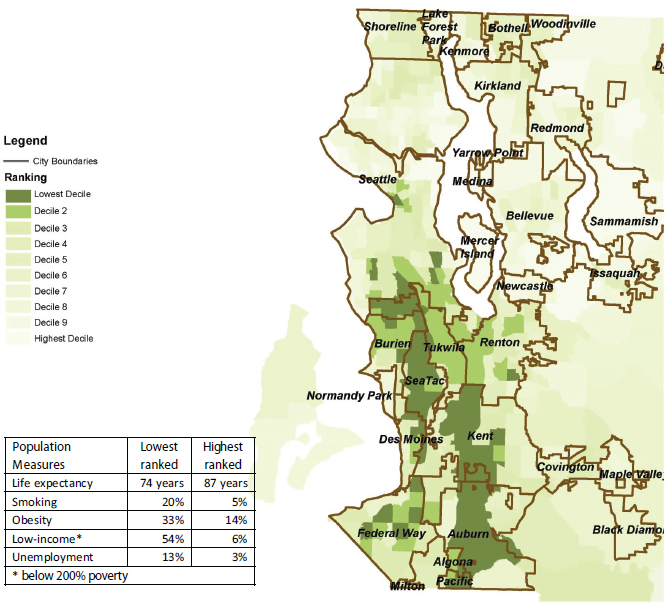
SOURCE: King County. 2014. Health and Human Services transformation plan and communities of opportunity. King County, Washington. Available at http://www.kingcounty.gov/exec/HHStransformation/coo.aspx.
EARLY POST-DISASTER RECOVERY PRIORITIES
The early recovery period often overlaps with and runs parallel to the disaster response phase. During this time, communities assess the extent of the disaster-related damage and begin restoration efforts. Although it is tempting to postpone considerations related to rebuilding in ways that support health, resilience, and sustainability, without these goals in mind, early restoration efforts may be undertaken in a manner that impedes future betterment opportunities.
Assessing Disaster Impacts on Community Systems
In the early stages of disaster recovery, it is important to conduct an impact assessment. This assessment will dictate what resources are needed, how the available funding will best be allocated, as well as
what players and stakeholders need to be engaged quickly. As mentioned previously, if a tornado destroys a neighborhood or private businesses, much of the recovery can be funded by private insurance, and a robust effort to overhaul the social fabric of a community will not be warranted. However, if public facilities are affected, infrastructure is destroyed past the point of repair, or an already declining area is heavily impacted, it will be necessary to assess the impacts quickly and facilitate the community’s transition from disaster response to disaster recovery planning—not waiting until the response ends to plan the recovery needs.
Restoring Critical Infrastructure and Remediating Immediate Health Threats
Following an impact assessment, early restoration operations needed for the short term, including those addressing infrastructure, land use, and environmental management, should be conducted. A comprehensive examination of the restoration phase of recovery is beyond the scope of this report, but the sections below highlight restoration needs related to protecting health.
Infrastructure and Transportation
In the initial phases of recovery, communities should address post-disaster challenges of transportation access in a prioritized manner. FEMA Public Assistance funds often cover emergency repair of public infrastructure and debris removal. However, debris removal can be a rate-limiting step for recovery activities and is critical to restoring access to goods and services that are essential to health. With the passage of the Sandy Recovery Improvement Act of 2013,7 FEMA developed a pilot program to incentivize rapid debris removal. Upon receiving a debris management plan prior to a declared disaster, FEMA will provide a one-time incentive of a 2 percent cost share adjustment for the first 90 days of debris removal activities, beginning the first day of the declared incident period, provided the plan is implemented for that disaster (FEMA, 2014c).
Selection of an appropriate site for dumping of debris is important to prevent potential health risks to nearby or future populations. Historically, careful site selection has not occurred, leading to issues of environmental justice (Allen, 2007). In light of the increased emphasis on green infrastructure and design discussed earlier in this chapter, a community also may want to consider a recycling program for debris, which could lessen the workload of disposal as well as contain costs. Through the FEMA pilot program, costs of sorting debris for a recycling program are eligible for reimbursement.
Reopening roads is another key recovery priority and can impact health. In setting criteria for reopening roads and restoring power, access roads to hospitals and other medical and ancillary facilities (e.g., pharmacies) should have priority. The need for alternative transit routes should be evaluated as well. If large temporary housing sites are set up in an area outside typical access routes, for example, community leaders may need to ensure that they are serviced by public transit so those temporarily displaced residents without access to personal vehicles can access essential goods and services as well as employment.
Another critical early priority is the restoration of utilities and communications systems. For example, water treatment facilities need to be up and running to prevent illness from contaminated water supplies and power is essential to health facilities and individuals requiring electricity-dependent medical equipment. Reestablishment of communication infrastructure is important for continued use of health information systems after a disaster, particularly for providers using cloud-based record storage. For those organizations that established backup measures in advance of the disaster (e.g., power generators, physical servers at nearby sites) as part of resilience-building efforts, such systems can be used until critical infrastructure is restored, thereby protecting against adverse health outcomes.
________________
7 Sandy Recovery Improvement Act of 2013, 113th Congress, H.R. 219 (January 29, 2013).
Land Use
Although there is often pressure to get a community “back to normal” after a disaster, it is important to discourage immediate rebuilding in potentially hazardous areas. A moratorium on immediate rebuilding may be the best option when there has been a great deal of destruction so that authorities and building owners can explore the advantages and disadvantages of rebuilding in the same location. Instituting a building moratorium also can prevent unscrupulous contractors who come into the affected community from taking advantage of people who have been traumatized and are willing to pay the first person who offers to help them get their home and life back. Following the Cedar Rapids, Iowa, floods in 2008, the city developed a model that required anyone doing repair or reconstruction in the city to first visit city hall and become certified as qualified and trustworthy (Schwab, 2014).
On the other hand, it is also important to examine options holistically and to consider the downstream effects a moratorium could have. Low-income housing often tends to be in vulnerable (e.g., low-lying) areas of a community. Delays in rebuilding public housing could add even more strain to parts of a community that are in great need (APA, 2014b). An extreme consequence could be increasing homelessness for residents and families who are unable to find affordable housing options. With this in mind, if a moratorium is deemed necessary while authorities examine mitigation strategies, particular attention should be given to temporary housing needs to ensure that vulnerable populations are provided for. (Temporary housing needs are explored in further detail in Chapter 10.) Many actions that should be taken at the local level are described in the American Planning Association’s model recovery ordinance described earlier in this chapter.
Environmental Management
Another early recovery priority is securing public sites contaminated with hazardous materials. It is important for municipal leadership to understand that this is a priority even if no immediate health effects are noticed. Following removal of hazardous materials, immediate environmental remediation should be executed to ensure that these materials do not pose a risk to the community in the months or years to follow.
The health promotion strategies discussed in this section are evidence-based but communities will need to determine what is appropriate to their local conditions and community vision. Communities should inventory their prior plans to identify opportunities to apply disaster-related resources to meet previously agreed-upon objectives. If those plans focus on safe access to healthy foods, for example, the recovery plan might include locating new or rebuilding retail grocery businesses or farmer’s markets in areas with demonstrated need. However, it is important to remember that the severity of the disaster may dictate what is possible with respect to strategies and desired outcomes of recovery. In cases of widespread damage, comprehensive initiatives such as mixed-use and transit-oriented development are possible, but if the impact is not as widespread and the corresponding recovery funding is more limited, smaller-scale initiatives, such as creating buffer areas around rivers, may be more practical.
In many cases, farsighted approaches focusing on long-term health, resilience, and sustainability will require an upfront investment. Incentives may be necessary to overcome aversion to added costs and complexity. In Hillsborough County, Florida, for example, the post-disaster redevelopment plan recommends the use of financial incentives for preestablished healthy community priorities such as giving permitting preference to redevelopment plans that incorporate walkable streets or green infrastructure (Hillsborough County Government, 2010).
Developing Transportation and Land Use Strategies
As discussed earlier, transportation and land use strategies can impact health status in a variety of ways, including promotion of active lifestyles; injury reduction; improved access to essential goods, services, and employment; promotion of social cohesion; and improved environmental sustainability (e.g., reduced vehicle emissions). A well-thought-out, transit-oriented design can achieve multiple health benefits for the residents of a neighborhood or town. Developing such a design prior to a disaster can create an opportunity for a community to allocate recovery funds in a balanced and comprehensive manner when rebuilding. As an example, Atlanta, Georgia—typically regarded as a commuter city with urban sprawl—is currently engaged in a project to revitalize its “Beltline” and decrease dependence on vehicles. Once completed, the Atlanta project will have developed 33 miles of multiuse trails, 1,300 acres of parks, and 5,600 units of affordable housing, linking 45 neighborhoods through enhanced transit (ULI, 2013). Even if the funds needed to execute the entire plan are not available prior to a disaster, envisioning such a plan, identifying vendors, and determining implementation methods during steady-state times can allow for quick action toward becoming more sustainable and creating healthy, livable environments following a disaster. To implement such improvements after a disaster, the cross-sector collaboration discussed throughout this report is essential.
A number of strategies can be employed to build more livable and active communities after a disaster. Historically, many cities and towns have been zoned to keep residential and commercial areas separate, but there is now increased awareness that zoning for mixed-use development creates more walkable and bikeable communities, which have been increasing in demand in recent years. Traffic-calming measures, such as speed bumps or pedestrian islands, also have been shown both to increase pedestrian and bicycle safety and to increase active travel (Winters et al., 2010). The introduction or expansion of public transportation systems has a positive effect on active travel as well (What Works for Health, 2010). More accessible transit options in a community also support the “aging in place” concept—enabling seniors to stay at home and provide for themselves.8
While improved streetscape design, zoning regulations, and mixed-use development can contribute to a much more active population, also key to success is combining physical infrastructure improvements with social programs. Walking school buses and Safe Routes to School programs, for example, are designed to give children better active options for getting to school. California’s Safe Routes to School program helped communities build and improve sidewalks, street crossings, and traffic controls, and an evaluation of the program found that as a result, more children were walking and cycling to school (Transportation Research Board, 2005). Such programs are important because simply improving infrastructure and widening sidewalks will not result in more children being active. If streets are still unsafe, or there is no chaperone to ensure a timely arrival, many parents may still choose the school bus as a better option.
Developing Community Development Strategies
Post-disaster neighborhood revitalization represents one of the largest opportunities to improve long-term health outcomes and community resilience. As discussed in Chapter 2, the social determinants of health (e.g., housing, education, poverty) are in most cases also the determinants of social vulnerability to disasters. During post-disaster redevelopment, one of the greatest opportunities to improve both community health status and social vulnerability is to leverage the recovery funds that often become available to address the needs of low-income individuals and families—most notably CDBG-DR funding, but possibly also economic development and rural development funds. A number of place-based strategies can address blight and reduce socioeconomic and health disparities through interventions that provide access
________________
8 AARP recently developed a disaster recovery toolkit that provides policy information, tools, and resources for building more livable communities after disasters, available at http://www.aarp.org/livable-communities/tool-kits-resources/info-2015/disasterrecovery-tool-kit.html (accessed April 9, 2015).
BOX 9-3
Transit-Oriented Development and Zoning and
Planning in Mission Bay, San Francisco
The Mission Bay development in San Francisco is a good example of how a station area plan was combined with tax increment financing (TIF) and a novel inclusionary housing strategy to create value for both the master developer and the broader community. In this case, the station area plan is, in fact, a redevelopment plan for an area with multiple transit providers, including CalTrain commuter rail service, electric buses, and MUNI METRO light rail, all of which co-terminate and share a common intermodal facility.
Mission Bay is a 303-acre redevelopment project along San Francisco’s waterfront, adjacent to both that transit facility and to SBC Park, which is the San Francisco Giants baseball stadium. At the start of the planning process, the area was owned almost entirely by Catellus, a real estate company spun off to shareholders in 1990 to develop property owned by Santa Fe Pacific Corporation. The project area will eventually include over 6,000 residential units, 5 million square feet of corporate offices and biotech space, a new campus for the University of California, San Francisco, a hotel and conference center, 750,000 square feet of retail, and 49 acres of parks and open space. So far, nearly 40 percent of the housing is complete or under construction, along with much of the new University of California, San Francisco, campus.
As part of the development agreement with the San Francisco Redevelopment Agency (SFRA), Catellus agreed to dedicate 14 parcels to the SFRA for the purpose of developing affordable housing. The SFRA then competitively selected developers and provided both land and TIF funds to build mixed-use affordable housing complexes throughout the development. Catellus and the SFRA created a unique land dedication and funding strategy that enabled 28 percent of the housing—which will be created in both standalone affordable housing developments and as part of larger market-rate condominium developments—to be affordable to very low-, low-, and moderate-income households. For example, Rich Sorro Commons is a 100-unit rental apartment development with a 40-child Head Start program and 10,000 square feet of ground floor retail. Around the corner, the SFRA provided land and TIF funds to Mercy Housing California to develop a 100-unit senior care community with a local library on the ground floor. These two developments are sandwiched among a half-dozen market-rate condominium developments that include a grocery store and thousands of square feet of local retail.
SOURCE: Excerpted from Shoemaker, 2006, p. 17.
to such resources as affordable housing, employment, nutritious food, and health services. Some of these strategies are discussed below.
Housing, discussed in more detail in Chapter 10, is one of the greatest and most immediate needs after a disaster and can be particularly challenging for already vulnerable populations. Communities need to take steps to prevent former low-income residents from being forced out of their neighborhoods (sometimes called disaster gentrification) and ensure that they have access to essential services, community amenities (e.g., libraries), and centers of employment. Initiatives ensuring that a certain percentage of newly constructed housing is affordable and near transit centers can prevent some of the health inequities described earlier. Low-income populations are often most in need of public transportation, but market prices may exclude these vulnerable populations, necessitating creative market interventions. Mission Bay in San Francisco, California (see Box 9-3), for example, created affordable housing and community elements such as a Head Start program and a senior care community, accessible via multiple transit routes, reducing the parking burden in the area and allowing people of all income levels to obtain goods and services safely and easily.
Although evidence on the health benefits of mixed-income housing is inconclusive (as discussed further in Chapter 10), reducing dense clusters of vulnerable populations in segregated areas of a city may have
other benefits in terms of reduced social vulnerability. Where mixed-income housing is incorporated into mixed-use developments, there may be added benefits. A report by the Urban Land Institute, Housing in America, highlights an example of an unexpected consequence of mixed-use development:
A study of the 1995 heat wave in Chicago found that residents—particularly vulnerable populations, including low-income individuals and the elderly—were at lower mortality risk during the heat wave if they lived in neighborhoods with “dense commercial activity” and “streets with more vibrant social ecologies.” This reduced risk was attributed to the fact that residents without air conditioning were more readily able to seek relief from high temperatures in local stores. A dense mix of uses and pedestrian-friendly environments enabled the neighborhood’s most vulnerable residents to seek shelter from the extreme heat. (ULI, 2014, p. 8)
Education campaigns regarding these benefits can help stem concerns among some buyers and residents about rent control and tax breaks for certain income levels when mixed-income developments are being planned.
Another disaster-related challenge associated with housing is the problem of blighted, abandoned buildings—which, according to Pat Morrissy, executive director of Housing and Neighborhood Development Services, Inc., often can be one of the most significant contributors to a neighborhood’s demise, affecting health, crime rates, fire potential, and market values (Mallach, 2006). Two years after Hurricane Katrina, the New Orleans Redevelopment Authority developed the Lot Next Door Program. This program gives the neighboring businesses or owners the opportunity to buy the “lot next door” property for fair market value (New Orleans Redevelopment Authority, 2014). Vacant lots also can be transformed into community gardens that not only reduce blight but also provide access to fresh produce. A community development council in Philadelphia, for example, realized the effect abandoned buildings and lots were having and partnered with the Pennsylvania Horticultural Society to start a vacant land management program in the late 1990s. By 2004 they had reclaimed more than 600 of the vacant lots, planting trees and reselling many of the lots to homeowners for gardens and side yards. They also developed a community garden center and worked to create .75-acre urban farm on another abandoned site, which now sells produce to top area restaurants (Mallach, 2006). Within 10 years, the program had tremendous impact, again showing the multitude of benefits thoughtful redevelopment and environmental management can have in addressing issues of the social determinants of health.
Many vulnerable neighborhoods lack access to nutritious food even before a disaster. Taking the opportunity to address this gap in a long-term recovery process can improve health, resilience, and sustainability. A global program called Urban Farming, for example, began working in Detroit, Michigan, to encourage people to start gardens, grow their own food, and incorporate healthy eating into their lifestyle. In addition to improving nutritional status and reducing reliance on unsustainable food systems, such measures also serve as a disaster risk reduction strategy by improving food security (ULI, 2013). Another example of access to healthy food is the Fresh Food Retailer Initiative in New Orleans, started in 2011 to increase the number of fresh food markets in low-income neighborhoods and communities. While the problem of inadequate access to healthy food existed prior to Hurricane Katrina, it was exacerbated by that event, and the program provided welcome assistance to the neighborhood (ULI, 2013).
The community development sector employs a variety of complementary approaches to improve access of low-income populations to community services and amenities. After a disaster, this could entail strategic placement of new schools and community health clinics near public and affordable housing developments. Changes to land use policies can be complementary to reconstruction of physical infrastructure. Joint-use agreements that enable community members to use school facilities (libraries, pools, athletic fields) during non-school hours, for example, can provide opportunities for recreation in a safe environment and reduce disparities associated with unequal access to community amenities. In addition to the physical health benefits, creating a school-centered community site that supports different kinds of extracurricular activity may also enhance social cohesion in a community, contributing to closer social connections among
neighbors and greater awareness of and engagement in community issues. As discussed throughout this report, social cohesion can have positive effects on people’s stress levels and mental health.
Redevelopment designs that address community needs holistically are difficult to fashion and complicated to implement. The obvious goal of such designs would be to reconfigure land uses such that residential developments such as assisted living facilities, independent living facilities, senior housing, and affordable housing are situated in a pattern that aligns with business services and employment centers. Most communities lack administrative and management capacity to plan and carry out such ambitious initiatives in a short time, however, and special surge resources are needed to carry them out in a compressed timeframe after a disaster. Disasters that result in widespread devastation, such as the Joplin, Missouri, tornado, may offer special opportunities to replace outmoded pre-disaster land use patterns in creative ways. The case of the C.J. Peete housing redevelopment following Hurricane Katrina exemplifies many of the concepts of approaching the recovery of a community holistically to promote a healthy and sustainable future (see Box 9-4). Coming together after a disaster with multiple parties to consider the implications of the damage and the options available for addressing it is an important part of successful recovery planning.
Developing Environmental Management Strategies
Green, or environmentally responsible, strategies generally focus on environmental sustainability and associated benefits, such as reduced energy consumption and cost, but they also have demonstrated parallel health benefits. When air quality is better, for example, asthma attacks are reduced, which leads in turn to reductions in health care costs and absenteeism from school (Kats, 2006). Typically, green infrastructure is understood as entailing such elements as rain gardens, green roofs, wetlands, and walking trails. However, the design of physical structures also can play a role in encouraging healthy behaviors and promoting healthy environments.
Indoor Environments
A study conducted by McGraw Hill Construction, commissioned by the American Institute of Architects, found that decisions about building design, construction, and operations are critical to the well-being of building occupants and demonstrated the strong role buildings can play within the surrounding communities (McGraw Hill Construction, 2014). Indoor environments with poor air quality can contribute to adverse health effects and, in turn, to more doctor visits, higher medical bills, and even cost to employers (Loftness et al., 2007). Sustainable building design depends on material selection, which can impact not just air quality but also health issues related to whether the materials selected promote mold, toxicity in fires, or cancer-causing fibers (Dainoff, 1990). Examples discussed below illustrate health impacts in schools and economic impacts in neighborhoods, but this topic is explored further with regard to housing in Chapter 10.
Outdoor Environment
The American Society of Landscape Architects (ASLA) offers examples of and strategies for green infrastructure and design that not only can mitigate future hazards in a community but also have positive economic benefits. “In the typical market, an additional 1 point increase in [a community’s] walk score was associated with between a $700 and $3,000 increase in home values” (Cortright, 2009, p. 2). The use of less impervious surfaces such as rain gardens, porous concrete, or green roofs can be more sustainable, prevent stormwater runoff and water pooling, and make a community more resilient to storms or floods.
The High Line Park in New York City is an example of the combined use of green infrastructure and community development, focused on revitalizing an abandoned railroad track running through Manhattan. A neighborhood group advocated for its preservation and reuse as public open space. Through zoning amendments and competitive green design, the park now spans over 20 blocks, with more phases to follow (ASLA, 2013). There are many layers within the “living roof” on the elevated rail line, which will help
BOX 9-4
New Orleans’ C.J. Peete Public Housing Redevelopment
Even before Hurricane Katrina flooded New Orleans, the neighborhood of Central City was suffering—the neighborhood was racially segregated and poor, and lacked the services and opportunities that might help residents escape poverty. The large public housing development, C.J. Peete, was in the process of being demolished, with only half of the original 1,403 units remaining and the previous residents having been displaced. After the storm, C.J. Peete was largely undamaged, but the city’s housing authority chose to take the storm as an opportunity to demolish it and redevelop the housing facilities.
The Annie E. Casey Foundation joined with other philanthropic and community organizations to support the redevelopment of C.J. Peete and the revitalization of the Central City neighborhood. Along with a for-profit developer and its nonprofit community development subsidiary, the foundation and its partners followed a guiding framework of “holistic community redevelopment and transformation.” This framework, rather than focusing solely on rebuilding the physical structures of the neighborhood, gave equal priority to all elements of a healthy community, including: affordable mixed-income housing, authentic resident engagement, good schools, jobs and job training, integrated services, access to transportation, and building the capacity of residents and community organizations. Flexible funding from a variety of sources allowed the project to fund some of these unconventional objectives.
Many residents had lived in C.J. Peete for generations and were deeply rooted in the community, and some opposed the plan to demolish and rebuild. The developer took the time to get residents on board and to engage them meaningfully in the process. First, the developer’s nonprofit subsidiary spent substantial time reaching out to displaced residents, stabilizing families, and providing case management and referrals to services. Residents were offered training in leadership skills, job training, and literacy and financial management classes. Second, the developer involved the residents in the planning of the new community, holding conversations about residents’ priorities, hopes, and needs, and residents weighed in on decisions that affected them. The developer and the residents signed memorandums of understanding, and when tensions arose, the developer addressed residents’ concerns. Some residents even helped build the new development—after a 13-week construction training program, 29 new jobs were filled by low-income neighborhood residents.
Six years after the hurricane, the end result of this process was Harmony Oaks, a mixed-income housing development that, along with the surrounding Central City neighborhood, includes a new elementary school; a park; a business incubator; and a community center with Head Start, a health clinic, a playground, and offices for state services. Almost 400 Harmony Oaks residents have received employment training and assistance, and the employment rate has risen 42 percent since the project began. One success story encapsulates the unique impact of Harmony Oaks: the building’s first resident, who had lived in C.J. Peete, received case management for 3 years, became certified as a nurse, found a steady job, and moved into Harmony Oaks as a market-rate renter.
SOURCE: AECF, 2013.
filter stormwater runoff and prevent pooling of water and flooding. Considerable planning for long-term sustainability was conducted as well, resulting in the use of special long-lasting concrete to reduce waste caused by later replacements and the selection of native, drought-resistant plant species capable of withstanding the specific microclimate. Additionally, plans are being made to harvest rainwater from nearby buildings to reduce environmental impact (ASLA, 2013). In addition to its function as green infrastructure, the placement and design of High Line Park also encourage elements of a healthy community described throughout this report, such as active lifestyles and positive community interaction, which can contribute to increased social cohesion. The park also has been incorporated into the local school curriculum, and a “youth corps” program was created to employ teenagers in tending the park landscape and facilitating park-related educational and community engagement efforts (ASLA, 2014).
In September 1999, flooding caused by Hurricanes Dennis and Floyd devastated the town of Kinston, North Carolina. More than three-quarters of homes in the flood plain and many businesses were damaged or completely destroyed. In its recovery strategy, the town decided to take a two-pronged approach encompassing community redevelopment and hazard mitigation strategies discussed throughout this chapter. The objectives were to reduce the impacts of future floods while revitalizing existing neighborhoods and businesses to increase self-sufficiency and promote long-term sustainability. To accomplish the first objective, they used GIS mapping to identify flood-prone areas and determine which areas were suitable for development and which should remain as buffers and open space. To protect social networks, residents from the same neighborhoods were relocated together. In addition, they developed a cooperative green infrastructure plan with the nearby University of North Carolina at Chapel Hill and a conservation nonprofit to create different types of green space, allowing for all types of recreation as well as promotion of heritage tourism (Natural Hazards Center, 2006).
Incorporating Hazard Mitigation, Resilience, and Sustainability Planning
Disaster risk reduction or hazard mitigation can increase resilience in a community and decrease the impact of future events (NRC, 2012). As climate change brings increasing numbers of disasters of increased severity, as well as sea-level rise and coastal erosion, many communities across the nation, and indeed worldwide, have been taking a closer look at their needs and vulnerabilities (NRC, 2014). Hazard mitigation is particularly critical for facilities and other infrastructure that need to remain functional after a disaster, including hospitals (see Chapter 6), emergency operations centers, public safety facilities, and utilities. Both structural and nonstructural mitigation strategies are available, each with their advantages and disadvantages (NRC, 2012). Structural options include levees; floodwalls; dams; floodways; impact-resistant construction materials; and elevation of critical elements such as rails, highways, and homes. Nonstructural options include buyouts or natural defenses such as coastal sand dunes or wetlands, similar to some of the green design elements described previously. When feasible, communities should select redevelopment areas outside of known hazards areas (e.g., flood zones9 and man-made pollution such as busy highways), and they may consider discouraging rebuilding in hazard zones by withholding public funds for reconstruction. However, telling a community it needs to move is much easier in policy than in practice, and these kinds of discussions can be highly political and contentious (benefits and challenges related to buyouts are discussed in Box 9-5). Even if moving a community appears necessary because of concerns about coastal resilience, simply relocating infrastructure may not result in successful transplantation. In many cases, communities will lean toward employing structural and nonstructural mitigation measures to build resilience before attempting to move. In the event of a presidentially declared disaster, funding for mitigation measures is available from FEMA (Hazard Mitigation Grant Program and Section 406 Stafford Act mitigation funds) and, following a supplemental appropriation, HUD’s CDBG-DR.
While there are many strategies for hazard mitigation, the national or even regional vision to undertake these important efforts often is lacking. According to a recent report of the National Research Council (2014, p. 6), “Studies have reported benefit-cost ratios between 5:1 and 8:1 for nonstructural and design strategies that reduce the consequences of flooding, but between 2004 and 2012, federal funds for such strategies were only about 5 percent of disaster relief funds.” That report notes further that “the vast majority of funding for coastal risk-related issues is provided only after a disaster occurs, through emergency supplemental appropriations” (NRC, 2014, p. 4). Thus, as with many other sources of disaster funding, these issues receive little attention and funding prior to a disaster. Even once funding is available, often only a very small percentage is allocated for mitigation and risk reduction efforts.10 However,
________________
9 FEMA has been modifying flood plain maps and 100-year flood projections and evacuation zones, which may help direct funding for mitigation strategies to certain areas and may alter eligibility for participation in the National Flood Insurance Program (FEMA, 2015a).
10 As discussed in Chapter 4, Section 406 of the Stafford Act authorizes funding to be used for mitigation measures during rebuilding as long as it will contribute to protection from subsequent events.
BOX 9-5
Managed Retreat: Benefits and Challenges Related to Buyouts
Difficult choices are ahead in the years to come as climate change threatens to result in sea-level rise, coastal erosion, and more severe storms. Although communities have started implementing a variety of structural and nonstructural adaptive strategies to harden infrastructure and increase resilience in waterside communities, it will not be possible or financially feasible for some to adequately protect public safety and property using these measures.
Hazardous events such as Hurricane Sandy have spurred greater interest in the use of buyout programs to facilitate a managed retreat from flood-prone areas. The Federal Emergency Management Agency’s (FEMA’s) Hazard Mitigation Grant Program and the Department of Housing and Urban Development’s (HUD’s) Community Development Block Grant for Disaster Recovery are two funding sources commonly used to finance buyouts, and homeowners generally are offered prestorm market value for their homes. Both programs require that the acquired properties not be redeveloped but remain as open space with such functions as recreation and/or environmental management (e.g., wetlands).
Because of the contentiousness surrounding government acquisition of private property, such buyout programs often are voluntary. For targeted areas with high risk, incentives can be used to encourage homeowners to relocate. In New York, for example, 10 percent of fair market house value was offered as an incentive for residents in targeted areas, who received an additional 5 percent if they relocated within the same county. While these kinds of incentives are valuable motivators, homeowners in some cases will resist or be unable to accept a buyout (if, for example, they owe far more on their mortgage than the prestorm market value). In such cases, governments may consider exercising eminent domain to ensure that all or most properties in a high-risk area are relocated. Despite the distinct possibility of public outcry, this may be necessary to protect the lives of residents and the responders responsible for rescue operations, to reduce expenditures of public funds associated with recovery needs, and to create more effective environmental conservation areas.
SOURCE: Bova-Hiatt et al., 2014.
FEMA’s National Mitigation Framework, created in 2013, represents a major step forward for mitigation and disaster risk reduction at the national level, and states and regions need to follow suit. The FEMA framework describes mitigation roles within a community to embed risk management within community priorities and plans (e.g., critical infrastructure, land use, capital improvement, sustainability, recovery, health improvement) (FEMA, 2015b). Seven core capabilities in the framework and an example of a critical task for each are listed below:
- “Threats and Hazard Identification. Build cooperation between private and public sectors by protecting internal interests but sharing threats and hazard identification resources and benefits.
- Risk and Disaster Resilience Assessment. Perform credible risk assessments using scientifically valid and widely used risk assessment techniques.
- Planning. Incorporate the findings from assessment of risk and disaster resilience into the planning process.
- Community Resilience. Recognize the interdependent nature of the economy, health and social services, housing infrastructure, and natural and cultural resources within a community.
- Public Information and Warning. Target messages to reach organizations representing children, individuals with disabilities or access and functional needs, diverse communities and people with limited English proficiency.
- Long-Term Vulnerability Reduction. Adopt and enforce a suitable building code to ensure resilient construction.
- Operational Coordination. Capitalize on opportunities for mitigation actions following disasters and incidents” (FEMA, 2015b).
Unfortunately, disasters themselves are one of the most powerful motivators for instituting hazard mitigation strategies. Once municipalities and states have been exposed to the debilitating effects and costs of disasters, leaders often are more likely to focus on reducing exposures for future incidents. After Hurricane Sandy in 2012, for example, Governor Cuomo convened a NYS2100 Commission to review the vulnerabilities of the state’s infrastructure systems and make recommendations for increasing the state’s resilience in five different areas: transportation, energy, land use, insurance, and infrastructure finance (NYS 2100 Commission, 2013). The commission developed several cross-cutting recommendations, as well as recommendations specific to each of the sectors, focused both on the recovery process and on mitigation of future hazards and decreased vulnerability. The nine cross-cutting recommendations, listed below, highlight the integration needed across systems:
- Protect, upgrade, and strengthen existing systems.
- Rebuild smarter: ensure replacement with better options and alternatives.
- Encourage the use of green and natural infrastructure.
- Create shared equipment and resource reserves.
- Promote integrated planning and develop criteria for integrated decision making for capital investments.
- Enhance institutional coordination.
- Improve data, mapping, visualization, and communication systems.
- Create new incentive programs to encourage resilient behaviors and reduce vulnerabilities.
- Expand education, job training, and workforce development opportunities. (NYS 2100 Commission, 2013, p. 12-13)
Hurricane Sandy also spurred the launch of Rebuild by Design, a competition funded by HUD through a supplemental congressional appropriation to challenge local and global designers to develop innovative large-scale infrastructure solutions to build resiliency in the impacted region. The case study in Box 9-6 is an example of natural hazard mitigation efforts developed in the context of this competition.
Given the physical, psychological, economic, and social consequences of disasters, recommendations for leveraging long-term recovery planning to build healthier communities need to encompass hazard mitigation and risk reduction to protect against the effects of future disasters. Hazard mitigation plans (like health improvement plans) need to be incorporated into a community’s comprehensive plan, not created in isolation. Hazard mitigation plans most commonly are developed by the emergency management sector, but those efforts should be supplemented by the multiple sectors and stakeholders mentioned throughout this chapter to ensure cross-sector involvement and streamlined goal setting. Health sector (public health, behavioral health, health care) stakeholders have a clear role in advocating for mitigation actions that will protect against future disaster-related physical and psychological trauma and can help inform mitigation decisions through health impact assessments (see Box 3-6 in Chapter 3). Further, the health sector can work with the emergency management sector to educate the broader community about the importance of reducing social vulnerability as part of a larger disaster risk reduction strategy.
Problems faced by a community often are multifaceted. As a result, complementary investments are needed to address complex challenges and achieve synergies. For example, preserving undeveloped buffer zones around rivers that present a flood hazard can mitigate future disasters but also can provide rec-
BOX 9-6
Rebuild by Design Case Study: Living with the Bay, Nassau County, New York
The damage from Hurricane Sandy was caused primarily by storm surge. Unfortunately, however, storm surge is not Long Island’s only water-related threat. Because groundwater is insufficiently recharged, for example, saltwater intrusion is contaminating the aquifer. And Long Island faces serious threats from sea-level rise, stormwater, and wastewater. The latter two threats are a major source of pollution: unfiltered stormwater runoff entering the bay by way of the region’s rivers and creeks threatens the bay’s ecology. Effluent from the Bay Park Sewage Treatment Plant—which is currently released in the bay—exacerbates nitrogen levels that cause harmful algae blooms, hypoxia, and excessive seaweed growth, and that also deteriorate salt marshes that could otherwise help protect Long Islanders from storm surge. To address these challenges, Nassau County, New York, formulated a plan for making the South Shore more resilient.
Strategies for the Ocean Shore: Sediment Flow
The drowning of the marshland will be stopped only when plates grow along with sea-level rise, and for this purpose, the plan includes a multifaceted approach to recovering the region’s sediment system. Overall, this strategy is focused on using the available amount of sediment within the active system in a smart way so that it can move around the system and strengthen it, with sediment from outside the active system being added to allow the area to grow along with the rising sea level.
Strategies for the Barrier Island: The Smart Barrier
As a result of their location and topography, Long Island’s barrier islands are vulnerable to sea-level rise and storm surge. The plan includes the addition of protective infrastructure that would also serve as a landscape amenity, ensuring access to the bay shore and providing a place where stormwater can be stored, cleaned, and replenished.
Strategies for the Marsh: The Eco-Edge
Urban development has negatively affected Nassau County’s wetlands, which play a critical role in buffering coastal communities. The plan includes the development of new marsh islands that would reduce wave action, improve the bay ecology, and provide new recreational opportunities.
Strategies for the Lowlands: Slow Streams
Flooding from coastal surges and stormwater inundation threatens the areas around southern Nassau’s north-south tributaries. The plan addresses these threats—along with other problems such as water quality and ecological recovery—through a series of interconnected interventions designed to transform rivers into green-blue corridors that would simultaneously store and filter water and provide public space and space for new urban development.
SOURCE: Rebuild by Design, 2014.
reation areas if used for trails. This is often the case with environmental management efforts and green designs. The ecology created can mitigate many hazards, improve air quality, and moderate temperature while also contributing to healthy communities by promoting active lifestyles and vibrant community centers and activities. At the same time, it is important to remember that addressing just the physical infrastructure of a community cannot bring about healthy, resilient, and sustainable communities; reduc-
ing social vulnerabilities is critical as well for both health improvement and disaster risk reduction. This essential synergy reinforces the emphasis throughout this report on collaboration across sectors and with multiple stakeholders. Table 9-1 provides a summary of strategies that can be employed in this kind of complementary approach.
TABLE 9-1 Summary of Strategies for Healthy Community Planning
| Guidance Area | Rationale | Healthy Community Planning Strategies |
| Transportation and Land Use | Community design that promotes active lifestyles, injury reduction, and social cohesion while improving access to goods and services and encouraging environmental sustainability can enhance the community’s overall health. |
|
| Community Development | Developing placed-based strategies targeting community redevelopment can provide access to such resources as affordable housing, employment, nutritious food, and health services that can reduce socioeconomic and health disparities. |
|
| Environmental Management | Community design that focuses on environmental sustainability can have a lasting impact on air, water, food, and soil quality, contributing to a healthier environment as well as making a community more resilient to disasters. |
|
| Guidance Area | Rationale | Healthy Community Planning Strategies |
| Hazard Mitigation | Disaster risk reduction or hazard mitigation can increase resilience in a community and reduce the health, social, and economic impacts of future emergencies. |
|
The committee found both domestic and international examples of communities taking advantage of the synergies of complementary approaches. Following the floods in Iowa in 2008, for example, the city of Cedar Rapids developed a recovery plan that addressed hazard mitigation, active lifestyles, and the need to reduce social vulnerability through affordable housing (see Box 9-7). And in Sendai City, Japan, measures taken to create energy self-sufficient neighborhoods contributed to both sustainability and disaster risk reduction (see Box 9-8).
In June 2008, Cedar Rapids, Iowa, experienced a record-setting flood causing an estimated $6 billion in damages that affected more than 5,000 residential properties and 20,000 residents. The flood damaged not only residential properties but also many of the city’s main public service buildings. Just months before the flood occurred, however, the city council and manager had engaged the community in an inclusive process of developing a shared vision for the city’s future. This existing engagement process, the resultant community vision, and a related effort to adopt a systems approach to government operations all enabled the community to come together quickly after the flood around a plan for what their new community would look like. The plan included such goals as encouraging active, healthy lifestyles; ensuring equitable redevelopment; building resource-efficient and resilient buildings; and protecting the city against future floods by rebuilding outside of flood-prone areas.
An immediate need for the city after the flood was to find housing for the 20,000 displaced residents. Temporary housing was offered through the help of the Federal Emergency Management Agency (FEMA), rental communities, and property managers. The city’s long-term plan was to build affordable housing for residents of all income levels. Consistent with pre-disaster plans, redevelopment was focused on making the community more compact and urban by offering an array of options, including multifamily housing rebuilt in denser neighborhoods closer to downtown. By educating the community on the benefits of higher-density neighborhoods, Cedar Rapids was able to avoid much of the “not in my backyard” attitude that can often impede equitable development initiatives. Developers received tax incentives, both state and local, for plans with a focus on mixed-use development. A request for proposals was submitted for city-owned parcels located outside the 100-year flood plain; this competitive process ensured that the city received high-quality proposals from local developers. These projects were joint ventures between the city and the developers. Development companies were encouraged to use resilient designs (e.g., raising buildings off the ground and having parking spaces on the first floor) to increase sustainability and flood resistance.
The city was able to move residents through voluntary property acquisitions—the city purchased about 1,400 properties, helping homeowners move on from the disaster, both physically and financially. Public resources for rebuilding were not given for parcels located within the 100-year flood plain to discourage redevelopment in areas at higher risk of future damage. Community development funds were awarded from the U.S. Department of Housing and Urban Development’s Community Development Block Grant program, which granted $300 million for recovery and rebuilding, with a focus on low- and middle-income households and the Home Investment Partnership fund. Low-income housing tax credits also were used to rebuild affordable multifamily units. City staff met regularly with local housing groups to determine which neighborhoods needed improvement to be considered high-functioning and equitable.
To encourage the community members to live healthy, active lifestyles, part of the recovery plan focused on providing connectivity and walkability from the planned housing developments to make the downtown core more accessible. Included in steps toward attaining this goal was the addition of a large green space area that was acquired through the city-purchased voluntary property acquisitions program. In a good example of an approach yielding multiple simultaneous benefits, a flood protection strategy created by city staff, stakeholders, and residents included a levy and floodwall system with some floodable greenway, which allowed the community to keep enjoying the accessible downtown area as well as the Cedar River.
Key to the success of Cedar Rapids’ recovery was the fact that the community already had in place initiatives aimed at increasing density in the downtown area and building housing near municipal services and employment centers. After the flood, these initiatives were accelerated and integrated into the community’s comprehensive plan, Envision CR, helping the community focus not on just the immediate disaster response but also on investing in the city’s recovery and future goals 15 to 20 years down the line.
As a result of its efforts to use the disaster recovery process to build back healthier by increasing physical activity, social connectedness, and a sense of belonging as a community, Cedar Rapids is now a Blue Zones Community and was awarded the 2014 National Civic League’s All-American City Award.
SOURCE: ULI, 2014.
BOX 9-8
Complementary Approaches to Achieving Resilience and Sustainability in
Sendai City, Japan
After the Great East Japan Earthquake and subsequent typhoon devastated a coastal area of Sendai City in Japan, Kokusai Kogyo Co., Ltd., a private civil engineering consulting firm, led an environmentally friendly property development project that also incorporated disaster risk reduction strategies (UNISDR, 2013). The firm was responsible for developing one of the city’s mass relocation areas and, conscious of the hardships the survivors (particularly those dependent on electricity for medical equipment) had experienced as a result of power loss after the disaster, included in its plan for the development a goal of energy self-sufficiency. Kokusai Kogyo was able to achieve this goal by obtaining government subsidies to offset the added costs of implementing these innovative disaster risk reduction measures; thus, public–private partnerships were essential to the success of the initiative. “The disaster resilient, low-carbon-footprint, nature-embracing Green Community Tagonishi, designed with the comfort of its residents in mind, has garnered attention as the embodiment of a new and positive direction in the reconstruction of disaster-affected areas and urban renewal” (UNISDR, 2013, p. 7).
In the process of developing its guidance and recommendations specific to place-based recovery strategies, the committee noted the need for research to address the following questions:
- How do high levels of collaboration at the local level among the community development and health and social services sectors to examine problems holistically translate to better post-disaster recovery?
- How does the built environment impact social cohesion, behavioral health, and well-being, and how can this knowledge be transformed into resilience-building strategies?
- What are the best ways to incorporate healthy community outcomes into transportation planning? Are there best practices for educating both internal and external stakeholders in this area?
- What risk-based strategies can be employed during recovery planning to reduce the physical, psychological, economic, and social consequences of future disasters?
SUMMARY OF FINDINGS AND RECOMMENDATIONS
This chapter has presented a number of strategies that integrate public health and social services goals with other community systems involved in place-based redevelopment. Each of these strategies builds on a prior investment in planning. For decades, metropolitan and rural areas—supported by the programs of the agencies now comprising the Partnership for Sustainable Communities—have been implementing community redevelopment plans of all kinds, many of them comprehensive in nature, which can serve as the foundation for an integrated approach to disaster planning and recovery. While major disasters can facilitate widespread redevelopment and improvements, even more isolated instances of flooding or storm surge, for example, can present opportunities to formulate and execute a vision of recovery, particularly one focused on reducing concentrations of poverty and improving other social determinants of health.
In most cases, communities dealing with disaster recovery fail to recognize the opportunities for advancing such a vision. Two federal departments, HUD and HHS, place great emphasis on this transformative aspect of community investments, and their respective socioeconomic programs have broad untapped potential to bolster disaster recovery in most communities. Proportionately, only a small fraction of the nation’s local governments are affected by disasters, but nearly all of them are and indeed have for decades engaged in HUD- and HHS-funded programs that target similar objectives. Unfortunately, those initiatives (at federal, state and local levels) have not been adequately integrated into the disaster recovery planning process.
Disasters often necessitate significant efforts to restore the physical infrastructure of a community, including repair of roads and bridges, reconstruction of housing and other buildings, repair of public works, and restoration of natural resources. Rather than rebuilding to a prior state, the recovery process offers a unique opportunity to mitigate against future hazards and create environments intentionally designed to support health. Such strategies focus on healthier housing and community features that enhance active lifestyles and improve equitable access to critical goods (e.g., healthy food), community services (e.g., medical care), and amenities (e.g., libraries, schools). A well-planned recovery also attends to the economic vitality of the affected area, fostering commercial revitalization, industrial and business development, and greater employment opportunities, thereby improving financial prospects for both residents and businesses. To ensure that these opportunities are not missed, planning and design, housing, community development, and environmental and public health professionals should be engaged in the development of pre- and post-disaster recovery strategies, which should be linked to community plans for improving health and social well-being developed in advance of a disaster. Communities that have such plans in hand when a disaster strikes are better equipped to undertake recovery more quickly with the long-term objectives of health, resilience, and sustainability. Given that the pool of resources for recovery is limited, creative uses of funds that simultaneously meet multiple objectives can improve the efficiency of recovery and leverage
opportunities to integrate health considerations. Such opportunities deserve special attention in disaster recovery plans.
Recommendation 10: Design for Healthy Post-Disaster Communities.
State and federal agencies (the Federal Emergency Management Agency, the U.S. Department of Transportation, the U.S. Department of Housing and Urban Development, the U.S. Environmental Protection Agency, the U.S. Department of Health and Human Services, and others), acting alone or as components of the federal Partnership for Sustainable Communities, should ensure through funding requirements that the use of federal community development and disaster recovery and preparedness funds optimizes the built environment in support of healthy communities by creating places that protect against health threats, promote good health, and address unmet social needs.
Local and state planning entities should develop a team-based approach to integrated recovery planning aligned with the policies and processes of the Partnership for Sustainable Communities so as to maximize efficiency in the use of federal resources to enhance smart growth, equity, hazard mitigation, resilience, sustainability, and other elements necessary to the creation of healthy communities. Priority areas for funding should specifically address the following essential health-enhancing requirements that are pertinent to the community’s needs as laid out in pre- and post-disaster health improvement and comprehensive plans:
- physical activity-enhancing infrastructure that includes trails, bike paths, sidewalks, and parks and recreational spaces, as well as walkable, mixed-use neighborhood designs; and
- comprehensive transportation infrastructure and land use policies that ensure the accessibility of healthy food retail outlets, employment, health and social services, schools, and community amenities such as libraries and community centers for all residents.
Optimal health, social well-being, and safety are dependent on avoiding or reducing the impacts of disasters by using best practices of hazard mitigation, including both structural and nonstructural (e.g., zoning and land use) standards and strategies. Forward-looking strategic plans, improved infrastructure, and stronger construction codes need to be used in combination to address identified community vulnerabilities, thereby reversing the nation’s trend toward higher disaster losses and the attendant human misery and social and economic costs, as well as preparing the nation for the potential effects of climate change.
Recommendation 11: Mitigate Against Future Health Hazards.
Building on the National Mitigation Framework, federal agencies, led by the Federal Emergency Management Agency, should immediately intensify their efforts, undertaken collectively and supported by aligned funding eligibility requirements, to ensure that all critical infrastructure and facilities—such as hospitals (public and private), nursing homes, fire stations, and public utilities—constructed after a disaster are designed and built with a level of protection that better ensures post-disaster safety and functionality essential to protecting health and recovering more quickly. When feasible, they should be located outside of known hazard zones. Additionally, requirements should ensure that existing critical infrastructure and facilities restored with federal recovery funds are upgraded to the new standards.
PLACE-BASED RECOVERY STRATEGIES CHECKLIST
The committee has identified two pre-event and six post-disaster critical recovery priorities for the planning, community development, environmental management, and transportation sectors that are
inextricably linked to strengthening the health, resilience, and sustainability of a community. Action steps for each of these priorities are provided in the following checklist. Although leaders of these sectors will need to adapt these actions to the local context, this guidance provides an indicative set of concerns to be considered during recovery, and also identifies potentially new and different stakeholders that should be included as partners. The checklist illustrates how the following five key recovery strategies, identified as recurring themes at the beginning of this chapter, apply to individual priority areas:
- Reduce health disparities and improve access to essential goods, services, and opportunities.
- Preserve and promote social connectedness.
- Use a systems approach to community redevelopment that acknowledges the connection among social, cultural, economic, and physical environments.
- Seek holistic solutions to socioeconomic disparities and their perverse effects on population health through place-based interventions.
- Rebuild for resilience and sustainability.
- Capitalize on existing planning networks to strengthen recovery planning, including attention to public health, medical, and social services, especially for vulnerable populations.
Pre-Event
Priority: Organize for Future Disaster Recovery Planning
Primary Actors1: Elected Officials and Community Leaders, Emergency Management Agencies
Key Partners: Urban and Regional Planning Agencies, State/Local Health Departments,2 Community Development Organizations, Social Services Agencies, Housing Agencies, Community- and Faith-Based Organizations
Key Recovery Strategy:
- Capitalize on existing planning networks to strengthen recovery planning, including attention to public health, medical, and social services, especially for vulnerable populations.
Activities include but are not limited to:
![]() Hold community planning and visioning workshops (charrettes).
Hold community planning and visioning workshops (charrettes).
![]() Consider adopting a model recovery ordinance to help organize for short- and long-term recovery.
Consider adopting a model recovery ordinance to help organize for short- and long-term recovery.
![]() Identify agencies and/or individuals as designated leads for Recovery Support Functions (RSFs) following a disaster.
Identify agencies and/or individuals as designated leads for Recovery Support Functions (RSFs) following a disaster.
- – Consider contingencies for when specific groups should or should not be included based on the type and severity of a disaster and recovery needs.
![]() Create a plan for debris management for Federal Emergency Management Agency (FEMA) incentive eligibility.
Create a plan for debris management for Federal Emergency Management Agency (FEMA) incentive eligibility.
- – Identify vendors for selection when needed following a disaster.
--------------------------
Priority: Conduct Vulnerability and Capacity Assessments
Primary Actors: Elected Officials and Community Leaders, Emergency Management Agencies, Urban and Regional Planning Agencies
Key Partners: State/Local Health Departments, Chamber of Commerce, Private Sector, Community- and Faith-Based Organizations
Key Recovery Strategies:
- Capitalize on existing planning networks to strengthen recovery planning, including attention to public health, medical, and social services, especially for vulnerable populations.
- Rebuild for resilience and sustainability.
Activities include but are not limited to:
![]() Review comprehensive emergency management plans, community health assessments, and other information sources on community vulnerability and risk.
Review comprehensive emergency management plans, community health assessments, and other information sources on community vulnerability and risk.
________________
1 See Appendix F for further description of terms used to describe Primary Actors and Key Partners in this checklist.
2 Throughout this checklist, “State/Local” is used for the purposes of brevity but should be inferred to include tribal and territorial as well.
Pre-Event
![]() Use risk assessment tools to simulate damage and measure the effects of different disaster events.
Use risk assessment tools to simulate damage and measure the effects of different disaster events.
![]() If available, use geographic information systems (GIS) to map the socioeconomic profile of communities.
If available, use geographic information systems (GIS) to map the socioeconomic profile of communities.
- – Analyze results and prioritize specific needs of different locations during the recovery phase.
![]() Assess planning and regulatory capacity, the status of programs, and potential impacts on post-disaster redevelopment.
Assess planning and regulatory capacity, the status of programs, and potential impacts on post-disaster redevelopment.
- – Examine for gaps or weaknesses.
![]() Assess political will for long-term recovery and redevelopment.
Assess political will for long-term recovery and redevelopment.
![]() Assess fiscal capacity for projects.
Assess fiscal capacity for projects.
- – Determine which redevelopment projects already have seed funding and which require new money for completion.
Short-Term Recovery
Priority: Assess Disaster Impacts on Community Systems
Primary Actor: Emergency Management Agencies
Key Partners: Environmental Health Agencies, Community Development Organizations, Public Works and Utilities, Housing Agencies, Social Services Agencies
Key Recovery Strategy:
- Use a systems approach to community redevelopment that acknowledges the connection among social, cultural, economic, and physical environments.
Activities include but are not limited to:
![]() Assess the extent of damage to public facilities, roads, and hospitals.
Assess the extent of damage to public facilities, roads, and hospitals.
![]() Project the types of expanded capacity needed to facilitate rapid recovery.
Project the types of expanded capacity needed to facilitate rapid recovery.
- – Determine needs for previously arranged memorandums of understanding.
- – Determine needs for waiving regulations to speed recovery.
![]() Consider the need for a moratorium on immediate rebuilding.
Consider the need for a moratorium on immediate rebuilding.
--------------------------
Priority: Restore Critical Infrastructure and Remediate Immediate Health Threats
Primary Actors: Emergency Management Agencies, Urban and Regional Planning Agencies, Public Works and Utilities
Key Partners: Environmental Health Agencies, Federal Agencies (including the Environmental Protection Agency and the U.S. Army Corps of Engineers), Private Sector (including Environmental Remediation and Debris Removal Vendors)
Key Recovery Strategy:
- Rebuild for resilience and sustainability.
Activities include but are not limited to:
![]() Implement the debris management plan (if created prior to the event).
Implement the debris management plan (if created prior to the event).
- – Perform site selection to ensure environmental justice when dumping.
![]() Examine changes to FEMA 100-year flood maps to confirm that rebuilding locations are appropriate.
Examine changes to FEMA 100-year flood maps to confirm that rebuilding locations are appropriate.
![]() Prioritize reopening of roads required for access to medical facilities.
Prioritize reopening of roads required for access to medical facilities.
![]() Ensure that public transportation is available to residents of temporary mass relocations sites.
Ensure that public transportation is available to residents of temporary mass relocations sites.
![]() Restore critical infrastructure including water treatment facilities, power, and communication infrastructure.
Restore critical infrastructure including water treatment facilities, power, and communication infrastructure.
![]() Remediate indoor and outdoor environments contaminated with toxic pollutants.
Remediate indoor and outdoor environments contaminated with toxic pollutants.
Intermediate- to Long-Term Recovery
Priority: Develop Transportation and Land Use Strategies to Improve Health
Primary Actors: Urban and Regional Planning Agencies, Transportation Agencies
Key Partners: State/Local Health Departments, Education System
Key Recovery Strategies:
- Reduce health disparities and improve access to essential goods, services, and opportunities.
- Preserve and promote social connectedness.
- Use a systems approach to community redevelopment that acknowledges the connection among social, cultural, economic, and physical environments.
- Seek holistic solutions to socioeconomic disparities and their perverse effects on population health through place-based interventions.
- Rebuild for resilience and sustainability.
- Capitalize on existing planning networks to strengthen recovery planning, including attention to public health, medical, and social services, especially for vulnerable populations.
Activities include but are not limited to:
![]() Inventory prior plans for transit-oriented development to promote active living.
Inventory prior plans for transit-oriented development to promote active living.
![]() Review 1-year, 5-year, and long-term transportation and land use plans in the disaster context.
Review 1-year, 5-year, and long-term transportation and land use plans in the disaster context.
![]() Develop schedules for the implementation of transportation recovery actions that align with all other recovery plan elements.
Develop schedules for the implementation of transportation recovery actions that align with all other recovery plan elements.
![]() Identify opportunities to stimulate recovery and overcome access disparities.
Identify opportunities to stimulate recovery and overcome access disparities.
![]() Review existing bus and rail lines between vulnerable neighborhoods and common commercial and retail centers.
Review existing bus and rail lines between vulnerable neighborhoods and common commercial and retail centers.
![]() Target disadvantaged neighborhoods where access upgrades will stimulate investments.
Target disadvantaged neighborhoods where access upgrades will stimulate investments.
![]() Explore alternative pedestrian and cycling strategies for both recreation and commuting purposes.
Explore alternative pedestrian and cycling strategies for both recreation and commuting purposes.
![]() Promote trail investments through discretionary programs such as the U.S. Department of Transportation’s (DOT) Transportation Investment Generating Economic Recovery (TIGER) program.
Promote trail investments through discretionary programs such as the U.S. Department of Transportation’s (DOT) Transportation Investment Generating Economic Recovery (TIGER) program.
![]() Review and upgrade development standards and zoning and subdivision regulations for resiliency.
Review and upgrade development standards and zoning and subdivision regulations for resiliency.
--------------------------
Priority: Develop Community Development Strategies to Reduce Health and Socioeconomic Disparities
Primary Actors: Community Development Organizations, Housing Agencies, Social Services Agencies
Key Partners: Urban and Regional Planning Agencies, State/Local Health Departments, Federal Agencies (including HUD), Private Sector (including Architects, Designers, and Developers), Community- and Faith-Based Organizations
Intermediate- to Long-Term Recovery
Key Recovery Strategies:
- Reduce health disparities and improve access to essential goods, services, and opportunities.
- Preserve and promote social connectedness.
- Use a systems approach to community redevelopment that acknowledges the connection among social, cultural, economic, and physical environments.
- Seek holistic solutions to socioeconomic disparities and their perverse effects on population health through place-based interventions.
- Rebuild for resilience and sustainability.
- Capitalize on existing planning networks to strengthen recovery planning, including attention to public health, medical, and social services, especially for vulnerable populations.
Activities include but are not limited to:
![]() Assess and categorize existing and proposed revitalization programs for commercial areas.
Assess and categorize existing and proposed revitalization programs for commercial areas.
![]() Review priorities for vulnerable neighborhoods, blight, social indicators, and unmet needs.
Review priorities for vulnerable neighborhoods, blight, social indicators, and unmet needs.
![]() Promote community use of schools and facilities after school hours.
Promote community use of schools and facilities after school hours.
![]() Ensure that affordable housing is maintained in areas where established communities exist and social networks are preserved.
Ensure that affordable housing is maintained in areas where established communities exist and social networks are preserved.
![]() Consider pilot projects or partnerships to provide better access to nutritious food for underserved areas.
Consider pilot projects or partnerships to provide better access to nutritious food for underserved areas.
![]() Examine the potential for integrating health care providers into community areas to provide better access.
Examine the potential for integrating health care providers into community areas to provide better access.
![]() Evaluate potential partnerships between federally qualified health centers and community development organizations.
Evaluate potential partnerships between federally qualified health centers and community development organizations.
![]() Evaluate and build upon collaborations with community- and faith-based organizations.
Evaluate and build upon collaborations with community- and faith-based organizations.
![]() Explore partnerships to encourage community gardens, educational opportunities, and employment.
Explore partnerships to encourage community gardens, educational opportunities, and employment.
![]() Encourage the creative use of architecture, engineering, and landscape architecture in recovery plans to serve multiple purposes.
Encourage the creative use of architecture, engineering, and landscape architecture in recovery plans to serve multiple purposes.
![]() Educate the community on the benefits of mixed-income housing, and explore options and incentives for affordable housing in new residential buildings.
Educate the community on the benefits of mixed-income housing, and explore options and incentives for affordable housing in new residential buildings.
![]() Explore opportunities for open green space and trees.
Explore opportunities for open green space and trees.
Priority: Develop Environmental Management Strategies to Improve Environmental Quality and Sustainability
Primary Actors: Urban and Regional Planning Agencies, Public Works and Utilities, Environmental Health Agencies
Key Partners: Private Sector (including Landscape Architects), Community- and Faith-Based Organizations, Community Development Organizations
Intermediate- to Long-Term Recovery
Key Recovery Strategies:
- Rebuild for resilience and sustainability.
- Use a systems approach to community redevelopment that acknowledges the connection among social, cultural, economic, and physical environments.
Activities include but are not limited to:
![]() Consider using green infrastructure to improve sustainability and health.
Consider using green infrastructure to improve sustainability and health.
![]() Determine plant species and supplies that can be sourced locally and are suitable for the climate.
Determine plant species and supplies that can be sourced locally and are suitable for the climate.
![]() Integrate stormwater management planning into the recovery plan.
Integrate stormwater management planning into the recovery plan.
![]() Incorporate flood plain studies, mitigation plans, and buyout opportunities.
Incorporate flood plain studies, mitigation plans, and buyout opportunities.
![]() Evaluate watershed area planning.
Evaluate watershed area planning.
![]() Review and incorporate regulatory standards, ordinances, and subdivision designs.
Review and incorporate regulatory standards, ordinances, and subdivision designs.
--------------------------
Priority: Incorporate Hazard Mitigation, Resilience, and Sustainability Planning into a Recovery Strategy
Primary Actors: Urban and Regional Planning Agencies, Emergency Management Agencies, Environmental Health Agencies, Coastal and Hazard Agencies
Key Partners: Conservation Groups and Agencies, Water Resource Agencies, Federal Agencies (including FEMA and the U.S. Department of Agriculture), Education System
Key Recovery Strategy:
- Rebuild for resilience and sustainability.
Activities include but are not limited to:
![]() Assess long-term damage and areas of future vulnerability.
Assess long-term damage and areas of future vulnerability.
![]() Merge hazard mitigation into comprehensive planning, together with strategies for resilience and sustainability.
Merge hazard mitigation into comprehensive planning, together with strategies for resilience and sustainability.
![]() Consider such options as stormwater utility fees to augment funding for recovery efforts and future mitigation practices.
Consider such options as stormwater utility fees to augment funding for recovery efforts and future mitigation practices.
![]() Review and upgrade development standards, zoning, and subdivision regulations to support innovative site designs and resilient infrastructure.
Review and upgrade development standards, zoning, and subdivision regulations to support innovative site designs and resilient infrastructure.
![]() Consider structural and nonstructural options for hazard mitigation and the cost-benefit ratio of potential efforts, including
Consider structural and nonstructural options for hazard mitigation and the cost-benefit ratio of potential efforts, including
![]() brownfield redevelopment;
brownfield redevelopment;
![]() riparian buffers, retention basins; and
riparian buffers, retention basins; and
![]() green infrastructure.
green infrastructure.
![]() Ensure compliance with Planning Advisory Service 560 recommendations on integration with the comprehensive plan.
Ensure compliance with Planning Advisory Service 560 recommendations on integration with the comprehensive plan.
![]() Set priorities for reducing risk, reducing damages, and planning for recovery.
Set priorities for reducing risk, reducing damages, and planning for recovery.
![]() Maximize use of the Hazard Mitigation Grant Program (HMGP) to fund crucial investments/ buyouts.
Maximize use of the Hazard Mitigation Grant Program (HMGP) to fund crucial investments/ buyouts.
![]() Maximize use of Stafford Act Section 406 Mitigation during recovery and redevelopment.
Maximize use of Stafford Act Section 406 Mitigation during recovery and redevelopment.
Abramson, D. M., and D. Culp. 2013. At the crossroads of long-term recovery: Joplin, Missouri six months after the May 22, 2011 tornado. http://academiccommons.columbia.edu/catalog/ac%3A166312 (accessed December 3, 2014).
AECF (Annie E. Casey Foundation). 2013. Investing in New Orleans: Lessons for philanthropy in public housing redevelopment. Baltimore, MD: AECF.
AIA (American Institute of Architects). 2014. AIA establishes new design and health agenda. http://www.aia.org/practicing/AIAB103676 (accessed December 3, 2014).
Allen, B. L. 2007. Environmental justice and expert knowledge in the wake of a disaster. Social Studies of Science 37(1):103-110.
APA (American Planning Association). 2014a. Model pre-event recovery ordinance. https://www.planning.org/research/postdisaster/pdf/modelrecoveryordinance.pdf (accessed December 3, 2014).
APA. 2014b. Post-disaster recovery briefing papers. https://www.planning.org/research/postdisaster/briefingpapers (accessed February 22, 2014).
ASLA (American Society of Landscape Architects). 2010. Leveraging the landscape to manage water. http://www.asla.org/sustainablelandscapes/Vid_Watermanagement.html (accessed December 3, 2014).
ASLA. 2013. High Line Park. http://www.asla.org/sustainablelandscapes/highline.html (accessed March 25, 2015).
ASLA. 2014. High Line Park: New York City, New York, U.S.A. http://www.asla.org/sustainablelandscapes/pdfs/High_Line_Fact_Sheet.pdf (accessed December 3, 2014).
Belsky, E. S., and J. Fauth. 2012. Crossing over to an improved era of community development. In Investing in what works for America’s communities: Essays on people, place and purpose, edited by N. O. Andrews and D. J. Erickson. San Francisco, CA: Federal Reserve Bank of San Francisco and Low Income Investment Fund. Pp. 72-103.
Bingler, S. 2011. Building the community nexus: A community centered approach to planning and design. Educational Facility Planner 45(3):35-37.
Bingler. 2014. Nexus case studies: Design, engagement and planning. Portland, OR: Concordia.
Boehmer, T. K., S. L. Foster, J. R. Henry, E. L. Woghiren-Akinnifesi, and F. Y. Yip. 2013. Residential proximity to major highways—United States, 2010. Morbidity and Mortality Weekly Report Supplements 62(03):46-50.
Boston Public Health Commission. 2010. Take Action. http://www.bphc.org/wyhc/Pages/TakeAction.aspx (accessed December 3, 2014).
Bova-Hiatt, L., M. Millea, and J. Redente. 2014. Rising waters and storm resiliency. Paper presented at The Land Use Law Center’s 13th Annual Land Use and Sustainable Development Conference: Transitioning Communities, New York.
CDC (Centers for Disease Control and Prevention). 2009. Respiratory health & air pollution. http://www.cdc.gov/healthyplaces/healthtopics/airpollution.htm (accessed December 3, 2014).
CDC. 2011. Physical activity and health. http://www.cdc.gov/physicalactivity/everyone/health/index.html#LiveLonger (accessed December 3, 2014).
CDC. 2013a. Adolescents and school health: Health disparities. http://www.cdc.gov/healthyyouth/disparities (accessed December 3, 2014).
CDC. 2013b. CDC’s built environment and health initiative. http://www.cdc.gov/nceh/information/built_environment.htm (accessed March 30, 2015).
CDC. 2013c. CDC health disparities and inequalities report—United States, 2013. Morbidity and Mortality Weekly Report Supplements 62(3):1-187.
CDC. 2014a. Facts about physical activity. http://www.cdc.gov/physicalactivity/data/facts.html (accessed December 3, 2014).
CDC. 2014b. Investing in healthier communities. http://www.cdc.gov/nccdphp/dch/programs/communitytransformation (accessed December 3, 2014).
CDC. 2014c. National diabetes statistics report, 2014. http://www.cdc.gov/diabetes/pubs/statsreport14/nationaldiabetes-report-web.pdf (accessed December 3, 2014).
Cortright, J. 2009. Walking the walk: How walkability raises home values in U.S. cities. Cleveland, OH: CEOs for Cities.
CRS. 2014. Congressional primer on responding to major disasters and emergencies. Washington, DC: CRS, Library of Congress.
Dainoff, M. J. 1990. Ergonomic improvements in VDT workstations: Health and performance effects. In Promoting health and productivity in the computerized office: Models of successful ergonomic interventions, edited by S. L. Sauter, M. J. Dainoff, and M. J. Smith. London: Taylor & Francis. Pp. 49-67.
DeSalvo, K., N. Lurie, K. Finne, C. Worrall, A. Bogdanov, A. Dinkler, S. Babcock, and J. Kelman. 2014. Using Medicare data to identify individuals who are electricity dependent to improve disaster preparedness and response. American Journal of Public Health 104(7):1160-1164.
DOT (U.S. Department of Transportation), EPA (U.S. Environmental Protection Agency), and HUD (U.S. Department of Housing and Urban Development). 2014. Partnership for sustainable communities: Five years of learning from communities and coordinating federal investments. Washington, DC: DOT, EPA, and HUD.
DOT. 2015. About TIGER grants. http://www.dot.gov/tiger/about (accessed March 25, 2015).
EDA (U.S. Economic Development Administration). 2015. Disaster Recovery. http://www.eda.gov/about/disasterrecovery.htm (accessed April 9, 2015).
Elmendorf, B. 2008. Managing natural resources: A guide for municipal commissions. State College: Pennsylvania State University.
EPA. 2009. Smart growth guidelines for sustainable design and development. http://www.epa.gov/smartgrowth/sg_guidelines.htm (accessed December 3, 2014).
EPA. 2013. Creating equitable, healthy, and sustainable communities: Strategies for advancing smart growth, environmental justice, and equitable development. Washington, DC: EPA.
EPA. 2014. Building blocks for sustainable communities. http://www.epa.gov/smartgrowth/buildingblocks.htm (accessed December 3, 2014).
Erickson, D., and N. Andrews. 2011. Partnerships among community development, public health, and health care could improve the well-being of low-income people. Health Affairs (Millwood) 30(11):2056-2063.
FEMA (Federal Emergency Management Agency). 2014a. The importance of building codes in earthquake-prone communities fact sheet. http://www.fema.gov/media-library-data/1410554614185-e0da148255b25cd17a5510a80b0d9f48/Building%20Code%20Fact%20Sheet%20Revised%20August%202014.pdf (accessed December 3, 2014).
FEMA. 2014b. National disaster recovery framework: Overview. https://www.fema.gov/national-disaster-recovery-framework-overview (accessed December 3, 2014).
FEMA. 2014c. Public assistance alternative procedures pilot program guide for debris removal (Version 2). Washington, DC: FEMA.
FEMA. 2015a. Coastal frequently asked questions. https://www.fema.gov/coastal-frequently-asked-questions (accessed April 9, 2015).
FEMA. 2015b. National mitigation framework. https://www.fema.gov/national-mitigation-framework (accessed April 9, 2015).
FHWA (Federal Highway Administration). 2005. Safety effects of marked versus unmarked crosswalks at uncontrolled locations: Final report and recommended guidelines. McLean, VA: DOT.
FHWA. 2015. Health in Transportation Working Group. http://www.fhwa.dot.gov/planning/health_in_transportation/workgroup/ (accessed April 9, 2015).
Francis, S. E. 2010. Gray to green: Jumpstarting private investment in green stormwater infrastructure. http://www.sbnphiladelphia.org/images/uploads/EIP_GrayToGreen_final_lowres.pdf (accessed December 3, 2014).
Friedman, M. S., K. E. Powell, L. Hutwagner, L. M. Graham, and W. G. Teague. 2001. Impact of changes in transportation and commuting behaviors during the 1996 summer olympic games in Atlanta on air quality and childhood asthma. Journal of the American Medical Association 285(7):897-905.
Gaffield, S. J., R. L. Goo, L. A. Richards, and R. J. Jackson. 2003. Public health effects of inadequately managed stormwater runoff. American Journal of Public Health 93(9):1527-1533.
Gordon-Larsen, P., M. C. Nelson, P. Page, and B. M. Popkin. 2006. Inequality in the built environment underlies key health disparities in physical activity and obesity. Pediatrics 117(2):417-424.
Grimm, K. A., L. V. Moore, and K. S. Scanlon. 2013. Access to healthier food retailers—United States, 2011. Morbidity and Mortality Weekly Report Supplements 62(03):20-26.
Hillsborough County Government. 2010. Post-disaster redevelopment plan. http://www.hillsboroughcounty.org/index.aspx?nid=1795 (accessed November 3, 2014).
Hoxie, N. J., J. P. Davis, J. M. Vergeront, R. D. Nashold, and K. A. Blair. 1997. Cryptosporidiosis-associated mortality following a massive waterborne outbreak in Milwaukee, Wisconsin. American Journal of Public Health 87(12):2032-2035.
HUD. 2012. U.S. Department of Housing and Urban Development: Leveraging LEED-ND as a sustainability tool. http://www.usgbc.org/Docs/Archive/General/Docs10503.pdf (accessed December 3, 2014).
HUD. 2014. Community Development Block Grant Disaster Recovery program. https://www.hudexchange.info/cdbg-dr (accessed December 3, 2014).
HUD. 2015. Questions and answers about HUD. http://portal.hud.gov/hudportal/HUD?src=/about/qaintro (accessed April 9, 2015).
Hurricane Sandy Rebuilding Task Force. 2013. Hurricane strategy rebuilding strategy: Stronger communities, a resilient region. Washington, DC: HUD.
IOM (Institute of Medicine). 2014a. Applying a health lens to decision making in non-health sectors: Workshop summary. Washington, DC: The National Academies Press.
IOM. 2014b. Financing population health improvement: Workshop summary. Washington, DC: The National Academies Press.
Kats, G. 2006. Greening America’s schools: Costs and benefits. http://www.usgbc.org/Docs/Archive/General/Docs2908.pdf (accessed March 30, 2015).
Kaufman, M. M., and M. Wurtz. 1997. Hydraulic and economic benefits of downspout diversion. JAWRA Journal of the American Water Resources Association 33(2):491-497.
King County. 2011. Planning for healthy communities. King County, WA: King County Board of Health.
Kirkland, G. 2012. U.S. Department of Housing and Urban Development Office of Inspector General Audit Report: The State of Texas did not follow requirements for its infrastructure and revitalization contracts funded with CDBG disaster recovery program funds. https://www.hudoig.gov/sites/default/files/documents/audit-reports//2012-fw-1005.pdf (accessed April 12, 2015).
Kwarteng, J. L., A. J. Schulz, G. B. Mentz, S. N. Zenk, and A. A. Opperman. 2013. Associations between observed neighborhood characteristics and physical activity: Findings from a multiethnic urban community. Journal of Public Health 36(3):358-367.
LaVeist, T., K. Pollack, R. Thorpe, R. Fesahazion, and D. Gaskin. 2011. Place, not race: Disparities dissipate in Southwest Baltimore when blacks and whites live under similar conditions. Health Affairs 30(10):1880-1887.
Lee, K. K. 2012. Developing and implementing the active design guidelines in New York City. Health Place 18(1):5-7.
Lee, M., and V. Rubin. 2007. The impact of the built environment on community health: The state of current practice and next steps for a growing movement. Los Angeles, CA: The California Endowment.
Loftness, V., B. Hakkinen, O. Adan, and A. Nevalainen. 2007. Elements that contribute to healthy building design. Environmental Health Perspectives 115(6):965-970.
Maas, J., R. A. Verheij, P. P. Groenewegen, S. de Vries, and P. Spreeuwenberg. 2006. Green space, urbanity, and health: How strong is the relation? Journal of Epidemiology and Community Health 60(7):587-592.
Mac Kenzie, W. R., N. J. Hoxie, M. E. Proctor, M. S. Gradus, K. A. Blair, D. E. Peterson, J. J. Kazmierczak, D. G. Addiss, K. R. Fox, J. B. Rose, and J. P. Davis. 1994. A massive outbreak in Milwaukee of cryptosporidium infection transmitted through the public water supply. New England Journal of Medicine 331(3):161-167.
Mallach, A. 2006. From eyesores to assets: CDC abandoned property strategies. Shelterforce Online (146). http://www.nhi.org/online/issues/146/researchupdate.html (accessed December 3, 2014).
Marks, J. S. 2009. Why your zip code may be more important to your health than your genetic code. The Huffington Post. http://www.huffingtonpost.com/james-s-marks/why-your-zip-code-may-be_b_190650.html? (accessed April 8, 2015).
Mattessich, P. W., and E. J. Rausch. 2013. Collaboration to build healthier communities: A report for the Robert Wood Johnson Foundation Commission to Build a Healthier America. http://www.rwjf.org/content/dam/farm/reports/surveys_and_polls/2013/rwjf406479 (accessed November 18, 2014).
McGraw Hill Construction. 2014. The drive toward healthier buildings: The market drivers and impact of building design on occupant health, well-being and productivity. Washington, DC: Dodge Data & Analytics.
McPherson, E. G. 1994. Cooling urban heat islands with sustainable landscapes. In The ecological city: Preserving and restoring urban biodiversity, edited by R. H. Platt, R. A. Rowntree, and P. C. Muick. Boston, MA: University of Massachusetts Press. Pp. 161-171.
Mueller. 2014. About us. http://www.muelleraustinonline.com/about.php (accessed December 3, 2014).
Murphy, S. L., J. Xu, and K. D. Kochanek. 2013. Deaths: Final data for 2010. National Vital Statistics Reports 61(4):1-118.
Natural Hazards Center. 2006. Holistic disaster recovery: Ideas for building local sustainability after a natural disaster. Fairfax, VA: Public Entity Risk Institute.
New Orleans Redevelopment Authority. 2014. Lot next door 3.0. http://www.noraworks.org/lnd3 (accessed December 3, 2014).
NHTSA (National Highway Traffic Safety Administration). 2008. National motor vehicle crash causation survey: Report to Congress. Washington, DC: DOT.
NHTSA. 2012. National survey of bicyclist and pedestrian attitudes and behavior. Washington, DC: DOT.
NHTSA. 2014. 2013 motor vehicle crashes: Overview. Washington, DC: DOT.
NRC (National Research Council). 2012. Disaster resilience: A national imperative. Washington, DC: The National Academies Press.
NRC. 2014. Reducing coastal risk on the east and gulf coasts. Washington, DC: The National Academies Press.
NYS 2100 Commission. 2013. Recommendations to improve the strength and resilience of the empire state’s infrastructure. New York: The Rockefeller Foundation.
Ogden, C. L., M. D. Carroll, B. K. Kit, and K. M. Flegal. 2014. Prevalence of childhood and adult obesity in the United States, 2011-2012. Journal of the American Medical Association 311(8):806-814.
Olmedo, O., I. F. Goldstein, L. Acosta, A. Divjan, A. G. Rundle, G. L. Chew, R. B. Mellins, L. Hoepner, H. Andrews, S. Lopez-Pintado, J. W. Quinn, F. P. Perera, R. L. Miller, J. S. Jacobson, and M. S. Perzanowski. 2011. Neighborhood differences in exposure and sensitization to cockroach, mouse, dust mite, cat, and dog allergens in New York City. Journal of Allergy and Clinical Immunology 128(2):284-292.
Olshansky, R. 2014. Post-disaster recovery: How to rebuild cities in compressed time. Paper presented at IOM Committee on Post-Disaster Recovery of a Community’s Public Health, Medical, and Social Services: Meeting Two, February 3, Washington, DC.
Pinellas County. 2012. Pinellas County post-disaster redevelopment plan. Pinellas County, FL: Pinellas County.
Prevention Institute. 2011. Fact sheet: Links between violence and health equity. http://www.preventioninstitute.org/component/jlibrary/article/id-311/127.html (accessed December 3, 2014).
Rebuild by Design. 2014. Living with the bay: A comprehensive regional resiliency plan for Nassau County’s South Shore. http://www.rebuildbydesign.org/project/interboro-team-final-proposal (accessed December 3, 2014).
Redlener, I. 2014. Post-disaster recovery: Restoring lives, fast. Paper presented at IOM Committee on Post-disaster Recovery of a Community’s Public Health, Medical, and Social Services: Meeting Two, February 3, Washington, DC.
Rexrode, C., and V. Dobnik. 2012. Hurricane Sandy: New Jersey, New York still struggle with power outages. The Huffington Post. http://www.huffingtonpost.com/2012/11/11/hurricane-sandy-new-jersey-york-poweroutage_n_2113856.html (accessed April 8, 2015).
Ricklin, A., A. Klein, and E. Musiol. 2012. Healthy planning: An evaluation of comprehensive and sustainability plans addressing public health. Chicago, IL: APA.
RWJF (Robert Wood Johnson Foundation). 2014. Time to act: Investing in the health of our children and communities. Princeton, NJ: RWJF.
Sallis, J. F., M. F. Floyd, D. A. Rodríguez, and B. E. Saelens. 2012. Role of built environments in physical activity, obesity, and cardiovascular disease. Circulation 125(5):729-737.
Schwab, J. 2014. Post-disaster recovery plans: Types and purposes. Paper presented at IOM Committee on Post-Disaster Recovery of a Community’s Public Health, Medical, and Social Services: Meeting Two, February 3, Washington, DC.
Shoemaker, D. 2006. Tools for mixed-income TOD. http://community-wealth.org/sites/clone.community-wealth.org/files/downloads/tool-CTOD-mixed-income_0.pdf (accessed November 30, 2014).
Springfield Redevelopment Authority. 2012. Rebuild Springfield. Springfield, MA: Springfield Redevelopment Authority.
State of the Air. 2013. Particle pollution. http://www.stateoftheair.org/2013/health-risks/health-risks-particle.html (accessed December 3, 2014).
Transportation Research Board. 2005. Does the built environment influence physical activity?: Examining the evidence. Washington, DC: National Academy of Sciences.
TRF (The Reinvestment Fund). 2015. About. http://www.trfund.com/about/ (accessed April 9, 2015).
Tsai, A. G., D. F. Williamson, and H. A. Glick. 2011. Direct medical cost of overweight and obesity in the USA: A quantitative systematic review. Obesity Reviews 12(1):50-61.
ULI (Urban Land Institute). 2013. Intersections: Health and the built environment. Washington, DC: ULI.
ULI. 2014. Housing in America: Integrating housing, health, and resilience in a changing environment. Washington, DC: ULI.
UNISDR (United Nations International Strategy for Disaster Reduction). 2013. Private sector strengths applied: Good practices in disaster risk reduction from Japan. http://www.unisdr.org/files/33594_privatesectorstrengthsapplied2013di.pdf (accessed March 15, 2015).
U.S. Department of the Treasury. 2014. About the CDFI Fund. http://www.cdfifund.gov/who_we_are/about_us.asp (accessed December 3, 2014).
USDA (U.S. Department of Agriculture). 2014. Urban wildlife. http://www.fs.fed.us/research/wildlife-fish/themes/urban-wildlife.php (accessed December 3, 2014).
Washington Emergency Management Division. 2014. Puget Sound transportation recovery annex. http://mil.wa.gov/uploads/pdf/PLANS/transportationrecoveryannexnew.pdf (accessed December 3, 2014).
What Works for Health. 2010. Physical environment—housing & transit. http://whatworksforhealth.wisc.edu/factor.php?id=126 (accessed December 3, 2014).
The White House. 2009. Developing effective place-based policies for the FY 2011 budget. http://www.whitehouse.gov/sites/default/files/omb/assets/memoranda_fy2009/m09-28.pdf (accessed March 4, 2015).
WHO (World Health Organization). 2014. Social determinants of health. http://www.wpro.who.int/topics/social_determinants_health/en (accessed December 1, 2014).
Williams, C. 2007. The built environment and physical activity: What is the relationship? Princeton, NJ: RWJF.
Winters, M., M. Brauer, E. M. Setton, and K. Teschke. 2010. Built environment influences on healthy transportation choices: Bicycling versus driving. Journal of Urban Health 87(6):969-993.














































