
7
The Effect on Tobacco Use of Raising the Minimum Age of Legal Access to Tobacco Products
The charge to the committee, as discussed in Chapter 1, was to assess the public health implications of raising the minimum age of legal access to tobacco products (MLA) through a review of the literature on tobacco initiation, modeling, and other approaches, as appropriate. This chapter provides the rationale for the committee’s consensus conclusions about the likely effects of raising the MLA on tobacco initiation. The committee’s conclusions serve as inputs to the two commissioned models, which provide quantification of the likely effects of increases in the MLA on smoking prevalence in the United States. The two simulation models used for the findings presented in both this chapter and the next (the Cancer Intervention and Surveillance Modeling Network [CISNET] and SimSmoke models) are well established approaches for estimating the likely impact of changes in tobacco control policies on population-level smoking initiation and prevalence, and on population health outcomes. The next chapter (Chapter 8) uses the results presented in this chapter (i.e., the estimates of the effects of different MLA policies on smoking initiation) as inputs for modeling several important public health outcomes, smoking-related morbidity and mortality. Chapter 8 concludes with a discussion of the likely effect of a change in the MLA on the many tobacco-related health effects not modeled.
The committee followed a principled and evidence-based process to arrive at its estimates of the potential impact of a change in the MLA on
tobacco initiation behavior. First, the committee conducted a review of relevant literature and synthesized the background evidence relevant to understanding age-related effects of tobacco use. This review included attention to the effects of MLA enforcement and the sources through which underage adolescents and young adults get tobacco as well as the development of an understanding of the biological, psychological, social, and environmental influences on tobacco use during adolescence and young adulthood.
Second, through an iterative and consensus-driven process, the committee considered how these age-related effects would translate into potential changes in rates of initiation across different age segments in adolescence and young adulthood. The committee considered the likely magnitude of changes in initiation effects that each of the three policy options under consideration (raising the MLA to 19, 21, or 25 years of age) would have on the different age segments and arrived at ordered, categorical estimates labeled as “small,” “medium,” or “large.”
Third, once consensus about the magnitude of the effect at each age segment and policy option combination was reached, the committee attached numeric ranges to each of the magnitude estimate descriptors. These ranges were developed through consideration of reasonable and conservative estimates of effects from a variety of public health interventions, including prior tobacco-related policy changes and data from the experience of changing the minimum age for alcohol purchase and use. These estimates were well vetted over a series of discussions in the committee. The committee selected ranges that showed increasing relationships with the ordered categories and which ranged in increments of 5 percent (to avoid implying an unrealistic precision in the estimates) from 5 to 30 percent for potential changes in initiation.
Finally, the committee discussed how to deal with the fact that there is scant direct evidence about how raising the MLA would affect tobacco use at different ages and thus that there is necessarily less confidence about some effects than others. The committee has most confidence about the estimates for the effects of raising the MLA to 19 and 21, and it is much less confident in estimates for an MLA of 25 because of the greater degree of extrapolation needed for estimating change. Thus, the inputs of estimates for the simulation models in Chapters 7 and 8 also include a range of potential values, with a broader range for the MLA of 25.
In assessing the possible impact of raising the MLA, the committee made a number of assumptions that affect the conclusions about the magnitude of the estimates and the inputs into the simulation models. Some of these assumptions are discussed in this chapter; others are discussed in Chapter 9. These assumptions include
- While policies implemented in the past will continue to have effects in the future, existing tobacco policies will remain in effect at their current rates and no new policies will be implemented. This assumption was made to isolate the effects of the new MLA.
- Levels of enforcement and of retailers’ compliance with age-based laws will remain at levels similar to those that currently exist.
- Noncommercial or social sources (e.g., through social networks of peers, families, and coworkers) of tobacco products will remain essentially as they are now, and no new efforts will be made to enforce the MLA restrictions against noncommercial or social sources who provide tobacco products to underage users.
- Sanctions will be directed as they are now, primarily toward retailers and not toward individual users.
- The new MLA will be applied to all tobacco products. However, the estimates of the magnitudes of effects are based on decades of research on cigarette use and not on other products. The committee acknowledges that the tobacco use landscape is changing rapidly with the introduction of a variety of tobacco products, including electronic nicotine delivery systems (ENDS; e.g., “e-cigarettes”). How these products may change existing patterns of cigarette use is not yet known, however, and thus these potential sources of influence could not be reasonably considered in arriving at estimates.
- The estimate of effects will be constant over time.
- Subpopulation differences in tobacco use that currently exist and that go into current initiation and prevalence rates will continue into the future. The committee did not consider whether there would be differential effects in subpopulations over future years.
- Rates of use of alcohol and other illicit drugs will not change in response to a change in the MLA for tobacco.
Estimating changes in the prevalence of tobacco use following a change in the MLA requires consideration of how each of the dynamic and interacting biological, psychosocial, and environmental factors contributing to use may vary by age. At any age, prevalence is a function of the rates of initiation (defined here as reaching a minimum of 100 cigarettes/lifetime) and the rates of cessation (defined in models as no use for 2 years after achieving the threshold for initiation). Both initiation and cessation are strongly related to age: Initiation decreases dramatically after young adult-
hood, and cessation rates start to increase during that same period. Thus, changes in the MLA will have their strongest impact on rates of initiation.
The committee based its estimates on an understanding of factors that are most relevant to achieving the threshold of 100 cigarettes for initiation, the data about which come from the National Health Interview Survey and are used in the simulation models in Chapter 8. The committee considered factors that operate both directly on tobacco use, such as access to tobacco products, and factors that operate more indirectly or distally, such as changes in biological vulnerability to the effects of nicotine with age or changes in social norms that indirectly affect motives for use. Smoking at least 100 cigarettes in one’s lifetime goes beyond occasionally trying cigarettes or “experimentation.” To achieve the benchmark of 100 cigarettes, an individual must have access to cigarettes over a period of time and is also likely to have developed symptoms of dependence and stronger motives for use beyond any perceived peer or social group pressure (Dierker and Mermelstein, 2010). Thus, the factors that influence vulnerabilities to developing dependence are more central to achieving the initiation threshold than factors related to the vulnerabilities to trying just one cigarette.
A critical component in the development of dependence and in continued tobacco use is the reinforcing effects of nicotine. As reviewed in Chapter 3, adolescents are at a heightened sensitivity to the rewarding effects of nicotine, and this sensitivity diminishes with age (Adriani et al., 2006; Jamner et al., 2003). Thus, the probability of use escalating to dependence after the first few trials is likely to decrease as one moves further away from adolescence. In addition, better developed executive functions provide young adults with increased decision-making capacity compared to younger adolescents, especially during times of emotional arousal (Steinberg, 2007), and, as a consequence, young adults may be less susceptible to cues to use tobacco than adolescents. These changes in biological vulnerabilities with age provide good support for suggesting that initiation rates and overall prevalence will decline with each increase in the MLA.
However, changes in the prevalence of tobacco use may not necessarily be linear with increases in the MLA or equal for all segments of underage individuals. Consider, for example, the declarative effect of raising the MLA. Changing the MLA has an indirect effect of helping to change norms about the acceptability of tobacco use, but this effect may take time to build. In addition, norms about the acceptability of tobacco use are also likely to vary by age, with a more stringent perceived unacceptability the farther away one is in age from the MLA. For example, if the MLA increases to 21, the social unacceptability of smoking is greater for a 16-year-old than it is for a 20-year-old.
Given this assumption that changes in the MLA will have different effects on adolescents at different ages, the committee considered possible
changes in initiation rates for three age divisions: (1) children and adolescents under age 15, (2) adolescents between 15 and 17, and (3) individuals at age 18 (for estimates of MLA of 19) or individuals at ages 18–20 or 21–24, for an MLA change to either 21 or 25. These age groupings reflect not just differences in years from the MLA but several important life developmental transitions that play a role in tobacco use as well. These developmental transitions include the increased mobility that comes with driving privileges, changes in social networks as adolescents enter and leave high school or transition to higher education, changes in employment levels and venues, leaving home, and potential changes in relationship status (e.g., marriage) and parenthood (Arnett, 2000, 2004; IOM and NRC, 2014; Settersten and Ray, 2010). Each of these life transitions and markers changes both potential sources of access to tobacco as well as motives for use (Bachman et al., 2002).
Adolescents Less Than 15 Years of Age
A substantial percentage of adolescents under age 15 are not yet in high school and, importantly, not yet of driving age. Adolescents under 15 are less likely to have peer networks that include individuals who are over the MLA (and the distance increases as the MLA increases), and these adolescents are also unlikely to be working in established work environments where they have coworkers who are over the MLA. Thus, social network sources and mobility are most restricted for adolescents under age 15. Social sources are the greatest access point for tobacco for underage youth (see Tables 5-2 and 5-3 in Chapter 5), and changes to the MLA affect the relative ease of availability of tobacco through social sources. For adolescents under 15 years of age, raising the MLA from 18 to 19 may have only a modest impact on reducing social sources, given the closeness in age. If adolescents already have networks with 18-year-olds, then these networks may also include 19-year-olds who have access to tobacco. Increasing the MLA to 21, however, provides a greater distancing of social sources. Although 19-year-olds may still be in high schools and thus potentially influence those under 15, it is far less likely that 21-year-olds are in the same social networks. Increasing the MLA from 21 to 25, however, is not likely to achieve any additional notable reductions in social sources for those under 15 than what is achieved with the 21-year-old MLA policy.
Although social sources play a central role in establishing adolescent tobacco use patterns, other factors that contribute to early adolescent tobacco use (for those who initiate before age 15) may place a limit on the reductions that would be achieved with increases in the MLA. Adolescents who reach a level of 100 cigarettes prior to age 15 may be those who are most susceptible to the reinforcing effects of nicotine, given their neuro-
developmental stage and the brain’s increased sensitivity to nicotine during those prime adolescent years (Jamner et al., 2003; Slotkin, 2002; Spear, 2000). These adolescents are also likely to be ones who have higher levels of psychological or substance use comorbidities, and ones for whom tobacco use has critical mood management properties (Kassel et al., 2003). These adolescents are the ones most likely to have a combination of problem behaviors, of which tobacco use is one manifestation (Ellickson et al., 2001; Silk et al., 2003). Their early use may be accelerated by these reinforcing and functional properties of nicotine, and these benefits of tobacco use may outweigh perceived consequences (Baker et al., 2004). These more vulnerable adolescents may also have social networks within which tobacco and other substances are more readily available, regardless of age, or they may have more contact with older individuals (Kobus, 2003). Thus, the committee expects that there may be a limit to the effect that changes in the MLA have on this subset of adolescents who initiate prior to age 15 and that changes in the MLA will not totally eliminate initiation at this young age. Thus, considering the balance of these factors, the committee estimates that, for adolescents under age 15, reductions in initiation will be small for an MLA of 19 and medium for MLAs of 21 and 25.
Adolescents 15 to 17 Years of Age
The committee expects that the greatest gains in reducing tobacco use will be achieved for adolescents between the ages of 15 and 17. This is a critical period in which to intervene to prevent not only an initial trial of tobacco use but also escalation to reach a threshold for initiation. A substantial proportion of adolescents try tobacco during these high school years, but most of these adolescents do not escalate beyond initial “experimentation,” and continued access to tobacco products is a major factor in this progression of use (Widome et al., 2007). Initial trials are often motivated by opportunity, social influences, as well as in-the-moment image enhancement, curiosity, and emotional arousals (both positive and negative) (Sarason et al., 1992). For this age group, negative consequences for tobacco use, through parental or school controls, are still relevant (IOM and NRC, 2011), and changes in the MLA are likely to increase these negative consequences as social norms adjust. Yet access to tobacco will still exist. Adolescents in this age group are still most likely to get tobacco through social sources (CDC, 2014; Johnston et al., 2014b). Between the ages of 15 and 17, youth mobility increases with the arrival driving privileges. Adolescents’ social networks and potential social sources of tobacco start to grow as some take on formal, part-time jobs with coworkers who may be over the MLA. Changing the MLA for tobacco to 19 may not change social sources substantially for these adolescents, but the committee expects
that raising the MLA to 21 will have a substantial impact in reducing the prevalence of tobacco use. Raising the MLA further to 25 may provide only an additional modest reduction in prevalence over that achieved with an MLA of 21, given that the resulting changes to social network sources may not be substantially different. However, boosting the MLA to 25 does have the additional benefit of social norm change.
Balancing these factors, the committee estimates that, for all the policy options considered, the reduction in initiation in the 15- to 17-year-old age group will likely be greater than the reduction in initiation among adolescents less than 15 years of age. Furthermore, the committee estimates that the higher the MLA is raised, the greater the effect on initiation rates is likely to be.
Young Adults 18 to 20 Years of Age
By age 18, many adolescents graduate from high school and have numerous transitions, including entering higher education, being exposed to more adults in the workforce, leaving home, and often experiencing significant changes in social networks (Arnett, 2000, 2004; Bachman et al., 2002; IOM and NRC, 2014; Settersten and Ray, 2010). To date, patterns of initiation have shown a tailing off in initiation by age 18 (see Table 2-8 in Chapter 2). The committee considered an estimate for this age group specifically only in the case of a raise in the MLA to 19, when individuals at age 18 are most directly affected by this policy change. Given that the social networks of 18-year-olds overlap more with the 19-year-olds, the committee expected a small reduction in initiation for 18-year-olds under an MLA of 19. The expected effect on initiation rates is higher for an MLA of 21 and higher still for an MLA of 25. The committee expects the effects of increasing the MLA to 21 or 25 on the initiation rates of 19- and 20-year-olds will be similar to the effects on 18-year-olds. This expectation of increased effect is due primarily to the increased social distancing expected when the MLA is raised to 21 or 25, but it also takes into account the benefits of the additional maturing of executive functions, the decreased sensitivity to the rewarding properties of nicotine, the additional social norms proscribing tobacco use, and the decreased social value of tobacco and motives for its use as individuals enter the workforce or parenthood.
Young Adults 21 to 24 Years of Age
Changes in initiation rates for young adults in the 21–24 age group were considered only for the case of raising the MLA to 25. The probability of initiation at these ages is substantially less than at earlier ages, given the developmental changes in life settings and milestones which are likely to
reduce the various motives for smoking (Bachman et al., 2002). In addition, young adults who have not yet begun smoking have likely developed coping strategies other than smoking for dealing with mood management and life stressors. Thus, the overall probability of new initiation is substantially lower. However, current patterns of tobacco marketing suggest that young adults are increasingly being targeted in tobacco promotions (Ling and Glantz, 2002), and tobacco promotions are frequently linked with bar settings and alcohol consumption, which may also keep this age group susceptible to initiation (Ling and Glantz, 2002). In addition, the committee considered that there may be more lax enforcement for an MLA of 25. Considering the balance of factors, the committee anticipates that some reduction in initiation would still occur with a raise in the MLA to 25 but that this reduction will be small.
Changes in the MLA for tobacco may also create some rebound effects—that is, delaying initiation to a later age. Rebound will result in increases in initiation over what has been seen historically in a given age group. The committee anticipates that most of the potential rebound from delayed initiation will occur in the first year after the new MLA and that this effect is likely to be modest. The changes in the MLA are likely to have an effect of further moving social norms and attitudes toward discouraging tobacco use and making it less appealing. These social normative changes may help to reduce rebound effects. Rebound may be most likely at the lower end of young adulthood (18–21) and very unlikely after age 25, when decision making has matured, individuals have established other coping strategies, and normative developmental life changes often further push individuals away from tobacco use.
The models commissioned by the committee considered only changes in initiation and not changes in intensity of smoking. Intensity is important to consider both because of its strong association with nicotine dependence (Fagerstrom et al., 1990; Prokhorov et al., 1996), and thus difficulties in quitting tobacco use and also because of the strong dose–response relationship between smoking intensity and morbidity (Hu et al., 2006). It is reasonable to expect that changes in the MLA for tobacco will also change the intensity of smoking for underage individuals, given the likely resulting changes in the ease of access to tobacco. At the same time, though, there is a background of ongoing historical changes, with overall consumption and intensity both decreasing among smokers, as there are more environmental
restrictions on tobacco use and increasing prices (HHS, 2014). Thus, it is difficult to estimate the independent gains in reducing intensity that will result from changes in the MLA, although the committee expects that these additional gains may be modest. Given this level of uncertainty and the lack of data about potential reductions in intensity, changes in intensity are not included in the modeling. For that reason the overall model estimates may ultimately underrepresent the potential health gains of changes in the MLA for tobacco.
Table 7-1 summarizes the committee’s ordered, categorical estimates of the effects that changes in the MLA will have in reducing initiation for the different age groups. The committee has more confidence in its estimates pertaining to the raising of the MLA to 19 or 21 than it does for raising the MLA to 25 because of the greater level of extrapolation needed for estimating change and other factors with increasing age. There are a variety of reasons for the uncertainty in these estimates. One is the lack of empirical evidence directly linking changes in the MLA and levels of MLA enforcement with changes in tobacco use. Another is the changing array of available tobacco products and uncertainty about how these new products may change patterns of tobacco use. The estimates being used as inputs for the simulation models include a range of potential values, with a broader range for the MLA of 25.
Conclusion 7-1: Increasing the minimum age of legal access to tobacco products will likely prevent or delay initiation of tobacco use by adolescents and young adults.
Conclusion 7-2: Although changes in the minimum age of legal access to tobacco products will directly pertain to individuals who are age 18 or older, the largest proportionate reduction in the initiation of tobacco use will likely occur among adolescents 15 to 17 years old.
Conclusion 7-3: The impact on initiation of tobacco use of raising the minimum age of legal access to tobacco products (MLA) to 21 will likely be substantially higher than raising it to 19, but the added effect of raising the MLA beyond age 21 to age 25 will likely be considerably smaller.
The previous section outlined, in qualitative terms, the expected effects of raising the MLA on initiation of tobacco use. The modeling exercise
TABLE 7-1 Committee Estimates Regarding Effects on Initiation
| Reduction in Initiation by Age Group | MLA 19 | MLA 21 | MLA 25 | ||
| Reduction in initiation for adolescents under age 15 | small | medium | medium | ||
| Reduction in initiation for adolescents ages 15–17 | small | large | large | ||
| Reduction in initiation for young adults age 18 | small | medium | medium | ||
| Reduction in initiation for young adults ages 19–20 | n/a | medium | medium | ||
| Reduction in initiation for young adults ages 21–24 | n/a | n/a | small | ||
| Characteristics of the Age Group That Might Influence Responsiveness to an MLA Increase | Factors Related to Effects on This Age Group as the MLA Increase Is Larger | ||||
| The youngest adolescents who have access to tobacco products and who persist in using tobacco beyond the first experimentation with them are ones who may be most susceptible to the reinforcing effects of nicotine or who have higher levels of psychological or substance use comorbidities, placing them at greater risk for escalation beyond 100 cigarettes and into established initiation and smoking. These youth may be less affected by increases in the MLA than even slightly older youth. | Younger adolescents are less likely to be in social groups with older adolescents or young adults. Their mobility is most restricted, depending on parents and other adults for transportation, thus reducing ease of access. Social sources remain the greatest access point for tobacco products, so the characteristics of social networks and the problem behaviors in those networks matter. Thus, the effect of MLA 19 will be less than that of MLA 21 or MLA 25. | ||||
| Changes in the MLA will increase the negative social consequences of tobacco use; adolescents at this age are most likely to get tobacco from social sources, including from coworkers above the MLA. | MLA 21 will begin to change access to tobacco products from social sources, much more so than MLA 19. MLA 25 will have only modest additional changes to social network, but includes benefits of social norm change. | ||||
| Most graduate from high school and experience life transitions. However, some 18-year-olds are in high school with, or are friends with, 19-year-olds who could purchase tobacco products. | Networks of 18-year-olds overlap with 19-year-olds but less so with those 21 or over. | ||||
| Young adults benefit from increased executive functioning, as well as decreased sensitivity to rewarding properties of nicotine and decreased social value of tobacco and motives for use as individuals enter workforce or parenthood. | 19- and 20-year-olds are often in college or the workforce, and their network of friends includes those age 21 and older. MLA 25 will have only modest additional changes to their social network, but includes benefits of social norm change. | ||||
| The probability of initiation among young adults ages 21 to 24 is substantially less than at earlier ages. Developmental changes in life setting and milestones are likely to reduce motives for smoking. Young adults in this age group have likely developed coping strategies other than smoking. | There could be more lax enforcement of MLA 25 in this age group. The tobacco industry engages in extensive marketing in bars to which this age group will have legal access; many young adults link smoking and drinking behaviors. | ||||
undertaken by the committee required quantification of these effects; the next section details the process by which the committee translated the qualitative terms into specific quantitative estimates of effects on the rate of initiation of smoking for various age segments. The SimSmoke and CISNET models used those committee-estimated initiation rates to project the effects of a change in the MLA on smoking prevalence. Chapter 8 then translates those quantitative estimates of effects on initiation and prevalence into quantitative estimates of effects on smoking-related premature mortality, lung cancer mortality, and maternal and child health outcomes using the simulation models that track lifetime trajectories of smoking behavior post-initiation. Chapter 8 also includes a discussion of the likely effect of changes in tobacco use on the many important adverse health effects not encompassed by the modeling exercises.
ESTIMATED INITIATION EFFECT SIZES
As described above, the committee used a consensus process to arrive at estimates for changes in initiation rates. As shown above in Table 7-1, the committee decided on three qualitative descriptors, labeled small, medium, and large. The committee attached numeric ranges to each of these magnitude descriptors. The ranges increase in increments of 5 percent (to avoid implying an unrealistic precision in the estimates) from 5 to 30 percent for potential changes in initiation. Small effects were considered to be 5 and 10 percent; medium effects were 15 and 20 percent; and large effects were 25 and 30 percent.
These estimates can be compared to effect sizes from a variety of tobacco control policies. The committee provides this brief summary not to make direct comparisons between other researchers’ findings and the committee’s estimates but to illustrate that the committee’s informed judgment about the likely effects of raising the MLA falls within the range of relevant effect sizes identified by or considered reasonable by other tobacco control researchers.
For example, tobacco control policy modules incorporated into the SimSmoke model used estimates from an expert judgment process to project the effects of a variety of interventions on adolescent, young adult, and adult smoking behaviors. As shown in Table D-1, these effects range from 1 percent to 50 percent. Of note, the effect size of the youth access restriction module in SimSmoke range from 2.5 percent to 30 percent. A modeling exercise assessing the cost-effectiveness of raising the legal smoking age in California, an effort not dissimilar from that in this report, used a range of 10 to 50 percent decrease in initiation for the projected effect on those under age 21 (Ahmad, 2005).
Flay (2007) summarized the effects of school-based prevention programs using a relative risk reduction calculation and estimated that the
potential medium-term (2–4 years) effects of a national program of well-implemented, school-based smoking prevention programs of proven effectiveness would be approximately 28 percent, rising to a potential 31 percent if the programming included a mass media component as well. A recent review of the effectiveness of increases in tobacco product excise taxes and fees on initiation of tobacco use in young people reports −0.43 as the median estimate of the elasticity of adolescent initiation with respect to price, meaning that a 10 percent increase in price would result in a 4.30 percent decrease in initiation (CPSTF, 2012).
Table 7-2 summarizes the committee’s estimates for percent reductions in initiation rates and potential rebound effects for the different age groupings assuming a change in the MLA to 19, 21, or 25 years of age, referred to as MLA 19, MLA 21, or MLA 25, respectively. The effect sizes used in the modeling reflect the committee’s judgment about the effect of an increase in the MLA on the entire United States. Some regions or subpopulations might experience larger effects, some smaller. The largest effect size used in other modeling exercises identified by the committee is 50 percent. The committee thinks that is overly optimistic and chose to use more conservative estimates in the modeling, although upper estimates are provided.
In addition, the committee recognized that although there is limited direct evidence about how raising the MLA might affect tobacco use at different ages, there is less confidence about some effects than others. The committee is the most confident about the estimates related to an MLA of 19 and 21 and is much less confident regarding estimates related to an MLA of 25 because of the greater level of extrapolation needed for estimating changes. To address this uncertainty, the committee includes ranges (upper and lower estimates) around each mid-estimate that vary according to the degree of the committee’s uncertainty. Thus, the estimates for the MLA of 25 used the broader range. The effect ranges do not represent bounds or a measure of uncertainty in the classical statistical sense. Rather these values reflect ranges that the committee deemed plausible (see Table 7-3). As will be discussed, the models simulate national cigarette smoking patterns and, in Chapter 8, their consequences. However, the committee’s effect sizes are percentage decreases from the status quo and thus would apply to any jurisdiction of any size assuming the jurisdiction roughly mirrors the United States as a whole. Absolute numbers of people affected would vary with the size of the population. The implications of this are discussed in Chapter 9.
For this report, the committee used the CISNET smoking population model (hereafter referred to simply as the CISNET model) calibrated to data from 36 National Health Interview Surveys covering the years 1965–
TABLE 7-2 Committee Estimates Regarding Effects on Initiation with Qualitative Descriptors and Numeric Estimates
|
MLA 19 |
MLA 21 |
MLA 25 |
|||||||
| Reduction in Initiation by Age Group | Qualitative Descriptor | Numeric Estimate | Qualitative Descriptor | Numeric Estimate | Qualitative Descriptor | Numeric Estimate | |||
| Reduction in initiation for adolescents under age 15 | small | 5% | medium | 15% | medium | 15% | |||
| Reduction in initiation for adolescents ages 15–17 | small | 10% | large | 25% | large | 30% | |||
| Reduction in initiation for young adults age 18 | small | 10% | medium | 15% | medium | 20% | |||
| Reduction in initiation for young adults ages 19–20 | n/a | n/a | medium | 15% | medium | 20% | |||
| Reduction in initiation for young adults ages 21–24 | n/a | n/a | n/a | n/a | small | 5% | |||
TABLE 7-3 Committee Inputs to the Model for Each MLA Policy Option with Qualitative Descriptors, Numeric Estimates, and Upper and Lower Range Estimates
|
MLA 19 |
MLA 21 |
MLA 25 |
|||||||
| Change in Initiation | Qualitative Descriptor and Numeric Estimate | Upper and Lower Estimatesa | Qualitative Descriptor and Numeric Estimate | Upper and Lower Estimatesa | Qualitative Descriptor and Numeric Estimate | Upper and Lower Estimatesa | |||
| Reduction in initiation for adolescents under age 15 | small (5%) | (4.2%, 6%) | medium (15%) | (12.5%, 18%) | medium (15%) | (10.7%, 21%) | |||
| Reduction in initiation for adolescents ages 15–17 | small (10%) | (8.3%, 12%) | large (25%) | (20.8%, 30%) | large (30%) | (21.4%, 42%) | |||
| Reduction in initiation for young adults age 18 | small (10%) | (8.3%, 12%) | medium (15%) | (12.5%, 18%) | medium (20%) | (14.3%, 28%) | |||
| Reduction in initiation for young adults ages 19–20 | n/a | n/a | medium (15%) | (12.5%, 18%) | medium (20%) | (14.3%, 28%) | |||
| Reduction in initiation for young adults ages 21–24 | n/a | n/a | n/a | n/a | small (5%) | (3.6%, 7%) | |||
| Rebound | small (5%) | (4.2%, 6%) | small (5%) | (4.2%, 6%) | none (0%) | n/a | |||
| Duration of rebound (in number of years) | 2 | n/a | 2 | n/a | 0 | n/a | |||
a Upper and lower estimates reflect the uncertainty ranges, with a smaller range (1.2) for MLA 19 and MLA 21, and a larger range (1.4) for MLA 25. The mid-estimate is treated as a geometric mean, not an arithmetic mean, thus, upper estimates are calculated as 1.2(x) and lower estimates as x/1.2 for MLA 19 and MLA 21 and as 1.4(x) and x/1.4 for MLA 25, resulting in slightly nonsymmetric ranges around the mid-estimates. These ranges do not represent bounds or a measure of uncertainty in a classical statistical sense. Rather, these values reflect ranges that the committee deemed plausible as described in the text.
2012 (Holford et al., 2014) to simulate age-specific smoking prevalence and mortality outcomes for birth cohorts projected through 2100. Using the smoking initiation estimates developed by the committee as inputs, the model was used to assess the potential effects of raising the MLA on U.S. smoking patterns by birth cohort and calendar year and the corresponding smoking-attributable mortality, life expectancy, and lung cancer deaths, using lung cancer projections from the CISNET Yale Lung Cancer Model (Holford et al., 2012).This report also used a recently updated version of the SimSmoke model that assumes the same smoking-rate inputs used by the CISNET model based on NHIS (Holford et al., 2014) and beginning in 1965. SimSmoke is able to reproduce the population smoking patterns by gender and by age in the United States from 1965 through 2012 (Levy, under review; Levy et al., under review), and it predicts the impact of current and future policies from 2015 through 2100. The initiation rates from 2015 forward reflect the effect of past policies under the assumption that policies other than raising the MLA will remain at 2014 levels into the future. As such, the initiation rates remain constant in future years under the status quo policy option. More details about the models can be found in Appendix D.
The models focused on characterizing the potential effects of raising the MLA on future rates of smoking initiation rates by age (the probability of becoming an established smoker at a given age, conditional on not having started before), considering both the prevention of smoking initiation for individuals younger than the new MLA (prevented initiation) and the delay of smoking initiation for some individuals who will start at an older age because of the policy (delayed initiation). The modeled policy effects varied by age, with assumed reductions in smoking initiation rates among individuals younger than the new MLA, while allowing for a potential increase (rebound) in the smoking initiation rates for individuals of or above the MLA (delayed smoking initiation).
Effects of Raising the MLA on Smoking Initiation
Figure 7-1 shows the initiation rates for the baseline (the current MLA) for both CISNET and SimSmoke and the corresponding mid-estimate for the smoking initiation inputs for the MLA 21. The SimSmoke baseline initiation rates are generally higher than those of the CISNET model. The specific initiation rates used in both models can be accessed on the CISNET webpage.1 Applying the CISNET initiation rates directly to a hypothetical birth cohort of 100,000 individuals would result roughly in 30,000 ever smokers by age 40. Applying the reductions in the mid MLA 21 scenario
________________
1 See https://resources.cisnet.cancer.gov/projects/#shg/iomr.
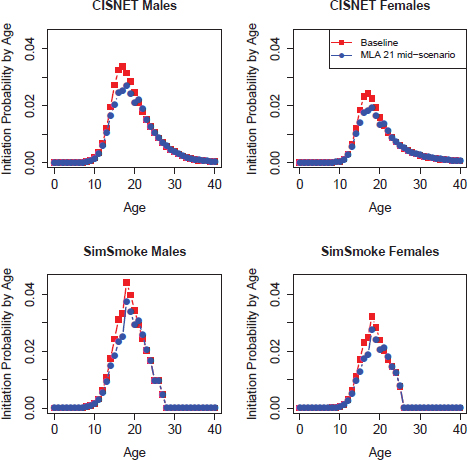
FIGURE 7-1 Initiation rates by age under baseline and middle scenarios for the effects of raising the MLA to 21.
would translate into 10 percent fewer smokers, with approximately 3,000 individuals never initiating plus another 600 individuals delaying smoking initiation until an older age (data not shown).
The models estimate the impact of reduced and delayed initiation on future annual U.S. smoking prevalence (described below) and smoking-related health outcomes (shown in Chapter 8), assuming that the MLA would change in 2015 and go into full effect immediately (with progressive staggered implementation evaluated in sensitivity analyses). Although raising the MLA could also affect future rates of cessation and smoking
intensity, the models did not incorporate effects on these rates because of uncertainty about the potential impacts. Thus, this represents a conservative assumption (one that underestimates the health benefits of the MLA policy), considering the substantial evidence linking delayed initiation with higher smoking cessation and lower smoking consumption rates.
Status Quo Projections
Any projections into the future imply some uncertainty because one cannot observe future outcomes before they occur. However, models provide an opportunity to explore the potential outcomes associated with various policy options and compare with the status quo, assuming all else remains unchanged. Both of the models employed by the committee begin with the creation of a baseline projection that assumes no change in the MLA; this serves as the status quo projection. The models are then run assuming the altered initiation rates provided by the committee (see Table 7-2) beginning after 2015. To characterize the incremental impacts of policy changes that are predicted by the model, the committee subtracted the outcome result for the baseline or status quo policy from the outcome result for the new MLA policy and then divided by the baseline outcome result, thus expressing the change as a percentage.
Both models project the baseline smoking prevalence in the United States from 2015 to 2100 assuming that smoking initiation and cessation rates will remain the same in all future years, but they do so in different ways and at different levels. CISNET projects that the age-specific initiation and cessation rates by gender estimated for the 1980 birth cohort will apply to all future birth cohorts. By contrast, SimSmoke assumes that the estimated age-specific initiation and cessation rates by gender observed for the year 2014 will persist throughout the modeled horizon (effectively assuming that tobacco control policies will remain at current levels). Although the differences may seem relatively minor, they lead to different projected smoking rates at the baseline for the two models. To facilitate comparison of the projected policy consequences associated with raising the MLA, the focus here will be on the relative effects of the MLA policy (i.e., the percentage reductions in smoking, mortality, and other health outcomes) while noting uncertainty about the absolute magnitude of the status quo.
Effects of Changing the MLA on Smoking Prevalence
Figure 7-2 shows projected smoking prevalence in the United States from 2014 to 2100 by gender as estimated by the CISNET model for the status quo and the three MLAs considered. The figure shows that even under the status quo, the CISNET model predicts a decrease in adult smok-
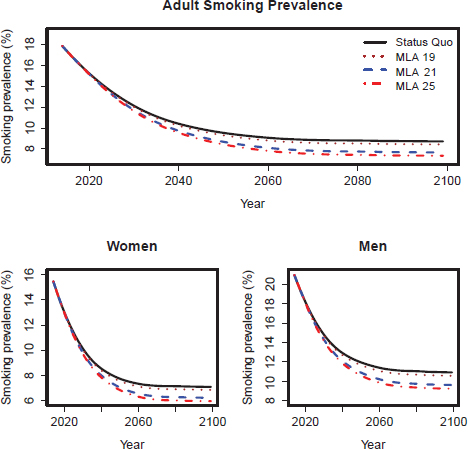
FIGURE 7-2 CISNET model-projected smoking prevalence for the three mid-MLA scenarios for adults (18+), adult women, and adult men in the United States for 2014–2100.
ing prevalence from 18 percent in 2014 to 9 percent in 2100 (15 percent in 2014 to 7 percent in 2100 for females and 21 percent in 2014 to 11 percent in 2100 for males).
The figure also suggests that the MLA 21 and MLA 25 options lead to considerable further reductions in smoking prevalence relative to MLA 19. Switching to a progressive staggered implementation of the policy (i.e., for an MLA greater than 19, increasing the MLA by 1 year each calendar year until reaching the desired MLA) did not significantly change the results (not shown).
Figure 7-3 shows the corresponding projection from the SimSmoke model. As can be seen, the SimSmoke model also projects a significant
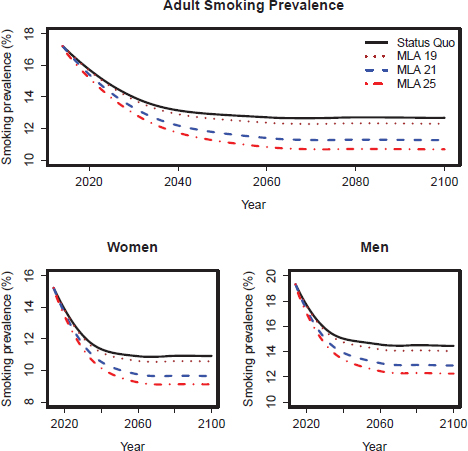
FIGURE 7-3 Projected smoking prevalence predicted by the SimSmoke model for adults (18+), adult women, and adult men in the United States for 2014–2100.
reduction in adult smoking prevalence—from 17 percent in 2014 to 13 percent in 2100 (15 percent in 2014 to 11 percent in 2100 for females and 19 percent in 2014 to 14 percent in 2100 for males)—to occur in the following decades. As shown in these figures, the SimSmoke model projects smaller decreases in prevalence than does the CISNET model because of the underlying lower baseline smoking initiation and higher (not shown) cessation rates in the CISNET model. Both models project that MLA 21 and MLA 25 would lead to larger reductions in smoking prevalence compared to MLA 19.
Table 7-4 shows a comparison between the two models of the projected adult smoking prevalence and the absolute percentage reductions in prevalence versus the status quo for selected years. The ranges in percentage
TABLE 7-4 Adult (18+) Smoking Prevalence (%) and Percentage (%) Reduction for Selected Years for the Mid-Estimates of Initiation Inputs from Table 7-3 (lower and upper estimate results shown in parentheses)
| MLA/Outcome | 2020 | 2040 | 2060 | 2080 | 2100 |
| SQ (status quo) | |||||
| SimSmoke prevalence |
15.7 |
13.1 |
12.7 |
12.7 |
12.7 |
| CISNET prevalence |
15.2 |
10.4 |
9.1 |
8.8 |
8.7 |
| MLA 19 | |||||
| SimSmoke prevalence |
15.7 |
12.9 |
12.4 |
12.3 |
12.3 |
| reduction versus SQ |
0.4% |
1.8% |
2.7% |
3.0% |
3.0% |
|
(0.2, 0.6) |
(1.3, 2.4) |
(1.9, 3.5) |
(2.1, 3.9) |
(2.1, 3.9) |
|
| CISNET prevalence |
15.2 |
10.2 |
8.8 |
8.5 |
8.4 |
| reduction versus SQ |
0.2% |
1.8% |
2.9% |
3.3% |
3.3% |
|
(0.14, 0.21) |
(1.5, 2.3) |
(2.4, 3.8) |
(2.7, 4.3) |
(2.7, 4.3) |
|
| MLA 21 | |||||
| SimSmoke prevalence |
15.4 |
12.2 |
11.4 |
11.3 |
11.2 |
| reduction versus SQ |
2.0% |
8.3% |
10.3% |
11.2% |
11.2% |
|
(1.5, 2.4) |
(5.8, 8.9) |
(8.3, 12.7) |
(9.0, 13.7) |
(9.0, 13.7) |
|
| CISNET prevalence |
15.1 |
9.7 |
8.1 |
7.8 |
7.7 |
| reduction versus SQ |
0.4% |
6.4% |
10.6% |
11.9% |
12.0% |
|
(0.37, 0.53) |
(5.4, 8.8) |
(8.8, 12.9) |
(9.9, 14.5) |
(10.0, 14.7) |
|
| MLA 25 | |||||
| SimSmoke prevalence |
15.2 |
11.7 |
10.8 |
10.7 |
10.7 |
| reduction versus SQ |
3.4% |
10.8% |
14.8% |
15.8% |
15.8% |
|
(2.9, 4.8) |
(9.2, 15.2) |
(12.6, 20.9) |
(13.4, 22.3) |
(13.4, 22.3) |
|
| CISNET prevalence |
15.1 |
9.5 |
7.8 |
7.4 |
7.3 |
| reduction versus SQ |
0.5% |
8.3% |
13.8% |
15.6% |
15.7% |
|
(0.36, 0.71) |
(5.9, 11.7) |
(9.8, 19.4) |
(11.1, 21.9) |
(11.2, 22.1) |
|
reduction represent the results from the lower and upper estimate scenarios (see Table 7-3) for effects on initiation for each MLA option. The results in Table 7-4 demonstrate that although the absolute prevalence predictions differ between the models, the two models predict similar percentage reductions in smoking for each MLA relative to the status quo. Specifically, both models estimate a roughly 3 percent decrease in the 2100 prevalence for the mid-MLA 19, an 11–12 percent decrease for the mid-MLA 21 scenario, and a 15.7 percent decrease for the mid-MLA 25 scenario.
Summary of Smoking Prevalence Projections
The modeling analysis suggests that raising the MLA for tobacco products could lead to considerable reductions in smoking prevalence. Both models suggest that it would take about a decade for the reductions in population-wide smoking prevalence to become meaningful; the delay can be attributed to the nature of the policy, which primarily affects children, adolescents, and young adults, so the effects become apparent only after those individuals affected by the policy have aged. Still, the projections show that with time the potential reductions and delays in smoking initiation would accumulate and lead to considerable decreases in prevalence.
Both models suggest that there is a considerable difference between the results of MLA 19 and MLA 21. Increasing the MLA from 21 to 25 leads to additional reductions, but they are smaller than the changes seen increasing the MLA from 19 to 21. This reflects the uncertainty in the assumed smoking initiation reductions for each MLA and the overlapping ranges for MLA 21 and MLA 25 (wider effect ranges for MLA 25).
Finding 7-1: Two policy simulation models project significant reductions in smoking prevalence from 2015 to 2100 in the United States in a status quo policy that captures the benefits from prior tobacco control policies.
Finding 7-2: The models predict that raising the minimum age of legal access to tobacco products would lead to additional reductions beyond the status quo in smoking prevalence based on reasonably conservative assumptions about the potential reductions in smoking initiation rates.
Finding 7-3: Raising the minimum age of legal access to tobacco products to 21 or 25 years would lead to larger reductions in smoking prevalence than the status quo or an increase of the MLA to 19.
Conclusion 7-4: Based on the modeling, raising the minimum age of legal access to tobacco products, particularly to age 21 or 25, will likely lead to substantial reductions in smoking prevalence.
As discussed in Chapter 2, tobacco use is far from uniform among various subpopulations and varies, for example, by race and ethnicity, social and economic status, geography, incarceration status, and the presence of mental illness (Bachman et al., 2011; Cropsey et al., 2004, 2008; Goodman and Capitman, 2000; Green et al., 2007; HHS, 2012; Johnson et al., 2000; Johnston et al., 2014a; Kann et al., 2014; Melnick et al., 2001; Peek et al., in preparation; SAMHSA, 2012; Welte et al., 2011; Ziedonis et al., 2008). Tobacco control advocates interested in decreasing tobacco use are particularly concerned about closing the “equity gap” by reducing tobacco use among the highest-risk populations. An important consideration for the committee is whether a change in the MLA would differentially affect high-risk populations with initiation rates that vary significantly from the national averages considered in this report, including the rates contained in the modeling. One possibility is that groups with higher-than-average initiation rates would remain relatively resistant to tobacco control interventions and the effect would be smaller in those populations, widening the equity gap. The equity gap could be narrowed if groups with lower-than-average initiation rates respond less to an increase in the MLA. The third possibility is that the effects will not vary significantly between groups.
The literature provides little evidence to clarify this issue. Two recent systematic reviews of the effects of population-level tobacco control interventions on adolescents and young adults found no clear evidence of a differential impact by social factors. One review found “little evidence of policies that have the potential to increase inequalities” (Thomas et al., 2008, p. 235). The second review identified price as the only intervention with a consistent effect that would decrease the inequalities in smoking initiation (Brown et al., 2014). Given the extremely limited data available and the fact that the models are not equipped to analyze according to high-risk populations, the committee did not produce separate analyses of the effect of raising the MLA by subpopulation. The committee’s conclusions also do not anticipate the changing landscape of tobacco products—in particular, the burgeoning popularity of electronic nicotine delivery systems (ENDS) (e.g., “e-cigarettes”). This new pattern of tobacco use creates various unknowns. The committee has no basis on which to conclude that the effect of a change in the MLA would have more or less effect on initiation with ENDS than with other tobacco products. Both of these limitations are discussed further in Chapter 9.
Adriani, W., V. Deroche-Gamonet, M. Le Moal, G. Laviola, and P. V. Piazza. 2006. Preexposure during or following adolescence differently affects nicotine-rewarding properties in adult rats. Psychopharmacology 184(3–4):382–390.
Ahmad, S. 2005. Closing the youth access gap: The projected health benefits and cost savings of a national policy to raise the legal smoking age to 21 in the United States. Health Policy 75(1):74–84.
Arnett, J. J. 2000. Emerging adulthood: A theory of development from the late teens through the twenties. American Psychologist 55(5):469–480.
———. 2004. Emerging adulthood: The winding road from the late teens through the twenties. New York: Oxford University Press.
Bachman, J. G., P. M. O’Malley, J. E. Schulenberg, L. D. Johnston, A. L. Bryant, and A. C. Merline. 2002. The decline of substance use in young adulthood changes in social activities, roles, and beliefs. Mahwah, NJ: Lawrence Erlbaum Associates.
Bachman, J. G., P. M. O’Malley, L. D. Johnston, J. E. Schulenberg, and J. M. Wallace, Jr. 2011. Racial/ethnic differences in the relationship between parental education and substance use among U.S. 8th-, 10th-, and 12th-grade students: Findings from the Monitoring the Future project. Journal of Studies on Alcohol and Drugs 72(2):279–285.
Baker, T. B., T. H. Brandon, and L. Chassin. 2004. Motivational influences on cigarette smoking. Annual Review of Psychology 55:463–491.
Brown, T., S. Platt, and A. Amos. 2014. Equity impact of interventions and policies to reduce smoking in youth: Systematic review. Tobacco Control 23(e2):e98–e105.
CDC (Centers for Disease Control and Prevention). 2014. National Youth Tobacco Survey. http://www.cdc.gov/tobacco/data_statistics/surveys/nyts (accessed February 8, 2015).
CPSTF (Community Preventive Services Task Force). 2012. Reducing tobacco use and secondhand smoke exposure: Interventions to increase the unit price for tobacco products. http://www.thecommunityguide.org/tobacco/RRincreasingunitprice.html (accessed January 20, 2015).
Cropsey, K., G. D. Eldridge, and T. Ladner. 2004. Smoking among female prisoners: An ignored public health epidemic. Addictive Behaviors 29(2):425–431.
Cropsey, K. L., J. A. Linker, and D. E. Waite. 2008. An analysis of racial and sex differences for smoking among adolescents in a juvenile correctional center. Drug and Alcohol Dependence 92(1–3):156–163.
Dierker, L., and R. Mermelstein. 2010. Early emerging nicotine-dependence symptoms: A signal of propensity for chronic smoking behavior in adolescents. Journal of Pediatrics 156(5):818–822.
Ellickson, P. L., J. S. Tucker, and D. J. Klein. 2001. High-risk behaviors associated with early smoking: Results from a 5-year follow-up. Journal of Adolescent Health 28(6):465–473.
Fagerstrom, K. O., T. F. Heatherton, and L. Kozlowski. 1990. Nicotine addiction and its assessment. Ear, Nose, and Throat Journal 69(11):763–765.
Flay, B. R. 2007. The long-term promise of effective school-based smoking prevention programs. Paper commmissioned by the Committee on Reducing Tobacco Use: Strategies, Barriers, and Consequences, Institute of Medicine. In Ending the tobacco problem (see Appendix D). Edited by R. J. Bonnie. Washington, DC: The National Academies Press.
Goodman, E., and J. Capitman. 2000. Depressive symptoms and cigarette smoking among teens. Pediatrics 106(4):748–755.
Green, M. P., K. L. McCausland, H. Xiao, J. C. Duke, D. M. Vallone, and C. G. Healton. 2007. A closer look at smoking among young adults: Where tobacco control should focus its attention. American Journal of Public Health 97(8):1427–1433.
HHS (Department of Health and Human Services). 2012. Preventing tobacco use among youth and young adults: A report of the Surgeon General. Atlanta GA: U.S. Department of Health and Human Services, Centers for Disease Control and Prevention, National Center for Chronic Disease Prevention and Health Promotion, Office on Smoking and Health.
———. 2014. The health consequences of smoking—50 years of progress: A report of the Surgeon General. Atlanta, GA: U.S. Department of Health and Human Services, Centers for Disease Control and Prevention, National Center for Chronic Disease Prevention and Health Promotion, Office on Smoking and Health.
Holford, T. R., K. Ebisu, L. McKay, C. Oh, and T. Zheng. 2012. Chapter 12: Yale lung cancer model. Risk Analysis 32(Suppl 1):S151–S165.
Holford, T. R., D. T. Levy, L. A. McKay, L. Clarke, B. Racine, R. Meza, S. Land, J. Jeon, and E. J. Feuer. 2014. Patterns of birth cohort-specific smoking histories, 1965–2009. American Journal of Preventive Medicine 46(2):e31–e37.
Hu, M. C., M. Davies, and D. B. Kandel. 2006. Epidemiology and correlates of daily smoking and nicotine dependence among young adults in the United States. American Journal of Public Health 96(2):299–308.
IOM and NRC (Institute of Medicine and National Research Council). 2011. The science of adolescent risk-taking: Workshop report. Washington, DC: The National Academies Press.
———. 2014. Investing in the health and well-being of young adults. Edited by R. J. Bonnie, C. Stroud, and H. Breiner. Washington, DC: The National Academies Press.
Jamner, L. D., C. K. Whalen, S. E. Loughlin, R. Mermelstein, J. Audrain-McGovern, S. Krishnan-Sarin, J. K. Worden, and F. M. Leslie. 2003. Tobacco use across the formative years: A road map to developmental vulnerabilities. Nicotine & Tobacco Research 5(Suppl 1):S71–S87.
Johnson, J. G., P. Cohen, D. S. Pine, D. F. Klein, S. Kasen, and J. S. Brook. 2000. Association between cigarette smoking and anxiety disorders during adolescence and early adulthood. JAMA 284(18):2348–2351.
Johnston, L. D., P. M. O’Malley, J. G. Bachman, J. E. Schulenberg, and R. A. Miech. 2014a. Monitoring the Future: National survey results on drug use, 1975–2013. Volume 1: Secondary school students. Ann Arbor, MI: Institute for Social Research, University of Michigan.
Johnston, L. D., P. M. O’Malley, R. A. Miech, J. G. Bachman, and J. E. Schulenberg. 2014b. Monitoring the Future: National survey results on drug use, 1975–2013: Overview, key findings on adolescent drug use. Ann Arbor, MI: Institute for Social Research, University of Michigan.
Kann, L., S. Kinchen, S. L. Shanklin, K. H. Flint, J. Hawkins, W. A. Harris, R. Lowry, E. O’Malley Olsen, T. McManus, D. Chyen, L. Whittle, E. Taylor, Z. Demissie, N. Brener, J. Thornton, J. Moore, and S. Zaza. 2014. Youth risk behavior surveillance—United States, 2013. Morbidity and Mortality Weekly Report 63(4):1–168.
Kassel, J. D., L. R. Stroud, and C. A. Paronis. 2003. Smoking, stress, and negative affect: Correlation, causation, and context across stages of smoking. Psychological Bulletin 129(2):270–304.
Kobus, K. 2003. Peers and adolescent smoking. Addiction 98(Suppl 1):37–55.
Levy, D. T. Under review. The use of SimSmoke to investigate maternal child health outcomes with exposure to cigarette smoke in the United States.
Levy, D. T., R. Meza, Y. Zhang, and T. R. Holford. Under review. The role of tobacco control policies in reducing US smoking prevalence from 1965-2012: Results from the SimSmoke Tobacco Policy Simulation Model.
Ling, P. M., and S. A. Glantz. 2002. Why and how the tobacco industry sells cigarettes to young adults: Evidence from industry documents. American Journal of Public Health 92(6):908–916.
Melnick, M. J., K. E. Miller, D. F. Sabo, M. P. Farrell, and G. M. Barnes. 2001. Tobacco use among high school athletes and nonathletes: Results of the 1997 Youth Risk Behavior Survey. Adolescence 36(144):727–747.
Peek, K. J., J. Kusel, S. L. Eyre, C. L. Auerswald, and B. L. Halpern-Felsher. In preparation. Understanding smokeless tobacco initiation and use among rural youth: An unexplored population.
Prokhorov, A. V., U. E. Pallonen, J. L. Fava, L. Ding, and R. Niaura. 1996. Measuring nicotine dependence among high-risk adolescent smokers. Addictive Behaviors 21(1):117–127.
SAMHSA (Substance Abuse and Mental Health Services Administration). 2012. National Survey on Drug Use and Health: Comparison of 2002–2003 and 2010–2011 model-based prevalence estimates (50 states and the District of Columbia). Rockville, MD: Substance Abuse and Mental Health Services Administration, Center for Behavioral Statistics and Quality, Department of Population Surveys.
Sarason, I. G., E. S. Mankowski, A. V. Peterson, Jr., and K. T. Dinh. 1992. Adolescents’ reasons for smoking. Journal of School Health 62(5):185–190.
Settersten, R., and B. E. Ray. 2010. Not quite adults. New York: Bantam Books.
Silk, J. S., L. Steinberg, and A. S. Morris. 2003. Adolescents’ emotion regulation in daily life: Links to depressive symptoms and problem behavior. Child Development 74(6):1869–1880.
Slotkin, T. A. 2002. Nicotine and the adolescent brain: Insights from an animal model. Neurotoxicology and Teratology 24(3):369–384.
Spear, L. P. 2000. The adolescent brain and age-related behavioral manifestations. Neuroscience and Biobehavioral Reviews 24(4):417–463.
Steinberg, L. 2007. Risk taking in adolescence: New perspectives from brain and behavioral science. Current Directions in Psychological Science 16(2):55–59.
Thomas, S., D. Fayter, K. Misso, D. Ogilvie, M. Petticrew, A. Sowden, M. Whitehead, and G. Worthy. 2008. Population tobacco control interventions and their effects on social inequalities in smoking: Systematic review. Tobacco Control 17(4):230–237.
Welte, J. W., G. M. Barnes, M.-C. O. Tidwell, and J. H. Hoffman. 2011. Tobacco use, heavy use, and dependence among adolescents and young adults in the United States. Substance Use and Misuse 46(9):1090–1098.
Widome, R., J. L. Forster, P. J. Hannan, and C. L. Perry. 2007. Longitudinal patterns of youth access to cigarettes and smoking progression: Minnesota Adolescent Community Cohort (MACC) study (2000–2003). Preventive Medicine 45(6):442–446.
Ziedonis, D., B. Hitsman, J. C. Beckham, M. Zvolensky, L. E. Adler, J. Audrain-McGovern, N. Breslau, R. A. Brown, T. P. George, and J. Williams. 2008. Tobacco use and cessation in psychiatric disorders: National Institute of Mental Health report. Nicotine & Tobacco Research 10(12):1691–1715.


























