
7
Social Enterprise and Investment in Health
Key Messages
Specifically the model that we talk is about scaling impact, not about scaling organizations and not about scaling volume of services provided. And we know that we have to scale impact because the problems far exceed the current solutions.
—Krishna Udayakumar
I am a huge believer that the funding should be structured for the need and not the other way around. Many funders tend to have very strict requirements on how their capital is deployed, and it ends up having the recipients or the organizations [struggle] to fit that.
—Beth Bafford
Up until now we have not figured out how to make leadership what economists call endogenous because now it is totally exogenous, like a superstar that comes out of nowhere. The system has to make leadership endogenous.
—Oscar Picazo
How does empowerment start? In the past it was often self-empowerment, but can we find the few people [who] we can empower [so] that [they] can help others be empowered?
—Monique Dolfing-Vogelenzang
Social enterprise represents one possible approach to leveraging the strength and reach of an empowered nursing and midwifery workforce. Because many social enterprises have a commercial focus, but are small and medium sized, they often lack access to traditional means of funding. Speakers shared perspectives on models of social enterprise, such as franchises, that could embed nurses and midwives in communities, as well as innovative financing mechanisms to fund them.
THE ROLE OF SOCIAL ENTERPRISE1
Social enterprises are businesses whose primary purpose is the common good; they use business practices and the marketplace to advance social justice and development. Krishna Udayakumar explained that there are characteristics that define a social enterprise: it addresses a social need, it generates income mainly through its commercial activities, and it focuses primarily on the common good. Additionally, social enterprises have clear rules about the reinvestment of profits to further its “social mission.” Social Enterprise Canada uses a graph model to explain that social enterprises have a “blended value return on investment”; they fit between charities, whose focus is social return on funding, and traditional for-profit enterprises, whose focus is financial return on investment (see Figure 7-1).
Udayakumar cautioned that these definitions leave room for interpretation, depending on the lens through which they are viewed. He noted that some traditional for-profit structures, such as pharmaceutical companies, produce social goods and could be considered social enterprises under these definitions. At Duke University, he observed that social entrepreneurs are viewed as change agents who:
- Adopt a mission to create and sustain social value,
- Recognize and pursue new solutions,
- Engage in continuous innovation and learning,
- Act without being constrained by current resources, and
- Are accountable to the populations they serve.
________________
1 This section summarizes information presented by Krishna Udayakumar, International Partnership for Innovative Healthcare Delivery (IPIHD).
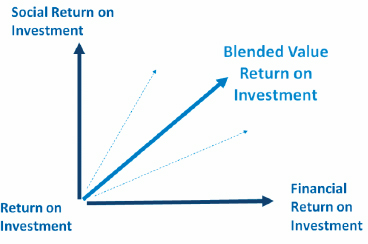
FIGURE 7-1 Social enterprise seeks a blended return on investment.
NOTE: For more information, visit the Social Enterprise Canada website: http://www.socialenterprisecanada.ca/en/learn/nav/whatisasocialenterprise.html (accessed November 4, 2014).
SOURCE: Social Enterprise Canada, n.d.
Social entrepreneurship runs the risk of constantly creating innovations, or having “pilot-itis.” Udayakumar noted that the main focus in the field should be on scaling up, and specifically scaling up impact rather than scaling organizations or volume of services. Ideally, solutions presented by social entrepreneurs expand faster than current problems to reduce their magnitude. He described three ways to scale impact: scaling out, scaling deep, and changing the ecosystem. For scaling out, he proposed building solutions with potential to spread to new markets and locations, or increase reach. This could include branching, affiliating, or disseminating. For scaling deep, he proposed creating new services for the same end users, or enhancing quality of existing services. Lastly, to change the ecosystem, he proposed modifying the context and behavior to enhance the work of other organizations or individuals.
INVESTING IN GLOBAL HEALTH2
Financing for social enterprise can be creative, including debt, equity, grants, donor funding, and public funding. Beth Bafford explained that even within traditional means, innovative financing mechanisms can be constructed depending on outcomes desired. She described the Global Health Investment Landscaping Project (GHILP), whose goal was to provide a
________________
2 This section summarizes information presented by Beth Bafford, Calvert Foundation.
picture of current sources of debt and equity financing for global health entrepreneurs in East Africa and India. Its objectives were three-fold: to understand the range of available financial options, to explore potential partners, and to share findings with other interested investors. GHILP focused on debt and equity providers, health or health-as-vertical organizations, and funds with an explicit impact orientation.
Lessons Learned
Bafford described four important lessons that were learned in this exercise. First, there is a great and growing interest in investing in health care. There are multiple reasons for this, including a growing middle class with an increased willingness and ability to pay and better technology and access to information. Multinational companies also see emerging markets as growth opportunities, and high-income country “medical elite” see opportunities to spread capabilities and capacities.
Secondly, she said, there is a financial gap in the sector that is ripe for impact investors. Currently, there is a lot of focus from donors and grant providers on rural populations and the “bottom of the pyramid” (BOP). There is also traditional private equity and debt seeking high returns from urban and suburban high-income populations. In between is a gap where both BOP and middle-class populations can be addressed via debt and equity investment models. In particular, low-margin, high-volume models for the BOP and higher-margin models for the middle class could be particularly suitable for social enterprises that could balance return and impact.
The third lesson Bafford described is the need for better communication and coordination. There is not a lot of information passed between actors in this space, particularly between those in the public sector and those in the private sector, she said. There is also not a lot of discussion around policies that enhance private-sector delivery, or coordination around services.
Lastly, Bafford said that there are key parts of the value chain that need greater attention from government and philanthropy. Market-based business models can address some of the issues of health care delivery and ease the burden on the public sector. However, government and philanthropy need to focus on providing the proper support for social enterprise to thrive, particularly professional education and research and development.
Innovative Financing Mechanisms
Bafford went on to describe two innovative financing mechanisms that her institution has developed to fill some of the unmet needs in funding. One is a type of social impact bond in which the Calvert Foundation loaned funds to a childhood asthma management organization to scale up its pro-
gram. This arrangement covers upfront funding for prevention interventions as well as evaluation, which yields cost savings to the health system each year over 3 years. From these savings, the health care provider who realizes the savings pays back the loan with interest over those 3 years. The second mechanism is a bridging loan to close the time gap between grant approval for commodities and supplies on the donor side and disbursement of funds to the nongovernmental organization (NGO). Because the Calvert Foundation can provide the funds more quickly, the NGO has better negotiating ability when ordering the goods. When the funds are disbursed, they go toward paying back the loan.
INNOVATIONS IN THE PROVISION OF HEALTH SERVICES USING EMPOWERED NURSES AND MIDWIVES IN THE PHILIPPINES3
Oscar Picazo presented some thoughts about health systems and the health care workforce that were drawn from two decades of personal experiences working in health economics, financing and policy, and human resources for health in the Philippines and around the world. A paper he developed to enrich discussions at the workshop highlighted four innovations using nurse or midwife empowerment as a basis for their establishment. Each of these private-sector initiatives comes from the Philippines and focuses on deployment of nurses and midwives to underserved areas by employing more sustainable business models that emphasize the health needs of low-income populations. Below are the four innovations profiled in Picazo’s paper that can be found in Appendix D of this report:
- Well-Family Midwife Franchise Clinics
- Mother Bles Birthing Clinics, a public–private partnership
- Blue Star Pilipinas Clinics
- EntrepreNurse Cooperatives
Innovative Models
The Well-Family Midwife Clinics
The Well-Family Midwife Clinics was created in 1997 as a U.S. Agency for International Development (USAID) project, and then became a social
________________
3 This section summarizes information presented by Oscar Picazo, Philippine Institute for Development Studies.
franchise with trained nurses taking on the role of the midwives.4 There are now 120 clinics in Manila and 28 provinces. Picazo explained that this innovation scaled up successfully and has become mainstream.
Mother Bles Birthing Clinics
Mother Bles Birthing Clinics was established in 2009 by a local foundation. It is a public–private partnership with local governments providing land or facility space, and the foundation providing seed capital, training, and management systems. Currently there are 50 clinics in 10 provinces all accredited by PhilHealth.
Blue Star Pilipinas Clinics
Blue Star Pilipinas Clinics is a nonprofit franchise of clinics, originally created by two international NGOs, but currently run by a local corporation that acts as the franchiser. Midwives are the franchisees. There are now 200 clinics in peri-urban areas.
EntrepreNurse Cooperatives
The Well-Family Midwife Clinics, the Mother Bles Birthing Clinics, and the Blue Star Pilipinas Clinics are all well established. Picazo then described a fourth model, EntrepreNurse, which is gaining more traction in the Philippines. EntrepreNurse was established by the Department of Labor and Employment because there was a drop in emigration opportunities for nurses, resulting in high unemployment of nurses in the Philippines. Nurses were organized into cooperatives, with services including home care, primary health care, medical transcription, emergency services, and wellness and fitness. There are now five nurse cooperatives in one region. The idea has been adopted by another region, but because the documentation is poor and there is no donor funding, it is difficult to assess how many cooperatives there are in total.
Challenges Faced
These models function because there is high availability of nurses and midwives; approximately 260,000 nurses graduate per year, with one-third of them being licensed. They are also dependent on visionary leadership and
________________
4 For more information about the Well-Family Midwife Clinics, please visit their website: http://healthmarketinnovations.org/program/well-family-midwife-clinic (accessed November 4, 2014).
investment; all of these models were championed by an individual willing to take risks and mobilize novel resources. Picazo noted that one challenge is fostering such leadership within the system, rather than relying on the external individual. He queried, how can leadership be made endogenous? Is it by training, inspiration, coaching, or something else? Finally, he stated that a third element of success is the support of PhilHealth and its expanded reimbursement of reproductive health clinics.
However, there are a few constraints. Regulatory obstacles mean it can take anywhere from 18 months to 2–3 years to receive an operating license because there is no sense of urgency to issue them. Another constraint is professional territoriality that has been especially evident between obstetricians and gynecologists on one side and nurses and midwives on the other. Third, there is inadequate training of nurses and midwives particularly in terms of business management.
Next Steps
When asked about next steps for improving health systems and empowering nurses and midwives in the Philippines, Picazo proposed three possibilities: scaling, improving reimbursement, and training.
Scaling
Currently, most of the franchise clinic models focus on reproductive health, maternal health, and family planning. Expanding to include care for patients with malaria, tuberculosis, and mental health would provide more comprehensive and responsive services. Successful programs with integrated services could potentially spread their practices more broadly.
Improving Reimbursement
PhilHealth currently has a generous payment scheme for birthing services, but Picazo commented that for other services, rates are lower than the prevailing cost for some of these franchises. This limits revenue, which ultimately limits growth.
Training
Currently, the government and donors offer technical training only to public-sector health workers and not to the private sector. Because many nurse and midwife franchises offer public health services, additional training by government could be obtained to assist nurses and midwives in widening their scope through newly acquired technical skills.
FRANCHISE APPROACH TO SOCIAL FINANCE AND SOCIAL ENTEPRISE
In the discussion that followed, participants further explored the breadth of training that nurses and midwives receive in formal education. Some participants questioned whether teaching business skills should be a default part of licensing or degree programs, particularly when students are focused on honing clinical skills. Others differentiated between management skills, such as learning how to work as part of a team, and entrepreneurial skills. One participant explained that if nurses are in graduate school or in the field and do not understand business, they will be excluded from decision making. However, if training nurses and midwives to be business-oriented is a key goal, then it is a criterion that should be considered upon entry to training programs.
The franchise model was reiterated as one way to distinguish between those who prefer to focus on clinical practice and those who might desire to be an independent professional and who might display additional skills such as business acumen. In the franchise model, whether it is traditional or more socially driven, the broader organization drives the business centrally and can embed systematic practices, such as back-office operations and accounting. The franchisees plug the system into their own context and offload administrative tasks so they can focus on their clinical practice.
Franchising can also allow a nurse or a midwife to deepen her scope of practice even in different disciplines; for example, the four franchises that Picazo discussed started with family planning, reproductive health, and maternal health as their main scope, but there is an opportunity to include tuberculosis, mental health, and youth reproductive health into their practice. Franchises can also help create networks between practitioners that can leverage economies of scale and collective power, compared to the relatively minimal impact of solo individual practices.
FRANCHISE EXAMPLE IN GHANA5
Monique Dolfing-Vogelenzang described a for-profit franchise network being developed in Ghana to provide care to middle-income families. The model includes four important components: (1) customer focus, (2) efficient operations, (3) quality care, and (4) skilled staff. Its objectives include building a scalable model to improve access to and quality of health care at affordable prices. Its intended outputs include the establishment of 10 family health clinics that increase economic activity in health and associated
________________
5 This section summarizes information presented by Monique Dolfing-Vogelenzang, Medical Credit Fund (MCF).
sectors and patient–provider contact, while its outputs include a recognized brand of high-quality health care use that provides a business case for greater investment. Its intended impact includes greater gender equity, job creation, better population health, and increased investment in the private health sector.
The model is based on a partnership, which includes multinational corporations. Dolfing-Vogelenzang cautioned that nonexclusivity is an essential part of the process, particularly when partnering with entities producing goods (such as pharmaceutical or medical device manufacturers). Other partners she recommended include those with expertise in training using multiple media and in different settings, as well as finance entities. At the center of the partnership is the shared services organization that owns the model and its parts, and who franchises the model to network clinics.
Dolfing-Vogelenzang described the steps she and her colleagues have identified to establish the franchise, from inception to feasibility analysis, procurement, contracting, implementation, and monitoring and evaluation. Procurement and contracting requires finding the right person to run the operation and incentivize partners, she explained. It also means connecting to the right people in-country, perhaps with access to high levels of government, to mobilize support and interest. Another participant raised the possibility of twinning or partnering with similar organizations in another country to build capacity.
REFERENCE
Social Enterprise Canada. n.d. What is a social enterprise? http://www.socialenterprisecanada.ca/en/learn/nav/whatisasocialenterprise.html (accessed November 4, 2014).
This page intentionally left blank.










