
4
Nursing and Midwifery Education and Enterprise
Key Messages
In most of the world, nursing and midwifery are at a postsecondary educational level, which in itself is a barrier for many girls going into a profession because girls, especially in low- and middle-income countries, [often] drop out before completion of secondary education for a variety of reasons.
—Mary Barger
Strengthening women’s own capabilities to care for themselves and their families is empowerment of more than one person. It is not just the midwife who knows how to do this, but also the woman, and her family, and her community, and ultimately also her child.
—Petra ten Hoope-Bender
Younger nurses are more business- and leadership-oriented; if given the proper support, they could be transformational in the health system.
—Barbara Parfitt
SETTING THE STAGE1
Mary Barger pointed out that midwifery and nursing are two separate disciplines, even though they are often joined together in the United States. In most of the world, the two are at a postsecondary educational level; this can be a barrier for many young women who do not complete secondary education. However, if these young people can be retained through secondary school, then the fields of nursing and midwifery can be areas for further education. She gave the example of a nonprofit organization in Malawi that assists young women to purchase schools uniforms, books, and other supplies, and then provides stipends to continue in nursing and midwifery providing that they work at a government facility for roughly 2 years after graduating.
Barger stated that there are international competencies for midwifery, which were developed by the International Confederation of Midwives (ICM). Additionally, she said, there is some question as to whether auxiliary midwives meet those competencies. There are also questions around the number of months of education, short programs versus longer ones, and clinical teaching structures. In some countries, the results of entrance exams determine which health professional tract students will be placed. However, health professionals often take basic courses together, and Barger stated this can cause friction if students in “lower” tracts outperform those in “higher” tracts in the same course. Also, the accreditation process for schools and certification for specialty skills can vary, and curricula can sometimes be outdated.
The context of care for nurses and midwives is also diverse, ranging from the standard hospital settings to clinics and community-based care. Barger remarked that in refugee situations, nurses and midwives are frequently organizing the services, often engaging in innovative public health approaches. Nurses and midwives often find themselves playing the role of supervisor, particularly to community health workers, regardless of whether they have received the necessary leadership skills training.
STATE OF THE WORLD’S MIDWIFERY2
There are a number of perspectives on midwifery, according to Petra ten Hoope-Bender, and a recent Lancet series provides an independent space to share and analyze those perspectives. It defines midwifery as:
________________
1 This section summarizes information presented by Mary Barger, University of San Diego.
2 This section summarizes information presented by Petra ten Hoope-Bender, ICS Integrare (Instituto de Cooperación Social Integrare).
Skilled, knowledgeable, and compassionate care for childbearing women, newborn infants, and families across the continuum throughout prepregnancy, pregnancy, birth, postpartum, and the early weeks of life. Core characteristics include optimizing normal biological, psychological, social, and cultural processes of reproduction and early life; timely prevention and management of complications; consultation with and referral to other services; respecting women’s individual circumstances and views; and working in partnership with women to strengthen women’s own capabilities to care for themselves and their families. (Renfrew et al., 2014, p. 1130)
Ten Hoope-Bender highlighted the last section of the definition, which states that a core responsibility of midwives is to strengthen a woman’s own capability to care for herself and her family. Because of this, investment in health promotion strengthens not only the midwife, but also the woman, her family, her child, and her community.
The Lancet series illustrated a number of important elements (see Figure 4-1). Health care, ten Hoope-Bender noted, should be “organized, available, accessible, acceptable, [and] good quality.” Values include respectful and tailored care and community knowledge, while the philosophy of care involves optimizing mental, physical, social, and cultural processes. Ten Hoope-Bender expanded on the latter; maternal and newborn care should be grounded in pregnancy and birth as a normal, not necessarily medical, process that is healthy for both mother and baby, and more realistic for “close-to-client” care provision.
On a related front, ten Hoope-Bender also shared the State of the World’s Midwifery Report 2014, which examined 73 countries over a 15-year projection (UNFPA et al., 2014). It established a baseline on workforce, education, interventions, and productivity, and then costed scenarios with assumptions of reasonable improvement in these areas. For example, it considered lower staffing attrition (among all health care staff, not just midwives), more standardized education, and better family planning. Among some of the outcome measures included are an estimated 16 percent return on investment in midwives when regarding lives saved and caesarean sections prevented, as well as recognition that when midwives are trained to international standards, they can provide 87 percent of the essential interventions necessary for women and newborns.
Ten Hoope-Bender shared some examples of innovations that can help promote a greater global understanding of the role midwives can play in a more effective health system:
- Jacaranda Health is a social venture combining business and clinical innovations that targets women living in Nairobi, Kenya’s peri-urban areas. It provides high-quality, friendly, and affordable
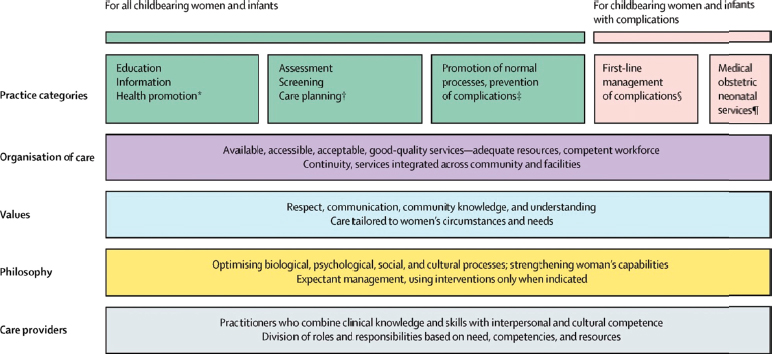
FIGURE 4-1 The framework for quality maternal and newborn care: maternal and newborn health components of a health system needed by childbearing women and newborn infants.
SOURCE: Renfrew et al., 2014. Reprinted with permission from Elsevier (Lancet, 2014, 384(9948):1129-1145).
-
maternal care through a set of self-sustaining and scalable clinics. The program has a dual focus of addressing the needs of the female patients it serves, as well as improving the standard of care.
- Manoshi is a program focused on migrant populations living in informal urban settlements in Bangladesh, where birth usually occurs in homes of 10–15 inhabitants, and there is no privacy. Clean birthing centers were established, and community health workers reached out to the population regarding prenatal and antenatal care. Additionally, they developed a referral service where they could transport women to hospitals and assist them through administration at the hospital and into the delivery room, cutting out several of the serious delays that can cost women their life.
- The Afghanistan community midwife program selects women in the community to be trained as midwives and then return to the community to work. It has led to the creation of the very visible Afghanistan Midwife Association in 2006, with 3,000 members.
ANNOTATIONS TO FIGURE 4-1
* Examples of education, information, and health promotion include maternal nutrition, family planning, and breastfeeding promotion.
† Examples of assessment, screening, and care planning include planning for transfer to other services as needed, screening for sexually transmitted diseases, diabetes, HIV, pre-eclampsia, mental health problems, and assessment of labor progress.
‡ Examples of promoting normal processes and preventing complications include prevention of mother-to-child transmission of HIV, encouraging mobility in labor, clinical, emotional, and psychosocial care during uncomplicated labor and birth, immediate care of the newborn baby, skin-to-skin contact, and support for breastfeeding.
§ Examples of first-line management of complications include treatment of infections in pregnancy, anti-D administration in pregnancy for rhesus-negative women, external cephalic version for breech presentation, and basic and emergency obstetric and newborn baby care (WHO 2009 monitoring emergency care), such as management of pre-eclampsia, post-partum iron deficiency anemia, and post-partum hemorrhage.
¶ Examples of management of serious complications include elective and emergency caesarean section, blood transfusion, care for women with multiple births and medical complications such as HIV and diabetes, and services for preterm, small for gestational age, and sick neonates.
TABLE 4-1 Hypothetical Model of Inadequate Access to Antenatal Care in Low and Middle Income Countries
| Program Design Standard antenatal programs (WHO, 2002) |
Women’s views and Experiences Findings from meta-synthesis (Finlayson and Downe, 2013) |
||
| Theories that underpin antenatal care programs | Pregnancy is potentially risky for mother and baby | Beliefs and attitudes | Pregnancy is a healthy physical state |
| Pregnancy is a positive social state that will, in general, be welcomed by the family and community | Pregnancy can be socially risky. It can be subject to malign magical forces from jealous relatives and community members | ||
| Women and families have enough resources to make rational economic choices to access care | A choice to access care might mean a risk to survival, either due to resultant lack of food in the future, or because of the difficulties and dangers associated with travel to health care facilities | ||
| Principles of care delivery | Antenatal care is affordable | Experience of care delivery | Antenatal care is subject to unexpected costs levied at the point of need |
| Staff attitude is not relevant and/or is generally positive | Staff attitude is highly relevant, and can be discriminatory, neglectful, or even abusive | ||
| All the resources needed for the level of care on offer are present | Resources are often not available, and transfer is then necessary to the next level of care | ||
NOTE: This table represents one section of the original table. The complete version of this table can be found in Finlayson and Downe, 2013.
SOURCE: Finlayson and Downe, 2013.
-
The training of these midwives and the establishment of standards of care contributed to a more than 50 percent reduction in maternal mortality. Additionally, the midwives gained standing in their communities and were consulted on women’s and family issues.
- The Community-Based Midwifery Diploma Program at BRAC University in Bangladesh is a hub-and-spoke model of education in which faculty and curricula are developed at the “hub” and students are locally selected at the “spokes.” An assessment of the program noted that the investment yielded major returns in fewer obstetric complications and surgeries as well as more infant and maternal lives saved.
Ten Hoope-Bender distilled some lessons from these programs, culminating in the concept of midwife-led units for birthing and early childcare. This approach keeps midwives close to the community, with outreach through community health workers. A Cochrane review showed that such an approach could lead to higher maternal satisfaction and better maternal and neonatal outcomes (Sandall et al., 2013). She concluded, cautiously, that such approaches should be implemented incrementally with transition models and country-level health system internalization. She also reiterated the need to make programs consumer-focused by embedding consumers into the initial design. She shared the details of some research that shows there can be a disconnection between the perspectives of program designers and the end-users, using the example of antenatal care centers (see Table 4-1).
Following the presentation, speakers and participants raised additional questions about enhancing nursing and midwifery education and impact:
- What is the informal impact of empowering nurses and midwives on their families and communities, and how is that impact measured? Is there a cost savings for informal services nurses and midwives might provide outside of health care settings?
- When women are not traditionally part of the leadership in a community, are there ways to ensure they are heard and respected as technical experts? One participant described a program in Egypt in which social change agents are identified to support the nurse or midwife’s efforts.
WOMEN’S EMPOWERMENT THROUGH EDUCATION USING A SOCIAL BUSINESS MODEL3
Barbara Parfitt stated that women are disadvantaged in countries in South and Central Asia, which reduces their employment opportunities and has an effect on nursing. Nursing is a low-status profession, she explained, with low salaries, poor working conditions, and little investment. It is primarily controlled by doctors who make all of the decisions around what nurses do, and in some cases, inhibit the development of nursing. The private sector is variable in standards, innovations, and quality of care, while the government hospitals are overused, poorly resourced, undersupported, and badly managed. Nurses are considered “extra hands” for doctors and are not given much agency. There are few nurses in community health centers, which consist mainly of paramedics and community health workers.
At the same time, the environment is changing rapidly. Prestige is given to educational qualifications, which can help improve the status of nursing and of women. Younger nurses are more business and leadership oriented; if given the proper support, they could be transformational in the health system. The government is issuing new policies toward the goal of improving nursing care, but sometimes the top-down process is slow and difficult to implement.
Parfitt described another approach to improving nursing care through the private sector. She and her colleagues have helped develop a private nursing college, the Grameen Caledonian College of Nursing in Dhaka, Bangladesh, with a 3-year joint diploma in nursing and midwifery in collaboration with the government; it has government approval and uses the government curriculum. The faculty at the college in Bangladesh were mentored and trained by faculty at Glasgow Caledonian University, resulting in a much higher standard of nurse educator. The students not only learn the curriculum in a high-quality educational environment, but are also empowered with entrepreneurial, leadership, and technical skills to become change agents in the health system. The college also continues to mentor and support students after graduation. She explained that the evaluation of the program will focus on four key questions:
- Is the program improving the poverty levels of the students and their families?
- Is it improving their health and families’ health?
- Are young women being developed as skilled nurses at the highest evidence-based international standards?
- Are the students demonstrating leadership skills and empowerment?
________________
3 This section summarizes information presented by Barbara Parfitt, Glasgow Caledonian University.
Parfitt also emphasized that the program is not a charity, but a social business that pays at market rates and does not have shareholders. Thus, it required funds for start-up in the form of loans for both the business and the students’ tuition; this means that students would pay fees, and at 500 students, the college would be self-sustainable. Once the success of the program has been demonstrated, she and her colleagues plan to scale up to 10 more colleges in Bangladesh.
When asked how the program ensures that graduates remain in their communities working, Parfitt underscored that she did not believe empowerment programs should restrict opportunities. She felt that if students want to emigrate, it should be their decision. She also noted that nurses who emigrate to work in other countries often return to their home countries. In interviews with students applying to the program, she discovered that many of the students have a strong tie to their communities and prefer to remain and work toward their improvement.
In addressing tension that arises within the traditional doctor community in response to this changing role of nurses, Parfitt explained that she invites doctors to join workshops with the nurses so they can see the program in action. She also pointed out that the program requires cooperation with the hospitals so they can place the nurses in those settings for their clinical training; as a result, the program leaders meet directly with doctors to help them see the value of their program and to ask for their help to place their nurses.
In closing, Parfitt discussed strategies for integrating nursing care into community health that included training and supervising community health workers. Some of the nurses spend a few weeks in community-based primary care for their clinical rotations. The trainees partner with groups developing “clinics in a box” (also known as “shipping container clinics”) that provide basic health services to people located in rural villages. Parfitt explained that she plans to install a community health clinic staffed by students at Grameen Caledonian College in Dhaka to serve the nearby population living in informal urban settlements. This will provide nursing students more immediate experience in community health that will help develop their clinical skills in hospital settings.
REFERENCES
Finlayson, K., and S. Downe. 2013. Why do women not use antenatal services in low- and middle-income countries? A meta-synthesis of qualitative studies. PLoS Medicine 10(1):e1001373.
Renfrew, M. J., A. McFadden, M. H. Bastos, J. Campbell, A. A. Channon, N. F. Cheung, D. R. Silva, S. Downe, H. P. Kennedy, A. Malata, F. McCormick, L. Wick, and E. Declercq. 2014. Midwifery and quality care: Findings from a new evidence-informed framework for maternal and newborn care. Lancet 384(9948):1129-1145.
Sandall, J., H. Soltani, S. Gates, A. Shennan, and D. Devane. 2013. Midwife-led continuity models versus other models of care for childbearing women. Cochrane Database Systematic Review 8:Cd004667.
UNFPA (United Nations Population Fund), ICM (International Confederation of Midwives), and WHO (World Health Organization). 2014. The state of the world’s midwifery 2014: A universal pathway. A woman’s right to health. United Nations Publications.
WHO. 2002. WHO antenatal care randomized trial: Manual for the implementation of the new model. Geneva, Switzerland: WHO.










