
2
Overview of the Key Issues Involved in Informed Consent
The workshop’s first panel provided an overview of why informed consent is important and reviewed some of the best practices for obtaining informed consent. Jeremy Sugarman, the Harvey M. Meyerhoff Professor of Bioethics and Medicine and deputy director for medicine of the Berman Institute of Bioethics at Johns Hopkins University, spoke about the ethical imperative to gain informed consent from patients and research participants. Linda Aldoory, Endowed Chair and Director of the Herschel S. Horowitz Center for Health Literacy and associate professor in behavioral and community health at the University of Maryland, College Park, discussed a commissioned paper reviewing the impact of informed consent regulations on health-literate communications that she and her team wrote for the roundtable (Aldoory et al., 2014). An open discussion followed the two presentations.
INFORMED CONSENT: WHY DO WE CARE?1
Jeremy Sugarman Johns Hopkins University
Though informed consent procedures for medical treatment and research evolved separately, today they use similar processes, said Jeremy
_____________
1 This section is based on the presentation by Jeremy Sugarman, the Harvey M. Meyerhoff Professor of Bioethics and Medicine at Johns Hopkins University, and the statements are not endorsed or verified by the IOM.
Sugarman. For medical treatment, informed consent evolved largely through patient litigation. “Doctors did things to patients without their permission, and litigation resulted in a series of court cases which then led to legislation and regulation regarding the need for consent,” he explained. For research, early consent practices evolved because investigators thought that it was important to inform human subjects who were normal volunteers about potential risks of participating in research. Various scandals involving human research—the Tuskegee Syphilis Study perhaps being the most infamous example—triggered more formal efforts to strengthen and codify informed consent regulations.
Treatment-associated informed consent owes its origins to a case from the turn of the 20th century that involved a patient in New York with a large abdominal mass, Sugarman said. The state of the art at that time was to palpate the mass while the patient was under anesthesia, which relaxes the abdominal and pelvic musculature, to determine whether the mass was a tumor. This exam revealed the likely presence of fibroids. Because the patient was asleep, the physicians decided to remove the fibroids, a benign tumor, along with the woman’s uterus. As Sugarman explained, the patient was distressed on learning what had happened, and she sued the doctors. In a ruling issued in 1914, Justice Benjamin Cordozo, then sitting on the New York Court of Appeals, wrote, “Every human being of adult years and sound mind has a right to determine what shall be done with his own body; and a surgeon who performs an operation without his patient’s consent commits an assault for which he is liable in damages. This is true except in cases of emergency where the patient is unconscious and where it is necessary to operate before consent can be obtained.”
This statement began a cascade of court cases that formed the basis for informed consent relating to medical treatment, and every state has since passed laws requiring consent for medical practice. “Whenever the medical profession was not good about particular features of consent, when things were risky or scary, legislatures jumped in to provide additional rules and regulations,” said Sugarman. Until recently, for example, every state had a separate consent regulation for HIV counseling and testing, and almost every state has statutes regarding consent for abortion. Several states have regulations specific to electroconvulsive therapy.
Research-related informed consent originated, Sugarman explained, when researchers realized that if they were doing research with volunteers, they needed to get consent. A famous early instance of researchers deciding consent was necessary involved Walter Reed’s experiments proving that yellow fever was transmitted by mosquitoes. These experiments, conducted in 1906 in Cuba following the Spanish-American War, required that healthy volunteers be exposed to mosquitoes that had bitten someone with yellow fever. Before doing so, Reed obtained written consent in English and
Spanish and witnessed by two witnesses. “There were no rules. He just thought it was the appropriate way to go,” explained Sugarman. Consent was not perfect—compensation for participating in the study was excessive and volunteers were not allowed to withdraw from the study once they gave consent—but the notion of getting consent was in place.
Sugarman then discussed a conceptual model of consent developed by Ruth Faden and Tom Beauchamp (Faden and Beauchamp, 1986) that spells out what he characterized as the two senses of informed consent: autonomous authorization and the social rules of consent. Autonomous authorization, he explained, addresses the ethical principle of respect for persons or autonomy, the right to liberty or the right to be left alone that is one of the founding principles of the nation and that is embedded in multiple court decisions. “This notion of liberty—the right to be left alone—is really central to who we are,” said Sugarman. “This idea about being left alone is really critical to justifying what it means to make our own decisions and to give consent for research or in the health care setting. It is a powerful construct.” Although the exact specification of this construct can differ culturally—different cultures around the world have their own sense of acceptable social distance and personal space—all cultures have notions of what it means to be respected, to be left alone, and to have the right to liberty. The social rules of consent, he explained, relate for example to consent of minors, the use of special forms, and the need for witnesses to consent.
The rules for consent can be confusing, Sugarman acknowledged, but the regulatory details are there to remind physicians and researchers to do a thorough job. “In and of themselves, [the rules] are inherently not interesting,” said Sugarman. “They are there in large part to serve as a reminder to meet the ethical goal.” However, he added, “the conceptual models for consent do not quite capture all of the things that happen in the informed consent process and why we ought to care.” There are other considerations, for example, such as whether a patient knows something about herself or himself that can change a side-effect profile. “They may know that if any pill makes them nauseous at all, they are not going to take it,” he said, or a research subject might have a moral objection to the use of a human embryonic stem cell line as a therapy for their illness. Individuals may be concerned about group harms or the distribution of benefits, and they may worry about transparency. “These are welfare considerations that go beyond our typical evidence base regarding consent,” he explained.
Another important consideration he discussed involves the notion of trust. “We know that trust is central to participation in research. If we don’t create a trustworthy system, we are not going to engage enough people in research,” said Sugarman. “Unfortunately, consent has been the place
where all of this is taking place, and none of the federal regulations are going to capture this.”
Some of these challenges associated with obtaining informed consent are related to literacy, and others are not, he said, and associating literacy concerns with those aspects that are unrelated to literacy may be a poor use of resources. “Not everything is about understanding. Part of it is about these other features,” he said.
Turning to the actual process of informed consent—what needs to be done in practice to meet the ethical goals of consent—Sugarman said that informed consent is largely, though not completely, a cognitive task. “We think of it as a cognitive task, but sometimes when we are obtaining consent, people have already made a decision to participate in medical care or research. Other times you are enticing people in the process of getting consent to participate or to do something you believe is in their interest or in the interest of a researcher,” he explained. Regardless, there is a large cognitive element to informed consent, which means that individuals need to have decision-making capacity or competency, and that, in turn, can be influenced by factors such as whether an individual is using a psychoactive substance and the nature of that substance. An individual on an antidepressant medication, for example, may be in a better position to make an informed decision, whereas the first-time crack cocaine user is not. The critical factor, said Sugarman, is whether a particular individual is able to take in, process, and use new information. “You have to be able to make a choice and express that choice,” he said.
In some instances, said Sugarman, patients may know more or think they know more than their doctors or the person obtaining consent because of research they have done prior to the consent process. “It is not always information giving—sometimes it’s information correcting,” he said. The consent process is not all about intelligence, either, and he used the example of Dustin Hoffman’s character in the movie Rain Man, who was intelligent and could take in information, but who could not make a responsible choice.
An important threshold for consent is that an individual has to be positioned to make a voluntary choice. Without decision-making capacity, he noted, a person is not positioned to make a voluntary choice. As an example, he used the situation of a person about to have surgery who is asked to sign consent forms in the preoperative waiting area. The patient already has his arms secured because he has intravenous lines connected to both arms, and a research assistant comes in and explains that the anesthesiologist, whom the patient has not yet met, is conducting a study and would like enroll the patient in that study. Sugarman noted that none of the federal regulations prohibit approaching people who are “naked, cold, scared, and about to have surgery,” yet he was worried about why consent
was not done when the patient was dressed and in a more reassuring environment, one that would not have the effect of impairing voluntariness.
Once this voluntary threshold is achieved, existing federal rules are good about spelling out the type of information that the potential research participant needs to make an informed decision. That information includes details about what is going to happen; the risks, benefits, alternatives, and procedures to be followed; who to call if something goes wrong or whom to call for information about rights and interests; and confidentiality provisions. The trick, though, is to provide that information in a way that is understandable.
Sugarman noted that he and his colleagues have done some empirical work for the White House Advisory Commission on Human Radiation Experiments and found that the very terms used to describe the research process have different denotative and connotative meanings to the people involved. The word “experiment,” for example, implies something risky and scary. The word “study” had the complete opposite connotation—that the physician was going to study up on the patient and his or her disease. He added that being able to describe the research process to an individual is just as important as being able to explain all of the relevant medical terms. “Is this a survey? Or is this trial a first in human study of a drug that has never been tested, and we don’t know what is going to happen? Those are very different things and very nuanced differences that matter completely in peoples’ understanding of what is going on. In order for informed consent to be obtained, you have got to give information in a way that is understandable,” said Sugarman.
The final step in the consent process is to give the individuals the consent document for them to examine. Giving the consent document to the patient can accomplish two things. First, handing this document to the patient gives them the opportunity to read it independently or to have it read to them. Second, it allows the patient use it later and to look up all of things they might have been afraid to ask at the time of consent and to use it as a reference source. “So the documents themselves are doing things besides being the be-all and end-all in giving information,” said Sugarman. He concluded his presentation with the comment that “respect for persons is manifest in the expectations of a meaningful informed consent process. We ought to care about consent.”
BEST PRACTICES AND NEW MODELS OF HEALTH LITERACY FOR INFORMED CONSENT2
Linda Aldoory
University of Maryland
The challenge to create informed consent documents that are understandable by the average patient or potential research subject is not a new one, said Linda Aldoory, citing several papers from as early as 1972 (Ingelfinger, 1972) to as recently as 2010 (Fernandez, 2010). “The body of knowledge on informed consent and health literacy is actually quite massive,” she said, noting that in much of this literature, the authors struggle to create more understandable documents for the purposes of informed consent within the constraints of federal regulations. “Federal regulations often interfere with our ability to create health-literate informed consent,” added Aldoory.
However, upon conducting a systematic literature review of more than 100 studies, government reports, videos, toolkits, websites, and presentations, along with several in-depth interviews with experts in the field, Aldoory’s team identified a set of best practices and lessons learned as well as gaps that can serve as a research agenda going forward. Aldoory’s team also created two models of health-literate informed consent that they detailed in the commissioned paper (Aldoory et al., 2014).
The literature review spotted a number of trends in informed consent procedures and health literacy. Approaches today are more patient centered, are more likely to enable empowered and active decision making, and are increasingly emphasizing meaningful consent as opposed to or in addition to completion of an informed consent form, Aldoory said. Over the past decade in particular, researchers are using technology to streamline the informed consent process and improve understanding. As an example of how technology is being used to improve the health literacy of the informed consent process, though not necessarily as a best practice, Aldoory cited the Enroll system developed by Mytrus. This interactive electronic informed consent learning tool measures an individual’s understanding of the risks and benefits of participation while delivering the necessary information to obtain informed consent.
Aldoory said that the commissioned paper summarizes 30 of the top best practices (see Appendix C for the complete list), and she described sev-
_____________
2 This section is based on the presentation by Linda Aldoory, Endowed Chair and Director of the Herschel S. Horowitz Center for Health Literacy and associate professor in behavioral and community health at the University of Maryland, College Park, and the statements are not endorsed or verified by the IOM.
eral of them, noting in the process that these best practices are supported by findings from earlier decades. Best practices today recognize the importance of time, and she referred to the example that Sugarman gave about seeking consent earlier than the last minute before treatment is about to begin. She noted that research suggests that the longer the time that patients or participants have to consider the informed consent documents and ask questions, the better prepared they are to make a decision when they begin treatment or enrollment in a research study. In the best cases, patients or participants receive documents and information a week or two ahead of time.
Many researchers today are considering the level of risk involved in a clinical trial or therapy when they decide how much information to put into the informed consent document, Aldoory said. Instead of following the federal regulations to the letter and putting all necessary information into informed consent documents when the risk is minimal, they are looking at what information is needed by patients or participants to make an informed, meaningful decision. As an example, Aldoory cited what she characterized as a wonderful template for informed consent forms for minimal risk research developed by the Agency for Healthcare Research and Quality (AHRQ).
Aldoory explained that best practices today also view other individuals as part of the decision-making process and, in particular, consider cultural and language differences. In many cultures, it is common for people to bring their family members or other important individuals with them and to make decisions as a family or group. Accounting for this type of group decision-making process can improve the informed consent process.
Best practices check to make sure that informed consent documents are written at or below an eighth-grade reading level—research has shown repeatedly that documents are often written at more than a high school reading level, Aldoory explained—and they use teach-back and teach-to-goal techniques to increase understanding of the information in these documents. Not only do best practices involve asking patients to recite what they learned or how they are interpreting information, but they do that continually through the consent process until the patient or participant understands each piece of the informed consent procedure.
One example of a best practice in clinical research that Aldoory and her colleagues learned about during an interview brings potential participants together in groups and uses a combination of interactive PowerPoint presentations on informed consent and group discussions to increase understanding before each participant consents individually. This approach greatly reduced study dropout rates, Aldoory noted. She added that there are comprehensive toolkits, other resources, and templates for informed consent available on the Web from AHRQ, the National Cancer Institute
(NCI), the Food and Drug Administration (FDA), and various nonprofit organizations.
Multimedia and online approaches to improve informed consent in both treatment and research settings have been an area of focus over the past decade, but the findings on the effectiveness of these methods have been mixed, said Aldoory (see Figure 2-1). On the pro side, authors have found that the approaches using Internet-based interactive tools, as well as video and audio, create a more user-centered environment where the participant has more control over the situation. Researchers have also found that these approaches offer more consistency across the different individuals in the study and that they lower anxiety among participants. Multimedia and online approaches have the advantages of allowing for an audit trail and reducing staff time and costs.
There are mixed findings on the efficacy of these methods, however, and every situation is different and must take into account different factors, such as low health literacy. Aldoory said that research on low health literacy has not yet found solid evidence that alternative formats beyond verbal and written communications have been effective and that, further-
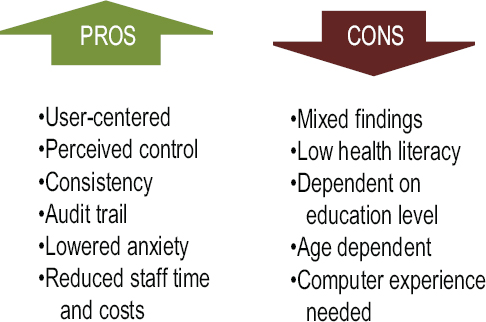
FIGURE 2-1 Pros and cons of the effectiveness of multimedia and online approaches.
SOURCE: Aldoory et al., 2014.
more, the effectiveness of these alternative formats depends on education level, age, and computer experience. “Some researchers have suggested that in the absence of consistent findings, the format to use should depend on the level of risk in the study,” said Aldoory. “If it is minimal risk, you may be able to use different formats that are appropriate for the audience. If it is high risk, you may need to combine written and oral with multimedia.”
Turning to the subject of the two models that she and her colleagues developed after completing their review and expert interviews, Aldoory said that she views these as prototypes that will require dialogue, revision, and empirical testing to show that they work beyond the context of their review. These two models, she explained, are based on the universal precautions approach to health literacy and a situational communication framework that is context dependent. The models also fill some of the gaps in research that they identified.
The first model, which assumes that the target participants have low health literacy, uses a roadmap to health-literate informed consent and is a step-by-step visualization of the sequential order of larger process phases to complete in order to reach patient understanding regardless of the level of health literacy (see Figure 2-2). Each step in the roadmap builds on the one before it and embeds the best practices identified during the review and interview process.
The first step, Aldoory explained, is to know the setting and risks, which includes understanding practitioner characteristics such as training of the people who are giving informed consent. The second step is staff training on both study details and informed consent. The third step is to understand the participants’ cultural differences, literacy differences, ages, and technological skills and to use that understanding in the fourth step, which is to simplify written forms. Step five considers alternative formats, including multimedia and computer-based forms, and step six involves dialogue. “We have found that verbal exchange is still core to increasing understanding and informed decision making among participants and patients,” said Aldoory. The seventh step involves assessing comprehension using teach-back and teach-to-goal methods, and the eighth and final step is to assess the system used to improve the entire process.
The second model is a situational risk model for communicating informed consent (see Figure 2-3). This model incorporates a more tailored approach to communicating with different audiences based on level of risk in the study and uses the AHRQ template and other templates that are based on minimal risk or high risk. As risk increases, the model adds more information in the informed consent documents, such as additional details on the right to refuse or discontinue participation and on common side effects, alternative treatments, and postsurgery plans.
In closing, Aldoory said that some of the suggestions she and her
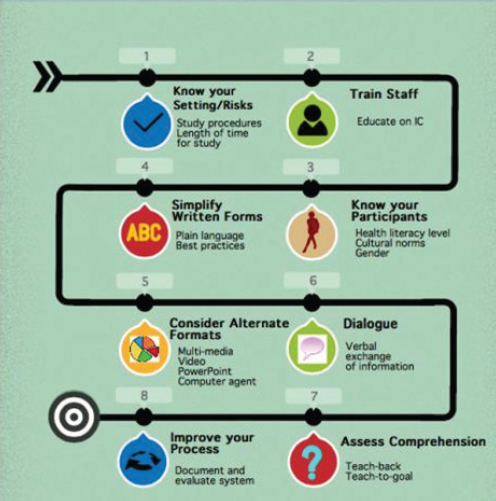
FIGURE 2-2 A roadmap to health-literate informed consent.
NOTE: IC = informed consent.
SOURCE: Aldoory et al., 2014.
colleagues found were simple, such as spending more time meeting with participants and patients and using clear language. Others were more complicated, and as an example she cited one study that developed computer avatars that teach participants about decision making and informed consent. “What was surprising to us was that even with an accumulation of this information, there continue to be barriers to informed consent,” she said. “Authors continue to talk about the restrictive federal guidelines and how challenging it is to reach meaningful informed consent.” She said that her hope is that the commissioned paper and the discussions at this workshop
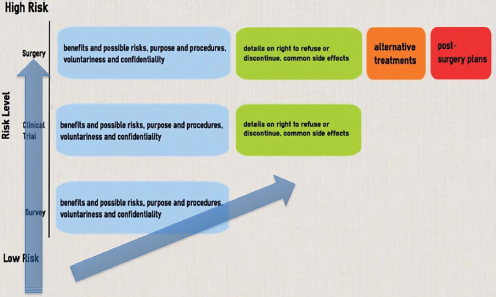
FIGURE 2-3 Situation risk model for communicating informed consent.
SOURCE: Aldoory et al., 2014.
would increase meaningful dialogue about these barriers and identify ways to improve health-literate communication during the informed consent process.
Cindy Brach, senior health policy researcher with AHRQ and a roundtable member, started the discussion by saying that she has been working on moving from the AHRQ toolkit for informed consent and authorization for minimal-risk research to a set of trainings for hospital staff or for clinical practice and that she has been getting bogged down in some of the practicalities to make this transition. Brach remarked, for example, that patients being prepared for surgery often have questions about anesthesia when talking to the surgeon during the informed consent process but that the surgeon then refers those questions to the anesthesiologist, whom the patient has yet to meet. She then asked Sugarman if he had any ideas on how this process could work better. He replied that Brach had identified a structural problem that exists in many health care organizations and that these organizations are trying to address this problem as part of the need to increase the efficiency of the health delivery system. Some health systems, such as Johns Hopkins, have created preoperative clinics at which patients can meet with an anesthesiologist in advance of surgery.
Sugarman noted that unexpected illnesses can also present a challenge. “I see patients on Tuesdays, but not all my patients get sick on Tuesdays,” he said. “If they come in on a different day, there is going to be a different process. Not all of health care can be planned.” He added that when structural issues act as barriers to informed consent, the goal should be to fix those problems rather than trying to correct them by changing the consent process at the end.
Ruth Parker, professor of medicine, pediatrics, and public health at Emory University School of Medicine and roundtable member, asked the panelists if they had any ideas on how to handle potential conflicts of interest in the consent process, and she cited the use of new technologies as something that could be perceived by some as a conflict of interest. Sugarman based his reply in part on the results of the Conflict of Interest Notification Study he and his colleagues conducted with funding from the National Institutes of Health (NIH) (Weinfurt et al., 2009). The issue they studied was that, although every IRB wanted investigators to disclose potential conflicts of interest as a first step, it was unclear who on a research team should disclose, when and how disclosure should occur, and what the impact of disclosure would be on the research enterprise and potential participants. The bottom line, said Sugarman, was that most people do not care about most financial interests in research in spite of the attention that is brought to this issue. “If an investigator is paid by a company to do research, if there is a per capita payment, the general public understands that money changes hands to do different kinds of research,” he said. What people do care about is equity interest in research. “The fact that researchers stand to gain financially depending upon how the investigator physician interprets things matters to people.” Sugarman and his colleagues have since developed template language that can be used to accurately describe certain financial interests in research. He also noted that discussions about conflict of interest are sometimes about conflict of obligation between the integrity of the research process versus the obligation to the patient and not a conflict of interest per se.
In terms of whether a particular technology would be viewed by the consumer as a conflict of interest, Sugarman said he did not know the answer of how to address conflict of interest. “That’s an empirical question that needs to be asked,” he said. Sugarman went on to describe that he and his colleague Philip Lavori put together the Brief Informed Consent Evaluation Protocol, which serves as a tool for measuring the quality of the informed consent process independent of the experience of a research participant (Sugarman et al., 2005). This protocol involves having the participant call a phone bank immediately after obtaining informed consent and going through a process that maps to Faden and Beauchamp’s conceptual model he had discussed in his presentation. In a site-randomized clinical
trial involving some 800 patients at 30 sites, Sugarman and his colleagues tested a checklist and found that although every research coordinator involved in the study liked the idea of a checklist to improve informed consent, the data showed that a checklist did not improve the consent process and that there is room for improvement in the informed consent process of research (Lavori, 2007).
Aldoory added that research supports Sugarman’s answers and that it also shows that too much information has been found to be negatively associated with participation. “If you give too much, it actually increases confusion, and it makes people not want to participate in trials and makes them more nervous,” she said. “Sometimes the conflict-of-interest information comes in at a level of too much information if it is beyond what they really need to know.”
In a general comment to the two panelists, Kim Parson, strategic consultant in the Corporate Consumer Experience Center of Excellence at Humana, stressed the importance of engaging actual consumers and doing human-centered design when plotting these different efforts. Parson commented that it is important to vet these different models iteratively in real time and even co-create them with consumers. Sugarman agreed that such testing is important when the risk profile of the research matters but that there are other types of research where it would not matter as much. As an example, he discussed the vaginal microbicide trials that were conducted among sex workers in Africa to test the prevention of HIV transmission. “The stakes were enormous, and we made sure that we did really careful formative research to figure out how we could communicate to people who had less than 4 or 5 years of education in a six-arm randomized trial of different gels,” said Sugarman. In the end, they used a 15-page consent document that had three sentences and pictures per page, and they used two dice to explain randomization. With two or three rolls of the dice, people without education could understand randomization.
In response to a question from roundtable member Wilma Alvarado-Little, director for community engagement/outreach at the University at Albany’s Center for the Elimination of Minority Health Disparities, about whether adolescents are considered to have their own culture, Aldoory said that she did not find any studies where adolescence was considered a cultural difference. “There were cultural differences in terms of older adults,” Aldoory noted. She added that in terms of accommodations for the visually impaired, which Alvarado-Little also asked about, a few studies looked at visual impairment and other situations, such as patients with schizophrenia. The findings in those cases tended to show that one-to-one oral communication seems to be the best way to communicate. Oral communication, she noted, allows people to ask questions more easily and to question information that is not clear. In addition, it allows the person doing the consent
process to use nonverbal clues to judge whether the individual understands the consent process. “That really seemed to increase comprehension more than the other modalities,” said Aldoory.
Robert Logan, communications research scientist at the National Library of Medicine, asked Aldoory to discuss some of the major gaps in research that she uncovered. One significant gap, Aldoory replied, was the lack of visual models of any kind that used infographics or sequential ordering to help people who might be at the beginning stages of understanding informed consent. Researchers may have years of experience with the informed consent process, whereas people involved in a clinical trial may be doing so for the first time or may not have the expertise to know what they are doing, she explained. Another gap was that there has been little work done on the role of situational factors such as risk levels and how they affect informed consent. “We found many essays and conclusions from studies that said risk level is probably a dependent factor on how much we should communicate, but we haven’t found any empirical studies looking at those factors and their effects,” said Aldoory.
She also reiterated her earlier statement that research on new technologies and multimedia approaches has largely generated mixed results and that more work is needed to understand why that is true. There has also been little research on low-health-literate populations, and there is a dearth of studies on developing models for informed consent in community-based research studies.
Benard Dreyer, professor of pediatrics at the New York University Langone Medical Center and a roundtable member, asked the panelists to comment on the issue of providing too much information in the treatment setting, as opposed to the research setting. As an example, he noted that in his career he has seen three children die during tonsillectomies, mostly from anesthesia reaction, and he wondered whether it was necessary to mention the risk of death from anesthesia, a real but nonetheless rare risk, when obtaining consent from patients for the tonsillectomy. “From the ethical point of view and maybe from the practical point of view, how does one make a decision to throw yourself back from the ledge of too much information?” he asked. Sugarman replied that the issue of understanding the disutility of information is a challenging one because each individual has a different tolerance or desire for ever more information. “The bottom line is the big things matter to most people. Death matters to most people, and major risks are things that need to be on the table,” said Sugarman. “People have talked about the idea of drilling down into more and more information and making information available to people if they want to hear more and coming up with a bulleted list of main items, with additional information put behind them.” Sugarman also said that different risks are
important to different people. A musician, for example, might be very interested in even small risks for ototoxicity or peripheral neuropathy.
Sugarman noted in this regard that informed consent documents for HIV prevention trials funded by the NIH are “ridiculously long—they are 20 or 30 pages—it can take a day for people to go through the consent document,” he said, adding that individuals are getting little usable information from these documents. He and his colleagues are trying to determine how to shorten these documents, and they are running up against institutional constraints. His team is asking all of the stakeholders in the process to identify what could be successfully eliminated from the consent form and why, and then see if they can reach a consensus as to what is really needed in these forms.
Aldoory added that the research she reviewed showed the importance of giving people time to assimilate risks prior to surgery. When giving consent in the minutes before surgery, patients may have some vague idea of risk and benefit, but at that point they have little choice, which increases their fear. Another problem is that people often come into the clinic full of misinformation that they gleaned from the Internet, which leads to their giving meaning to information beyond what they are actually hearing from the health professional conducting the consent process.
George Isham, senior advisor at HealthPartners, senior fellow at the HealthPartners Institute for Education and Research, and roundtable chair, asked Aldoory whether the situational risk model applies to everybody or whether there needs to be segmentation of the audience, given that different people have different values about different outcomes. “Is there an ethical question about providing people with different levels of information?” he asked. “Is a one-size-fits-all approach equitable and yet not helpful to a lot of the people? It seems like there is a bit of tension there between different concepts in terms of what you provide the people and yet tailoring the information to what matters to people given their levels of situation and also their level of literacy.” Aldoory said that her team asked themselves those very same questions. “When we wanted to come up with visual models, we wanted to find a way to incorporate both the universal precautions approach and tailored communication approach,” she explained, noting that each of these two philosophies are beneficial in the situation of informed consent. She acknowledged that she does not have answers yet to Isham’s questions but noted that these questions are indeed on the table for study.
Sugarman added that enormous debates in court cases have led to the development of consent processes for the clinical setting. He explained that there are three standards for adequate disclosure of information during the consent process: a professional standard, a reasonable patient standard, and a subjective standard. The professional standard concerns what the aver-
age professional would want to know in a given situation. In the case of tonsillectomies, for example, do most pediatric otolaryngologists describe the risk of death? The courts have leaned toward this standard because, as Sugarman put it, “it is easier to haul in a bunch of professionals in a court setting where there is an allegation of improper consent. That doesn’t mean it is the right way to go, but it is the court doing its business.”
This issue is easier to resolve in the research setting, he said. A phase I first-in-human study is a different situation from a research survey study, for example. He noted that with comparative effectiveness research that uses data that are already going to be acquired in the normal course of practicing medicine in the health care setting, there is the question of why there is even the need for consent, given that there is no incremental burden or risk to the patient. “There is a bit of push-back now against always building up consent to be the most important element,” said Sugarman.
Bernard Rosof, chief executive officer of the Quality in Healthcare Advisory Group and a roundtable member, noted that the complicating impact of federal regulations on the health literacy level of the informed consent document was mentioned frequently in the commissioned paper and asked Aldoory if she could comment more on that with regard to clinical research on community health benefits. She responded that the chief complaint voiced by researchers concerns the volume of information that has to be communicated in the informed consent process. “I do not think that it is anything in terms of structural or behavioral restrictions that the researchers feel,” she said. What she and her colleagues learned in studying the regulations carefully is that many things are actually optional, which is why they developed the situational-risk model. Federal regulations, she explained, state that there is basic information that needs to be conveyed—what the study is about, what the risks are, and a few other factors—but that the regulations are not as restrictive as they are made out to be. She also noted that the paper does list a few best practices that do relate to community-based work, as does the example she discussed about holding group meetings prior to obtaining individual consent
Roundtable member Winston Wong, medical director for Community Benefit and director of Disparities Improvement and Quality Initiatives at Kaiser Permanente, asked how political power factors into the conversations around informed consent, particularly with regard to safety net organizations that may be seeing significant numbers of undocumented individuals who may come in seeking care. Aldoory said that research in this area has not panned out, at least in the context of health literacy, though she noted that there is a much broader body of knowledge around issues of informed consent that do not address health literacy and that were not part of her review. However, this subject did come up in the interviews she and her team conducted, and the interviewees pointed out the importance of tak-
ing time to provide an understanding of the informed consent process long before discussing what the study was about and eventually seeking consent. She added that some interviewees commented on the difficulties they encountered with their IRBs getting approval for using informed consent processes aimed at low-literacy populations. “They became advocates of their populations, but they had to battle the IRB,” said Aldoory.
Sugarman said that he was not aware of any empirical literature on political power and consent but that this highlights the critical issue of voluntariness, one of the understudied areas of the consent process. In a literature review he conducted about 15 years ago, he found that many hypotheses were addressed, and most were about understanding and disclosure, whereas only a handful were about voluntariness (Sugarman, 1999). “If we really want to get to consent, we want to think about voluntariness,” said Sugarman. He did note that in certain circumstances the federal regulations do provide some leeway for waiving the need for a consent document. Roundtable member Laurie Francis, senior director of Clinical Operations and Quality at the Oregon Primary Care Association, remarked that the power differential in society can be an important influence on voluntariness and asked whether there had been any research on that issue. Aldoory replied that most of the research on health literacy and informed consent focused on the literacy end and that there was only one formalized empirical study looking at self-efficacy. Sugarman added that one way of reducing the power differential is to have people other than the doctor or nurse involved in the consent process. However, solving this problem does not get rid of literacy issues.
Brach noted that many of these issues have to do with what Sugarman called the subjective standard for informed consent, which she interpreted as relating to those pieces of information that would make a difference to each individual. Although this standard would be difficult to enforce legally, given the challenge of knowing what specific individuals need to make their decision, it is what the field should be striving for in the consent process. “There is a model out there that says what we should be telling people is what is going to be important for them to make that decision,” said Brach. She also remarked that page length is not a good measure of literacy, as Sugarman’s example of the 15-page form with three sentences per page illustrates. She commented, too, on the use of short and simplified forms to better guide those who are conducting the consent discussion and to ensure that they are in fact communicating all of the important information needed for meaningful informed consent.
Parker asked the two panelists to name one or two areas that are ripe for the roundtable to tackle. Aldoory nominated the use of multimedia and interactive technologies, given the mixed results obtained so far. She said she would like to see more dialogue to tease out the reason for the mixed
results that have been observed so far. Sugarman agreed with Aldoory’s suggestion, saying that gathering good data on these newer approaches is humbling and noting how hard it is to develop these methods and test them. He added that developing health-literate consent documents is about more than just information giving and understanding. “Any model that reduces it prematurely to that simple question is going to fail,” he said. The first step, he said, should be to make a model that reflects this complexity and then generate data before introducing recommendations. “The things that we think about in closed rooms without data can be hazardous and resource intensive,” he remarked.
The final comment in this discussion came from Isham, who asked Sugarman to clarify his statement that financial conflicts of interest do not matter, given the public’s concern about the costs of medical care. Sugarman reiterated that although most patients want to know about financial interests in research they do not care about most of them, but they do care about equity interests. “The question is if it is something that poses a threat to [a patient’s] welfare, then it should matter,” Sugarman said. “I think the dominant paradigm for conflicts of interest is that it is critical to simply disclose them during the consent process, but I think we need to come up with management strategies for conflicts of interest and research rather than rely on the consent process to solve all of the issues with it.” He noted in closing the discussion that his summary paper (Weinfurt, 2009) made reference to language that IRBs and investigators can use to describe different financial interests and that he and his colleagues have used this language with thousands of people. He asked Isham to look at that paper and see whether he saw problems with that language.


















