
11
The Knowledge Exchange Process: From Research into Practice
The success of the preventive intervention research cycle, described in Chapter 10, for a given research program lies only partly in how well it works to expand the knowledge base for prevention. The cycle's ultimate merit—and the justification for the expenditure of large amounts of research monies—lies in how effectively that knowledge can be exchanged among researchers, community practitioners, and policymakers to successfully implement the program in real-life settings and ultimately, with widespread application, to reduce the incidence of mental disorders.
This chapter focuses on the process of exchanging knowledge. The term knowledge exchange has been chosen for this process because it implies two-way communication, including the feedbacks represented by the loop in Figure 10.1. The term dissemination is used when only a one-way flow of information is implied, for example, from researchers to other researchers through publication of a journal article. Therefore, although the role the researchers play, as described in Chapter 10, is critical to the success of knowledge exchange, it is only one part of a more complicated process. The community's role is equally important, not only in how it implements the program and provides feedback, but also in how it goes about gathering the needed information. Policymakers at federal, state, and local levels also have a critical role to play in gathering information to use in setting priorities for research and in supporting standards of excellence.
Researchers and community practitioners come to the knowledge exchange table with very different perspectives and value systems. Most
researchers, by nature, are cautious. They appreciate the complexity of etiology and the diverse pathways in the occurrence of mental disorders and usually are skeptical about unidimensional interventions, which may not generalize across populations diverse in age and culture. They have high standards for the quality of the evidence they believe is needed before practice recommendations can be made. This circumspect approach contributes to slowness in publication of evidence. For example, pilot studies and early field trials often are not published because the researchers believe that doing so might be “premature. ”
Although community practitioners, along with representatives from community organizations, may understand the reasons for caution, they are faced on a daily basis with the need for preventive services, and they often are frustrated by what they perceive as the unwillingness of the researchers to provide direction. The bottom line for practitioners, who often must answer to policymakers in state legislatures and local councils, is straightforward: What works? How long does it take? How much will it cost?
When these questions cannot be answered from the results of completed field trials within the research cycle, or when practitioners have creative ideas for new interventions, they proceed to create their own prevention programs. Currently, this is being done at the federal, state, and local levels of government and by private foundations. Such programs are primarily “service” in nature, although some, including demonstration projects, have evaluation components attached to them. The result is that large expenditures are being made without knowing the effectiveness of these services.
THE ROLE OF THE COMMUNITY
The role of the community—defined here as policymakers, community practitioners, and representatives of host organizations—is complicated and time-consuming. Part of this complexity is due to the very nature of “community,” which can rarely be regarded as a unitary whole. Rather, it is a heterogeneous group of individuals, institutions, and special interest groups, among whom it can be difficult to achieve consensus. The role of the community includes the following functions: defining the problem and assessing the needs, ensuring the readiness of the host organization, selecting a model program, balancing fidelity and adaptability while implementing the program, evaluating the program's effectiveness, and providing feedback to the researchers. Attention to this process is necessary for programmatic planning at federal, state, and local levels of government and with private foundations.
Defining the Problem and Assessing the Needs
When community leaders, pressed by the urgency of local needs, must decide whether to initiate a service program for a particular mental disorder or problem, many factors will influence their decision. These include the degree of community concern about a specific problem, such as substance abuse, compared with concern over other priorities, such as education and police protection; the scarcity of resources for health care, especially mental health care; the availability of an effective model; the safety and cultural relevance of the model; and the availability of local interveners to deliver the program.
The community must define for itself what needs and problems it has and what it wants to accomplish. Initially, a community may be more interested in treatment and maintenance programs than preventive interventions. The timing for the introduction of a prevention program must be right for a community; a program foisted onto a community, even by a local practitioner rather than a researcher, is unlikely to succeed.
Ensuring the Readiness of the Host Organization
If the host organization, such as a service agency, school, church, or city council, has had success in reaching out into its geographic community previously, has developed referral sources, and is respected within its community, it will have a better chance of success. Also, if the bureaucratic structure within the organization has some flexibility regarding its structures for communication, coordination, decision making, and role definition, it will be more able to adapt and implement a prevention program (Price and Lorion, 1989).
Selecting a Model Program
The questions that the community and the host organization will focus on in selecting a particular model program include: Does the program address the needs and problems identified by the community? Is the program really ready for distribution? Has it demonstrated its efficacy and effectiveness? What aspects of the program would have to be adapted to fit the needs of this particular community, such as cultural issues? How much does the program cost, and how long must it continue to achieve positive effects? Is technical assistance available from someone who understands this particular program, such as someone from the original research team?
Criteria to Use in Examining Programs
For a community searching for a model, practicality is paramount. An ideal model that has proved its efficacy and effectiveness through confirmatory, replication, and large-scale field trials is as yet, owing to the status of current prevention research, unlikely to be available. Nevertheless, communities can be guided by the quality of evidence that is available from various prevention programs, some that have been tested in trials and others that have not. The following guidelines regarding a hierarchy of evidence have been adapted from work by the Canadian Task Force on the Periodic Health Examination and the U.S. Preventive Service Task Force (Battista and Fletcher, 1988; Spitzer, 1979).
|
Grade I: |
Evidence obtained from multiple randomized controlled trials (confirmatory and replication trials and large-scale field trials). |
|
Grade II: |
Evidence obtained from multiple randomized controlled trials (confirmatory and replication trials but no large-scale field trial). |
|
Grade III: |
Evidence obtained from at least one properly randomized controlled trial. |
|
Grade IV: |
Evidence obtained from well-designed controlled trials without randomization. |
|
Grade V: |
Evidence obtained from well-designed cohort or case-control studies, preferably more than one. |
|
Grade VI: |
Evidence obtained from multiple time series studies with or without the intervention. Dramatic results in uncontrolled experiments (such as the results of the introduction of penicillin in the 1940s) could constitute this type of evidence. |
|
Grade VII: |
Evidence suggested by respected authorities, based on clinical experience, descriptive studies, prior service delivery programs, or reports by expert committees. |
A community can use the criteria listed in Chapter 7 to assess the quality of preventive intervention research programs. It can also use the forward-looking methodologies presented in Chapter 10 to guide its selection of a program. By making opinion subordinate to evidence and by searching for the highest level of evidence available, the community, in its program selection, increases the likelihood that its efforts will be successful.
Information Sources to Use in Examining Programs
Throughout the preventive intervention research cycle, there can be information and data ready to be exchanged with community practitioners and policymakers for general use. There are five main routes by which research findings are commonly disseminated: academic journals and books, manuals, clearinghouses, professional conferences, and direct working relationships between researchers and communities to facilitate implementation of the prevention programs. When a research program is being reviewed by a community, published papers and manuals should be obtained from libraries, clearinghouses, or the researchers themselves.
The committee reviewed the amount of knowledge dissemination currently available for examination by community practitioners and policymakers, as well as by other researchers. A description of this review process and the findings follows.
Research Publications. Peer-reviewed journal publication is the usual method of dissemination in all scientific fields, but it does entail a time lag between establishment of the data, the acceptance of the paper, and the distribution of the journal. In addition, many of these journals can be difficult for nonresearchers to locate.
The first step in the committee's review was to determine how large the prevention literature related to mental disorders was; then it could determine what portion of this was based on research. The following sources of information were used:
-
MEDLINE searches.
-
Computer Retrieval of Information on Scientific Projects (CRISP) files from 1988 through 1992 on research grants that identified prevention of mental disorder, alcoholism, or drug addiction as one of the main areas of emphasis. These files included grants from all three of the former ADAMHA research institutes—National Institute of Mental Health (NIMH), National Institute of Drug Abuse (NIDA), and National Institute of Alcoholism and Alcohol Abuse (NIAAA)—as well as other National Institutes of Health research institutes and the former Office of Substance Abuse Prevention (OSAP).
-
Lists of research grants from the Prevention Research Branches of NIMH, NIDA, and NIAAA.
-
Personal inquiries to NIMH Preventive Intervention Research Center (PIRC) directors as well as researchers of numerous “illustrative programs” identified by the research institutes, service agencies, private foundations, and many other sources.
-
An annotated bibliography prepared under contract for NIMH. In 1991, NIMH contracted to compile an annotated bibliography of published work in the field of primary prevention in mental health (Trickett, Dahiyat, and Selby, in press). This compendium was a follow-up of an earlier bibliography that covered materials on primary prevention in mental health through early 1983 (Buckner, Trickett, and Corse, 1985). Because the field of prevention continues to have multiple definitions of its scope and boundaries, the editors' decisions as to what to include in both bibliographies were, by necessity, arbitrary. The second bibliography focused on published materials from later 1983 through mid-1991. It emphasized primary prevention, but where the boundaries between primary and secondary prevention were not clear, publications were included. A broad definition of primary prevention was used, including the concept of risk, prevention of specific disorders, enhancement of specific competences, empowerment, early intervention, and biosocial approaches to development. Although the main emphasis was on preventive interventions, articles were included if they had direct implications for preventive interventions or provided a conceptual perspective that was “heuristically rich. ” The data bases used for the search included PsycINFO, MEDLINE, SOCIOFILE, ERIC, and AIDS at the National Library of Medicine. The search also included journals that were identified as specifically representing the field, volumes emanating from primary prevention conferences, and information derived directly from NIMH Prevention Research Branch (PRB) researchers and the NIMH Panel on Biosocial Approaches.
In summary, the editors noted that, compared with the 1985 annotated bibliography, the second bibliography reflected how “the boundaries of primary prevention are stretching both in a biosocial direction on the one hand, and in an empowerment direction on the other” (Trickett et al., in press).
The committee analyzed the second bibliography and treated it as a main source for locating literature on prevention. Although it was not an all-encompassing source of available and/or relevant literature, and did not use the definitions of prevention and prevention research that the committee adopted (see Chapter 2), it was the most complete annotated bibliography dealing with prevention of mental disorders available.
The committee's findings are as follows. The bibliography has 1,326 entries, with 1,990 authors. These entries include journal articles, books, chapters, and monographs. For the committee's purposes, 109 of these entries were excluded from analysis because they centered on AIDS, a topic outside the committee's purview. Of the remaining references, 808
were journal articles, which included theoretical papers; findings from risk studies; descriptions of methodologies; descriptions of prevention programs, some with evaluation components; results from quasi-experimental research studies; and findings from approximately 25 preventive intervention research programs that, according to the abstracts, had used randomized controlled trial designs. These 808 articles were published in 224 journals. (This wide array of journals publishing prevention articles related to mental disorders from 1983 to 1991, compiled by using only the NIMH prevention bibliography as the source, can be found in Appendix E.) More than half of these 224 journals published only one prevention article. Many prestigious academic journals have published few or no prevention papers related to mental disorders. Notably absent from representation in the bibliography or publishing only one article were journals such as The New England Journal of Medicine, Nature, Lancet, British Journal of Medicine, and Science.
Table 11.1 lists the journals that have published the most prevention articles. The editors of the bibliography identified Prevention in Human Services and the Journal of Primary Prevention as the two journals that specifically represent this field, and indeed they may be because they have the most publications, 92 and 82, respectively, accounting for approximately 22 percent of the 808 journal articles. Unfortunately, these journals are not readily accessible, nor is their existence common knowledge. During the committee 's work, the Journal of Primary Prevention was not easy to locate, even in the academic libraries in the Washington, D.C., area. It is not indexed in MEDLINE, nor is it available at the National Library of Medicine (NLM) or the NIH library. Prevention in Human Services is indexed and can be found at the NLM but not at the NIH library. The limited library circulation of these two journals make them essentially unavailable except by individual subscription.
During the course of its work, the committee compiled approximately 2,000 references. This data base, quite different from the NIMH prevention bibliography, is available as part of the background materials (available as indicated in Appendix D).
The committee next wanted to determine, in general, how many publications had been made available from funded research programs related to prevention of mental disorders. To do this, a cross-referencing of research projects and published work was done for one representative funding agency. The committee used NIMH as the example and cross-referenced NIMH-funded principal investigators with the bibliography prepared for NIMH. This check did not necessarily reveal that the investigators had published findings from NIMH-supported research,
TABLE 11.1 Journals Cited Most Often in NIMH Prevention Bibliography, 1983 to 1991
|
Number of Articles |
|
|
Prevention in Human Services |
92 |
|
Journal of Primary Prevention |
82 |
|
American Journal of Community Psychology |
49 |
|
Journal of Preventive Psychiatry and Allied Disciplines |
25 |
|
Journal of Drug Education |
24 |
|
Personnel and Guidance Journal |
23 |
|
American Journal of Orthopsychiatry |
19 |
|
American Psychologist |
18 |
|
Child Abuse and Neglect: The International Journal |
18 |
|
Journal of Consulting and Clinical Psychology |
18 |
|
Journal of School Health |
15 |
|
Journal of Community Psychology |
13 |
|
Community Mental Health Journal |
10 |
|
Infant Mental Health Journal |
10 |
|
School Psychology Review |
10 |
|
Journal of the American Academy of Child and Adolescent Psychiatry |
8 |
|
International Journal of the Addictions |
7 |
|
Public Health Reports |
7 |
|
Social Science and Medicine |
7 |
|
Acta Psychiatrica Scandinavica |
6 |
|
American Journal of Psychiatry |
6 |
|
Health Psychology |
6 |
|
Journal of Behavioral Medicine |
6 |
|
Journal of Drug Issues |
6 |
|
Journal of Studies on Alcohol |
6 |
only that they had written and published material on prevention. Of the 112 grantees funded by the NIMH PRB from FY 1985 through FY 1991, 43 had entries in the bibliography. The entries totaled 168, but one researcher accounted for 28 of these. Many NIMH PRB researchers, including those whose projects are completed, have never published their findings in peer-reviewed academic journals; others have written book chapters that contain some data.
At the request of the committee, each NIMH PIRC director prepared a list of publications generated directly from support of the PIRCs. Table 11.2 shows the number and type of publications from the six centers and the number of years the centers have been funded (one center is no longer in existence). These publications were mostly in the areas of theory, methodology, and risk, but some included data from preventive intervention research trials. The publication rates generated from the
TABLE 11.2 Publications from NIMH Preventive Intervention Research Centers (as of August 1993)
|
Type of Publication |
||||||||
|
Years in Operation |
Peer-Reviewed Journal Articles* |
Books* |
Chapters* |
Research Manuals |
Bibliographies |
Manuscripts Submitted |
Total |
|
|
Prevention Research Center, Hahnemann University |
(1983–1987) |
2 |
0 |
3 |
1 |
0 |
0 |
6 |
|
Michigan Prevention Research Center, University of Michigan |
(1983-present) |
26 |
0 |
17 |
17 |
4 |
5 |
69 |
|
Preventive Intervention Research Center for Child Health, Albert Einstein College of Medicine, Montefiore Medical Center |
(1983-present) |
53 |
2 |
37 |
0 |
1 |
10 |
103 |
|
Prevention Research Center, Department of Mental Hygiene, The Johns Hopkins School of Hygiene and Public Health |
(1984-present) |
12 |
1 |
8 |
3 |
0 |
5 |
29 |
|
Program for Prevention Research, Arizona State University |
(1984-present) |
53 |
2 |
15 |
8 |
0 |
12 |
90 |
|
Oregon Social Learning Center, University of Oregon |
(1990-present) |
5 |
0 |
1 |
0 |
0 |
0 |
6 |
|
* Published or in press. |
||||||||
PIRCs have been uneven. It is recognized that many preventive interventions require a long follow-up period to assess the effects of the programs and investigators are reluctant to publish findings prematurely. However, if the theory, methods, and results are not published in a timely fashion, communities and practitioners have little access to this information and cannot use it in designing their local programs.
Manuals. The advantage of manuals is that they can include details of the prevention intervention method that journals may not be interested in but which are crucial in the replication of a program by other researchers and in the adoption of the program by a community. However, preparation of manuals is very time-consuming; it is difficult to get funding for their printing and distribution; and they receive little recognition by academic departments when reviewing researchers ' careers for promotion and tenure. The bibliography did not contain any entries for manuals. However, several of the researchers funded by the NIMH PRB, including those working within the PIRCs, have produced manuals. (See the abstracts in the background materials, available as indicated in Appendix D, for examples of programs that have manuals.)
Clearinghouses. There is no federal clearinghouse for published information on prevention of mental disorders. Table 11.3 lists several clearinghouses with materials relevant to prevention of mental disorders. The Center for Substance Abuse Prevention (CSAP, formerly OSAP) has one of the world's largest clearinghouses in its topic area, but little of its information deals with findings from rigorous preventive intervention research programs. The National Center on Child Abuse and Neglect (NCCAN) has a clearinghouse on child maltreatment literature, but only a small part of it is relevant to prevention. The National Prevention Coalition (NPC), a private, nonprofit organization affiliated with the National Mental Health Association, has the only clearinghouse that includes a concentrated focus on preventive intervention programs, and some of this material is research based. NPC currently has a grant from the Pew Foundation to provide program information to communities, but it does not have the capability to provide ongoing assistance on highly technical issues.
National Conferences. NIMH, NIDA, CSAP, and NIAAA hold national conferences focused on prevention, and others such as NCCAN have national conferences with some attention to prevention issues, but the crossover between agencies in each other's meetings is still rather
TABLE 11.3 Clearinghouses That Provide Information Related to the Prevention of Mental Disorders
|
CSAP National Resource Center for the Prevention of Perinatal Abuse of Alcohol and Other Drugs Center for Substance Abuse Prevention Substance Abuse and Mental Health Services Administration U.S. Department of Health and Human Services Lewin-VHI 9302 Lee Highway Suite 310 Fairfax, VA 22031 703-218-5600 Clearinghouse on Child Abuse and Neglect Information National Center on Child Abuse and Neglect U.S. Department of Health and Human Services P.O. Box 1182 Washington, DC 20013-1182 1-800-FYI-3366 Mental Health Policy Resource Center 1730 Rhode Island Avenue, NW Suite 308 Washington, DC 20036 202-775-8826 National Clearinghouse for Alcohol and Drug Information Center for Substance Abuse Prevention Substance Abuse and Mental Health Services Administration U.S. Department of Health and Human Services P.O. Box 2345 Rockville, MD 20847-2345 301-468-2600 National Committee to Prevent Child Abuse 332 South Michigan Avenue Suite 1600 Chicago, IL 60604 312-663-3520 National Criminal Justice Reference Service National Institute of Justice Clearinghouse Department of Justice 1600 Research Blvd Dept. F Rockville, MD 20850 1-800-851-3420 |
|
National Maternal and Child Health Clearinghouse Maternal and Child Health Bureau U.S. Department of Health and Human Services 8201 Greensboro Drive, Suite 600 McLean, VA 22102 703-821-8955 National Mental Health Association National Prevention Coalition 1021 Prince Street Alexandria, VA 22314-2971 703-684-7722 National Prevention Evaluation Research Collection Center for Substance Abuse Prevention Substance Abuse and Mental Health Services Administration U.S. Department of Health and Human Services Aspen Systems Corporation 1600 Research Blvd MS-1C Rockville, MD 20850 301-251-5180 National Resource Center on Worksite Health Promotion 777 North Capitol Street, NE Suite 800 Washington, DC 20002 202-408-9320 ODPHP National Health Information Center Office of Disease Prevention and Health Promotion U.S. Department of Health and Human Services P.O. Box 1133 Washington, DC 20013-1133 1-800-336-4797 Ontario Prevention Clearinghouse The Ministry of Community and Social Services 415 Yonge Street Suite 1200 Toronto, Ontario M5B 2E7 Canada 416-408-2121 Resource Center on Substance Abuse Prevention and Disability 1331 F Street, NW Suite 800 Washington, DC 20077-1514 202-783-2900 |
limited. There is, however, an increasing awareness of the need for more cross-fertilization of ideas and exchange of research data.
Working Directly with Researchers. After reviewing information sources regarding prevention programs, a community may choose to seek direct consultation with prevention researchers, especially those who have conducted the program the community is interested in adopting. Currently, however, there is no formal federally funded mechanism for researchers to work directly with communities to develop preventive interventions for mental disorders. Sometimes this interaction does take place on an ad hoc basis. The NIMH PRB has recognized the need to include plans for knowledge exchange in continuation grant applications of the PIRCs. SAMHSA's Center for Mental Health Services has indicated an interest in being a link between prevention researchers and communities. However, its current Prevention and Program Development Branch was not mandated in the ADAMHA reorganization, so its continued existence is not ensured, nor does it currently have its own funding. Prevention resources have been limited to discretionary management funds from the director 's office. The Centers for Disease Control and Prevention (CDC) works directly with communities through an extensive network of state public health departments on issues such as violence and suicide and has recently made a commitment to the scaling-up of the Infant Health and Development Program (see Chapter 7 and Chapter 10). The Department of Health and Human Services' Office of Disease Prevention and Health Promotion has disseminated some information on prevention of mental disorders but concentrates its efforts on physical disorders. At the state level, mental health departments or authorities are a possible mechanism for researchers to work directly with communities, but few states have made a significant commitment to prevention of mental disorders (Goldston, 1991).
Balancing Fidelity and Adaptability While Implementing the Program
Maintaining fidelity means that a program seeks to maintain the original tested model as closely as possible, whereas allowing adaptability means that a program is permitted to have leeway and is encouraged to use innovations wherever necessary to adjust to local circumstances. As mentioned in Chapter 10, Price and Lorion (1989) have proposed that the appropriate resolution of the fidelity versus adaptability dilemma requires distinguishing between the core elements of the intervention and the adaptable characteristics that can be adjusted to local circumstances.
|
BOX 11.1 Case Study: Replication of the Prenatal/Early Infancy Project “The Prenatal/Early Infancy Project in Elmira, New York, demonstrated impacts on birthweight, maternal health, reduction in child abuse, and improved maternal education or employment status when it was an experimental research program, but when the local health department took it over, the program was altered. As a demonstration project, the program had multiple sources of funding, including HHS, The Robert Wood Johnson Foundation, and the W. T. Grant Foundation. When the six-year grant funding ended in 1983, the local health department absorbed the program, while changing its definition and extent of services, target population, and caseload per home visitor. As a result of these changes, all of the original home visitors left within a few months. One director of county services told us that the program was no longer achieving the same reductions in low birthweight as the original project. “The program's absence of final evaluation data in 1983, reduced financial support, and location within the local health department all contributed to the changes. Some of these changes resulted from a reluctance to invest substantially in a program whose benefits had not yet been fully demonstrated at that time. But a difference in philosophy also prompted the change in program focus. Local officials told us there was not unanimous agreement with the research program's broad health and social service orientation and intensity. They also did not agree with limiting services to the target population of first-time mothers —particularly low-income, unmarried teen mothers—even though these women were among the ones who benefited most from the experimental program. Local officials believed that some minimum level of home-visiting services should be provided to a larger group of pregnant women, which may be diluting the overall impact of the formerly targeted, high-intensity services.” (GAO, 1990). |
Unfortunately, researchers have rarely described their prevention programs in these terms. Sometimes it may be possible in retrospect to distinguish between what is core technology and what is not. When these elements are not specified, it is left to the community practitioners to decide, not always with the best results. The accompanying case study (see Box 11.1) shows what can happen to a preventive intervention program when fidelity is not maintained. (See Chapter 7 for a description of the original program.)
Evaluating the Program's Effectiveness
Because the transfer of programs from research to community settings always necessitates some adaptation, if for no other reason than that
new personnel are involved, the success of the program should never be taken for granted. The true test of a prevention program is not the efficacy and effectiveness in the research setting but the effectiveness in the real-life setting with the community in charge of the program. To determine that effectiveness, a program evaluation is done after the program has been completed. Ideally, evaluation is also done at multiple points along the way while the preventive services are being delivered. To increase objectivity, at least some of the program evaluators should be external to the program delivery process. The program evaluators must be involved from the beginning of the program 's implementation in the community so they understand what the core elements and adaptable characteristics are. Ideally, such an evaluation not only critiques the prevention program but also provides feedback about the effects of the program on the needs and problems originally identified by the community.
Quality assurance and quality control are a major concern, especially as prevention programs are “reinvented.” These programs evolve and change in response to adaptations required by real-life exigencies. Thus quality assurance issues must be included in the documentation and evaluation of prevention programs that are installed in community settings. For example, it is essential that the goals and interventions are explicitly stated in written form; that documentation of the provision or delivery of the preventive interventions in the community fits the description of the interventions in the prevention program manual and provides a paper trail to audit the program's quality; and that all documentation be readily available for review.
Evaluation of a prevention program will ensure its quality if (1) there are frequent audits of the fidelity of the interventions to their program design; (2) there are in-person reviews of the program by senior-level personnel; (3) staff are held accountable for the quality of the preventive interventions; (4) the program designers and agency leadership are held accountable for achieving desired outcomes; and (5) opportunities exist for frequent reviews by all personnel to resolve problems, suggest changes, modify program design, and provide mutual support.
Providing Feedback to the Researchers
Researchers need to receive feedback from the community about their programs—the successes, the problems, and the creative solutions developed at the local level. It is also critical that they hear about current community needs so that when research priorities are set, these needs can be taken into consideration. The community can also raise ethical
issues, including selection of targeted populations, consideration of the values and interests of diverse cultures, and potential negative effects. (See the commissioned paper by Fawcett and colleagues, and the commentaries by Rothman and Gallimore, in the background materials, available as indicated in Appendix D.)
STRATEGIES FOR OVERCOMING BARRIERS TO THE KNOWLEDGE EXCHANGE PROCESS
There are many barriers to the knowledge exchange process. Barriers to the adoption of innovative and effective prevention programs include those related to the prevention programs themselves; to the practitioners, clinicians, educators, and administrators involved in the service delivery; and to the host organizations.
Barriers in the Prevention Program
One of the challenges to innovators in the prevention field will be to “package” their programs in such a way as to make them easy to disseminate and “user-friendly.” User-friendliness can be increased by encouraging second- and third-generation users of the program to reinvent the program to better fit the constraints and opportunities in the local jurisdiction. Giving those responsible for implementing a prevention program permission to adapt the program components to fit local conditions—as long as the adaptations do not jeopardize the fidelity of the key, effective core elements of the program—increases the likelihood that the program will be accepted by the community.
Another element that can increase user-friendliness is “packaging.” For widespread adoption of a prevention program to occur, the program needs to be packaged in a format that enables potential adopters or users to readily acquire the skills required for faithful utilization. Such packaging includes print materials with high degrees of specificity and operational description, audiovisual demonstrations of the methods in action, and well-designed workshops and training programs.
Barriers Related to the Practitioner, Clinician, Educator, or Administrator
Many attitudinal obstacles to the use of prevention programs can arise in a wide diversity of audiences. For example, prevention programs are sometimes viewed by clinicians and others in the mental health enterprise as foreign to their traditional mandate to “treat the sick.” Skepti-
cism and nihilism toward shifting resources to prevention are often expressed. Moreover, innovations in prevention programs that are complex, demanding, extended in time, and linked to a team for implementation can encounter problems in fidelity of delivery (Yeaton and Sechrest, 1981).
One of the keys to unlocking any potential opposition to engaging in preventive interventions is to provide relevant training to practitioners, educators, and other human service workers, equipping them with new knowledge, attitudes, and competences that will enable them to use the prevention programs with confidence. Thus, training the host of professional and paraprofessional interveners for prevention programs is a major requirement in elevating the status of prevention in mental health. One prerequisite for productive training or retraining of clinicians is to have trainers and consultants available who possess clinical credibility and administrative savvy and are readily recognized and respected by organization staff and managers alike. Teaching techniques—employing such methods as setting educational objectives, modeling or demonstrating the new skills to be learned, behavioral rehearsal with active coaching, and positive feedback for performance of the requisite skills (Kuehnel and Flanagan, 1984)—need to be used so that new competences can be successfully acquired and used.
Overcoming resistance among clinicians can also be achieved by a process of consultation and technical assistance similar in nature to that discussed in Chapter 10 at the point in the research cycle when trials are moved into the community. In the service arena the process before implementation of the prevention program includes (1) the identification of a relevant need in the target organization and among the organization's staff; (2) a feasibility assessment related to personal and organizational readiness for adoption of the prevention program; (3) the development of consensus for adoption of the prevention program; (4) the broadening of job descriptions and performance appraisals to include competences related to preventive interventions; and (5) the development of an implementation strategy.
Barriers Within the Host Organization
To overcome bureaucratic and other inertia within the institutions that will be the legitimate purveyors of prevention programs, a sine qua non is to have the active support of the host organization—from top management to local unit chiefs and team leaders. Support must be translated into oral and written endorsements of prevention as a priority within the organization's mission statement and long-term goals; con-
cordance with the philosophy and basic assumptions of prevention; and allocation of resources (including time, staff, space, and equipment), as enunciated in annual reports and statements of goals, that matches the priorities and support needs of the prevention program.
Also vital for successful implementation of prevention programming is the presence, within the organization, of an advocate of prevention who is a credible formal or informal leader in the organization. This person coordinates the initial efforts to introduce an innovative prevention program, consults with the experts who are disseminating the program, communicates with top management as well as with line-level staff to solve problems related to implementation, and offers training and encouragement to those applying the prevention program.
Staff roles must be defined by the functions explicitly described by the prevention program, and conflicts involving overlapping roles and disciplinary differences—as can arise on an interdisciplinary team—should be openly discussed and resolved. Resolution of staff conflicts can be facilitated by reconciling job descriptions with the competences needed for delivering the prevention program.
IMPROVING COMMUNITY ACCESS TO RESEARCH KNOWLEDGE
As described above, several existing federal and state institutions —such as SAMHSA's CSAP and CMHS, the Office of Disease Prevention and Health Promotion, the Centers for Disease Control and Prevention, and state mental health departments—are currently serving as brokers to communities of information provided by prevention researchers on intervention programs related to mental disorders. However, these efforts have been scattered, without mandate, and “catch-as-catch-can.” Perhaps the utilization of prevention programs in mental health can take cues from successful experiences in technology transfer found in other areas of our society. For example, in agriculture, field agents of a state university' s extension services work hand-in-hand with farmers to help them adopt new seeds, fertilizers, pesticides, equipment, and planting and harvesting techniques. Another example comes from the pharmaceutical industry, where “detail” sales representatives visit physicians in their offices and hospitals to provide information on new drugs and facilitate their adoption.
Any national research agenda for prevention of mental disorders will have to include the development of mechanisms for promoting the proper utilization and application of prevention technologies that have been validated in confirmatory, replication, and large-scale field trials. One model that could be considered is the concept of research knowl-
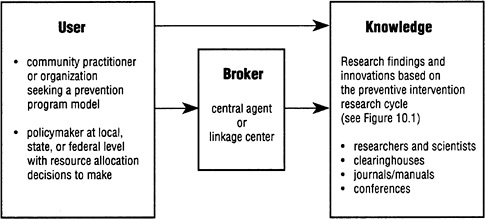
FIGURE 11.1 The process by which practitioners and policymakers access knowledge based on prevention research. Length of arrow indicates relative ease of access.
edge exchange centers, adapted from work by Liberman and Phipps (1987), which could be established regionally or nationally to serve as the broker, linkage center, or central agent between prevention researchers and scientists on the one hand, and practitioners, educators, administrators, and policymakers on the other. Figure 11.1 depicts a model that shows how such a center could provide this link.
Among the training and consulting roles that such a center would fill are (1) identifying new prevention programs from the scientific literature, clearinghouses, and conferences and from ongoing communication and liaison with innovators in the prevention field; (2) reviewing the quality of evidence regarding efficacy and effectiveness provided from the programs; (3) assisting “user communities” to choose and adapt prevention programs to fit their local constraints and resources and to ensure fidelity to the core characteristics of the program; (4) facilitating communities' evaluation of their prevention programs; and (5) using the feedback gained from working with the communities to assist researchers in refining and improving their prevention innovations so they can be ever more effective, efficient, and practical.
Of course, the community could go directly to the researchers and data sources themselves, but access to knowledge about effective preventive intervention research programs may be easier through a linkage center or broker. The amount and quality of interpersonal contacts between the linkage center or broker and the recipient organization may be critical to the successful adoption of the preventive program by the community.
CONCLUSION
The committee's examination of the knowledge exchange process uncovered a number of points worthy of special attention:
-
When a prevention research program is adopted for use as a community service program, issues of fidelity are paramount. Consideration of community needs and special populations becomes moot if a program is changed so much that it no longer is effective. Communities must be informed about the hazards of assuming that a program effective with one population will necessarily be generalizable to another.
-
Increased methodological rigor must be applied to the design of preventive intervention research programs over the next decade. This is likely to lead to more articles being published in high-quality journals.
-
Many research findings relevant to the prevention of mental disorders never have a chance to make an impact because they are never made known to the practitioners, educators, administrators, and policy makers who would use them. A coordinated plan for dissemination of the fruits of prevention research is needed, whether it be through existing institutions or newly created brokering or linkage centers.
-
In order for communities to learn how to obtain and make the best possible use of the research knowledge, they will need the help of a new breed of prevention program facilitator who can bridge research and practice.
REFERENCES
Battista, R. N.; Fletcher, S. W. ( 1988) Making recommendations on preventive practices: Methodological issues . In: R. N. Battista and R. S. Lawrence, Eds. Implementing Preventive Services. Suppl. to the American Journal of Preventive Medicine; 4(4). New York, NY: Oxford University Press; 53–67.
Buckner, J. C.; Trickett, E. J.; Corse, S. J. ( 1985) Primary Prevention in Mental Health: An Annotated Bibliography. Rockville, MD: DHHS Pub. No. (ADM) 85–1405.
GAO (Government Accounting Office). ( 1990) Home Visiting: A promising early intervention strategy for at-risk families. Report to the Chairman, Subcommittee on Labor, Health and Human Services, Education, and Related Agencies, Committee on Appropriations, U.S. Senate. GAO/HRD-90–93.
Goldston, S. E. ( 1991) A survey of prevention activities in state mental health authorities . Professional Psychology: Research and Practice; 22(4): 315–321.
Kuehnel, T. G.; Flanagan, S. G. ( 1984) Training the professionals: Guidelines for effective continuing education workshops. The Behavior Therapist; 7: 85–87.
Liberman, R. P.; Phipps, C. C. ( 1987) Innovative treatment and rehabilitation techniques for the chronic mentally ill. In: W. W. Merringer and G. Hannah, Eds. The Chronic Mental Patient—II. Washington, DC: American Psychiatric Press; 93–130.
Price, R. H.; Lorion, R. P. ( 1989) Prevention programming as organizational reinvention: From research to implementation. In: D. Shaffer, I. Philips, and N.B. Enzer, Eds. Prevention of Mental Disorders, Alcohol and other Drug Use in Children and Adolescents. Rockville, MD: Department of Health and Human Services.
Spitzer, W. O. ( 1979) Report of the Task Force on the Periodic Health Examination. Canadian Medical Association Journal; 121: 1193–1254.
Trickett, E. J.; Dahiyat, C.; Selby, P. (in press) Primary Prevention in Mental Health: An Annotated Bibliography. Rockville, MD: Department of Health and Human Services.
Yeaton, W. H.; Sechrest, L. ( 1981) Critical dimensions in the choice and maintenance of successful treatments: Strengths, integrity, effectiveness. Journal of Consulting and Clinical Psychology; 49: 156–167.






















